Embed Size (px)
Citation preview
Page 1/15
Blood Loss from Transverse Versus LongitudinalUterine Incision in Abdominal Myomectomy: ARandomized Controlled TrialAlaa Elguindy
Ain Shams UniversityHosam Hemeda
Ain Shams UniversityMohamed Esmat Shawky
Ain Shams UniversityMohamed Elsenity
Ain Shams UniversityMedhat Adel Elsayed
Ain Shams UniversityAhmed Fahim
Ain Shams UniversityKhaled A��
Ain Shams UniversityMaii Nawara ( [email protected] )
Ain Shams University https://orcid.org/0000-0003-2443-9459
Research article
Keywords: myomectomy, blood loss, transverse uterine incision, longitudinal uterine incision, randomizedcontrolled study
Posted Date: May 25th, 2020
DOI: https://doi.org/10.21203/rs.2.9943/v3
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Version of Record: A version of this preprint was published on December 28th, 2020. See the publishedversion at https://doi.org/10.1186/s12905-020-01113-3.

Page 2/15
AbstractBackground: It is unclear whether transverse uterine incision is non-inferior to longitudinal incision duringmyomectomy with regard to bleeding. Our aim was to compare between transverse and longitudinaluterine incisions in myomectomy.
Methods: A parallel randomized controlled single-blinded study in a university a�liated hospital, in theperiod between January 2017 and April 2018, in which 52 women candidates for abdominalmyomectomy were randomized into transverse uterine incision or longitudinal uterine incision groups (26in each group). Intraoperative blood loss (estimated directly by blood volume in suction bottle and linentowels and indirectly by difference between preoperative and postoperative hematocrit), operative timeand postoperative fever were analyzed.
Results: No statistically signi�cant difference was found between transverse and longitudinal incisionsregarding intraoperative blood loss (389.7 ± 98.56 ml vs 485.04 ± 230.6 ml respectively, p value=0.07),operative time (59.96 ± 16.78 min vs 66.58 ± 17.33 min respectively, p value=0.18), and postoperativefever (4% vs 8.33%, p value=0.6).
Conclusion: Transverse uterine incision does not cause more blood loss than longitudinal incision and isa reasonable option during abdominal myomectomy.
Trial registration: NCT03009812 at clinicaltrials.gov, registered January 2017
BackgroundMyomectomy is the typical surgical management option for various women who suffer from myomasand require future childbearing or basically desire preservation of their uterus. Various surgicalapproaches for myomectomy are used in practice involving laparotomy, laparoscopy, and hysteroscopy.[1,2]
Being a reconstructive surgery, the goals of myomectomy operation include removal of the tumor masswithout excessive blood loss, closure of the dead space without hematoma formation, ensuring a good-quality uterine scar that can withstand subsequent pregnancies without dehiscence and minimizingpostoperative formation of adhesions.
Midline anterior longitudinal uterine incision was originally advocated as being best suited for removal ofmultiple myomas through a single serosal incision[3,4]. This single incision approach aimed to decreasethe incidence of obstetric complications related to multiple uterine scarring and to minimizepostoperative adhesion with ensuing infertility. Another advantage of the midline incisions is minimizingthe risk of inadvertent extension to the cornu, tubes, or the large vessels along the lateral uterine border [5],and hence was thought to be associated with less intraoperative blood loss.[6] However, based onanatomical studies of myometrial vasculature [7,8], it was logically proposed that transverse uterine

Page 3/15
incisions were more hemostatically ideal compared to the classic midline longitudinal ones [9]. Thus,transverse incisions were deemed practically appealing especially in cases where the midline longitudinalincision loses the advantage of its single incision approach, i.e. excision of a single myoma or whenmultiple incisions are inevitable [4]. Despite that, transverse uterine incisions did not gain popularity andwere recommended historically by only few references [8,10,11]. This –at least in part– is a consequence ofthe paucity of the studies addressing the differences between the two approaches.
In theory, a transverse uterine incision would serve two main advantages: �rst, ensuring adequatehemostasis following enucleation of the myoma that is of paramount importance in minimizing the riskof hematoma formation, which is related directly to postoperative bleeding and weak scar formation withensuing scar dehiscence in subsequent pregnancies [12]. Second, transverse incisions might achieve abetter scar quality. It is well established that classic longitudinal incisions are associated with weakerscars and higher incidence of subsequent uterine rupture compared to lower segment transverseincisions during cesarean delivery.[13,14] Despite the unique process of uterine involution and remodelingafter delivery[15], which hinders extrapolating outcomes of wound healing to myomectomy incisions;some correlations might prove some relevance. Relative strength of low transverse uterine scars wasreported in preterm uteri with yet under-developed lower segment, compared to the classic longitudinalscars. [16]
With all these theoretical uncertainties, the current research study aims to explore one aspect of suchcomparison: the amount of intra-operative blood loss during open myomectomy. Unfortunately, to ourknowledge, no previous studies addressed this issue.
MethodsStudy design:
A parallel randomized controlled pilot study conducted at Ain Shams University Maternity Hospital in theperiod between January 2017 and April 2018, in which �fty-two cases were recruited from thoseattending the outpatient gynecologic clinic, who were candidates for myomectomy.
Sample size calculation:
Sample size was calculated using the Power & Sample Size Calculator®, setting the power (1-b) at 0.8and the type-1 error (a) at 0.05. The primary outcome of the current study is the mean intraoperativeestimated blood loss (EBL). Reviewing the literature revealed no direct comparison between vertical andtransverse uterine incision for abdominal myomectomy. A trial comparing the two types of incision inlaparoscopic myomectomy was, however, found. This latter trial showed that the mean values forintraoperative EBL in transverse versus vertical uterine incision in laparoscopic myomectomy were 110.5± 81.7 ml and 136.4 ± 108.5 ml, respectively [17]. Therefore, transverse uterine incision would be assumedto reduce the mean intraoperative EBL by almost 18.9%. A previous study showed that the average blood
Page 4/15
loss during conventional abdominal myomectomy (which utilizes vertical uterine incision) was 621±121ml [18]. The mean intraoperative EBL with transverse uterine incision would, therefore, be assumed to be503 ml. Calculation according to these values, produces a minimal sample size of 17 women in eachgroup. Considering an attrition rate of 35% (to compensate for drop-outs due to the limited surgicalexperience with the novel technique in di�cult myomectomies), a total of 52 women were recruited.
Recruitment:
Criteria for inclusion in the study were as follows; single myoma measuring 5-10 cm in diameter, causingabnormal uterine bleeding, uterine pressure-related symptoms, infertility or recurrent pregnancy loss inwomen between 20 and 35 years of age, with BMI between 18.5-29.9 kg/m2. Candidates were excludedfrom the study if they had any of the following criteria; pregnancy, cases with bleeding tendency, priorlaparotomies, cases having coexisting pelvic pathologies, as ovarian cysts. All candidates had acomplete preoperative evaluation via clinical history taking, clinical examination and sonographicexamination for con�rmation of the exact site, size and number of uterine �broids and to exclude anycoexisting pelvic pathology, a venous blood sample for blood picture, liver and kidney functions as wellas coagulation pro�le, as a part of anesthetic workup.
Convenience sampling was utilized. The process of recruitment and handling the study population duringthe course of the study is shown in the CONSORT �ow diagram. Candidates were randomly assigned(with 1:1 allocation ratio) to one of two groups according to a computer generated sequence, distributedin sequentially numbered sealed opaque envelopes, allocated by the seventh author. Only the researchcandidates were blinded to the surgical technique.
Intervention:
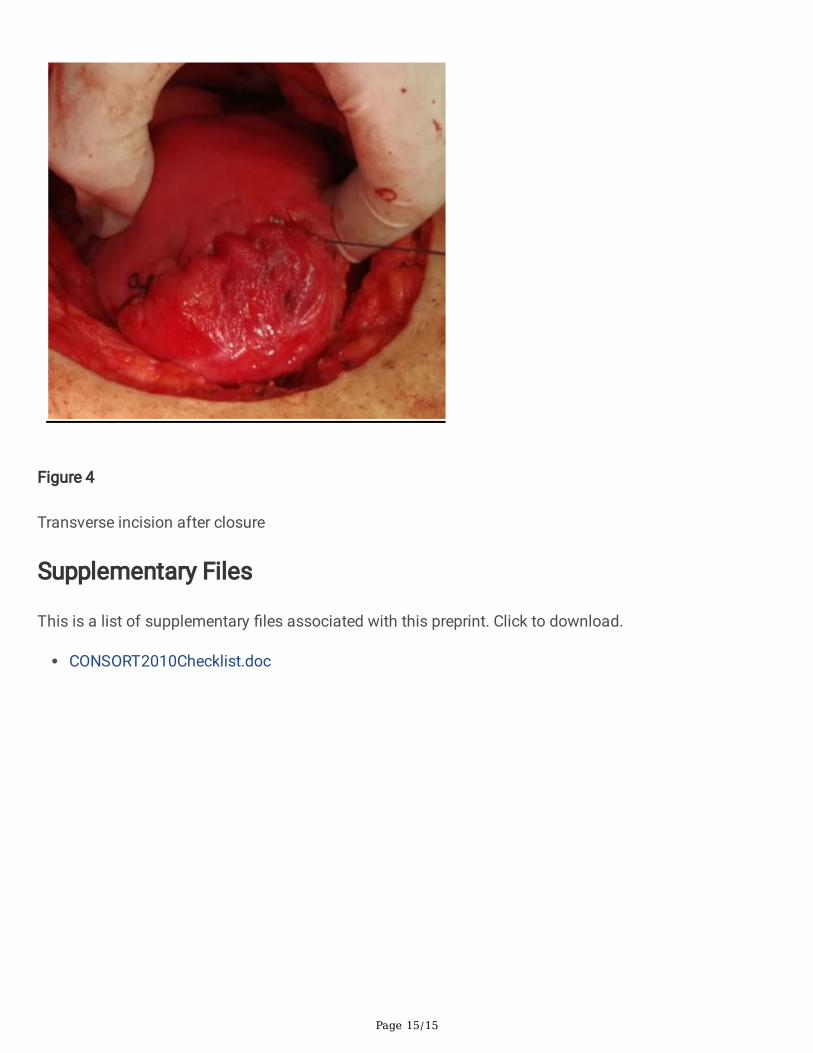
All candidates received general anesthesia and the abdominal cavity was accessed through aPfannenstiel incision. Research group A included 26 women who were planned for transverse uterineincision in which a transverse elliptical uterine incision is accustomed within the pseudocapsule in amanner that its transverse diameter is almost centralized over the myoma with a slight anterior shift. Itslength is 2 cm shorter than the maximum diameter of the myoma and ends well away from the tubalostia. Breadth of the ellipse is fashioned so that its edges wouldn't be under tension or redundant afterclosure, usually the breadth equals one third of its length [Figure 1]. Tissue planes are bluntly and/orsharply dissected and the myoma is resected with the overlying ellipse of myometrium andpseudocapsule leaving a relatively smaller zone of dead space for closure [Figure 2]. Myometrium is re-approximated in two layers using absorbable suture [Figure 3]. The uterine serosa is sutured in a runningfashion, exposing minimal suture material and raw area to minimize adhesion formation [Figure 4].Research group B included 26 women who were planned for standard longitudinal uterine incision.[5] Novasopressin or any other hemostatics were used to avoid their confounding effect on blood loss. Noperitoneal toilet was done and intra-peritoneal suction drains were left in all cases. Blood loss during theoperation was estimated as follows: obtaining the volume difference of blood in suction bottle containers
Page 5/15
(in ml), obtaining weight difference of linen towels (in gm) [weight of soaked linen towels – weight ofdry linen towels].[19] These differences were estimated from the beginning of the uterine incision till itsclosure. Estimated blood loss was also calculated by obtaining the difference between preoperative and24 hours postoperative hematocrit using the following formula:
EBV x (Hi-Hf)
Hi
Where the Hi is the preoperative blood hematocrit, Hf is the postoperative one and EBV is the estimatedblood volume. The estimated blood volume could be calculated by multiplying weight times averageblood volume which is around 65ml/kg in females.[20]
After exclusion of three patients (as shown in the CONSORT �ow diagram), a total of 25 women in theTransverse Uterine Incision group and 24 women in the Longitudinal Uterine Incision group were eligiblefor statistical analysis.
Postoperatively, all women were subjected to postoperative follow-up of vital data and suction drains for24 hours, and received NSAIDs for analgesia.
Research Study Outcomes:
Intraoperative blood loss as primary outcome, operative time and postoperative fever, de�ned astemperature of 38 C in the �rst 48 postoperative hours and persisting more than 24 hours [21], assecondary outcomes.
Statistical analysis:
Conducted using SPSS for Windows version 20. Per protocol analysis was adopted to avoid dilution oftreatment effect by excluded patients with surgically-di�cult myomectomies.
Data was represented as mean+/- SD (95% CI) for continuous parametric variables and median (IQR) fornon-parametric ones. Difference between two unrelated groups was analyzed using the independentStudent’s t test as well as the mean difference [MD] and its 95% con�dence interval [95% CI] (for numericparametric variables); Mann-Whitney’s U test (for numeric non-parametric variables); paired t test (forpaired numerical parametric variables); chi-squared test and Fischer exact test (for categorical variables).Signi�cance level was set at 0.05.
ResultsNo statistically signi�cant differences were found between women of both groups regarding age, bodymass index or parity. Also there were no signi�cant differences between women of both groups regarding

Page 6/15
frequency distribution of indications for myomectomy, myoma location according to FIGO sub-classi�cation [22], mean myoma size, preoperative hemoglobin or hematocrit. (Table 1)
Directly-estimated intra-operative blood loss (based on weight difference of gauze and towels andsuctioned blood volume) was lower in the transverse uterine incision group compared to the longitudinaluterine incision group (389.7 ± 98.56 vs 485.04 ± 230.6); though this difference failed to reach statisticalsigni�cance. (p value=0.07). Only one case needed postoperative blood transfusion, due to anemicsymptoms in the longitudinal incision group after an estimated blood loss of 1000 ml, but that was notstatistically signi�cant. (p value =0.48) (Table 2)
Postoperative repeated analysis of hemoglobin concentration revealed higher drop in hemoglobinconcentration in the longitudinal uterine incision group in comparison to the transverse uterine incisiongroup; though lacking statistical signi�cance. (p value=0.68) Similar �ndings were found on analysis ofhematocrit values in the two groups (p value=0.72). Calculated intraoperative blood loss (derived fromdifference between pre- and post-operative hematocrit values) between the two groups was higher in thelongitudinal incision group, yet this difference did not reach statistical signi�cance (p value=0.07). (Table2)
No statistically signi�cant difference was observed between the transverse uterine incision group and thelongitudinal uterine incision group regarding the operative time (p value=0.18). (Table 3)
There was no statistically signi�cant difference as regards the amount of �uid lost in the suction drain orincidence of postoperative pyrexia (p value =0.27,0.60 consecutively). (Table 3)
DiscussionAccording to the anatomical studies of the distribution of myometrial blood vessels, arcuate arteries runtransversely from lateral to medial, to join at the median plane. They give off radial arteries and spiralarterioles, which course centripetally towards the endometrium in also a transverse plane [7,23,24]. Thus, atleast theoretically, a longitudinal uterine incision will transect a large number of transversely runningarteries and arterioles. In comparison, a transverse uterine incision will parallel their course, leading to thetransection of a fewer number [9].
Moreover, suturing of a vertical incision places the sutures parallel to the course of the transverselyrunning vessels, which hinders adequate ligation of all transected arteries and veins, together with theirbranches and tributaries respectively. On the contrary, suturing transverse incisions places the suturesperpendicular to them, and thus, provides an effective hemostatic seal that surround all transectedvessels [9].
However, all these assumptions were based upon anatomical studies of normal uteri. Few studiesaddressed the distortion of myometrial vascular anatomy by the growing myomas. Studies of thevascular pattern of myomatous uteri by injection, micro-radiographic and histologic techniques revealed
Page 7/15
absence of an intrinsic vascular network to supply the �broid mass. However, vascular supply dependsupon localized expansion of the normal myometrial vasculature, where surrounding displaced anddistorted arcuate and radial arteries give off a number of small arteries that penetrate the myomaanywhere along its circumference [25]. Angiographic study by Discepola and his colleagues, of the courseof the arterial blood vessels encircling uterine myomas revealed that the neo-vessels, developing aroundmyomas, do not follow the normal anatomy of myometrial vasculature. Instead, on the surface ofanterior and posterior wall myomas, blood vessels run mostly diagonally, e.g. 49.2% of the blood vesselson the surface of posterior wall myomas run diagonally with an angle 30-60◦ with the horizontal plane,and 21.7% run mostly horizontally with an angle 0-30◦; whereas 29.2% run mostly vertically with an angle60-90◦. In addition, nearly 40% of the vessels crossed the myoma midline [26].
Based on these �ndings, Discepola and his colleagues concluded that arterial vessels on the surface ofmyomas can be injured whatever the direction of uterine incision[26]. However, it seems that thisconclusion stems more from a radiological perspective, rather than a surgical one. Since the inherentnature of surgery implies injury of some blood vessels, and it is the art of surgery that strives forrespecting anatomy and minimizing tissue damage, especially to large vessels and vital structures. Infact, it is logically plausible from a surgical perspective that if a major portion of blood vessels runs withan angle between 0-60◦, a transverse incision would be less traumatic than a longitudinal incisiontransecting all horizontally- and transversely-directed arterial vessels. Moreover, the conclusion ofDiscepola and his colleagues is further limited by the fact arteriographic techniques usually fail tovisualize veins and small arterial vessels. They are usually limited to arterial vessels with a diameterexceeding that of the 5-F catheter (1.67 mm).[26]
Micro-radiographic and histologic studies revealed that the venous drainage of �broids is sparsecompared to the arterial supply, with only few moderate-sized draining veins are occasionally seen.However, intramural �broids cause signi�cant compression and distention of the surrounding arcuatevenous plexus. These distended venous channels contribute substantially to the heavy bleeding duringmyomectomy [25]. Thus, a transverse uterine incision would be least traumatic to the transversely directedmyometrial arteries, aretrioles and venous channels, and to the diagonally directed �broid feedingvessels.
This theory was previously questioned by Morita and his colleagues in the setting of laparoscopicmyomectomy. Transverse uterine incisions were associated with signi�cant decline in operative bloodloss compared to longitudinal incisions (137.6 ± 88.1 vs. 235.8 ± 169.4 mL respectively). This declinewas more evident in large myomas (> 7 cm in diameter); with an estimated blood loss 158.9 ± 87.1 mL intransverse incisions, compared to 362.3 ± 147.3 mL in longitudinal incisions. Whereas no statisticallysigni�cant differences were found between either incisions in smaller myoma (< 7 cm).[17] Logically, asthe uterine incision is extended longitudinally, its traumatic effect is more pronounced, with the greatertransection of traversing vessels; in contrast to the transection of vessels of the same axial plane withextension of the transverse incision. This effect might not be evident with smaller myomas. However,

Page 8/15
validation by further studies is needed, as the proposed effect of myoma size in the study of Morita [17] isconfounded by the large difference in operative time with myomas > 7 cm between longitudinal incision(165.4 min) and transverse incision (129 min), owing to the easier suturing technique of transverseincisions relative to the longitudinal ones.
Despite the disparities between the laparoscopic and open approaches for myomectomy, in addition topretreatment with gonadotrophin-releasing hormone analogs and intra-myometrial vasopressin injectionin the study of Morita; however, the underlying surgical theory of transection of more transversely runningvessels with longitudinal incisions might also be held true in case of open myomectomies.
In consistence with the same theory, the results of this study report the absence of statistically signi�cantdifferences in intra-operative blood loss using either incisions. It should be noted that only myomas < 10cm in diameter were included in our study, with an average myoma size of approximately 8 cm.
Postoperative pyrexia following myomectomy has been linked to the development of myoma-bedhematoma [21], which is linked with the subsequent weakening of the developing scar [12]. In this study,postoperative pyrexia developed in one patient in the transverse incision group and in two patients in thelongitudinal incision group. However, being a secondary outcome, our sample size is underpowered todetect a signi�cant difference in the incidence of such uncommon complication.
To sum up, based on our results, it is evident that blood loss is comparable using transverse orlongitudinal incisions, at least with myomas ranging < 10 cm in size. This provides the base for furtherstudies investigating the impact of incision direction on blood loss in larger myomas, incidence ofmyoma-bed hematoma, obstetric-quality of the ensuing scar, and formation of pelvic adhesions.
Among the strengths of this study: (1) up to our knowledge, this is the �rst study to explore the effect ofuterine incision direction in open myomectomy; (2) homogeneity of patients within the two groupsregarding the number, size and site of myomas; (3) estimation of intraoperative blood loss both directlyand indirectly. Limitations include: (1) although we tried to restrict the range of myoma sizes, we failed tostatistically adjust blood loss to varying myoma size due to limited sample size; (2) different surgeonswere involved in the study, although all had similar adequate experience.
ConclusionBlood loss from transverse uterine incision is comparable to longitudinal incision in open myomectomy.
AbbreviationsAUB: abnormal uterine bleeding
BMI: body mass index
EBV: estimated blood volume
Page 9/15
EBL: estimated blood loss
RPL: recurrent pregnancy loss
DeclarationsEthics approval and consent to participate:
The study was approved by Ain Shams University, Faculty of Medicine Research Ethics Committee (FWA000017585) in September 2016 (with the number FMASU MD 264/2016) and was registered as a clinicaltrial with the number NCT03009812 in January 2017. All candidates signed a written informed consent.
Consent for publication:
Not applicable.
Availability of Data and Materials:
The data used to support our �ndings are available from the corresponding author if requested.
Con�icts of interest:
The authors declare that they have no con�icts of interest.
Funding:
This research was not funded by any organization.
Authors’ contribution:
The �rst author; AE was concerned with the planning of the research, AF was responsible for datagathering, KA conducted the statistical analysis, last author MN was responsible for writing and revisingthe manuscript, and all authors; AE, HH, MES, ME, MAE, AF, KA and MN contributed to the experimentalwork.
Acknowledgements:
Not applicable.
References1. Marret H, Fritel X, Ouldamer L, Bendifallah S, Brun JL, De Jesus I, Derrien J, Giraudet G, Kahn V,
Koskas M, Legendre G, Lucot JP, Niro J, Panel P, Pelage JP, Fernandez H, CNGOF (French College ofGynecology and Obstetrics). Therapeutic management of uterine �broid tumors: updated Frenchguidelines. Eur J Obstet Gynecol Reprod Biol. 2012 Dec;165(2):156-64.
Page 10/15
2. Tinelli A, Mettler L, Malvasi A. Impact of surgical approach on blood loss during intracapsularmyomectomy. Minim Invasive Ther Allied Technol. 2014; 23(2): 87-95.
3. Berkeley C, Bonney V. A Textbook of Gynaecological Surgery. NewYork, NY: Funk and Wagnalls;1911:418–420
4. Verkauf BS. Changing trends in the treatment of leiomyomata uteri (review). Curren. Opin. Obstet.Gynaecol. 1993; 5:301-310.
5. Breech LL, Rock JA. Leiomyomata Uteri and Myomectomy. In: TeLinde’s operative gynecology, 10th
ed, Rock JA, Jones HW III (Eds), Lippincott Williams & Wilkins, Philadelphia 2008. P. 716-718
�. Falcone T, Drake RL, Hurd WW. Surgical anatomy of the abdomen and pelvis. In: ClinicalReproductive Medicine and Surgery, Falcone T, Hurd WW (Eds), Mosby Elsevier, Philadelphia 2007.P.123.
7. Farrer‐Brown G, Beilby JO, Tarbit MH. The blood supply of the uterus: 1. Arterial vasculature. BJOG:An International Journal of Obstetrics & Gynaecology. 1970 Aug;77(8):673-81.
�. Saeki M, Kotaki S. Vasculature of uterine myoma for myomectomy. Acta Obstet Gynecol Jpn1974;26:335-42.
9. Igarashi M. Value of myomectomy in the treatment of infertility [letter]. Fertil Steril. 1993;59:1331
10. Louros NC. Conservative myomectomy. Postgrad Med 1964;35:52-6.
11. Parsons L, Ulfelder H. An atlas of pelvic operations. 2nd ed. Philadelphia: WB Saunders, 1968:70-1.
12. Dubuisson, J.B., Chavet, X., Chapron, C Gregorakis SS, Morice P. Uterine rupture during pregnancyafter laparoscopic myomectomy. Hum. Reprod. 1995, 10, 1475–1477.
13. Royal College of Obstetricians and Gynaecologists (RCOG). Birth after Previous Caesarean Birth(Green-top Guideline No. 45). London. RCOG; October 2015.
14. Greene RA, Fitzpatrick C, Turner MJ. What are the maternal implications of a classical caesareansection? J Obstet Gynaecol. 1998;18(4):345‐347. doi:10.1080/01443619867083
15. Takamoto N, Leppert PC, Yu SY. Cell death and proliferation and its relation to collagen degradationin uterine involution of rat. Connect Tissue Res. 1998;37:163–175.
1�. Halperin ME, Moore DC, Hannah WJ. Classical versus low-segment transverse incision for pretermcaesarean section: maternal complications and outcome of subsequent pregnancies. Br J ObstetGynecol. 1988;95(10):990-6.
17. Morita M, Asakawa Y, Uchiide I, Nakakuma M, Kubo H. Surgery results using different uterine wallincision directions in laparoscopic myomectomy of the intramural myoma. Reprod Med Biol 2004;3(1): 33-7.
1�. Celik H, Sapmaz E. "Use of a single preoperative dose of misoprostol is e�cacious for patients whoundergo abdominal myomectomy": Fertil Steril, 2003; 79 (5): 1207-10.
19. Al Kadri HM, Al Anazi BK, Tamim HM. Visual estimation versus gravimetric measurement ofpostpartum blood loss: a prospective cohort study. Arch Gynecol Obstet. 2011;283(6):1207-13.
Page 11/15
20. Miller RD. Transfusion Therapy. In: RD Miller Editor. Anesthesia, Philadelphia Churchill-Livingston 5thEdition, 2000; Ch. 46: 1613-7.
21. Vavilis D., Togaridou E, and Agorastos T. Abdominal myomectomy and febrile morbidity. Int JGynecol Obstet 2005;88(1):61
22. Munro MG, Critchley HO, Broder MS, Fraser IS, and FIGO Working Group on Menstrual Disorders."FIGO classi�cation system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravidwomen of reproductive age": Int J Gynaecol Obstet, 2011; 113: 3–13.
23. Sampson JA. The in�uence of myomata on the blood supply of the uterus, with special reference toabdominal uterine bleeding. Surg Gynecol Obstet 1913; 16: 144–180.
24. Faulkner RL.An injection study of uterine blood vessels.Am J Obstet Gynecol 1945; 49: 1–9.
25. Farrer-Brown G, Beilby JO, Tarbit MH. The vascular patterns in myomatous uteri. J Obstet GynaecolBr Commonw 1970; 77: 967–975.
2�. Discepola F, Valenti DA, Reinhold C, Tulandi T. "Analysis of arterial blood vessels surrounding themyoma: relevance to myomectomy": Obstet Gynecol, 2007; 110: 1301.
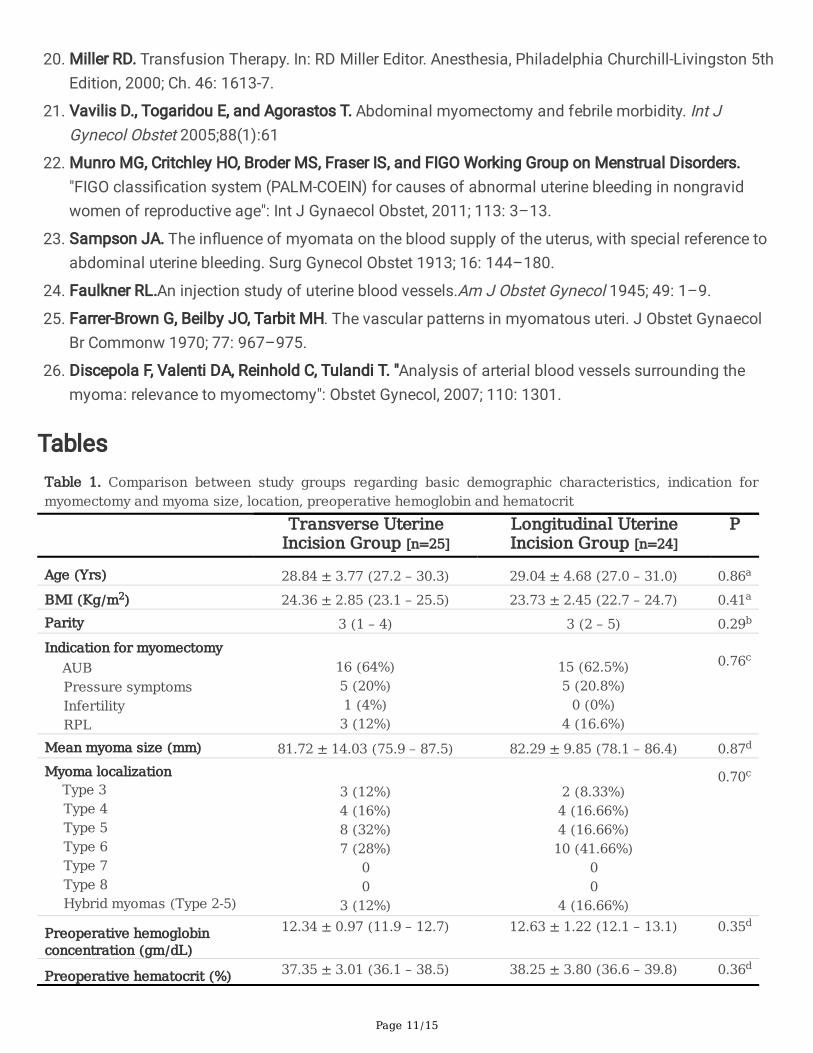
TablesTable 1. Comparison between study groups regarding basic demographic characteristics, indication formyomectomy and myoma size, location, preoperative hemoglobin and hematocrit
Transverse UterineIncision Group [n=25]
Longitudinal UterineIncision Group [n=24]
P
Age (Yrs) 28.84 ± 3.77 (27.2 – 30.3) 29.04 ± 4.68 (27.0 – 31.0) 0.86a
BMI (Kg/m2) 24.36 ± 2.85 (23.1 – 25.5) 23.73 ± 2.45 (22.7 – 24.7) 0.41a
Parity 3 (1 – 4) 3 (2 – 5) 0.29b
Indication for myomectomyAUBPressure symptomsInfertilityRPL
16 (64%)5 (20%)1 (4%)3 (12%)
15 (62.5%)5 (20.8%)
0 (0%)4 (16.6%)
0.76c
Mean myoma size (mm) 81.72 ± 14.03 (75.9 – 87.5) 82.29 ± 9.85 (78.1 – 86.4) 0.87d
Myoma localizationType 3Type 4Type 5Type 6Type 7Type 8Hybrid myomas (Type 2-5)
3 (12%)4 (16%)8 (32%)7 (28%)
00
3 (12%)
2 (8.33%)4 (16.66%)4 (16.66%)10 (41.66%)
00
4 (16.66%)
0.70c
Preoperative hemoglobinconcentration (gm/dL)
12.34 ± 0.97 (11.9 – 12.7) 12.63 ± 1.22 (12.1 – 13.1) 0.35d
Preoperative hematocrit (%) 37.35 ± 3.01 (36.1 – 38.5) 38.25 ± 3.80 (36.6 – 39.8) 0.36d

Page 12/15
AUB, abnormal uterine bleeding; RPL, recurrent pregnancy lossa Analysis using unpaired t-test.b Analysis using Mann-Whitney U-test.c Analysis using chi squared test.d Analysis using unpaired t-test with Welch’s correction.e According to the Leiomyoma FIGO sub-classification system [22]
Table 2. Comparison between study groups regarding directly-estimated intra-operative blood loss, need forblood transfusion, postoperative hemoglobin and hematocrit drop and calculated blood loss.
Transverse UterineIncision Group [n=25]
Longitudinal UterineIncision Group [n=24]
P
Estimated intra-operativeblood loss (mL)
389.7 ± 98.56 (349.0 – 430.4) 485.04 ± 230.6 (387.6 – 582.4) 0.07a
Need for blood transfusion 0 (0%) 1 (4.16%) 0.48b
Hemoglobin concentration(gm/dL)
PreoperativePostoperativeMean Paired difference (95% CI)
12.34 ± 0.9710.68 ± 1.02-1.65 ± 0.71
(-1.95 – -1.36)
12.63 ± 1.2210.13 ± 1.81-2.50 ± 1.84
(-3.28 – -1.72)
0.68c
Hematocrit (%)PreoperativePostoperativeMean Paired difference (95% CI)
37.35 ± 3.0129.92 ± 2.88-7.43 ± 2.12
(-8.31 – -6.55)
38.25 ± 3.8028.37 ± 5.07-9.87 ± 5.28
(-12.10 – -7.64)
0.72c
Calculated intraoperativeblood loss (mL)
311.78 ± 78.85 (279.2 – 344.3) 388.03 ± 184.55 (310.1 – 465.9) 0.07d
a Analysis using unpaired t-test with Welch’s correction.
b Analysis using Fisher’s exact test.
c Analysis using repeated measure ANOVA test. Only p value for between-subject effect is displayed.
d Analysis using unpaired t-test.

Page 13/15
Table 3. Comparison between study groups regarding operative time, fluid in suction drain and incidence ofpostoperative pyrexia.
Transverse Uterine IncisionGroup [n=25]
Longitudinal Uterine IncisionGroup [n=24]
P
Total operativetime (min)
59.96 ± 16.78 (53.0 – 66.8) 66.58 ± 17.33 (59.2 – 73.9) 0.18a
Fluid in suctiondrain (mL)
123.0 ± 37.79 (107.3 – 138.6) 113.5 ± 20.27 (104.9 – 122.0) 0.27b
Postoperativepyrexia
1 (4.0%) 2 (8.33%) 0.60c
a Analysis using Mann-Whitney U-test.
bAnalysis using unpaired t-test.
c Analysis using Fisher’s exact test.
Figures
Figure 1
Transverse elliptical uterine incision

Page 14/15
Figure 2
Transverse incision after removal of the myoma
Figure 3
Closure of transverse incision
Page 15/15
Figure 4
Transverse incision after closure
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.
CONSORT2010Checklist.doc