Embed Size (px)
Citation preview
I
AirtqtsMtasj
DB
mi
8
Radiology Resident DictationInstruction: Effectiveness of the
Didactic LectureCourtney A. Woodfield, MD, Martha B. Mainiero, MD
Purpose: The study’s purpose was to determine the effectiveness of a didactic lecture for teaching andevaluating radiology resident dictation skills.
Methods: A 23-question test was created to assess resident knowledge of the American College of Radiologypractice guidelines for reporting and our institution-specific requirements for communication of diagnosticimaging results. The test was administered to 23 residents before and after a 40-minute didactic lecture coveringthe structure of radiology reports and requirements for communication of imaging findings. The pre- andpostlecture tests were graded on the basis of the number of correct answers. Data were analyzed using the mixedlinear model for repeated measures and the Holm test for group comparisons.
Results: Mean pre- and postlecture test scores were 74.6% � 2.73% and 94.6% � 5.94% for postgraduateyear (PGY) 2, 88.1% � 5.55% and 95.6% � 4.50% for PGY 3, 94.8% � 2.5% and 100% � 0% for PGY 4,and 96.8% � 1.79% and 98.4% � 2.19% for PGY 5, respectively. The increase of pre- to postlecture test scoreswas statistically significant for PGY 2, PGY 3, and PGY 4 residents (P � .005). Pre- to postlecture testimprovement was greatest for PGY 2 residents. Test performance of PGY 2 residents compared with PGY 5residents was statistically different.
Conclusion: Test scores for PGY 2 to PGY 4 residents significantly increased after didactic instruction on thereporting and communication of diagnostic imaging results. These findings suggest that a lecture and testformat can be used to teach and assess radiology resident reporting and communication skills.
Key Words: Education, dictation, residents
J Am Coll Radiol 2008;5:842-846. Copyright © 2008 American College of Radiology
ofdt“d
idt8to3rmset
NTRODUCTION
n important component of radiology residency trainings learning how to dictate accurate, clear, and conciseeports for a variety of imaging modalities and examina-ions. Traditionally, dictation skills are gradually ac-uired and honed over the course of a 4-year residencyhrough observation of fellow residents and attendingtaff. However, the Accreditation Council for Graduate
edical Education (ACGME) competency-based initia-ive is moving graduate medical education away from thepprentice model of education to a competency-basedystem that requires the establishment of goals and ob-ectives for education in various competencies along with
epartment of Diagnostic Imaging, The Warren Alpert Medical School ofrown University, Rhode Island Hospital, Providence, Rhode Island.
Corresponding author and reprints: Courtney A. Woodfield, MD, Depart-ent of Diagnostic Imaging, Rhode Island Hospital, 593 Eddy Street, Prov-
vdence, RI 02903; e-mail: [email protected].
42
bjective assessment tools that demonstrate that the goalsor competency have been met. In the instance of resi-ent dictation skills, there is a new ACGME requirementhat diagnostic radiology residency programs documentformal evaluation of quality dictated reports” by resi-ents [1].A 2002 to 2003 survey of program directors of accred-
ted US radiology residencies found that most programso not incorporate formal radiology dictation instruc-ion or feedback into training. The survey revealed that6% of responding programs provide residents with lesshan one hour per year of didactic instruction in radiol-gy reporting [2]. In addition, through a recent series of8 resident interviews, Steele et al [3] found that 78% ofesidents learn to dictate by listening to their peers orore senior residents, 13% by listening to faculty or
taff, and 8% by reading other radiology reports. How-ver, most of these residents would prefer a more struc-ured process of learning how to dictate. The increasing
ariety and complexity of imaging examinations to© 2008 American College of Radiology0091-2182/08/$34.00 ● DOI 10.1016/j.jacr.2008.01.007
wldemwaetdt
M
IfwAo(
bAwstwtnbsWsam
ctoocqfit
odg1
Woodfield, Mainero/Radiology Resident Dictation Instruction 843
hich residents are exposed during training further high-ight the importance of providing them with early formalictation instruction. In addition, residents need to beducated on proper reporting for appropriate reimburse-ent both for the financial health of the department inhich they are working and for their future practice. To
ddress the need for both organized resident dictationducation and evaluation, we developed a didactic dicta-ion lecture and a pre- and postlecture test. The test wasesigned to test both baseline dictation knowledge andhe effectiveness of the didactic lecture.
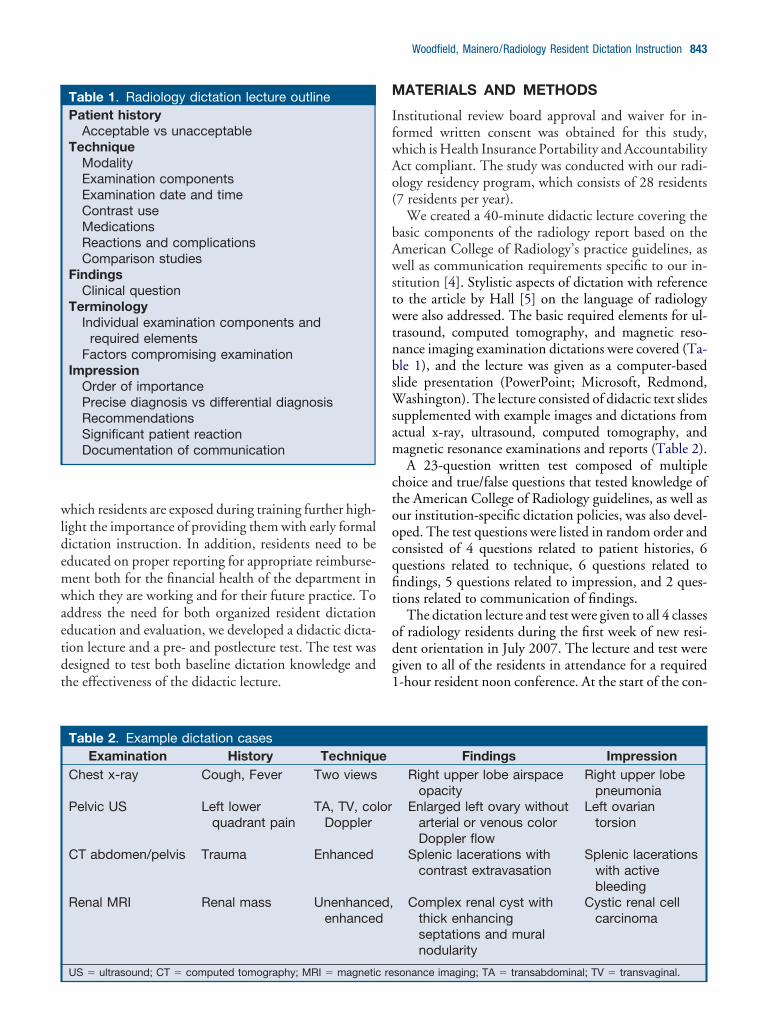
Table 1. Radiology dictation lecture outlinePatient history
Acceptable vs unacceptableTechnique
ModalityExamination componentsExamination date and timeContrast useMedicationsReactions and complicationsComparison studies
FindingsClinical question
TerminologyIndividual examination components and
required elementsFactors compromising examination
ImpressionOrder of importancePrecise diagnosis vs differential diagnosisRecommendationsSignificant patient reactionDocumentation of communication
Table 2. Example dictation casesExamination History Techniqu
Chest x-ray Cough, Fever Two views
Pelvic US Left lowerquadrant pain
TA, TV, coDoppler
CT abdomen/pelvis Trauma Enhanced
Renal MRI Renal mass Unenhanceenhanced
US � ultrasound; CT � computed tomography; MRI � magnetic re
ATERIALS AND METHODS
nstitutional review board approval and waiver for in-ormed written consent was obtained for this study,hich is Health Insurance Portability and Accountabilityct compliant. The study was conducted with our radi-logy residency program, which consists of 28 residents7 residents per year).
We created a 40-minute didactic lecture covering theasic components of the radiology report based on themerican College of Radiology’s practice guidelines, asell as communication requirements specific to our in-
titution [4]. Stylistic aspects of dictation with referenceo the article by Hall [5] on the language of radiologyere also addressed. The basic required elements for ul-
rasound, computed tomography, and magnetic reso-ance imaging examination dictations were covered (Ta-le 1), and the lecture was given as a computer-basedlide presentation (PowerPoint; Microsoft, Redmond,
ashington). The lecture consisted of didactic text slidesupplemented with example images and dictations fromctual x-ray, ultrasound, computed tomography, andagnetic resonance examinations and reports (Table 2).A 23-question written test composed of multiple
hoice and true/false questions that tested knowledge ofhe American College of Radiology guidelines, as well asur institution-specific dictation policies, was also devel-ped. The test questions were listed in random order andonsisted of 4 questions related to patient histories, 6uestions related to technique, 6 questions related tondings, 5 questions related to impression, and 2 ques-ions related to communication of findings.
The dictation lecture and test were given to all 4 classesf radiology residents during the first week of new resi-ent orientation in July 2007. The lecture and test wereiven to all of the residents in attendance for a required-hour resident noon conference. At the start of the con-
Findings ImpressionRight upper lobe airspace
opacityRight upper lobe
pneumoniaEnlarged left ovary without
arterial or venous colorDoppler flow
Left ovariantorsion
Splenic lacerations withcontrast extravasation
Splenic lacerationswith activebleeding
Complex renal cyst withthick enhancingseptations and muralnodularity
Cystic renal cellcarcinoma
e
lor
d,
sonance imaging; TA � transabdominal; TV � transvaginal.
fplpqdtg4Tdrt
alafsa
S
TtlmiPPitdpi
R
TdlSrtvFwsP9tm1Tp
rmdPdst
alintaaOt
D
AdituospPe9
Fc
844 Journal of the American College of Radiology/Vol. 5 No. 7 July 2008
erence, each resident was randomly given a numberedacket containing 2 copies of the test, one titled pre-
ecture and the other titled postlecture. The pre- andostlecture tests were identical, composed of the same 23uestions. The only identifying information that resi-ents indicated on their test packets was their year inraining. At the start of the conference, the residents wereiven 10 minutes to complete the pre-lecture test. The0-minute didactic dictation lecture was then given.ime was allotted for questions to be asked and answereduring the lecture. Immediately after the lecture, theesidents then all took the same 23-question postlectureest.
On completion of the postlecture test, residents werelso asked to indicate how helpful they found the didacticecture and test based on a 5-point scale of strongly agree,gree, neutral, disagree, and strongly disagree with roomor written comments. The pre- and postlecture test re-ults were graded on the basis of the number of correctnswers.
tatistical Analysis
he mean scores and ranges for the pre- and postlectureests for each residency class were calculated. The mixedinear model for repeated measures was used to deter-
ine whether there was a statistically significant increasen the mean pre- to postlecture test score for each class.ositive statistical significance was determined using avalue less than .005. The Holm test for group compar-
sons also was used to assess for statistical difference be-ween postgraduate year (PGY) 2 and more senior resi-ent test performance. The expectation was that testerformance would improve after the lecture and withncreasing resident level of experience.
ESULTS
wenty-three of the 28 residents in our radiology resi-ency program were present for the didactic dictation
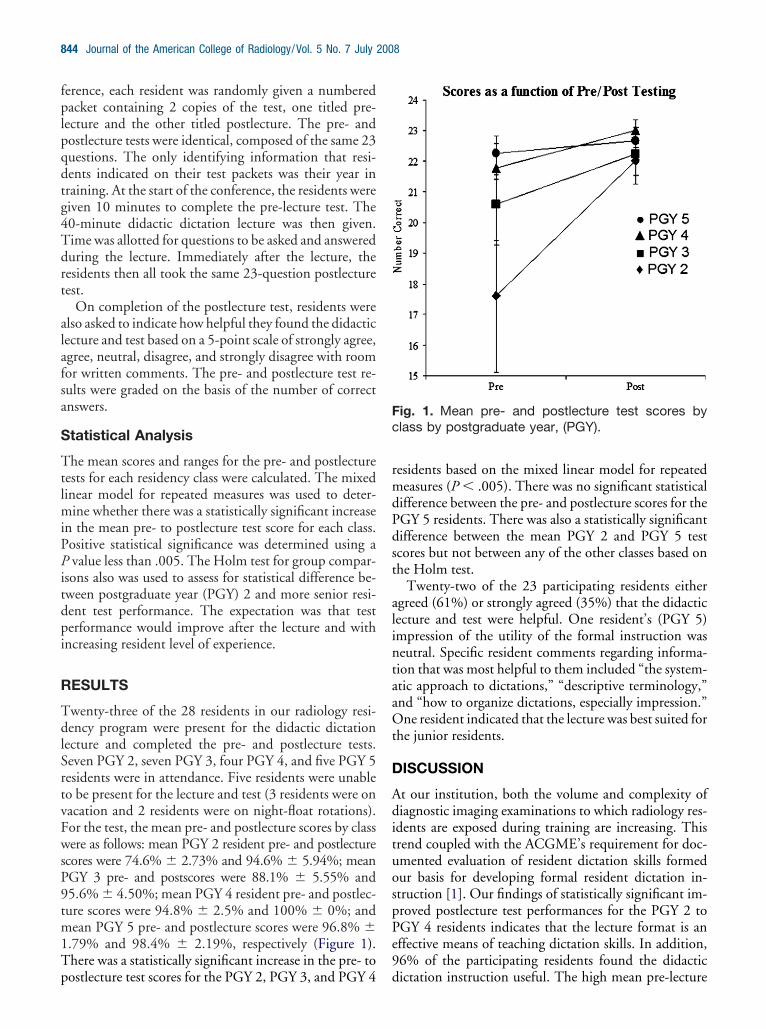
ecture and completed the pre- and postlecture tests.even PGY 2, seven PGY 3, four PGY 4, and five PGY 5esidents were in attendance. Five residents were unableo be present for the lecture and test (3 residents were onacation and 2 residents were on night-float rotations).or the test, the mean pre- and postlecture scores by classere as follows: mean PGY 2 resident pre- and postlecture
cores were 74.6% � 2.73% and 94.6% � 5.94%; meanGY 3 pre- and postscores were 88.1% � 5.55% and5.6% � 4.50%; mean PGY 4 resident pre- and postlec-ure scores were 94.8% � 2.5% and 100% � 0%; andean PGY 5 pre- and postlecture scores were 96.8% �
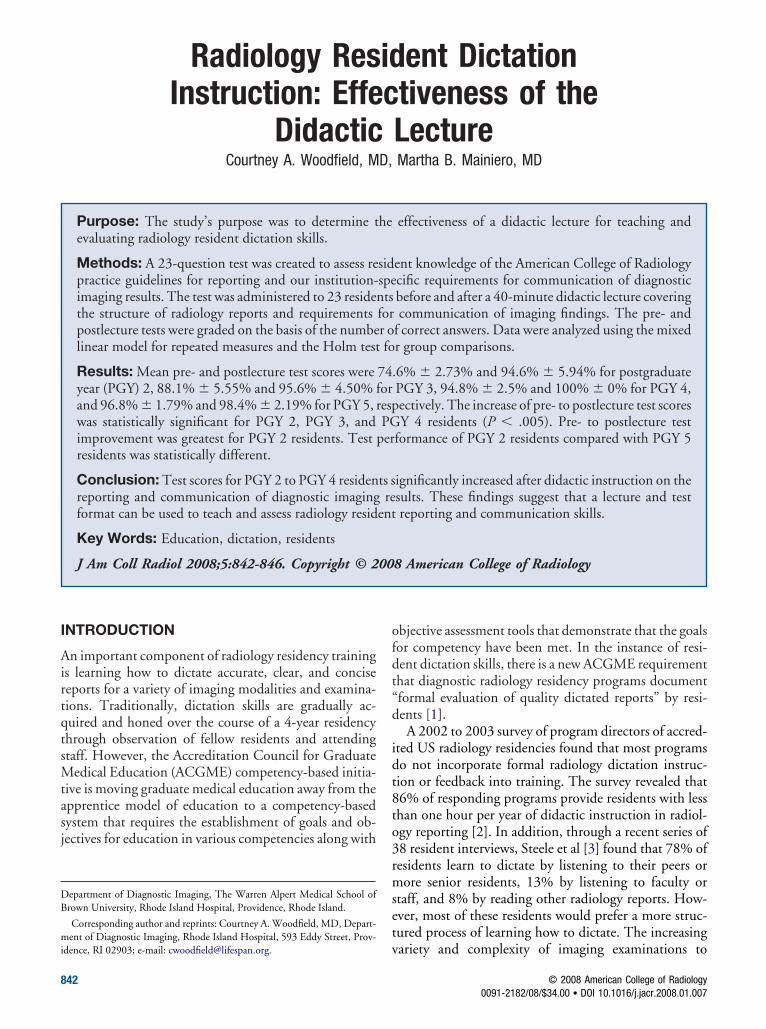
.79% and 98.4% � 2.19%, respectively (Figure 1).here was a statistically significant increase in the pre- to
ostlecture test scores for the PGY 2, PGY 3, and PGY 4 desidents based on the mixed linear model for repeatedeasures (P � .005). There was no significant statistical
ifference between the pre- and postlecture scores for theGY 5 residents. There was also a statistically significantifference between the mean PGY 2 and PGY 5 testcores but not between any of the other classes based onhe Holm test.
Twenty-two of the 23 participating residents eithergreed (61%) or strongly agreed (35%) that the didacticecture and test were helpful. One resident’s (PGY 5)mpression of the utility of the formal instruction waseutral. Specific resident comments regarding informa-ion that was most helpful to them included “the system-tic approach to dictations,” “descriptive terminology,”nd “how to organize dictations, especially impression.”ne resident indicated that the lecture was best suited for
he junior residents.
ISCUSSION
t our institution, both the volume and complexity ofiagnostic imaging examinations to which radiology res-
dents are exposed during training are increasing. Thisrend coupled with the ACGME’s requirement for doc-mented evaluation of resident dictation skills formedur basis for developing formal resident dictation in-truction [1]. Our findings of statistically significant im-roved postlecture test performances for the PGY 2 toGY 4 residents indicates that the lecture format is anffective means of teaching dictation skills. In addition,6% of the participating residents found the didactic
ig. 1. Mean pre- and postlecture test scores bylass by postgraduate year, (PGY).
ictation instruction useful. The high mean pre-lecture

qrc
rrspirldsiicsmCirads
etwaprarpwn3rpdcnpppta
wldfcfi
idtdpr
boztdtrmffiarirod
cpaadpotftsqbrtteacpbtltwe
f
Woodfield, Mainero/Radiology Resident Dictation Instruction 845
uiz score for the PGY 5 residents also indicates thatequisite dictation skills are eventually acquired over theourse of residency training.
A review of the radiology literature revealed no prioreports on the utility of the lecture format for teachingesidents how to dictate. However, another recently de-cribed method for teaching and evaluating resident re-orting skills is the Objective Structured Clinical Exam-nation (OSCE). Assessment of radiology residenteporting skills with the OSCE was described by Wil-iamson et al [6], who compared resident and attendingictations for sample radiographs with respect to well-pecified impressions. A linear trend of improved report-ng skills with increasing experience was found, indicat-ng that the OSCE is an effective technique for evaluatingommunication skills. The OSCE could also potentiallyerve as means of assessing the effectiveness of other for-al dictation instruction, including a didactic lecture.oakley et al [7] also found that routine attending edit-
ng of radiology resident reports improves the perceivedeport quality with respect to clarity, brevity, readability,nd quality of impression. Both of these studies furtheremonstrate the need for more structured dictation in-tructing during training.
The focus of our dictation lecture was on the requiredlements and general structure of radiology reports withhe goal of providing residents with a basic template fromhich even the most complex dictations could be cre-
ted. This concept of more standardized radiology re-orting was first proposed by Hickey in 1922 [8]. Moreecently, there has been renewed interest in the structurend quality of the radiology report with respect to refer-ing physician preferences. A 1988 survey of referringhysicians revealed that 40% thought radiology reportsere occasionally confusing, 49% said the reports didot always clearly address the clinical question, and only8% read the entire report [9]. In another survey ofeferring physicians, accuracy, followed by clarity, com-leteness, and timeliness was reported to be the mostesired radiology report quality [10]. In addition, reportsontaining long and complex sentences may be viewedegatively by referring physicians, and both referringhysicians and radiologists tend to prefer itemized overrose reports [11,12]. Our lecture emphasized this im-ortance of creating timely, accurate, and concise reportshat address the clinical question and include relevantnd clear impressions.
Our institution currently uses traditional dictationith transcription for radiology report generation, which
imits the number of standardized reports used by resi-ents. We do have standard normal dictation templatesor most studies, and all incoming residents receive aopy of these standard dictations. However, during their
rst 6 months of training, the first-year residents are lnstructed to fully dictate all reports using the normalictation templates for reference only. By learning howo efficiently dictate normal reports, we believe the resi-ents are better able to generate clear and organized re-orts for abnormal examinations while still addressing allequired report elements.
Our residents also review and edit all of their reportsefore attending review and sign-off. This gives them anpportunity to personally assess the quality and organi-ation of their reports. We anticipate that with the even-ual transition to voice recognition dictation, our resi-ents will rely more heavily on standardized reportingemplates to learn how to dictate. In addition, with voiceecognition, the preliminary resident report may be im-ediately available for review by referring clinicians be-
ore attending editing, which further highlights the needor teaching residents accurate, concise, and clear report-ng skills. Faster report generation with voice recognitionlso will allow for timelier faculty review and feedback ofesident reports. Faculty review of resident radiographicnterpretations has been shown to improve subsequentesident performance, which suggests that faculty reviewf resident reports with feedback could also improveictation performance [13].Limitations of our study include a general lack of
onsensus as to what constitutes a good radiology report,articularly with respect to terminology [5]. The stylisticspects of dictating are difficult to teach given the vari-bility of report style even at the attending level. We alsoo not know whether improvement in postlecture testerformance also translated into actual improved radiol-gy report dictations. Additional studies could look athe quality of resident dictations both before and afterormal dictation instruction to further assess the effec-iveness and retention of structured teaching. A potentialource of bias in our study was the use of the sameuestion set for the pre- and postlecture tests. It is possi-le that the residents focused on lecture informationelated to questions they found difficult on the pre-lec-ure test, allowing them to score higher on the postlectureest. In this manner, the pre-lecture test may have alsonhanced the learning experience by focusing residentttention on individual areas of weakness during theourse of didactic instruction. If we had used differentre- and postlecture test questions, there also would haveeen bias if the level of question difficulty was not iden-ical for both tests. Finally, the results of our study may beimited to programs that primarily use traditional dicta-ion where the report has to be structured by the residentithout the help of a voice recognition, computer-gen-
rated template.The high and similar pre- and postlecture test scores
or the PGY 5 residents implies that dictation skills are
earned by the fourth year of training, and senior resi-
dsifitTntbioHtpsifwteti
tbmicttifoiia
C
At
pfid
R
1
1
1
1
1
846 Journal of the American College of Radiology/Vol. 5 No. 7 July 2008
ents are therefore less likely to benefit from formal in-truction. To expedite the learning process and help jun-or residents learn to construct quality dictations in therst year of training, we plan to give the didactic dicta-ion lecture and test to all incoming radiology residents.he correct test answers also will be reviewed with theew residents, which will give them an additional oppor-unity to ask questions and learn from mistakes. Weelieve the lecture format for instruction can be readilyncorporated into a training program. A variable amountf time is initially required to create a didactic lecture.owever, such instruction can then be easily adminis-
ered to 1 or more classes of residents during a single lectureeriod. As our senior residents have learned these skills onervice, we anticipate that the knowledge the junior res-dents gained by the didactic instruction will be rein-orced by daily use and on-service feedback. Long term,e can monitor resident retention of instructional dicta-
ion information via our monthly electronic attendingvaluations of resident performance. One component ofhese monthly evaluations is assessing the quality of res-dent dictations.
Although we plan to give only the first-year residentshe general dictation lecture, all residents would likelyenefit from periodic updates on required reporting ele-ents. For example, the Centers for Medicare & Med-
caid Services’ Physician Quality Reporting Initiativeurrently requires specific report elements for computedomography and magnetic resonance imaging examina-ions of the brain and for carotid imaging studies, and its likely to mandate additional reporting standards in theuture [14]. As the preliminary dictators of many radiol-gy reports, residents need to remain current with report-ng standards. If the required reporting elements are notncluded in preliminary resident reports, it will requiredditional attending time and editing of reports.
ONCLUSIONS
didactic lecture is an effective means of teaching dicta-
ion skills, as evidenced by the improved postlecture testerformance of the PGY 2 to PGY 4 residents and overallavorable resident feedback. Such a lecture can readily bencorporated into a residency training program and mayecrease the radiology dictation learning curve.
EFERENCES
1. ACGME (Accreditation Council for Graduate Medical Education) Pro-gram Requirements for Resident Education in Diagnostic Radiology.Available at: http://www.acgme.org/acWebsite/RRC_420/420_prIndex.asp. Accessed July 1, 2008.
2. Sistrom C, Lanier L, Mancuso A. Reporting instruction for radiologyresidents. Acad Radiol 2004;11:76-84.
3. Steele JL, Nyce JM, Williamson KB, et al. Learning to report. Acad Radiol2002;9:817-20.
4. American College of Radiology. ACR standard for communication: diag-nostic radiology. Revised 2005 (Res. 11), effective October 1, 2005.
5. Hall FM. Language of the radiology report: primer for residents andwayward radiologists. AJR Am J Roentgenol 2000;175:1239-42.
6. Williamson KB, Steele JL, Wilkin TD, et al. Assessing radiology residentreporting skills. Radiology 2002;225:719-22.
7. Coakley FV, Heinze SB, Shadbolt CL, et al. Routine editing of trainee-generated radiology reports: effect on style quality. Acad Radiol 2003;10:289-94.
8. Hickey PM. Standardization of roentgen-ray reports. AJR Am J Roent-genol 1922;9:519-21.
9. Clinger NJ, Hunter TB, Hillman BJ. Radiology reporting. Attitudes ofreferring physicians. Radiology 1988;169:825-6.
0. Johnson AJ, Ying J, Swan JS, et al. Improving the quality of radiologyreporting: a physician survey to define the target. J Am Coll Radiol2004;1:497-505.
1. Sierra AE, Bisesi MA, Rosenbaum TL, et al. Readability of the radiologicreport. Invest Radiol 1992;27:236-9.
2. Naik SS, Hanbidge A, Wilson SR. Radiology reports: examining radiol-ogist and clinician preferences regarding style and content. AJR Am JRoentgenol 2001;176:591-8.
3. Seltzer SE, Doubilet PM, Sherif CR, et al. Educational impact of facultyreview on radiology residents’ radiographic interpretations. Invest Radiol1984;19:61-4.
4. Centers for Medicaid and Medicare Services: Physician QualityReporting Initiative. Available at: http://www.cms.hhs.gov/PQRI/
Downloads/2008PQRIMeasureSpecs.pdf.