Embed Size (px)
Citation preview

Randomised clinical trials are the gold stan-dard for testing the efficacy of therapeuticinterventions in Phase III studies.
Consequently, clinical trial guidelines stress thatthe method of randomisation used should bedescribed in detail and, in cases where randomisa-tion is impossible, this omission must be justified.1
But despite the crucial role of randomisation, manyinvolved in designing clinical trials seem to beunaware of the wealth of randomisation algorithmsavailable and their respective advantages and dis-advantages for a particular study. In this article, wewill consider the case of a two-armed study com-paring an experimental with a standard interven-tion. We will address the following questions:What are the reasons for and against randomisa-tion? Which types of randomisation algorithmsexist? How can randomisation be employed inpractice?
Randomisation is one of the most importantdesign techniques available for reducing bias.2
Although increasing the sample size can reduce ran-dom errors, systematic differences between groupscan still occur. There several reasons for this as thefollowing examples show:• Historical controls and time trends. A novel
intervention is offered to newly diagnosedpatients. Their outcome is compared with thatof patients who had previously been treatedwith a standard therapy. However, these twogroups of patients might differ systematicallybecause, for example, diagnostic techniqueshave changed over time.
• Selection bias by predictability. The decisionto offer trial participation to an individualpatient might, intentionally or not, be influ-enced by knowledge of whether he or she willreceive the experimental or the standard inter-
vention. For example, one might be tempted toconsider less severely affected patients for theexperimental treatment.
• Accidental bias by unknown prognostic factors. Using a deterministic allocationscheme, it is possible to balance the groupswith regard to important known prognostic fac-tors like age and gender. However, factors thatare not explicitly considered might differbetween groups. For example, assigningpatients in a trial on hay fever to the experi-mental treatment every other week may lead topronounced treatment differences due tochanges in the weather.Randomisation is also important because it forms
the basis for inferential statistical testing. Statisticaltheory relies on the idea of random sampling, andalthough this is never fully achieved in a clinical trial,randomisation helps to fulfil this premise.
Another technical advantage of randomisationis that it helps to perform double-blind studies. Ifthe allocation scheme is known, the accidental orpurposeful unblinding of a single patient
Randomisation
27GCPj © 2004 PJB Publications Ltd October 2004 www.GCPj.com
Don’t leave randomisation to chanceRandomised controlled clinical trials are the gold standard for clinicalresearch, but the process is not as simple as it might first appear.Dr Inke R König, Friedrich Pahlke and Professor Andreas Zieglersum up the rationale behind randomisation and the algorithmsresearchers can employ to optimise the design of their Phase III studies
Despite the crucial roleof randomisation,many clinical trialdesigners seemunaware of the wealthof algorithms availableto help them randomise subjects

might lead to an unblinding of all.Finally, anecdotal reports, as well as system-
atic studies, suggest that the estimation of thera-peutic effect from non-randomised studies issubject to bias. For example, Sacks et al comparedthe outcome of 56 studies using historical controlswith the outcome of 50 studies using randomisedcontrols to investigate the same intervention.3
They found that the therapeutic effect using histor-ical controls was larger than when randomisedcontrols were used. Other authors showed that inother instances, the therapeutic effect might beunderestimated.4
On the other hand, some interesting argumentsagainst the use of randomisation have beenvoiced.5, 6 Firstly, it has been argued that the num-ber of newly introduced therapies and therapyvariants is too large to allow testing in controlledrandomised trials. Secondly, for some interven-tions the setting of a randomised trial does notmatch the way the therapy is used in practice. For
instance, if a over-the-counter medicine istested in a research hospital under expertsupervision, the generalisability, and thusthe external validity, of the study might bequestioned.
Thirdly, there are dramatic effects likethe effect of penicillin against infections thatclearly do not require testing in a randomisedtrial. Finally, as an ethical reason, whenevera clinical study is performed, collectiveequipoise has to be assumed, that is, it mustbe generally accepted that the superiority ofone of the compared interventions is notknown. However, if the individual treatingclinician does not accept this because he is
convinced of the superiority of one or the other, itwould not be ethical for him to participate andinclude patients in the trial.
Algorithms for randomisationOnce it has been decided that a proposed study willbe randomised, the most appropriate algorithmmust be selected. Researchers have several optionsto choose from.
There are two components to randomisation.7
Firstly, each patient has a known and, in most situ-ations the same, probability of being allocated to aspecific treatment arm. For most trials, the eligiblepatient has a probability of 50% of receiving theexperimental therapy. Secondly, the treatment allo-cation is not predictable. These conditions are bestmet by using simple randomisation that is akin tousing the toss of a coin.8 The advantage of this pro-cedure is the perfect unpredictability of the out-come; thus it is ideally suited for open studies.
However, the disadvantage is that it might lead
Randomisation
28 GCPj © 2003 PJB Publications Ltd October 2003www.GCPj.com
Features of the Randomisation In Treatment Arms tool
Minimisation is selected as the randomisation procedure from a range of algorithms. For initialisation, a real random seed can be loadedfrom the Internet, or a pseudo random seed isgenerated. At the same time, the right-handwindow displays the current settings
For specific study, users can choose from a selection of randomisation algorithms, including:• Simple randomisation• Biased-coin design• Urn model• Permuted-block randomisation• Permuted-block randomisation within strata• Minimisation (see left)• Self-adjusting design
The tool allows for:• Inclusion of any number of groups, prognostic
factors and strata within factors, addition of further strata later in the study
• Randomisation of single probands or batches ofprobands with immediate display of group balance
• Saving current state of study, work with severalstudies in parallel
• Detailed output and exact reproducibility ofresults
• Off-line randomisation of next patients, if required
• Simple handling and availability of detailed help
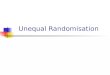
Are both treatmentarms of equal size?
Use simplerandomisation
Use higher probabilityto allocate patient to
smaller groupNO
YES
Figure 1: Procedure of biased coin design.10

to an imbalance in group sizes, which is amajor drawback for small studies. As the sam-ple sizes can be approximated using specificstatistical distributions, in this case the bino-mial distribution, it is possible to calculate theprobability of achieving an imbalance of aspecific size or greater. it is possible to calcu-late the probability of achieving an imbalanceof a specific size or greater. For example, witha total sample size of 50 patients, the proba-bility of an imbalance of 18–32 or more is5%. With sample sizes of 200 or morepatients, the expected imbalance is verysmall. If smaller sample sizes are included, arestricted randomisation might therefore befavoured over simple randomisation.
Restricted randomisationThe characteristic feature of these algorithms isthat the randomness of the allocation isrestricted in order to balance the group sizes.Examples include the popular permuted-blockdesign and the biased-coin design.9 The latter hasbeen recommended for use (see Figure 1).10 Thebiased-coin design works as follows. Whenever anew patient is included in the trial, the current sizesof both treatment groups are compared. If they areequal, the patient is allocated by simple randomisa-tion. If not, the patient is assigned to the smallergroup with a given probability. The value of thisprobability must be greater than 50% and specified inadvance, and it determines the characteristics of thedesign: the closer the probability approaches 100%,the higher is the predictability of treatment alloca-tion, but the better is the balance of the group sizes.
One criticism of the biased coin design is thatthis probability value is fixed throughout the study,so other designs have been suggested that allowvariations depending on the current group balance.These are referred to as adaptive biased coindesigns.11
In many clinical trials it is important explicitlyto balance the treatment groups in terms of theirprognosis.2 Most importantly, in a multicentre trialit would not be enough to achieve equal treatmentgroups overall. Instead, one has to make sure that abalance is achieved in every participating studycentre. In principle this can be achieved by using arestricted randomisation procedure separatelywithin each centre. However, the sample size hereis smaller, thus forcing the problematic trade-offbetween predictability and balance. Also, whenseveral prognostic factors need to be considered,this procedure becomes impractical.
Covariate-adaptive randomisationWhen several prognostic factors have to be takeninto account, alternative randomisation procedurescan be used that randomise overall while at thesame time explicitly including prognostic factors.Important examples of these algorithms are the self-
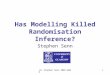
adjusting12 and the minimisation13, 14 designs (seeFigure 2). When a new patient is enrolled, the con-sequences of allocating him or her to either groupare considered for his or her specific combination ofprognostic factors. For each factor, the lack ofgroup balance is calculated if the patient was ran-domised to the experimental or the standard group.From this, the lack of balance is summarised overall factors. If this sum is equal for both groups, thepatient is allocated by simple randomisation.Otherwise, he is attributed to the group with thegreater lack of balance either automatically14 or witha specified higher probability.13
Compared with simple randomisation proce-dures, covariate-adaptive randomisation certainlyleads to a higher predictability, which might beproblematic in open trials. As with the biased-coindesign, the predictability of minimisation dependson the allocation probability. Compared withrestricted randomisation algorithms, covariate-adaptive randomisation is rather complex, but avery good group balance can be achieved, espe-cially in trials where many prognostic factors needto be considered.
Choosing an algorithmThe use of more complex randomisation algo-rithms like covariate-adaptive procedures is facili-tated by appropriate software. For example, werecently developed Randomisation In TreatmentArms (RITA) as a software tool for randomised tri-als (see www.statsol.de), which is described in thebox opposite.
The randomisation algorithms we havedescribed above differ with regard to the follow-ing important features:• The less predictable the group assignment is, the
lower is the probability for bias. Hence, thisattribute is most important in open trials. It is
Randomisation
29GCPj © 2003 PJB Publications Ltd October 2003 www.GCPj.com
Calculate overalllack of balance
Is lack of balanceequal in both
treatment arms?
Use simple randomisation
For current patient:Calculate lack of balance
within each prognostic factor
Use higher probabilityto allocate patient to
group with most shortfallNO
YES
Figure 2: Procedure of minimisation.13, 14

provided optimally using simple randomisation.• A lower predictability of the randomisation out-
come leads to a worse balance of the treatmentgroup sizes. Restricting the predictability inorder to achieve a better balance is more impor-tant in trials with small sample sizes.
• In some trials, it might be crucial to control forprognostic factors in the randomisation pro-cess. This can be achieved using covariate-adaptive procedures, paying the price of ahigher complexity.Consequently, the choice of randomisation
algorithm depends on whether blinding of patientsand treating physicians is included. In an open trial,the unpredictability should be paid most attention.Then the sample size overall, at every interim anal-ysis, and in any interesting subgroup, needs to beconsidered: with smaller sample sizes, the balanceof treatment groups becomes a crucial issue. Next,the number of prognostic factors determines theoptimal choice. Although it is rare for more thantwo or three factors to have to be accounted for,2 analgorithm that explicitly allows for the balancewithin these factors is to be preferred. Finally, thespecific logistics of the trial are important. If, forexample, patients are not entered sequentially inthe trial but en bloc, the unpredictability of alloca-tion is no longer an issue.
References1 ICH E3. ‘Structure and content of clinical study
reports’, The European Agency for the Evaluation of
Medicinal Products – Human Medicines Evaluation
Unit, 1995 (www.emea.eu.int/pdfs/human/ich/
013795en.pdf).
2 ICH E9. ‘Statistical principles for clinical trials,
CPMP/ICH/363/96’, The European Agency for the
Evaluation of Medicinal Products – Human
Medicines Evaluation Unit, 1998 (www.emea.eu.int/
pdfs/human/ewp/215899en.pdf).
3 H Sacks, TC Chalmers, H Smith Jr. ‘Randomised
versus historical controls for clinical trials’,
American Journal of Medicine, 72, pp233–40, 1982.
4 R Kunz, AD Oxman. ‘The unpredictability paradox:
review of empirical comparisons of randomised and
non-randomised clinical trials’, British Medical
Journal, 317, pp1185–90, 1998.
5 AR Feinstein. ‘Clinical Biostatistics XXIV. The role
of randomisation in sampling, testing, allocation and
credulous idolatry’, Clinical Pharmacology and
Therapeutics, 14, pp1035–1051, 1973.
6 N Black. ‘Why we need observational studies to
evaluate the effectiveness of healthcare’, British
Medical Journal, 312, pp1215–1218, 1996.
7 DG Altman, JM Bland. ‘Statistics notes: Treatment
allocation in controlled trials: why randomise?’,
British Medical Journal, 318, pp1209, 1999.
8 D Blackwell, J Hodges. ‘Design for the control of
selection bias’, Annals of Mathematical Statistics,
28, pp449–460, 1957.
9 B Efron. ‘Forcing a sequential experiment to be
balanced’, Biometrika, 58, pp403–417, 1978.
10 KF Schulz, DA Grimes. ‘Generation of allocation
sequences in randomised trials: chance, not choice’,
The Lancet, 359, pp515–519, 2002.
11 LJ Wei, JM Lachin. ‘Properties of the urn
randomisation in clinical trials’, Controlled Clinical
Trials, 9, pp345–64, 1988.
12 O Nordle, B Brantmark. ‘A self-adjusting
randomisation plan for allocation of patients into
two treatment groups’, Clinical Pharmacology and
Therapeutics, 22, pp825–830, 1977.
13 SJ Pocock, R Simon. ‘Sequential treatment
assignment with balancing for prognostic factors in
the controlled clinical trial’, Biometrics, 31,
pp103–115, 1975.
14 D Taves. ‘Minimisation: a new method of assigning
patients to treatment and control groups’, Clinical
Pharmacology and Therapeutics, 15, pp443–453,
1974.
Randomisation
30 GCPj © 2003 PJB Publications Ltd October 2003www.GCPj.com
Dr Inke R König, Friedrich Pahlke, ProfessorAndreas Ziegler
Institute of Medical Biometry and Statistics, UniversityHospital Schleswig-Holstein, Campus Lübeck, Germany
Tel: +49 (0)451 500 2789Fax: +49 (0)451 500 2999
E-mail: [email protected]