Embed Size (px)
Citation preview

Radiography (2004) 10, 251e258
Radiographers attitudes to mandatory CPD: acomparative study in the United Kingdomand New Zealand
S.M. Henwooda,), J. Yielderb, D. Flintonc
aMacmillan National Institute of Education, Macmillan Cancer Relief, 89 Albert Embankment,London SE1 7UQ, UKbUNITEC, Auckland, New ZealandcCity University, London, UK
Received 22 March 2004; accepted 25 May 2004
Abstract This study explores the attitudes of radiographers in two countries (UKand New Zealand) to mandatory CPD prior to a mandatory CPD policy being imple-mented. Postal questionnaires were sent to 1739 radiographers (250 in the UK and1489 in New Zealand), in collaboration with the respective professional bodies inboth countries.
The study showed that there is a general ambivalent attitude towards CPD andthere are a number of barriers which individuals identify to explain relatively lowrates of participation in CPD. The study also showed that there is a very restrictedview of what constitutes CPD around attendance at study days and formal activitiesand subsequently less formal activities are not being recognised and valued. Thelack of recording of CPD activity was highlighted along with problems related topoor staffing levels and in places, lack of employer support.
The study will be repeated and attitudes compared two years following the im-plementation of the mandatory CPD policy in both countries.ª 2004 The College of Radiographers. Published by Elsevier Ltd. All rightsreserved.
KEYWORDSContinuing
ProfessionalDevelopment(CPD);
Mandatory;Attitudes;International
comparison
Introduction
CPD in radiography is an issue which has been ex-plored in health care for some time. In the UKand in New Zealand CPD has been a voluntary
) Corresponding author. Tel.: D44-20-7840-4687.E-mail address: [email protected] (S.M.
Henwood).
1078-8174/$ - see front matter ª 2004 The College of Radiographdoi:10.1016/j.radi.2004.05.008
(though expected and some would argue an oblig-atory) aspect of professional practice. In bothcountries, however, in 2001 (UK) and 2003 (NewZealand) legislative change has introduced theissue of mandatory CPD, so that the respectivecountries are now exploring (UK) and implement-ing (NZ) a mandatory policy. The UK expects to im-plement the new policy in 2005 and in NewZealand the introduction of the legislation requiresimplementation by September 2004.
ers. Published by Elsevier Ltd. All rights reserved.

252 S.M. Henwood et al.
In the UK, it is the establishment of the HealthProfessions Council, which will introduce a CPD re-quirement as a condition of ongoing state registra-tion. The exact nature of that requirement is notyet clear, but it has been reported that it willrelate to demonstration of ongoing competenceand will not be purely a points or hours collectingsystem.
In New Zealand, the Health Professionals Com-petency Assurance Act (2003), incorporates man-datory CPD. Medical Radiation Technologists(MRTs) will be required to show a minimum of800 h practice (in each scope of practice) overthe previous three years, satisfactory performancereview over the last 12 months, satisfactory partic-ipation in an approved CPD scheme over the last 12months, compliance with the MRTB code of ethics,a personal medical statement and a personal com-petency statement.
In nursing, Walsh Arneson1 looked at nurses atti-tudes to CPD before and after the implementationof a mandatory policy. In the follow up study twoyears later, she demonstrated that attitudes be-came more positive. This finding is supported byEdwards2,3 in a similar study completed inFlorida, America.
This study conducted by South Bank UniversityLondon, City University London and UNITEC, Auck-land, aims to replicate that study in radiography,in both countries, once the mandate has been im-plemented. This paper presents the first stage,showing attitudes towards CPD prior to the man-date being introduced.
The Society of Radiographers (SOR) and the NewZealand Institute of Medical Radiation Technolo-gists (NZIMRT) were approached to collaborate onthe respective phase of this study to give greatercredibility to the questionnaire and hopefully in-crease the response rates. In both countries theprofessional body endorsed the questionnaire andtheir logo was added to the top of the first page.
Method
A postal questionnaire was used, which was de-signed initially for a UK audience, and was thensubsequently adapted for use in New Zealand toensure appropriate and understandable termi-nology. For example, the name of the professionalbody had to be changed, along with the title ofthe journals sent directly to radiographers. Anotherchange which had to be taken into account was thedifferent career structure and role titles in the twocountries.
In the United Kingdom, a small random sampleof 250 radiographers was selected from the Councilfor Professions Supplementary to Medicine (CPSM)register ( prior to the HPC being established). InNew Zealand, the questionnaire was sent to allMRTs with a current annual practising certificate,which at that time numbered 1489.
Statistical analysis was performed using SPSS�
11.5 for windows. Statistical significance was setat p ¼ 0:05.
Results
In the United Kingdom, of the 250 radiographers inthe sample, 130 returned the questionnaire, con-stituting a 52% response rate. In New Zealand, ofthe 1489 MRTs in the sample, 44 were returned un-delivered due to incorrect postal details. Of the1444 remaining, 598 responses were received, con-stituting a 41% response rate.
Following is a sample of some of the main re-sults from within the quantitative data. Qualita-tive comments are integrated in Discussion. Notethat some responders offered no opinion in certainsections as although still registered as radiogra-phers they either had retired or were no longerworking in radiography, resulting in a reduced ‘n’used in some calculations.
Tables 1e4 present the main demographic datafrom the survey.
Part two of the questionnaire was classified intofive themes, as shown in Table 5.
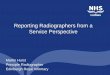
Table 5 reports the results of the questions byclassification into discrete themes, where a scoregreater than four is positive, and less than four isnegative. This is shown differently in Fig. 1 wherethe average deviation from the neutral position isdemonstrated with confidence limits. This figureshows both the differences between NZ and theUK and whether the issue is being viewed in a
Table 1 Gender
% Male Female
UK 13.9 86.1NZ 12.9 87.1
Table 2 Age
% Mean age S.D.
UK 40.15 9.0NZ 38.67 9.9

Radiographers attitudes to mandatory CPD 253
positive or negative light. The confidence bars rep-resent the statistics: if the bars go through 0 thenthere is no statistical difference even though apositive trend may be indicated. Fig. 1 showsthat most of the bars would not reach zero andtherefore there is a true negative/positive feelingaround the theme. Note that the bars are alwayssmaller for the NZ people reflecting the largernumbers in the NZ sample.
From this set of figures, only two of the themesshowed statistical significance in terms of differen-ces between the two countries. These two themeswere ‘support’, t ¼ �2:4, df ¼ 98:6, p ¼ 0:02 and‘outcome’, t ¼ �2:2, df ¼ 544, p ¼ 0:03. In allcases except ‘activity’, New Zealand MRTs are gen-erally more positive in their overall approach/viewtowards CPD, with support and outcome showinga significant difference. The type of questions con-tributing to these two areas included:
Support: whether radiographers get financialsupport, time off, help in CPD selec-tion, information on notice boards,departmental CPD activities etc.
Outcome: the opinion that CPD maintains orenhances competence, improves pa-tient care, maintains confidence, pos-itively affects practice, helps toprotect the public etc.
Two further key questions from the survey askedwhether MRTs/radiographers currently record theirCPD activities and whether or not they thought CPDshould be compulsory, as shown in Tables 6 and 7.
The quantitative data were subject to statisticalanalysis. No significant differences in attitudestowards CPD were established between the twocountries in respect to gender, age or length ofbreaks in service. However, there was a difference(p ¼ 0:002) in the percentage of MRTs/radiogra-phers who have taken a break in their service(higher in New Zealand).
Table 3 Break from service
Break inservice (%)
No break inservice (%)
Length ofbreak ( years)
S.D.
UK 33.8 66.2 5.8 5.3NZ 53.1 46.9 5.8 5.4
Table 4 ‘Type’ of MRT/radiographer
% Diagnostic Therapy Dual qualification
UK 84.8 1.3 13.9NZ 87.6 10.7 1.7
Discussion
The demographic results from the two countrieswere surprisingly similar. In addition, few statisti-cally significant differences were demonstratedwhen comparing the attitudes of MRTs and radiog-raphers in the two countries. One area of concernfor both countries is the overall lack of recordingof CPD, which will be an issue once a mandate is in-troduced and evidence of participation in CPD is re-quired. The percentage of those recording CPD isslightly higher in the UK and this may reflect thelength of time a CPD policy has been in place(1997 as opposed to 2000 in New Zealand) indicat-ing that staff in the UK have ‘got used’ to the ideaand CPD is beginning to be incorporated into theprofessional culture. In addition, from very earlyon it has been anticipated that the UK policy wouldmove from voluntary to mandatory and this mayhave encouraged radiographers to put a recordingmechanism in place. The SOR also made availablea recording mechanism to all members (initiallyat cost, but subsequently free), although studieshave shown that this has not been widely utilised.4
Table 5 Mean scores by CPD classification
Mean score Nationality n Mean scale1�vee8Dve
Total (CPD score) UK 79 4.1NZ 467 4.3
Recording UK 79 3.7NZ 467 3.7
Activity UK 79 4.4NZ 467 4.2
Support UK 79 3.9NZ 467 4.2
Status UK 79 4.3NZ 467 4.5
Outcome UK 79 4.5NZ 467 4.8
Recording
Activity
Support
Status
Outcome
Overall
-1.0
-0.5
0.0
0.5
1.0UKNZ
CPD Classification
Differen
ce fro
m
mid
-p
oin
t o
f scale
Figure 1 CPD classification of themes.

254 S.M. Henwood et al.
Like the number of radiographers recordingCPD, the percentage of radiographers who thinkCPD should be mandatory is also slightly higher inthe UK (57.7% as opposed to 42.3%). Again thismay reflect on the fact that radiographers in theUK have had longer to acclimatise to the idea ofcompulsory CPD. Anecdotally, however, there issome suggestion that the continual delays to theactual implementation of the mandate has raisedquestions as to whether it will happen in practiceand may have contributed to a decrease in atti-tudes towards CPD over time.
The qualitative comments about CPD frequentlyindicated very emotive and polarised attitudesand this paper concentrates on that qualitativedata, giving depth and understanding to some ofthe issues raised and attitudes highlighted. (NewZealand quotes are presented in italic text andUK quotes are presented in bold italic text so thatstaff from the two countries can be identified.)The qualitative comments were clustered intoseveral themes.
Financial implications
There was an expectation that CPD would be eitherfunded in full or assistance with funding wouldbe forthcoming from the employer:
Unless hospitals/departments are willing tofully support CPD and financially aid them it isdifficult to get people to volunteer to do CPD
I think initially the only way forward wouldbe to have clear cut guidelines and a stat-utory obligation from the NHS to providemore funding
Staff in both countries expressed concern at thecost of joining a recognised CPD programme in ad-dition to having to pay for CPD events:
Opposed to the use of the NZIMRT systemfor recording CPD, but support continuing
Table 6 MRTs recording their CPD activity
Country % Recording CPD % Not recording
UK 38.0 62.0NZ 27.2 72.8
Table 7 Should CPD be compulsory?
Country Compulsory (%) Not compulsory (%)
UK 57.7 46.1NZ 42.3 53.9
development. I will not pay to register forthe NZIMRT system.
The society is out of touch and usually hasan ulterior motive in everything and Iwould begrudge paying them any moremoney than I do. I would be tempted toleave rather than pay them for somethingthat they don’t contribute to in any way.
Cost has previously been shown to be a significantbarrier to CPD participation5e12 and clearlyremains to be so in the new century.
Remoteness/access
There is clearly an issue of access for staff workingin remote regions of New Zealand:
Consideration needs to be given to MRTsworking in small or remote areas, whereaccess to courses and funding may be moredifficult.
We are a small rural hospital with only twostaff covering a 24 hour service. This makesour free time very valuable and also meansthat we cannot always (or even often) get toCPD lectures etc, especially as travel isusually involved.
This was not raised as an issue by UK radiographersin this study, but in other studies in the UK dis-tance away from London in particular and otherareas with educational facilities was shown to bean issue.13
Short staffing/sole charge roles
Inadequate staffing and associated high workloadswas raised in both countries as a major stress in re-lation to the ability to participate in CPD activities.
We are too tired, busy, during the day due tobeing short staffed to attend any CPDactivities. We are always filling in due tosickness/holidays, time off can’t be con-firmed for further education, especially dueto staff shortages.
To put it succinctly, unless we can attractstaff or are allowed to appoint/employ extrastaff to release existing staff, I would find itimpossible to entertain the aspirations of CPD.
With the pressure of work and due to staffshortages, CPD is difficult to maintain andit is difficult to get time off for CPD.

Radiographers attitudes to mandatory CPD 255
With over stretched manpower and far toomuch on call e exhaustion is the chiefconcern!
Related to this was the perceived value of CPD andhow high a priority it should be given in the currentclimate of staff shortages. There is no proven linkbetween CPD and any direct improvement in pa-tient care or any link to competence to practice.Some studies have shown links,14e16 at least inthe short term for very specific skills basedcourses, but in terms of a general and broad CPDpolicy, there is no link to improvement in out-comes for the individual, the patient or the profes-sions. Some staff expressed the view that untilsuch a link could be demonstrated, they wouldbe reluctant to put further pressure on existingstaff by taking time out of the working day to un-dertake CPD. It is important to note though thatstaff were not keen to use their own time to under-take CPD activity, which means that in practiceCPD is not being undertaken.
Other commitments
Commitments outside of work lives were oftencited as a reason why CPD was not undertakenmore often by MRTs/radiographers. Interestingly,part-timers saw that their other commitmentswere a larger factor than for full-timers, whilethose working full time saw this as even morereason why outside commitments had precedence:
I’m only working 2 days per week e have twoyoung children and no time to do CPD as itdisrupts home/work balance. As long as Istay reasonably up to date and performwithin the limits of my work environmentthen I feel competent
I have three young children - more time willbe spent on CPD when they are older andmore independent.
CPD is important in order for a professionalto keep up to date with new ideas andtechniques but to make it mandatorywould make it difficult for someone suchas myself (a mother of 2 small children) tokeep the career going
Full time MRTs have minimal free timeanyway and part-timers have other impor-tant commitments (usually children).
Interesting that the last participant did not imme-diately think that those working full time might
also have similar outside commitments, in additionto full time hours.
Studies by Yielder12 and McQuillan17 have shownthat family commitments and personal activitieswere considered to be a moderate barrier, rankingfourth out of seven and fourth out of eight(respectively) in order of importance. (In this studyparticipants were not asked to rank the barriers.)
Time and timing
Many comments were made about the lack of timeavailable and the need for time to be made avail-able for MRTs/radiographers to be involved in CPD.Most felt that employers should allow time duringthe working day. Again, this area generated strongopinions:
I resent doing CPD. I feel very pressured togive up my time to do it. I sometimes readinteresting articles of my own choice. Mymanager is very supportive, finance is given,but as a part timer I am expected to do it inmy time! This is precious to me and I am fullycommitted in it. I do not think CPD enhancespatient care. University graduate MRTs lackpeople skills and experience and are rigid intheir practice. Reading about it doesn’tmake you good at it.
Time should be made available for CPD
.it is difficult to get time off for CPD
The qualitative data in this study suggest that ifprovision was made for study leave by employers(an issue being pursued by the SOR in the UK), thiscould make a difference to individual attitudes.
Radiographic literature on this subject is mixed.McQuillan17 and Henwood and Huggett6 demon-strated that participants had a clear preferencefor attending CPD activities in work time, whereasin Yielder’s12 study, respondents were divided,with many indicating a preference for CPD to beconducted outside of working hours.
Management/employer attitudes andsupport
Radiographers cited both positive and negative ex-perience in terms of attitudes towards their staffsCPD activity. Positively it was said that:
At our practice we do not record CPD buthave a strong commitment to on-goingeducation and all staff are encouraged toattend lectures and conferences whereverpossible. Records are kept of all attendances.

256 S.M. Henwood et al.
I feel very strongly in favour of CPD and amvery privileged to have the support of mymanager and Charge MRT. I realise that I amalso working in an exceptional circumstance,where we can schedule a study day in for allour staff, and we can re-schedule appoint-ments (none of us do call or weekend work).Also, the fact that our managers have alwayssupported staff workshop/study days andthis has become integrated into our year(two to three every year for all staff). It’snot like that in most departments/practices.The benefits for all staff are considerableand not just the radiographers
And negatively:
Where I work, it doesn’t matter where yourgift or skill is, management do not want torecognise it, especially if extra money isinvolved. The bottom line is, managementDON’T CARE!
From what I hear and see, some employersdo not give their staff encouragement tostretch themselves as all
I am in a small departmentemy boss and thedistrict superintendent make no effort toencourage or support any CPD effort onbehalf ofmyself or the other ‘general’ radio-graphers e the sonographers are requiredto attend the main unit for meetings andappraisalsdthey also get study days. Thedepartment nurse whose boss is in the mainunit gets to go on study days. I was a seniorbefore my career break and found when Ireturned that I had more skills than the Supt.III in charge ofme. She is reluctant for me andother radiographers stuck doing generalduties to do any role expansion at all. Wewould enjoy the opportunity for CPD but aretold that most of the things we are inter-ested in are of ‘no benefit’ to our job here!
However there was a general view that:
Bosses/management should see the benefitsof professional development.
Career structure/salary issues
Participants expressed concerns about lack of ca-reer structure and poor salaries and felt that im-provements in both areas may help more staff to‘buy in’ to CPD. For example:
I do strongly feel that if I am expected to doa lot of postgraduate study to maintain my
skills as a ‘professional’ then our wages needa review as they definitely don’t support theview that we are ‘professionals’.
Until MRTs are paid as professionals witha salary that reflects our status and impor-tance in a hospital environment. Otherwisewhy should we bother?
I feel I do a good job which is appreciatedby my patients, although the salary andrecognition fall far short. The membersof the public make me want to keepworking
In two recent studies on retention and job satis-faction by Tubb18 and Blaas,19 it was confirmedthat MRTs in New Zealand think that better promo-tion and CPD opportunities would increase theirlevel of job satisfaction and aid in retention ofstaff, this is supported by Henwood13 in the UK.
Lack of information/understanding
There was generally a poor awareness of thebreadth and scope of activities which constituteCPD. Many of the more negative commentsstemmed from the continued misconception thatCPD is about having to do courses or attend studydays. For example:
The thought of sitting a degree is mind-boggling. I could not do it. As long as thedoctors and radiologists are happy with myfilms then I see no need to sit any exams.
As our profession is very practical, a lot ofacademic work/reading does not necessarilymean we will be better at our job, providinga better service.
Going on a course especially if it is notparticularly relevant to your job does notmake you a good radiographer
There was little conception as to the range of ac-tivities considered to be CPD. This means that inpractice they are unlikely to recognise or valuethe CPD they are already undertaking.
On occasions when the wider aspects of CPD arerecognised, how to record them was in some casescausing difficulty:
I started off with good intentions with thefirst Society software. As time has gone onI am getting more frustrated as to whatand how to record any reading activityas well as occasional tutorials withindepartment.

Radiographers attitudes to mandatory CPD 257
I Don’t Need It
Many participants were adamant that they arecompletely competent and did not need to do CPD:
I am very competent at the job that I do. CPDwould not affect or enhance my competencyin any way.
What worries me is the system run by theNZIMRTdoesn’tallowfora lotofpart-timeolderstaff, who have been doing the same things foryears and have no intention of developing intoaCT/MRI orwhateverMRT.Theydon’t needCPDto x-ray chests and wrists etc.
As long as the doctors and radiologists arehappy with my films then I see no need to sitany exams
CPD is not really necessary for a radiogra-pher in the last 5 years of a career. All thereflective daily practice is automaticallydone mentally as a professional.
This was, as outlined by the comments above, oftenrelated to their particular role or stage of career.
Others were less negative towards CPD, butcould see no need to formalise it:
I feel I don’t need the NZIMRT board todecide whether or not my CPD is up-to-dateor good enough for them, via the paperwork Iput forth. I would struggle to find a radiog-rapher who hasn’t improved their career inone form or another within the last two years
These comments are a reflection of the generalnegativity and apathy that was evidenced frommany of the qualitative comments. Many radiogra-phers cannot see how CPD will improve their job,and unless a positive effort is made to educatethem in regard to why CPD is important, they arelikely to ‘‘be dragged along, screaming and kick-ing, having lost the opportunity for taking controlof their own destinies’’.20( p 24)
Positive attitude
While there were many negative comments in thequalitative section of the questionnaire, therewere also some extremely positive comments insupport of CPD. Some agreed that CPD is a goodidea, but do not accept that mandatory CPD willbe beneficial:
CPD is a good idea, but I do not agree withcompulsory involvement. Staff will onlylearn if they are participating willingly.
This is certainly supported by theory on adult educa-tion. For example, Morrison21 argues that any formof compulsory education, particularly for re-licensure, is incongruent with the nature of bothbeing a professional and an adult. As professionalswe should be self-directed enough to undertake fur-ther training and education from an autonomousrather than a mandatory motivation. However, theargument for mandatory CPD, according to Maple,22
is to protect the public from professionals who aretoo lazy to participate voluntarily, to remove peo-ple who no longer practice, to increase professionalinterchange, and to foster and maintain public con-fidence in the profession. If all radiographers wereparticipating voluntarily there would be no needto implement a mandatory policy.
Positive comments seemed to come mostly frompeople who have already tried it. For example:
I am enjoying doing the CPDe it is not as hardas I thought it would be, and it has encouragedme to be active in ensuringmy own education.I would encourage all MRTs to give it a go.
Taking up study in my 50s was personally veryfulfilling, and humbling too; I had forgottenso many basics over 30 years, and thatshouldn’t have happened.
The main qualifications to these comments werethat it needs to be achievable, flexible and thatthere need to be more opportunities. This feed-back concurs with the results of previous studiesby Yielder,12 McQuillan17 and Henwood.13 Employ-ers and organisations providing CPD programmesand CPD activities will need to provide positive incen-tives for involvement until attitudes change. This willmean information, time, financial support, and theintroduction of flexible and interesting activities.
In terms of personal motivation, the main moti-vating factors identified by McQuillan17 andHenwood13 were the fulfilment of personal self-interest. That is, they had an intrinsic motivationto be involved in CPD. Yielder’s12 study identifiedjob enhancement as the main motivator, followedby personal interest. With the desire to fulfil per-sonal self interest identified as such a high motiva-tor it is imperative to identify those interests inorder to try to fulfil them within CPD if we wantto enhance current CPD activity, both in terms ofparticipation in CPD and positive outcomes fromundertaking any activity.
Conclusion
This study has shown that, on the whole, MRTs/radiographers in New Zealand and the UK have

258 S.M. Henwood et al.
a fairly ambivalent attitude towards CPD. Therewere few differences in attitude identified be-tween the New Zealand and the UK respondents,other than New Zealand MRTs showing a slightlymore positive attitude overall towards CPD. It willbe interesting to see if this impacts on the resultsof the follow up study once mandatory CPD hasbeen implemented. Other minor differences in-cluded that a slightly higher percentage of radiog-raphers in the UK record their CPD and also morethink it should be compulsory, though neither dif-ference was statistically significant.
The qualitative comments from this question-naire were mostly received from New Zealand re-spondents (due to the larger sample size). Theywere grouped into several themes, which werelargely congruent with two other CPD studies con-ducted on MRTs in New Zealand prior to this one.They indicated that there are several factors thatMRTs perceive to be substantial barriers to partici-pating in CPD. However, it is also noted that unlessMRTs can become intrinsically motivated to partic-ipate in CPD, they are likely to create barriers out ofany difficulty encountered. In order for an attitudechange, they need to first come to a full acceptanceof responsibility and accountability for their profes-sional status, excellence and quality in practice,and to support the growth of their profession.
It is anticipated that this study will be repli-cated two years after CPD has become mandatoryin New Zealand, then in the UK, to ascertainwhether there have been any changes in attitudestowards CPD by MRTs/radiographers as was shownby Walsh Arenson in Iowa.
References
1. Walsh Arneson S. Iowa nurses’ attitudes toward mandatorycontinuing education: a two-year follow-up study. J Con-tinuing Educ Nurs 1985;16(1):13e8.
2. Edwards T. An investigation to determine the influence ofmotivational orientation and selected demographic char-acteristics of radiographers on their participation in and
application of continuing professional education, PhDthesis, Orlando, Florida, University of Central Florida; 1990.
3. Edwards T. Continuing education: do mandates matter?Radiol Technol 1993;63(3):184e6.
4. Tallett K. Unpublished study undertaken in Kent, UK;undated.
5. Becher T. The learning professionals. Stud Higher Educ1996;21(1):43e55.
6. Henwood S, Huggett S. Radiographic CPD requirementsda regional study. Radiography 1999;5(1):3e10.
7. Karp NV. Physical therapy continuing education. Part I:perceived barriers and preferences. J Continu Educ HealthProf 1992;12:111e20.
8. Pardee C. Commentary on continuing nursing education:why don’t nurses go? Why don’t they use what they learn?(abstract). ENA’s Nurs Scan Emerg Care 1994;4(1):22.
9. Taylor I, Burgess H. Orientation to self-directed learning:paradox or paradigm? Stud Higher Educ 1995;20(1):87e97.
10. Walker K. Continuing education in the professions: a discus-sion. Radiographer 1995;42(4):99e102, 145e7.
11. Westbrook C. To MSc or not to MScdthat is the question?Synergy 1997;34e5.
12. Yielder J. Transition and beyond: continuing professionaleducation in medical imaging. Auckland: unpublishedMasters thesis, University of Auckland; 1997.
13. Henwood SM. Continuing professional development indiagnostic radiography: a grounded theory study. PhDthesis, London South Bank University; 2003.
14. Alexander MA. Evaluation of a training program in breastcancer nursing. J Continu Educ Nurs 1990;21(6):260e6.
15. Bignell A, Crotty M. Continuing education: does it enhancepatient care? Senior Nurse 1988;8(4):26e9.
16. Loughran C. Reporting of fracture radiographs by radiogra-phers: the impact of a training programme. Br J Radiol1994;67(802):945e50.
17. McQuillan C. Medical imaging: the barriers to continuingprofessional development. Auckland: unpublished researchreport, UNITEC Institute of Technology; 2000.
18. Tubb E. Medical imaging staff retention: a study in to thejob satisfaction of medical radiation technologists in NewZealand. Auckland: unpublished research report, UNITECInstitute of Technology; 2003.
19. Blaas A. An evaluation of the global shortage of medicalradiation technologists. Auckland: unpublished researchreport, UNITEC Institute of Technology; 2003.
20. Henwood S, Benwell M. Continuing professional develop-ment for radiographersda review of the literature. J DiagnRadiogr Imaging 1998;1:17e25.
21. Morrison A. Resisting compulsory continuing professionaleducation. Aust J Adult Commun Educ 1992;32(3):146e9.
22. Maple G. Continuing education for the health sciences. Thevoluntary/mandatory debate. Aust J Adult Educ 1987;27(2):22e8.