Embed Size (px)
Citation preview

Radiotherapy
in Head & Neck
cancer
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

The Goal
1. Higher LR control and survival rates inlimited stage disease
2. Increased survival in locally advanceddisease (improved LR control, reducedprobability of DM and 2nd malignancies)
3. Increased organ preservation in resectableand unresectable tumors
4. Increased therapeutic ratio (cure/toxicity)
The best treatment in H&N cancer patients
should be made to obtain:
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Stage I / II Single modality (Surgery or RT)
Stage III / IV Combined modality - Surgery + RT (in most patients)- CT+ RT/CT (in selected patients)
Management for H&N Cancers
When different modalities have same results, one offering better QoL, with organ preservation and
good cosmetic results should be used
When different modalities are available, one with maximum chance of cure should be used
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

An example …..
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

An example …..
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

6
Improvement in
Clinical Results
Improvement in
TechnologyDo not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

• IMRT/IGRT (organ sparing)
• Radiosurgery (brain & body)
• IG-Brachytherapy
• Particle Therapy (Hadrons)
High Precision Radiotherapy
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Early Stages
(T1, T2 N0)
Nasopharynx
Oropharynx
Larynx
Hypopharynx
Oral cavity
Lip
External Beam RT (EBRT)→
Brachytherapy Intestitial
Contact
Endocavitary
RT as single modality
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

EBRT as single modality
T1 glottic
▪ LC rate: 82-94%
▪ Ultimate LC: 90-96%
▪ Larynx preservation:
83-95%
T2 glottic
▪ LC rate: 61-89%
▪ Ultimate LC: 80-91%
▪ Larynx preservation:
60-82%
Vocal cord
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Brachytherapy as single modality
▪T1 N0, mobile tongue
▪LC rate: 85-90%
▪Ultimate LC: 95%
Low dose rate
High/Pulsed Dose Rate
Oral cavity
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

SBRT BRT
SBRT or BRT as boost modality
Nasopharynx
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Study N. patients Follow-up
(months)
Dose (Gy)/
Fractions (n.) Response Toxicity
Vargo, 2015 50 18 40-44 / 5 1-y OS: 40% G3: 6%
Lartigau, 2013 60 11.4 36 / 6 RR: 58.4%
1-y OS: 47.5%
G3: 9%
Unger, 2010 65 26 30 / 5 2-y OS: 33% G4: 4.9%
Roh, 2009 36 17.3 18-40 / 3-5 RR: 80%
2-y OS: 30.9%
G3: 50%
Necrosis: 8%
Voynov, 2006 22 19 10-36 / NA 2-y LC: 26%
2-y OS: 22%
No G4
Orecchia, 1992 16 36 12-46 /2-6 CR: 43.7%
2-y OS: 28%
3-y OS 10%
G3: 32%
G4: 6%
SBRT for recurrent NPC
From: Baliga S et al, SBRT for recurrent head and neck cancer: a critical review. Head & Neck 2017 (modified)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

▪ Larynx and hypopharynx sites
▪ T2N+, and T3
▪ Selective T4 (without massive cartilage invasion and or
extension in the surrounding soft tissues)
▪ Baseline normal laryngeal function
▪ Good performance status
▪ Fit for treatment
▪ Patients’ desires
▪ Experience of the treating physicians
▪ Possibility of adequate follow-up
- No tracheotomy
- No vocal cord fixation
Organ and Function Preservation
Who?
Denaro, Radiother Oncol 2014
Forastiere , JCO 2015
Bonomi, Oral Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Organ and Function Preservation
Induction CT-RT
1. Induction CT-RT is the preferred treatment approach in Europe
2. Induction CT did not compromise subsequent treatment(salvage surgery or RT) in terms of tolerance or efficacy
3. None of the different induction CT regimens (PF or TPF) hasbeen able to improve survival in larynx preservation programs.Better rate of larynx preservation with TPF (+ 13% in GORTECgroup)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Organ and Function Preservation
Concurrent CT-RT1. Concurrent CT-RT is the preferred treatment approach in US
2. Concurrent CT-RT provides the highest larynx preservation ratedefined as the larynx in place
3. Concurrent CT-RT generates a substantial acute toxicity (twicehigher than other regimens)
4. Late toxicity after concurrent CT-RT may compromise thelaryngeal function (up to more than 40% of severe toxicity)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Postoperative management
Risk-adapted strategies
▪ Involved margins
▪ N3 disease
▪ 2+ invaded nodes
▪ Node 3+ cm
▪ Extra-capsular extension
▪ T4 disease
▪ Tumor volume
▪ Perineural invasion
▪ Perivascular extension
▪ Oral cavity primary
▪ RT only (54-60 Gy)
▪ Duration (shorter)
▪ Interval (6 weeks)
▪ RT-CT (higher risk)Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO

Interval Surgery - RT
Graboyes EM et al, Cancer 2017
National Cancer Data Base2006-2014
47,273 H&N patients
55.7% failed to commence PORT within 6 weeks
of surgery
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Patient set-up
MLC/ MMLC
Export
Dose evaluation
Treatment technique
Targeting
Dose prescription
ContouringLocalization
ImageFusion
MRI / PET-CT
Image acquisition
Treatment
Immobilization Device
Imaging Treatment Planning Hardware
CT
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

T2 SCC of the internal wall of the right piriform sinus
T4a SCC of the glottic larynx
Gregoire V et al,
Radiother Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Recommendations for Neck CTV
Node-negative neck: DAHANCA,
EORTC, GORTEC, NCIC, RTOG
Radiother Oncol 2003
Node-positive neck and PORT:
Radiother Oncol 2006
Neck node levels: DAHANCA,
EORTC, HKN-PCSG, NCIC CTG,
NCRI, RTOG; TROG
Radiother Oncol 2014
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

IMRT is the standard !
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Non-modulated vs modulated RT
CTV
OR
CTV
OR
Conformal with
non-modulated beams-3DCRTConformal with modulated
beams-IMRT
Prescription Dose
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Lesion
Radiation Critical Organs
Multileaf Collimator
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Planning CT 3 weeks into RT
Planning CT Mid course RT
Physically Adapted IMRT
Re-planning
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Biologically Adapted RT
Dose Painting
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

IMRT
1. To reduce xerostomia in all naso-, oro-, and hypo-pharyngeal, laryngeal, oral cavity and unknownprimary cancers
2. To reduce ocular toxicities in nasal and paranasalsinus cancer or other sites where the disease isjuxtaposed to the optic apparatus
3. To reduce osteoradionecrosis in oral cavity, naso-and oro-pharynx, paranasal sinuses and wheresignificant dose of radiation are required
4. Related to clinical outcomes (LC and OS) there areno study data to support or refuse IMRT over 2D- or3D-RT in any H&N sites
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Parotid sparing
(<26 Gy)
3D-CRT
IMRT
Prevention of xerostomia
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Constrictor muscles sparing
Swallowing muscles dose-volume parameters are strongly related with
chronic RAD (Radiation Associated Dysphagia)
Alterio D, … R.Orecchia.
Contouring of the Pharyngeal Superior Constrictor Muscle
(PSMC). A cooperative study of the Italian Association of
Radiation Oncology (AIRO) Head and Neck Group.
Radiother Oncol 2014
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

85% Isodose
2 Gy/die
95% Isodose
2,2 Gy/die
30 fractions
66 Gy Tumor
60 Gy Lymph nodes
Simultaneous Integrated Boost SIB
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

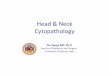
Improved survival using IMRT in H&N cancers. A SEER-Medicare analysis
Beadle BM et al, Cancer 2014
IMRT patients
No IMRT patients
Overall Survival
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Radiosensitivity in H&N cancer
1. The radiosensitivity index values for patients withH&N cancer is heterogeneous – the differencebetween the most sensitive and most resistantsamples is more than 3 time (less in OP cancer)
2. This variability implies that a uniform strategy isnot always recommended in clinical practice, andthe use of integrating approaches based onindividual difference could improve results
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Molecular signature for H&N RT
There is a tremendous
potential to apply molecular
signature to predict response
to RT
Many pathways are known to
regulate radiation
sensitivity, and novel markers are emerging
Pardo-Reoyo S et al, Ann Transl Med 2016
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Radiotherapy de-intensifications
HPV16+ versus HPV16-
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Trial Phase N.
patients
Inclusion criteria Response
NRG HN-002 II 296 T1-2, N1-2b, or T3, N0-2b
HPV+, OPC
<10 PY
Reduced IMRT dose (60
Gy)
with/without weekly
cisplatin
NCT01530997 II 40 T1-3, N0-2c
HPV+, OPSCC
<10 Py or >5y abstinence
IMRT (54-60 Gy) with
weekly cisplatin
ECOG 1308 II 80 Resectable IIIA/IIIB, IVA/IVB
HPV+, OPSCC
(p-16 high or HPV-16 ISH+)
IC, then response
adapted RT (54 or 66-70
Gy) with cetuximab
Quarterback III 365 III/IV (M0)
HPV associated
OPSCC/Unknown/NPC
<20 PY / no active smokers
IC with TPF: CR/PR
randomly assigned 2:1
to CBDCA with RT (56
versus 70 Gy). Non responders: standard RT
RT de-intensification trials
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Lassen P et al, Radiother Oncol 2018
815 patients from 4 randomized trials: RTOG 9003, Dahanca 6&9,
RTOG 0129, ARTSCAN
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Lassen P et al, Radiother Oncol 2018
• Clear advantage
in OS for p16+
patients, and never
smokers
(+24.2% at 10-y)
• Small advantage
for never smokers
patients also in p16-
patients
(+8.4% at 10-y)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Particle Therapy (Hadrons)
X-rays
electron
negative
ions
proton
neutronHelium Carbon
ArgonBoronNeon
General RadiationFrom Lighter to Heavier Particles
Oxygen
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Particles versus Photons (X-rays)
▪ Irradiate smaller volume of normal tissues
▪Photon beam decreases exponentially with depth in the
irradiated tissues
▪Hadrons have a finite
range (no exit dose)
▪Hadrons deposit most
of their radiation energy
in what is known as
Braggs peak
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Particles. A new dimension …….
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Carotid artery
Optic nerve
Mandibular boneBrain Stem
Main Goal: OARs Sparing
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

10 – 20 keV/mm = 100 – 200 MeV/cm =
20 – 40 eV/(2 nm)
Radiobiological Effectiveness (C12)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Carbon ion
in Chiba (J)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Take Home Message (I)
1. About 75% of patients with H&N SCC benefits fromRT as part of their primary treatment or as adjuvantmodality
2. Loco-regional control has improved in the last 10-15years, and these improvements have translated intogains in survival rates
3. As a consequence, a progressive shift has beenobserved from primary surgery to function-preservation RT
4. Significant progress has been made in improving theQoL of the patients by decreasing the long-termadverse effects of RT, such as xerostomia andswallowing difficulties
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Take Home Message (II)
5. IMRT is today the standard technique for H&Ncancers, with BRT and SBRT available to treatspecial cases
6. Increasing interest in particle therapy is justified bythe possibility to spare OARs and to overcameradio-resistance in specific tumor types
7. Molecular signatures on individuals could help inthe next future for properlyselecting patients to betreated by intensifing combinedtherapies and/or de-intensifingapproaches
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Thank You for Your attention !!!!...
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO