Embed Size (px)
Citation preview

RADIATION ONCOLOGY—ORIGINAL ARTICLE jmiro_2334 109..115
Radiotherapy in the management of high-grade gliomasdiagnosed in Western Australia: A patterns of care studyMelanie Jackson,1 Sean Bydder,1,4 Eric Maujean,3,6 Mandy Taylor1 and Anna Nowak2,5
1Departments of Radiation Oncology and 2Medical Oncology, and 3Western Australian Cancer and Palliative Care Network, Sir Charles Gairdner
Hospital, and 4School of Surgery, and 5School of Medicine and Pharmacology, University of Western Australia, Nedlands, and 6WA Clinical Oncology
Group, West Perth, Western Australia, Australia
M Jackson MBBS; S Bydder FRANZCR, MBA;
E Maujean BSc, MPH; M Taylor MBBS,
FRANZCR; A Nowak MBBS FRACP.
CorrespondenceDr Melanie Jackson, Department of Radiation
Oncology, Sir Charles Gairdner Hospital,
Hospital Avenue, Nedlands 6009, Western
Australia, Australia.
Email: [email protected]
Conflicts of interest: None.
Submitted 1 March 2011; accepted 19 June
2011.
doi:10.1111/j.1754-9485.2011.02334.x
Abstract
Purpose: Radiotherapy (RT) plays an integral role in the management ofhigh-grade glioma (HGG). However, there is little information on the patternsof care in unselected Australian patients with HGG.Patient and Methods: This prospective cohort study collected information onpatients with a diagnosis of HGG managed in Western Australia over a25-month period from 2006 to 2008. RT treatment and survival data wereanalysed.Results: 86% of Western Australian patients with HGG were treated at thestudy site over this period. Of these, 80% were reviewed by a radiationoncologist with RT recommended in 88% of cases. One hundred eighty-sevenpatients proceeded to have RT, with most receiving 60 Gy in 30 fractions withlimited field external beam radiotherapy (LFRT). Median survival from diag-nosis was 13.6 months for all patients and 15.4 months for those planned fortreatment with 60 Gy in 30 fractions. The median time from surgery to thestart of RT was 41 days. Longer waiting times were not predictors of poorsurvival. Failure to receive all planned treatment (13% of patients) predictedfor poor survival (hazard ratio 0.38).Conclusion: Dose and fractionation practices show concordance with publisheddata and guidelines. Survival is also consistent with clinical trial data forpatients planned for aggressive therapy. Nevertheless, a substantial numberof patients are not suited to aggressive therapy or fail to complete plannedtherapy, and these patients have poor outcomes. Treatment delays did notaffect survival outcomes but are confounded by earlier treatment of thoseunsuited to LFRT.
Key words: brain tumour; glioblastoma; glioma; multidisciplinary care;radiotherapy.
Introduction
High-grade gliomas (HGG) are the most commonprimary malignant brain tumour in adults and generallyhave a poor prognosis. Until recently, standard treat-ment consisted of maximal safe surgical debulkingfollowed by radiotherapy (RT). Post-operative RTextends survival, with a 1-year mortality risk ratio of0.81 compared to no RT.1 There was a significant change
to the standard of care in 2005, after Stupp et al. dem-onstrated a survival benefit with the addition of concur-rent and adjuvant temozolomide to limited field 60 GyRT in patients with World Health Organization (WHO)grade IV disease.2 Hence, a multimodality approach totreatment is now commonly recommended.
Despite the central role of radiation oncology in themanagement of HGG, there are little data aboutcurrent practice, survival and resource utilisation in the
Journal of Medical Imaging and Radiation Oncology 56 (2012) 109–115
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 109

Australian tertiary context. Ideally, such data would beuseful to assess the extent to which evidence-basedmanagement is practised, identify system deficienciesand generate questions for further research. Forexample, one concern is the possible negative effectsof delay in initiating post-operative RT. Resourcingissues in many countries have been reported toresult in longer than ideal delays between surgery andstart of RT.3–5 Glioblastoma cell lines have shortdoubling times in vitro,6 but there is conflicting evi-dence on whether this translates to adverse clinicaloutcomes.7–10
In this study, data were collected on the patterns ofcare for patients treated in a single tertiary institution.This institution is the major elective neurosurgical siteserving a population of over 2 million and the referralcentre for most patients with HGG in Western Australia.Here, we report on the RT management details from thiscohort. The aim of this study was to examine the utili-sation of RT in patients with HGG, how well-plannedtreatment was delivered, the timeliness of commencingtreatment and the effect this has on patient survival.Data on surgical management and chemotherapy arereported separately.11
Patient and methods
Study design
This was a prospective cohort study performed at a singletertiary centre – Sir Charles Gairdner Hospital (SCGH),Perth, Western Australia. SCGH encompasses the statecentre for neuro-oncologic surgery and the state’s onlycomprehensive cancer centre. Multidisciplinary meetings(MDM) are conducted weekly where the diagnosticimaging, pathology and initial surgical management arediscussed and ongoing management formulated.
Prior to collation of data, ethics approval for this studywas obtained from the Institutional Human ResearchEthics Committee and Western Australian Confidentialityof Health Information Committee. Approval was alsogiven to waive individual written consent for inclusion inthe database.
Following pertinent literature review and consensusdiscussion with a multidisciplinary team of experts, data-base fields were developed for implementation inMicrosoft Access 2003. Fields included patient demo-graphics, time from surgery to outpatient review, date ofoutpatient review in radiation oncology department,initial management recommendation, RT details andreasons for not completing treatment. Data wereobtained from data sheets completed by clinicians. Theresults of automated electronic retrieval of histopathol-ogy, allied health and radiology information fromrespective management databases were also collated.Patient case notes were examined if there was missinginformation.
Patient identification and eligibility criteria
All adult patients in Western Australia with a diagnosis ofWHO grade III or IV supratentorial glioma were includedin the cohort. This included patients with biopsy-provendiagnosis of either new or recurrent HGG and also thosewith a new diagnosis on imaging alone where obtaininga pathological diagnosis was deemed inappropriate.Lower-grade tumours confirmed histologically to haveprogressed to grade III or IV were also included. Fullclinical information was obtained only from those whoreceived surgery, RT or chemotherapy at the study site.The accrual period was over 25 months from 1 June2006 to 30 June 2008. Patients were identified through:(i) a database of neurosurgical procedures conducted atthe study site; (ii) automated identification of all surgicalspecimens with relevant histopathology codes; (iii)recording of cases presented at a weekly multidisci-plinary neuro-oncology meeting; (iv) identification ofpatients from medical and radiation oncology consulta-tions; and (v) identification of patients with relevantcodes from the Western Australian Cancer Registry(WACR). There were no exclusion criteria on the basis ofage, treatment received, performance status or site oforiginal tumour.
Radiotherapy data collection and treatment
Management recommendations generated at an initialappointment with a radiation oncologist were assessed.RT treatment received was defined as limited field exter-nal beam radiotherapy (LFRT), whole-brain externalbeam radiotherapy (WBRT) or stereotactic radiosurgery(SRS). Treatment selection was determined by routineclinical practice, physician discretion, patient’s perfor-mance status and discussion in the MDM. All patientswere treated using megavoltage linear accelerators.LFRT were CT planned using MRI fusion unless thisimaging modality was contraindicated. Patients receivingWBRT were planned using two-dimensional simulation orCT. The Brown–Roberts–Wells frame was used for SRS,and treatments were planned with CT and MRI fusion.Intensity-modulated radiotherapy was not used in anypatients.
The analysis of the effect of RT delay was limited tothose with grade IV disease. They were divided intoquartiles according to RT delay; starting less than34 days after surgery, 34 to 42 days after surgery, 42to 51 days after surgery or more than 51 days aftersurgery. Only grade IV disease was examined here toexclude the confounding effect of less aggressive histol-ogy on perceived RT urgency.
Statistical methods
Survival was measured from time of diagnosis to death.If no surgical procedure was undertaken, time of
M Jackson et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists110

diagnosis was defined from either the procedure yieldingpathological diagnosis or the imaging used for diagnosis.Statistical analysis was conducted using SPSS forWindows package version 16.0 (SPSS Inc., Chicago, IL,USA). Other differences between groups were analysedusing an independent samples t-test or Mann–WhitneyU-test depending on the distribution of the data. Survivaldata were analysed using the Kaplan–Meier method andCox regression analysis. Results were considered signifi-cant if P � 0.05.
Results
From June 2006 to June 2008, 328 patients with adiagnosis of HGG were identified and included in the finaldataset. Of those, 283 (86%) received some portion oftheir treatment at the study site. The rest were managedwholly elsewhere. Baseline demographics are listed onTable 1.
Radiation therapy
Of the 283 patients with HGG seen in our institution, 227(80%) patients were reviewed by an institutional radia-tion oncologist. Of those, 93% had their initial consulta-tion following their primary surgical procedure and 3%following surgery for recurrence. The remainder repre-sented referral for radiosurgery (as this was not per-formed in other RT centres in Western Australia). Intotal, 199 of 227 patients seen (88%) were recom-mended active management including RT. At least 16 ofthe 56 patients not seen by an institutional radiationoncologist were identified as having initial RT outside ofthe study institution.
At the initial RT consultation, combined chemoradia-tion (CRT) was the most common treatment recommen-
dation made (Table 2). This usually pre-datedconsultation with the medical oncology team who wereultimately responsible for the final chemotherapy recom-mendation. One hundred eighty-seven of the 199patients recommended to have RT proceeded to havetreatment in the department.
Initial RT treatment received at SCGH is shown inTable 3. The majority received LFRT, including 94% ofpatients with WHO grade III and 82% with grade IVdisease. The small proportion of patients who hadreceived initial treatment elsewhere accounts for thosepatients having SRS as their initial treatment in ourinstitution. SRS was recommended either as a boostcomponent following WBRT or LFRT or as re-irradiationfor attempted salvage.
The mean dose prescribed for patients having onlyLFRT was 54 Gy (median 60 Gy), with a mean of 51 Gyreceived (median 60 Gy). For WBRT, a mean of 26.7 Gy(median 24.5 Gy) was prescribed and 26.3 Gy (median24.5 Gy) was received. For SRS, a mean of 15.7 Gy(median 15 Gy) was prescribed. The majority of patientshaving LFRT were prescribed 60 Gy in 30 fractions(n = 112, 71%).
Re-irradiation
Eighteen patients received a second course of RT. Eight(44%) of these patients had initially received 60 Gy in 30fractions, three (17%) had received 45 Gy in 15 frac-tions, four (22%) had shorter courses and two (11%)had not completed their initial prescribed course. The
Table 1. Baseline characteristics of patients in final dataset with HGG
Measure SCGH WACR Total %
Sex
Female 115 21 192 59
Male 168 24 136 41
Total 283 45 328
Mean age at diagnosis (range) 57 (42–72) 70 (52–88) 60
Domicile
Metropolitan 207 34 241 74
Rural 75 10 85 26
Socioeconomic quintiles
1 (lowest) 0 0 0 0
2 14 0 14 4
3 153 25 178 55
4 78 9 87 27
5 (highest) 37 10 47 14
SCGH, Sir Charles Gairdner Hospital; WACR, Western Australian Cancer
Registry.
Table 2. Initial management recommendation by radiation oncologist
Management recommendation Frequency Percentage
Chemoradiotherapy 177 78.0
Chemotherapy alone† 3 1.3
Radiotherapy alone 22 9.7
Supportive care only 24 10.5
Data missing 1 0.4
Total 227 100.0
†Medical oncology was responsible for chemotherapy recommendation.
Table 3. Tumour grade and first course of radiation received in SCGH†
Tumour grade LFRT WBRT LFRT + WBRT SRS Total
WHO grade III 34 1 1 0 36
WHO grade IV 120 17 8 1 146
Diagnosed on imaging 3 1 1 0 5
Total 157 19 10 1 187
†As outlined in Results section. LFRT, limited field external beam radio-
therapy; SRS, stereotactic radiosurgery; WBRT, whole-brain external
beam radiation therapy.
Radiotherapy for HGG in Western Australia
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 111

majority (n = 15, 83%) had a diagnosis of WHO grade IVdisease. Eleven (61%) were re-irradiated using SRS withthe most common doses being 15 Gy and 20 Gy, whilefive (28%) received LFRT and two (11%) receivedWBRT. The mean time between first and second courseof RT was 564 days (range 120–1260 days). Fourpatients had a third episode of RT. For most, the docu-mented reasons for re-irradiation with a second courseof RT were for progression or recurrence. One patienthad re-treatment with SRS (18 Gy) following 60 Gy in 30fractions for persistent disease, and this was docu-mented as a boost.
Treatment delays and discontinuation
The median interval between surgery and radiation oncol-ogy consultation was 11 days (range 1–102 days). Thedelay from surgery to the initiation of RT was analysed inpatients with grade IV glioma. For these 136 patients, themedian time from surgery to the start of RT was 41 days.Thirty-three patients (24%) waited 50 days or more, and13 patients (10%) waited 60 days or more.
Of 187 patients receiving their first course of RT forHGG, 163 (87%) received all treatment as prescribed.Twelve per cent of patients prescribed LFRT did notcomplete RT (8% where 60 Gy was prescribed) com-pared with 19% of those prescribed WBRT The majorityof patients who did not complete treatment had gradeIV disease (21 of 24, 87%). Of those who did not com-plete treatment, reasons included disease progression(n = 12; 6%), patient refusal (n = 5; 3%), unrelatedmedical problems (n = 4; 2%), treatment toxicity (n = 1)and other (n = 2). Six out of the 24 patients (25%) didnot start their planned course of treatment. Other dis-continuations were evenly spread as a proportion ofplanned treatment. Non-receipt of planned treatment didnot correlate with increasing age (P = 0.6).
Survival
Of the patients who were seen in our institution, 30%were still alive at the end of the follow-up period. Mediansurvival for all patients treated with RT was 13.6 monthsfrom diagnosis. The median survival for patients withWHO grade III and IV tumours was 50 and 13 months,respectively. The survival for patients with grade IVdisease who received 60 Gy was 14.9 months. Forpatients who did not receive 60 Gy, the average survivalwas 9.0 months. Many of the patients with grade IIIdiseases were censored for survival as follow-up wasrelatively short. Hence, our data do not illustrate thebetter survival for this group of patients.
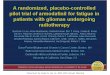
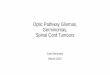
Older age (P < 0.0001), grade IV disease (P = 0.0002),failure to receive all treatment (hazard ratio 0.38,P < 0.0001) and treatment other than LFRT (P = 0.014)predicted for poorer survival on univariate analysis(Figs 1–4). On multivariate analysis, only age (P < 0.001)
and failure to receive all planned treatment (P = 0.001)remained independent prognostic factors. Patients withgrade IV disease who did not receive all planned treat-ment had a median survival of 5.6 months, as opposed to13.9 months for those completing treatment.
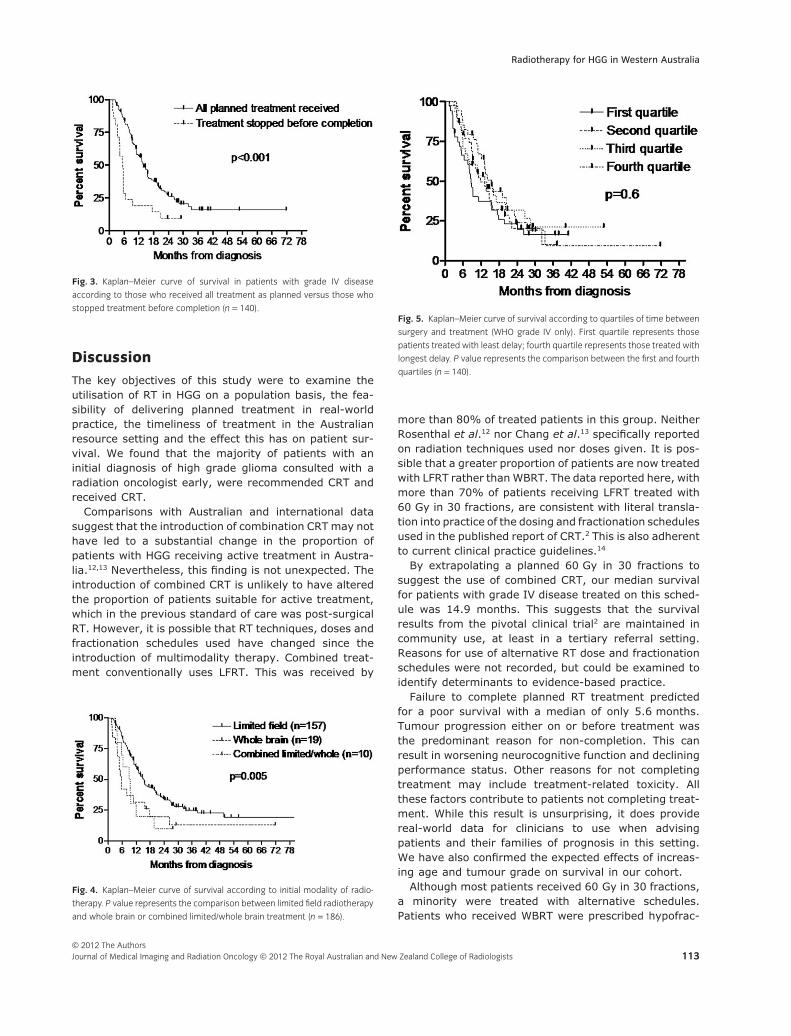
Patients with grade IV disease were divided into quar-tiles according to RT delay (Fig. 5). Median survivalswere 8.9, 11.7, 15.6 and 13.2 months, respectively,from shortest to longest delay (P = 0.6). There was asignificantly shorter wait time to receive WBRT (29 days)than LFRT (42 days, P = 0.04). However, excluding thepatients who received WBRT did not significantly alterthe survival within quartiles (9.4, 13.3, 13.9, and15.6 month from shortest to longest wait, P = 0.96).Patients having LFRT as their first treatment survivedlonger than those treated by WBRT or those who had acombination of LFRT and WBRT (15.4 months versus6.3 months, P = 0.005) (see Fig. 4).
Fig. 1. Kaplan–Meier curve of survival according to age for all patients
(n = 187).
Fig. 2. Kaplan–Meier curve of survival according to WHO tumour grade from
all patients with histopathology (n = 182).
M Jackson et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists112
Discussion
The key objectives of this study were to examine theutilisation of RT in HGG on a population basis, the fea-sibility of delivering planned treatment in real-worldpractice, the timeliness of treatment in the Australianresource setting and the effect this has on patient sur-vival. We found that the majority of patients with aninitial diagnosis of high grade glioma consulted with aradiation oncologist early, were recommended CRT andreceived CRT.
Comparisons with Australian and international datasuggest that the introduction of combination CRT may nothave led to a substantial change in the proportion ofpatients with HGG receiving active treatment in Austra-lia.12,13 Nevertheless, this finding is not unexpected. Theintroduction of combined CRT is unlikely to have alteredthe proportion of patients suitable for active treatment,which in the previous standard of care was post-surgicalRT. However, it is possible that RT techniques, doses andfractionation schedules used have changed since theintroduction of multimodality therapy. Combined treat-ment conventionally uses LFRT. This was received by
more than 80% of treated patients in this group. NeitherRosenthal et al.12 nor Chang et al.13 specifically reportedon radiation techniques used nor doses given. It is pos-sible that a greater proportion of patients are now treatedwith LFRT rather than WBRT. The data reported here, withmore than 70% of patients receiving LFRT treated with60 Gy in 30 fractions, are consistent with literal transla-tion into practice of the dosing and fractionation schedulesused in the published report of CRT.2 This is also adherentto current clinical practice guidelines.14
By extrapolating a planned 60 Gy in 30 fractions tosuggest the use of combined CRT, our median survivalfor patients with grade IV disease treated on this sched-ule was 14.9 months. This suggests that the survivalresults from the pivotal clinical trial2 are maintained incommunity use, at least in a tertiary referral setting.Reasons for use of alternative RT dose and fractionationschedules were not recorded, but could be examined toidentify determinants to evidence-based practice.
Failure to complete planned RT treatment predictedfor a poor survival with a median of only 5.6 months.Tumour progression either on or before treatment wasthe predominant reason for non-completion. This canresult in worsening neurocognitive function and decliningperformance status. Other reasons for not completingtreatment may include treatment-related toxicity. Allthese factors contribute to patients not completing treat-ment. While this result is unsurprising, it does providereal-world data for clinicians to use when advisingpatients and their families of prognosis in this setting.We have also confirmed the expected effects of increas-ing age and tumour grade on survival in our cohort.
Although most patients received 60 Gy in 30 fractions,a minority were treated with alternative schedules.Patients who received WBRT were prescribed hypofrac-
Fig. 3. Kaplan–Meier curve of survival in patients with grade IV disease
according to those who received all treatment as planned versus those who
stopped treatment before completion (n = 140).
Fig. 4. Kaplan–Meier curve of survival according to initial modality of radio-
therapy. P value represents the comparison between limited field radiotherapy
and whole brain or combined limited/whole brain treatment (n = 186).
Fig. 5. Kaplan–Meier curve of survival according to quartiles of time between
surgery and treatment (WHO grade IV only). First quartile represents those
patients treated with least delay; fourth quartile represents those treated with
longest delay. P value represents the comparison between the first and fourth
quartiles (n = 140).
Radiotherapy for HGG in Western Australia
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 113

tionated palliative doses. These patients had substan-tially worse survival than those treated with conventionalfractionation. This finding may be attributed to the manyfactors that lead to patient selection for shorter coursetreatment. Reasons for using this technique although notprospectively identified include the need to expeditetreatment due to clinical progression, patient inability totolerate prolonged courses, patient preference for ashorter treatment course for logistical and social reasonsor the palliative treatment of patients in whom chemo-therapy was not recommended. There have been severalsmall single-arm prospective studies where palliativecourses were used for patients with adverse prognosticfeatures such as older age and poorer performancestatus.15–17 As prospective collection of performancestatus data was incomplete in our dataset, we are unableto describe the role of performance status in the treat-ment recommendations made for our patient cohort.Nevertheless, these findings suggest that more aggres-sive therapy is being appropriately reserved for thosepatients who are most likely to benefit.
Reassuringly, we did not detect a deleterious effect ofdelay in commencement of post-operative RT. Patientsare seen in a very timely manner in the setting of anAustralian tertiary referral centre that runs a routineweekly MDM. In the median time of 11 days betweensurgery and radiation oncology review, patients recoverfrom their procedure, histological diagnosis is confirmedand most cases are discussed in MDM. This is in contrastto another Australian study in which the median timefrom biopsy to radiation consultation was 26 days.8 Theprompt implementation of RT is desired in most oncologycases as it is often suggested that delay in the initiationof RT may be detrimental to patient outcomes.
There are several studies which address the delay ofirradiation in HGG.7–10 Burnet et al. showed a steepdecline in median survival after a delay of 40 days frominitial consultation with radiation oncology.9 Do et al.found that there was a detrimental effect on patientsurvival with survival decreasing by 2% per day fromtime to presentation in RT department to commence-ment of radiation.8 Similarly, Irwin et al. showed thateach week of delay from surgery to starting RT increasesthe risk of death (hazard ratio) by 8.9%.10 In contrast,retrospective analysis of a Radiation Therapy OncologyGroup database of patients comprising around 3000patients showed that patients have superior outcomewhen RT was delayed 4 weeks from surgery.7 Also,patients did not appear to have reduced survival if RTstarted more than 6 weeks after their initial surgicalprocedure.
From our cohort, we observed no significant detrimentto survival with longer waiting times. Indeed, those withthe shortest times between surgery and the start of RTtrended towards the poorest survival. In this non-randomised setting, it is likely that patients whose situ-ation generated more clinical concern for aggressive
disease or who experienced early deterioration wereprioritised for early treatment. Additionally, we observedthat waiting times were significantly shorter for palliativehypofractionated courses compared to longer conven-tionally fractionated courses. This suggests that patientswho were less suitable for aggressive treatment dueto disease characteristics, performance status orco-morbidities experienced shorter waits for treatment.Hence, the apparent poor survival in patients treatedearliest is not unexpected and these data cannot beconsidered as support for the safety of extended delays.
The study identified patients who were re-treated withsecond and third courses of RT treatment. Our institutiondoes not have an aggressive policy on re-treatment.However, re-irradiation is occasionally used for patientswho progress or who develop recurrent disease with anotherwise good performance status. Notably, the mediantime to re-treatment was over 18 months, suggestingthat these are a highly selected group of patients whohave experienced a favourable clinical course.
Weaknesses of this study include uncertainty regard-ing RT treatment in the small numbers who were treatedelsewhere. The apparent 20% of patients who did notsee a radiation oncologist overestimates the proportionnot receiving a radiation oncology opinion. At least 16 of56 patients who did not receive an opinion were identi-fied as having had prior RT in the private sector. Inaddition, these data did not capture patients who werediscussed in a neuro-oncology MDM where a decisionwas made that referral to a radiation oncologist wasinappropriate. Furthermore, radiation oncology consul-tations made in the inpatient setting may have resultedin a recommendation for no treatment. Reasons for thisinclude poor performance status, significant comorbidityor treatment refusal. Subsequently, these patients maynot have been offered an outpatient appointment and noRT file was made for them. For this reason, while RT wasrecommended in 70% of all patients seen, and afterwardreceived in 66%, this slightly underestimates the actualdelivery of RT to HGG in Western Australia. This figure iscomparable to the numbers seen by Rosenthal et al.statewide in Victoria, where 68% of patients with HGGreceived RT as part of their management. However,documentation of the use of RT appears lower than in theNorth American data where 87% received RT,13 despitecaveats that some patients were treated elsewhere.Another weakness is the absence of clinical data docu-menting comorbidities and performance status whichmay have influenced treatment decisions. Furthermore,a recent study by Keime-Guibert et al.18 showed that theaddition of RT to management improves survival inelderly patients with HGG. This fact may not have beenappreciated during the period of accrual to the study. Inaddition, while follow-up was adequate for the cohort ofpatients with grade IV disease given low long-term sur-vival rates, a longer follow-up would allow for betterreporting of outcomes of patients with grade III disease.
M Jackson et al.
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists114

This was a prospective cohort study which is one of themain strengths of the data. Also, a high proportion ofincident cases of HGG are included in this dataset giventhe denominator provided by the WACR figures. With86% of patients with HGG receiving some portion of theircare at this study site, this dataset likely representscurrent practice in this state, and may represent realisticoutcomes for a relatively unselected patient group inthe setting of multidisciplinary evidence-based practiceoutside of a clinical trial.
Conclusion
We have described contemporary radiation oncologypatterns of care for HGG in an era of combination CRTand increased optimism surrounding the treatment ofHGG. Dose and fractionation practices appear concor-dant with published data and guidelines in most patientsreceiving LFRT. Survival is also consistent with clinicaltrial data for patients planned for aggressive therapy.However, despite this, the morbidity and mortality asso-ciated with the diagnosis of HGG remain high. The pro-portion of patients suitable for active managementappears unchanged from previous Australian data, and asubstantial number of patients still receive short-coursepalliative treatment and have poor outcomes. Survival isparticularly poor in those in whom treatment is aborted.Nevertheless, in a centralised tertiary setting with anactive MDM, patients appropriate for aggressive inten-sive therapy are identified and subsequently seenpromptly in the clinic. Most patients start their RT in atimely manner, but poor survival of those treated earliestmay reflect perceived clinical urgency in deterioratingpatients. The debate regarding the effects of RT delaywill not be resolved without appropriate randomisedclinical trials. However, many investigators may not feelsufficient clinical equipoise to make such trials feasible.
References
1. Laperriere N, Zuraw L, Cairncross G. The CancerCare Ontario Practice Guidelines InitiativeNeuro-Oncology Disease Site Group. Radiotherapy fornewly diagnosed malignant glioma in adults: asystemic review. Radiother Oncol 2002; 64: 259–73.
2. Stupp R, Mason WP, Van den Bent MJ et al.Radiotherapy plus concomitant and adjuvanttemozolomide for glioblastoma. N Engl J Med 2005;352: 987–96.
3. Denham JW, Hamilton CS, Joseph DJ. How should awaiting list for treatment be managed? AustralasRadiol 1992; 36: 274–5.
4. Esco R, Palacios A, Pardo J et al. Infrastructure ofradiotherapy in Spain: a minimal standard ofradiotherapy resources. Int J Radiat Oncol Biol Phys2003; 56: 319–27.
5. Mackillop WJ, Fu H, Quirt CF, Dixon P, Brundage M,Zhou Y. Waiting for radiotherapy in Ontario. Int JRadiat Oncol Biol Phys 1994; 30: 221–8.
6. Taghian A, Ramsay J, Allalunis-Turner J et al.Intrinsic radiation sensitivity may not be thedeterminant of the poor clinical outcome in GBM. IntJ Radiat Oncol Biol Phys 1993; 25: 243–9.
7. Blumethal DT, Won M, Mehta MP et al. Short delay ininitiation of radiotherapy may not affect outcome ofpatients with glioblastoma: a secondary analysis fromthe Radiation Therapy Oncology Group database.J Clin Oncol 2009; 27: 733–9.
8. Do V, Gebski V, Barton MB. The effect of waiting forradiotherapy for grade III/IV gliomas. RadiotherOncol 2000; 57: 131–6.
9. Burnet NG, Jena R, Jefferies SJ, Stenning SP,Kirkby NF. Mathematical modeling of survival ofglioblastoma patients suggests a role for radiotherapydose escalation and predicts poorer outcome afterdelay to start treatment. Clin Oncol (R Coll Radiol)2006; 18: 93–103.
10. Irwin C, Hunn M, Purdie G, Hamilton D. Delayin radiotherapy shortens survival in patients withhigh grade glioma. J Neurooncol 2007; 85:339–43.
11. Nowak AK, Maujean JE, Jackson M, Knuckey N. Aprospective study of surgical patterns of care forhigh grade glioma in the current era of multimodalitytherapy. J Clin Neurosci 2011; 18: 227–31.
12. Rosenthal MA, Drummond KJ, Dally M et al.Management of glioma in Victoria (1998–2000):retrospective cohort study. Med J Aust 2006; 184:270–3.
13. Chang SM, Parney IF, Huang W et al. Patterns ofcare for adults with newly diagnosed malignantglioma. JAMA 2005; 293: 557–64.
14. Clinical Practice Guidelines for the Managementof Adult Gliomas: Astrocytomas andOligodendrogliomas. August 2009. Cancer CouncilAustralia/Australian Cancer Network/ClinicalOncological Society of Australia.
15. Hoegler DB, Davey P. A prospective study ofshort course radiotherapy in elderly patients withmalignant glioma. J Neurooncol 1997; 33: 201–4.
16. Kleinberg L, Slick T, Enger C, Grossman S, Brem H,Wharam MD Jr. Short course radiotherapy is anappropriate option for most malignant gliomapatients. Int J Radiat Oncol Biol Phys 1997; 38:31–6.
17. Bauman GS, Gaspar LE, Fisher BJ, Halperin EC,Macdonald DR, Cairncross JG. A prospective study ofshort-course radiotherapy in poor prognosisglioblastoma multiforme. Int J Radiat Oncol Biol Phys1994; 29: 835–9.
18. Keime-Guibert F, Chinot O, Taillandier L et al.Radiotherapy for glioblastoma in the elderly. N Engl JMed 2007; 356: 1572–35.
Radiotherapy for HGG in Western Australia
© 2012 The AuthorsJournal of Medical Imaging and Radiation Oncology © 2012 The Royal Australian and New Zealand College of Radiologists 115




![Interactive Semi-automated Method Author Proof Using Non ...users.rowan.edu/~bouaynaya/Brats-Book-chapter.pdf · diagnosed with low and high grade gliomas. ... [2,7]. The basic idea](https://img.pdfslide.us/doc/110x75/5a728b7d7f8b9ab1538d9305/interactive-semi-automated-method-author-proof-using-non-usersrowanedubouaynayabrats-book-chapterpdfpdf.jpg)