Embed Size (px)
Citation preview

NULL HYPOTHESIS CLASS OF EVIDENCE
Randomized placebo-controlled trial of theeffects of aspirin on dementia and cognitivedeclineJoanne Ryan PhD Elsdon Storey MB DPhil Anne M Murray MD MSc Robyn L Woods PhD
Rory Wolfe PhD Christopher M Reid PhD Mark R Nelson MB PhD Trevor TJ Chong MBBS PhD
Jeff D Williamson MD MHS Stephanie A Ward BMed MPH Jessica E Lockery MB BS
Suzanne G Orchard PhD Ruth Trevaks PhD Brenda Kirpach CCRA Anne B Newman MD MPH
Michael E Ernst PharmD John J McNeil MB PhD and Raj C ShahMD on behalf of the ASPREE Investigator Group
Neurologyreg 202095e320-e331 doi101212WNL0000000000009277
Correspondence
Dr Storey
elsdonstoreymonashedu
or Dr Ryan
joanneryanmonashedu
AbstractObjectiveTodetermine the effect of low-dose aspirin vs placebo on incident all-cause dementia incident Alzheimer disease (AD)mild cognitive impairment (MCI) and cognitive decline in older individuals
MethodsAspirin in Reducing Events in the Elderly (ASPREE) was a double-blind placebo-controlled trial of low-doseaspirin In the United States and Australia community-dwelling individuals aged ge70 years (US minorities ge65years) and free of cardiovascular disease physical disability and diagnosed dementia were enrolled Participantswere randomized 11ndash100 mg daily aspirin or placebo TheModifiedMini-Mental State Examination HopkinsVerbal Learning TestndashRevised Symbol Digit Modalities Test and Controlled Oral Word Association Testassessed cognition at baseline and over follow-up Additional cognitive testing was performed in participantswith suspected dementia (ldquotriggerrdquo) based on within-study assessments or clinical history Dementia wasadjudicated according to DSM-IV criteria National Institute on AgingndashAlzheimerrsquos Association criteria wereused for AD and MCI subclassification
ResultsA total of 19114 participants were followed over a median 47 years and 964 triggered further dementiaassessments There were 575 adjudicated dementia cases and 41 were classified as clinically probable ADThere was no substantial difference in the risk of all dementia triggers (hazard ratio [HR] 103 95 confidenceinterval [CI] 091ndash117) probable AD (HR 096 95 CI 074ndash124) or MCI (HR 112 95 CI 092ndash137)between aspirin and placebo Cognitive change over time was similar in the aspirin and placebo groups
ConclusionsThere was no evidence that aspirin was effective in reducing risk of dementia MCI or cognitive declineFollow-up of these outcomes after initial exposure is ongoing
Classification of evidenceThis study provides Class II evidence that for healthy older individuals low-dose aspirin does not significantlyreduce the incidence of dementia probable AD MCI or cognitive decline
Clinicaltrialsgov identifierNCT01038583
RELATED ARTICLE
EditorialThe quest for dementiaprevention does notinclude an aspirin a day
Page 105
MORE ONLINE
Class of EvidenceCriteria for ratingtherapeutic and diagnosticstudies
NPuborgcoe
These authors contributed equally to this work
From the School of Public Health and Preventive Medicine (JR ES RLW RW CMR SAW JEL SGO RT JJM) and the Turner Institute for Brain and Mental Health (TTJC)Monash University Melbourne Australia Berman Center for Outcomes and Clinical Research (AMM BK) Hennepin Health Research Institute Division of Geriatrics Departmentof Medicine (AMM BK) Hennepin Healthcare Minneapolis MN School of Public Health (CMR) Curtin University Perth Menzies Institute for Medical Research (MRN)University of Tasmania Hobart Australia Sticht Center on Aging and Alzheimerrsquos Prevention Section on Gerontology and Geriatric Medicine Department of Internal Medicine(JDW) Wake Forest School of Medicine Winston-Salem NC Center for Aging and Population Health (ABN) University of Pittsburgh PA Department of Pharmacy Practice andScience College of Pharmacy and the Department of Family Medicine Carver College of Medicine (MEE) University of Iowa Iowa City and Department of Family Medicine and RushAlzheimerrsquos Disease Center (RCS) Rush University Medical Center Chicago IL
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
Coinvestigators are listed in the appendix at the end of the article
This Null Hypothesis article is published as part of a collaborative effort between Neurologyreg and CBMRT
e320 Copyright copy 2020 American Academy of Neurology
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Low-dose aspirin is one of the most widely used treatmentsfor the secondary prevention of cardiovascular disease1 As ananti-inflammatory and antiplatelet agent aspirin also has thepotential to prevent or delay the onset of dementia In-flammation is one of the driving forces in Alzheimer disease(AD) pathology2 and aspirin may also act through a reductionin amyloid pathology3 A reduction in cerebrovascular diseaseincluding strokes with aspirin treatment may also help pre-vent vascular dementia4
Observational data have suggested that nonsteroidal anti-inflammatory drugs (NSAIDs) including aspirin may beneuroprotective reducing cognitive decline and incident de-mentia5 However there has been a dearth of large high-quality randomized controlled trials of NSAIDs particularlythose investigating the effects of low-dose aspirin6
The Aspirin in Reducing Events in the Elderly (ASPREE) trialwas a randomized placebo-controlled trial of low-dose aspirinin healthy older individuals We previously reported that as-pirin did not prolong disability-free survival nor did it de-crease the risk of incident dementia a component of thedisability-free survival composite endpoint7 However asdementia is a clinical syndrome with heterogeneous patho-logic causes the focus on all-cause dementia may dilute out aneffect on AD specifically Furthermore given the long pro-dromal stage in AD an effect earlier in the trajectory ofcognitive decline may have been overlooked Here we de-scribe the effect of aspirin on the prespecified secondaryoutcomes incident clinically probable and possible AD andmild cognitive impairment (MCI) as well as on the rate ofcognitive decline
MethodsStudy designFull details regarding the rationale and study design includingdetailed inclusion and exclusion criteria have been reportedpreviously78 In brief between March 2010 and December2014 initially healthy community-dwelling individuals aged70 years and over were identified through partnership withgt2000 general practitioners (GPs) in Australia and in theUnited States through clinic-based mailing lists electronicmedical screening and media advertisements9 For AfricanAmerican and Hispanic patients in the United States the agelimit was lowered to 65 years and over due to their higher riskof disease Individuals were then sent a letter inviting them to
participate in eligibility screening Eligibility criteria includedbeing free from cardiovascular disease and physical disabilityand being expected to survive for at least 5 years Individualswith a self-report or physician diagnosis of dementia at re-cruitment or with a Modified Mini-Mental State Examination(3MS)10 score of less than 78 were also ineligible There wereno other inclusionexclusion criteria for cognitive functionmeaning it was possible that some individuals had preva-lent MCI
The double-blind treatment phase of the trial initiallyscheduled to run for 5 years was stopped 6 months early bythe sponsor on June 12 2017 because of futility for the pri-mary composite outcome of disability-free survival (survivalfree from persistent physical disability dementia or death)
Randomization and treatment allocationEligible participants were enrolled in a 4-week run-in phasewhere adherence was monitored to placebo tablets theidentity of which was not disclosed to the participant Par-ticipants with 80 or higher compliance were then random-ized 11 to receive daily either 100 mg enteric coated aspirin(Bayer Pharma AG Leverkusen Germany) or an identical-appearing placebo tablet Block randomization with a com-puter-generated randomization procedure in Stata Statisticalsoftware (StataCorp College Station TX) was used and wasstratified according to location of general practice in Australiaregional site in the United States and age (65ndash79 or ge80years) to ensure balanced allocation across groups Partic-ipants study investigators and GPs were all blinded totreatment assignment for the entire period of the trial
Data were gathered through quarterly contact with partic-ipants by telephone and by annual in-person clinical assess-ments Monitoring of safety was conducted as describedpreviously7 with the trial sponsor (the National Institute onAging [NIA]) and an independent data and safety monitoringboard reviewing the reports on the accumulating data atregular intervals Site monitoring reports were reviewed by aninternational data management committee to monitor in-formation about adherence to the protocol and data quality
Standard protocol approvals registrationsand patient consentsThe study protocol was approved by institutional reviewboards in both countries and the NIH All participants pro-vided written informed consent The study is registered atClinicaltrialsgov (NCT01038583)
Glossary3MS = Modified Mini-Mental State Examination AD = Alzheimer disease ASPREE = Aspirin in Reducing Events in theElderly CI = confidence interval COWAT = Controlled Oral Word Association Test DSM-IV = Diagnostic and StatisticalManual of Mental Disorders 4th edition GP = general practitioner HR = hazard ratio HVLT-R = Hopkins Verbal LearningTestndashRevisedMCI =mild cognitive impairmentNIA =National Institute on AgingNSAID = nonsteroidal anti-inflammatorydrug SDMT = Symbol Digit Modalities Test
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e321
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Outcome measuresCognitive assessments were administered by trained andaccredited staff at baseline and year 1 and then biennially overthe follow-up period (year 3 year 5 and year 7 or close-outvisit in 2017) The cognitive battery included the 3MS tomeasure global cognition11 the Hopkins Verbal LearningTestndashRevised (HVLT-R)12 Delayed Recall task for episodicmemory the single letter (F) Controlled Oral Word Associ-ation Test (COWAT)13 for language and executive functionand the Symbol Digit Modalities Test (SDMT)14 to measurepsychomotor speed
Incident dementiaIndividuals with a suspected dementia diagnosis (ldquotriggerrdquo)were referred for further standardized cognitive and functionalassessments Dementia triggers were defined as a 3MS scorelt7815 a drop of more than 1015 points from the predictedscore based on their own baseline 3MS and after adjustment forage and education16 a report of memory concerns or othercognitive problems to a specialist or as noted on the partic-ipantrsquos medical records a clinician diagnosis of dementia orprescription of cholinesterase inhibitors (this latter criteria wasan automatic trigger in Australia as an AD diagnosis bya medical specialist was a requirement for a PharmaceuticalBenefits Scheme subsidized prescription in the United Statesthese were reviewed by the local sites to determine if the pre-scription was for a cognitive indication) Additional evaluationswere administered at least 6 weeks after the initial dementiatrigger to reduce the possibility of delirium These included theAlzheimerrsquos Disease Assessment ScalendashCognitive subscale17
Color Trails18 Lurian overlapping figures19 and the AlzheimerDisease Cooperative Study Activities of Daily Living scalecompleted by the participant and if available study partner20
Other documentation relevant to the dementia assessmentincluding laboratory tests brain CT or MRI the results ofblood tests and clinical case notes were also sought fromclinical providers and hospitals along with initial impression forcognitive change from the evaluating clinician
The available information was reviewed by the dementia ad-judication committee a panel of neurologists neuro-psychologists and geriatricians from Australia and the UnitedStates with expertise in dementia who were blinded to treat-ment allocation Dementia was adjudicated according to DSM-IV criteria21 This required evidence of memory impairmentplus evidence of at least one of the following aphasia apraxiaagnosia or executive dysfunction The cognitive impairmentsneeded to have caused significant impairment in social or oc-cupational functioning and to have represented a significantdecline from a previous level of functioning The date of di-agnosis of dementia was taken as the date the dementia triggeroccurred that resulted in a confirmed dementia diagnosis by theadjudication committee
Subclassification of dementiaWith supplementary funding in 2012 subclassification of alldementia cases into clinically probable and possible AD was
performed according to the 2011 NIAndashAlzheimerrsquos Associa-tion core clinical criteria22 This includes insidious onsetworsening over time and amnestic or nonamnestic pre-sentation Possible AD was classified as individuals who meetthe core AD criteria but with an atypical course or etiologicmixed presentation including those with neuroimaging con-sistent with moderate or marked cerebrovascular pathologyincluding white matter ischemia
Mild cognitive impairmentMCI was defined as participants with a dementia trigger whowere subsequently adjudicated as not reaching the dementiaendpoint by the dementia adjudication committee Sub-classification as MCI probably due to AD or ldquootherrdquo(including participants with evidence of functional decline orMCI not consistent with AD or insufficient information todetermine) was made using standard criteria23
Cognitive decline and changeIn participants without a dementia trigger we also definedthose with significant cognitive decline as a gt15 SD decline incognitive score from their own baseline value on the HVLT-RDelayed Recall SDMT or COWAT This definition did notinclude participants with evidence of only a transient decline(eg those with a gt15 SD drop at 1 follow-up but scoringabove this threshold at a subsequent follow-up)
Cognitive change was examined using the continuous scoreson each of the cognitive tests over the follow-up period
SubgroupsPrespecified subgroup analyses in the trial protocol includedsex (male vs female) age (below or median and above)country of recruitment (United States vs Australia) ethnicityrace (white vs African American vs HispanicLatino vs other)diabetes (no vs yes) hypertension (no vs yes) dyslipidemia(no vs yes) smoking (current vs former vs never) previousregular aspirin use (no vs yes) body mass index and frailtyusing adapted Fried frailty criteria (not frail vs prefrail vs frail)24
Statistical analysisAll analyses were restricted to events that occurred on or prior toJune 12 2017 during the intervention phase of the trial andcompared aspirin and placebo groups using an intention-to-treatapproach For the time-to-event analysis the difference betweenthe date at randomization to studymedication and the event wascalculated The sample size of 19000 was based on the primaryoutcome disability-free survival with 90 power to detecta hazard ratio of 123 comparing the aspirin and placebo groups
Cox proportional hazards regression models with time-to-event analysis were used to compare the aspirin and placebogroups Hazard ratios (HRs) were calculated for dementiatriggers and all-cause dementia A cumulative incidence func-tion was used to display the risk of dementia triggers or all-cause dementia based on a competing risks regression modelstratified by treatment group and allowing for the competing
e322 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
risk of death25 Proportional hazards assumptions were testedas a null hypothesis of zero slope in a regression of scaledSchoenfeld residuals against time all p values were found to begt01 indicating satisfaction of the assumption for all outcomes
Subgroup analysis was used to investigate the effect of aspirinvs placebo across prespecified subgroups24 An interactionterm in the Cox proportional hazards models provided anestimate of the effect heterogeneity between subgroups
Similar analyses were undertaken to investigate probable andpossible AD MCI and cognitive decline
Linear mixed models were used to compare change in cognitivefunction over time in the participants randomized to aspirin vsplacebo All randomized participants were included and con-tributed data to the estimation of intercepts at baseline and atfollow-ups when available Given the small number of partic-ipants who had cognitive assessment at the year 2 and year 7follow-ups (lt100 participants) the cognitive scores from thesetimepoints were not included in the analysis Each of the 4cognitive tests (3MS HVLT-R Delayed Recall SDMT andCOWAT) was investigated individually and we also analyzeda global composite measure derived using a summed z score
(average of the 4 tests) Composite scores are commonly used incognitive research as they have less variability than individualneuropsychological test scores and can reduce floor and ceilingeffects26 Each model included treatment group (aspirin vs pla-cebo) annual visittime (0 [baseline] 1 3 4 5 6) a participant-specific intercept (baseline score) and a participant-specificslope describing change in score over time (per annual visit) Toexamine whether the trajectory of cognitive scores for an averageparticipant differed between treatment groups a treatment bytime interaction was included in the model Analyses wereperformed using Stata software release 15 (StataCorp)
Classification of evidenceThis prospective randomized double-blind placebo-controlled clinical trial (ASPREE) assessed the effect oftreatment with 100 mg once daily enteric-coated aspirin vsplacebo over 5 years on the prespecified secondary outcomesincident dementia and MCI overall and in prespecified sub-groups An ancillary study (supplement awarded in 2012) toASPREE had a prespecified primary aim to examine the effectof daily low-dose aspirin on AD This study provides Class IIevidence that aspirin does not affect the incidence of probableAD MCI or cognitive decline over a median 47 years inindividuals aged ge65 years without dementia at baseline
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of participants in the Aspirin in ReducingEvents in the Elderly (ASPREE) trial
All randomized participants were included in the final analysis For participants who withdrew from the trial or died all information up to the point ofwithdrawaldeath was included in the analysis
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e323
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Data availabilityAll individual participant data (re-identifiable) that underlie theresults reported in this article are available upon request toqualified researchers without limit of time subject to approval ofthe analyses by the principal investigators and a standard datasharing agreement Details regarding requests to access the datawill be available through the study web site (ASPREEorg) Thedata will then bemade available through a web-based data portalsafe haven at Monash University Australia The ASPREE trialprotocol and statistical analysis plan have been published7
ResultsStudy participantsA total of 19114 participants were recruited with 9525 ran-domized to aspirin and 9589 to placebo (figure 1) Participantsranged in age from 65 to 98 years and 874 were recruited inAustralia No significant differences were identified in baselinecharacteristics between participants randomized to aspirin andplacebo including health factors and cognitive performancethat may predispose to cognitive impairment (table 1)
The median duration of follow-up was the same in the 2 groups(47 years interquartile range 36ndash57 years) At the end of thefollow-up period face-to-face visits were still being conductedon 82 of participants 97 via review of medical records onlyand 55 had died (11) Loss to follow-up was defined as nocontact with participants either in person or by phone in the12 months before the end of the trial period (June 12 2017)and no record of the participant having attended the medicalpractice within the last 12 months Only 12 of participantswithdrew consent for any follow-up and this was balancedacross the 2 study groups (figure 1) As reported previouslyaspirin did not prolong disability-free survival (HR 101 95confidence interval [CI] 092ndash111)7
Incident dementia and probable ADIn the aspirin group 488 participants (116 per 1000person-years) reached the dementia trigger criteria com-pared with 476 participants (113 per 1000 person-years) inthe placebo group (HR 103 95 CI 091ndash117) The typeof dementia trigger was similar across the aspirin and placebogroups with similar rates of reported memory problems (44and 46 per 1000 person-years respectively) 3MS score lt78(41 and 43 per 1000 person-years respectively) gt10-pointdrop in predicted 3MS from baseline (15 and 17 per 1000person-years respectively) and prescribed a cholinesteraseinhibitor (10 and 07 per 1000 person-years respectively)
The rate of incident dementia in the aspirin group was 67 eventsper 1000 person-years and in the placebo group 69 events per1000 person-years (table 2) Fewer than half of all adjudicateddementia cases (41) were classified as clinically probable AD
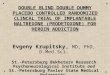
The 95 CI for HR indicating the difference in the risk ofincident clinically probable AD and possible AD in the aspirinand placebo groups overlaps 10 (figure 2)
There were no significant interactions between treatmentgroup and any prespecified subgroup for dementia (figure 3)or probable AD (data not shown) with the exception offrailty but in this latter case the direction of effect was in-consistent across frailty categories
Table 1 Selected participant characteristics atrandomization according to treatment groupa
Aspirin(n = 9525)
Placebo(n = 9589)
Ethno-racial group n ()
Australian white 8169 (858) 8193 (854)
US white 539 (57) 549 (57)
African American 451 (47) 450 (47)
HispanicLatino 240 (25) 248 (26)
Other 126 (13) 149 (16)
Age y n ()
65ndash69b 284 (30) 280 (29)
65ndash74 5243 (550) 5356 (559)
75ndash84 3618 (380) 3601 (376)
ge85 380 (40) 352 (37)
Education y n ()
lt12 4307 (452) 4329 (452)
12ndash15 2802 (294) 2772 (289)
16+ 2415 (254) 2488 (260)
Male n () 4152 (436) 4180 (436)
Drinks alcohol n () 7309 (767) 7333 (765)
Current or past smoker n () 4261 (447) 4273 (446)
Obese ge30 kgm2 n () 2820 (297) 2857 (299)
Depression n ()c 925 (97) 954 (100)
3MS mean (SD) 934 (47) 935 (46)
COWAT mean (SD) 121 (46) 121 (46)
SDMT mean (SD) 367 (101) 368 (102)
HVLT-R mean (SD)
Total recall 225 (55) 225 (55)
Delayed Recall 77 (28) 77 (28)
Retention 832 (222) 833 (221)
RDI 107 (17) 107 (18)
Abbreviations 3MS = Modified Mini-Mental State Examination COWAT =Controlled Oral Word Association Test HVLT-R = Hopkins Verbal LearningTestndashRevised RDI = Recognition Discrimination Index SDMT = Symbol DigitModalities Testa Prior published data indicate no difference by trial group for a range of otherhealth conditions including diabetes hypertension and body mass index7b All US ethnic minoritiesc Depression was defined as a score of ge8 on the 10-item Center for Epide-miologic Studies Depression Scale (CES-D-10)
e324 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
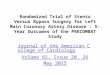
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Low-dose aspirin is one of the most widely used treatmentsfor the secondary prevention of cardiovascular disease1 As ananti-inflammatory and antiplatelet agent aspirin also has thepotential to prevent or delay the onset of dementia In-flammation is one of the driving forces in Alzheimer disease(AD) pathology2 and aspirin may also act through a reductionin amyloid pathology3 A reduction in cerebrovascular diseaseincluding strokes with aspirin treatment may also help pre-vent vascular dementia4
Observational data have suggested that nonsteroidal anti-inflammatory drugs (NSAIDs) including aspirin may beneuroprotective reducing cognitive decline and incident de-mentia5 However there has been a dearth of large high-quality randomized controlled trials of NSAIDs particularlythose investigating the effects of low-dose aspirin6
The Aspirin in Reducing Events in the Elderly (ASPREE) trialwas a randomized placebo-controlled trial of low-dose aspirinin healthy older individuals We previously reported that as-pirin did not prolong disability-free survival nor did it de-crease the risk of incident dementia a component of thedisability-free survival composite endpoint7 However asdementia is a clinical syndrome with heterogeneous patho-logic causes the focus on all-cause dementia may dilute out aneffect on AD specifically Furthermore given the long pro-dromal stage in AD an effect earlier in the trajectory ofcognitive decline may have been overlooked Here we de-scribe the effect of aspirin on the prespecified secondaryoutcomes incident clinically probable and possible AD andmild cognitive impairment (MCI) as well as on the rate ofcognitive decline
MethodsStudy designFull details regarding the rationale and study design includingdetailed inclusion and exclusion criteria have been reportedpreviously78 In brief between March 2010 and December2014 initially healthy community-dwelling individuals aged70 years and over were identified through partnership withgt2000 general practitioners (GPs) in Australia and in theUnited States through clinic-based mailing lists electronicmedical screening and media advertisements9 For AfricanAmerican and Hispanic patients in the United States the agelimit was lowered to 65 years and over due to their higher riskof disease Individuals were then sent a letter inviting them to
participate in eligibility screening Eligibility criteria includedbeing free from cardiovascular disease and physical disabilityand being expected to survive for at least 5 years Individualswith a self-report or physician diagnosis of dementia at re-cruitment or with a Modified Mini-Mental State Examination(3MS)10 score of less than 78 were also ineligible There wereno other inclusionexclusion criteria for cognitive functionmeaning it was possible that some individuals had preva-lent MCI
The double-blind treatment phase of the trial initiallyscheduled to run for 5 years was stopped 6 months early bythe sponsor on June 12 2017 because of futility for the pri-mary composite outcome of disability-free survival (survivalfree from persistent physical disability dementia or death)
Randomization and treatment allocationEligible participants were enrolled in a 4-week run-in phasewhere adherence was monitored to placebo tablets theidentity of which was not disclosed to the participant Par-ticipants with 80 or higher compliance were then random-ized 11 to receive daily either 100 mg enteric coated aspirin(Bayer Pharma AG Leverkusen Germany) or an identical-appearing placebo tablet Block randomization with a com-puter-generated randomization procedure in Stata Statisticalsoftware (StataCorp College Station TX) was used and wasstratified according to location of general practice in Australiaregional site in the United States and age (65ndash79 or ge80years) to ensure balanced allocation across groups Partic-ipants study investigators and GPs were all blinded totreatment assignment for the entire period of the trial
Data were gathered through quarterly contact with partic-ipants by telephone and by annual in-person clinical assess-ments Monitoring of safety was conducted as describedpreviously7 with the trial sponsor (the National Institute onAging [NIA]) and an independent data and safety monitoringboard reviewing the reports on the accumulating data atregular intervals Site monitoring reports were reviewed by aninternational data management committee to monitor in-formation about adherence to the protocol and data quality
Standard protocol approvals registrationsand patient consentsThe study protocol was approved by institutional reviewboards in both countries and the NIH All participants pro-vided written informed consent The study is registered atClinicaltrialsgov (NCT01038583)
Glossary3MS = Modified Mini-Mental State Examination AD = Alzheimer disease ASPREE = Aspirin in Reducing Events in theElderly CI = confidence interval COWAT = Controlled Oral Word Association Test DSM-IV = Diagnostic and StatisticalManual of Mental Disorders 4th edition GP = general practitioner HR = hazard ratio HVLT-R = Hopkins Verbal LearningTestndashRevisedMCI =mild cognitive impairmentNIA =National Institute on AgingNSAID = nonsteroidal anti-inflammatorydrug SDMT = Symbol Digit Modalities Test
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e321
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Outcome measuresCognitive assessments were administered by trained andaccredited staff at baseline and year 1 and then biennially overthe follow-up period (year 3 year 5 and year 7 or close-outvisit in 2017) The cognitive battery included the 3MS tomeasure global cognition11 the Hopkins Verbal LearningTestndashRevised (HVLT-R)12 Delayed Recall task for episodicmemory the single letter (F) Controlled Oral Word Associ-ation Test (COWAT)13 for language and executive functionand the Symbol Digit Modalities Test (SDMT)14 to measurepsychomotor speed
Incident dementiaIndividuals with a suspected dementia diagnosis (ldquotriggerrdquo)were referred for further standardized cognitive and functionalassessments Dementia triggers were defined as a 3MS scorelt7815 a drop of more than 1015 points from the predictedscore based on their own baseline 3MS and after adjustment forage and education16 a report of memory concerns or othercognitive problems to a specialist or as noted on the partic-ipantrsquos medical records a clinician diagnosis of dementia orprescription of cholinesterase inhibitors (this latter criteria wasan automatic trigger in Australia as an AD diagnosis bya medical specialist was a requirement for a PharmaceuticalBenefits Scheme subsidized prescription in the United Statesthese were reviewed by the local sites to determine if the pre-scription was for a cognitive indication) Additional evaluationswere administered at least 6 weeks after the initial dementiatrigger to reduce the possibility of delirium These included theAlzheimerrsquos Disease Assessment ScalendashCognitive subscale17
Color Trails18 Lurian overlapping figures19 and the AlzheimerDisease Cooperative Study Activities of Daily Living scalecompleted by the participant and if available study partner20
Other documentation relevant to the dementia assessmentincluding laboratory tests brain CT or MRI the results ofblood tests and clinical case notes were also sought fromclinical providers and hospitals along with initial impression forcognitive change from the evaluating clinician
The available information was reviewed by the dementia ad-judication committee a panel of neurologists neuro-psychologists and geriatricians from Australia and the UnitedStates with expertise in dementia who were blinded to treat-ment allocation Dementia was adjudicated according to DSM-IV criteria21 This required evidence of memory impairmentplus evidence of at least one of the following aphasia apraxiaagnosia or executive dysfunction The cognitive impairmentsneeded to have caused significant impairment in social or oc-cupational functioning and to have represented a significantdecline from a previous level of functioning The date of di-agnosis of dementia was taken as the date the dementia triggeroccurred that resulted in a confirmed dementia diagnosis by theadjudication committee
Subclassification of dementiaWith supplementary funding in 2012 subclassification of alldementia cases into clinically probable and possible AD was
performed according to the 2011 NIAndashAlzheimerrsquos Associa-tion core clinical criteria22 This includes insidious onsetworsening over time and amnestic or nonamnestic pre-sentation Possible AD was classified as individuals who meetthe core AD criteria but with an atypical course or etiologicmixed presentation including those with neuroimaging con-sistent with moderate or marked cerebrovascular pathologyincluding white matter ischemia
Mild cognitive impairmentMCI was defined as participants with a dementia trigger whowere subsequently adjudicated as not reaching the dementiaendpoint by the dementia adjudication committee Sub-classification as MCI probably due to AD or ldquootherrdquo(including participants with evidence of functional decline orMCI not consistent with AD or insufficient information todetermine) was made using standard criteria23
Cognitive decline and changeIn participants without a dementia trigger we also definedthose with significant cognitive decline as a gt15 SD decline incognitive score from their own baseline value on the HVLT-RDelayed Recall SDMT or COWAT This definition did notinclude participants with evidence of only a transient decline(eg those with a gt15 SD drop at 1 follow-up but scoringabove this threshold at a subsequent follow-up)
Cognitive change was examined using the continuous scoreson each of the cognitive tests over the follow-up period
SubgroupsPrespecified subgroup analyses in the trial protocol includedsex (male vs female) age (below or median and above)country of recruitment (United States vs Australia) ethnicityrace (white vs African American vs HispanicLatino vs other)diabetes (no vs yes) hypertension (no vs yes) dyslipidemia(no vs yes) smoking (current vs former vs never) previousregular aspirin use (no vs yes) body mass index and frailtyusing adapted Fried frailty criteria (not frail vs prefrail vs frail)24
Statistical analysisAll analyses were restricted to events that occurred on or prior toJune 12 2017 during the intervention phase of the trial andcompared aspirin and placebo groups using an intention-to-treatapproach For the time-to-event analysis the difference betweenthe date at randomization to studymedication and the event wascalculated The sample size of 19000 was based on the primaryoutcome disability-free survival with 90 power to detecta hazard ratio of 123 comparing the aspirin and placebo groups
Cox proportional hazards regression models with time-to-event analysis were used to compare the aspirin and placebogroups Hazard ratios (HRs) were calculated for dementiatriggers and all-cause dementia A cumulative incidence func-tion was used to display the risk of dementia triggers or all-cause dementia based on a competing risks regression modelstratified by treatment group and allowing for the competing
e322 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
risk of death25 Proportional hazards assumptions were testedas a null hypothesis of zero slope in a regression of scaledSchoenfeld residuals against time all p values were found to begt01 indicating satisfaction of the assumption for all outcomes
Subgroup analysis was used to investigate the effect of aspirinvs placebo across prespecified subgroups24 An interactionterm in the Cox proportional hazards models provided anestimate of the effect heterogeneity between subgroups
Similar analyses were undertaken to investigate probable andpossible AD MCI and cognitive decline
Linear mixed models were used to compare change in cognitivefunction over time in the participants randomized to aspirin vsplacebo All randomized participants were included and con-tributed data to the estimation of intercepts at baseline and atfollow-ups when available Given the small number of partic-ipants who had cognitive assessment at the year 2 and year 7follow-ups (lt100 participants) the cognitive scores from thesetimepoints were not included in the analysis Each of the 4cognitive tests (3MS HVLT-R Delayed Recall SDMT andCOWAT) was investigated individually and we also analyzeda global composite measure derived using a summed z score
(average of the 4 tests) Composite scores are commonly used incognitive research as they have less variability than individualneuropsychological test scores and can reduce floor and ceilingeffects26 Each model included treatment group (aspirin vs pla-cebo) annual visittime (0 [baseline] 1 3 4 5 6) a participant-specific intercept (baseline score) and a participant-specificslope describing change in score over time (per annual visit) Toexamine whether the trajectory of cognitive scores for an averageparticipant differed between treatment groups a treatment bytime interaction was included in the model Analyses wereperformed using Stata software release 15 (StataCorp)
Classification of evidenceThis prospective randomized double-blind placebo-controlled clinical trial (ASPREE) assessed the effect oftreatment with 100 mg once daily enteric-coated aspirin vsplacebo over 5 years on the prespecified secondary outcomesincident dementia and MCI overall and in prespecified sub-groups An ancillary study (supplement awarded in 2012) toASPREE had a prespecified primary aim to examine the effectof daily low-dose aspirin on AD This study provides Class IIevidence that aspirin does not affect the incidence of probableAD MCI or cognitive decline over a median 47 years inindividuals aged ge65 years without dementia at baseline
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of participants in the Aspirin in ReducingEvents in the Elderly (ASPREE) trial
All randomized participants were included in the final analysis For participants who withdrew from the trial or died all information up to the point ofwithdrawaldeath was included in the analysis
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e323
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Data availabilityAll individual participant data (re-identifiable) that underlie theresults reported in this article are available upon request toqualified researchers without limit of time subject to approval ofthe analyses by the principal investigators and a standard datasharing agreement Details regarding requests to access the datawill be available through the study web site (ASPREEorg) Thedata will then bemade available through a web-based data portalsafe haven at Monash University Australia The ASPREE trialprotocol and statistical analysis plan have been published7
ResultsStudy participantsA total of 19114 participants were recruited with 9525 ran-domized to aspirin and 9589 to placebo (figure 1) Participantsranged in age from 65 to 98 years and 874 were recruited inAustralia No significant differences were identified in baselinecharacteristics between participants randomized to aspirin andplacebo including health factors and cognitive performancethat may predispose to cognitive impairment (table 1)
The median duration of follow-up was the same in the 2 groups(47 years interquartile range 36ndash57 years) At the end of thefollow-up period face-to-face visits were still being conductedon 82 of participants 97 via review of medical records onlyand 55 had died (11) Loss to follow-up was defined as nocontact with participants either in person or by phone in the12 months before the end of the trial period (June 12 2017)and no record of the participant having attended the medicalpractice within the last 12 months Only 12 of participantswithdrew consent for any follow-up and this was balancedacross the 2 study groups (figure 1) As reported previouslyaspirin did not prolong disability-free survival (HR 101 95confidence interval [CI] 092ndash111)7
Incident dementia and probable ADIn the aspirin group 488 participants (116 per 1000person-years) reached the dementia trigger criteria com-pared with 476 participants (113 per 1000 person-years) inthe placebo group (HR 103 95 CI 091ndash117) The typeof dementia trigger was similar across the aspirin and placebogroups with similar rates of reported memory problems (44and 46 per 1000 person-years respectively) 3MS score lt78(41 and 43 per 1000 person-years respectively) gt10-pointdrop in predicted 3MS from baseline (15 and 17 per 1000person-years respectively) and prescribed a cholinesteraseinhibitor (10 and 07 per 1000 person-years respectively)
The rate of incident dementia in the aspirin group was 67 eventsper 1000 person-years and in the placebo group 69 events per1000 person-years (table 2) Fewer than half of all adjudicateddementia cases (41) were classified as clinically probable AD
The 95 CI for HR indicating the difference in the risk ofincident clinically probable AD and possible AD in the aspirinand placebo groups overlaps 10 (figure 2)
There were no significant interactions between treatmentgroup and any prespecified subgroup for dementia (figure 3)or probable AD (data not shown) with the exception offrailty but in this latter case the direction of effect was in-consistent across frailty categories
Table 1 Selected participant characteristics atrandomization according to treatment groupa
Aspirin(n = 9525)
Placebo(n = 9589)
Ethno-racial group n ()
Australian white 8169 (858) 8193 (854)
US white 539 (57) 549 (57)
African American 451 (47) 450 (47)
HispanicLatino 240 (25) 248 (26)
Other 126 (13) 149 (16)
Age y n ()
65ndash69b 284 (30) 280 (29)
65ndash74 5243 (550) 5356 (559)
75ndash84 3618 (380) 3601 (376)
ge85 380 (40) 352 (37)
Education y n ()
lt12 4307 (452) 4329 (452)
12ndash15 2802 (294) 2772 (289)
16+ 2415 (254) 2488 (260)
Male n () 4152 (436) 4180 (436)
Drinks alcohol n () 7309 (767) 7333 (765)
Current or past smoker n () 4261 (447) 4273 (446)
Obese ge30 kgm2 n () 2820 (297) 2857 (299)
Depression n ()c 925 (97) 954 (100)
3MS mean (SD) 934 (47) 935 (46)
COWAT mean (SD) 121 (46) 121 (46)
SDMT mean (SD) 367 (101) 368 (102)
HVLT-R mean (SD)
Total recall 225 (55) 225 (55)
Delayed Recall 77 (28) 77 (28)
Retention 832 (222) 833 (221)
RDI 107 (17) 107 (18)
Abbreviations 3MS = Modified Mini-Mental State Examination COWAT =Controlled Oral Word Association Test HVLT-R = Hopkins Verbal LearningTestndashRevised RDI = Recognition Discrimination Index SDMT = Symbol DigitModalities Testa Prior published data indicate no difference by trial group for a range of otherhealth conditions including diabetes hypertension and body mass index7b All US ethnic minoritiesc Depression was defined as a score of ge8 on the 10-item Center for Epide-miologic Studies Depression Scale (CES-D-10)
e324 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Outcome measuresCognitive assessments were administered by trained andaccredited staff at baseline and year 1 and then biennially overthe follow-up period (year 3 year 5 and year 7 or close-outvisit in 2017) The cognitive battery included the 3MS tomeasure global cognition11 the Hopkins Verbal LearningTestndashRevised (HVLT-R)12 Delayed Recall task for episodicmemory the single letter (F) Controlled Oral Word Associ-ation Test (COWAT)13 for language and executive functionand the Symbol Digit Modalities Test (SDMT)14 to measurepsychomotor speed
Incident dementiaIndividuals with a suspected dementia diagnosis (ldquotriggerrdquo)were referred for further standardized cognitive and functionalassessments Dementia triggers were defined as a 3MS scorelt7815 a drop of more than 1015 points from the predictedscore based on their own baseline 3MS and after adjustment forage and education16 a report of memory concerns or othercognitive problems to a specialist or as noted on the partic-ipantrsquos medical records a clinician diagnosis of dementia orprescription of cholinesterase inhibitors (this latter criteria wasan automatic trigger in Australia as an AD diagnosis bya medical specialist was a requirement for a PharmaceuticalBenefits Scheme subsidized prescription in the United Statesthese were reviewed by the local sites to determine if the pre-scription was for a cognitive indication) Additional evaluationswere administered at least 6 weeks after the initial dementiatrigger to reduce the possibility of delirium These included theAlzheimerrsquos Disease Assessment ScalendashCognitive subscale17
Color Trails18 Lurian overlapping figures19 and the AlzheimerDisease Cooperative Study Activities of Daily Living scalecompleted by the participant and if available study partner20
Other documentation relevant to the dementia assessmentincluding laboratory tests brain CT or MRI the results ofblood tests and clinical case notes were also sought fromclinical providers and hospitals along with initial impression forcognitive change from the evaluating clinician
The available information was reviewed by the dementia ad-judication committee a panel of neurologists neuro-psychologists and geriatricians from Australia and the UnitedStates with expertise in dementia who were blinded to treat-ment allocation Dementia was adjudicated according to DSM-IV criteria21 This required evidence of memory impairmentplus evidence of at least one of the following aphasia apraxiaagnosia or executive dysfunction The cognitive impairmentsneeded to have caused significant impairment in social or oc-cupational functioning and to have represented a significantdecline from a previous level of functioning The date of di-agnosis of dementia was taken as the date the dementia triggeroccurred that resulted in a confirmed dementia diagnosis by theadjudication committee
Subclassification of dementiaWith supplementary funding in 2012 subclassification of alldementia cases into clinically probable and possible AD was
performed according to the 2011 NIAndashAlzheimerrsquos Associa-tion core clinical criteria22 This includes insidious onsetworsening over time and amnestic or nonamnestic pre-sentation Possible AD was classified as individuals who meetthe core AD criteria but with an atypical course or etiologicmixed presentation including those with neuroimaging con-sistent with moderate or marked cerebrovascular pathologyincluding white matter ischemia
Mild cognitive impairmentMCI was defined as participants with a dementia trigger whowere subsequently adjudicated as not reaching the dementiaendpoint by the dementia adjudication committee Sub-classification as MCI probably due to AD or ldquootherrdquo(including participants with evidence of functional decline orMCI not consistent with AD or insufficient information todetermine) was made using standard criteria23
Cognitive decline and changeIn participants without a dementia trigger we also definedthose with significant cognitive decline as a gt15 SD decline incognitive score from their own baseline value on the HVLT-RDelayed Recall SDMT or COWAT This definition did notinclude participants with evidence of only a transient decline(eg those with a gt15 SD drop at 1 follow-up but scoringabove this threshold at a subsequent follow-up)
Cognitive change was examined using the continuous scoreson each of the cognitive tests over the follow-up period
SubgroupsPrespecified subgroup analyses in the trial protocol includedsex (male vs female) age (below or median and above)country of recruitment (United States vs Australia) ethnicityrace (white vs African American vs HispanicLatino vs other)diabetes (no vs yes) hypertension (no vs yes) dyslipidemia(no vs yes) smoking (current vs former vs never) previousregular aspirin use (no vs yes) body mass index and frailtyusing adapted Fried frailty criteria (not frail vs prefrail vs frail)24
Statistical analysisAll analyses were restricted to events that occurred on or prior toJune 12 2017 during the intervention phase of the trial andcompared aspirin and placebo groups using an intention-to-treatapproach For the time-to-event analysis the difference betweenthe date at randomization to studymedication and the event wascalculated The sample size of 19000 was based on the primaryoutcome disability-free survival with 90 power to detecta hazard ratio of 123 comparing the aspirin and placebo groups
Cox proportional hazards regression models with time-to-event analysis were used to compare the aspirin and placebogroups Hazard ratios (HRs) were calculated for dementiatriggers and all-cause dementia A cumulative incidence func-tion was used to display the risk of dementia triggers or all-cause dementia based on a competing risks regression modelstratified by treatment group and allowing for the competing
e322 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
risk of death25 Proportional hazards assumptions were testedas a null hypothesis of zero slope in a regression of scaledSchoenfeld residuals against time all p values were found to begt01 indicating satisfaction of the assumption for all outcomes
Subgroup analysis was used to investigate the effect of aspirinvs placebo across prespecified subgroups24 An interactionterm in the Cox proportional hazards models provided anestimate of the effect heterogeneity between subgroups
Similar analyses were undertaken to investigate probable andpossible AD MCI and cognitive decline
Linear mixed models were used to compare change in cognitivefunction over time in the participants randomized to aspirin vsplacebo All randomized participants were included and con-tributed data to the estimation of intercepts at baseline and atfollow-ups when available Given the small number of partic-ipants who had cognitive assessment at the year 2 and year 7follow-ups (lt100 participants) the cognitive scores from thesetimepoints were not included in the analysis Each of the 4cognitive tests (3MS HVLT-R Delayed Recall SDMT andCOWAT) was investigated individually and we also analyzeda global composite measure derived using a summed z score
(average of the 4 tests) Composite scores are commonly used incognitive research as they have less variability than individualneuropsychological test scores and can reduce floor and ceilingeffects26 Each model included treatment group (aspirin vs pla-cebo) annual visittime (0 [baseline] 1 3 4 5 6) a participant-specific intercept (baseline score) and a participant-specificslope describing change in score over time (per annual visit) Toexamine whether the trajectory of cognitive scores for an averageparticipant differed between treatment groups a treatment bytime interaction was included in the model Analyses wereperformed using Stata software release 15 (StataCorp)
Classification of evidenceThis prospective randomized double-blind placebo-controlled clinical trial (ASPREE) assessed the effect oftreatment with 100 mg once daily enteric-coated aspirin vsplacebo over 5 years on the prespecified secondary outcomesincident dementia and MCI overall and in prespecified sub-groups An ancillary study (supplement awarded in 2012) toASPREE had a prespecified primary aim to examine the effectof daily low-dose aspirin on AD This study provides Class IIevidence that aspirin does not affect the incidence of probableAD MCI or cognitive decline over a median 47 years inindividuals aged ge65 years without dementia at baseline
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of participants in the Aspirin in ReducingEvents in the Elderly (ASPREE) trial
All randomized participants were included in the final analysis For participants who withdrew from the trial or died all information up to the point ofwithdrawaldeath was included in the analysis
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e323
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Data availabilityAll individual participant data (re-identifiable) that underlie theresults reported in this article are available upon request toqualified researchers without limit of time subject to approval ofthe analyses by the principal investigators and a standard datasharing agreement Details regarding requests to access the datawill be available through the study web site (ASPREEorg) Thedata will then bemade available through a web-based data portalsafe haven at Monash University Australia The ASPREE trialprotocol and statistical analysis plan have been published7
ResultsStudy participantsA total of 19114 participants were recruited with 9525 ran-domized to aspirin and 9589 to placebo (figure 1) Participantsranged in age from 65 to 98 years and 874 were recruited inAustralia No significant differences were identified in baselinecharacteristics between participants randomized to aspirin andplacebo including health factors and cognitive performancethat may predispose to cognitive impairment (table 1)
The median duration of follow-up was the same in the 2 groups(47 years interquartile range 36ndash57 years) At the end of thefollow-up period face-to-face visits were still being conductedon 82 of participants 97 via review of medical records onlyand 55 had died (11) Loss to follow-up was defined as nocontact with participants either in person or by phone in the12 months before the end of the trial period (June 12 2017)and no record of the participant having attended the medicalpractice within the last 12 months Only 12 of participantswithdrew consent for any follow-up and this was balancedacross the 2 study groups (figure 1) As reported previouslyaspirin did not prolong disability-free survival (HR 101 95confidence interval [CI] 092ndash111)7
Incident dementia and probable ADIn the aspirin group 488 participants (116 per 1000person-years) reached the dementia trigger criteria com-pared with 476 participants (113 per 1000 person-years) inthe placebo group (HR 103 95 CI 091ndash117) The typeof dementia trigger was similar across the aspirin and placebogroups with similar rates of reported memory problems (44and 46 per 1000 person-years respectively) 3MS score lt78(41 and 43 per 1000 person-years respectively) gt10-pointdrop in predicted 3MS from baseline (15 and 17 per 1000person-years respectively) and prescribed a cholinesteraseinhibitor (10 and 07 per 1000 person-years respectively)
The rate of incident dementia in the aspirin group was 67 eventsper 1000 person-years and in the placebo group 69 events per1000 person-years (table 2) Fewer than half of all adjudicateddementia cases (41) were classified as clinically probable AD
The 95 CI for HR indicating the difference in the risk ofincident clinically probable AD and possible AD in the aspirinand placebo groups overlaps 10 (figure 2)
There were no significant interactions between treatmentgroup and any prespecified subgroup for dementia (figure 3)or probable AD (data not shown) with the exception offrailty but in this latter case the direction of effect was in-consistent across frailty categories
Table 1 Selected participant characteristics atrandomization according to treatment groupa
Aspirin(n = 9525)
Placebo(n = 9589)
Ethno-racial group n ()
Australian white 8169 (858) 8193 (854)
US white 539 (57) 549 (57)
African American 451 (47) 450 (47)
HispanicLatino 240 (25) 248 (26)
Other 126 (13) 149 (16)
Age y n ()
65ndash69b 284 (30) 280 (29)
65ndash74 5243 (550) 5356 (559)
75ndash84 3618 (380) 3601 (376)
ge85 380 (40) 352 (37)
Education y n ()
lt12 4307 (452) 4329 (452)
12ndash15 2802 (294) 2772 (289)
16+ 2415 (254) 2488 (260)
Male n () 4152 (436) 4180 (436)
Drinks alcohol n () 7309 (767) 7333 (765)
Current or past smoker n () 4261 (447) 4273 (446)
Obese ge30 kgm2 n () 2820 (297) 2857 (299)
Depression n ()c 925 (97) 954 (100)
3MS mean (SD) 934 (47) 935 (46)
COWAT mean (SD) 121 (46) 121 (46)
SDMT mean (SD) 367 (101) 368 (102)
HVLT-R mean (SD)
Total recall 225 (55) 225 (55)
Delayed Recall 77 (28) 77 (28)
Retention 832 (222) 833 (221)
RDI 107 (17) 107 (18)
Abbreviations 3MS = Modified Mini-Mental State Examination COWAT =Controlled Oral Word Association Test HVLT-R = Hopkins Verbal LearningTestndashRevised RDI = Recognition Discrimination Index SDMT = Symbol DigitModalities Testa Prior published data indicate no difference by trial group for a range of otherhealth conditions including diabetes hypertension and body mass index7b All US ethnic minoritiesc Depression was defined as a score of ge8 on the 10-item Center for Epide-miologic Studies Depression Scale (CES-D-10)
e324 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

risk of death25 Proportional hazards assumptions were testedas a null hypothesis of zero slope in a regression of scaledSchoenfeld residuals against time all p values were found to begt01 indicating satisfaction of the assumption for all outcomes
Subgroup analysis was used to investigate the effect of aspirinvs placebo across prespecified subgroups24 An interactionterm in the Cox proportional hazards models provided anestimate of the effect heterogeneity between subgroups
Similar analyses were undertaken to investigate probable andpossible AD MCI and cognitive decline
Linear mixed models were used to compare change in cognitivefunction over time in the participants randomized to aspirin vsplacebo All randomized participants were included and con-tributed data to the estimation of intercepts at baseline and atfollow-ups when available Given the small number of partic-ipants who had cognitive assessment at the year 2 and year 7follow-ups (lt100 participants) the cognitive scores from thesetimepoints were not included in the analysis Each of the 4cognitive tests (3MS HVLT-R Delayed Recall SDMT andCOWAT) was investigated individually and we also analyzeda global composite measure derived using a summed z score
(average of the 4 tests) Composite scores are commonly used incognitive research as they have less variability than individualneuropsychological test scores and can reduce floor and ceilingeffects26 Each model included treatment group (aspirin vs pla-cebo) annual visittime (0 [baseline] 1 3 4 5 6) a participant-specific intercept (baseline score) and a participant-specificslope describing change in score over time (per annual visit) Toexamine whether the trajectory of cognitive scores for an averageparticipant differed between treatment groups a treatment bytime interaction was included in the model Analyses wereperformed using Stata software release 15 (StataCorp)
Classification of evidenceThis prospective randomized double-blind placebo-controlled clinical trial (ASPREE) assessed the effect oftreatment with 100 mg once daily enteric-coated aspirin vsplacebo over 5 years on the prespecified secondary outcomesincident dementia and MCI overall and in prespecified sub-groups An ancillary study (supplement awarded in 2012) toASPREE had a prespecified primary aim to examine the effectof daily low-dose aspirin on AD This study provides Class IIevidence that aspirin does not affect the incidence of probableAD MCI or cognitive decline over a median 47 years inindividuals aged ge65 years without dementia at baseline
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram of participants in the Aspirin in ReducingEvents in the Elderly (ASPREE) trial
All randomized participants were included in the final analysis For participants who withdrew from the trial or died all information up to the point ofwithdrawaldeath was included in the analysis
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e323
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Data availabilityAll individual participant data (re-identifiable) that underlie theresults reported in this article are available upon request toqualified researchers without limit of time subject to approval ofthe analyses by the principal investigators and a standard datasharing agreement Details regarding requests to access the datawill be available through the study web site (ASPREEorg) Thedata will then bemade available through a web-based data portalsafe haven at Monash University Australia The ASPREE trialprotocol and statistical analysis plan have been published7
ResultsStudy participantsA total of 19114 participants were recruited with 9525 ran-domized to aspirin and 9589 to placebo (figure 1) Participantsranged in age from 65 to 98 years and 874 were recruited inAustralia No significant differences were identified in baselinecharacteristics between participants randomized to aspirin andplacebo including health factors and cognitive performancethat may predispose to cognitive impairment (table 1)
The median duration of follow-up was the same in the 2 groups(47 years interquartile range 36ndash57 years) At the end of thefollow-up period face-to-face visits were still being conductedon 82 of participants 97 via review of medical records onlyand 55 had died (11) Loss to follow-up was defined as nocontact with participants either in person or by phone in the12 months before the end of the trial period (June 12 2017)and no record of the participant having attended the medicalpractice within the last 12 months Only 12 of participantswithdrew consent for any follow-up and this was balancedacross the 2 study groups (figure 1) As reported previouslyaspirin did not prolong disability-free survival (HR 101 95confidence interval [CI] 092ndash111)7
Incident dementia and probable ADIn the aspirin group 488 participants (116 per 1000person-years) reached the dementia trigger criteria com-pared with 476 participants (113 per 1000 person-years) inthe placebo group (HR 103 95 CI 091ndash117) The typeof dementia trigger was similar across the aspirin and placebogroups with similar rates of reported memory problems (44and 46 per 1000 person-years respectively) 3MS score lt78(41 and 43 per 1000 person-years respectively) gt10-pointdrop in predicted 3MS from baseline (15 and 17 per 1000person-years respectively) and prescribed a cholinesteraseinhibitor (10 and 07 per 1000 person-years respectively)
The rate of incident dementia in the aspirin group was 67 eventsper 1000 person-years and in the placebo group 69 events per1000 person-years (table 2) Fewer than half of all adjudicateddementia cases (41) were classified as clinically probable AD
The 95 CI for HR indicating the difference in the risk ofincident clinically probable AD and possible AD in the aspirinand placebo groups overlaps 10 (figure 2)
There were no significant interactions between treatmentgroup and any prespecified subgroup for dementia (figure 3)or probable AD (data not shown) with the exception offrailty but in this latter case the direction of effect was in-consistent across frailty categories
Table 1 Selected participant characteristics atrandomization according to treatment groupa
Aspirin(n = 9525)
Placebo(n = 9589)
Ethno-racial group n ()
Australian white 8169 (858) 8193 (854)
US white 539 (57) 549 (57)
African American 451 (47) 450 (47)
HispanicLatino 240 (25) 248 (26)
Other 126 (13) 149 (16)
Age y n ()
65ndash69b 284 (30) 280 (29)
65ndash74 5243 (550) 5356 (559)
75ndash84 3618 (380) 3601 (376)
ge85 380 (40) 352 (37)
Education y n ()
lt12 4307 (452) 4329 (452)
12ndash15 2802 (294) 2772 (289)
16+ 2415 (254) 2488 (260)
Male n () 4152 (436) 4180 (436)
Drinks alcohol n () 7309 (767) 7333 (765)
Current or past smoker n () 4261 (447) 4273 (446)
Obese ge30 kgm2 n () 2820 (297) 2857 (299)
Depression n ()c 925 (97) 954 (100)
3MS mean (SD) 934 (47) 935 (46)
COWAT mean (SD) 121 (46) 121 (46)
SDMT mean (SD) 367 (101) 368 (102)
HVLT-R mean (SD)
Total recall 225 (55) 225 (55)
Delayed Recall 77 (28) 77 (28)
Retention 832 (222) 833 (221)
RDI 107 (17) 107 (18)
Abbreviations 3MS = Modified Mini-Mental State Examination COWAT =Controlled Oral Word Association Test HVLT-R = Hopkins Verbal LearningTestndashRevised RDI = Recognition Discrimination Index SDMT = Symbol DigitModalities Testa Prior published data indicate no difference by trial group for a range of otherhealth conditions including diabetes hypertension and body mass index7b All US ethnic minoritiesc Depression was defined as a score of ge8 on the 10-item Center for Epide-miologic Studies Depression Scale (CES-D-10)
e324 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Data availabilityAll individual participant data (re-identifiable) that underlie theresults reported in this article are available upon request toqualified researchers without limit of time subject to approval ofthe analyses by the principal investigators and a standard datasharing agreement Details regarding requests to access the datawill be available through the study web site (ASPREEorg) Thedata will then bemade available through a web-based data portalsafe haven at Monash University Australia The ASPREE trialprotocol and statistical analysis plan have been published7
ResultsStudy participantsA total of 19114 participants were recruited with 9525 ran-domized to aspirin and 9589 to placebo (figure 1) Participantsranged in age from 65 to 98 years and 874 were recruited inAustralia No significant differences were identified in baselinecharacteristics between participants randomized to aspirin andplacebo including health factors and cognitive performancethat may predispose to cognitive impairment (table 1)
The median duration of follow-up was the same in the 2 groups(47 years interquartile range 36ndash57 years) At the end of thefollow-up period face-to-face visits were still being conductedon 82 of participants 97 via review of medical records onlyand 55 had died (11) Loss to follow-up was defined as nocontact with participants either in person or by phone in the12 months before the end of the trial period (June 12 2017)and no record of the participant having attended the medicalpractice within the last 12 months Only 12 of participantswithdrew consent for any follow-up and this was balancedacross the 2 study groups (figure 1) As reported previouslyaspirin did not prolong disability-free survival (HR 101 95confidence interval [CI] 092ndash111)7
Incident dementia and probable ADIn the aspirin group 488 participants (116 per 1000person-years) reached the dementia trigger criteria com-pared with 476 participants (113 per 1000 person-years) inthe placebo group (HR 103 95 CI 091ndash117) The typeof dementia trigger was similar across the aspirin and placebogroups with similar rates of reported memory problems (44and 46 per 1000 person-years respectively) 3MS score lt78(41 and 43 per 1000 person-years respectively) gt10-pointdrop in predicted 3MS from baseline (15 and 17 per 1000person-years respectively) and prescribed a cholinesteraseinhibitor (10 and 07 per 1000 person-years respectively)
The rate of incident dementia in the aspirin group was 67 eventsper 1000 person-years and in the placebo group 69 events per1000 person-years (table 2) Fewer than half of all adjudicateddementia cases (41) were classified as clinically probable AD
The 95 CI for HR indicating the difference in the risk ofincident clinically probable AD and possible AD in the aspirinand placebo groups overlaps 10 (figure 2)
There were no significant interactions between treatmentgroup and any prespecified subgroup for dementia (figure 3)or probable AD (data not shown) with the exception offrailty but in this latter case the direction of effect was in-consistent across frailty categories
Table 1 Selected participant characteristics atrandomization according to treatment groupa
Aspirin(n = 9525)
Placebo(n = 9589)
Ethno-racial group n ()
Australian white 8169 (858) 8193 (854)
US white 539 (57) 549 (57)
African American 451 (47) 450 (47)
HispanicLatino 240 (25) 248 (26)
Other 126 (13) 149 (16)
Age y n ()
65ndash69b 284 (30) 280 (29)
65ndash74 5243 (550) 5356 (559)
75ndash84 3618 (380) 3601 (376)
ge85 380 (40) 352 (37)
Education y n ()
lt12 4307 (452) 4329 (452)
12ndash15 2802 (294) 2772 (289)
16+ 2415 (254) 2488 (260)
Male n () 4152 (436) 4180 (436)
Drinks alcohol n () 7309 (767) 7333 (765)
Current or past smoker n () 4261 (447) 4273 (446)
Obese ge30 kgm2 n () 2820 (297) 2857 (299)
Depression n ()c 925 (97) 954 (100)
3MS mean (SD) 934 (47) 935 (46)
COWAT mean (SD) 121 (46) 121 (46)
SDMT mean (SD) 367 (101) 368 (102)
HVLT-R mean (SD)
Total recall 225 (55) 225 (55)
Delayed Recall 77 (28) 77 (28)
Retention 832 (222) 833 (221)
RDI 107 (17) 107 (18)
Abbreviations 3MS = Modified Mini-Mental State Examination COWAT =Controlled Oral Word Association Test HVLT-R = Hopkins Verbal LearningTestndashRevised RDI = Recognition Discrimination Index SDMT = Symbol DigitModalities Testa Prior published data indicate no difference by trial group for a range of otherhealth conditions including diabetes hypertension and body mass index7b All US ethnic minoritiesc Depression was defined as a score of ge8 on the 10-item Center for Epide-miologic Studies Depression Scale (CES-D-10)
e324 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

MCI and cognitive declineOverall there were 389 participants with incident MCI with22 classified as MCI due to AD The rates were similarbetween the aspirin and placebo groups (figure 4)
In the aspirin group 838 participants (265 per 1000 person-years) were defined as having cognitive decline comparedwith 816 participants (256 per 1000 person-years) in theplacebo group (HR 104 95 CI 094ndash114)
Cognitive changeCognitive performance over follow-up in the aspirin and pla-cebo groups is shown in table 3 There were small changes incognitive function over time but there was no evidence that theaverage trajectory differed between aspirin and placebo groups
These findings remained essentially unchanged in sensitivityanalysis excluding individuals who had died or reached thedementia endpoint or to help account for possible practiceeffects by removing baseline performance from the analysis
DiscussionWe previously reported in ASPREE that daily low-dose as-pirin initiated in older adults did not prolong disability-freesurvival but increased the risk of major hemorrhage com-pared with placebo7 Low-dose aspirin exposure had nooverall effect on all-cause dementia incidence
In this study we extend our initial findings to include prespecifiedsubgroup analysis and assessment of secondary cognitive
Table 2 The effect of aspirin vs placebo on incident dementia Alzheimer disease (AD) and mild cognitive impairment(MCI)
Aspirin (n = 9525) Placebo (n = 9589)
Hazard ratio(95 CI)
No of participantswith event
Rate per 1000person-years
No of participantswith event
Rate per 1000person-years
Dementia diagnosis 283 67 292 69 098 (083ndash115)
Clinically probable AD 116 28 122 29 096 (074ndash124)
Clinically possible AD 166 39 163 38 103 (083ndash127)
Likely non-AD 1 002 6 014 017 (002ndash139)
MCI 205 49 184 44 112 (092ndash137)
MCI consistent with AD 47 11 38 09 113 (081ndash191)
MCI othera 158 38 146 35 110 (087ndash137)
Cognitive decline 838 265 816 256 104 (094ndash114)
Abbreviation CI = confidence intervala Includes participants with evidence of functional decline or MCI not consistent with AD or insufficient information to determine
Figure 2 Cumulative incidence of dementia subtype
Cumulative incidences of all events of clinically probable Alzheimer disease (AD) and possible AD that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e325
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

outcomes We report a consistent lack of benefit of aspirin onrates of clinically probable and possible AD MCI and cognitivedecline which were approximately equal between the treatmentgroups There was no effect of aspirin vs placebo on globalcognition or specific cognitive domains (ie memory psycho-motor speed language and executive function) Furthermoretreatment effects did not vary across subgroups including those
defined by age sex ethno-racial group health factors or priorNSAID use
Given the rigor of this large double-blinded placebo-controlled trial and the consideration of potential effects ofaspirin on early and more severe stages of cognitive impair-ment this study provides strong evidence that in older
Figure 3 Forest plot for adjudicated incidence of dementia (all-cause) in prespecified subgroups
Arrows indicate that the 95 confidence intervals (CIs) were beyond the scale Other ethnicracial group included individuals whowere not Hispanic but whodid not state another race or ethnic group (18) or any other categorywith fewer than 200 participants overall This includedAboriginal or Torres Strait Islander(12 participants) Native American (6)multiple races or ethnic groups (64) andNativeHawaiian or Pacific Islander (11) The presence of diabeteswas basedonparticipantsrsquo report of diabetes mellitus or a fasting glucose level of at least 126 mgdL (ge7 mmolL) or receipt of treatment for diabetes Hypertension wasdefined as treatment for high blood pressure or a blood pressure of greater than 14090 mm Hg at trial entry Dyslipidemia was defined as the receipt ofcholesterol-lowering medication or as a serum cholesterol level of at least 212 mgdL (ge55 mmolL) in Australia and at least 240 mgdL (ge62 mmolL) in theUnited States or as a low-density lipoprotein level of more than 160 mgdL (gt41 mmolL) Previous regular aspirin use was defined according to participant-reported regular use of aspirin immediately before the first baseline visit with a 1-month washout period before randomization Frailty was categorized onthe basis of the adapted Fried frailty criteria which included body weight strength exhaustion walking speed and physical activity The category of prefrailincluded participants whomet 1 or 2 criteria and the category of frail included those whomet 3 or more criteria Body mass index is the weight in kilogramsdivided by the square of the height in meters
e326 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

individuals initiation of low-dose aspirin and continuationover a median 47 years is not effective in reducing the risk ofcognitive decline dementia or AD
The pharmacologic properties of aspirin have raised thepossibility of a preventive effect in reducing cognitive declineand the incidence of both AD and vascular dementia It hasbeen hypothesized that aspirinrsquos potential beneficial effectcould be via the suppression of inflammation2 or preventionof ischemic damage and a reduction in cerebrovascular dis-ease4 On the other hand aspirin could potentially increasethe risk of cerebral microbleeds27 which have been associatedwith cognitive impairment28 A recent meta-analysis of ob-servational data from 16 cohorts involving 236022 partic-ipants found that ever use of NSAIDs was associated witha reduced risk of AD29 However interpretation of significantfindings from observational studies can be difficult as pre-scription and health user bias as well as residual confoundingmay account for reported associations30
Two previous trials of low-dose aspirin have been reported butneither has specifically investigated the effect on all-cause de-mentia or AD A study involving a subsample of 6377 womenaged 65 years from the Womenrsquos Health Study found that low-dose aspirin (100 mg on alternate days) for a mean of 96 yearswas not associated with overall change in global cognition orcognitive decline although they did find some evidence for re-duced decline in category (semantic) fluency31 The other largetrial (The Aspirin for Asymptomatic Atherosclerosis Trial) ofaspirin (100 mg daily) in 3350 men and women over 50 yearsand at moderately increased risk of cardiovascular disease alsofailed to show any benefit in preserving cognitive function32
Although NSAIDs are structurally diverse and aspirin differs inpharmacokinetic and pharmacodynamic properties from otherNSAIDs33 the results of our study are in keeping with trials of
other NSAIDs The Alzheimerrsquos Disease Anti-InflammatoryPrevention Trial (ADAPT) investigated the effect of a median15 years of naproxen or celecoxib treatment in 2528 individualsaged 70 years and over at high risk of AD34 Cognitive declineand incident ADwere assessed over a 7-year follow-up The trialfound no evidence for efficacy34 The smaller Investigation ofNaproxen Treatment Effects in Pre-symptomatic AlzheimerrsquosDisease (INTREPAD) trial also examined the effect of dailynaproxen over 2 years in 195 asymptomatic individuals witha strong family history of AD aged 60 years and over35 Theyfound no beneficial effect on cognition or a composite measureof cognition imaging and blood biomarkers
The ASPREE sample was community-based meaning that it isgeneralizable to individuals in the primary care setting How-ever there are limitations to the study that need to be con-sidered when interpreting the null results First the reducedincidence of dementia and MCI compared with the ratesreported in previous studies3637 may have reduced the likeli-hood of detecting efficacy This lower incidence is likelyexplained by the inclusion of participants who were relativelyhealthy at baseline without established cardiovascular diseaseor other major illnesses and with a 3MS score above 77 Ofnote however vascular risk factors were not uncommonamong participants in the trial with for example 11 havingdiabetes mellitus and 74 hypertension at baseline7 Anotherpossible explanation for the low incidence ofMCI is likely to bethe stringent criteria that were applied in this study which maynot have identified all cases of incident MCI However ourdefinition of cognitive decline (gt15 SD drop on at least onecognitive test) in individuals without dementia likely capturesa broader MCI definition with a gt5-fold higher incidence andthe findings were consistent A second possible limitation isthat the low dose of aspirin employed may have been in-sufficient to suppress inflammation although its antiplateleteffects could still benefit cognition33 Third it is plausible that
Figure 4 Cumulative incidence of mild cognitive impairment (MCI) and cognitive decline
Cumulative incidences of all events of incident MCI and cognitive decline that were observed during the trial CI = confidence interval
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e327
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Table 3 Cognitive performance by treatment group at each follow-up
Time
Treatment group Mixed modela analysis with interactions
Aspirin Placebo
Type Coefficient p ValueNo Mean (SD) No Mean (SD)
Modified Mini-Mental StateExamination (3MS)
Baseline 9525 934 (47) 9589 935 (46) Time minus008 lt0001
Year 1 8895 942 (48) 8974 942 (47) Group times time minus002 023
Year 3 7344 939 (54) 7385 939 (53)
Year 4 851 939 (62) 877 939 (54)
Year 5 3456 935 (65) 3528 935 (64)
Year 6 820 940 (71) 834 941 (63)
Hopkins Verbal Learning TestndashRevised(HVLT-R) Delayed Recall
Baseline 9473 77 (28) 9534 77 (28) Time 001 001
Year 1 8787 82 (31) 8876 82 (30) Group times time minus0004 058
Year 3 7148 82 (32) 7216 82 (32)
Year 4 832 83 (32) 860 81 (32)
Year 5 3335 82 (33) 3403 82 (33)
Year 6 792 85 (33) 811 86 (32)
Controlled Oral Word AssociationTest (COWAT) (F)
Baseline 9509 121 (46) 9574 121 (45) Time 023 lt0001
Year 1 8865 132 (49) 8942 132 (48) Group times time minus0003 080
Year 3 7285 133 (50) 7329 134 (49)
Year 4 847 135 (50) 871 132 (47)
Year 5 3428 135 (52) 3496 137 (51)
Year 6 813 138 (50) 827 142 (51)
Symbol Digit Modalities Test (SDMT)
Baseline 9491 367 (101) 9539 368 (102) Time minus052 lt0001
Year 1 8818 368 (101) 8883 370 (101) Group times time minus0007 076
Year 3 7219 358 (102) 7237 359 (101)
Year 4 839 358 (105) 865 357 (102)
Year 5 3363 349 (101) 3424 351 (102)
Year 6 803 358 (102) 813 357 (107)
Composite cognitive scoreb
Baseline 9442 minus001 (29) 9491 003 (28) Time 001 lt0001
Year 1 8742 059 (30) 8800 063 (30) Group times time 0001 089
Year 3 7078 050 (32) 7122 049 (32)
Year 4 826 058 (34) 853 043 (32)
Year 5 3274 041 (35) 3346 049 (34)
Year 6 782 083 (35) 796 091 (35)
a A separatemixed-effects linear regression model for each cognitive test Thesemodels contained the fixed effect of treatment group (aspirin vs placebo) atbaseline (not shown above) which was not significant for any individual test and time (annual visits) as main effects and the 2-way interaction betweentreatment group and annual visit (which compared the mean change in cognitive function over time between groups)b Composite cognition is a global composite cognitive score an average of the cognitive tests 3MS HVLT-RDelayed Recall COWAT and SDMTusing z scores ofeach test Scores for each test were standardized into z scores based on mean and SD of the test at baseline
e328 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

the median 47 years of follow-up was insufficient to see aneffect of aspirin on dementia incidence and cognitive declineGiven the long prodromal phase of AD (the most commonpathologic cause of dementia) participants diagnosed duringthe course of our study likely had significant dementia neuro-pathology when they enrolled Prior studies have found thataspirin is ineffective in delaying progression of cognitive declinein individuals already diagnosed with dementia38 Although weinvestigated the effect of aspirin on cognitive change in indi-viduals without dementia orMCI there was onlyminor changein cognitive function in this sample over the median 47-yeartime frame Finally our results do not address the question ofwhether aspirin could be beneficial for preservation of cognitivefunction in middle-aged adults when neurodegenerative pro-cesses are likely to begin and the targeting of midlife vascularfactors appears to be particularly crucial39
ASPREE was the first prospectively planned placebo-controlled trial of aspirin therapy undertaken among indi-viduals aged predominantly 70 years and over among whomthe risk of cognitive decline is greater and where an effectiveintervention could have the largest net benefit This studyprovides no evidence that low-dose aspirin initiated in rela-tively healthy older adults is effective in preventing dementiaclinically probable AD or MCI or in reducing cognitive de-cline during active treatment over a median 47 years Thisconclusion was consistent across a series of participant sub-groups The potential longer-term legacy effects of aspirin onthese outcomes will be assessed with ongoing follow-up of theparticipants
AcknowledgmentBayer AG (Germany) provided the trial drug (aspirin) andplacebo but had no other role in the trial The authorsthank the staff in Australia and the United States forconducting the trial the ASPREE participants and thegeneral practitioners and staff of the medical clinics whocared for the participants
Study fundingThe work was supported by the National Institute on Aging andthe National Cancer Institute at the NIH (U01AG029824) theNational Health and Medical Research Council (NHMRC) ofAustralia (334047 and 1127060) Monash University and theVictorian Cancer Agency J Ryan is funded by an NHMRCDementia Research Leader Fellowship (APP1135727) C Reidis supported through an NHMRC Principal Research Fellow-ship (APP1136372)
DisclosureA Murray reports receiving consulting and travel fees fromBayer AG to present ASPREE primary results after theirpublication consulting fees from Alkahest Inc and grantsfrom the National Institute on Aging M Nelson reports re-ceiving consulting and travel fees from Bayer AG R Shahreports grants for clinical research regarding dementia andAlzheimer disease from NIH the Centers for Medicare and
Medicaid Services the Department of Defense and the Illi-nois Department of Public Health being a noncompensatedboard member of the Alzheimerrsquos Association IllinoisChapter and being the site principal investigator or sub-investigator for clinical trials for which his institution (RushUniversity Medical Center) is compensated (Amylyx Phar-maceuticals Inc Eli Lilly amp Co Inc Genentech Inc Merckamp Co Inc Navidea Biopharmaceuticals Novartis Pharma-ceuticals Inc Roche Holdings AG and Takeda De-velopment Center Americas Inc) Drs J Ryan E Storey RWoods R Wolfe C Reid T Chong J Williamson S WardJ Lockery S Orchard R Trevaks B Kirpach A NewmanMErnst and J McNeil report no disclosures relevant to themanuscript Go to NeurologyorgN for full disclosures
Publication historyReceived by Neurology September 2 2019 Accepted in final formJanuary 13 2020
Appendix 1 Authors
Name Location Contribution
Trevor T-JChong MBBSPhD
Monash UniversityMelbourne Australia
Data interpretationrevised the manuscriptfor intellectual content
Michael EErnstPharmD
The University of IowaIowa City
Major role in acquisitionof data revised themanuscript forintellectual content
BrendaKirpachCCRA
Berman Center for ClinicalOutcomes and ResearchHennepin Health ResearchInstitute Minneapolis MN
Major role in acquisitionof data revised themanuscript forintellectual content
JessicaLockeryMBBS
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectual content
John McNeilMBBS PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne MMurray MDMSc
Hennepin Healthcare andUniversity of MinnesotaMinneapolis
Designed andconceptualized the studyinterpreted the datarevised the manuscriptfor intellectual content
Mark NelsonMB PhD
Menzies Institute forMedical ResearchUniversity of TasmaniaHobart Australia
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
Anne BNewmanMD MPH
University of Pittsburgh PA Designed andconceptualized the studyrevised the manuscriptfor intellectualcontent
Suzanne GOrchard PhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datarevised the manuscriptfor intellectualcontent
Continued
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e329
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

References1 Piepoli MF Hoes AW Agewall S et al 2016 European guidelines on cardiovascular
disease prevention in clinical practice the sixth joint task force of the EuropeanSociety of Cardiology and other societies on cardiovascular disease prevention inclinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European Association for Cardiovas-cular Prevention amp Rehabilitation (EACPR) Atherosclerosis 2016252207ndash274
2 Kinney JW Bemiller SMMurtishawAS LeisgangAM Salazar AM LambBT Inflammationas a central mechanism in Alzheimerrsquos disease Alzheimers Dement 20184575ndash590
3 Chandra S Jana M Pahan K Aspirin induces lysosomal biogenesis and attenuatesamyloid plaque pathology in a mouse model of Alzheimerrsquos disease via PPARalphaJ Neurosci 2018386682ndash6699
4 Hachinski V Einhaupl K Ganten D et al Preventing dementia by preventing strokethe Berlin Manifesto Alzheimers Dement 201915961ndash984
5 McGeer PL Rogers J McGeer EG Inflammation antiinflammatory agents andAlzheimerrsquos disease the last 22 years J Alzheimers Dis 201654853ndash857
6 Fink HA Jutkowitz E McCarten JR et al Pharmacologic interventions to preventcognitive decline mild cognitive impairment and clinical Alzheimer-type dementiaa systematic review Ann Intern Med 201816839ndash51
7 McNeil JJ Woods RL Nelson MR et al Effect of aspirin on disability-free survival inthe healthy elderly N Engl J Med 20183791499ndash1508
8 ASPREE IG Study design of Aspirin in Reducing Events in the Elderly (ASPREE)a randomized controlled trial Contemp Clin Trials 201336555ndash564
Appendix 2 Coinvestigators
Name Location Role Contribution
WalterAbhayaratna
Australian NationalUniversity
Internationalsteeringcommittee
Coinvestigator
Lawrie Beilin University of WesternAustralia
Internationalsteeringcommittee
Coinvestigator
Appendix 1 (continued)
Name Location Contribution
ChristopherM Reid PhD
Curtin University PerthMonash UniversityMelbourne Australia
Designed andconceptualized theASPREE study designedprocess associated withacquisition of datareviewed manuscript forintellectual content
Joanne RyanPhD
Monash UniversityMelbourne Australia
Analyzed and interpretedthe data drafted themanuscript forintellectual content
Raj C ShahMD
Rush University Chicago IL Designed andconceptualized the studymajor role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
ElsdonStorey MBBSPhD
Monash UniversityMelbourne Australia
Designed andconceptualized the studytaught and certifiedAustralian field staffinterpreted the datarevised the manuscriptfor intellectual content
Ruth TrevaksPhD
Monash UniversityMelbourne Australia
Major role in theacquisition of datainterpreted the datarevised the manuscriptfor intellectual content
StephanieWard BMedFRACP MPH
Monash UniversityMelbourne Australia
Interpreted the datarevised the manuscriptfor intellectual content
JeffWilliamsonMD MHS
Wake Forest School ofMedicine Winston-SalemNC
Designed andconceptualized theASPREE study revisedthe manuscript forintellectual content
RobynWoods PhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study major rolein the acquisition of datarevised the manuscriptfor intellectualcontent
Rory WolfePhD
Monash UniversityMelbourne Australia
Designed andconceptualized theASPREE study advised onstatistical analysis andinterpretation revisedthe manuscript forintellectual content
Appendix 2 (continued)
Name Location Role Contribution
AndrewChan
MassachusettsGeneral Hospital
Internationalsteeringcommittee
Coinvestigator
JamehlDemons
Gerontology andGeriatric MedicineWake Forest ClinicalTrials Office
Internationalsteeringcommittee
Coinvestigator
GeoffreyDonnan
The Florey Institute ofNeuroscience andMental Health
Internationalsteeringcommittee
Coinvestigator
SaraEspinoza
UT Health ScienceCenter
Internationalsteeringcommittee
Coinvestigator
MatthewGoetz
Mayo Clinic CancerCenter
Internationalsteeringcommittee
Coinvestigator
ColinJohnston
Monash University Internationalsteeringcommittee
Coinvestigator
Danny Liew Monash University Internationalsteeringcommittee
Coinvestigator
Karen LMargolis
HealthPartnersInstitute forEducation ampResearch
Internationalsteeringcommittee
Coinvestigator
FrankMeyskens
Biological ChemistrySchool of MedicineUCI Chao FamilyComprehensiveCancer Center
Internationalsteeringcommittee
Coinvestigator
Nigel Stocks University ofAdelaide
Internationalsteeringcommittee
Coinvestigator
AndrewTonkin
Monash University Internationalsteeringcommittee
Coinvestigator
JohnZalcberg
Monash University Internationalsteeringcommittee
Coinvestigator
e330 Neurology | Volume 95 Number 3 | July 21 2020 NeurologyorgN
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

9 Lockery JE Collyer TA Abhayaratna WP et al Recruiting general practice patientsfor large clinical trials lessons from the Aspirin in Reducing Events in the Elderly(ASPREE) study Med J Aust 2019210168ndash173
10 Teng EL Chui HC The Modified Mini-Mental State (3MS) examination J ClinPsychiatry 198748314ndash318
11 Ryan J Woods RL Britt C et al Normative performance of healthy older individualson the Modified Mini-Mental State (3MS) examination according to ethno-racialgroup gender age and education level Clin Neuropsychol 201833779ndash797
12 Benedict RHB Schretlen D Groninger L Brandt J Hopkins Verbal LearningTestndashRevised normative data and analysis of inter-form and test-retest reliabilityClin Neuropsychol 20011243ndash55
13 Ross TP The reliability of cluster and switch scores for the Controlled Oral WordAssociation Test Arch Clin Neuropsychol 200318153ndash164
14 Smith A Symbol Digit Modalities Test (SDMT) Manual (Revised) Los AngelesWestern Psychological Services 1982
15 Bland RC Newman SC Mild dementia or cognitive impairment the Modified Mini-Mental State Examination (3MS) as a screen for dementia Can J Psychiatry 200146506ndash510
16 Tombaugh TN Test-retest reliable coefficients and 5-year change scores for theMMSE and 3MS Arch Clin Neuropsychol 200520485ndash503
17 Graham DP Cully JA Snow AL Massman P Doody R The Alzheimerrsquos DiseaseAssessment ScalendashCognitive Subscale normative data for older adult controls Alz-heimer Dis Assoc Disord 200418236ndash240
18 DrsquoElia L Color Trails Test Professional Manual Odessa FL Psychological Assess-ment Resources 1996
19 AlegretM Boada-RoviraMVinyes-JunqueG et al Detection of visuoperceptual deficitsin preclinical and mild Alzheimerrsquos disease J Clin Exp Neuropsychol 200931860ndash867
20 J F Alzheimerrsquos Disease Cooperative Study ADL Scale In Encyclopedia of ClinicalNeuropsychology New York Springer 2011
21 American Psychiatric Association Diagnostic and Statistical Manual of Mental Dis-orders (DSM-IV) Washington DC American Psychiatric Association 1994
22 McKhann GM Knopman DS Chertkow H et al The diagnosis of dementia due toAlzheimerrsquos disease recommendations from the National Institute on AgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquos diseaseAlzheimers Dement 20117263ndash269
23 Albert MS DeKosky ST Dickson D et al The diagnosis of mild cognitive impairmentdue to Alzheimerrsquos disease recommendations from the National Institute onAgingndashAlzheimerrsquos Association workgroups on diagnostic guidelines for Alzheimerrsquosdisease Alzheimers Dement 20117270ndash279
24 Wolfe R Murray AM Woods RL et al The Aspirin in Reducing Events in the ElderlyTrial statistical analysis plan Int J Stroke 201813335ndash338
25 Andersen PK Geskus RB de Witte T Putter H Competing risks in epidemiologypossibilities and pitfalls Int J Epidemiol 201241861ndash870
26 Jutten RJ Harrison JE Lee Meeuw Kjoe PR et al Assessing cognition and dailyfunction in early dementia using the cognitive-functional composite findings from theCatch-Cog study cohort Alzheimers Res Ther 20191145
27 Naka H Nomura E Kitamura J Imamura E Wakabayashi S Matsumoto M Anti-platelet therapy as a risk factor for microbleeds in intracerebral hemorrhage patientsanalysis using specific antiplatelet agents J Stroke Cerebrovasc Dis 201322834ndash840
28 Martinez-Ramirez S Greenberg SM Viswanathan A Cerebral microbleeds overviewand implications in cognitive impairment Alzheimers Res Ther 2014633
29 Zhang C Wang Y Wang D Zhang J Zhang F NSAID exposure and risk of Alz-heimerrsquos disease an updated meta-analysis from cohort studies Front Aging Neurosci20181083
30 de Craen AJ Gussekloo J Vrijsen B Westendorp RG Meta-analysis of nonsteroidalantiinflammatory drug use and risk of dementia Am J Epidemiol 2005161114ndash120
31 Kang JH Cook N Manson J Buring JE Grodstein F Low dose aspirin and cognitivefunction in the Womenrsquos Health Study cognitive cohort BMJ 2007334987
32 Price JF Stewart MC Deary IJ et al Low dose aspirin and cognitive function inmiddle aged to elderly adults randomised controlled trial BMJ 2008337a1198
33 Gargiulo G Capodanno D Longo G Capranzano P Tamburino C Updates onNSAIDs in patients with and without coronary artery disease pitfalls interactions andcardiovascular outcomes Expert Rev Cardiovasc Ther 2014121185ndash1203
34 ADAPT Results of a follow-up study to the randomized Alzheimerrsquos Disease Anti-Inflammatory Prevention Trial (ADAPT) Alzheimers Dement 20139714ndash723
35 Meyer PF Tremblay-Mercier J Leoutsakos J et al INTREPAD a randomized trial ofnaproxen to slow progress of presymptomatic Alzheimer disease Neurology 201992e2070ndashe2080
36 Mehta KM Yeo GW Systematic review of dementia prevalence and incidence inUnited States raceethnic populations Alzheimers Dement 20171372ndash83
37 Roberts RO Geda YE Knopman DS et al The incidence of MCI differs by subtypeand is higher in men the Mayo Clinic Study of Aging Neurology 201278342ndash351
38 Bentham P Gray R Sellwood E Hills R Crome P Raftery J Aspirin in Alzheimerrsquosdisease (AD2000) a randomised open-label trial Lancet Neurol 2008741ndash49
39 Knopman DS Gottesman RF Sharrett AR et al Midlife vascular risk factors andmidlife cognitive status in relation to prevalence of mild cognitive impairment anddementia in later life the Atherosclerosis Risk in Communities Study AlzheimersDement 2018141406ndash1415
NeurologyorgN Neurology | Volume 95 Number 3 | July 21 2020 e331
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000009277202095e320-e331 Published Online before print March 25 2020Neurology Joanne Ryan Elsdon Storey Anne M Murray et al
declineRandomized placebo-controlled trial of the effects of aspirin on dementia and cognitive
This information is current as of March 25 2020
ServicesUpdated Information amp
httpnneurologyorgcontent953e320fullincluding high resolution figures can be found at
References httpnneurologyorgcontent953e320fullref-list-1
This article cites 35 articles 5 of which you can access for free at
Citations httpnneurologyorgcontent953e320fullotherarticles
This article has been cited by 3 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionmci_mild_cognitive_impairmentMCI (mild cognitive impairment)
lled_consort_agreementhttpnneurologyorgcgicollectionclinical_trials_randomized_controClinical trials Randomized controlled (CONSORT agreement)
httpnneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
httpnneurologyorgcgicollectionall_cbmrt_null_hypothesisAll CBMRTNull Hypothesisfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
rights reserved Print ISSN 0028-3878 Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright copy 2020 American Academy of Neurology All
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology