Embed Size (px)
Citation preview

767
Randomised trial of late thrombolysis in patients with suspectedacute myocardial infarction
*Steering Committee: E Paolasso (study chairman), E San Martín(co-chairman), G Ravizzini (ECG analysis), R Díaz, G Covelli(international coordinators) (Argentina). G Romero (Argentina);JE Sousa, L Soares Piegas (Brasil); H Chamorro, I Mordoh (Chile);M Adorno Artaza (Paraguay); E Besada, E Sandoya (Uruguay); andJ Isea Perez, C Dávila (Venezuela) (national coordinators).
Correspondence to: Dr Ernesto Paolasso, EMERAS, Mendoza1507-5° Piso "A", 2000 Rosario, Argentina
SummaryIn 1985 an overview of clinical trials confirmed that patientstreated within 6 h of the onset of symptoms of myocardialinfarction benefited from thrombolytic therapy. Doubt
remained about treatment later than this and this uncertaintyprompted further randomised studies. The South Americanmulticentre trial EMERAS is one of these.
4534 patients entering hospital up to 24 h after the onsetof suspected acute myocardial infarction were randomisedbetween intravenous streptokinase (SK) 1 5 MU and placebo,during the period January, 1988, to January, 1991. Once theresults of ISIS-2 were known, only patients presenting morethan 6 h after symptom onset were randomised. There was no
significant difference in mortality during the hospital stay(269/2257 [11·9%] deaths among SK patients vs 282/2277 [12 4%] in controls). Among the 2080 patientspresenting 7-12 h from symptom onset there was a non-significant trend towards fewer deaths with SK (11 7% SK vs13 2% control; 14% [SD 12] reduction with 95% confidenceinterval [Cl] of 33% reduction to 12% increase), whereas therewas little difference among the 1791 patients presenting after13-24 h (11 4% vs 10 7%; 8% [16] increase with a 95% Cl of20% reduction to 45% increase). These 95% Cls are wide andare consistent with the results of previous studies amongpatients presenting late after symptom onset.The EMERAS results, though not conclusive on their own, do
contribute substantially to accumulating evidence on thequestion of whether fibrinolytic therapy really does produce anyworthwhile improvement in survival among such patients.
Lancet 1993; 342: 767-72
Introduction
Fibrinolytic therapy reduces mortality among patientstreated within a few hours of the onset of acute myocardialinfarction (AMI).14 However, many patients with
suspected AMI do not reach hospital until several hoursafter symptoms begin. An overview of fibrinolytic trialsthat were completed during the 1960s and 1970s suggestedsome benefit even when patients were treated more than afew hours after symptom onset,s and this was subsequentlysupported by large randomised trials of rapid high-doseintravenous streptokinase (SK), notably, ISIS-21 andGISSI-1.2 An overview of these high-dose SK trials leftlittle doubt that mortality is reduced by a worthwhileamount among patients treated within 0-3 h (31%) and at3-6 h (22%) but the benefit was less certain among patientstreated more than 6 h after symptom onset (10-8% deathamong SK patients vs 12-3% among controls).1 Theapparent avoidance of 15 deaths per 1000 patients treatedafter 6 h might seem medically worthwhile but the 95%confidence interval (CI) around this 14%, reduction was1-24%, consistent with there being little or even no effecton mortality.To help determine more reliably the "time window" for
worthwhile benefit from fibrinolytic therapy, EMERAS(Estudio Multicentrico Estreptoquinasa Republicas deAmerica del Sur) randomised to SK or placebo patientspresenting up to 24 h from the onset of pain in whom therewas not thought to be a clear indication for fibrinolytictherapy. It was also planned6 that the results wouldcontribute to a collaborative overview of trials addressingthe late thrombolysis issue.7
Patients and methods
To encourage recruitment, the trial was kept simple-with wideeligibility, minimal data collection, and no restrictions on ancillarytreatments.6,8 4534 patients were randomised between January,1988, and January, 1991, in a network of 236 hospitals in six SouthAmerican countries. The trial was organised in Argentina byregional coordinators and in the other countries by nationalcoordinators. Overall coordination was by the EMERAS
Coordinating Centre in Rosario, Argentina, in collaboration withthe Clinical Trial Service Unit in Oxford, UK.
EligibilityInitially, patients were eligible if they were thought to be within24 h of the onset of suspected AMI (with or without
electrocardiographic [ECG] changes), and to have no clearindication for, or contraindication to, SK. Soon after the studybegan, it became clear that fibrinolytic therapy was beneficial forpatients presenting within 6 hl,2 so the entry criteria were altered toinclude only those patients presenting betwen 6 and 24 h fromonset. The only absolute contraindications to SK specified by theprotocol were a history of stroke, gastrointestinal haemorrhage, orulcer within the previous 6 months. Other contraindications werespecified not by the protocol but by the physician responsible, and

768
the organisers merely suggested that these might include severetrauma such as major surgery, head injury, or biopsy within theprevious 2 weeks, prolonged cardiac massage in the previous 24 h,persistent severe hypertension, valvulopathy or cardiomyopathywith atrial fibrillation, active pericarditis, known allergy to SK, SKtreatment within the previous 6 months, pregnancy, severe renal orhepatic impairment, or some other life-threatening disease.
Patients were to be entered once only into EMERAS.
ConsentPrevious studies had demonstrated that the sooner fibrinolytictherapy was started the more effective it was at saving lives.uz Sothe degree and timing of consent was left to individual doctors todecide for individual patients, in the light of local requirements andadvice from the local ethics committees who gave approval for thestudy.
Randomisation
Eligible patients were randomised in each participating centre byuse of sequentially numbered sealed envelopes prepared centrallyby the Clinical Trial Service Unit. Baseline details were to berecorded (table 1) on the entry form attached to the next envelopeavailable before the envelope was opened. This entry form was tobe sent immediately to the coordinating centre. Active treatmentand placebo were evenly allocated in blocks of 8 within eachcentre.
TreatmentSK (1 -5 MU Streptase) or matching placebo (hepatitis-B-antigen-free albumin) was infused intravenously over about 1 h in 100, mLsaline. The trial infusion was to be interrupted only if this wasthought by the responsible physician to be clearly indicated. At thebeginning of the study, patients were also being randomly allocatedto oral aspirin or placebo in a 2 x 2 factorial design. The emergenceof clear evidence of benefits from aspirin use in AMI’ led tocollaborators being informed in May, 1988, after 324 patients hadentered the study, that this comparison was to be discontinued andthat daily low-dose aspirin (160 mg) was recommended strongly forall patients unless there was a clear contraindication. In all otherrespects, physicians were free to use whatever additional therapy(including anticoagulants) they considered indicated. Compliancewith trial treatment and the use of non-trial therapy was recordedon the single-sided form completed after discharge. Whether or notthe correct trial treatment was given, patients remained in thegroup to which they had been randomised, for an intention-to-treatanalysis.9
Data recorded
After discharge, a pre-randomisation ECG and a simple single-sided form were sent to the national coordinators who would returnthe forms for completion if data were missing. They were thenforwarded to the coordinating centre. These forms providedidentifiers to assist central 1-year mortality follow-up, and alsobrief details of medical history, treatments given, side-effects oftrial treatment, and major events (and their timing) in hospital.ECGs were read "blind" to treatment allocation by three
observers. Analysable ECGs were not received for 11 % of patients.If bundle-branch block (BBB) was present (7% of ECGs), thisalone was noted, otherwise the ECG categories were:Anterior ST elevation (37%). 2 mm in at least two of leads V, toV6, I, or aVL.Inferior ST elevation (30%). 1 mm in at least two of II, III, oraVF.Inferior and anterior ST elevation (6%). both of the above.ST depression (4%). None of the above, but with ST depression of 1 mm in at least two limb leads or 2 mm in at least two
precordial leads.Other abnormality (14%). None of the above, but with: (a)pathological Q-waves (9"o) 2 mm and 30 ms in any lead otherthan aVR or V1; or (b) no Q-waves but T-wave inversion (4%) inany lead other than aVR or V 1; or (c) left-ventricular hypertrophy,
BP = blood pressure.
Table 1: Baseline characteristics (% of number randomised)
conduction defects (eg, atrioventricular block), or arrhythmias (eg,atrial fibrillation, supraeventricular tachycardia).Normal (2%). Any remaining ECGs.For any stroke, the day on which it occurred was recorded,
allowing separate examination of strokes on days 0-1 (when anexcess was observed with SK in ISIS-21) or later (when a shortfallwith SK had previously been reported.)* Collaborators were alsoasked to seek a neurological opinion as to whether the stroke wasprobably haemorrhagic or probably ischaemic, and whether thedisability was likely to prove significant or not significant.l For allreports of stroke, further details (including investigations such ascomputerised tomographic scans and necropsy reports) were thenrequested from investigators. Confirmation or refutation of strokeand its aetiology was based on blind central review of the records bya committee comprising a neurologist, cardiologist, and generalphysician.
Follow-upIn-hospital follow-up was based on the discharge forms. 1-yearfollow-up was of vital status only and was obtained by nationalcoordinators contacting patients or their relatives. Discharge formswere available for all randomised patients but 41 (23 SK, 18placebo). Discharge alive was at a median of 11 days, and thecompleteness of mortality follow-up is 99°° to discharge, 97% to 5weeks, and 90% to 1 year, with no systematic differences betweenthe treatment groups. About nine-tenths of all deaths in the first 5weeks occur in hospital, so it is probable that more than 98% of the5-week deaths among all randomised patients have been included.
Statistical methods
The main end-points were to be mortality in hospital and at the endof the first year. In the light of results from the previous overview5(and from more recent large trials1,2), it seemed reasonable that
fibrinolytic therapy might reduce early morbidity by at least 15-20deaths per 1000 patients treated. For reasonable power to detectsuch an effect, it was planned to randomise more than 4000 patientsby EMERAS. The principal subsidiary analysis was to be of theeffects of SK on in-hospital mortality subdivided by hours frompain onset (0-6, 7-12, 13-24), with a similar analysis for 5-weeksmortality to allow for comparisons with other major fibrinolytictrials. Comparisons of survival to 1 year involve time-to-death
analysis with log-rank methods,9 but for events in hospital anddeaths during the first 5 weeks, comparisons were by simpleanalysis of total numbers affected.7 Probability values are two-sided throughout and 2p > 0-05 is "not significant" (NS).
769
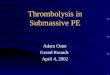
*May also have been given subcutaneous heparin.
Table 2: Compliance with allocated treatment and othermedical management in hospital (as % of those surviving todischarge for whom discharge form was received
Interim data monitoringDuring recruitment, interim results on events in hospital werereviewed three times by an independent data-monitoringcommittee, which, in the light of these analyses or any otherevidence or advice, would tell the coordinators if, in their view,there was at any time proof beyond reasonable doubt (ie, at least3 SD) that for all or for some types of patient either treatment wasclearly indicated or clearly contraindicated in terms of a netdifference in mortality. (This approach had the practical advantagethat the exact number of interim analyses would be of littleimportance.9) Otherwise, the coordinators, organising committee,collaborators, and sponsors were to remain ignorant to the interimresults. The demonstration in another trial’ of a survival benefitwith aspirin led to that comparison being discontinued. For thefibrinolytic comparison, however, no clear differences emergedduring this monitoring, and randomisation continued until Jan 31,1991, by which time almost all the SK and matching placeboprovided for the trial had been used.
Results
Of 8124 consecutive patients admitted to the participatingcentres with a diagnosis of suspected AMI, 4534 wererandomised, with 128 (3%) presenting within 3 h of
symptom onset, 535 (12%) between 4 and 6 h, 2080 (46%)between 7 and 12 h, and 1791 (40%) between 13 and 24 h(table 1). The main reasons for exclusion were a delay fromsymptom onset to presentation of less than 6 h or of morethan 24 h (66%), contraindications to SK (13%), doubtfulMI (8%), and administrative reasons (10%), no reasonbeing recorded in only 4% of patients, 2257 patients wereallocated to receive SK and 2277 placebo, and baselinecharacteristics were well balanced (table 1). The mediantime to entry from pain onset was 11 h, which is, as
intended, longer than in previous trials. Half the patientswere still in pain at the time of randomisation. The studyincluded a high proportion of older patients and of patientswithout ST elevation on their entry ECG (table 1).Among those patients who were discharged alive (at a
median of 11 days), the infusion had been completed in 98 %of patients allocated placebo and 96% of those allocatedSK. Aspirin was strongly recommended in the protocolafter ISIS-2, and 82% of patients received aspirin or someother antiplatelet regimen. Anticoagulation use was
optional, with 23% receiving intravenous heparin and anadditional 14% receiving subcutaneous heparin alone.
Antiplatelet and anticoagulant use was similar in the twogroups (table 2).
Possible side-effects and other events in hospitalThe reported excesses with SK of hypotension, allergicreactions, minor non-cerebral bleeds, major bleeds (ie,those requiring transfusion of at least one unit of blood),gastrointestinal symptoms, and arrhythmias were similar tothose in previous studies (table 3).1,2 Hypotension led todiscontinuation of trial treatment in only a small proportionof patients. Allergic reactions were in most cases confined to
n = no with discharge form. *% SK minus % placebo.
Table 3: Possible side-effects reported in hospital
rash, pyrexia, or shivering, and only 2 reports of
anaphylactic shock (both in the SK group) were confirmedon blind review. There was a significant trend (2 p > 0-01)towards the excess of any bleeds caused by SK increasingwith the addition of heparin (absolute excess with noheparin 45% [SD 1-1], with subcutaneous heparin alone5-3% [1’4], and with intravenous heparin 5-6% [1’3]).
Overall there was no significant difference between thetreatment groups in the incidence of stroke in hospital (table4). Early after the start of treatment there was a small butsignificant excess of strokes. After this early period, therewere non-significantly fewer strokes in the SK group. Halfthe patients who had a stroke died in hospital and aboutone-quarter of the survivors were considered to be disabled.MI was confirmed in 89% of patients, with no significantdifferences between the treatment groups in the reportedfrequency of infarct confirmation or other clinical eventsrecorded in hospital. In particular, among patientsallocated SK, most of whom also received aspirin, there wasno excess of reinfarction.
Effects on mortality subdivided by delay from symptomonset to randomisation
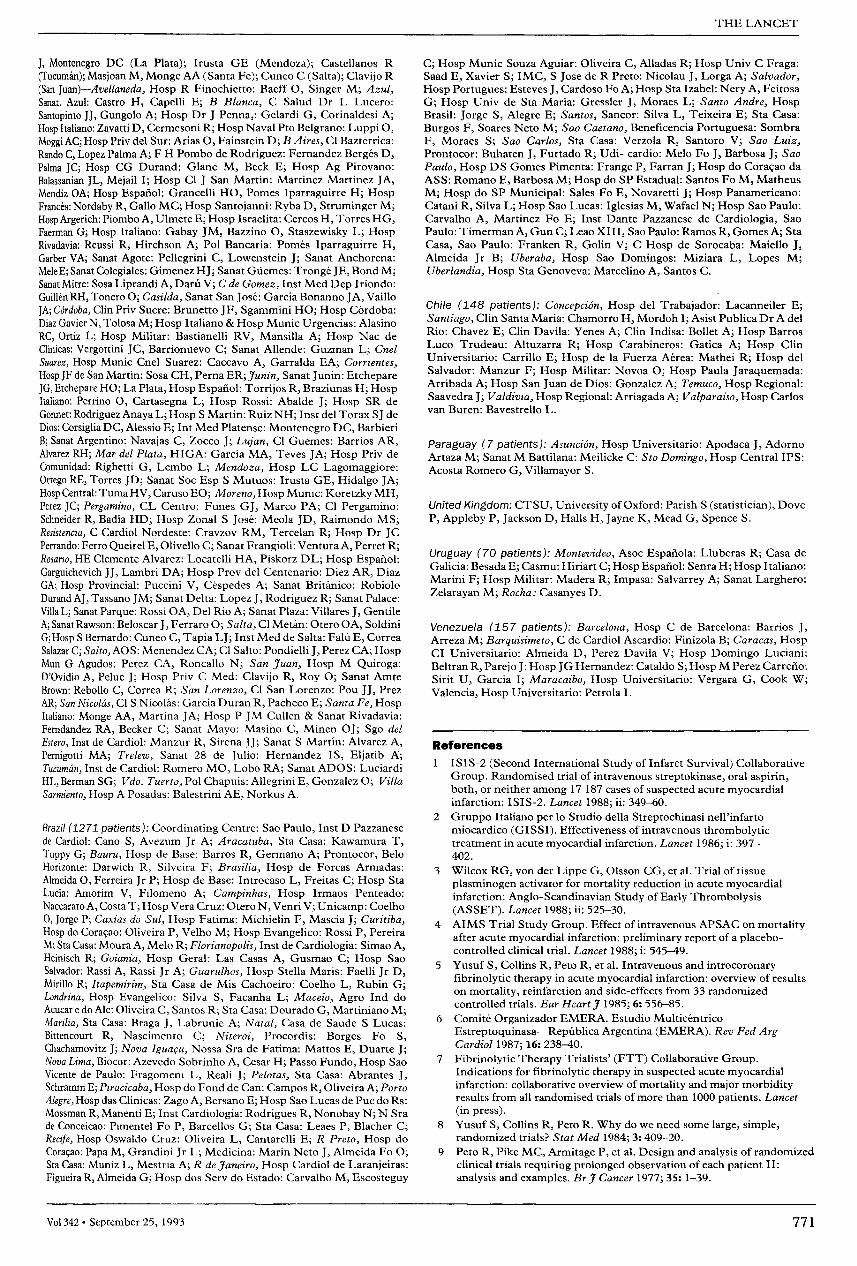
Overall, there were no significant differences in mortalityduring the hospital stay (11-9% deaths among SK patients
n = no with discharge form. *% placebo minus % SK.
Table 4: Effects of allocated treatments on clinical events in
hospital (up to day 35 or prior discharge)

770
Figure: Deaths In hospital and in days 0-35, subdivided by hoursfrom pain onsetRatio of odds of death in SK group to that in controls is plotted for eachsubdivision (black squares with area proportional to amount ofinformation contributed’), with 95% CI (horizontal line). Overall resultsand 95% CI intervals represented by diamonds.
vs 12-4% in controls, figure). Among the 2080 presenting7-12 h from symptom onset there was a non-significanttrend towards fewer deaths with SK (a 14% [12] reductionwith 95% CI of 33% reduction to 12% increase), whereasthere was little difference apparent among the 1791 patientspresenting after 13-24 h (8% [16] increase with 95% CI of20% reduction to 45% increase). These 95% CIs are wide,and the results are consistent with the moderate differences
suggested by previous trials.14No significant differences, overall or in those
prospectively defined delay-from-pain subgroups, wereseen with further follow-up to day 35 (figure) or to 1 year(table 5). When analyses were confined to patients with STelevation or BBB on the presenting ECG, there were still nosignificant differences in survival and the CIs for 35-daysurvival were even wider for those presenting in 0-6 h (a 4%[14] reduction with a 95% CI of 28% reduction to 27%increase; and for 7-12 h a4% [17] increase with a 95% CIof24% reduction to 44% increase). Further subdivision ofmortality results with respect to other baselinecharacteristics did not suggest any differences from theoverall results. In particular, the effect on in-hospitalmortality was similar among those patients who still hadchest pain at the time of randomisation (13-3% dead amongSK-allocated patients vs 13-5% among controls; 1% [12]reduction) and among those who did not (10-1 % 10-5%;4% [15] reduction).
Discussion
EMERAS confirms previous findings that fibrinolytictherapy increases the risk of stroke during the first few daysafter treatment,1,7 but this early and significant excess waslargely offset by a later reduction in ischaemic strokes, andthere was little difference in total strokes. No excess ofreinfarction was observed in the SK group (over 80% ofwhom also received aspirin or some other antiplateletagent), which is consistent with the ISIS-2 results for
*% placebo minus % SK (with 95% CI).Life-table analyses: median follow-up is 13 months.
Table 5: Effects of treatment on death by 1 year
patients allocated to SK and aspirin.’ There was a trend,albeit non-significant (2p=0’08), towards fewer cardiacarrests among the patients allocated to SK. If confirmed byother studies among patients presenting late after the onsetof infarction, it would be consistent with the hypothesis thatlate thrombolysis produces benefit, at least in part, throughan antiarrhythmic effect. 10
In experimental infarction, coronary reperfusion leads tosignificant myocardial salvage only when instituted earlyafter coronary occlusion.11-14 In patients, however, there iswide variability in the speed of infarct evolution, withevidence of infarction continuing over several hours in alarge proportion of patients.’ Patients may experience"stuttering" symptoms, reflecting intermittent coronaryocclusion and spontaneous recanalisation, 16 and in thissituation fibrinolytic therapy may limit the eventual extentof infarction even if given late. Moreover, laterecanalisation may limit infarct extension by providingcollateral flow in the event of subsequent coronary arteryocclusion.1O Late fibrinolytic therapy may produce benefitthrough a variety of other mechanisms, including improvedventricular function,17 limitation of post-infarctionventricular dilatation and aneurysm formation,18,20reduction of ventricular electrical instability and the
frequency of serious arrhythmias,l 1,22 and reduction of theoccurrence of left ventricular thrombus formation.23
Overviews of previous studies of long-term infusion ofSKS and of high-dose intravenous SK1 suggested that delayto treatment is associated with a gradual diminution of themortality reduction produced by SK. Among patientstreated more than 6 h after pain onset in the previoushigh-dose SK trials there was a 14% (SD 6) reduction in35-day mortality.’ Although EMERAS recruited 4000patients, it did not prove to be large enough to detect orexclude such effects reliably,6 and the CIs around theobserved effects on mortality among patients treated 7-12 hfrom symptom onset (15% [12] reduction; not significant)and 13-24 h from onset (0% [14] reduction; not significant)are wide. The results from EMERAS are, however,consistent with the possibility of modest mortalityreductions among patients treated within 6-12 h, and theycontribute to the totality of the evidence on the questionwhether fibrinolytic therapy produces any worthwhileimprovement in survival among patients presentingafter 6 h.
The most important acknowledgment is to the thousands of patients whotook part in EMERAS, and to the hundreds of doctors and nurses whocollaborated with the national coordinators.
The study was conducted under the auspices of Federacion Argentina deCardiologia, Sociedad Brasileira de Cardiologia, Sociedad Chilena deCardiologia y Cirugia Cardiovascular y Sociedad Uruguaya deCardiologia. Sterling Drugs donated aspirin, but otherwise the entirestudy was financed by Behringwerke (Dr J Muller, Dr A Jessel, Dr UDelvos), a subsidiary of Hoechst, the manufacturers of the SK brand used(Streptase). The study was, however, designed, conducted, analysed, andinterpreted independently of the companies by the EMERASCoordinating Centre in Rosario, Argentina, in collaboration with theClinical Trial Service Unit (CTSU) in Oxford.
The following centres and investigators collaborated in EMERAS:
Data-monitoring committee: Doll R (Chairman) UK; Bertolasi C,Argentina; Robiolo 0, Argentina; Yusuf S (NHLBI Bethesda, USA,currently at McMaster University, Hamilton, Canada); Peto R, CTSUOxford, UK; Collins R, CTSU Coordinator, UK.
Argentina (2881 patients): EMERAS Coordinating Centre, Rosario:Dapoto ML, Genisans MI, Rasetti MD; Regional Coordinators: SantopintoJJ (Bahia Blanca); Tajer C, Colombo Berra F (Buenos Aires); Schneider R(Buenos Aires Norte); Guzman L (Cordoba); Garcia J (Corrientes); Pollola
771
J, Montenegro DC (La Plata); Irusta GE (Mendoza); Castellanos R
(Tucuman); Masjoan M, Monge AA (Santa Fe); Cuneo C (Salta); Clavijo R(San Juan)-Avellaneda, Hosp R Finochietto: Baeff 0, Singer M; Azul,Sanat. Azul: Castro H, Capelli E; B Blanca, C Salud Dr L Lucero:Santopinto JJ, Gungolo A; Hosp Dr J Penna,: Gelardi G, Corinaldesi A;Hosp Italiano: Zavatti D, Cermesoni R; Hosp Naval Pto Belgrano: Luppi 0,Moggi AC; Hosp Priv del Sur: Arias 0, Fainstein D; B Aires, Cl Bazterrica:Rando C, Lopez Palma A; F H Pombo de Rodriguez: Fernandez Berges D,Palma JC; Hosp CG Durand: Glanc M, Beck E; Hosp Ag Pirovano:Balassanian JL, Mejail I; Hosp Cl J San Martin: Martinez Martinez JA,Mendiz OA; Hosp Espanol: Grancelli HO, Pomes Iparraguirre H; HospFrances : Nordaby R, Gallo MC; Hosp Santojanni: Ryba D, Struminger M;Hosp Argerich: Piombo A, Ulmete E; Hosp Israelita: Cercos H, Torres HG,Faerman G; Hosp Italiano: Gabay JM, Bazzino 0, Staszewisky L; HospRivadavia: Reussi R, Hirchson A; Pol Bancaria: Pomes Iparraguirre H,Garber VA; Sanat Agote: Pellegrini C, Lowenstein J; Sanat Anchorena:Mele E; Sanat Colegiales: Gimenez HJ; Sanat Gtiemes: Tronge JE, Bond M;Sanat Mitre: Sosa Liprandi A, Darit V; C de Gomez, Inst Med Dep Iriondo:Guillen RH, Tonero 0; Casilda, Sanat San Jose : Garcia Bonanno JA, VailloJA; Córdoba, Clin Priv Sucre: Brunetto JF, Sgammini HO; Hosp Cordoba:Diaz Gavier N, Tolosa M; Hosp Italiano & Hosp Munic Urgencias: AlasinoRC, Ortiz L; Hosp Militar: Bastianelli RV, Mansilla A; Hosp Nac deClinicas: Vergottini JC, Barrionuevo C; Sanat Allende: Guzman L; CnelSuarez, Hosp Munic Cnel Suarez: Caccavo A, Garralda EA; Corrientes,Hosp JF de San Martin: Sosa CH, Perna ER;yt<K:’M, Sanat Junin: EtchepareJG, Etchepare HO; La Plata, Hosp Espanol: Torrijos R, Braziunas H; HospItaliano: Perrino 0, Cartasegna L; Hosp Rossi: Abalde J; Hosp SR deGonnet: Rodriguez Anaya L; Hosp S Martin: Ruiz NH; Inst del Torax SJ deDios: Corsiglia DC, Alessio E; Int Med Platense: Montenegro DC, BarbieriB; Sanat Argentino: Navajas C, Zocco J; Lujan, Cl Guemes: Barrios AR,Alvarez RH; Mar del Plata, HIGA: Garcia MA, Teves JA; Hosp Priv deComunidad: Righetti G, Lembo L; Mendoza, Hosp LC Lagomaggiore:Ortego RE, Torres JD; Sanat Soc Esp S Mutuos: Irusta GE, Hidalgo JA;Hosp Central: Tuma HV, Caruso EO; Moreno, Hosp Munic : Koretzky MH,Perez JC; Pergamino, CL Centro: Funes GJ, Marco PA; Cl Pergamino:Schneider R, Badia HD; Hosp Zonal S Jose : Meola JD, Raimondo MS;Resistencza, C Cardiol Nordeste: Cravzov RM, Tercelan R; Hosp Dr JCPerrando: Ferro Queirel E, Olivello C; Sanat Frangioli: Ventura A, Perret R;Rosario, HE Clemente Alvarez: Locatelli HA, Piskorz DL; Hosp Espanol:Garguichevich JJ, Lambri DA; Hosp Prov del Centenario: Diez AR, DiazGA; Hosp Provincial: Puccini V, Cespedes A; Sanat Britanico: RobioloDurand AJ, Tassano JM; Sanat Delta: Lopez J, Rodriguez R; Sanat Palace:Villa L; Sanat Parque: Rossi OA, Del Rio A; Sanat Plaza: Villares J, GentileA; Sanat Rawson: Beloscar J, Ferraro 0; Salta, Cl Metan: Otero OA, SoldiniG; Hosp S Bernardo: Cuneo C, Tapia LJ; Inst Med de Salta: Falu E, CorreaSalazar C; Salto, AOS: Menendez CA; Cl Salto: Pondielli J, Perez CA; HospMun G Agudos: Perez CA, Roncallo N; San Juan, Hosp M Quiroga:D’Ovidio A, Peluc J; Hosp Priv C Med: Clavijo R, Roy 0; Sanat AmteBrown: Rebollo C, Correa R; San Lorenzo, Cl San Lorenzo: Pou 11, PrezAR; San Nicolas, Cl S Nicolás: Garcia Duran R, Pacheco E; Santa Fe, HospItaliano: Monge AA, Martina JA; Hosp P JM Cullen & Sanat Rivadavia:Ferndandez RA, Becker C; Sanat Mayo: Masino C, Minen OJ; Sgo delEstero, Inst de Cardiol: Manzur R, Sirena JJ; Sanat S Martin: Alvarez A,Pernigotti MA; Trelew, Sanat 28 de Julio: Hernandez IS, Eljatib A;Tucumin, Inst de Cardiol: Romero MO, Lobo RA; Sanat ADOS: LuciardiHL, Berman SG; Vdo. Tuerto, Pol Chapuis: Allegrini E, Gonzalez 0; VillaSarmiento, Hosp A Posadas: Balestrini AE, Norkus A.
Brazil (1271 patients): Coordinating Centre: Sao Paulo, Inst D Pazzanesede Cardiol: Cano S, Avezum Jr A; Aracatuba, Sta Casa: Kawamura T,Tuppy G; Bauru, Hosp de Base: Barros R, Germano A; Prontocor, BeloHorizonte: Darwich R, Silveira F; Brasilia, Hosp de Forcas Armadas:Almeida 0, Ferreira Jr P; Hosp de Base: Introcaso L, Freitas C; Hosp StaLucia: Amorim V, Filomeno A; Campinhas, Hosp Irmaos Penteado:Naccarato A, Costa T; Hosp Vera Cruz: Otero N, Venri V; Unicamp: Coelho0, Jorge P; Caxias do Sul, Hosp Fatima: Michielin F, Mascia J; Curitiba,Hosp do Coraeao: Oliveira P, Velho M; Hosp Evangelico: Rossi P, PereiraM; Sta Casa: Moura A, Melo R; Florianopolis, Inst de Cardiologia: Simao A,Heinisch R; Goiania, Hosp Geral: Las Casas A, Gusmao C; Hosp SaoSalvador: Rassi A, Rassi Jr A; Guarulhos, Hosp Stella Maris: Faelli Jr D,Mirillo R; Itapemirim, Sta Casa de Mis Cachoeiro: Coelho L, Rubin G;Londrina Hosp Evangelico: Silva S, Facanha L; Maceio, Agro Ind doAcucar e do Ale: Oliveira C, Santos R; Sta Casa: Dourado G, Martiniano M;Marilia, Sta Casa: Braga J, Labrunie A; Natal, Casa de Saude S Lucas:Bittencourt R, Nascimento C; Niteroi, Procordis: Borges Fo S,Chachamovitz J; Nova 19uaçu, Nossa Sra de Fatima: Mattos E, Duarte J;Nova Lima, Biocor: Azevedo Sobrinho A, Cesar H; Passo Fundo, Hosp SaoVicente de Paulo: Fragomeni L, Reali J; Pelotas, Sta Casa: Abrantes J,Schramm E; pzracicaba, Hosp do Fond de Can: Campos R, Oliveira A; PortoAlegre, Hosp das Clinicas: Zago A, Bersano E; Hosp Sao Lucas de Puc do Rs:Mossman R, Manenti E; Inst Cardiologia: Rodrigues R, Nonohay N; N Srade Conceicao: Pimentel Fo P, Barcellos G; Sta Casa: Leaes P, Blacher C;Recife, Hosp Oswaldo Cruz: Oliveira L, Cantarelli E; R Preto, Hosp doCoraeao: Papa M, Grandini Jr L; Medicina: Marin Neto J, Almeida Fo 0;Sta Casa: Muniz L, Mestria A; R de Janeiro, Hosp Cardiol de Laranjeiras:Figueira R, Almeida G; Hosp dos Serv do Estado: Carvalho M, Escosteguy
C; Hosp Munic Souza Aguiar: Oliveira C, Alladas R; Hosp Univ C Fraga:Saad E, Xavier S; IMC, S Jose de R Preto: Nicolau J, Lorga A; Salvador,Hosp Portugues: Esteves J, Cardoso Fo A; Hosp Sta Izabel: Nery A, FeitosaG; Hosp Univ de Sta Maria: Gressler J, Moraes L; Santo Andre, HospBrasil: Jorge S, Alegre E; Santos, Sancor: Silva L, Teixeira E; Sta Casa:Burgos F, Soares Neto M; Sao Caetano, Beneficencia Portuguesa: SombraF, Moraes S; Sao Carlos, Sta Casa: Verzola R, Santoro V; Sao Luiz,Prontocor: Buhaten J, Furtado R; Udi- cardio: Melo Fo J, Barbosa J; SaoPaulo, Hosp DS Gomes Pimenta: Frange P, Farran J; Hosp do Coracao daASS: Romano E, Barbosa M; Hosp do SP Estadual: Santos Fo M, MatheusM; Hosp do SP Municipal: Sales Fo E, Novaretti J; Hosp Panamericano:Catani R, Silva L; Hosp Sao Lucas: Iglesias M, Wafael N; Hosp Sao Paulo:Carvalho A, Martinez Fo E; Inst Dante Pazzanese de Cardiologia, SaoPaulo: Timerman A, Gun C; Leao XIII, Sao Paulo: Ramos R, Gomes A; StaCasa, Sao Paulo: Franken R, Golin V; C Hosp de Sorocaba: Maiello J,Almeida Jr B; Uberaba, Hosp Sao Domingos: Miziara L, Lopes M;Uberlandia, Hosp Sta Genoveva: Marcelino A, Santos C.
Chile (148 patients): Concepci6n, Hosp del Trabajador: Lacanneiler E;Santiago, Clin Santa Maria: Chamorro H, Mordoh I; Asist Publica Dr A delRio: Chavez E; Clin Davila: Yenes A; Clin Indisa: Bollet A; Hosp BarrosLuco Trudeau: Altuzarra R; Hosp Carabineros: Gatica A; Hosp ClinUniversitario: Carrillo E; Hosp de la Fuerza Aerea: Mathei R; Hosp delSalvador: Manzur F; Hosp Militar: Novoa 0; Hosp Paula Jaraquemada:Arribada A; Hosp San Juan de Dios: Gonzalez A; Temuco, Hosp Regional:Saavedra J; Valdivza, Hosp Regional: Arriagada A; Valparaiso, Hosp Carlosvan Buren: Bavestrello L.
Paraguay (7 patients): Asunci6n, Hosp Universitario: Apodaca J, AdornoArtaza M; Sanat M Battilana: Meilicke C: Sto Domingo, Hosp Central IPS:Acosta Romero G, Villamayor S.
United Kingdom: CTSU, University of Oxford: Parish S (statistician), DoveP, Appleby P, Jackson D, Halls H, Jayne K, Mead G, Spence S.
Uruguay (70 patients): Montevideo, Asoc Espanola: Lluberas R; Casa deGalicia: Besada E; Casmu: Hiriart C; Hosp Espanol: Senra H; Hosp Italiano:Marini F; Hosp Militar: Madera R; Impasa: Salvarrey A; Sanat Larghero:Zelarayan M; Rocha: Casanyes D.
Venezuela (157 patients): Barcelona, Hosp C de Barcelona: Barrios J,Arreza M; Barquisimeto, C de Cardiol Ascardio: Finizola B; Caracas, HospCI Universitario: Almeida D, Perez Davila V; Hosp Domingo Luciani:Beltran R, Parejo J: Hosp JG Hernandez: Cataldo S; Hosp M Perez Carreno:Sirit U, Garcia 1; Maracaibo, Hosp Universitario: Vergara G, Cook W;Valencia, Hosp Universitario: Petrola I.
References
1 ISIS-2 (Second International Study of Infarct Survival) CollaborativeGroup. Randomised trial of intravenous streptokinase, oral aspirin,both, or neither among 17 187 cases of suspected acute myocardialinfarction: ISIS-2. Lancet 1988; ii: 349-60.
2 Gruppo Italiano per lo Studio della Streptochinasi nell’infartomiocardico (GISSI). Effectiveness of intravenous thrombolytictreatment in acute myocardial infarction. Lancet 1986; i: 397-402.
3 Wilcox RG, von der Lippe G, Olsson CG, et al. Trial of tissueplasminogen activator for mortality reduction in acute myocardialinfarction: Anglo-Scandinavian Study of Early Thrombolysis(ASSET). Lancet 1988; ii: 525-30.
4 AIMS Trial Study Group. Effect of intravenous APSAC on mortalityafter acute myocardial infarction: preliminary report of a placebo-controlled clinical trial. Lancet 1988; i: 545-49.
5 Yusuf S, Collins R, Peto R, et al. Intravenous and introcoronaryfibrinolytic therapy in acute myocardial infarction: overview of resultson mortality, reinfarction and side-effects from 33 randomizedcontrolled trials. Eur Heart J 1985; 6: 556-85.
6 Comité Organizador EMERA. Estudio MulticéntricoEstreptoquinasa—República Argentina (EMERA). Rev Fed ArgCardiol 1987; 16: 238-40.
7 Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group.Indications for fibrinolytic therapy in suspected acute myocardialinfarction: collaborative overview of mortality and major morbidityresults from all randomised trials of more than 1000 patients. Lancet(in press).
8 Yusuf S, Collins R, Peto R. Why do we need some large, simple,randomized trials? Stat Med 1984; 3: 409-20.
9 Peto R, Pike MC, Armitage P, et al. Design and analysis of randomizedclinical trials requiring prolonged observation of each patient II:analysis and examples. Br J Cancer 1977; 35: 1-39.
772
10 Braunwald E. Myocarcial reperfusion, limitation of infarct size,reduction of left ventricular dysfunction and improved survival: shouldthe paradigm be expanded? Circulation 1989; 79: 441-44.
11 Laffel GL, Braunwald E. Thrombolytic therapy: a new strategy for thetreatment of acute myocardial infarction. N Engl J Med 1984; 311:710-17.
12 Schaper W. Natural defense mechanism during ischaemia. Eur Heart J1983; 4: (suppl D): 73-78.
13 Reimer KA, Lowe JE, Resmussen MM, Jennings RB. The wave frontphenomenon in ischemia cell death I: myocardial infarct size versusduration of coronary occlusion. Circulation 1977; 56: 786-94.
14 Banka VS, Chadda KD, Helfant RH. Limitations of myocardialrevascularization in restoration of regional contraction anomalies bycoronary occlusion. Am J Cardiol 1974; 34: 164-70.
15 Yusuf S, Lopez R, Madison A, Sleight P. Variability ofelectrocardiographic and enzyme evolution of myocardial infarction inman. Br Heart J 1981; 45: 271-80.
16 Muller DWM, Topol EJ. Selection of patients with acute myocardialinfarction for thrombolytic therapy. Ann Intern Med 1990; 113:949-60.
17 Schroeder R, Neuhaus K-L, Linderer T, Brüggermann T, Tebbe U,Wegsheider K. Impact of late coronary artery reperfusion onleft ventricular function one month after acute myocardialinfarction: Results from ISAM Study. Am J Cardiol 1989; 64:879-84.
18 Hochman JS, Choo H. Limitation of myocardial infarct expansion by
reperfusion independent of myocardial salvage. Circulation 1987; 75:299-306.
19 Bonaduce D, Petretta M, Villari B, et al. Effects of late administrationof tissue-type plasminogen activator on left ventricular remodellingand function after myocardial infarction. Am J Coll Cardiol 1990; 16:1561-68.
20 Hale SL, Kloner RA. Left ventricular topographic alterations in thecompletely healed rat infarct caused by early and late coronary arteryreperfusion. Am Heart J 1988; 116: 1508-13.
21 Sager PT, Perlmutter RA, Rosenfeld LE, McPherson CA,Wackers FJ, Batsford WP. Electrophysiologic effects of thrombolytictherapy in patients with a transmural anterior myocardial infarctioncomplicated by left ventricular aneurysm formation. J Am Coll Cardiol1988; 12: 19-24.
22 Gang E, Hong M, Wang F, Velazquez I, Nalos P, Myers M, Lew AS.Does reperfusion influence the incidence of ventricular late potentialsin acute myocardial infarction? Circulation 1987; 76 (suppl IV): 342(abstr).
23 Eigler N, Maurer G, Shah PK. Effect of early systemic thrombolytictherapy on left ventricular thrombus formation in acute anteriormyocardial infarction. Am J Cardiol 1984; 54: 261-63.
24 ISIS-3 (Third International Study of Infarct Survival) CollaborativeGroup. ISIS-3: a randomised trial of streptokinase vs tissueplasminogen activator vs anistreplase and of aspirin plus heparin vsaspirin alone among 41 299 cases of suspected acute myocardialinfarction. Lancet 1992; 339: 753-70.
Comparative efficacy of rice-based and glucose-based oralrehydration salts plus early reintroduction of food
SummaryThe use of oral rehydration salts (ORS) to restore fluid balancein children with diarrhoea is universally accepted. However,there is uncertainty about whether glucose-based ORS or ORSbased on precooked rice powder is more effective. In a
randomised trial we compared the two types of ORS in childrenwho were given food immediately after completion of
rehydration.460 boys aged 3-18 months, admitted to hospital with
acute diarrhoea and signs of dehydration, were randomlyassigned to groups receiving rice-based and glucose-basedORS solution (230 to each group). After full rehydration(4-12 h), a weaning food consisting of rice and mixed
vegetables was given until the diarrhoea stopped. Continuinglosses of liquid stool and vomitus were replaced with theassigned ORS solution. There were no differences between the
groups during the rehydration phase in stool volume, volume ofORS solution taken, duration of rehydration phase, or weightgain. However, after initiation of feeding, the glucose-basedORS group had significantly lower stool volumes than therice-based ORS group (142 [95% Cl 117-173] vs 96
[77-120] g/kg); they also took a smaller amount of ORSsolution (153 [127-185] vs 111 [90-136] mL/kg) and hada shorter duration of diarrhoea (55 [SD 35] vs 44 [35] h).Glucose-based ORS solution was more effective than
rice-based ORS solution for the treatment of diarrhoea in
children when feeding with a rice-based diet was started soonafter correction of dehydration. These results support thecontinued recommendation of glucose-based ORS solution asstandard therapy for treatment of children with acute
diarrhoea and emphasise the importance of resuming feedingas soon as dehydration has been corrected.
Lancet 1993; 342: 772-75
Introduction
Acute diarrhoea is a principal cause of morbidity andmortality among children in developing countries. For thepast 20 years, the World Health Organization andUNICEF have recommended that children with
dehydration due to diarrhoea be treated with an oral glucoseelectrolyte solution, provided that they are able to drink anddo not have signs of severe dehydration.1,2 The prompt andcorrect use of this solution, combined with continued
Hospital Abu El Reeche, Gastroenterology Department, CairoUniversity, Calro, Egypt (Prof I M Fayad MD, M Hashem MD,M Refat MD, M Bakir MD); World Health Organization, DiarrhoealDisease Control Programme, Geneva, Switzerland (O Fontaine MD);and Department of International Health, Johns Hopkins University,School of Hygiene and Public Health, Baltimore, Maryland, USA(C Duggan MD, Prof M Santosham MD)
Correspondence to: Prof M Santosham, Johns Hopkins University,School of Hygiene and Public Health, Department of InternationalHealth, 615 North Wolfe Street, Baltimore, Maryland 21205, USA











![Role of ticagrelor in the treatment of coronary artery disease · Prasugrel–Thrombolysis in Myocardial Infarction 38 (TRITON–TIMI 38) study [10]. However, the higher level of](https://img.pdfslide.us/doc/110x75/5f8e3e6f18496b37da0ba95a/role-of-ticagrelor-in-the-treatment-of-coronary-artery-disease-prasugrelathrombolysis.jpg)