Embed Size (px)
Citation preview
RRAJ
LAtoswmoltst
*
†
S
A
1d
adiogenomics Predicting Tumoresponses to Radiotherapy in Lung Cancer
mit K. Das, PhD,* Marcus H. Bell,* Chaitanya S. Nirodi, PhD,† Michael D. Story, PhD,† andohn D. Minna, MD*
The recently developed ability to interrogate genome-wide data arrays has provided invaluableinsights into the molecular pathogenesis of lung cancer. These data have also providedinformation for developing targeted therapy in lung cancer patients based on the identificationof cancer-specific vulnerabilities and set the stage for molecular biomarkers that provideinformation on clinical outcome and response to treatment. In addition, there are now largepanels of lung cancer cell lines, both non–small-cell lung cancer and small-cell lung cancer,that have distinct chemotherapy and radiation response phenotypes. We anticipate that theintegration of molecular data with therapy response data will allow for the generation ofbiomarker signatures that predict response to therapy. These signatures will need to bevalidated in clinical studies, at first retrospective analyses and then prospective clinical trials,to show that the use of these biomarkers can aid in predicting patient outcomes (eg, in the caseof radiation therapy for local control and survival). This review highlights recent advances inmolecular profiling of tumor responses to radiotherapy and identifies challenges and opportu-nities in developing molecular biomarker signatures for predicting radiation response forindividual patients with lung cancer.Semin Radiat Oncol 20:149-155 © 2010 Elsevier Inc. All rights reserved.
ntta
lmloibtbtaafiseohrca
ung cancer represents the leading cause of cancer-relateddeaths in the United States and many Western countries.
lthough many advances have been made in understandinghe molecular pathogenesis and treatment of this disease, theverall 5-year survival rate is 15% to 20%, improving onlylightly over the past 20 years.1 The incidence of lung cancerorldwide continues to rise and is responsible for over 1illion deaths each year.2 A major contributing factor to the
bserved high mortality rate is that approximately 50% ofung cancer patients present with metastatic disease. Addi-ionally, 30% to 50% of the patients who present at an earliertage and are treated initially with surgery or thoracic radio-herapy will die of metastatic recurrence, underscoring the
The University of Texas Southwestern Medical Center, The Hamon Centerfor Therapeutic Oncology Research, Dallas, TX.
Department of Radiation Oncology, Division of Molecular Radiation Biol-ogy, The University of Texas Southwestern Medical center, Dallas, TX.
upported by NIH/NCI the University of Texas SPORE in Lung Cancer 5P50CA 70907 (Dr John D. Minna) and NASA/DOE NASA Specialized Centerof Research (NSCOR) NNJ05HD36G/DEAI0205ER64068 (Dr John D.Minna).
ddress reprint requests to Amit K. Das, PhD, The University of TexasSouthwestern Medical Center, The Hamon Center for Therapeutic On-cology Research, 6000 Harry Hines Blvd., Dallas, TX 75390-8593.
cE-mail: [email protected]
053-4296/10/$-see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.semradonc.2010.01.002
eed for more effective systemic therapy.3 Overall, greaterhan 50% of all lung cancer patients will require radiationherapy (either for thoracic disease or for extrathoracic met-static sites).
Approximately 80% all lung cancers are non–small-cellung cancers (NSCLCs), including adenocarcinoma, squa-
ous-cell carcinoma, and large cell carcinoma. Small-cellung cancer (SCLC) constitutes approximately 15% to 20%f cases, and the overall incidence of SCLC has been decreas-ng over the last several years in the United States.4 SCLC haseen recognized to be much more responsive to radiationherapy than NSCLC for nearly 30 years, but the molecularasis for this responsiveness is unknown. In contrast, NSCLCumors exhibit a wide spectrum of response to radiation ther-py. Some patients have a robust response to radiation ther-py with long-term local control, whereas others relapse ineld even with high-dose treatment. This variance is ob-erved in clinical toxicity as well with some patients experi-ncing severe, acute, and chronic toxicities from treatment;thers experience minimal side effects. Therefore, given theeterogeneity of response to therapy as well as treatment-elated toxicities, a method to reliably predict clinical out-ome would be of significant benefit in this disease. Onepproach to solve this problem is to identify biomarkers that
an predict response to treatment (the development of “per-149
siptl
ToPLpiicsc
twtfuNSSop
y(SSdtNtRal
PTMeDp[mmic
cakt
150 A.K. Das et al
onalized medicine.”) This article reviews recent advances indentifying lung cancer radiation response phenotypes andotential biomarker signatures predictive of tumor responseo radiation alone or integrated with chemotherapy/molecu-arly targeted therapy.
he Heterogeneityf the Radiation Responsehenotype in Lung Cancer
ung cancer cell lines vary widely in their radiation responsehenotypes. This is evidenced by the large observed variance
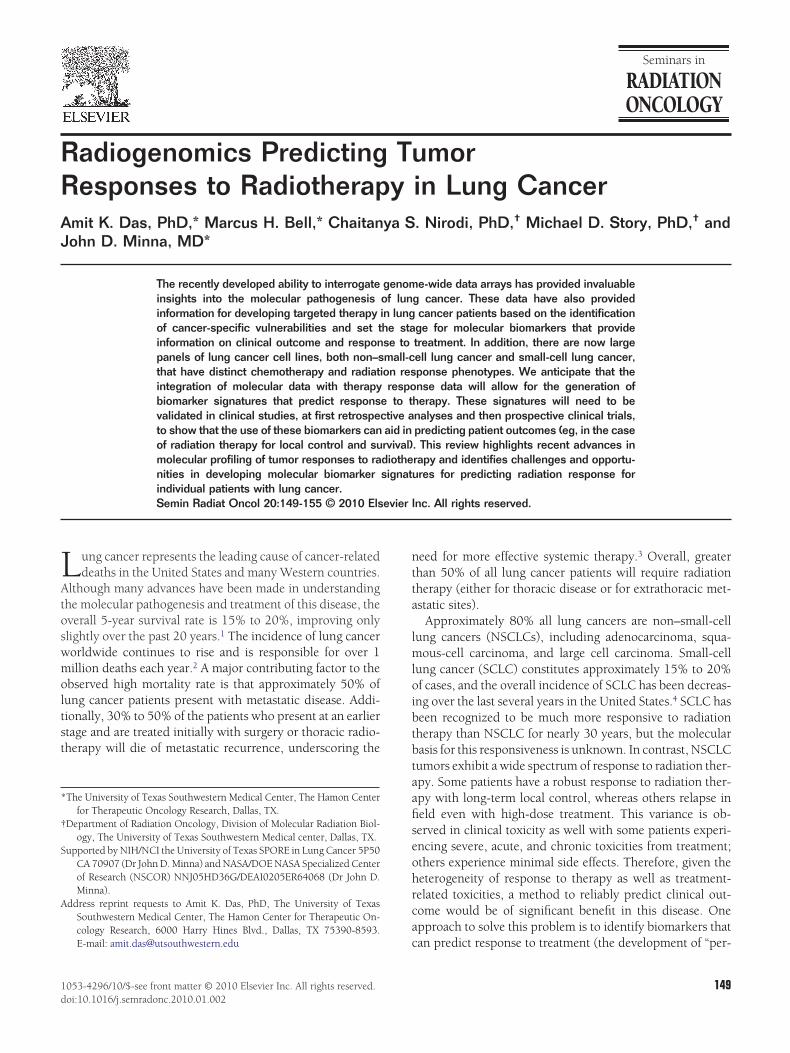
n the survival of lung cancer cell lines after receiving 2 Gy ofonizing radiation (SF2). In a study of 17 human lung cancerell lines (14 NSCLC and 3 SCLC), NSCLC cell lines were lessensitive to radiation and had a broader shoulder in survivalurves than SCLC cell lines as shown in Figure 1.5
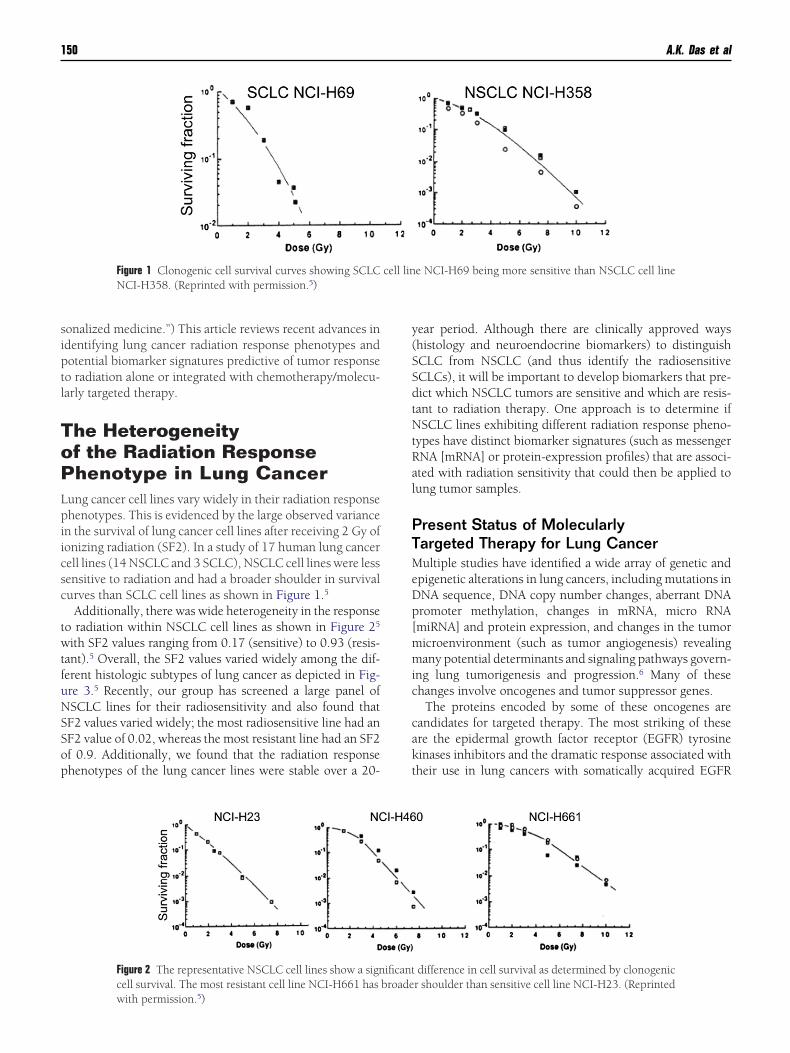
Additionally, there was wide heterogeneity in the responseo radiation within NSCLC cell lines as shown in Figure 25
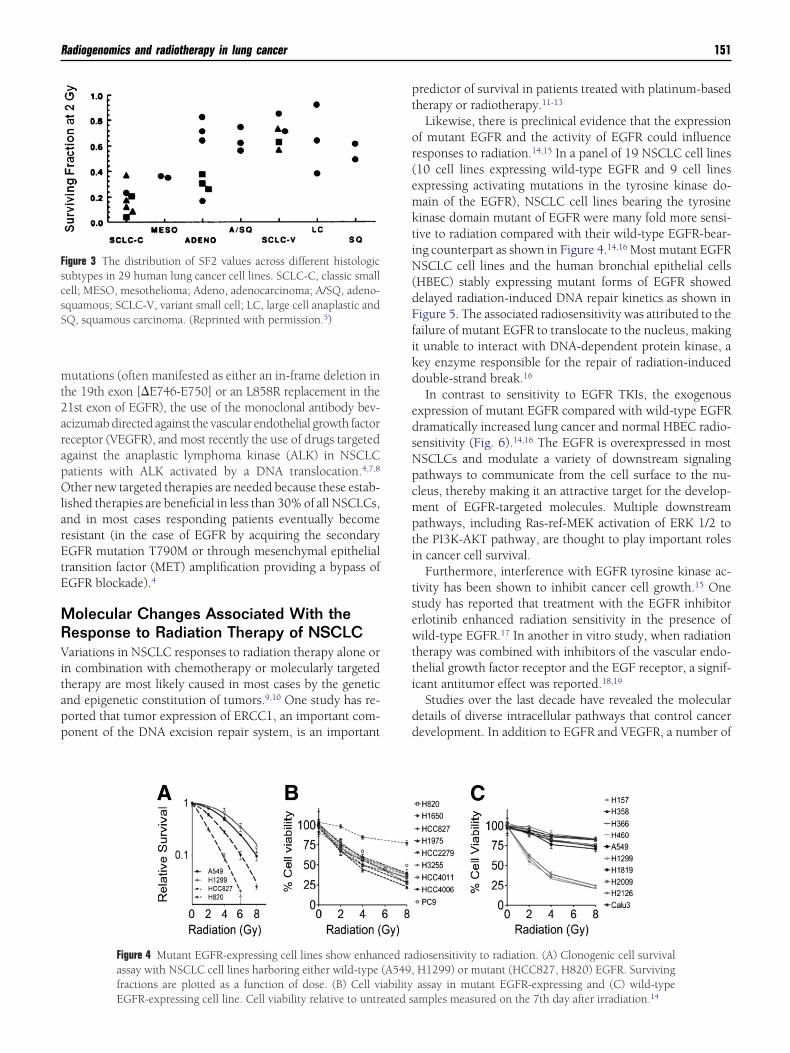
ith SF2 values ranging from 0.17 (sensitive) to 0.93 (resis-ant).5 Overall, the SF2 values varied widely among the dif-erent histologic subtypes of lung cancer as depicted in Fig-re 3.5 Recently, our group has screened a large panel ofSCLC lines for their radiosensitivity and also found thatF2 values varied widely; the most radiosensitive line had anF2 value of 0.02, whereas the most resistant line had an SF2f 0.9. Additionally, we found that the radiation responsehenotypes of the lung cancer lines were stable over a 20-
Figure 1 Clonogenic cell survival curves showing SCLCNCI-H358. (Reprinted with permission.5)
Figure 2 The representative NSCLC cell lines show a signcell survival. The most resistant cell line NCI-H661 has
with permission.5)ear period. Although there are clinically approved wayshistology and neuroendocrine biomarkers) to distinguishCLC from NSCLC (and thus identify the radiosensitiveCLCs), it will be important to develop biomarkers that pre-ict which NSCLC tumors are sensitive and which are resis-ant to radiation therapy. One approach is to determine ifSCLC lines exhibiting different radiation response pheno-
ypes have distinct biomarker signatures (such as messengerNA [mRNA] or protein-expression profiles) that are associ-ted with radiation sensitivity that could then be applied toung tumor samples.
resent Status of Molecularlyargeted Therapy for Lung Cancerultiple studies have identified a wide array of genetic and
pigenetic alterations in lung cancers, including mutations inNA sequence, DNA copy number changes, aberrant DNAromoter methylation, changes in mRNA, micro RNAmiRNA] and protein expression, and changes in the tumoricroenvironment (such as tumor angiogenesis) revealingany potential determinants and signaling pathways govern-
ng lung tumorigenesis and progression.6 Many of thesehanges involve oncogenes and tumor suppressor genes.
The proteins encoded by some of these oncogenes areandidates for targeted therapy. The most striking of thesere the epidermal growth factor receptor (EGFR) tyrosineinases inhibitors and the dramatic response associated withheir use in lung cancers with somatically acquired EGFR
e NCI-H69 being more sensitive than NSCLC cell line
difference in cell survival as determined by clonogenicr shoulder than sensitive cell line NCI-H23. (Reprinted
cell lin
ificantbroade
mt2arapOlarEtE
MRVitapp
pt
or(emktiN(dFfikd
edsNpcmpti
tsewtti
dd
FscsS
Radiogenomics and radiotherapy in lung cancer 151
utations (often manifested as either an in-frame deletion inhe 19th exon [�E746-E750] or an L858R replacement in the1st exon of EGFR), the use of the monoclonal antibody bev-cizumab directed against the vascular endothelial growth factoreceptor (VEGFR), and most recently the use of drugs targetedgainst the anaplastic lymphoma kinase (ALK) in NSCLCatients with ALK activated by a DNA translocation.4,7,8
ther new targeted therapies are needed because these estab-ished therapies are beneficial in less than 30% of all NSCLCs,nd in most cases responding patients eventually becomeesistant (in the case of EGFR by acquiring the secondaryGFR mutation T790M or through mesenchymal epithelial
ransition factor (MET) amplification providing a bypass ofGFR blockade).4
olecular Changes Associated With theesponse to Radiation Therapy of NSCLCariations in NSCLC responses to radiation therapy alone or
n combination with chemotherapy or molecularly targetedherapy are most likely caused in most cases by the geneticnd epigenetic constitution of tumors.9,10 One study has re-orted that tumor expression of ERCC1, an important com-onent of the DNA excision repair system, is an important
igure 3 The distribution of SF2 values across different histologicubtypes in 29 human lung cancer cell lines. SCLC-C, classic smallell; MESO, mesothelioma; Adeno, adenocarcinoma; A/SQ, adeno-quamous; SCLC-V, variant small cell; LC, large cell anaplastic andQ, squamous carcinoma. (Reprinted with permission.5)
Figure 4 Mutant EGFR-expressing cell lines show enhanassay with NSCLC cell lines harboring either wild-typefractions are plotted as a function of dose. (B) Cell vi
EGFR-expressing cell line. Cell viability relative to untreated sredictor of survival in patients treated with platinum-basedherapy or radiotherapy.11-13
Likewise, there is preclinical evidence that the expressionf mutant EGFR and the activity of EGFR could influenceesponses to radiation.14,15 In a panel of 19 NSCLC cell lines10 cell lines expressing wild-type EGFR and 9 cell linesxpressing activating mutations in the tyrosine kinase do-ain of the EGFR), NSCLC cell lines bearing the tyrosine
inase domain mutant of EGFR were many fold more sensi-ive to radiation compared with their wild-type EGFR-bear-ng counterpart as shown in Figure 4.14,16 Most mutant EGFRSCLC cell lines and the human bronchial epithelial cells
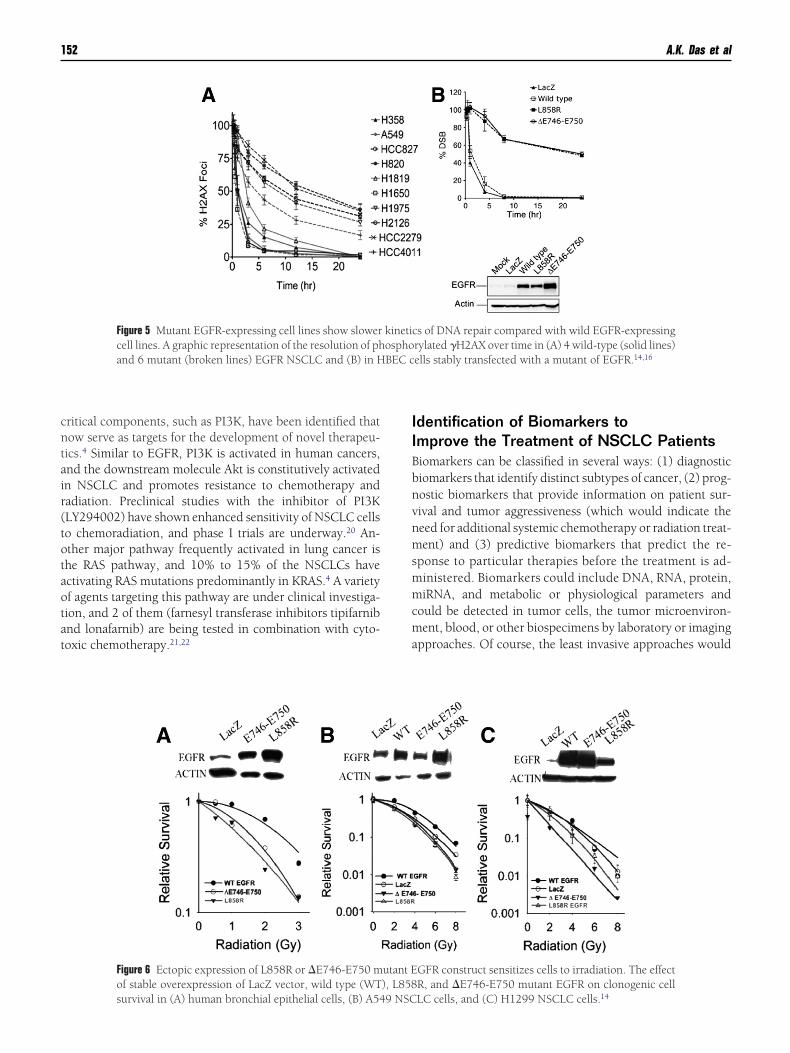
HBEC) stably expressing mutant forms of EGFR showedelayed radiation-induced DNA repair kinetics as shown inigure 5. The associated radiosensitivity was attributed to theailure of mutant EGFR to translocate to the nucleus, makingt unable to interact with DNA-dependent protein kinase, aey enzyme responsible for the repair of radiation-inducedouble-strand break.16
In contrast to sensitivity to EGFR TKIs, the exogenousxpression of mutant EGFR compared with wild-type EGFRramatically increased lung cancer and normal HBEC radio-ensitivity (Fig. 6).14,16 The EGFR is overexpressed in mostSCLCs and modulate a variety of downstream signalingathways to communicate from the cell surface to the nu-leus, thereby making it an attractive target for the develop-ent of EGFR-targeted molecules. Multiple downstreamathways, including Ras-ref-MEK activation of ERK 1/2 tohe PI3K-AKT pathway, are thought to play important rolesn cancer cell survival.
Furthermore, interference with EGFR tyrosine kinase ac-ivity has been shown to inhibit cancer cell growth.15 Onetudy has reported that treatment with the EGFR inhibitorrlotinib enhanced radiation sensitivity in the presence ofild-type EGFR.17 In another in vitro study, when radiation
herapy was combined with inhibitors of the vascular endo-helial growth factor receptor and the EGF receptor, a signif-cant antitumor effect was reported.18,19
Studies over the last decade have revealed the molecularetails of diverse intracellular pathways that control cancerevelopment. In addition to EGFR and VEGFR, a number of
diosensitivity to radiation. (A) Clonogenic cell survivalH1299) or mutant (HCC827, H820) EGFR. Survivingassay in mutant EGFR-expressing and (C) wild-type
ced ra(A549,ability
amples measured on the 7th day after irradiation.14
cntair(totaotat
IIBbnvnmsmmcma
BEC c
152 A.K. Das et al
ritical components, such as PI3K, have been identified thatow serve as targets for the development of novel therapeu-ics.4 Similar to EGFR, PI3K is activated in human cancers,nd the downstream molecule Akt is constitutively activatedn NSCLC and promotes resistance to chemotherapy andadiation. Preclinical studies with the inhibitor of PI3KLY294002) have shown enhanced sensitivity of NSCLC cellso chemoradiation, and phase I trials are underway.20 An-ther major pathway frequently activated in lung cancer ishe RAS pathway, and 10% to 15% of the NSCLCs havectivating RAS mutations predominantly in KRAS.4 A varietyf agents targeting this pathway are under clinical investiga-ion, and 2 of them (farnesyl transferase inhibitors tipifarnibnd lonafarnib) are being tested in combination with cyto-oxic chemotherapy.21,22
Figure 5 Mutant EGFR-expressing cell lines show slowercell lines. A graphic representation of the resolution of phand 6 mutant (broken lines) EGFR NSCLC and (B) in H
Figure 6 Ectopic expression of L858R or �E746-E750 mof stable overexpression of LacZ vector, wild type (WT
survival in (A) human bronchial epithelial cells, (B) A549 NSCdentification of Biomarkers tomprove the Treatment of NSCLC Patientsiomarkers can be classified in several ways: (1) diagnosticiomarkers that identify distinct subtypes of cancer, (2) prog-ostic biomarkers that provide information on patient sur-ival and tumor aggressiveness (which would indicate theeed for additional systemic chemotherapy or radiation treat-ent) and (3) predictive biomarkers that predict the re-
ponse to particular therapies before the treatment is ad-inistered. Biomarkers could include DNA, RNA, protein,iRNA, and metabolic or physiological parameters and
ould be detected in tumor cells, the tumor microenviron-ent, blood, or other biospecimens by laboratory or imaging
pproaches. Of course, the least invasive approaches would
s of DNA repair compared with wild EGFR-expressingrylated �H2AX over time in (A) 4 wild-type (solid lines)ells stably transfected with a mutant of EGFR.14,16
GFR construct sensitizes cells to irradiation. The effectR, and �E746-E750 mutant EGFR on clonogenic cell
kineticospho
utant E), L858
LC cells, and (C) H1299 NSCLC cells.14

ba
osNtgeltigscoa
BTttasNlsbNaN
dgt3sfimrdscc
mngGwc1trvwT
grb(ggif
prrpfnl
tuifm“rStbadtcoct
sdtcscwmotwrnmoNctttds
Radiogenomics and radiotherapy in lung cancer 153
e the most feasible to apply in the clinic and may include thenalysis of biomarkers in circulating tumor cells.
The identification of early diagnostic and predictive bi-markers in NSCLC has the potential to impact on the overallurvival.23,24 A recent study in tumor xenografts derived fromSCLC patients revealed a high degree of similarity of me-
astases with the original primary tumor specimen with re-ard to histology, immunohistochemistry, and overall gene-xpression profiling.25 Although there is a vast amount ofiterature in existence regarding the development of predic-ive biomarkers, most of these signatures have not been val-dated with tumor-derived xenografts. Multiple studies usingenome-wide mRNA microarrays to obtain tumor-expres-ion profiles have been implemented (including in lung can-er), and these have identified potential signatures predictivef chemotherapy sensitivity and resistance.10 Similar studiesre needed for the prediction of radiation response.
iomarkers for Radiation Responsehe ability to predict individual tumor radiosensitivity
hrough the development of a predictive assay is central tohe development of personalized treatment strategies in radi-tion oncology. However, there are no validated biomarkerignatures addressing radiation response phenotypes inSCLC. Recently, 3 independent studies of human cancer
ines have reported sets of genes involved in radiation re-ponse using their models to predict the radiosensitivityased on SF2 values. All groups used cell lines from theCI-60 panel, which includes a spectrum of tumor types andrelatively small number of lung cancer lines (SCLC andSCLC).Torres-Roca et al26 developed a radiation classifier to pre-
ict the radiosensitivity of tumor cell lines based on basalene-expression profiles. Their classifier correctly predictedhe SF2 values in 22 of 35 cell lines. Gene selection identified
novel genes, RbAp48, RGS10, and R5PIA, whose expres-ion values correlated with radiation sensitivity. They con-rmed the gene expression by quantitative real-time poly-erase chain reaction and also biologically validated the
esults by showing that 3 different tumor cell lines were ra-iosensitized by overexpression of RbAp48. However, thistudy had substantial limitations because their panel in-luded only 4 NSCLC cell lines, and they were able to predictorrect SF2 values for only 2 of the 4 NSCLC lines evaluated.
Amundson et al27 reported mRNA signatures obtained byicroarray profiling in response to radiation rather than sig-atures based on basal gene expression. They identified 22enes differentially expressed in cells with low survival at 2y (SF2 �0.2) and 14 genes associated with cell lines thatere more sensitive to 8 Gy (SF8 �0.001) of radiation, in-
luding 5 genes that were common to both. They also found8 genes that were overexpressed in radioresistant cell lineshat were presumed to be competent in double-strand breakepair (because these cell lines have broader shoulder in sur-ival curves). Interesting and unexplained is that this gene setas not enriched with DNA repair genes except XRCC1.
his is contrary to the earlier findings by 2 independent wroups (Ross et al28 and Shankavaram et al29) who haveeported a consistent relationship between tumor-specificasal gene/protein expression pattern and tissue of originorgan of origin) in the NCI-60 panel and were able toroup specific tumor types according to the organ of ori-in.28,29 Amundson et al27 have reported that radiation-nduced gene expression did not substantially differ as aunction of tissue of origin.
Amundson et al27 also identified a set of 25 genes that werereferentially upregulated in tumors with wild-type p53 afteradiation, and 15 of these previously had been reported toespond to radiation in a p53-dependent manner. By com-aring the SF2 and SF8 (survival fraction at 8 Gy) values as aunction of p53 status (wild type vs mutant), the authors didot find any statistically significant difference in tumor cell
ine clonogenic survival.As an extension to the Torres-Roca study,26 Eschrich et al30
ook a systems-biology approach (in which different molec-lar regulatory networks are organized as complex interact-
ng networks) in understanding radiosensitivity and identi-ying radiation-specific markers. Their model, based onRNA expression profiles, identified 10 gene networks or
hubs” (anchored in the different cases by c-Jun, HDAC1,eal [p65 subunit of NFKB], PKC-beta, Sumo-1, c-ABL,TAT1, AR, CDK1, and IRF1). Although none of the genes inhe 10 hubs were directly related to double-strand repairreak, almost all the double-strand break repair genes inter-cted with the network either directly or indirectly. As vali-ation of one of their larger networks with c-Jun as the hub,hey found that when they knocked down c-Jun in 8 differentancer cell lines (lung, colon, and breast cancer), there was anverall trend toward radioresistance, predominantly in lungancers, but not in the breast or colon cancers, implying thathe tissue of origin was important.
They reported a direct correlation between gene expres-ion and radiosensitivity of the lung cancer cell lines andeveloped a model that identified 4 different clusters of geneshat were markers for radiosensitivity. This model also in-luded tumor tissue of origin specificity and KRAS mutationtatus, which interacted with gene expression to play a criti-al role in determining cellular radiosensitivity. This modelas further used to assess its predictive abilities in the re-aining cell lines of the NCI-60 panel and was correct for 5
f the remaining 12 lines. The definition of correct was arbi-rary in that the prediction was scored as accurate if it wasithin 0.10 of the reported SF2 value. These 12-cell lines
epresented 6 different tumor types from leukemia to centralervous system (CNS). The model did not predict for leuke-ia or CNS; it was accurate for 1 each of the 2 breast or
varian cancer cell lines, and was accurate for 2 of the 3SCLC lines. Because of the limited numbers of validation
ell lines, it is not clear whether the model is poorly predic-ive or whether tumor-site specificity is driving the results,he lack of accuracy is likely dependent on both. These au-hors are to be commended for their approach given theirecision to predict an SF2 value, and as more cell lines of apecific origin are examined, the question of site specificity
ill be resolved. It should be noted that none of these differ-
esdb
CLalcsvccrwftaphsc
tibvprtpdcttsppbnofietdcartr
cpway
soat
R
1
1
1
1
1
1
1
1
1
1
2
2
154 A.K. Das et al
nt signatures have been validated in retrospective or pro-pective studies of tumors in patients. Furthermore, suchiscovery-based approaches are potentially associated withiases such as overfitting.31
onclusionsung cancers show dramatically different responses to radi-tion therapy in the clinic, and lung tumor lines also exhibitarge quantitative differences in response to radiation in pre-linical studies. One striking correlation is the radiation sen-itivity of SCLC in patients and in tumor cell lines initro.5,32,33 Other studies in lung cancer and other humanancer cell lines show that there are several biomarkers, in-luding mRNA expression profiles that are associated withadiation sensitivity and resistance. In addition, there areell-known tests of DNA repair and DNA repair–associated
actors that can serve as biomarkers in preclinical systemshat are potentially predictive of response to radiation. Thessociation of EGFR mutations with radiation sensitivity inreclinical in vitro studies is an important new finding thatas potential therapeutic importance. It will be important toee if this radiation response phenotype extends to lung can-ers with EGFR mutations in the clinical setting.
Although this review has focused on biomarkers found inumors, the tumor microenvironment also plays a critical rolen determining intrinsic radiosensitivity. Further studies oniomarkers of the relationship between the tumor microen-ironment and radiation response are ongoing. Another im-ortant component that can potentially influence the tumoradiosensitivity is the cancer stem cell population.34 In addi-ion, with the availability of high-density single-nucleotideolymorphism arrays, germline genome-wide studies of in-ividual variation in response to radiation, including lungancer response and radiation toxicity, are in progress. Al-hough the first studies have focused on mRNA profiles, pro-eomic studies will also be important because mRNA expres-ion is not always correlated with protein expression orosttranslational modification. Of course, it will also be im-ortant to develop signatures predicting response to com-ined modality chemotherapy and radiation therapy. Theext big step will be to test the biomarker signatures devel-ped in the tumor cell lines (such as the mRNA signatures) inrst retrospective and then prospective clinical studies. Forxample, it would be of great interest to determine if signa-ures predicting radiation resistance in NSCLC lines also pre-ict for in-field recurrences of lung cancers (that have re-eived technically appropriate radiation therapy). Likewisessessing biomarker profiles of lung cancers before and afteradiation therapy (eg, at the time of local recurrence) to see ifhe surviving tumor has a signature correlated with radiationesistance would also yield important insights.
Recent developments in high-density genome-wide DNAopy number with high-density single-nucleotide polymor-hism arrays, genome-wide methylation status, and genome-ide miRNA expression status are also being studied for
ssociation with radiation response. Finally, in the next 3 to 5
ears, new DNA sequencing approaches (“NextGen” DNA 2equencing) will allow a comprehensive look at the sequencef the total tumor, and the presence of specific mutations maylso prove to be biomarkers predictive of sensitivity or resis-ance to radiation therapy.
eferences1. Jemal A, Siegel R, Ward E: Cancer statistics, 2006. CA Cancer J Clin
56:106-130, 20062. Parkin DM, Bray F, Ferlay J: Global cancer statistics, 2002. CA Cancer
J Clin 55:74-108, 20053. Shedden K, Taylor JM, Enkemann SA: Gene expression-based survival
prediction in lung adenocarcinoma: A multi-site, blinded validationstudy. Nat Med 14:822-827, 2008
4. Sun S, Schiller JH, Spinola M: New molecularly targeted therapies forlung cancer. J Clin Invest 117:2740-2750, 2007
5. Carmichael J, Degraff WG, Gamson J: Radiation sensitivity of humanlung cancer cell lines. Eur J Cancer Clin Oncol 25:527-534, 1989
6. Sato M, Shames DS, Gazdar AF: A translational view of the molecularpathogenesis of lung cancer. J Thorac Oncol 2:327-343, 2007
7. Sabbatini P, Korenchuk S, Rowand JL: GSK1838705A inhibits the in-sulin-like growth factor-1 receptor and anaplastic lymphoma kinaseand shows antitumor activity in experimental models of human can-cers. Mol Cancer Ther 8:2811-2820, 2009
8. McDermott U, Iafrate AJ, Gray NS: Genomic alterations of anaplasticlymphoma kinase may sensitize tumors to anaplastic lymphoma kinaseinhibitors. Cancer Res 68:3389-3395, 2008
9. Pao W, Kris MG, Iafrate AJ: Integration of molecular profiling into thelung cancer clinic. Clin Cancer Res 15:5317-5322, 2009
0. Minna JD, Girard L, Xie Y: Tumor mRNA expression profiles predictresponses to chemotherapy. J Clin Oncol 25:4329-4336, 2007
1. Hwang IG, Ahn MJ, Park BB: ERCC1 expression as a prognostic markerin N2(�) nonsmall-cell lung cancer patients treated with platinum-based neoadjuvant concurrent chemoradiotherapy. Cancer 113:1379-1386, 2008
2. Fujii T, Toyooka S, Ichimura K: ERCC1 protein expression predicts theresponse of cisplatin-based neoadjuvant chemotherapy in non-small-cell lung cancer. Lung Cancer 59:377-384, 2008
3. Lee HW, Han JH, Kim JH: Expression of excision repair cross-comple-mentation group 1 protein predicts poor outcome in patients withsmall cell lung cancer. Lung Cancer 59:95-104, 2008
4. Das AK, Sato M, Story MD: Non-small-cell lung cancers with kinasedomain mutations in the epidermal growth factor receptor are sensitiveto ionizing radiation. Cancer Res 66:9601-9608, 2006
5. Raben D, Helfrich B, Bunn PA Jr: Targeted therapies for non-small-celllung cancer: Biology, rationale, and preclinical results from a radia-tion oncology perspective. Int J Radiat Oncol Biol Phys 59:27-38,2004 (2 Suppl)
6. Das AK, Chen BP, Story MD: Somatic mutations in the tyrosine kinasedomain of epidermal growth factor receptor (EGFR) abrogate EGFR-mediated radioprotection in non-small cell lung carcinoma. Cancer Res67:5267-5274, 2007
7. Chinnaiyan P, Huang S, Vallabhaneni G: Mechanisms of enhancedradiation response following epidermal growth factor receptor signal-ing inhibition by erlotinib (Tarceva). Cancer Res 65:3328-3335, 2005
8. Shibuya K, Komaki R, Shintani T: Targeted therapy against VEGFR andEGFR with ZD6474 enhances the therapeutic efficacy of irradiation inan orthotopic model of human non-small-cell lung cancer. Int J RadiatOncol Biol Phys 69:1534-1543, 2007
9. Reck M, Crino L: Advances in anti-VEGF and anti-EGFR therapy foradvanced non-small cell lung cancer. Lung Cancer 63:1-9, 2009
0. Brognard J, Clark AS, Ni Y: Akt/protein kinase B is constitutively activein non-small cell lung cancer cells and promotes cellular survival andresistance to chemotherapy and radiation. Cancer Res 61:3986-3997,2001
1. Downward J: Targeting RAS signalling pathways in cancer therapy. NatRev Cancer 3:11-22, 2003
2. Isobe T, Herbst RS, Onn A: Current management of advanced non-

2
2
2
2
2
2
2
3
3
3
3
3
Radiogenomics and radiotherapy in lung cancer 155
small cell lung cancer: Targeted therapy. Semin Oncol 32:315-328,2005
3. Sung HJ, Cho JY: Biomarkers for the lung cancer diagnosis and theiradvances in proteomics. BMB Rep 41:615-625, 2008
4. Singhal S, Miller D, Ramalingam S: Gene expression profiling of non-small cell lung cancer. Lung Cancer 60:313-324, 2008
5. Fichtner I, Rolff J, Soong R: Establishment of patient-derived non-smallcell lung cancer xenografts as models for the identification of predictivebiomarkers. Clin Cancer Res 14:6456-6468, 2008
6. Torres-Roca JF, Eschrich S, Zhao H: Prediction of radiation sensitivityusing a gene expression classifier. Cancer Res 65:7169-7176, 2005
7. Amundson SA, Do KT, Vinikoor LC: Integrating global gene expres-sion and radiation survival parameters across the 60 cell lines of theNational Cancer Institute anticancer drug screen. Cancer Res 68:415-424, 2008
8. Ross DT, Scherf U, Eisen MB: Systematic variation in gene expression
patterns in human cancer cell lines. Nat Genet 24:227-235, 20009. Shankavaram UT, Reinhold WC, Nishizuka S: Transcript and proteinexpression profiles of the NCI-60 cancer cell panel: An integromicmicroarray study. Mol Cancer Ther 6:820-832, 2007
0. Eschrich S, Zhang H, Zhao H: Systems biology modeling of the radia-tion sensitivity network: A biomarker discovery platform. Int J RadiatOncol Biol Phys 75:497-505, 2009
1. Ransohoff DF: Rules of evidence for cancer molecular-marker discov-ery and validation. Nat Rev Cancer 4:309-314, 2004
2. Bayman NA, Sheikh H, Kularatne B: Radiotherapy for small-cell lungcancer-where are we heading? Lung Cancer 63:307-314, 2009
3. Carney DN, Mitchell JB, Kinsella TJ: In vitro radiation and chemother-apy sensitivity of established cell lines of human small cell lung cancerand its large cell morphological variants. Cancer Res 43:2806-2811,1983
4. Milas L, Hittelman WN: Cancer stem cells and tumor response totherapy: Current problems and future prospects. Semin Radiat Oncol
19:96-105, 2009