Embed Size (px)
Citation preview

Radiography of the Radiography of the GI SystemGI System
Chapter 17Chapter 17

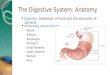
Anatomy Of Digestive SystemAnatomy Of Digestive System
Alimentary CanalAlimentary Canal MouthMouth PharynxPharynx EsophagusEsophagus StomachStomach Small / Large Small / Large
IntestineIntestine

Anatomy Of Digestive Anatomy Of Digestive SystemSystem
Accessory Accessory glandsglands LiverLiver GallbladderGallbladder Salivary Salivary
glandsglands PancreasPancreas

EsophagusEsophagus
Long muscular tube carries food Long muscular tube carries food and saliva from laryngopharynx to and saliva from laryngopharynx to stomachstomach
Approximately 10 in. long in adultApproximately 10 in. long in adult Lies in midsagittal planeLies in midsagittal plane

EsophagusEsophagus
Originates around Originates around C-6C-6
In thorax, it is In thorax, it is anterior to spine, anterior to spine, posterior to posterior to trachea and hearttrachea and heart
Passes through Passes through diaphragm through diaphragm through esophageal hiatusesophageal hiatus

EsophagusEsophagus Inferior to diaphragm Inferior to diaphragm
curves sharply leftcurves sharply left Increases in diameterIncreases in diameter Joins stomach at Joins stomach at
esophagogastric esophagogastric junctionjunction
At level of xyphoid tipAt level of xyphoid tip 4 layers of the 4 layers of the
esophagusesophagus Outermost - fibrousOutermost - fibrous MuscularMuscular SubmucosalSubmucosal Innermost - MucosalInnermost - Mucosal

StomachStomach
Dilated saclike Dilated saclike portion of portion of digestive tractdigestive tract
Composed of same Composed of same 4 layers as 4 layers as esophagusesophagus Outermost - fibrousOutermost - fibrous MuscularMuscular SubmucosalSubmucosal Innermost - MucosalInnermost - Mucosal

Stomach Stomach (cont’d)(cont’d)
Divided into 4 partsDivided into 4 parts CardiaCardia FundusFundus BodyBody Pyloric portionPyloric portion
Entrance to stomach is Entrance to stomach is cardiac orificecardiac orifice Controlled by cardiac Controlled by cardiac
sphinctersphincter Exit is the pyloric orificeExit is the pyloric orifice
Controlled by pyloric Controlled by pyloric sphinctersphincter

Stomach Stomach (cont’d)(cont’d)
BodyBody Begins at cardiac Begins at cardiac
notchnotch Contains rugaeContains rugae Terminates at Terminates at
angular notchangular notch Pyloric portionPyloric portion
Consists of pyloric Consists of pyloric antrum and canalantrum and canal
(antrum: cavity or (antrum: cavity or chamberchamber))

Body Habitus - Effect On Body Habitus - Effect On PositioningPositioning
HypersthenicHypersthenic Horizontal and superiorHorizontal and superior Dependent portion above umbilicusDependent portion above umbilicus
AsthenicAsthenic Vertical and inferiorVertical and inferior
SthenicSthenic Generally found between xyphoid process and iliac crestGenerally found between xyphoid process and iliac crest

Functions Of StomachFunctions Of Stomach
Breaks down food chemicallyBreaks down food chemically
Broken down material is called?Broken down material is called? chymechyme
A storage area for further digestionA storage area for further digestion

Small IntestineSmall Intestine Extends from pyloric Extends from pyloric
sphincter to ileocecal sphincter to ileocecal valvevalve Joins large intestine Joins large intestine
at right angleat right angle Digestion and Digestion and
absorption of food absorption of food occur in small occur in small intestineintestine
Approximately __ feet Approximately __ feet in length in adultin length in adult 2222

Small IntestineSmall Intestine Contains same four Contains same four
layers as stomach and layers as stomach and esophagusesophagus
Mucosa contains Mucosa contains projections called villi projections called villi to facilitate digestion to facilitate digestion and absorptionand absorption
Divided into 3 parts:Divided into 3 parts: DuodenumDuodenum JejunumJejunum IleumIleum

DuodenumDuodenum 8 - 10 inches in 8 - 10 inches in
lengthlength
Widest portion of Widest portion of small intestinesmall intestine
Follows a C-shaped Follows a C-shaped coursecourse
Contains 4 Contains 4 regionsregions Superior, Superior,
descending, descending, horizontal, horizontal, ascendingascending

Jejunum And IleumJejunum And Ileum
JejunumJejunum Upper remaining 2/5 of Upper remaining 2/5 of
small bowelsmall bowel IleumIleum
Terminates at ileocecal Terminates at ileocecal valvevalve
Both are gathered into Both are gathered into freely movable loops freely movable loops (gyri)(gyri)
Attached to posterior Attached to posterior abdominal wall by abdominal wall by mesentary mesentary
(the double layer of peritoneum)(the double layer of peritoneum)

Valvulae conniventesValvulae conniventes
Muscular bands Muscular bands encircling small encircling small bowel usually seen to bowel usually seen to traverse bowel wall traverse bowel wall at right angles to at right angles to long axis of the bowellong axis of the bowel

Large IntestineLarge Intestine
What is the main purpose?What is the main purpose? Reabsorbs fluids and eliminate waste productsReabsorbs fluids and eliminate waste products
About _____ feet in length in About _____ feet in length in adultadult 55
Greater in diameter than Greater in diameter than small intestinesmall intestine
Contains same four layers as Contains same four layers as esophagus, small intestine, esophagus, small intestine, and stomachand stomach
Which are?Which are?

Portions Of Large IntestinePortions Of Large Intestine
CecumCecum AscendingAscending
Joins transverse colon Joins transverse colon at right colic flexureat right colic flexure
TransverseTransverse DescendingDescending
Joins transverse colon Joins transverse colon at left colic flexureat left colic flexure
SigmoidSigmoid RectumRectum Anal canalAnal canal

Large IntestineLarge Intestine
The muscular portion contains The muscular portion contains external bands of muscle known as external bands of muscle known as taeniae colitaeniae coli
These bands create a series of These bands create a series of pouches known as?pouches known as? haustrahaustra

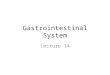
CompareCompare
Haustra
Large bowel
Valvulae conniventes
Small bowel

Variations In Body HabitusVariations In Body Habitus
HypersthenicHypersthenic Colon lies in periphery of abdomenColon lies in periphery of abdomen May need double films!May need double films!
AsthenicAsthenic Intestines are bunched together in lower abdomenIntestines are bunched together in lower abdomen

Radiographic ExamsRadiographic Exams

Contrast MediaContrast Media
Barium sulfateBarium sulfate Water insolubleWater insoluble
Iodinated contrast mediaIodinated contrast media Water solubleWater soluble
Horrible tasteHorrible taste Does not adhere to Does not adhere to
wall of alimentary tractwall of alimentary tract Indicated in case of Indicated in case of
perforationperforation

Contrast MediaContrast Media
AirAir Considered a Considered a
negativenegative contrast contrast Generally Generally
administered by administered by carbon dioxide carbon dioxide crystal ingestioncrystal ingestion
Barium and AirBarium and Air are are often used as a often used as a double contrast agentdouble contrast agent

Preparing pt. for GI Preparing pt. for GI studystudy
Have contrast agents mixed Have contrast agents mixed and ready to goand ready to go
Explain exam to pt.Explain exam to pt.
Ensure pt. has followed Ensure pt. has followed preparation instructions!preparation instructions!

Ensure that footboard is securely Ensure that footboard is securely on table!on table!
Use Use shortshort exposure times exposure times
Use Use high kVphigh kVp to penetrate barium to penetrate barium
Take exposures end of full Take exposures end of full expiration!expiration!
Preparation Preparation cont’dcont’d

Radiography Of Radiography Of EsophagusEsophagus
Can use double or Can use double or single contrastsingle contrast
Barium should flow to Barium should flow to sufficiently coat sufficiently coat esophagusesophagus
Can be done upright or Can be done upright or recumbentrecumbent
Exam will usually be Exam will usually be started with fluoroscopystarted with fluoroscopy

AP or PA ProjectionAP or PA Projection Pt. supine or pronePt. supine or prone Center midsagittal Center midsagittal
plane to cassetteplane to cassette Bottom of cassette Bottom of cassette
should be placed just should be placed just below tip of xyphoidbelow tip of xyphoid
Pt. drinks contrast Pt. drinks contrast before exposure and before exposure and continues drinking continues drinking during exposureduring exposure
Shield!Shield!

RAO or LAO PositionsRAO or LAO Positions Pt should be Pt should be
rotated 35 - 40 rotated 35 - 40 degreesdegrees
Center about 2 Center about 2 inches lateral inches lateral to MSPto MSP
Bottom of Bottom of cassette below cassette below xyphoidxyphoid

RAO or LAO PositionsRAO or LAO Positions
Pt must Pt must drink before drink before and during and during exposureexposure
Use Use shielding!shielding!

Lateral ProjectionLateral Projection Place pt in lateral Place pt in lateral
positionposition Center midcoronal Center midcoronal
plane to cassetteplane to cassette Bottom of cassette Bottom of cassette
below xyphoid below xyphoid processprocess
Pt must drink Pt must drink continuously before continuously before and during exposureand during exposure
Use shielding!Use shielding!

Structures Shown/Film Structures Shown/Film EvaluationEvaluation
Entire Entire barium filledbarium filled esophagus from lower esophagus from lower neck to stomachneck to stomach
Barium should be Barium should be sufficiently sufficiently penetratedpenetrated
Surrounding Surrounding structures should be structures should be visible, visible, not not overpenetratedoverpenetrated
No rotationNo rotation on AP, PA, on AP, PA, or lateral projectionsor lateral projections
Esophagus should be Esophagus should be displayed between displayed between heart and spine on heart and spine on oblique projectionsoblique projections

What is the Valsalva What is the Valsalva Maneuver?Maneuver?
Useful in demonstrating esophageal Useful in demonstrating esophageal varicesvarices
Have pt. first deeply inspireHave pt. first deeply inspire Swallow contrastSwallow contrast Bear downBear down Recumbent positionRecumbent position

Esophageal varicesExtremely dilated sub-mucosal veins in the lower esophagus
Most often a consequence of portal hypertension, commonly due to cirrhosis
Pts with esophageal varices have a strong tendency to develop bleeding

Radiography Of The StomachRadiography Of The Stomach
Upper GI SeriesUpper GI Series Generally consists of fluoroscopy and Generally consists of fluoroscopy and
serial radiographsserial radiographs Single or double contrast Single or double contrast Pt. should follow a low residue diet for Pt. should follow a low residue diet for
2 days prior to exam2 days prior to exam Pt. must be NPO after midnightPt. must be NPO after midnight AP scout generally obtained prior to AP scout generally obtained prior to
examexam

UGI Positioning - UGI Positioning - AP AP ProjectionProjection
PositionPosition SupineSupine
CRCR MSP at L1-L2MSP at L1-L2 Between MSP and left side if using small filmBetween MSP and left side if using small film At MSP if using 14 X 17At MSP if using 14 X 17
StructuresStructures Barium filled fundic portionBarium filled fundic portion Hiatal hernias, if presentHiatal hernias, if present

Single v. Double ContrastSingle v. Double Contrast
Single ContrastSingle Contrast Shows size, shape, Shows size, shape,
and position of and position of stomachstomach
Examines changing Examines changing contour of stomach contour of stomach during peristalsisduring peristalsis
Observe filling and Observe filling and emptying of emptying of duodenal bulbduodenal bulb

Double Double ContrastContrast
Mucosal lining Mucosal lining is well is well visualizedvisualized
Small lesions Small lesions are less easily are less easily obscuredobscured

Compare Single and Double Compare Single and Double ContrastContrast

Which is taken AP and which is Which is taken AP and which is taken PA?taken PA?

UGI Study - PA ProjectionUGI Study - PA Projection
Prone Prone PositionPosition Center at MSP if Center at MSP if
using 14 X 17using 14 X 17 CRCR
Perpendicular to Perpendicular to plane of film at plane of film at level of L1-L2level of L1-L2

UGI study - PA ProjectionUGI study - PA Projection
Structures Structures shown?shown?Size, shape, Size, shape, and relative and relative position of position of stomachstomach
Evaluation:All pertinent anatomy No rotationExposure sufficient to penetrate bariumSurrounding structures visible

UGI Positioning - UGI Positioning - PA ObliquePA Oblique ProjectionProjection
PositionPosition RecumbentRecumbent Body rotated 40 - 70 Body rotated 40 - 70
degreesdegrees Hypersthenic patients Hypersthenic patients
require more rotationrequire more rotation CRCR
Perpendicular to L1-Perpendicular to L1-L2L2
Between vertebral Between vertebral column and elevated column and elevated lateral border of the lateral border of the abdomenabdomen

UGI Positioning - UGI Positioning - PA ObliquePA Oblique ProjectionProjection
StructuresStructures Entire duodenal loopEntire duodenal loop Best image of Best image of
pyloric canal and pyloric canal and duodenal bulbduodenal bulb
EvaluationEvaluation All pertinent All pertinent
anatomyanatomy No superimposition No superimposition
of pylorus and of pylorus and duodenal bulbduodenal bulb
Duodenal bulb and Duodenal bulb and loop in profileloop in profile

UGI Positioning - UGI Positioning - AP ObliqueAP Oblique ProjectionProjection
PositionPosition SupineSupine Right side elevated 30 - 60 degreesRight side elevated 30 - 60 degrees Average about 45 degreesAverage about 45 degrees
CRCR Between vertebral column and left lateral border at L1-L2Between vertebral column and left lateral border at L1-L2
StructuresStructures Fundic portion of stomach filled with bariumFundic portion of stomach filled with barium
EvaluationEvaluation All pertinent anatomyAll pertinent anatomy No superimposition of pylorus and duodenal bulbNo superimposition of pylorus and duodenal bulb Barium filled fundusBarium filled fundus

Lateral ProjectionLateral Projection
PositionPosition Lateral Lateral
recumbent - recumbent - right sideright side
CRCR Level of L1-L2Level of L1-L2 Between Between
midcoronal and midcoronal and anterior of anterior of abdomenabdomen

Lateral ProjectionLateral Projection StructuresStructures
Pyloric canal Pyloric canal and duodenal and duodenal bulb in bulb in hypersthenic hypersthenic patientspatients
EvaluationEvaluation No rotationNo rotation All pertinent All pertinent
anatomyanatomy

Small Bowel Follow Small Bowel Follow ThroughThrough
PreparationPreparation Low residueLow residue diet for 2 days prior when possible diet for 2 days prior when possible NPO after midnight before examNPO after midnight before exam
Examination ProcedureExamination Procedure Scout film obtainedScout film obtained Patient drinks bariumPatient drinks barium Images obtained in prone or supine positionImages obtained in prone or supine position Images begin 15 minutes after barium ingestedImages begin 15 minutes after barium ingested Barium usually reaches ileocecal valve in about Barium usually reaches ileocecal valve in about
2 -3 hours2 -3 hours

Radiography Of Small Radiography Of Small IntestineIntestine
Contrast administration 3 WaysContrast administration 3 Ways OrallyOrally RetrogradeRetrograde
Reflux filling via barium enemaReflux filling via barium enema Direct injection of contrast Direct injection of contrast
through NG tubethrough NG tube EnteroclysisEnteroclysis ( (Radiocontrast is infused through tube Radiocontrast is infused through tube
inserted through nose to duodenum, and images are taken inserted through nose to duodenum, and images are taken in real time as contrast moves through) in real time as contrast moves through)

Small Bowel - AP/PA Small Bowel - AP/PA ProjectionProjection
Patient supine or pronePatient supine or prone CR centered to level of CR centered to level of
L2 for early filmsL2 for early films Iliac crest for later Iliac crest for later
filmsfilms Continue taking Continue taking
radiographs until radiographs until barium reaches barium reaches terminal ileumterminal ileum
Fluoroscopic spot films Fluoroscopic spot films may be taken of may be taken of terminal ileumterminal ileum

Immediate 15 minutes
Small Intestine Follow Small Intestine Follow ThroughThrough

Small Intestine Follow Small Intestine Follow ThroughThrough
30 minutes30 minutes 1 hour

T.I.T.I.
Demonstrates Ileocecal Valve

Radiography Of ColonRadiography Of Colon

Preparation of ColonPreparation of Colon
Pt must take laxative on day prior to Pt must take laxative on day prior to examexam
Pt may have clear liquid day prior to Pt may have clear liquid day prior to examexam
NPO after midnightNPO after midnight
Cleansing enemas may also be indicatedCleansing enemas may also be indicated

Pt. PreparationPt. Preparation Explain exam fully to Explain exam fully to
pt.pt. Use careUse care when when
inserting enema tip!inserting enema tip! Retention-type balloon Retention-type balloon
tipstips should only be should only be inflated under inflated under fluoroscopic controlfluoroscopic control
Barium should only be Barium should only be administered under administered under fluoroscopic control by fluoroscopic control by radiologistradiologist

Single or double contrastSingle or double contrast
Single Single demonstrates demonstrates anatomy and anatomy and tonus tonus (contraction)(contraction) of colon, along of colon, along with most with most abnormalitiesabnormalities
Feces

Double ContrastDouble Contrast
DoubleDouble allows allows visualization visualization of lumen of lumen along with along with any polyps any polyps or lesionsor lesions

AP Projection - Barium AP Projection - Barium EnemaEnema
SupineSupine MSP centered to MSP centered to
cassette cassette CR at iliac crestCR at iliac crest Entire colon must Entire colon must
be includedbe included Two cassettes are Two cassettes are
sometimes sometimes necessarynecessary

PA Projection - Barium PA Projection - Barium EnemaEnema
Pt. pronePt. prone MSP centered to filmMSP centered to film CR at iliac crestCR at iliac crest Entire colon must be Entire colon must be
visualizedvisualized Barium should be Barium should be
sufficiently sufficiently penetrated with penetrated with surrounding surrounding structures visiblestructures visible

PA Axial Projection - BEPA Axial Projection - BE
Pt. pronePt. prone MSP centered to IRMSP centered to IR CR directed 30 - 40 CR directed 30 - 40
degrees caudal to degrees caudal to ASISASIS
Demonstrates Demonstrates rectosigmoid area rectosigmoid area of colonof colon
Area must be Area must be centered to IRcentered to IR

PA Axial Projection - BEPA Axial Projection - BE

AP Oblique Projection - AP Oblique Projection - BEBE
Pt. SupinePt. Supine
Body rotated 35 - Body rotated 35 - 45 degrees45 degrees
CR 1 - 2 in. lateral CR 1 - 2 in. lateral to midline at iliac to midline at iliac crestcrest

AP Oblique Projection - BEAP Oblique Projection - BE
LPO - Right colic LPO - Right colic flexure, ascending flexure, ascending and sigmoid and sigmoid portions of colonportions of colon
RPO - Left colic RPO - Left colic flexure, descending flexure, descending coloncolon
Must demonstrate Must demonstrate entire colonentire colonWhich oblique is this?

PA Oblique Projection (RAO)- PA Oblique Projection (RAO)- Barium EnemaBarium Enema
Pt. pronePt. prone Left side elevated Left side elevated
35 - 45 degrees35 - 45 degrees CR at iliac crest, 1 CR at iliac crest, 1
-2 inches lateral to -2 inches lateral to midline of bodymidline of body

PA ObliquePA Oblique Projection (RAO)- Projection (RAO)- Barium EnemaBarium Enema
Best demonstrates Best demonstrates hepatic flexurehepatic flexure
Ascending and Ascending and sigmoid portionsigmoid portion
Entire colon must Entire colon must be visualizedbe visualized
What projection is What projection is this similar to?this similar to?

PA Oblique (LAO) - BEPA Oblique (LAO) - BE
Pt. pronePt. prone
Right side elevated Right side elevated 35 - 45 degrees35 - 45 degrees
CR to iliac crest, 1 CR to iliac crest, 1 - 2 inches lateral to - 2 inches lateral to midlinemidline

PA Oblique (LAO) - BEPA Oblique (LAO) - BE Demonstrates Demonstrates
descending portion of descending portion of coloncolon
Entire colon must be Entire colon must be visualizedvisualized
What flexture doe this What flexture doe this best demonstrate?best demonstrate? (splenic)(splenic)
What projection is it What projection is it comparable to?comparable to?

Lateral Projection - Barium Lateral Projection - Barium EnemaEnema
Lt. or Rt. lateral Lt. or Rt. lateral recumbent positionrecumbent position
Center midcoronal Center midcoronal plane to filmplane to film
CR enters CR enters midcoronal plane midcoronal plane at level of ASISat level of ASIS

Lateral Projection - Barium Lateral Projection - Barium EnemaEnema
Best Best demonstrates demonstrates rectum and rectum and distal sigmoiddistal sigmoid portions of colonportions of colonRectosigmoid Rectosigmoid area should be area should be centered, no centered, no rotationrotation

Lateral Decubitus Lateral Decubitus Positions - BEPositions - BE
AP or PA AP or PA projectionprojection

Left Lateral Decubitus Left Lateral Decubitus Positions - BEPositions - BE
Up side is air-Up side is air-filledfilled
Must include Must include entire colonentire colon
Air-filled portion Air-filled portion must not be must not be overpenetratedoverpenetrated

UprightUpright Position - Barium Position - Barium EnemaEnema
Demonstrates air-filled flexures and Demonstrates air-filled flexures and transverse colontransverse colon

Chassard Lapine’Chassard Lapine’
Demonstrates rectum, rectosigmoid juntion and sigmoid

Radiographic exam of defecation process under fluoroscopy
Used to evaluate disorders of lower bowel not evident by tests such as colonoscopy or sigmoidoscopy
What is a Defecography? (evacuation proctography)

Defecation
(Having a bowel movement) is a complex action requiring coordination with relaxation and contraction of a large number of muscles
Controlled by nervous system, but is also under voluntary control.

Defecation cont’d
Process is initiated by arrival of stool into rectum
This sensation leads to chain of events which ends in evacuation of stool from anus
Defecation is voluntarily controlled in healthy, normally functioning people.

Defecography is used to Evaluate:
Chronic Constipation Rectal prolapse (walls of rectum protrude
through anus and become visible outside body)
Rectocele (outpouching of rectum)
Fecal incontinence Anismus (inappropriate spasm of anal
sphincter)

DefecographyDefecography
A thickened barium contrast putty is injected into rectum
then excreted by
patient while radiologist watches and videotapes