Embed Size (px)
Citation preview

ABSTRACT
Traumatic dental injuries are a frequent occurrence among children, with 25% of school aged children experiencing dental trauma. Proper diagnosis, treatment and follow up are crucial in such cases in order to monitor the many possible sequelae of the dental trauma. This case report discusses the dental management of a 16-year-old healthy female patient who initially was evaluated at Rainbow Babies and Children’s Hospital eight years earlier after suffering a traumatic dental injury. Management of the initial luxation injuries to the maxillary permanent central incisor is discussed. The sequelae of the trauma that developed following the initial injury, specifically the loss of the maxillary right central incisor eight years following the injury is reviewed. This report will present the treatment rendered to our patient along with the considerations and evidence-based treatment options for managing such traumatic injuries.
DISCUSSION Managing traumatic dental injuries requires close follow up to address possible postoperative sequelae of trauma. As discussed in this case, the facial trauma suffered by this patient resulted in the eventual loss of both teeth 7 and 8. Healing following trauma is not predictable, thus requires close and careful follow up care and patient education. This case clearly demonstrates how the consequences of trauma may not be observed until several years after the initial injury. While the optimal age for decoronation is prior to the observance of infrapositioning, this patient was lost to follow up therefore treatment could not be initiated sooner. Following traumatic injuries, there is a severe risk of infrapositioning during the pubertal growth spurt. This patient is currently 16 years old and had already exhibited infrapositioning of #8, however decoronation was elected to preserve alveolar bone for future implant placement.
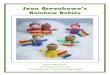
Management of buccal luxation of permanent maxillary incisors: a case report. Natisha Burner DDS, Margaret Ferretti DMD
Rainbow Babies and Children’s Hospital Department of Pediatric Dentistry Case Western Reserve University Department of Pediatric Dentistry
REFERENCES
Bourguignon C, Cohenca N, Lauridsen E, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol 2020;36:314-330. https://doi.org/10.1111/ edt.12578.
Malmgren, Barbro. “Ridge Preservation/Decoronation.” Journal of Endodontics, vol. 39, no. 3, 2013, pp. S67–72. Crossref, doi:10.1016/j.joen.2012.11.056.
8.17.2012 Initial Presentation
9.24.2012 Two month post-trauma
4.25.2013 Nine months post-trauma
1.31.2014 Eighteen months post-trauma
2.2.2016 Four years post-trauma 2.25.21
Decoronation 10.30.2020
Eight years post-trauma
CASE REPORT
This presentation discusses the management of a lateral luxation injury and the post-operative sequelae of trauma that developed. In August 2012, an eight-year-old female with no significant medical history presented to Rainbow Babies and Children’s Hospital Tapper Dental Clinic following facial trauma. The patient’s injury occurred on July 22, 2012. She was first evaluated at another emergency department for the injury which was diagnosed as avulsion of the maxillary right lateral incisor (#7) and lateral luxation of the maxillary right central incisor (#8). The patient was treated by a private pediatric dentist one week later who repositioned and splinted her maxillary anterior teeth and referred the patient to Tapper Dental for evaluation.
On August 17, 2012, approximately one month following the injury, the patient was evaluated by us. During this visit, the splint was replaced. She was treated on August 29, 2012 with apexification of teeth 7 and 8.
The patient was subsequently seen for apexification treatment on January 28, 2013 and August 23, 2013.
During January 2014, approximately 18 months following the initial injury, the patient began to exhibit spontaneous pain associated with tooth #7. Severe bone loss was evident radiographically and tooth #7 was determined to be non-restorable. Tooth #7 was subsequently extracted and an immediate interim partial denture was delivered to replace the missing maxillary right lateral incisor. The patient was dissatisfied with the removable nature of the appliance so the family sought care from an orthodontist to close the space of missing #7. The patient’s orthodontist moved the maxillary right canine mesially into the position of tooth #7 and contoured the canine to resemble a lateral incisor.
The patient was lost to follow up for a four-year time period and next evaluated at our clinic in October 2020.
The patient, now 16 years old, returned to our clinic to have tooth #8 evaluated with the chief complaint of
an asymptomatic “bleeding front tooth”. A periapical radiograph of #8 revealed significant internal root resorption. Clinically, the crown of #8 was facially inclined, exhibited class II mobility, and was infra-positioned compared to #9. The clinical presentation suggested ankylosis of tooth #8 as a result of trauma. Based on the clinical and radiographic findings, tooth #8 was determined to be non-restorable. Treatment options were discussed with the patient and parent including extraction of the maxillary right central incisor or decoronation. The family expressed that their ultimate treatment goal is an implant, thus elected decoronation to preserve bone for future implant placement. Following decoronation, an essix retainer replacing tooth #8 was delivered to the patient. After a six-week healing period, a Maryland bridge will be fabricated for the patient as an interim restoration until the patient can receive an implant.