Embed Size (px)
Citation preview

Radiological Evaluation and Classification of Pediatric
Fractures
By Nicholas White, HD and John Sty, MD MILWAUKEE, WISCONSIN
p e d i a t r i e represents a por- museuloskeletal trauma significant tion of visits to the emergency department. Following his- tory, physical exam, splinting, and pain management, radiologieal evaluation is the next essential step in the man-
agement of skeletal injuries. Radiologieal evaluation of fractures includes three equally important aspects: 1) obtaining the appro- priate imaging study, 2) accurate interpretation of the radio- graphic image, and 3) accurate description of the fracture. This article will focus on describing various imaging techniques avail- able for the evaluation of pediatric fractures, with a special focus on the radiographic examination of the elbow. A review of the proper terminology used for the description of fractures will follow.
Imaging Techniques
Obtaining the appropriate imaging study is the first and most important step in the radiologieal evaluation of pediatric museu- loskeletal injuries. Plain radiographs eontinue to be the mainstay of imaging, and are sufficient for the evaluation of most acute injuries of the axial and appendieular skeleton. However, there are elinieal circumstances when special imaging techniques are required to demonstrate or further delineate skeletal trauma. Some circumstances that may require further investigation in- elude: 1) children with normal plain radiographs that have strong clinical indicators for a fracture, 2) an extensive eomminuted fracture near a large joint, and 3) a fracture with a suspected
9 4 RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY

RADIOLOGtCAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY 95
TABLE I. ABC'S of Radiographic Interpretation A Adequacy
Alignment
B Bones
C Cartilage
S Soft tissues
Correct/comparison views, good technical quality
Joint alignment and position
Examine entire bone, end to end
Presence and type of fracture
Physeal involvement, ossification centers
Adjacent swelling, fat pads/joint effusions
associated vascular injury. Imaging techniques such as computed tomography (CT), magnetic res- onance imaging (MRI), bone scan, and ultrasound can provide valuable information in the evaluation of certain aeute fractures. A brief review of each of these techniques and the clinical situations in which they are most useful will be discussed.
Plain R a d iog raphs ( R o e n t g e n o g r a m s )
Plain radiographs remain the primary imaging modality for the evaluation of most pediatric frac- tures. Selection of the most appropriate views not only minimizes radiation exposure, but will also enhance one's ability to detect a subtle fracture.
Accurate assessment of a fracture requires at least two views at 90 ~ to each other, as subtle fractures are often missed or not visible on one view alone. Two views will also provide a true perspec- tive of the spatial relationships of the fracture frag- ments. These standard views usually include an anteroposterior (AP) and a lateral projection. Addi- tional oblique projections are sometimes necessary to detect fractures of the elbow joint and carpal bones, or when true lateral projections cannot be obtained, as is frequently the ease with radiographs of the hip and shoulder. Comparison views of the opposite limb may also be useful, as epiphyseal lines and accessory ossieles often mimic frac- tures. ~-4
The radiographic evaluation of a long bone frac- ture should include the entire length of the bone, from the joint above to the joint below, to ensure that an associated fracture or dislocation is not present. Although this may not always be neeessaI3, for injuries at the ends of long bones, it is manda- tory for those involving the diaphysis when injuries of an adjacent joint may co-exist. Monteggia's in- jury (ulnar fracture with radial head dislocation) and Galeazzi's injury (radial shaft fracture with dis- tal radioulnar joint dislocation) are both examples of injuries that may be overlooked bv inadequate radiologie evaluation.
Repeat radiographs are sometimes useful in chil- dren with continuing bone pain and tenderness who initially had normal plain films. Subtle stress fractures may be demonstrated by the appearance of a periosteal reaction at the fracture site, although this usually takes at least 5 to 7 days to appear. 1-4
Once the appropriate radiographs have been ob- tained, a systematic approach to interpretation is essential, as subtle fractures and dislocations can easily be missed. Following the "ABC'S" is a useful approaeh (Table 1).
C o m p u t e d T o m o g r a p h y
When plain radiography is unable to provide suf- ficient information regarding skeletal trauma, CT remains the mainstay of emergency department imaging. CT is regarded as the most accurate means of assessing bony anatomy and detecting or exclud- ing a fracture that was equivocal on plain film, or to further delineate the extent of a previously diag- nosed fracture. Advantages over plain radiography include improved soft tissue visualization and ex- cellent bony detail in multiple planes. Its multipla- nar reconstructions are invaluable in assessing complex fractures, as it displays various compo- nents in isolation, free of overlap by surrounding structures. Specific areas of particular use include evaluation of pelvie fractures, shoulder fractures, sternodavieular fraetures, spinal fractures, carpal/ tarsal fractures, and caleaneous fractures. 3.5-n
In pelvic fractures, CT can further define the extent of injury, improve visualization of fracture displaeement, assess pelvie instability, detect sub- tle saero-iliae disruptions, and demonstrate soft tis- sue injuries in the pelvis. Axial projections provide good visualization of the femoral head and neck and its relationship to the aeetabulum, allowing detec- tion of non-displaced fractures of the femoral head and occult fractures of the aeetabulum.r, s
CT has been shown to be superior to plain radio- graphs in evaluation of complex fractures of the proximal humerus and in detecting scapular frae-

9 6 RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY
TABLE 2. Aspects of Fracture Description
Clinical Radiographic
Age and sex
Mechanism of injury
Anatomic location (bone involved)
Neurovascular status
Soft tissue involvement (open or closed)
Anatomic location of fracture line
Pattern of fracture
Relationship of fracture fragments
Physeal involvement (Salter- Harris type)
Joint involvement (alignment/fat pads)
tures, which can be subtle on plain radiographs and are commonly missed. 9
Fractures and dislocations of the sternoclavi- clar joint are often accompanied by superior rib fractures and shoulder injuries. When posterior dislocation occurs, it may be associated with me- diastinal injury. Plain radiographs are rarely helpful in these circumstances, whereas CT is well suited to evaluate these complex injuries that often involve the trachea and thoracic vas- culature. 10
CT scans are also useful in evaluating the C1-C2 articulation and C6-T1 regions of the cervical spine that are not adequately demonstrated on plain films, and are more sensitive than plain films for detection of cervical spine fractures. CT is also useful to confirm and further define spinal injuries suspected on plain films. 6,11
Magnet ic R e s o n a n c e Imaging
MRI is seldom used for the evaluation of pedi- atric fractures in the emergency depar tment set- ting. In addition to its lower cost, the widespread availability, speed and versatility of CT make it a more suitable follow up to plain films. However, advances in MRI technology have led to its in- creased utilization for the evaluation of complex fractures. MRI remains the method of choice for imaging many soft tissue injuries, providing di- rect visualization of ligaments, tendons, cartilage, muscle, and bone marrow that are difficult to see on plain radiography and that are not clearly distinguished by CT. 3A2-15
MRI is particularly useful in patients who have injury to the knee but have normal findings on plain radiographs. It allows for the identification of chon- dral fractures, osteochondral fractures, meniseal
injuries, ligamentous injuries, and stress frac- tures.16,17
The ability of MRI to clearly visualize unossified cartilage makes it an excellent choice for the eval- uation of physeal injuries. However, studies com- paring MRI and plain films for the evaluation of acute tibial fractures and acute elbow fractures found that even though MRI reveals bone and soft tissue injuries well beyond those recognized by plain radiographs, this additional information had little bearing on treatment or clinical outcome. Nonetheless, MRI is excellent for following the heal- ing of physeal injuries in the non-acute set- ting.12,18A9
As a result of increasing use of MRI in the eval- uation of acute musculoskeletal injury, incidental intraosseous abnormalities not visible on plain ra- diography have become increasingly recognized. These abnormalities have been termed occult in- traosseous fractures or bone bruises. Bone bruising is a term used to describe local marrow edema and hemorrhage within the cancellous bone following an extensive microtrabecular fracture injury. While bone bruising is being increasingly recognized, little is lmown about its short-term resolution, clinical symptoms, or long-term prognosis. In general, bone bruises resolve in 6 to 16 weeks and increase the patient's risk of post-traumatic arthritis. 13,2~
Bone Scan (Skele ta l Sc in t ig raphy)
Radioisotope bone scanning or skeletal seintig- raphy is a valuable adjunct to plain film radiogra-
TABLE 3. Fracture Classification by Anatomic
Type
Location
Location of fracture
Diaphyseal
Metaphyseal
Epiphyseal
Physeal
Articular
Supracondylar
Transcondylar
Epicondylar
Intercondylar
Subcapital
Central shaft of long bone
Widened end of long bone
Chondro-osseous end of long bone
Involve growth plate; subclassified by Salter-Harris type
Cartilaginous joint surface
Proximal to condyles
Traverses the condyles
Next to condylar surface
Between the condyles
Just below the epiphyseal head

RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY 9 7
A B C E
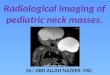
G H I Figure I. Illustration of fracture patterns. (A) Longitudinal--fracture line parallel to bony axis. (B) Transverse--fracture line perpendicular to bony axis. (C) Oblique~fracture line at angle to bony axis. (D) Spiral--fracture line runs curvilinear course to bony axis. (E) Impacted--fractured bone ends compressed together. (F) Comminuted~fragmentation of bone into 3 or more parts. (G) Greenstick--bending of bone with incomplete fracture of convex side. (H) Bowing--bony plastic deformation. (I) Torus--buckling fracture.
phy in the assessment of skeletal trauma. Scintigraphy involves labeling a bone-seeking phar- maceutical substance with a radioactive isotope that is actively incorporated into the musculoskel- etal system. Technet ium-99m-labeled polyphos- phates are the most common radiopharmaeeut ieals used today. Two hours after intravenous injection, levels of concent ra t ion (photon energy emit ted by the isotopes) are measured using a ~/camera. The isotope concent ra tes in areas of increased bone turnover, such as growth plates, fracture margins, infection, tumor, arthritis, and periostitis. In- creased uptake of the isotope will result in "hot spots" on the bone scan. Differences in uptake can then be compared between the affected and non- affected sides.
Bone scan has a high sensitivity for the detect ion of fractures, but low specificity when compared to plain radiographs. The principal objective of a bone scan is to identify fractures that are not apparent on plain films. A bone scan reveals the metabolic dis- turbance (early osteoblastie react ion) at an acute fracture site within 24 to 72 hours of injury. If there is no evidence of increased radioactivity, a fracture can safely be ruled out. Bone scan is non-specific, however, and the cause of increased uptake cannot be stated with certainty. Correlation with plain films, CT, or MRI is often necessary to establish the diagnosis.
Bone scan is useful in the diagnosis of fractures of the scapula, s ternum, sacrum and portions of the pelvis that are clinically suspected but difficult to

9 8 RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WRITE AND STY
effusions, subtle periosteal elevations, and subperi- osteal hemorrhages that m a y be associated with physeal injuries. 1,3,5
Classification and Terminology of Fractures
Emergency physic ians mus t be aware of the ap- propr ia te terminology used to describe fractures. Accura te f racture descript ion is essential in assist-
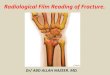
Figure 2. Oblique forearm radiograph. Arrow marks greensdck fracture.
demonstrate with plain radiography due to their an- atomic location. It is also useful for detecting occult fractures in the carpal or tarsal bones, radial head, or femoral neck that are not visible on initial radiogra- phy. Stress fractures are also seen on bone scan 2 to 6 weeks prior to becoming visible on plain films. As discussed later in this issue, bone scan is also useful in the assessment of the battered ehild. 1,-%5
U l t r a s o u n d
Ultrasound is useful in evaluating soft tissues. It is mos t valuable in identifying small t r aumat ic jo int
Figure 3. Anteroposterior lower leg radiograph. Small arrow marks bowing injury to fibula. Large arrow marks spiral frac- ture of tibia.

RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY 9 9
ing the orthopedie speeialist in providing manage- ment recommendations. There are 10 aspects that should be ineluded in any fracture description; 5 are clinical and 5 are radiographic (Table 2). The following discussion will focus on radiographic de- scription.
Radiographic Frac ture Descr ip t ion
Anatomic location. Anatomic terms are used to describe the location of the fracture line (Table 3). 4.23
Fracture patterns. The pattern of fractures in the pediatric population depends on the age of the child and their stage of development. Non-physeal fractures can be classified as complete or incom- plete. Complete fractures include longitudinal, transverse, oblique, spiral, impacted, and commi- nuted. Incomplete fractures are unique to childhood and include greenstick, bowing, and torus types (Fig- ure 1). 1'4'5'23-25
A greenstiek fracture is an incomplete transverse fracture of the bony cortex on the convex side, and a bowing deformity of the bony cortex on the con- cave or compression side (Figure 2).
Bowing fractures occur when a force exceeds the elastic limits of a bone, causing it to bend to a point of plastic deformation. Although a fracture line is not apparent radiographieally, multiple oblique mi- erofraetures are visible on histological examination. Detection can be difficult in mild eases without comparison view of the eontralateral extremity (Figure 3).
Torus ("little hill") fractures result from a buckling of the cortex and underlying trabeeular bone. An oblique or comparison view is often necessary to verify this subtle alteration in bony contour (Figure 4).
Fracture fragments. The relationship of frac- ture fragments can be described by the following terms: angulation, shortening, distraction, and dis- placement. When describing fracture fragments, the distal fragment should be described in relation to the proximal fragment, the latter being consid- ered as the stationary part. Angulation is measured by drawing a line through the normal bony axis, and then another through the axis of the fractured distal segment. Shortening occurs when an overlap of bony fragments causes a decrease in the normal length of the bone. Distraction occurs when frac- tured ends are vertically pulled apart from each other. Displacement occurs when fractured ends are horizontally pulled apart from each other (Fig- ure 5). 4'24
Physealfraeturcs. Approximately 10% to 30% of all fractures in children involve the physis. Most
Figure 4. lateral forearm radiograph. Arrow marks torus fracture.
physeal disruptions occur through the zone of car- tilage eell hypertrophy. This hypertrophic zone is the weakest portion of the growth plate due to its limited amount of collagenous matrix and the lack of significant calcification. Even when diagnosed and treated properly, physeal injuries may still re- sult in longitudinal or angular abnormalities, s,26-29
Because of the potential for long-term morbidity in patients with physeal fractures, great attention has been focused on the classification, diagnosis, treatment, and prognosis of physeal fractures. Og- den, Shapiro, Peterson, and others have classified these injuries, but the Salter-Harris classification system remains the most well known and widely used. The Salter-Harris classification, which is based on the roentgenographie appearance of the

I O 0 RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY
l &
g <
)
A. B. C. D. Figure 5. Relationship of fracture fragments. (A), Angulation. (B), Shortening. (C), Distraction. (D), Displacement.
fraeture, describes five types of growth plate frac- tures, each having specific prognostie and treat- ment implications (Figure 6). 24,3~
Salter-Harris type L Type I injuries consist of a fracture line passing horizontally through the phy- sis only, resulting in a pure epiphyseal separation. They account for approximately 5% of physeal in-
juries. Radiographie findings that suggest type I fractures include physeal widening and epiphyseal displacement (Figure 7). Radiographs, however, are often normal, and diagnosis is made clinically by demonstrating tenderness over the area of the growth plate. Type I fraetures are generally benign and the prognosis is favorable for normal growth if
Type I Type II Type III Type IV Type V Figure 6. Salter-Harris classification of physeal injuries.

RADIOLOGICAL EYALUATIOH OF PEDIATRIC FRACTURES I WHITE AND STY I 0 1
Figure 7. Anteroposterior wrist radiograph. Arrow marks a Salter-Harris Type I fracture. Note physeal widening.
near anatomic reduction is achieved. Exceptions include the proximal radius, proximal and distal femur, and proximal tibia. Type I fractures in these locations are subject to premature physeal closure and post traumatic growth arrest.
Salter-Harris type II. Type II injuries eonsist of a disruption that courses through a portion of the growth plate and then extends through the periph- eral aspect of the metaphysis. It is the most com- mon type of physeal injury, accounting for approximately 75% of all fraetures involving the growth plate. A fragment consisting of the entire epiphysis with an attached metaphyseal fragment is produced (Figure 8). Similar to type I injuries, prog- nosis is favorable.
Salter-Harris type IlL Type 1II injuries are in- traartieular fractures that involve the epiphysis and physis. The fraeture line begins on the articular surface and eourses vertically through to the epiph- ysis and then horizontally through the peripheral aspect of the physis. Type III injuries account for approximately 10% of physeal injuries, and usually occur in children with a partially closed physis.
This intraarticular injury creates a separate epiph- yseal fragment with no connection to the metaph- vsis (Figure 9). Anatomic position must be reestablished to restore normal joint function and prevent growth arrest. Prognosis can be quite poor, though growth arrest and deformities are rare if adequate reduction is achieved.
Salter-Harris type IV. Type IV injuries, like type III injuries, are intraarticular. The fracture line courses through the epiphysis, physis, and metaph- vsis. A single fragment that consists of both epiph- vsis and metaphysis is created and is usually separated from the parent bone (Figure 10). Type IV fractures account for approximately 10% of phy- seal injuries. Open reduction and internal fixation are almost always necessary. Growth arrest and
Figure 8. Anteropostermr wrist radiograph. Arrow marks a Salter-Harris Type II fracture.

10' l RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY
tion of the joint capsule. The elbow is perhaps the most challenging joint to evaluate radiographically.
Supraeondylar fractures account for more than 50% of elbow fractures in children. The presence of multiple epiphyseal ossification centers can make it difficult to distinguish them from fractures. Good quality frontal and true lateral (hourglass configu- ration to distal humerus) views must be obtained. Oblique projections are frequently needed for sub- tle radial head fractures. If standard projections are not obtainable because of pain and oblique views are all that are available, it may be helpful to obtain a radiograph of the contralateral elbow in the same position for comparison. There are five important radiographic features of the elbow to evaluate for fractures: 1) bony contour, 2) ossification centers, 3) fat pads, 4) the anterior humeral line, and 5) the radiocapitellar line.
Bony contour. Careful examination of the ends of the humerus, radius, and ulna for abnormalities in bony contour will assist in the detection of subtle fractures. The transition from the diaphysis to the metaphysis should be gradual and smooth, and free of any disruptions that may indicate a fracture.
Figure 9. Anteroposterior ankle radiograph. Arrow marks Salter-Harris Type III fracture.
joint deformities do occur with this injury, although they are minimized with proper orthopedic man- agement.
Salter-Harris type V. Type V injuries are sec- ondary to axial compression of the physis, and ac- count for about 1% of physeal injuries. Radiographic diagnosis is almost impossible to make at time of injury, as radiographs are often normal or only show subtle narrowing of the growth plate. Distinction between type I and type V inju- ries is often not apparent until subsequent growth abnormalities occur.
Joint involvement. The radiographic evaluation of a joint following trauma should include an exam- ination of the ends of the apposing bones, joint space width, the alignment of the joint, and nota- tion of any periarticular swelling caused by disten-
Figure 10. Anteroposterior elbow radiograph. Arrow marks Salter-Harris Type IV fracture.

RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY 1 0 3
F A
B
E
D
Ossification Center Appears Fuses
A. Capitellum 1-3 years (1) 16-18 years
B. Radial head 2-6 years (3) 15-20 years
C. Internal (medial) epicondyle 4-8 years (5) 16-18 years
D. Trochlea 7-12 years (7) 18 years
E. Olecranon 9-14 years (9) 16-20 years
F. External (lateral) epicondyle 10-12 years (11) 16-18 years
Figure I I. Anatomic position, appearance, and fusion of elbow epiphyses. (Adapted with permission from Carty H (ed): Emer- gency Pediatric Radiology. New York, NY, Springer-Veda& 1999.)
Ossification centers. The six centers of ossifica- tion are initially cartilaginous and not visible on standard radiographs. Eventually they be- come fused as the growth plates close. Ossification centers have well cor t icated margins that are smooth and round. A recent fracture fragment will have at least one edge of irregularity and are not well corticated. Often, one of the adja- cent bones will demonst ra te a similar irregular mar- gin, represent ing the site from which the fragment arose.
Although the age of appearance of the ossifica-
tion centers is variable, their chronological order of appearance is fairly constant. Knowing this se- quence can help de termine whether a bony struc- ture is an avulsion fracture or an ossification center . The mnemonic device for the appearance of these six ossification centers is CRITOE: Capitel- lum, Radial head, Internal or medial epicondyle, Trochlea, Olecranon, and External or lateral epi- condyle. The ages at which these ossification cen- ters appear and fuse vary. from person to person and between genders (approximately 6 months earlier in girls.) As a general guideline however, they ap- pear at 1, 3, 5, 7, 9, and 11 years of age (Figure 11).
Fat pads. The presence of an elbow joint effu- sion following t rauma is character ized by displace- ment of the humeral anter ior and posterior fat pads and is highly suggestive of an intracapsular fracture. The anter ior fat pad lies just over the coranoid fossa, and is visualized on normal radiographs as a thin radiolucent line just anter ior to the border of the distal humerus (Figure 12). The poster ior fat pad is deeply buried in the olecranon fossa, and is only visible as a thin radiolucent line along the posterior border of the distal humerus when a joint effusion is present. An effusion will elevate these fat pads, creating a more p rominen t anter ior fat pad lucency ("sail sign"), and allowing visualization of
Figure 12. Lateral elbow radiograph. Normal true lateral. Note hourglass configuration of the distal humerus. Arrow marks thin anterior fat pad. Anterior humeral line intersects middle third of capitellum. Radiocapitellar line intersects center of capitellum.

104. RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES / WHITE AND STY
Figure 13. Lateral elbow radiograph. Distal supracondylar frac- ture. Note anterior humeral line intersecting anterior third of capitellum. Small arrow marks posterior fat pad. Large arrow marks elevated anterior fat pad.
the deeply buried pos ter ior fat pad (Figure 13). A recent prospect ive s tudy demons t r a t ed tha t the poster ior fat pad sign was predict ive of an occult f racture of the elbow following t r auma in about 75% of chi ldren who had no o ther radiographic evidence of fracture. 34
Anterior humeral line. Posterior d i sp lacement of the distal humerus is c o m m o n in chi ldren with supraeondylar fractures. On a t rue lateral radio- graph, a line placed along the anter ior por t ion of the distal humera l shaft will normal ly in tersect the middle third of the eapi te l lum (Figure 12). How- ever, in the p resence of a supraeondylar fracture, this line will in tersect the anter ior third of the eapi tel lum or pass comple te ly anter ior to it (Figure 13).
RadiocapiteUar line. The radioeapitel lar line is impor tan t to de te rmine the relat ion of the radial head to the capi tel lum and is drawn along the axis of the proximal radius. This line should always in tersect the center of the capi te l lum regardless of the plane of the radiograph (Figure 12). Radial head dislocation or radial neck fracture should be sus- pec ted when this line does not in tersect the eapi- tellum.l,a-s
Summary
Despite advanees in medical seienee, s tandard r ad iog raphy- -d i s eove red by Wilhelm Roentgen in
184S- - r ema ins the p r imary me thod of evaluating skeletal injuries. The use of more sophis t icated im- aging techniques should be guided by our knowl- edge of pediatr ic or thopedics and the clinical scenario placed before us. Accura te descr ipt ion of findings to the or thopedis t requires the use of ap- propr ia te terminology. Effective communica t i on will assist the or thopedis t in providing t r e a t m e n t r ecommenda t ions .
References 1. Carty H (ed): Emergency Pediatric Radiology.
New York, NY, Springer-Verlag, 1999. 2. John 8D: Trends in pediatric emergency imaging.
Radiol Clin North Am 37:995-1034, 1999. 3. Juhl JH, Crummy AB, Kuhlman JE, (eds): Paul and
Juhl's Essentials of Radiographic Imaging. Philadelphia, PA, Lippineott Williams and Wilkins, 1998.
4. Simon RR, Roenigskneeht S J: Emergency Ortho- pedics. The Extremities. New York, NY, McGraw-Hill, 2001.
5. Bliekman JG: Pediatric Radiology. St Louis, MO, Mosby, 1994.
6. Pretorius ES, Fishman EK: Spiral CT and three- dimensional CT of museuloskeletal pathology: Emer- gency room applications. Radiol Clin North Am 37:953- 974, 1999.
7. Buekley SL, Burkus JK: Computerized axial to- mography of pelvic ring fractures. J Trauma 27:496-502, 1987.
8. Deutseh AL, Mink JH, Waxman, AD: Occult frac- tures of the proximal femur: MR imaging. Radiology 170: 113-116, 1989.
9. Pretorius ES, Scott WW, Fishman ER: Acute trauma to the shoulder: Role of spiral CT imaging. J Emerg Radiol 2:13-17, 1995.
10. Jurik AG, Albreehtsen J: Spiral CT with three- dimensional and multiplanar reconstruction in the diag- nosis of anterior chest wall joint and bone disorders. Aeta Radiol 35:468-472, 1994.
11. Nunez DB Jr, Zuluaga A, Puentes-Bernardo DA, et al: Cervical spine trauma: How much more do we learn by routinely using spiral CT? Radiographies 16:1307-1318, 1996.
12. Petit P: Acute fracture of the distal tibial physis: Role of gradient-echo MR imaging versus plain film ex- amination. A JR Am J Roentgenol 166:1203-1206, 1996.
13. Eustaee 8, Adams J, Assaf A: Emergency MR im- aging of orthopedic trauma. Current and future direc- tions. Radiol Clin North Am 37:975-994, 1999.
14. Naranja RJ Jr: Pediatric fraeture without radio- graphic abnormality: Description and significance. Clin Orthop 342:141-146, 1997.
15. Benedetti PF: MR imaging in emergency medicine. Radiographies 16:953-962, 1996.
16. Mink JH, Deutseh AL: Occult cartilage and bone injuries of the knee: Detection, elassifieation, and assess- ment with MR imaging. Radiology 170:823-829, 1989.

RADIOLOGICAL EVALUATION OF PEDIATRIC FRACTURES ! WHITE AND STY 105
17. Mink JH, Deutsch AL: Magnetic resonance imag- ing of the knee. Clin Orthop 244:29-47, 1989.
18. Beltran J, Rosenberg ZS, Kawelblum M, et al: Pe- diatric elbow fractures: MRI evaluation. Skeletal Radiol 23:277-281, 1994.
19. Griffith JF: Acute elbow trauma in children: Sec- trum of injury revealed by MR imaging not apparent on radiographs. A JR Am J Roentgenol 176:53-60, 2001.
20. Lee JK, Yao L: Occult intraosseous fracture: Mag- netic resonance appearance versus age of inju~,. Am J Sports Med 17:620-623, 1989.
21. Graf BK, Cook DA, De Smet AA, et al: "Bone bruises" on magnetic resonance imaging evaluation of anterior cruciate ligament injuries. Am J Sports Med 21:220-223, 1993.
22. Newberg AH, Wetzner SM: Bone bruises: Their patterns and significance. Semin Ultrasound CT MR 15: 396-409, 1994.
23. Zitelli B J, Davis IIW: Atlas of Pediatric Physical Diagnosis. St. Louis, MO, Mosby-Wolfe, 1997.
24. Fleisher GR, Ludwig S: Textbook of Pediatric Emergency Medicine. Philadelphia, PA, Lippincott Wil- liams and Wilkins, 2000.
25. Barkin R~I: Pediatric Emergency Medicine. Con- cepts and Clinical Practice. St. Louis, MO, Mosby, 1997.
26. Reed MtI: Fractures and dislocations of extremi- ties in children. J Trauma 17:351-354, 1977.
27. Pollen AG: Fractures involving the cpiphyseal plate. Reconstr Surg Traumatol 17:25-39, 1979.
28. Mann DC, Rajmaira S: Distribution of physeal and nonphyseal fractures in 2,650 long-bone fractures in chil- dren aged 0-16 years. J Pediatr Orthop 10:713-716, 1990.
29. Iannotti JP: Growth plate physiology and pathol- ogy. Orthop Clin North Am 21:1-17, 1990.
30. Ogden JA: Skeletal Injury. In The Child. Philadel- phia, PA, Lea and Febiger, 1982.
31. Peterson ItA: Physeal fractures: Part 3. Classifica- tion. J Pediatr Orthop 14:439-448, 1994.
32. Salter RB, Itarris WR: Injuries involving the epiphyseal plate. J Bone Joint Surg 45:587-622, 1963.
33. Shapiro F: Epiphyseal disorders. N Engl J Med 317:1702-1710, 1987.
34. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in chil- dren. J Bone Joint Surg Am 81:1429-1433, 1999.