Embed Size (px)
Citation preview

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
Report No. 4

About Public Health England
Public Health England exists to protect and improve the nation's health and wellbeing, and
reduce health inequalities. It does this through world-class science, knowledge and intelligence,
advocacy, partnerships and the delivery of specialist public health services. PHE is an
operationally autonomous executive agency of the Department of Health.
Public Health England
133–155 Waterloo Road
Wellington House
London SE1 8UG
T: 020 7654 8000
www.gov.uk/phe
Twitter: @PHE_uk
Facebook: www.facebook.com/PublicHealthEngland
© Crown copyright 2016
You may re-use this information (excluding logos) free of charge in any format or medium, under
the terms of the Open Government Licence v3.0. To view this licence, visit OGL or email
[email protected]. Where we have identified any third party copyright information
you will need to obtain permission from the copyright holders concerned.
Any enquiries regarding this publication should be sent to
Chilton Information Office
Centre for Radiation, Chemical and Environmental Hazards
Public Health England
Chilton, Didcot, Oxfordshire OX11 0RQ
Published September 2016
PHE publications gateway number: 2016255

PHE-CRCE-029
Centre for Radiation, Chemical and Environmental Hazards Public Health England Chilton, Didcot Oxfordshire OX11 0RQ
This report from the PHE Centre for Radiation, Chemical and Environmental Hazards reflects understanding and evaluation of the current scientific evidence as presented and referenced in this document.
Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
Report No. 4
Patient Safety in Radiotherapy Steering Group


iii
Executive summary
The fundamental role of reporting and learning systems is to enhance patient safety by
learning from failures of the healthcare system1. It is known that most problems are not just a
series of random, unconnected one-off events; they are provoked by poor systems and often
have common root causes that can be generalised and corrected. Although each event is
unique, there are likely to be similarities and patterns in sources of risk that may go unnoticed
if incidents are not reported and analysed.
Experience has shown that as an organisation’s reporting culture matures, staff become more
likely to report incidents. There is an emerging evidence base that organisations with a higher
rate of reporting have a stronger safety culture. High reporters aim to learn from incident
reporting to make patient care safer. With this in mind an increase in incident reporting should
not necessarily be taken as an indication of worsening patient safety, it may indicate an
increasing level of awareness of safety issues among healthcare professionals and a more
open and transparent culture across the organisation.
This report is the fourth in a series of two-year reports, providing an overview of Radiotherapy
Error (RTE) data reported voluntarily to the National Reporting and Learning System (NRLS)
and directly to PHE from December 2013 until November 2015. This report also contains data
received from the inspectorates for IR(ME)R for England, Wales, Northern Ireland and Scotland.
Use of the terminology, classification and coding of TSRT, together with implementation of the
national voluntary reporting system described within this report, allows clinical departments to
compare their local analysis to the national picture.
This report identifies errors in activities undertaken by various professional groups, throughout
the patient pathway and across different service providers. A total of 41.4% (n = 5254) of the
RTEs reported were associated with ‘treatment unit process’ and 16.2% (n = 2053) occurred
during ‘pretreatment planning process’. RTEs were spread across all 21 categories of process
code. The vast majority of reports were categorised as lower level events, thus not affecting
the outcome of patient care.
In this analysis the following processes have been identified as areas in the radiotherapy
pathway where RTEs commonly occur, in order of descending frequency:
on-set imaging: production process (13z)
use of on-set imaging (13i)
on-set imaging: approval process (13aa)
accuracy of data entry (12f)
documentation of instructions/information (10j)
on-set imaging: recording process (13bb)
management of process flow within planning (11o)
recording of patient specific instructions (11n)
movements from reference marks (13l)
bookings made according to protocol (6a)
When compared with the 2014 two-year report2 a slight change in error trends can be seen.
Eight of the same process subcodes were found in the most frequently reported list in both the
current and 2014 analyses, seven of these were also within the 2012 analyses2. These ranked
differently between analyses.

iv
In addition, when compared with results from the 20142 report there has been no overall
change in the percentage of reportable (1.7% in 2014 and 1.8% in 2016) and non-reportable
radiation incidents (1.3% in 2010 and 1.4% in 2016). However, there has been a slight
increase in the percentage of minor radiation incidents from 28.6% in 2014 to 31.5% in 2016.
There has been an overall decrease in the percentage of other non-conformances (41.6% in
2014 and 36.6% in 2016). It is known that clinical departments are more likely to submit
reports on higher level RTEs such as level 1 ‘reportable radiation incident’, level 2 ‘non-
reportable radiation incident’ and level 3 ‘minor radiation incident’3.
It is imperative that RTE trends continue to be reported, analysed and monitored on a cyclical
basis, in order to inform ongoing safe and effective radiotherapy practice. This is especially
pertinent as new techniques and technologies are implemented and as new clinical
radiotherapy departments are established. This work supports a risk-based approach to
improving safety both locally and nationally, and indicates a culture that is open, transparent
and already present in the UK radiotherapy community.
Key recommendations:
a) Radiotherapy departments across the UK should continue to use Towards Safer
Radiotherapy (TSRT) to classify and code all of their RTEs, including near misses for local
analysis to inform policy and practice
b) Radiotherapy departments across the UK should continue to submit coded and classified
RTE reports to the national voluntary reporting system using the mechanisms identified
within this report
c) To ensure timeliness of learning providers are encouraged to report on a monthly basis
d) Radiotherapy departments across the UK should consider all codes when coding RTE
and the use of secondary or additional subcodes
e) The Patient Safety in Radiotherapy Steering Group (PSRT) should continue to develop
analysis of the reports, with regular dissemination of findings to the radiotherapy
community for group learning
f) The data should be used both by the PSRT and by individual radiotherapy departments as
part of a risk-based approach to allocating resources for improving patient safety in
radiotherapy and to inform audit and research
g) The mechanism to enable departments in Scotland and Northern Ireland to submit RTE
reports to PHE for collation and analysis as part of a UK dataset should be further refined
h) A mechanism should be developed to enable independent radiotherapy providers to
submit RTE reports to PHE for collation and analysis as part of a UK dataset
i) The radiotherapy pathway coding as described in TSRT should be refined to reduce any
ambiguity of codes and to reflect the use of emerging techniques and technologies, this
should include safety barriers and causative factor taxonomies.
j) Radiotherapy departments across the UK should consider reviewing their end of process
checks and consider pause and check work
References 1. World Health Organization. Reporting and learning for patient safety. Available at
http://www.who.int/patientsafety/implementation/reporting_and_learning/en/ 2. PSRT. Data report on radiotherapy errors and near misses. Available at
www.gov.uk/government/publications/radiotherapy-errors-and-near-misses-data-report 3. PSRT. Safer radiotherapy: supplementary survey analysis. Report 3 (2014). Available at
www.gov.uk/government/publications/safer-radiotherapy-supplementary-survey-analysis

v
Contents
Executive Summary iii
1 Introduction 1
2 Background 1
3 Data 2
3.1 Number of reports 3
3.2 Obtaining the data 3
3.2.1 National voluntary reporting system 3
3.2.2 Northern Ireland and Scotland 4
3.3 Organisation of the database 4
3.4 Quality assurance of data 4
3.4.1 Consistency checking 4
3.4.2 Data quality 5
3.4.3 Lag time for reporting 6
4 Results 6
4.1 Classification level of RTE 6
4.2 Breakdown of classification by process code 7
4.2.1 Breakdown of level 1 (reportable radiation incident) RTE 7
4.2.2 Breakdown of level 2 (non-reportable radiation incident) RTE 9
4.2.3 Breakdown of level 3 (minor radiation incident) RTE 12
4.2.4 Breakdown of level 4 (near miss) RTE 14
4.2.5 Breakdown of level 5 (other non-conformance) RTE 16
4.3 Main themes of RTE 18
4.3.1 Breakdown of process codes 18
4.3.2 Breakdown of process subcodes 18
4.3.3 Additional process subcodes 19
4.3.4 End of process checks 20
4.4 Inspectorate data 21
5 Discussion 23
5.1 Increase in RTE reporting 23
5.2 Classification level of RTE 24
5.2.1 Level 1 (reportable radiation incident) RTE 26
5.2.2 Level 2 (non-reportable radiation incident) RTE 26
5.2.3 Level 3 (minor radiation incident) RTE 26
5.2.4 Level 4 (near miss) RTE 27
5.2.5 Level 5 (other non-conformance) RTE 27
5.3 Main themes 27
5.3.1 Breakdown of process codes 27
5.3.2 Breakdown of process subcodes 28
5.3.3 End of process checks 29
5.4 Inspectorate data 30
6 Conclusion 30

vi
7 Key recommendations 32
8 Acknowledgements 33
9 PSRT Steering Group Membership 33
10 References 34
Appendix A Radiotherapy error classification grid 35
Appendix B Radiotherapy pathway coding 36

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
1
1 Introduction
The fundamental role of reporting and learning reporting systems is to enhance patient safety
by learning from failures of the healthcare system1. It is known that most problems are not just
a series of random, unconnected one-off events; they are provoked by poor systems and often
have common root causes which can be generalised and corrected. Although each event is
unique, there are likely to be similarities and patterns in sources of risk that may go unnoticed
if incidents are not reported and analysed.
The need to further improve the safety of patients undergoing radiotherapy treatments has
gathered worldwide momentum in recent years. The 2006 report2 of the Chief Medical Officer
for England and Towards Safer Radiotherapy3 (TSRT), published in 2008, were seminal
documents in the field of radiotherapy safety; both contained practical recommendations for
the radiotherapy community aimed at improving safety and reducing errors.
More recently, recommendations of the Francis Report4 into failings at the Mid-Staffordshire
NHS Foundation Trust included a requirement for openness, transparency and candour
throughout the NHS to support a culture of protecting patients and removing poor practice.
Experience has shown that as an organisation’s reporting culture matures, staff become more
likely to report incidents. There is an emerging evidence base that organisations with a higher
rate of reporting have a stronger safety culture. High reporters aim to learn from incident
reporting to make patient care safer. With this in mind an increase in incident reporting should
not necessarily be taken as an indication of worsening patient safety. It may indicate an
increasing level of awareness of safety issues among healthcare professionals and a more
open and transparent culture across the organisation.
This report is the fourth in a series of two-year reports, providing an overview of Radiotherapy
Error (RTE) data reported voluntarily to the National Reporting and Learning System (NRLS)
and directly to PHE from December 2013 until November 2015.
2 Background
Towards Safer Radiotherapy3 (TSRT) provides definitions for the terminology to be used in
discussing radiotherapy errors that include near misses (RTE) and proposes two taxonomies
for use in describing RTEs. The ‘classification of radiotherapy errors grid’ (Appendix A)
describes the severity of the error and the ‘radiotherapy pathway coding’ (Appendix B)
describes where in the radiotherapy pathway the error occurred. The proposed terminology
and taxonomies have now been adopted and are in use in radiotherapy departments across
the UK.
In 2008, the Patient Safety in Radiotherapy Steering Group (PSRT) was tasked with
monitoring the implementation of the recommendations from TSRT, through a collaborative
programme of work with the radiotherapy community. PSRT membership includes
representatives from Public Health England (PHE), Royal College of Radiologists, Society and
College of Radiographers, Institute of Physics and Engineering in Medicine and a patient
representative. The group is currently chaired by PHE where detailed analysis of RTE reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
2
is undertaken, reported to the PSRT and disseminated to the radiotherapy community to
provide learning opportunities.
The NRLS operates an anonymised voluntary reporting system to collect and learn from
patient safety incidents for England and Wales. As of April 2016 the NRLS moved from NHS
England to NHS Improvement. PHE has a data sharing agreement with the NRLS and under
this agreement continues to extract RTE data from the NRLS, and share learning from these
events so as to make services safer for patients. This collaboration led to the publication in
July 20105 of the first two-year data report on a back catalogue of patient safety incidents
reported to the NRLS between August 2007 and November 2009. The first report aimed to
provide learning from incidents already reported, to trial the application of the taxonomies from
TSRT and to test the mechanism for reporting. Subsequently the PSRT asked radiotherapy
department staff to classify and code all errors according to the taxonomies presented in
TSRT within their local incident reporting systems for subsequent submission for analysis by
PHE staff as part of a voluntary reporting scheme.
This publication was closely followed in September 2010 by the introduction of a series of
newsletters entitled Safer Radiotherapy6 providing regular updates on the analysis of
radiotherapy error (RTE) reports for professionals working in the radiotherapy community. In
2012 a second report was published7. In November 2013 a mechanism for providers in
Northern Ireland and Scotland to contribute to this voluntary reporting scheme was introduced.
Subsequently data from across the UK, including data received from the inspectorates for
IR(M)ER for England, Wales, Northern Ireland and Scotland was then published within the
third two yearly report in November 20148.
This fourth report will compare data from previously published reports.
3 Data
The data presented in this report is anonymised and received as part of a voluntary reporting
scheme. As with any voluntary reporting system, the data will only reflect those incidents that
are reported and may not necessarily be representative of the actual level of occurrence. As
such, this data needs interpreting with care.
A total of 12,800 RTE reports were submitted to the voluntary reporting scheme between
December 2013 and November 2015 (Figure 1). On average 533 RTE reports were received
each month, this is a marked increase from average of 323 within the last report8. The number
of reports received ranged from 323 in March 2014 to 839 in November 2015.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
3
3.1 Number of reports
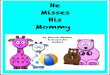
Figure 1: Number of RTE reports submitted to the national voluntary reporting system by month, from December 2013 to November 2015 (n = 12800)
Between December 2013 and November 2015 a total of 60 NHS providers submitted RTE.
The number of providers reporting per month fluctuated between 34 and 52 with a mean
average of 42 NHS providers reporting per month, this is a vast increase from the report in
2014 where an average of 28 providers submitted data each month8. The variation highlights
that not all providers report on a monthly basis.
3.2 Obtaining the data
The voluntary data was obtained through two distinct routes: from the NRLS for providers in
England and Wales and directly from providers in Northern Ireland and Scotland. These are
described in detail below.
3.2.1 National voluntary reporting system
The vast majority of reports came through the NRLS, which collates reports for England and
Wales. The NRLS operates a voluntary reporting system to collect and learn from patient
safety incidents. A patient safety incident (PSI) is defined as:
‘Any unintended or unexpected incident which could have or did lead to harm for one or more
patients receiving NHS care’9.
PSIs are reported by NHS staff through local trust risk management systems and web based
forms to the NRLS. Patients and carers can also report directly through an open access form.
The NRLS offers a unique dataset to help understand harm associated with healthcare. It was
established in 2003 and now has over 11.8 million PSI reports10
, from many areas of
healthcare, in the database.
0
100
200
300
400
500
600
700
800
900
Dec
-13
Jan-
14
Feb
-14
Mar
-14
Apr
-14
May
-14
Jun-
14
Jul-1
4
Aug
-14
Sep
-14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb
-15
Mar
-15
Apr
-15
May
-15
Jun-
15
Jul-1
5
Aug
-15
Sep
-15
Oct
-15
Nov
-15
Num
ber
of R
epor
ts

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
4
The NRLS can be interrogated for relevant incidents by searching the free text field of any
incident report using key words or search terms. During the development of this work, a
system was created to extract targeted data from the NRLS using a trigger code ‘TSRT9’. This
was proposed and described in ‘Implementing Towards Safer Radiotherapy: guidance on
reporting radiotherapy errors and near misses effectively’11
. This code could be searched for
in the free text field rather than using search terms that were less determinant. PSIs that were
not RTEs, such as a report of a patient falling in ‘radiotherapy’, would not be included in the
RTE dataset. An RTE is defined by TSRT as:
‘a non-conformance where there is an unintended divergence between a radiotherapy
treatment delivered or a radiotherapy process followed and that defined as correct by local
protocol’3.
3.2.2 Northern Ireland and Scotland
A mechanism was developed to enable departments in Northern Ireland and Scotland to
participate in this scheme in 2013. Once agreements for data sharing were achieved with
health boards and hospital trusts, predefined criteria consistent with those employed for the
NRLS data were shared with radiotherapy providers in Northern Ireland and Scotland for
inclusion in reports.
Anonymised data has been accepted from providers on Microsoft Excel spreadsheets for
direct upload into the PHE radiotherapy incident database to minimise the possibility of
transcription error and to ensure the anonymity of the data.
PHE is working to further streamline the reporting mechanism for providers in Northern Ireland
and Scotland while continuing to receive and include this data in the tri-annual analyses6.
3.3 Organisation of the database
An established database continues to act as a repository for the data. It also supports the
analysis of the data through the use of scripted reports on frequency and trends analysis.
The database has access restricted to named individuals directly involved with the quality
assurance and analysis of the data. All data was submitted for upload by PHE staff to the
database by import of Microsoft Excel spreadsheets. For the purposes of the analysis each
RTE report submitted is included as a single report.
3.4 Quality assurance of data
The data supplied was initially scrutinised by PHE staff and consistency checking of the
application of the coding and classification undertaken. Reports run in the database were
checked against manual calculations to verify the expected outcomes.
3.4.1 Consistency checking
On receipt of the reports, PHE staff with clinical radiotherapy expertise performed consistency
checking of the local application of the classification and coding from TSRT. Up to four
individual pathway codes can be allocated locally by radiotherapy departments to each RTE

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
5
report. This formed part of the data quality assurance process completed prior to analysis of
the reports.
Consistency checking of the appropriate application of the coding and classification
taxonomies remained high, with 87.1% agreed in this dataset, and is slightly higher than
83.7% agreement achieved in the 2014 report8.
It is thought the positive result in consistency checking is in part due to the publication of a
guidance document11
on the use of the trigger code and application of the coding and
classification, development of a supplementary series on good practice in RTE reporting12
and
familiarisation with the taxonomies.
All providers are asked to include a trigger code, classification and coding in RTE reports to
facilitate both local and national analysis.
3.4.2 Data quality
Reports were categorised into patient safety incidents (PSI), radiotherapy errors (RTE) and
incomplete radiotherapy errors (IRTE). PSI and RTE have been previously defined. IRTE
reports were defined as reports without the classification and coding being applied locally prior
to submission.
Radiotherapy department staff were asked to classify and code incidents according to the
taxonomies presented in TSRT within their current local incident reporting systems. The
introduction of the trigger code in August 2009 resulted in a significant reduction in the number
of unrelated non-radiotherapy errors for analysis (see Table 1).
Since the publication of the first two-year report in 20105 the quality of the data received has
improved significantly, as demonstrated in the table. Previously a significant number of non-
radiotherapy error (NRTE) reports had been included in the data. These included incident
reports from radiological disciplines other than radiotherapy. However in the 2016 report 1528
reports did not include the classification and coding outlined within TSRT, this may be due to
departments submitting RTE reports before the classification and coding has been included
locally.
Table 1: Comparison of data quality between the current dataset and the previous reports showing the overall percentage of reports submitted
Type of data report
2016 report (Dec 13 – Nov 15) (n = 12,800)
2014 report (Dec 11 – Nov 13) (n = 7742)
2012 report (Dec 09 – Nov 11) (n = 3411)
2010 report (Aug 07 – Nov 09) (n = 1365)
% RTE 87.2 90 97.2 46
% NRTE/PSI 0.8 1 2.4 41
% IRTE 12 9 <0.4 13
PSI patient safety incident; RTE radiotherapy error; IRTE incomplete radiotherapy error; NRTE non-radiotherapy error
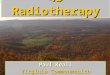
Of the 12,800 RTE reports received, a total of 12,691 reports were included in the analysis
11,163 had been classified and coded by local RT providers. There were 1,540 IRTE reports
of which 1,528 had sufficient detail to allow PHE staff to classify and code. The remaining 12
IRTE, in addition to 97 PSI reports, were excluded from the analysis (Figure 2).
A total of 99.1% (87.2% RTE and 11.9% IRTE) of the data submitted was included for analysis
in this report; this is consistent with reported data in 20148.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
6
Figure 2: Type of RTE identified in reports submitted from December 2013 to November 2015 (n = 12800)
3.4.3 Lag time for reporting
A lag time between the date of the incident and the date on which it was reported to PHE was
calculated for the dataset. This measures the time from the date of incident or discovery of the
incident through local reporting and on to PHE.
A minimum reporting lag of 1 day and a maximum of 864 days, with a mean reporting lag of
58.8 days and a mode of 21 days was found. There were two outliers of over 800 days; these
two outliers were reported on discovery of the error, which was not until a significant time after
the event. However the majority of departments are reporting in a timely fashion. To ensure
timeliness of learning providers are encouraged to report on a monthly basis.
4 Results
The use of the taxonomies from TSRT provided the focus for the analysis of this data. The
‘classification of radiotherapy errors grid’ describes the severity of the incident and is made up
of five levels, one being the most severe and five being a non-conformance. The classification
grid from TSRT is reproduced in Appendix A. The ‘radiotherapy pathway coding’ describes
where on the patient pathway the error has occurred. This has 21 constituent codes and 193
subcodes, which are reproduced from TSRT in Appendix B.
4.1 Classification level of RTE
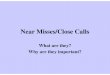
Each of the 12691 reports was classified as ‘other non-conformance’, ‘near miss’, ‘minor radiation
incident’, ‘non-reportable radiation incident’ and ‘reportable radiation incident’ (Figure 3).
Of the RTE reports, 65.3% (n = 8288) were near miss or other non-conformities with no
impact on patient outcome. In total, 31.5% (n = 3994) of the RTEs reported were not clinically
significant and were classified as ‘minor radiation incidents’. Of the remaining 3.2% (n = 409)
RTE (n=11163) 87.2%
PSI (n=97) 0.8%
IRTE included (n=1528)
11.9%
IRTE excluded (n=12) 0.1%
Other (n=1540) 12.0%

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
7
RTE reports, 1.8% (n = 232) were reportable under either of two statutory instruments, the
Ionising Radiation (Medical Exposure) Regulations (IR(ME)R)13
or the Ionising Radiations
Regulations (IRR99)14
, to the appropriate authority.
Figure 3: Classification of reports from December 2013 to November 2015 (n = 12691)
4.2 Breakdown of classification by process code
In this section the RTE reports are broken down by classification into their attributed process
codes and subcodes.
4.2.1 Breakdown of level 1 (reportable radiation incident) RTE
Reportable radiation incidents fall into the category of incidents reportable under either of the
statutory instruments, IR(ME)R13
or IRR9914
. Clearly, reporting to the national voluntary
reporting scheme does not negate regulatory requirements to report level 1 events to the
appropriate authority.
The majority of the level 1 events reported affected only a single fraction of treatment and thus
were correctable over the remaining fractions with no significant impact on the patient or
outcome of treatment. Reportable radiation incidents comprised 1.8% (n = 232) of the RTEs
reported (Figure 3). Of the level 1 events, 50.0% (n = 116) occurred during ‘treatment unit
process’, 22.0% (n = 51) during ‘pretreatment activities/imaging’ and 11.2% (n = 26) during
‘communication of intent’ (Figure 4).
0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000
5 Other non-conformance
4 Near miss
3 Minor radiation incident
2 Non-reportable radiation incident
1 Reportable radiation incident
Number of Reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
8
Figure 4: Breakdown of level 1 (reportable radiation incident) reports by process code, from December 2013 to November 2015 (n = 232)
Further analysis of the ‘treatment unit process’ reports indicates the points in the pathway on
the treatment unit at which the reportable radiation incidents occurred (Figure 5).
‘Movements from reference marks’ comprised 10.8% (n = 25) of all reportable radiation
incidents reported for this time period. Examples of these types of reports included moves
from reference marks to isocentre made in the wrong direction, the wrong dimension or not at
all. Some reports added the error was not picked up until images were reviewed offline.
Figure 5: Breakdown of the most frequently occurring level 1 (reportable radiation incident) reports associated with process code 13 (treatment unit process), from December 2013 to November 2015 (n = 94/116 subset of reports)
0 20 40 60 80 100 120
13 Treatment unit process
10 Pretreatment activities / imaging
5 Communication of intent
4 Referral for treatment
11 Pretreatment planning process
12 Treatment data entry process
9 Mould room/workshop activities
7 Process prior to first appointment
8 Pretreatment: preparation of patient
Number of reports
0 5 10 15 20 25
13l Movements from reference marks
13z On-set imaging: production process
13k ID of reference marks
13aa On-set imaging: approval process
13g Patient positioning
13i Use of on-set imaging
13q Setting of couch position/angle
13r Use of immobilisation devices
13m Setting of treatment machine parameters
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
9
Level 1 reports were also broken down by most frequently occurring process subcode
(Figure 6). This revealed ‘movements from reference marks’ followed equally by ‘on-set
imaging: production process’ and ‘localisation of intended volume’ as the most frequently
occurring process subcodes in this group. An example of the latter type of RTE was the
requirement to rescan a patient due to not capturing the intended volume on the initial scan.
A common example of ‘on-set imaging: production process’ RTE was repeat scans due to
selection of incorrect presets when performing cone beam CTs. On-set imaging: production
process was not part of the most frequently occurring level 1 process subcodes in the 2014
report8, the rise in incidence of this error may be due to an increased uptake in the use of on-
set imaging.
Figure 6: Breakdown of the most frequently occurring level 1 (reportable radiation incident) process subcodes, from December 2013 to November 2015 (n = 134/232 subset of reports)
4.2.2 Breakdown of level 2 (non-reportable radiation incident) RTE
A non-reportable radiation incident is defined by TSRT as a radiation incident ‘not reportable,
but of potential or actual clinical significance’3.
Non-reportable radiation incidents comprised 1.4% (n = 177) of the RTE reports. Of these
level 2 reports, 59.3% (n = 105) occurred during ‘treatment unit process’ (Figure 7). RTEs
were spread across 12 categories of process code for level 2 classifications. A subset of these
reports were grouped into ‘miscellaneous’ as the numbers reported within the process codes
were deemed statistically less significant.
0 5 10 15 20 25
13l Movements from reference marks
13z On-set imaging: production process
10c Localisation of intended volume
13k ID of reference marks
10b Positioning of patient
13aa On-set imaging: approval process
10f Production of images demonstrating correct detail
5a Completion of request for treatment
13g Patient positioning
5k Authorisation to irradiate
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
10
Figure 7: Breakdown of level 2 (non-reportable radiation incident) reports by process code, from December 2013 to November 2015 (n = 177)
Further analysis of the ‘treatment unit process’ indicates the points in the pathway on the
treatment unit at which the reportable radiation incidents occurred (Figure 8).
‘On-set imaging: approval process’ was notably the most frequently occurring event at 27.6%
(n = 29) within the subset of non-reportable radiation incidents (Figure 8). Examples of RTE
reports associated with ‘on-set imaging: approval process’ included the incorrect matching of
reference and verification image and several reports indicated this was due to matching to the
wrong vertebrae level.
Level 2 reports were also broken down by most frequently occurring process subcode
(Figure 9). Findings were consistent with those above, with ‘on-set imaging: approval process’
being the most frequently occurring event within this subset of non-reportable RTE.
0 20 40 60 80 100 120
13 Treatment unit process
10 Pretreatment activities / imaging
11 Pretreatment planning process
12 Treatment data entry process
5 Communication of intent
4 Referral for treatment
15 Brachytherapy
9 Mould room/workshop activities
2 New equipment
Miscellaneous
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
11
Figure 8: Breakdown of most frequently occurring level 2 (non-reportable radiation incident) reports associated with process code 13 (treatment unit process), from December 2013 to November 2015 (n = 84/105 subset of reports)
Figure 9: Breakdown of the most frequently occurring level 2 (non-reportable radiation incident) process subcodes, from December 2013 to November 2015 (n = 86/177 subset of reports)
0 5 10 15 20 25 30
13aa On-set imaging: approval process
13l Movements from reference marks
13z On-set imaging: production process
13i Use of on-set imaging
13m Setting of treatment machine parameters
13g Patient positioning
13q Setting of couch position/angle
13r Use of immobilisation devices
13c Patient data ID process
Number of reports
0 5 10 15 20 25 30
13aa On-set imaging: approval process
13l Movements from reference marks
13z On-set imaging: production process
13i Use of on-set imaging
13m Setting of treatment machine parameters
13g Patient positioning
13q Setting of couch position/angle
10f Production of images demonstrating correct detail
10b Positioning of patient
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
12
4.2.3 Breakdown of level 3 (minor radiation incident) RTE
A minor radiation incident is defined by TSRT as a radiation incident ‘in the technical sense
but one of no potential or actual clinical significance’3.
Minor radiation incidents comprised 31.5% (n = 3994) of the coded RTE reports as seen in
Figure 10. ‘Treatment unit process’ was the most common code for these reports, at 75.1%
(n = 2998). RTEs were spread across 18 categories of process code for level 3 classifications.
A subset of these reports was grouped into ‘miscellaneous’ as the numbers reported within
process codes were deemed statistically less significant.
Figure 10: Breakdown of level 3 (minor radiation incident) reports by process code, from December 2013 to November 2015 (n = 3994)
Further analysis of the ‘treatment unit process’ indicates the points in the pathway at which
the minor radiation incidents occurred (Figure 11). ‘On-set imaging: production process’ was
the most frequent occurring event, at 30.8% (n = 922) within the subset of minor radiation
incidents. Examples of this type of RTE included incorrect or inappropriate imaging settings
selected during verification imaging.
A review of the ‘on-set imaging production process’ subset of RTE reports revealed that
48.9% (n = 451) related to procedural failures, examples of which included ‘incorrect imaging
parameters selected’, ‘wrong image acquisition image mode selected’, ‘incorrect blade moved
for image capture’ and ‘imager not extended or appropriately positioned’. The remaining
51.1% (n = 471) of this subgroup related to equipment failure. Examples of these types of
reports included ‘failure of the imaging device during image acquisition’, ‘image not captured
after exposure’, ’flooded image’ or ‘image unavailable offline’. This resulted in additional
imaging being undertaken. Radiotherapy providers are encouraged to audit and report these
events locally so appropriate and timely preventative measures might be implemented. In
addition, the Medicines and Healthcare products Regulatory Agency (MHRA) should be
advised of all equipment failures.
0 500 1000 1500 2000 2500 3000
13 Treatment unit process
10 Pretreatment activities / imaging
11 Pretreatment planning process
12 Treatment data entry process
5 Communication of intent
18 Timing
9 Mould room/workshop activities
4 Referral for treatment
3 Routine machine QA
6 Booking process
Miscellaneous
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
13
Figure 11: Breakdown of the most frequently occurring level 3 (minor radiation incident) reports associated with process code 13 (treatment unit process), from December 2013 to November 2015 (n = 2690/2998 subset of reports)
Level 3 reports were also broken down by most frequently occurring process subcode (Figure 12).
The findings were consistent with those in Figure 11, with ‘on-set imaging: production process’
being the most frequently reported RTE within the minor radiation incident grouping. Of note
when compared to the 2014 report8 all of the most frequently occurring subcodes within this
classification were the same except for ‘patient positioning’ which replaces ‘setting of couch
position’.
Figure 12: Breakdown of the most frequently occurring process subcodes in level 3 (minor radiation incident) reports, from December 2013 to November 2015 (n = 2723/3994 subset of reports)
0 200 400 600 800 1000
13z On-set imaging: production process
13i Use of on-set imaging
13aa On-set imaging: approval process
13l Movements from reference marks
13bb On-set imaging: recording process
13u Use of compensators
13g Patient positioning
13cc Management of variations
13q Setting of couch position/angle
13r Use of immobilisation devices
Number of reports
0 200 400 600 800 1000
13z On-set imaging: production process
13i Use of on-set imaging
13aa On-set imaging: approval process
13l Movements from reference marks
13bb On-set imaging: recording process
13u Use of compensators
13g Patient positioning
12f Accuracy of data entry
13cc Management of variations
10j Generation of plan for approval
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
14
4.2.4 Breakdown of level 4 (near miss) RTE
A near miss is defined by TSRT as a potential radiation incident ‘that was detected and
prevented before treatment delivery’3.
Near misses comprised 28.7% (n = 3646) of the coded RTEs reported during this period.
Once again, ‘treatment unit process’ was the most common code for these reports, making up
32.2% (n = 1174) of them (Figure 13). RTEs were spread across 20 categories of process
code for level 4 classifications. A subset of these reports was grouped into ‘miscellaneous’ as
the numbers reported within the process codes were deemed statistically less significant.
Figure 13: Breakdown of level 4 (near miss) reports by process code, from December 2013 to November 2015 (n = 3646)
Further analysis of the ‘treatment unit process’ indicates the points in the pathway at which the
near misses occurred (Figure 14). A total of 34 different treatment unit process subcodes from
process code 13 are included in this classification. The top 10 most frequently occurring
processes are presented below, which made up 78.4% (921 out of 1174) of the RTEs reported
under process code 13 within this level. Pathway points of interest are focused on imaging
tasks and include ‘on-set imaging: approval process’, ‘use of on-set imaging’, ‘on-set imaging:
recording process’ and ‘on-set imaging: production process’ (Figure 14).
Level 4 reports were also broken down by most frequently occurring process subcode
(Figure 15). This revealed ‘documentation of instructions’ (15%, n = 262) and ‘accuracy of
data entry’ (15%, n = 261) as the most frequently reported RTEs within the near miss incident
grouping. Examples of RTE associated with documentation of instructions include incorrect or
missing patient set up information.
0 200 400 600 800 1000 1200
13 Treatment unit process
11 Pretreatment planning process
10 Pretreatment activities / imaging
12 Treatment data entry process
5 Communication of intent
4 Referral for treatment
6 Booking process
9 Mould room/workshop activities
7 Processes prior to first appointment
14 On-treatment review process
Miscellaneous
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
15
Figure 14: Breakdown of the most frequently occurring level 4 (near miss) reports associated with process code 13 (treatment unit process), from December 2013 to November 2015 (n = 921/1174 subset of reports)
Figure 15: Breakdown of the most frequently occurring process subcode in level 4 (near miss) reports, from December 2013 to November 2015 (n = 1741/3646 subset of reports)
0 50 100 150 200 250
13aa On-set imaging: approval process
13i Use of on-set imaging
13bb On-set imaging: recording process
13z On-set imaging: production process
13l Movements from reference marks
13h Use of IVD according to local protocol
13a Availability/timeliness of all required documentation
13cc Management of variations/unexpected events/errors
13g Patient positioning
13r Use of immobilisation devices
Number of reports
0 50 100 150 200 250 300
10j Documentation of instructions
12f Accuracy of data entry
13aa On-set imaging: approval process
13i Use of on-set imaging
13bb On-set imaging: recording process
11n Recording of patient specific instructions
11j Generation of plan for approval
11i Target and organ at risk delineation
13z On-set imaging: production process
11m Recording of definitive treatment prescription
5a Completion of request for treatment
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
16
4.2.5 Breakdown of level 5 (other non-conformance) RTE
Other non-conformance is defined by TSRT as ‘non-compliance with some other aspect of a
documented procedure but not directly affecting radiotherapy delivery’3 and made up 36.6%
(n = 4642) of those RTE reports coded.
A breakdown of level 5 reports revealed ‘pretreatment planning process’ as the most common
code for these reports, making up 22.2% (n = 1,032) of them. RTEs were spread across
20 categories of process code for level 5 classifications (Figure 16). A subset of these reports
was grouped into ‘miscellaneous’ as the numbers reported within the process codes were
deemed statistically less significant.
Figure 16: Breakdown of level 5 (other non-conformance) reports by process code, from December 2013 to November 2015 (n = 4642)
A total of 22 different pretreatment planning process subcodes have reports associated with
them in this classification. The top 10 most frequently occurring processes are presented here,
which made up 90.8% (937 of the 1,032) of the RTEs reported under process code 11 within
this level (Figure 17).
‘Management of process flow within planning’ can be seen to contribute significantly to the
number of RTEs reported. Examples of this type of RTE report included mismanagement of
changes made to plans leading to delays in planning and/or treatment.
Level 5 reports were also broken down by most frequently occurring process subcode
(Figure 18). This agreed with the above findings that ‘management of process flow within
planning’ was the most frequently reported RTE at 7.4% (n = 344) within the other non-
conformance grouping. 97 (28.2%) of these errors had secondary codes reported of which 72
(21%) elicited the error affected the ‘availability/timeliness of all required documentation’ at the
treatment unit.
0 200 400 600 800 1000 1200
11 Pretreatment planning process
13 Treatment unit process
6 Booking process
10 Pretreatment activities / imaging
5 Communication of intent
12 Treatment data entry process
4 Referral for treatment
7 Processes prior to first appointment
14 On-treatment review process
18 Timing
Miscellaneous
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
17
Figure 17: Breakdown of the most frequently occurring level 5 (other non-conformance) reports associated with process code 11 (pretreatment planning process), from December 2013 to November 2015 (n = 937/1032 subset of reports)
Figure 18: Breakdown of the most frequently occurring level 5 (other non-conformance) reports by process subcodes, from December 2013 to November 2015 (n = 1594 /4642 subset of reports)
0 50 100 150 200 250 300 350
11o Management of process flow within planning
11n Recording of patient specific instructions
11j Generation of plan for approval
11t End of process checks
11v Other
11q Timeliness of plan production
11i Target and organ at risk delineation
11m Recording of definitive treatment prescription
11k Authorisation of plan
11h Choice of technique
Number of reports
0 50 100 150 200 250 300 350
11o Management of process flow within planning
6a Bookings made according to protocol
6d Communication of appointments to patient
12f Accuracy of data entry
10j Documentation of instructions
5a Completion of request for treatment
4j Consent process
11n Recording of patient specific instructions
13bb On-set imaging: recording process
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
18
4.3 Main themes of RTE
The 12,691 RTE reports were categorised by process code or process subcode according to
TSRT and then by classification, so that the main themes could be derived.
4.3.1 Breakdown of process codes
The entire dataset was broken down by process code and classification level. 41.4%
(n = 5,254) of the RTEs reported were associated with ‘treatment unit process’ and 16.2%
(n = 2,053) occurred during ‘pretreatment planning process’. RTEs were spread across all
21 categories of process code. A subset of these reports was grouped into ‘miscellaneous’ as
the numbers reported within the process codes were deemed statistically less significant and
for this reason they are not included in Figure 19.
In this subset of data it may be seen that the majority (64.6% n = 7,821) of reports are made
up of ‘near misses’ (level 4) and ‘non-conformities’ (level 5). Minor radiation incidents (level 3)
comprised 32.2% (n = 3,895) of these reports. The remaining 3.3% (n = 394) reports were
‘reportable radiation incidents’ and ‘non-reportable radiation incidents’.
Figure 19: Breakdown of most frequently occurring process codes by classification, from December 2013 to November 2015 (n = 12110/12691 subset of reports)
4.3.2 Breakdown of process subcodes
The most frequently occurring process subcode was ‘on-set imaging: production process’,
making up 19.6% (n = 1,067) of all RTEs reported. This was followed by ‘use of on-set
imaging’, at 15.1% (n = 825), and ‘on-set imaging: approval process’, at 13.4% (n = 733). Of
note, on-set imaging processes represented 4 out of the 10 most frequently occurring process
0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000 5500
13 Treatment unit process
11 Pretreatment planning process
10 Pretreatment activities / imaging
12 Treatment data entry process
5 Communication of intent
6 Booking process
4 Referral for treatment
7 Processes prior to first appointment
18 Timing
14 On-treatment review process
Number of reports
Level 1
Level 2
Level 3
Level 4
Level 5

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
19
subcodes reported. The 10 most frequently reported subcodes and their classification levels
are presented in Figure 20.
It may be seen that the majority (52.8% n = 2,882) of reports are made up of ‘near misses’
(level 4) and ‘other non-conformities’ (level 5). In reality, the incidence of level 4 and 5 reports
is likely to be much higher as not all these events are currently reported under the national
voluntary reporting system. Minor radiation incidents (level 3) comprised 44.6% (n = 2,434) of
this subset of reports.
Figure 20: Breakdown of reports by most frequently occurring process subcode and classification level, from December 2013 to November 2015 (n = 5454/12691 subset of reports)
4.3.3 Additional process subcodes
The primary process subcode is the point in the pathway at which the RTE first occurred; each
of the 12,691 RTEs reported contained primary process codes. Each RTE can contain a
primary subcode and up to three further subcodes. Only 34.4% (n = 4,372) RTE contained a
secondary process code, indicating a second point in the pathway where the original had gone
undetected. A third process code was indicated in just 6.8% (n = 865) and a fourth in just
1.6% (n = 199) of all the RTEs. The most frequently occurring additional process subcodes
are presented in Figure 21. Departments are encouraged to consider additional process
subcodes, this allows the identification of all points in the pathway where errors occurred.
0 200 400 600 800 1000 1200
13z On-set imaging: production process
13i Use of on-set imaging
13aa On-set imaging: approval process
12f Accuracy of data entry
10j Documentation of instructions/information
13bb On-set imaging: recording process
11o Management of process flow within planning
11n Recording of patient specific instructions
13l Movements from reference marks
6a Bookings made according to protocol
Number of reports
Level 1
Level 2
Level 3
Level 4
Level 5

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
20
Figure 21: Breakdown of reports by most frequently occurring process subcodes across all four subcodes, from December 2013 to November 2015 (n = 3316/12691 subset of reports)
4.3.4 End of process checks
Owing to the complex and multifaceted nature of radiotherapy it is usual to have checking
processes in place at points in the pathway where patient data is handed over to a new part of
the pathway. Therefore the ‘end of process check’ subcode is repeated across the
radiotherapy pathway, for example following completion of ‘pretreatment activities’ or
‘pretreatment planning process’. A breakdown of all process subcodes within the dataset by
‘end of process check’ was undertaken. It includes process subcodes 9k, 10l, 11t, 12g and
13hh (Figure 22). 20.4% (n = 883) of the ‘end of process check’ RTEs reported were
associated with ‘treatment unit process’, of these 56.6% (n = 500) were associated with on-set
imaging.
A total of 20.4% (n = 2,584) of the RTEs reported were not captured during the ‘end of
process checks’. This would seem to suggest that the ‘end of process checks’ are failing to
detect RTEs in some cases. At time of writing it is understood ‘pause and check’ work is
underway to replicate the work of the operator checklist within clinical imaging15
for
radiotherapy departments.
0 200 400 600 800 1000
(13hh) End of process checks (treatment unit)
(11t) End of process checks (pretreatment planning)
(12g) End of process checks (treatment data entry)
(10l) End of process checks (pretreatment activities)
(13z) On-set imaging: production process
(13i) Use of on-set imaging
(13a) Availability/timeliness of all required documentation
(13l) Movements from reference marks
(13cc) Management of variations/unexpected events/errors
(13aa) On-set imaging: approval process
(12f) Accuracy of data entry
Number of reports

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
21
Figure 22: Breakdown of end of process checks by point in the radiotherapy pathway, from December 2013 to November 2015 (n = 2584)
4.4 Inspectorate data
There is a requirement that the appropriate authority is notified of all level 1 incidents13
. The
inspectorates for IR(ME)R for England, Wales, Northern Ireland and Scotland were
approached and asked to share their anonymised synopsis of closed reportable radiation
incidents from the same time period as for the voluntary system for this report.
A total of 437 reports were shared, this is a vast increase in numbers since the last report
where 103 reports were shared for the same period of time8. This increase may be due to
guidance notes published in 201216
. There were 232 level 1 reports received through the
voluntary scheme, this highlights a difference in the number of reports reported to the
appropriate authorities and the voluntary reporting and learning scheme.
The coding from TSRT3 was applied to these reports. On review of the inspectorate data it
became clear that there was wide variation on the locally applied classification of events, it
was found that 17.8% (n = 78) of the reported events could have also been reported as level 2
(non-reportable radiation incidents) or level 3 (minor radiation incidents).
Of the 437 level 1 RTE reports shared, 47.1% (n = 206) occurred during ‘treatment unit
process’ and 25.4% (n = 111) during ‘pretreatment activities’. A comparison of inspectorate
and voluntary data (Figure 23) revealed a similar pattern of spread in the higher frequency
reports. Interestingly reports associated with process codes ‘new equipment’, ‘routine machine
QA’, ‘booking process’, ‘follow up process’ and ‘document management’ were reported in the
inspectorate data, but not within the voluntary data. These outliers were deemed as
9k Mouldroom activities, 1%
10l Pretreatment activities , 15%
11t Pretreatment planning process,
27% 12g Treatment
data entry process, 23%
13hhTreatment unit process, 34%

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
22
statistically less significant and grouped as miscellaneous. The text descriptors for the
inspectorate data was more detailed than the voluntary data, which may explain this difference
in coding.
Figure 23: Percentage frequency of process codes found in reportable radiation incidents from the inspectorate and voluntary datasets, from December 2013 to November 2015 (n = 437 and 232, respectively)
Further analysis of the treatment unit process indicates the points in the pathway at which the
reportable radiation incidents most commonly occurred (Figure 24). ‘Movements from
reference marks’ formed 21.4% (n = 44) of the treatment unit inspectorate data, which is
similar to the 21.6% (n = 25) from the voluntary data.
Figure 24: Breakdown of inspectorate and voluntary data as a percentage of most frequently occurring reportable radiation incident reports within process code 13 (treatment unit process), from December 2013 to November 2015 (n = 174/206 and 91/116, respectively)
0 5 10 15 20 25 30 35 40 45 50
13 Treatment unit process
10 Pretreatment activities
5 Communication of intent
11 Pretreatment planning process
4 Referral for treatment
12 Treatment data entry process
15 Brachytherapy
9 Mould room/workshop activities
Miscellaneous
Percentage of reports
Voluntary data
Inspectorate data
0 5 10 15 20 25
(13l) Movements from reference marks
(13z) On-set imaging: production process
(13k) ID of reference marks
(13aa) On-set imaging: approval process
(13q) Setting of couch position/angle
(13c) Patient data ID process
(13g) Patient positioning
(13ff) Recording of delivered treatment data
(13i) Use of on-set imaging
(13w) Availability of treatment accessories
Percentage of reports
Voluntary data
Inspectorate data

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
23
The inspectorate data was also broken down by most frequently occurring process subcode.
This revealed treatment ‘movements from reference marks’ (10.1% n = 44) and pretreatment
‘localisation of intended volume’ (10.8% n = 41) were the most frequently occurring process
subcodes within the inspectorate data (Figure 25). ‘Movements from reference marks’ also
accounted for the most frequently occurring process subcodes within the level 1 voluntary
data, this was followed by localisation of intended volume’ and ‘on set imaging production
process’.
Figure 25: Breakdown of inspectorate and voluntary data as a percentage of most frequently occurring process subcodes, from December 2013 to November 2015 (n = 248/437 and 121/232, respectively)
A total of 67.0% (n = 293) of the inspectorate reports contained further process subcodes,
highlighting further points in the pathway where the error went undetected. Of these 54.9%
(n = 161) RTEs were not captured during the ‘end of process checks’.
5 Discussion
5.1 Increase in RTE reporting
During this two year reporting period there has been a large increase in the number of RTEs
reported to the national voluntary reporting system. A total of 12,691 reports were included in
this analysis for the period December 2013 until November 2015, compared with 7,655 for the
2014 report8 and 3,316 for the 2012 report
7. This is an increase in reporting levels of 66%
since 2014 report8and 282% since the 2012 report
7.
The number of providers contributing to this initiative has increased from the previous two year
report published in 20148 with an average of 28 providers reporting per month to an average
of 42 per month for this reporting period.
0 2 4 6 8 10 12
(13l) Movements from reference marks
(10c) Localisation of intended volume
(10f) Production of images demonstrating correct detail
(13z) On-set imaging: production process
(13k) ID of reference marks
(10b) Positioning of patient
(5a) Completion of request for treatment
(13aa) On-set imaging: approval process
(13q) Setting of couch position/angle
Percentage of reports
Voluntary data
Inspectorate data

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
24
The overall increase in voluntary reporting indicates a mature reporting culture. The increase
in providers contributing also demonstrates the radiotherapy community’s commitment to
maximise learning from these events to minimise the frequency of their occurrence in the
future.
Since November 2013 data has been collated, analysed and reported for the UK as a whole.
This and the increase in the average number of providers participating in this initiative may
explain the increase in RTE reporting. However, there is still some variation in the frequency
of reporting, this is shown in the increase in the average lag time from 49 days in the 2014
report8 and 58.8 days in this reporting period. To ensure timeliness of learning providers are
encouraged to report on a monthly basis.
Data received from NATCANSAT17
shows that activity for radiotherapy providers has also
increased slightly during this reporting period. Using the NATCANTSAT data for England UK-
wide data was extrapolated. An estimated 313,876 episodes of radiotherapy were delivered
during the period from December 2013 until November 2015 compared with 308,730 from the
2014 report8. Each episode is made up of multiple visits ranging 1 to 37. It should also be
noted that each episode of radiotherapy may consist of several prescriptions treated
consecutively and/ or concurrently. RTEs were detected and reported to the national voluntary
reporting scheme in 4.0% of episodes, which is an increase from 2.5% in the 2014 report8.
During this reporting period an estimated 397,402 prescriptions were delivered, compared to
413,730 prescriptions in the previous reporting period. RTEs were detected in 3.2% of
prescriptions, which is an increase from 1.9% during the last reporting period8. This decrease
in prescriptions and increase in activity may be due to an increase in complex radiotherapy
and hypofractionation regimes.
This increase in percentage of RTEs in relation to activity should be interpreted carefully and
reflects a maturing reporting culture.
Treatment unit process associated RTEs made up 41.4% (n = 5254) of all RTEs, an estimated
15,001,416 treatment exposures were delivered. A treatment exposure is the delivery of one
radiotherapy treatment field, this does not include imaging exposures. Treatment process
RTEs were detected in 0.03% of treatment exposures.
Further increases in the number of RTE reports submitted to the national voluntary reporting
system are expected as service provision increases and as providers develop full electronic
reporting solutions and reporting mechanisms are further streamlined.
5.2 Classification level of RTE
The vast majority of the RTE reports were of lower level events, thus not affecting the
outcome of patient care. Of the level 1 and 2 incidents reported, it is known the majority of
them affected only one fraction of a course of treatment. This meant that corrective action
could be taken over the remaining treatment fractions so the incident did not have a significant
impact on the patient or the outcome of their treatment.
This was similar to the trend seen in each of the previous biennial reports. A small number of
higher level incidents and a much greater number of lower level incidents is consistent with
findings in the literature. It is known that for every level 1 ‘reportable radiation incident’ that
occurs, many lower level incidents are also seen. Heinrich illustrated this point in 19313
(Figure 26), it may be seen that as the severity of an incident decreases, the probability of its

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
25
occurrence increases. The distribution of data in Figure 27, which shows a breakdown of the
entire dataset by classification, supports this theory.
Figure 26: Heinrich’s triangle (reproduced from Towards Safer Radiotherapy3)
Figure 27: Classification levels as a percentage of RTE reports across the four two-year reports, from December 2007 to November 2015
When compared with results from the 20148 report there has been no overall change in the
percentage of reportable (1.7% in 2014 and 1.8% in 2016) and non-reportable radiation
incidents (1.3% in 2014 and 1.4% in 2016). Although the percentage of level 1 RTEs has
remained similar since the last analysis in 2014 the number of reportable radiation incidents
has increased significantly (n = 128 in 2014 and n = 232 in 2016) with a slight increase in
0 5 10 15 20 25 30 35 40 45
5 Other non-conformance
4 Near miss
3 Minor radiation incident
2 Non-reportable radiation incident
1 Reportable radiation incident
Percentage of reports
2010 (n=680)
2012 (n=3316)
2014 (n=7655)
2016 (n=12691)

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
26
activity. Further analysis of the raw data indicates that this increase can be attributed to the
increase in reporting of pre-treatment and verification imaging exposure related RTEs to the
inspectorates.
There has been a slight increase in the percentage of minor radiation incidents from 28.6% in
2014 to 31.5% in 2016. There has been an overall decrease in the percentage of other non-
conformances (41.6% in 2014 and 36.6% in 2016). This might be explained in it is known that
clinical departments with limited resource are more likely to submit reports on higher level
RTEs such as level 1 ‘reportable radiation incident’, level 2 ‘non-reportable radiation incident’
and level 3 ‘minor radiation incident’18
only.
TSRT3 stated that root cause analysis of minor and near miss RTE events has been shown to
provide valuable lessons which can prevent serious incidents. Therefore to investigate this
theory in more detail the PSRT is committed to the collation of all levels of RTE events and
their inclusion in the analysis for promulgation to the radiotherapy community. Clinical
departments are encouraged to continue reporting all levels of RTE to facilitate this process.
5.2.1 Level 1 (reportable radiation incident) RTE
The spread of the level 1 RTE reports across process coding was similar to findings in the
2014 report8 with seven of the same process codes. An increase from 43.0% to 50.0% in
reports from ‘treatment unit processes’ has been seen. Whilst the contribution of the subcode
‘movements from reference marks’ remained comparable (10.9%, 2014 and 10.8%, 2016) the
subcode ‘on-set imaging: production process’ which accounted for 7.3% (n = 17) of level 1
errors in the 2016 report was not reported as a frequently occurring subcode in the 2014
report8. The increase in the process subcode ‘on-set imaging: production process’ may
explain the increase in treatment unit related reports.
5.2.2 Level 2 (non-reportable radiation incident) RTE
The spread of these RTE reports across process coding was similar to findings in the 2014
report8 with the seven most frequent process codes being the same for this subgroup.
‘On-set imaging: approval process’ was notably the most frequently occurring event at 16.3%
(n = 29), followed by ‘movements from reference marks’ (6.7%, n = 12) within the subset of
non-reportable radiation incidents. The 2014 report8 presented these two subcodes as equally
the most frequent subcodes each at 9.7% (n = 10).
5.2.3 Level 3 (minor radiation incident) RTE
The spread of RTE reports across process coding was consistent with findings in the 2014
report8 for this subgroup. ‘Treatment unit process’ was the most common code for these
reports, at 75.1% (n = 2,998).
The 2014 report8 presented the most frequently reported event within this subset of minor
radiation incidents as ‘On-set imaging: production process’ (13.8%, n = 302), this percentage
has increased to 23.1% (n = 922) within this reporting period. A review of the ‘on-set imaging
production process’ subset of RTE reports revealed that 48.9% (n = 451) related to procedural
failures and the remaining 51.1% (n = 471) of this subgroup related to equipment failure, this
is a decrease in percentage from the 2014 report8 where 61.2% (n = 185) were due to
equipment failure.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
27
Of note when compared to the 2014 report8, all of the most frequently occurring subcodes
within this classification were the same, apart from ‘patient positioning’ which replaces ‘setting
of couch position’.
It should be noted that equipment failure reports should be reported to local engineers, the
manufacturers and the MHRA, as appropriate. Equipment failure adverse incidents above the
threshold levels set out in PM7719
should continue to be reported to the Health and Safety
Executive (HSE). It would seem the errors reported in this subset are spread across
manufacturers and varied in type. Consideration should be given to undertaking a risk
assessment in the case of a frequently recurring fault, especially where no resultant image
acquisition is achievable to inform the treatment process as to whether imaging on that device
should continue.
5.2.4 Level 4 (near miss) RTE
Once again the spread of reported RTEs across process codes is consistent with the 2014
report8, ‘treatment unit process’ was the most common code for these reports, making up
32.2% (n = 1174).
Although treatment unit process was the most common code for these reports, the most
frequently occurring process subcodes were ‘documentation of instructions’ (7.2%, n = 262)
and ‘accuracy of data entry’ (7.2%, n = 261), the latter was also the most frequently reported
subcode presented within the near miss incident grouping in the 2014 report8
(9.3%, n = 191).
5.2.5 Level 5 (other non-conformance) RTE
‘Pretreatment planning process’ was the most common code for these reports making up
22.2% (n = 1,032) of them, this percentage is similar to the 2014 report8 where 20.0% (n =
638) were associated with pretreatment planning process.
The most frequently reported RTE within this classification was associated with ‘management
of process flow within planning’ at 7.4% (n = 344), this was followed by ‘bookings made
according to protocol’ at 5.0% (n = 233). This is a slight change from the 2014 report8 where
‘consent process’ was the most frequently reported RTE within this classification with 5.6% (n
= 177) followed by management of process flow within planning at 3.9% (n = 125).
5.3 Main themes
Analysis of the RTE reports demonstrates that generation of error is not confined to one
professional group or to any particular point in the pathway. It also indicates that the pattern of
errors is replicated across service providers in the UK.
5.3.1 Breakdown of process codes
Consistent with previous reports RTEs were spread across all 21 categories of process codes,
treatment unit process codes were the most frequently reported RTE (41.4%, n = 5,254). This
is to be expected as some radiotherapy treatments may span a number of visits, providing
many opportunities during the treatment unit process for RTE to occur. RTEs attributed to
treatment unit processes have increased from 33.5% (n = 2,568) in the 2014 report8 to 41.4%
(n = 5,254) within this reporting period. This may be due to a continued increase in the use of
imaging and imaging associated RTEs. Radiotherapy is evolving and the increase in RTE

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
28
associated with treatment unit process may continue due to the uptake in complex techniques
and adaptive radiotherapy20
.
5.3.2 Breakdown of process subcodes
The following processes have been identified as areas in the radiotherapy pathway where
RTEs frequently occur:
on-set imaging: production process (13z)
use of on-set imaging (13i)
on-set imaging: approval process (13aa)
accuracy of data entry (12f)
documentation of instructions/information (10j)
on-set imaging: recording process (13bb)
management of process flow within planning (11o)
recording of patient specific instructions (11n)
movements from reference marks (13l)
bookings made according to protocol (6a)
Guidance has already been published on how to minimise all of these frequently occurring
RTEs in the periodic newsletter Safer Radiotherapy through the ‘error of the month’ column,
as some of these trends were noted in the quarterly analyses6.
When compared with the 2014 two-year report8 a change in error trends can be seen. This
reinforces the need for a cyclical approach to reporting, analysis and timely sharing of learning
from these events. Eight of the same process subcodes were found in the most frequently
reported list in both the current and 2014 analyses, seven of these were also within the 2012
analyses. These ranked differently between analyses, as shown in Table 2.
‘Consent process’ and ‘generation of plan for approval’ did not appear in the most frequently
reported process subcode list in the current analysis. These were replaced by ‘bookings made
according to protocol’ and ‘management of process flow within planning’. This change may be
due to the increasing complexity of booking appointments and the management of workflow
throughout a department.
The most frequently occurring process subcode was ‘accuracy of data entry’ in the 2014
report8. Within this reporting period this is now the fourth most frequently occurring subcode,
this may be due to a change towards paper-light or electronic working and a reduction in
transcription. On-set imaging processes represented 4 out of the 10 most frequently occurring
process subcodes reported. This rise in ‘on-set imaging processes’ related reports may reflect
the increased uptake in on-set imaging due to its further availability and the recognition of its
preventive role in minimising geographical displacement during treatment21
. In addition, it is
likely that error rates might be higher as new techniques and technologies are adopted locally
in this field.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
29
Table2. Comparison of most frequently reported process subcodes in 2012, 2014 and 2016 report trends.
Process subcode
Number of reports
Percentage of reports
Increase 13z On-set imaging: production process 2012 109 3.3%
2014 366 4.8%
2016 1067 8.4%
13i Use of on-set imaging 2012 65 2.0%
2014 302 3.9%
2016 825 6.5%
10j Documentation of instructions/information 2012 120 3.6%
2014 295 3.9%
2016 528 4.2%
13bb On-set imaging: recording process 2012 74 2.2%
2014 222 2.9%
2016 463 3.6%
Decrease 13l Movements from reference marks 2012 130 3.9%
2014 226 3.0%
2016 313 2.5%
12f Accuracy of data entry 2012 188 5.7%
2014 387 5.1%
2016 543 4.3%
Neither 11n Recording of patient specific instructions 2012 80 2.4%
2014 223 2.9%
2016 336 2.6%
13aa On-set imaging: approval process 2012 194 5.9%
2014 343 4.5%
2016 733 5.8%
5.3.3 End of process checks
‘End of process checks’ are one form of safety barrier in error detection and, as such should
include safety-critical elements of the pathway. By their very nature they should be clearly
defined within local protocols with appropriately trained staff clearly assigned to undertake
these duties and their results should be clearly recorded3. The frequency and effectiveness of
checking and verifying procedures should be audited to ensure they are of value.
Not all RTE report submissions include secondary or subsequent process coding, so the
reported 20.4% (n = 2,584) of RTE including ‘end of process checks’ where points in the
pathway at which the RTE has gone undetected may be higher than those reported. This is a
slight percentage increase in the findings of the 2014 report8 where 17.9% (n = 1,369) RTE
included end of process checks.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
30
5.4 Inspectorate data
A total of 437 reports were shared by the inspectorates compared to 232 received through the
voluntary reporting system. The incongruity between the numbers of level 1 reports received
by the inspectorates and the voluntary reporting system may be explained by several factors.
Firstly only anonymised and closed events were shared by the inspectorates, some of which
could also have been reported to the voluntary scheme as lower level incidents. Secondly
data from the inspectorate for IRR9914
is not included nor are independent sectors. Finally
there is a greater time lag in submitting RTEs to the voluntary reporting scheme than to the
inspectorates.
Similar to the level 1 ‘reportable radiation incident’ reports received through the voluntary
reporting scheme, ‘movements from reference marks‘ emerged as the most common process
subcode. This was the jointly the most common process subcode within the inspectorate data
shared in the 2014 report8.
6 Conclusion
When the opportunity for error is weighed against the incidence of error, radiotherapy may be
seen as a safe form of treatment for cancer. Although RTEs are rare, when they do occur the
consequences can be significant so it is essential the radiotherapy community does not
become complacent about the associated risks.
The overall increase in voluntary reporting indicates a maturing reporting culture. It also
demonstrates the radiotherapy community’s commitment to maximise learning from these
events and to minimise the frequency of their occurrence in the future. A further increase in
the number of RTE reports submitted to the national voluntary reporting scheme is expected,
as more electronic systems are locally commissioned to enable streamlining of submission of
RTE at all levels. Clinical departments are encouraged to submit all levels of RTEs.
Use of the terminology, classification and coding of TSRT, together with implementation of the
national voluntary reporting system described within this report, allows clinical departments to
compare their local analysis to the national picture. In this, the first two-year report that
includes RTE reports from across the UK, it can be seen that with the addition of data from
Northern Ireland and Scotland the error trends in the types of RTE reported remain consistent.
This would suggest that the types of RTE that occur across the UK are consistent.
This report has identified errors in activities undertaken by various professional groups,
throughout the patient pathway and across different service providers. A total of 41.4%
(n = 5,254) of the RTEs reported were associated with ‘treatment unit process’ and 16.2%
(n = 2,053) occurred during ‘pretreatment planning process’. RTEs were spread across all
21 categories of process code. The vast majority of reports were categorised as lower level
events, thus not affecting the outcome of patient care.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
31
In this analysis the following processes have been identified as areas in the radiotherapy
pathway where RTEs commonly occur:
on-set imaging: production process (13z)
use of on-set imaging (13i)
on-set imaging: approval process (13aa)
accuracy of data entry (12f)
documentation of instructions/information (10j)
on-set imaging: recording process (13bb)
management of process flow within planning (11o)
recording of patient specific instructions (11n)
movements from reference marks (13l)
bookings made according to protocol (6a)
Guidance has already been published on how to minimise all of these frequently occurring
RTEs in the quarterly newsletter Safer Radiotherapy through the ‘error of the month’ column,
as some of these trends were noted in the routine analyses6.
When compared with the 2014 two-year report8 a slight change in error trends can be seen.
Eight of the same process subcodes were found in the most frequently reported list in both the
current and 2014 analyses, seven of these were also within the 2012 analyses. These ranked
differently between analyses.
In addition, when compared with results from the 20148 report there has been no overall
change in the percentage of reportable (1.7% in 2014 and 1.8% in 2016) and non-reportable
radiation incidents (1.3% in 2010 and 1.4% in 2016). However there has been a slight
increase in the percentage of minor radiation incidents from 28.6% in 2014 to 31.5% in 2016.
There has been an overall decrease in the percentage of other non-conformances (41.6% in
2014 and 36.6% in 2016). It is known that clinical departments are more likely to submit
reports on higher level RTEs such as level 1 ‘reportable radiation incident’, level 2 ‘non-
reportable radiation incident’ and level 3 ‘minor radiation incident’18
.
It is imperative that RTE trends continue to be reported, analysed and monitored on a cyclical
basis, in order to inform ongoing safe and effective radiotherapy practice. This is especially
pertinent as new techniques and technologies are implemented and as new clinical
radiotherapy departments are established. This work supports a risk based approach to
improving safety both locally and nationally and indicates a culture that is open, transparent
and already present in the UK radiotherapy community.

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
32
7 Key recommendations
a) Radiotherapy departments across the UK should continue to use TSRT to classify and
code all of their RTEs, including near misses for local analysis to inform policy and
practice
b) Radiotherapy departments across the UK should continue to submit coded and classified
RTE reports to the national voluntary reporting system using the mechanisms identified
within this report
c) To ensure timeliness of learning providers are encouraged to report on a monthly basis
d) Radiotherapy departments across the UK should consider all codes when coding RTE
and the use of secondary or additional subcodes
e) PSRT should continue to develop analysis of the reports, with regular dissemination of
findings to the radiotherapy community for group learning
f) The data should be used both by the PSRT and by individual radiotherapy departments as
part of a risk-based approach to allocating resources for improving patient safety in
radiotherapy and to inform audit and research
g) The mechanism to enable departments in Scotland and Northern Ireland to submit RTE
reports to PHE for collation and analysis as part of a UK dataset should be further refined
h) A mechanism should be developed to enable independent radiotherapy providers to
submit RTE reports to PHE for collation and analysis as part of a UK dataset
i) The radiotherapy pathway coding as described in TSRT should be refined to reduce any
ambiguity of codes and to reflect the use of emerging techniques and technologies, this
should include safety barriers and causative factor taxonomies.
j) Radiotherapy departments across the UK should consider reviewing their end of process
checks and consider safety critical elements of the pathway

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
33
8 Acknowledgements
National Clinical Analysis and Specialised Applications Team (NATCANSAT)
National Reporting and Learning System (NRLS)
NHS Radiotherapy Providers across the UK
Inspectorates for IR(ME)R
9 PSRT Steering Group Membership
Helen Best (Public Health England)
Martin Duxbury (Society and College of Radiographer’s Clinical Representative –
Deputy Head of Radiotherapy, St James Institute of Oncology, Leeds)
Úna Findlay (Public Health England and Group Chair)
Leslie Frew (Institute of Physics and Engineering in Medicine – Head of Radiotherapy Physics
Service, Belfast City Hospital)
Maria Murray (Society and College of Radiographers – Professional Officer for Scotland and
UK Radiation Protection Lead)
Tony Murphy (Lay Representative)
Madeleine Ottrey (Public Health England)
Tom Roques (Royal College of Radiologists – Consultant Clinical Oncologist and Clinical
Director for Oncology and Haematology, Norfolk and Norwich University Hospital NHS
Foundation Trust)
Carl Rowbottom (Institute of Physics and Engineering in Medicine – Head of Physics, The
Clatterbridge Cancer Centre NHS Foundation Trust)

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
34
10 References
1. World Health Organization. Reporting and learning for patient safety. Available at
http://www.who.int/patientsafety/implementation/reporting_and_learning/en/
2. Radiotherapy: Hidden Dangers. Chapter 5. Chief Medical Officer’s Annual Report 2006 (2007). Available at
webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/An
nualReports/DH_076817 3. RCR, SCoR, IPEM, NPSA, BIR. Towards Safer Radiotherapy. Royal College of Radiologists, Society and College of
Radiographers, Institute of Physics and Engineering in Medicine, National Patient Safety Agency, British Institute of Radiology. Royal College of Radiologists, London (2008). Available at www.rcr.ac.uk/towards-safer-radiotherapy
4. Francis R. Report of the Mid Staffordshire NHS Foundation Trust public enquiry. HMSO, London (2013). Available at
www.gov.uk/government/publications/report-of-the-mid-staffordshire-nhs-foundation-trust-public-inquiry
5. PSRT. Patient Safety in Radiotherapy Steering Group Activity (November 2007 – March 2010). Data report on patient
safety incidents from August 2007 until November 2009. 2010. HPA-CRCE-002 (2010). Available at
www.gov.uk/government/publications/radiotherapy-errors-and-near-misses-data-report
6. PHE. Safer Radiotherapy: Radiotherapy Newsletter of PHE (previously of the HPA) and Supplementary Data Analysis:
Full Quarterly Radiotherapy Error Data Analysis. Nos 1–19. Available at www.gov.uk/government/publications/safer-
radiotherapy-error-data-analysis-report
7. PSRT. Data report on radiotherapy errors and near misses (December 2009 – November 2011). HPA-CRCE-035
(2012). Available at www.gov.uk/government/publications/radiotherapy-errors-and-near-misses-data-report
8. PSRT. Data report on radiotherapy errors and near misses (December 2011 – November 2013). PHE-CRCE-016 (2014). Available at www.gov.uk/government/publications/radiotherapy-errors-and-near-misses-data-report
9. NPSA. Definition of a patient safety incident (PSI). Available at www.npsa.nhs.uk/nrls/reporting/what-is-a-patient-safety-incident/
10. NRLS. Quarterly Data Workbook up to March 2015. Available www.nrls.npsa.nhs.uk/resources/collections/quarterly-data-summaries/?entryid45=135507
11. NPSA. Implementing Towards Safer Radiotherapy: guidance on reporting radiotherapy errors and near misses effectively. Available at www.nrls.npsa.nhs.uk/resources/clinical-specialty/radiology-and-radiotherapy/
12. PHE. Supplementary Guidance Series: Good Practice in Radiotherapy Error Reporting. Nos 1–4. Available at
www.gov.uk/government/publications/radiotherapy-good-practice-in-error-reporting
13. The Ionising Radiation (Medical Exposure) Regulations (2000). The Stationery Office, London. SI 2000/1059. Available
at www.opsi.gov.uk/si/si2000/20001059.htm. The Ionising Radiation (Medical Exposure) Regulations (Northern Ireland)
(2000) The Stationery office, London NISR 2000/194. Available at www.legislation.gov.uk/nisr/2000/194/contents/made
The Ionising Radiation (Medical Exposure) (Amendment) Regulations (2006). The Stationery Office, London. SI
2006/2523. Available at www.opsi.gov.uk/si/si2006/20062523.htm The Ionising Radiation (Medical Exposure)
(Amendment) Regulations (Northern Ireland) 2010. The Stationery office, London NISR 2010/29. Available at
http://www.legislation.gov.uk/nisr/2010/29/contents/made and the Ionising Radiation (Medical Exposure) (Amendment)
Regulations (2011). The Stationery Office, London. SI 2011/1567. Available at
www.legislation.gov.uk/uksi/2011/1567/introduction/made
14. The Ionising Radiations Regulations (1999). The Stationery Office, London. SI 1999/3232. Available at
www.opsi.gov.uk/si/si1999/19993232.htm
15. Pause and check, SCoR Available at www.sor.org/sites/default/files/sor_pause_check_a2.pdf
16. DOH. Information on IRMER (2000) available
at www.gov.uk/government/uploads/system/uploads/attachment_data/file/329842/Medical_exposures.pdf
17. Natcansat www.natcansat.nhs.uk/ 18. PSRT. Safer radiotherapy: supplementary survey analysis. Report 3 (2014). Available at
www.gov.uk/government/publications/safer-radiotherapy-supplementary-survey-analysis
19. HSE. Equipment used in connection with medical exposure. Guidance Note PM77 (3rd ed) (2006). Available at
www.hse.gov.uk/pubns/guidance/pm77.pdf
20. Cancer research UK and NHS England. Vision for radiotherapy 2014-2024. (2014) available at
www.cancerresearchuk.org/sites/default/files/policy_feb2014_radiotherapy_vision2014-2024_final.pdf
21. National Radiotherapy Implementation Group. Image Guided Radiotherapy. Guidance for implementation and use.
National Cancer Action Team (2012). Available at www.sor.org/sites/default/files/document-
versions/National%20Radiotherapy%20Implementation%20Group%20Report%20IGRT%20Final.pdf

Appendix A
35
Appendix A Radiotherapy error classification grid
Reproduced from Towards Safer Radiotherapy3
No
No
Potentially or
actually clinically
significant?
Radiotherapy error
Yes No
Yes
No Yes
Yes
Correctable
radiation
incident?
Level 1
Reportable radiation
incident
Level 2
Non-reportable
radiation incident
Level 3
Minor radiation
incident
Level 4
Near miss
Level 5
Other non-
conformance
Potential for
radiation
incident?
Radiation
incident?
Reportable?
Yes
No

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
36
Appendix B Radiotherapy pathway coding
Reproduced from Towards Safer Radiotherapy3
Process code Activity code
0 Scientific infrastructure
0a Implementation of national and international codes of practice for radiation dosimetry
0b Development of dosimetry algorithms for local application
0c Development of treatment planning algorithms for local application
0d Other
Equipment-specific activities
1 Room design
1a Patient safety
1b Staff and public safety
1c Environmental controls
1d Access control
1e Other
2 New equipment
2a Installation
2b Manufacturer’s tests
2c Acceptance tests
2d Critical examination under IRR99
2e Customisation and configuration of equipment
2f Commissioning
2g Data recording
2h Preparation of data files for planning computers
2i Other
3 Routine machine QA
3a Daily consistency checks – geometric parameters
3b Daily consistency checks – dosimetric calibration
3c Daily consistency checks – safety (IRR compliance)
3d Daily verification of accuracy of data transfer between TPS, R&V system and treatment
equipment
3e Planned QA programme checks – geometric parameters
3f Planned QA programme checks – dosimetric calibration
3g Planned QA programme checks – safety (IRR compliance)
3h Planned QA programme checks – image quality parameters (including CT, MR, portal,
cone-beam, film processor)
3i Regular preventative maintenance and repair programme
3j Handover of radiotherapy equipment after planned QA and maintenance
3k Routine radiation safety checks
3l Other

Appendix B
37
Process code Activity code
Patient-specific activities
4 Referral for treatment
4a Identification of patient
4b Verification of diagnosis/extent/stage
4c Choice of dose
4d Choice of modality
4e Choice of energy
4f Choice of fractionation
4g Choice of start date
4h Consideration of patient condition/co-morbidities
4i Choice of other interventions and their sequencing
4j Consent process
4i Other
5 Communication of intent
5a Completion of request for treatment (paper/electronic)
5b Recording of patient ID
5c Completion of required demographics
5d Completion of tumour-specific information
5e Completion of radiation-specific information
5f Completion of details of other professionals
5g Completion of administrative data
5h Recording of previous treatment details
5i Recording of patient’s specific requirements
5j Recording of non-standard information/protocol variations
5k Authorisation to irradiate (IR(ME)R)
5l Other
6 Booking process (pretreatment and treatment)
6a Bookings made according to protocol
6b Bookings made according to request details
6c Recording of booked appointments
6d Communication of appointments to patient
6e Other
7 Processes prior to first appointment
7a New patient: registration with healthcare organisation’s PAS
7b New patient: registration with department PAS
7c New patient: generation of notes
7d Old patient: location of healthcare organisation’s notes
7e Old patient: location of department notes/previous treatment details
7f Availability of reports/imaging required by protocol for treatment
7g Availability of consent documentation

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
38
Process code Activity code
7h Other
8 Pretreatment: preparation of patient
8a Confirmation of ID
8b Confirmation of consent
8c Confirmation of fertility/pregnancy status
8d Advice on procedure
8e Other
9 Mould room/workshop activities
9a Confirmation of ID
9b Pre mould room diagnostics/interventions
9c Production of immobilisation devices
9d Checking/fitting of immobilisation devices
9e Production of other accessories/personalised beam shaping device
9f Checking of other accessories/personalised beam shaping device
9g Labelling of mould room/workshop outputs
9h Recording of information in patient record
9i Instructions to patient
9k End of process checks
9l Other
10 Pretreatment activities/imaging (to include CT, simulation, clinical mark-up)
10a Confirmation of ID
10b Positioning of patient
10c Localisation of intended volume
10d Production of images using correct imaging factors
10e Production of images using appropriate field sizes
10f Production of images demonstrating correct detail
10g Labelling of images
10h Saving of planning geometry data
10i Recording of radiation data
10j Documentation of instructions/information
10k Marking of patient or immobilisation device
10l End of process checks
10m Identification of staff
10n Other
11 Pretreatment planning process
11a Verification of patient ID to include all patient data, imaging etc
11b Recording of patient ID on plan
11c Importing of data from external administrative sources
11d Importing of data from external imaging sources
11e Choice of data

Appendix B
39
Process code Activity code
11f Choice of dose and fractionation inputs
11g Availability of source data
11h Choice of technique
11i Target and organ at risk delineation
11j Generation of plan for approval (to include DVH etc as app.)
11k Authorisation of plan
11l Verification of plan/identification of responsible staff
11m Recording of definitive treatment prescription
11n Recording of patient specific instructions
11o Management of process flow within planning
11p Management of authorisation process
11q Timeliness of plan production
11r Calculation process for non-planned treatments
11s Calculation checking process for non-planned treatments
11t End of process checks
11u Identification of responsible staff
11v Other
12 Treatment data entry process
12a Pre-data entry verification
12b Choice of data entry method (input vs transcription)
12c Use of correct data
12d Correct ID of patient/all patient input data
12e Correct ID of patient output data
12f Accuracy of data entry
12g End of process checks
12h Identification of responsible staff
12i Other
13 Treatment unit process
13a Availability/timeliness of all required documentation
13b Patient ID process
13c Patient data ID process
13d Explanation/instructions to patient
13e Confirmation of pregnancy/fertility status
13f Assessment of patient prior to treatment
13g Patient positioning
13h Use of IVD according to local protocol
13i Use of on-set imaging
13j Transfer of marks
13k ID of reference marks
13l Movements from reference marks
13m Setting of treatment machine parameters

Radiotherapy Errors and Near Misses Data Report (December 2013 to November 2015)
40
Process code Activity code
13n Setting of collimator angle
13o Setting of jaw position
13p Setting of asymmetry
13q Setting of couch position/angle
13r Use of immobilisation devices
13s Use of beam shaping devices
13t Use of beam direction aids/applicators
13u Use of compensators
13v Use of wedges
13w Availability of treatment accessories
13x Setting of energy
13y Setting of monitor units
13z On-set imaging: production process
13aa On-set imaging: approval process
13bb On-set imaging: recording process
13cc Management of variations/unexpected events/errors
13dd Communication between treatment unit and V&R
13ee Recording of patient attendance
13ff Recording of delivered treatment data
13gg Recording of additional information
13hh End of process checks
13ii Identification of responsible staff
13jj Other
14 On-treatment review process
14a On-treatment review of patient according to protocol by RT staff
14b On-treatment review of patient according to protocol by other professional
14c On-treatment review of notes/data to according protocol
14d Actions following on-treatment review
14e Other
15 Brachytherapy
15a Ordering of sources
15b Delivery of sources
15c Source calibration
15d Sterility of sources
15e Correct applicators/sources
15f Correct theatre equipment
15g Initial positioning of applicators/sources
15h Planning of treatment
15i Maintenance of position of applicators/sources
15j Removing of applicators/sources
15k Other

Appendix B
41
Process code Activity code
16 End of treatment process
16a Communication of appropriate end of treatment information to patient
16b Recording of treatment summary information in notes
16d Communication of information to referring clinician/GP/CNS etc
16e Organisation of follow-up appointment to protocol
16f Communication of follow-up to patient
16g Other
17 Follow-up process
17a Follow-up consultation and documentation
17b Management of non-attendance
17c Archiving of details of treatment
Other activities contributing to protocol violations
18 Timing
18a Timing of chemo/irradiation
18b Transport issues
18c Portering issues
19 Document management
19a Availability of current protocol documentation
20 Staff management
20a Availability of staff with competency appropriate to procedure