Embed Size (px)
Citation preview

Radiofrequency Lesions in Management of Pain
RADIOFREQUENCY LESIONING IN CHRONIC PAINNeuro-ablative techniques in clinical practice are directed to block the nerve impulse carrying
pain sensation to/ or inside the central nervous system to relief pain. This can be done through:1. Surgical destruction.2. Chemical destruction.3. Cryocoagulation.4. Lesioning with electric current, induction heating.5. Focused ultrasound.
PHYSICS OF RADIOFREQUENCYThe circuit consists of an active electrode, which delivers the current; a method for measuring
tissue temperature (thermistor or thermocouple); a radiofrequency generator; and a passive electrode with a large surface area. Current in the region of the active electrode generates heat. The heat generated is a function of the amount of current per unit area (current density) that flows in the region of the electrode. The active electrode itself does not generate heat but is heated as a result of local tissue warming. The current flows from the active to the passive electrode. Because of the much greater surface area of the passive electrode, the current density is much less. Therefore, heating and tissue damage do not usually occur at the passive electrode.
Heating of the active electrode is an important safety feature of this system, because tissue damage is related to the temperature generated. The newer electrodes have a low thermal coefficient, meaning that the electrode absorbs heat well and heats rapidly, leading to a faster response and improved safety of the system. Excessive heating causes more diffuse and permanent tissue damage. It is possible to boil tissues, and these tissues may then adhere to the electrode and be avulsed when the electrode is removed. The thermocouple lends itself better to miniaturization than the thermistor and is therefore more widely used.
Most electrodes are available in a number of sizes and lengths. Both reusable and disposable needles are used. Most have varying lengths of the exposed tip, and the electrode must be selected for the desired purpose. For example, an 18-gauge reusable electrode with a 2-mm exposed tip is suitable for radiofrequency denervation of the trigeminal nerve, whereas a 22-gauge electrode with a 4-mm exposed tip is appropriate for lumbar facet denervation. In some neurosurgical procedures, curved needles are used to generate eccentric lesions.Lesion Characteristics
It is critical to control lesion size. The size and consistency of the lesion are governed by four major factors: 1. Temperature generated: At higher temperatures, the local tissue reaction is greater. 2. Rate of thermal equilibrium: If there is more rapid equilibrium between tissues, the lesion
is more uniform. Conversely, if there is slow and incomplete equilibrium, the lesion is erratic. Usually thermal equilibrium is complete by 60 seconds. The lesion size initially rises exponentially with time but becomes independent of time after approximately 30 seconds (=90 seconds) .
3. Electrode size and configuration: Larger electrodes generate larger lesions. For example, an 18-gauge electrode generates a lesion with a radius of 2.2 mm, whereas a 22-gauge electrode generates a radius of only 1.9 mm. Larger electrodes generate bigger lesions but at the expense of more tissue trauma on insertion, unwanted neural destruction, and larger reversible zones.
4. Local tissue characteristics: Lesions in tissues in contact with tissues of low electrical resistance such as blood and cerebrospinal fluid may be reduced or irregular in size and shape. Blood may also act as a heat sink, removing heat from the area and thereby limiting local tissue temperature rise and lesion size. The size of the lesion does not correlate well with either the time or the power used, because
the temperature generated depends on tissue characteristics. The lesion generated is usually an inverted cone. In vitro evidence suggests that the lesion radius is maximal at the part of the exposed electrode farthest from the tip. The actual tip may not even be incorporated in the
Professor M. Omar Tawfik. MD October, 2003
1

Radiofrequency Lesions in Management of Painlesion, and this has important clinical implications. Nerves in contact with the tip may be only partially blocked, and an electrode placed tangential to the nerve generates a more effective lesion. The effect on tissues depends on the temperature generated. Above 45°C, irreversible tissue injury occurs. Between 42° and 45°C, temporary neural blockade occurs. In general, the larger the lesion, the larger is the zone of reversibility.
The histologic appearance of lesions generated by radiofrequency is one of local tissue burn. Nerve architecture is destroyed. After the lesion is created, wallerian degeneration becomes apparent. The perineurium may also be destroyed. In radiofrequency lesioning, unlike cryoneurolysis, neuroma formation is possible. Clinically, it appears that there is relative selectivity for small, unmyelinated fibers at lower temperatures. Therefore, by limiting the temperature, it may be possible to damage pain fibers selectively. Technique
Minimal sedation is used so that the patient can participate fully and accurately report the stimuli. All of the equipment, particularly the cables and thermocouple or thermistor, is checked before beginning the procedure. The lesion parameters, especially the maximal temperature, are preset. The radiofrequency probe must be of the appropriate size and length for the needle. In particular, the correct exposed tip length, needle diameter, and length are critical in improving the efficacy of the procedure and reducing the risk of inadvertent tissue injury. Fluoroscopy is mandatory.
The most common reason for failure to generate a lesion is a poor electrical connection, usually related to cable damage. Occasionally, the insulation on the active electrode is disrupted, with a subsequent reduction of current density and poor lesion generation. This may also lead to lesions further up along the shaft in other tissues traversed by the needle. Poor connection may also occur at the passive electrode, leading to poor conduction or even local tissue burning. The newer machines all measure impedance and can help isolate the source of the problem. Very high impedance (>2000 Ω) suggests electrical disconnection, whereas very low impedance (<200 Ω) implies a short circuit.
Inadequate temperature generation may occur if the temperature selected is too low. Lesions tend to be smaller when lower temperatures are used. Poor needle placement accounts for many technical failures. Newer lesion generators incorporate an electrical nerve stimulator to help locate the nerve.
NERVE LESION BY RADIOFREQUENCY.The advantages for the utilization of the radiofrequency techniques versus other neuro-
destructive methods are that:1. The lesion size can be adequately controlled.2. Good monitoring of the lesion temperature can be performed with a thermal coupled
electrode.3. Good placement of electrode is facilitated with electrical stimulation and impedance
monitoring.4. The ability to utilize the same radiofrequency cannula for different types of spinal axis
lesions.5. The ability to perform radiofrequency lesions under local or sedative anesthesia.6. Rapid recovery period following radiofrequency lesion.7. Low incidence of morbidity and mortality following properly applied radiofrequency
lesions.The lesion generators frequencies are of approximately 500 kilocycle. Frequencies in this
range are advantageous in producing uniform and better circumscribed lesions. Direct current (0 frequency) can produce thermal lesion. It is usually uncontrollable with
ragged edge. It depends on electrolysis and consequent depolarization and gas formation. Inadvertent boiling and charring, result in sticky electrodes that will produce damage and bleeding with its removal.
Galvanic current can produce electric lesion which is painful.
Professor M. Omar Tawfik. MD October, 2003
2

Radiofrequency Lesions in Management of PainRadiofrequency current is a high frequency, low
energy current that can build an electromagnetic field between electrodes. This will make the free charged ions move back and froth in a radiofrequency movement in fluid media called "ionic dissipation". The friction will produce rise of temperature that will be transmitted and concentrated in the active tip of electrode which is able to measure it.
In order to reach such arrangement, the 2 electrodes emerging from the radiofrequency generator are called the active electrode and the dispersive electrode.
The active electrode is inserted into the body for lesion making. The dispersive electrode should have a surface area at least 100 times larger than the
active electrode (150 cm2).In homogenous tissue, electrical stabilization occurs in 45 seconds which is sufficient to
produce lesion. In fluid media (CSF, blood, or local anesthetic solution) the rise of temperature is slow that failure to make lesion is probable an should not be done if CSF or blood is present in the area of lesion. On the other hand the rise of temperature in bone or disc tissue is rapid and lesion in this area it is unpredictable.
CLINICAL APPLICATIONS OF RADIOFREQUENCY LESIONSFirst, the clinician performing the lesions must have: Experience working under fluoroscopic x-ray guidance. Understanding of the three-dimensional anatomy of the spinal axis. The ability to coordinate hand-to-eye coordination Years of experience are required to become skilled in the use of radiofrequency and to
perform safe and effective thermal lesions. Only modern thermal-coupled electrode systems should be utilized and it is recommended
that disposable cannula systems be used whenever possible. The electrode systems as well as the wires that attach to the radiofrequency generator
should be gas-sterilized prior to operative procedures. It is not recommended that heat sterilization be used for the electrodes or cord systems. Chemical agents to be avoided (if possible) for electrode systems sterilization.
Patient selection is the most important factor for a positive outcome. Usually doing aradiofrequency lesion is indicated when drug treatment fails, and a positive results came from prognostic block.
One must be careful with patients having drug dependence or habituation that may contribute to success failure. A patient with psychological trait with operant learning may force failure of management. Patient’s expectations may overshoot the realistic outcome. Patients should be aware about the procedure and sign a consent covering the outcome, sequelae and possible complications.
A variety of pain syndromes have a high success rate with radiofrequency applications: Trigeminal neuralgia: Trigeminal gangliotomy. Intractable malignant pain: Percutaneous lateral cordotomy, and spinal gangliotomy. Pain due to vertebral pathology: Facet denervation, discogenic pain. Cervical syndromes and cervico-brachialgia. Intercostal neuralgia. Percutaneous sympathectomy, particularly, cervical and thoracic sympathectomy.
CRANIAL RADIOFREQUENCY
Professor M. Omar Tawfik. MD October, 2003
3

Radiofrequency Lesions in Management of PainTRIGEMINAL NEURALGIATrigeminal neuralgia is an
excruciatingly painful condition characterized by:
1. Paroxysms of shooting electric pain with completely free intervals in between.
2. Pain is usually spontaneous, but can also be provoked by light touch to certain trigger areas, chewing, swallowing, or change of temperature.
3. Pain usually starts in a restricted area in the supply of Mandibular or/ and Maxillary (3:2), or rarely the ophthalmic division (1-2%).
4. Usually no neurological signs are present, with the patient is completely normal in between the attacks, except in secondary trigeminal neuralgia.
It is more common in females than males. The intensity, and frequency of pain increases by time.
About 69% of patients can be controlled by carbamazepine, while 6% can be controlled but with serious side effects. 25% of patients are usually uncontrollable and need an interventional treatment.
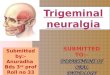
Trigeminal Gangliotomy1. A 10 cm, 2mm active tip, 22 gauge electrode is introduced
percutaneously through the foramen oval under fluoroscopic guidance. The foramen is visible between the mandible and maxillary sinus in a submento-vertical view with an angle of 20o.
2. Just before intering the foramen, I.V. Propofol 1.2 mg/kg is given.
3. Lateral fluoroscopy is attained, and the electrode is advanced until it is just passed the angle made by the pars petrosa and clivus.
4. In the cave of Meckel, the sensory arrangement is that the mandibular branches have an antero-lateral while the ophthalmic has a postero-medial arrangement.
5. The stylet is removed (CSF usually flows), and replaced with RF electrode.
6. The mandibular nerve has some motor fibers. If the nerve is stimulated at 2 Hz with 0.1 to 1.5 V, the muscle contraction of the lower mandible is observed. This is also a way of verifying that the needle is passed through the foramen ovale and is on the retrogasserian rootlets. If the first and second divisions are affected, there should be no motor response.
The second step is to seek paresthesia for proper localization. A stimulation at 50 to 100 Hz is given with 0.1 to 0.5 V. If the needle is properly located, there will be a tingling-like sensation or electric-like paresthesias in the innervation of that branch in the face. If this sensation is obtained after 0.5-V stimulation, then the needle should be redirected to
Professor M. Omar Tawfik. MD October, 2003
4

Radiofrequency Lesions in Management of Painget the same response at a lower voltage. However, it should be kept in mind that there might be residual sensorial deficits from a previous lesioning.
When the electrode is adjusted for localization, it should also be remembered that the gasserian ganglion and its retrogasserian rootlets lie on a plane running from a superomedial to inferolateral direction. If there is a motor response, it means that the needle is too lateral, and for a better response, it should be more medial.
After stimulation is completed, the physician should again rule out if the needle is in a vessel or not. If blood is aspirated, the needle position should be adjusted. If blood is still aspirated, the procedure should be terminated and a second attempt should be made another day. Impedance monitoring is not essential for trigeminal ganglion lesioning, but if used, it should be 150 to 350 Ω for rootlets bathing in the CSF and 1000 Ω if it is in a non-neural tissue.Lesioning
7. Propofol is re-injecting to put the patient in light sleep, and lesioning is done by increasing temperature, starting by 60oC for 90 seconds, and the sensitivity of the skin and cornea are tested. Several types of electrodes may be used for lesioning, such as cordotomy-type electrodes and trigeminal electrodes with the Tew needle and the Racz-Finch curved-blunt needle.
8. The lesioning is repeated with increasing temperature (70oC), until stimulation voltage threshold is increased 3-4 folds. Each lesioning is done under propofol anesthesia. The patient must be well informed and co-operative during assessment in between lesioning. Expected success rate is 96 %.
GLOSSOPHARYNGEAL NERVE LESIONING:The glossopharyngeal nerve contains both motor and
sensory fibers. The motor fibers innervate the stylopharyngeus muscle. The sensory portion of the nerve innervates the posterior third of the tongue, the palatine tonsil, and the mucous membranes of the mouth and pharynx. Special visceral afferent sensory fibers transmit information from the taste buds of the posterior third of the tongue. Information from the carotid sinus and body, which help control blood pressure, pulse, and respiration, are carried via the carotid sinus nerve, a branch of the glossopharyngeal nerve. Parasympathetic fibers pass via the glossopharyngeal nerve to the otic ganglion. Postganglionic fibers from the ganglion carry secretory information to the parotid gland.
The glossopharyngeal nerve exits the jugular foramen near the vagus and accessory nerves and the internal jugular vein. All three nerves lie in the groove between the internal jugular vein and internal carotid artery. Inadvertent puncture of either vessel during glossopharyngeal nerve block can result in intravascular injection or hematoma formation. Even small amounts of local anesthetic injected into the carotid artery at this site can produce profound local anesthetic toxicity.
TECHNIQUE One landmark for glossopharyngeal nerve block is the styloid process of the temporal bone.
This structure is the calcification of the cephalad end of the stylohyoid ligament. Although usually easy to identify, when ossification is limited, it may be difficult to locate with the exploring needle.
The patient is placed in the supine position. An imaginary line is visualized running from the mastoid process to the angle of the mandible. The fluoroscope should be placed in an oblique position and directed toward the area of the mandible and the mastoid process. The styloid process should lie just below the midpoint of this line. The skin is prepared with antiseptic solution. A 22-gauge,
1.5-inch needle attached to a 10-mL syringe is advanced at this midpoint location in a plane perpendicular to the skin.
Professor M. Omar Tawfik. MD October, 2003
5

Radiofrequency Lesions in Management of PainThe styloid process should be encountered within 3 cm. After contact is made, the needle is withdrawn and walked off the styloid process posteriorly. As soon as bony contact is lost and careful aspiration reveals no blood or cerebrospinal fluid.
Blunt RFTC needle is inserted until bone contacted and walked off bone posteriorly. Sensory and motor stimulation is done as per routine, pulsed electrode magnetic fields (pEMF) is done at 42°C with three cycles of 120 seconds, after injection of 0.5 lidocaine 2%.
COMPLICATIONSThe major complications associated with glossopharyngeal nerve block are related to trauma
to the internal jugular vein and carotid artery. Hematoma formation can cause a significant problems for the patient. Blockade of the motor portion of the glossopharyngeal nerve can result in dysphagia
secondary to weakness of the stylopharyngeus muscle. With numbness of half of the pharynx and the larynx, ingestion and swallowing are often
severely compromised. Dysesthesias in the area of anesthesia" anesthesia dolorosa" can be worse than the patient’s original pain and is often times harder to treat.
In chemical neurolysis or neurodestructive procedures: The vagus nerve is inadvertently blocked, as it often is during glossopharyngeal nerve
block, dysphonia secondary to paralysis of the ipsilateral vocal cord may occur. Reflex tachycardia secondary to vagal nerve block is also observed in some patients.
Inadvertent block of the hypoglossal and spinal accessory nerves during glossopharyngeal nerve block results in weakness of the tongue and trapezius muscle.
Often, patients with pharyngeal cancer will have undergone radical neck dissection and the sternocleidomastoid muscle will have been removed. This makes identification of the styloid process much easier, since this particular bony landmark is now almost subcutaneous, allowing this block to be performed easily.
SPHENOPALATINE GANGLION SPGThe SPG is the largest group of neurons outside the cranial
cavity. It lies in the pterygopalatine fossa, which is approximately 1 cm wide and 2 cm high and resembles a “vase” on a lateral fluoroscopic view. The pterygopalatine fossa is bordered anteriorly by the posterior wall of the maxillary sinus, posteriorly by the medial plate of the pterygoid process, medially by the perpendicular plate of the palatine bone, and superiorly by the sphenoid sinus, and laterally it communicates with the infratemporal fossa.
The foramen rotundum, through which the maxillary branch of the trigeminal nerve passes, is located on the superolateral aspect of the pterygopalatine fossa. The ganglion within the fossa is located posterior to the middle turbinate of the nose and lies a few millimeters deep to the lateral nasal mucosa. Also contained in the fossa is the maxillary artery and its multiple branches.
As a neural center, the ganglion has sensory, motor, and autonomic components. The sensory fibers arise from the maxillary nerve, pass through the SPG, and are distributed to the nasal membranes, the soft palate, and some parts of the pharynx. A few motor nerves are also believed to be carried with the sensory trunks.
The autonomic innervation is more complex. The sympathetic component begins with preganglionic sympathetic fibers originating in the upper thoracic spinal cord, forming the white rami communicantes, coursing through the sympathetic ganglion. The postganglionic fibers then join the carotid nerves before branching off and traveling through the deep petrosal and vidian nerves. The postganglionic sympathetic nerves continue their path through the SPG on their way to the lacrimal gland and the nasal and palatine mucosa.
Professor M. Omar Tawfik. MD October, 2003
6

Radiofrequency Lesions in Management of PainINDICATIONSCurrently, SPGB is used for relief of facial pain and headache: Sphenopalatine neuralgia. Trigeminal neuralgia. Headaches:
o Cluster.o Migraine.
Atypical facial pain. Herpes zoster ophthalmicusSphenopalatine neuralgia, described a unilateral facial pain at the root of the nose that
sometimes spread toward the zygoma and extended back to the mastoid and occiput. This pain is typically associated with the parasympathetic features such as lacrimation, rhinorrhea, or mucosal congestion.
Trigeminal neuralgia is also an indication for SPGB. The SPG is directly connected to the maxillary branch of the trigeminal nerve via the pterygopalatine nerves.
Cluster headache when patients fails to respond to oral and parenteral dosing and are forced to seek alternative methods for pain control, blockade of the SPG has been used in such cases, with varying success.
Atypical facial pain, when it is unilateral and described as constant, aching, and burning; and is not confined to the distribution of a cranial nerve. It may involve the entire face, scalp, and neck. The pain may have a sympathetic component, which makes the SPGB ideal, because the postganglionic sympathetic nerves pass through the ganglion.
TECHNIQUE:Rule out paranasal sinus infections, which can cause irritation of the ganglion resulting in
pain. Procedure is done under conscious sedation, and electrocardiograph, sphygmomanometer,
and pulse oximetry monitoring.
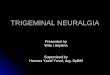
The patient lies supine with the head inside the C-arm. The anterior position view is then taken. The beam of the C-arm is directed toward one side of the face just below the orbit. B, This radiographic image shows the postero-anterior view of the front of the face, identifying the orbit and maxillary sinus.
Professor M. Omar Tawfik. MD October, 2003
7

Radiofrequency Lesions in Management of Pain
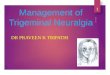
Site of Needle EntryThe needle is inserted under the zygoma in the coronoid notch. A lateral view of the upper
cervical spine and the mandible is obtained and the head is rotated until the rami of the mandible are superimposed one on the other. The C-arm is moved slightly cephalad until the pterygopalatine fossa is visualized. It should resemble a vase when the two pterygopalatine plates are superimposed on one another and are located just posterior to the posterior aspect of the maxillary sinus.Technique of Needle Entry
The needle is directed medial, cephalad, and slightly posterior toward the pterygopalatine fossa. An anteroposterior view confirms the proper direction and positioning of the needle. The tip of the needle should be advanced until it is adjacent to the lateral nasal mucosa. If resistance is felt at any time, the needle must be slightly withdrawn and redirected. The operator takes care to avoid advancing the needle through the lateral nasal wall. Injection of Local Anesthetic
Once it is properly positioned, 1 to 2 mL of local anesthetic is injected, with or without steroid. As much as 5 mL of local anesthetic can be injected for a diagnostic block.Radiofrequency Thermocoagulation Lesioning
Lesioning of the SPG can be performed with either RFTC or pulsed electrode magnetic fields (pEMF). With radiofrequency (RF), sensory testing is done after the needle is correctly placed radiographically.
Paresthesia should be felt at 0.5 to 0.7 V at 50 Hz when the needle is correctly situated on the ganglion:
If the paresthesia is felt in the upper teeth, the maxillary branch of the trigeminal nerve is being stimulated and the needle must be redirected more caudal.
Stimulation of the greater and lesser palatine nerves results in paresthesias of the hard palate. In this case, the needle is anterior and lateral and should be redirected in a more posterior and medial direction.
Before lesioning, 1 to 2 mL of local anesthetic is injected. Expected effect after local anesthetic block is numbness of the root of the nose and palate.
There may be lacrimation from the ipsilateral side of the eye.An insulated 20- or 22-gauge, 10-cm, curved, blunt-tipped RFK (Racz-Finch Kit) needle with a
5- to 10-mm active tip is used. After proper placement and stimulation as described in the technique section,
PEMF lesioning is performed at 42°C for 120 seconds. Two or three lesions (120 seconds) can be made without local anesthetic, since the temperature of the lesioning is barely above the normal body temperature.
Professor M. Omar Tawfik. MD October, 2003
8

Radiofrequency Lesions in Management of PainRF lesioning is performed for 70 to 90 seconds at 80°C. Two lesions are usually made.
Complications A reflex bradycardia can occur in some patients during RF and pEMF lesioning of the SPG. When the lesioning is halted, the bradycardia is resolved. In some patients, atropine may
need to be given to complete the lesioning. A reflex resembling the oculocardiac reflex may be the cause. The afferent information may travel back through the vidian nerve, geniculate ganglion, and nervus intermedius to reach the solitary tract nucleus, which has interconnections to the dorsal vagal nucleus.
Infection can occur if proper aseptic technique is breached. Epistaxis can occur if too much pressure is applied to the needle and it is pushed through
the lateral nasal wall. Hematoma formation is possible if the large venous plexus overlying the pterygopalatine
fossa or the maxillary artery is punctured. RF lesioning of the SPG can result in hypesthesia or numbness of the palate, maxilla, or
the posterior pharynx but is usually transient. PERCUTANEOUS CORDOTOMY PCCDestruction by radiofrequency thermal lesion to the contra-lateral spino-thalamic tract in the
cervical region is done to relieve cancer pain. Indications are severe cancer pain not relieved by drug therapy, or relieved with high incidence of side effects. Although unilateral percutaneous cervical cordotomy (PCC) can relieve unilateral pain, bilateral intractable cancer pain can be relieved by bilateral cordotomy done with 2 weeks interval in between.
Technique:1. Thorough explanation of the procedure and its complications are to be discussed with
the patient including the discomfort he is going to suffer from the cord stimulation, and he has to sign consent.
2. The procedure has to be made under local anesthesia.3. A special electrode: Levine’s thermocouple electrode is needed. It has a stainless
steel shaft is insulated with 2 mm exposed tip which is 0.3 mm in diameter that contains a thermocouple sensor for measurement of temperature.
4. The patient is placed in supine position with his head fixed with a Velcro band to the head rest in slightly flexed position.
5. Under lateral fluoroscopy a 22 G spinal needle is introduced between first and second cervical vertebrae.
6. As CSF flows, a mini myelogram is made by injecting water soluble, non-ionizable contrast medium to visualize the dentate ligament.
7. Before removing the spinal needle, the radiofrequency cannula at a right angle to the spinal cord is introduced just ventral to the dentate ligament, where the spinothalamic tract is situated.
8. The stylet is then removed and Levine’s thermocouple electrode is introduced and connected to the radiofrequency generator.
9. The electrode is then introduced inside the spinal cord guided with the impedance measurement that will rise from 300-500 ohms in CSF to 1200-1500 in the cord substance.
10. Motor stimulation (2 Hz, 0.5-2 volts) produces epsilateral contractions in neck muscles and trapezius, and sensory stimulation ( 50 Hz) producing contralateral thermal sensations. If this responses are not produced, no lesion is made, as the corticospinal tract is just beside the spinothalamic tract.
11. A series of lesions made 10 seconds each to temp 80-90 oC until the disappearance of deep pin prick on he contra-lateral side.
12. During each lesion, the muscular strength of the epsilateral arm and leg is checked.
Professor M. Omar Tawfik. MD October, 2003
9

Radiofrequency Lesions in Management of Pain
TECHNIQUE USING CT SCAN:The procedure was performed percutaneously under local anesthesia in a CT unit where CT images from a Siemens Somatom Plus 2 device, 512 x 512 matrix, and 2 mm slice thickness were used. A special temperature monitoring RF electrode system was used: KCTE Kanpolat CT Electrode Kit. Patients were injected with 10 ml (300 mg) iohexol contrast medium, via lumbar puncture into the subarachnoid space 20 minutes prior to the procedure and kept in a trendlenberg position to facilitate the spread of the contrast material in the cervical region. Patients were then placed in supine position. Proper positioning of the RF electrode within the anterolateral quadrant of the spinal cord
at the level of C1-C2.Contralateral parasthesia below the level of the shoulder in the form of (numbness, electric like, wind like, cold, hot or pain sensations) was elicited on sensory stimulation by 50 Hz, by 0.1 – 0.25 Volt were necessary before making the lesions. Then three to five lesions were made starting by tip temperature of 60° C for 40 seconds, increased gradually and the final lesion was made at 70 – 75° C for 60 seconds. This was performed until the required level of analgesia and hyposthesia elicited by pin prick, and temperature discrimination loss were obtained. Pulsed RF may be used for lesioning by a temperature of 42o for2 min.
Complications :( In best hands)Temporary:1. Fever.(70%) 2. Head and neck pain.(60%)3. Weakness in the lower limb.(50%)4. Urinary retention.(25%)Permanent:1.Horner syndrome (100%)2.Hemiparesis (10%).3.Urinary retention (7.5%)4. Mirror image pain (7.5%)Bilateral PCC:In bilateral intractable cancer pain, Bilateral PCC was attempted to relieve pain with 2 weeks
intervals between the 2 sessions.The most important complication that can commonly occur is sleep induced apnea “Ondines
curse”. Some authors clamed that, their series were free from this complication. However, the clearest impression is that a significantly lower success rate, with relatively higher incidence of permanent complications. Due to this fact most of authors do not recommend bilateral PCC.
VERTEBRAL RADIOFREQUENCYI. CERVICALClinically three types of cervical pain syndromes can be distinguished:1. Mechanical neck pain:Originating from the facet joints or from the disc. Facet joint pain is based on the patient's
history or on clinical examination. Paravertebral tenderness by palpation over the joints may indicate facet pain.
Professor M. Omar Tawfik. MD October, 2003
10

Radiofrequency Lesions in Management of PainDisc and facet joint pain can occur in the same segment (41%), sometimes with absence of
radiological findings. The condition can only be firmly diagnosed by the use of diagnostic facet joint blocks.
2. Cervicogenic headache: 1. Unilateral headache originating from the cervical spine: 2. Usually in the upper cervical region.3. Precipitated either by movements or by local pressure over the tender spots.4. Ipsilateral shoulder and arm pain is regularly seen together with a reduced range of
motion in the cervical region.5. Lower segmental levels can also contribute to cervicogenic headache as well as facet
joints C2-C3 and C4-C5.6. Diagnostic blockade of the segmental nerve C2 or C3 should abolish the pain of
cervicogenic headache transiently.CERVICAL SLEEVE ROOT
GANGLIOTOMYAnatomical Considerations:The anterior and posterior roots of cervical
nerves C2–C4 emerge from the spinal canal through their respective intervertebral foramina. The anterior primary rami of C2–C4 pass in an anterior-caudal lateral direction behind the vertebral artery and vein, in the gutter formed by the anterior and posterior tubercles of the corresponding transverse processes of the cervical vertebrae. The tubercles of the transverse processes lie 0.5 to 1.25 inches (1- 3.2 cm) below the skin, depending on the size of the patient and the cervical level. The lower cervical tubercles are more superficial than the tubercles of the upper cervical transverse processes. The anterior tubercles are located farther cephalad and medial than the posterior tubercles.
The anterior primary rami of C2–C4 are also held firmly on the transverse process by a fibrous tunnel. After leaving the transverse processes, these nerves are enclosed in a perineural space formed by the muscles and tendons attached to the anterior and posterior tubercles of their respective cervical vertebrae.
The ascending branches (small occipital and great auricular nerves) supply the occipitomastoid region of the head, the auricle of the ear, and the parotid gland.
The transverse branch (superficial cervical) innervates the anterior part of the neck between the lower border of the jaw and the sternum; and the descending branches (supraclavicular, and superacromial) supply the shoulder and upper pectoral region.
The cervical plexus also communicates with the vagus, hypoglossal, and accessory cervical nerves. These communications may explain some of the side effects often seen with cervical plexus blockade.
Indications Atlanto-occipital and atlantoaxial joint pain. Occipital headaches. Upper cervical pain. Occipital neuralgia. Technique
The patient is placed supine on the fluoroscopy table with the head and neck slightly extended. The neck, sub-mandibular, and retro-auricular regions are prepared. Lateral
Professor M. Omar Tawfik. MD October, 2003
11

Radiofrequency Lesions in Management of Painfluoroscopic images are obtained, and the “lateral mass” of C2 (including the C2 transverse process and inferior articular pillar) and the ventral aspect of the C2 vertebral body are identified. Parallax is eliminated with lateral rotation and cephalad or caudad angulation of the x-ray beam as needed. A skin entry site is marked and anesthetized below the angle of the mandible.
Anterior oblique angulation of the fluoroscopic unit is used initially; after the electrode has been introduced through the skin, lateral images are used to guide placement, because no clear radiographic landmarks are present on anterior oblique fluoroscopic images. (A coaxial, or “tunnel vision” approach is not feasible.) A 10-cm, 5-mm active-tip 20-gauge RF electrode with a small distal curve (10 to 15 degrees) is introduced under lateral fluoroscopic guidance and directed medially and cephalad under lateral fluoroscopic imaging toward the ventral lateral aspect of the C2 vertebral body at its junction with the ipsilateral ventral inferior medial C2 transverse process. The path of the electrode passes lateral and dorsal to the carotid sheath. Care is taken to stay ventral to the existing C3 nerve root and the vertebral artery yet dorsal to the pharyngeal structures. Bony contact may be made at the ventrolateral aspect of the lateral inferior end plate of the C2 vertebral body at its junction with the C2–C3 intervertebral disc. The electrode is then rotated and directed cephalad, hugging bone, into the sulcus along the ventral lateral aspect of the C2 vertebral body, medial to the ventral aspect of the C2 transverse process.
Careful aspiration is performed—no blood or other body fluid should be aspirated. A small-volume contrast study is then performed, using 0.2 to 0.4 mL of nonionic contrast medium, such as iohexol, 240 mg/mL. Contrast spread should be limited to the immediate perivertebral region, outlining the sulcus on antero-posterior view. In lateral radiographs, the contrast should appear to outline the ventral aspect of the transverse process of C2.
The electrode is manipulated with very small movements along the ventral sulcus of C2, until concordant suboccipital pain is reproduced when stimulation is done using stimulation by 0.15 to 0.2 V at 50 Hz.
Elicitation of sharp, radiating infra-auricular/neck pain indicates stimulation of the ventral C3 nerve root and is unacceptable.
Elicitation of deep or superficial infra-auricular pain or anterior cervical/ submandibular pain may indicate possible stimulation of the chorda tympani and is unacceptable.
There are no motor branches associated with the ramus communicans nerve; motor stimulation generally is not performed. Once concordant suboccipital pain has been elicited in a reproducible, patient-blinded fashion, 0.5 to 1 mL 2% lidocaine is injected before RF lesioning.
The RF lesion is performed at 80°C for a period of 60 seconds and repeated once the electrode tip has returned to ambient body temperature. The size of the lesion created by the 2-mm active tip is small, but this approach reduced the risk of inadvertent C3 or chorda tympani lesion that could occur with a 5-mm active tip. After the lesioning, a small amount of corticosteroid, with or without local anesthetic, may be injected and the electrode removed. The patient may be discharged after a 1- to 2-hour. Patients frequently complain of some deep neck soreness, which may last 2 to 3 days, and occasionally of pain with swallowing, which is similarly self-limited.
C3-C7 GANGLIOTOMYThe C-arm positioned to have the X-rays parallel to the axis of the
intervertebral foramen. ( as in cervical Facet denervation).This axis points 25-35° anteriorly and 10° caudally.
With the C-arm in this position, the entry point is marked by projecting a metal ruler over the caudal part of the foramen.
SMK C5 cannula with a 4 mm exposed tip is introduced in the direction of the X-rays. The direction is corrected while the tip is still in the superficial layers, until the needle is projected on the screen as a dot that should lie directly over the dorsal part of the intervertebral foramen at the transition between the middle and most caudal third part.
Professor M. Omar Tawfik. MD October, 2003
12

Radiofrequency Lesions in Management of PainThis dorsal position is chosen in order to avoid damage to the motor-fibers and to the
vertebral artery that runs anterior to the ventral part of the foramen. The direction of the X-rays is then changed to antero-posterior and the cannula is further introduced until the tip is projected over the middle of the facetal column.
The stylet is now replaced by the radiofrequency (RF) probe. After checking the impedance, electrical stimulation is started at a rate of 50 Hz. The patient
should feel a tingling sensation at a voltage in between 0.4 to 0.65 V. Next the frequency is changed to 2 Hz and the patient is observed for muscle contractions. These should not occur below a voltage of 1.5 times the sensory threshold.
0.5 ml of nonionic water soluble contrast medium is now injected to exclude an accidental intradural position of the electrode, and this is followed by 1-2 mL. of 2% lidocaine.
RF-current is then led through the electrode in order to increase the temperature at the tip slowly to 67° C. This temperature is maintained for 60 seconds.CERVICAL FACETS
PERCUTANEOUS FACET DENERVATION. For a facet denervation in the upper and middle cervical
area the patient is positioned supine on the operating table. The C-arm is positioned slightly oblique so that the X-rays are parallel to the axis of the intervertebral foramen and segmental nerves.
Entry points are marked approximately 1 cm posterior to the posterior border of the facetal column and slightly caudal to the target point
Electrodes (SMK C5 cannula with a 4 mm active tip) are introduced postero-laterally. This projection will make it easy to monitor a safe distance between the electrode tip and the emerging segmental nerve.The posterior primary ramus in this projection runs over the base of the superior articular process which can be clearly visible.
Electrodes are carefully advanced anteriorly and cranially until contact is made with the facetal column at the target point.
The position of the C-arm is then changed to the antero-posterior (AP) direction. This should confirm the position of the tip of the needle adjacent to the "belt" of the spine at the corresponding level.
50 Hz stimulation should now give a sensory response below 1V.
1 mL of lidocaine 2% is then injected.After waiting for 3 min., a lesion is made with temperature 80° C for 60 seconds. RF STELLATE BLOCK.
TECHNIQUE:The patient is on the operating table in a supine position.
Professor M. Omar Tawfik. MD October, 2003
13

Radiofrequency Lesions in Management of PainThe cervicothoracic spine is visualised in an antero-posterior view. The carotid artery is kept
aside.SMK C5 cannula with a 4 mm active tip is introduced to make contact with the C7 vertebral
body just medial to the origin of the transverse process. The proper position is confirmed on an oblique projection. The electrode tip should lie anterior to the anterior border of the foramen.
Sensory and motor stimulation should be of no response.1-2 ml of contrast is injected to confirm the characteristic spread, followed by 1-2 ml of 2%
lidocaine. A 60 seconds 80° C lesion is then made.
THORACIC RADIOFREQUENCYFor upper limb sympathetically maintained pain, sympathetic vascular diseases , or
hyperhydrosis, stellate ganglion lesion is not sufficient to eliminate the condition, Thoracic 2nd, and 3rd sympathetic ganglia should also be lesioned in the same session.
THORACIC SYMPATHETIC GANGLIOTOMYThe thoracic sympathetic chain continues in a caudal fashion and lies along the periosteum of
the vertebral body in a much more posterior position as compared to that of the lumbar sympathetic chain.
Thoracic sympathectomy with a radiofrequency cannula usually involves ablation of the thoracic sympathetic chain at the T2 and T3 levels. They can be involved in sympathetically maintained pain problems in upper limb.
Horner's syndrome should not be seen with procedures performed at the level of the T-2 and T-3 sympathetic chain.
TECHNIQUE 1. The patient is placed in a prone position. Postero-anterior view is obtained with C-arm fluoroscopic device to identify the vertebral
bodies of T2 and T3.
Professor M. Omar Tawfik. MD October, 2003
14

Radiofrequency Lesions in Management of PainThe device is angled in a cranial fashion to show sharp interspaces at the T1-2 and T2-3 disc
levels. This is done so that the upper and lower borders of the vertebral bodies are in sharp view that will allow for accurate placement of the Radiofrequency cannula.
The fluoroscopic device is then angled in an oblique fashion until a metallic marker, when placed over the angle of the ribs, will show an image directly over the lateral edge of the appropriate vertebral body.
The point that makes the needle appear as a point "tunnel vision", will be the point of entry for the radiofrequency cannula, that are introduced under local anestheia.We have always to Keep the cannula medial to the costal angle so as to prevent puncture of the lung.
Penetration is made just medial to the costal angle with SMK 150 mm with 5 mm active tips cannula; its tip is advanced parallel to the fluoroscopy beam and angled toward the lateral edge of the respective vertebral body.
Starting at the T2 level, the cannula is angled towards the lateral edge of the vertebral body just below the level of the rib. In a similar fashion, a second cannula is advanced until it touches the lateral edge of the T3 vertebral body just under the third rib.
A lateral fluoroscopic view is taken. The thoracic sympathetic chain sits in a rather posterior position and is only 5 mm anterior to the thoracic neural foramina. In that position, the exposed tip of the radiofrequency cannula should be far away enough from the outlet of the thoracic foramen so as to avoid injury to the segmental thoracic nerve.
0.5 ml of contrast material should be injected. There should be no spread of contrast material along the segmental thoracic nerves. A P-A view should then be taken to confirm that the contrast material is lying directly along the vertebral body just anterior to the thoracic neural foramina.
With 50 Hz,1V stimulation, the patient will note a deep aching feeling in the chest and back. Motor stimulation is then performed at 2 Hz and intercostal fasiculations should be absent at 3.0 Volts. Once these electrical criteria have been met, the cannula is considered to be in correct position for lesioning the thoracic sympathetic chain.
At that point, 1 ml of 2% Lidocaine solution is injected, and a 3-minute delay is allowed. A thermal lesion is then created through each cannula for 90 seconds at a temperature of 80 o
C. Each cannula is then advanced approximately 2 mm in an anterior fashion and a second
lesion is created for 90 seconds at a temperature of 80o C. Following the second lesion both cannula are removed.
A rapid warming and vasodilation of the affected upper extremity should be observed.The post-operative course for these patients is usually benign. A chest x-ray is done to rule
out the possibility of pneumothorax. Most patients will experience 7 to 10 days of postoperative discomfort from the procedure. 15 per cent of the patients will experience a burning sensation in the area of the breast and upper chest wall which lasts for 1 to 2 weeks from thoracic neuritis.
THORACIC VERTEBRAL RFThe thoracic spine is the least common site for spinal complaints, (5%-10%). Diagnostic investigations are important to exclude underlying pathology such as Disc
herniations, aneurysms, tumors, old fractures or infections. Clinically, two types of thoracic pain can be distinguished: A. Mechanical thoracic pain:
Professor M. Omar Tawfik. MD October, 2003
15

Radiofrequency Lesions in Management of Pain1. Facet joint pain can be diagnosed on the basis of patient's history or by physical
examination. It is usually related to degenerative process; collapse of a vertebra or to postural abnormalities. The diagnosis of thoracic facet syndrome is in line with the diagnosis in the cervical and the lumbar region:
Nearly continuous uni / bilateral pain in a localized area of the thoracic spine, without objective neurological signs.
Paravertebral tenderness by palpation over the facet joints.In half of the patients a transient relief of pain after a diagnostic block of the dorsal ramus of
the segmental nerve. 2. Thoracic discogenic pain: Local block to intervertebral disc completely relieves patient’s
pain for a short period.DORSAL ROOT SLEEVE AND GANGLIOTOMYThe following technique is used for an RF-DRG below the level of T7: A 100 mm cannula (SMK 22G, 5 mm active tip) is inserted 1 cm medial to the angle of the
ribs. It is carefully advanced at an angle parallel to the ribs until it is placed in the cranio-dorsal part of the intervertebral foramen.
The stylet of the cannula is replaced with an RF-probe and sensory stimulation is carried out at 50 Hz. Correct positioning is confirmed when the patients perceives a tingling sensation in the selected dermatome below 1 V stimulus.
Stimulation is then performed at 2 Hz. If the needle point is too close to the anterior root the muscles contract at a stimulation threshold below 1.5 Volts.
A nonionic water soluble contrast medium (0.4 ml) is injected to exclude intradural or intravascular spread. This is followed by 1-2 ml of 2% lidocaine, and wait for 3 min.
A 60 seconds 67° C lesion is made by using an RF-lesion generator system.
For an RF-
DRG at T7 and above a different technique is used:Above T8 the anatomy of the origin of the transverse process prevents accurate needle
positioning. To overcome this problem, under fluoroscopic control, a small hole is drilled with pneumatic drill through the lamina of the vertebra using a 16G Kirschner wire to gain access to the intervertebral foramen.
A 20G SMK 15 canula is used.Electrical stimulation and following Steps is then carried out as described above. THORACIC FACET DENERVATION:
TECHNIQUE A facet denervation is usually performed at 3 or 4 levels
since each facet joint is considered to be innervated by 2 medial branches.
Professor M. Omar Tawfik. MD October, 2003
16

Radiofrequency Lesions in Management of PainThe patient lies prone on an operating table. Under fluoroscopic control with a C-arm image intensifier in the antero-posterior position a
22G cannula (100 active tip 5 mm). The cannula is advanced until there is bone contact at the junction of the superior articular process and the transverse process. The C-arm is turned to the transverse position in order to check the depth of the cannula.
TC 10 RF probe is inserted in the cannula. A 50 Hz current with a voltage of less than 1 V should elicit
a tingling sensation paravertebrally. Motor stimulation with 2 Hz of a voltage of I V, or less, should provoke paravertebral muscle contractions.
When these criteria are met, 0.5 ml Lidocaine 2% is administered.
A lesion is made after waiting for 3 minutes at a temperature of 80° C. for 60 seconds.
LUMBAR VERTEBRAL RADIOFREQUENCY The lumbar spine is the most common site for chronic
spinal pain and is the presenting symptom of 45% of patients in the pain clinic. Clinically, two types of lumbar pain can be distinguished once serious pathology has been excluded:
a. Mechanical low back pain with pain mainly emanating from joint complex.
b. Low back pain with irradiation in the leg due to nerve root involvement.
Local anesthetic blockade of the nerve supply of the joint or an intra-articular block can confirm the diagnosis. However, RF-lesioning proved that these diagnostic blocks may lack specificity in predicting long-term response to denervation.
The lumbar disc is considered to be a source of lumbar pain. In this pain syndrome, disruption of the disc and leakage of the nucleus pulposus material into the annulus fibrosus is believed to be a source of pain.
1. PERCUTANEOUS FACET DENERVATION. With the patient prone on the operating table, the C-arm is positioned in a slightly (10-15o)
oblique projection until the grooves between the superior articular and transverse processes are clearly visualized.
Entry points are marked overlying the grooves at the L4, L5 and S1 level. In these grooves run the posterior primary rami of L3, L4 and L5. Another entry point is marked overlying the S1 foramen.
An SMK C10 cannula with a 5 mm active tip is introduced in each entry point. The upper three electrodes are positioned under tunnel vision until the tip lies in the groove. The lowest electrode is introduced slightly upwards until contact is made with bone just distal to the articular space.
This electrode should lesion the communicating nerve that runs cranially from the S1 foramen.
Professor M. Omar Tawfik. MD October, 2003
17

Radiofrequency Lesions in Management of PainThe proper position of the electrodes should always be checked on the Lateral view. This is
essential to prevent damage to the segmental nerves. 50 Hz stimulation should give a response below 1V.A 60 seconds 80° C lesion is made after waiting for 3 min.
INTRA-ARTICULAR FACET DENERVATION A percutaneous intra-articular facet denervation (PIFD) is
performed after a positive intra-articular diagnostic block in patients suffering from low back pain.
All procedures were performed in an outpatient setting using an image intensifier. The patient is positioned in the prone position without sedation or analgesic medication.
Patients with unilateral complaints underwent a unilateral diagnostic block, while in patients suffering from bilateral or axial complaints received a bilateral diagnostic block.
The C-arm is adjusted from the vertical plane to visualize the facet joint cavity, in the most minimal oblique position (maximal 10-15o). A 23 Gauge radio-contrast needle is inserted in the facet joint and 0.5 ml of a water soluble of aqueous contrast medium is injected intra-articularly to assure accurate needle placement, followed by 1 ml lidocaine 2%.
Special attention is paid to capsular rupture demonstrated by contrast medium leakage.After this diagnostic procedure, patients are asked to provoke their original pain if possible.If there is a temporary pain relief of 50% or more on the visual analogue scale a PIFD is
performed, in a separate session. The technique of PIFD is analogue to that diagnostic procedure.20 Gauge disposable needle of 100 mm length with a 5 mm active tip is guided into the
center of the articular cavity of the facet joint.Lateral fluoroscopy to ensure the proper location of the needle tip, avoiding the
vicinity of the intervertebral foramen.Electrical stimulation is performed using a 50 Hz current. The localization is
considered to be correct if a sensory response at a threshold of less than 1 V is found.After injection of 1 ml lidocaine 2%, three radiofrequency lesions (60 sec.- 22 V
(more than 80oC) are made in the articular cavity, central, rostral and caudal of the facet joint.
Professor M. Omar Tawfik. MD October, 2003
18

Radiofrequency Lesions in Management of PainWhy PIFD ?
1. Concerning the RF lesion at the lateral margin of the facet joint, the anatomical base is not relevant.
2. Performing RF lesions at the medial branch of the posterior primary (dorsal) ramus of the spinal segmental nerve, a two level sensory supply has to be blocked: a branch of the medial division of the posterior primary ramus at its own level (caudal part of the joint) and a descending branch from the level above (rostral part of the joint). Thus RF facet denervation has to be performed at least at two successive levels, inducing increased chance on inaccuracy.
3. The posterior primary ramus approach may be difficult by possible impediments like the overgrowth of the accessory process causing bony irregularities, or ossification of the mammillo-accessory ligament protecting the nerve.
4. On theoretical grounds, RF is not successful if the electrode contacts bone.
RF LUMBAR SYMPATHETIC BLOCK. This block is usually performed at the L3 and
L4-1evel. With the patient prone on the operating table the C-arm is positioned in an oblique direction so that the spinous processes are projected over the facet joint column of the opposite side.
1.An entry point is selected overlying the side of the vertebral body at the junction of the lower and middle third of the vertebra.
2. A 20G SMK C15 cannula with a 10 mm active tip is introduced under vision. It is carefully advanced, passing cranial to the segmental nerve and avoiding contact with the periosteum of the vertebral body.
3.The position is then checked on the tranverse and antero-posterior projections. The tip should lie in level with the anterior margin of the vertebra and just medial to the middle of the facetal column. This is important to avoid damage to the ilioinguinal nerve.
4. Injection of contrast should show the typical spread of contrast.
5. 2 ml of 2% lidocaine are injected.6. 60 seconds 80° C lesion is made after waiting for 3 minutes.
RF LUMBAR DISC INTRADERMAL ELECTROTHERMAL COAGULATION TECHNIQUEPrior to the procedure, the patient is given
intravenous antibiotic, strict sterilization is important.
The prorcedure is done under light sedation, and infiltration of the L2 root sleeve (transforaminal epidural) injection is recommended prior to the procedure.
For the placement of the introducer needle, the proper disc level is identified under fluoroscopic view. It is important to align the inferior end plates (bringing the superior pars “up” to the disc level) with some cephalocaudal trajectory to adjust for lordosis. This trajectory may be as much as 25 to 30 degrees. The
Professor M. Omar Tawfik. MD October, 2003
19

Radiofrequency Lesions in Management of Painfluoroscopic beam is then obliqued to place the spinous processes lateral, and the facet line should appear “midline”. It is important to obtain the required amount of oblique view, because less than adequate rotation will cause a lateral placement of the needle.
At the midpoint of the superior articular process, at the lateral edge, a skin wheal is raised with 1 ml of 1.5% lidocaine. It is important to anesthetize also the subcutaneous tissues to the level of the superior pars.
The 17-gauge introducer needle is inserted through the opening. A “tunnel” view is maintained and the needle is advanced to the superior pars. It is important to make contact with the superior pars at its most lateral aspect. This provides safety: As one barely touches the bone, it will not change the trajectory of the introducer needle causing lateral placement.
Frequent lateral views can provide an accurate depth of the needle. Keep the introducer needle facing the posterior wall of the discs as it enters the annulus. The annulus will provide resistance and feel “gritty” to the physician as the needle passes. This will be followed by a sudden loss of resistance. The needle should be placed in this transitional zone between the annulus and the nucleus; this should be confirmed in both the postero-anterior and lateral views.
Once the introducer needle is properly placed, the navigable catheter using the Spine-CATH system is threaded through the needle hub with the curve at the tip of the catheter and the white line on the catheter handle should be aligned with the bevel marker on the needle hub and facing to the posterior aspect of the disc.
As the catheter is advanced into the needle, note when the first bold depth marker on the catheter enters the needle hub. This indicates the tip of the catheter has reached the tip of the introducer needle. Using continuous fluoroscopic guidance, in the lateral view the catheter will pass in the transitional zone between the annulus and the nucleus and curl inside the disc at the interface of the nucleus and the interior annular wall.
Ideal placement is the posterior third of the disc, across the midline of the posterior wall, and centered between the plates. Note that the catheter must not be outside of the disc wall. Also note that when the second bold marker of the proximal shaft enters the needle, the heater end has completely exited the tip of the needle into the disc. The fluoroscope is then rotated cephalocaudad to view the catheter from the top of the disc. This should be observed as radiopaque markers of the resistive coil being outside of the introducer needle.
Care must be taken not to force the catheter or kinking will result. If the physician observes significant resistance to movement, especially during withdrawal of the catheter through the introducer needle, both the needle and the catheter should be immediately removed together.
Impedance should be monitored. Prior to placement of the catheter, this should be checked and verified that it is within the acceptable range of 120 to 200 Ω. This range should be maintained throughout the thermocoagulation and is an indicator of a functioning power circuit.
After proper catheter placement, the catheter is heated to 65°C. The temperature is then raised 1°C every 30 seconds until the desired therapy level is reached. Ideally, this is between 80°C and 90°C, 4 to 6 minutes, to thoroughly distribute the heat. The total time for a heating lasts between 14 to 17 minutes. As the temperature increases, the patient is continuously evaluated for back pain and any other signs of nerve root irritation such as extremity pain. It is expected that there may be reproduction of back or extremity pain concordant with the patient’s normal symptoms.
Professor M. Omar Tawfik. MD October, 2003
20

Radiofrequency Lesions in Management of PainThe catheter should be then withdrawn with some rotation. Intradiscal antibiotics (1 ml of 5
mg/ml cefobid) should be administered through the needle. After removal of the introducer needle, the site is covered with antibiotic ointment and dressing.
RF LESION OF THE COMMUNICATING RAMUS.With the patient prone on
the operating table the C-arm is adjusted as for lumbar sympathetic block.
An entry point is selected overlying the lateral part of the vertebral body just caudal to the transverse process.
A SMK C15 cannula with a 2 mm active tip is introduced under vision until it makes contact with bone at a point somewhat posterior to the middle of the vertebral body.
The position is checked in the lateral projection.
Electrical stimulation at 50 Hz should elicit a sensation in the back with less than 1.5 V. There should be no motor response to 2 Hz stimulation at 2 V.
If these conditions are not met the electrode is carefully manipulated both in the saggittal and in the transverse plane to find a better position.
A 60 seconds 80° C lesion is then made.TECHNIQUE OF RF LUMBAR DRG.With the patient prone on the operating table the C-arm is positioned in the antero-posterior
direction.A SMK C10 cannula with a 5 mm active tip is introduced at an entry point 8 cm from the
midline and 4 cm caudal to the relevant transverse process. The electrode is carefully advanced to make contact with the junction of the lower border of
the transverse process and the lamina. It is then manipulated slightly caudally and anteriorly until it slips into the cranio-dorsal part of the foramen.
It is advanced until the tip is projected over the middle of the facet column. Next the posterior position in the foramen is confirmed on the lateral view.The stylet is now replaced by an RF-probe, and the impedance is checked.Electrical stimulation is started at 50 Hz. The patient should feel a tingling sensation between
0.4 and 0.65 V.Next the frequency is changed to 2 Hz and the patient is observed for muscle contractions
with voltage less than 1V.
Professor M. Omar Tawfik. MD October, 2003
21

Radiofrequency Lesions in Management of Pain
SACRAL DORSAL ROOT GANGLIOTOMYBlock of the sacral nerve roots is accomplished through the posterior sacral foramen. The site
of entry is visualized by adjusting the fluoroscopic beam to align the chosen posterior foramen with the anterior foramen. Insert the angiocatheter and blunt needle through the posterior foramen and advance the blunt needle toward the anterior foramen until the tip is just anterior to the anterior sacral plate on lateral view. Contrast material and local anesthetic can then be injected.
A negative aspirate for blood and cerebrospinal fluid must precede any injection. All injections should be performed under fluoroscopic guidance to avoid intravascular or intrathecal spread.
A small amount (1 ml) of non-ionic, water-soluble contrast (iohexol) is injected slowly to avoid trauma to the nerve root. The spread of the contrast medium should delineate the nerve root only, with no spread into the epidural space or onto the peripheral plexus. If resistance is felt or vascular spread is noted, the needle must be redirected. After negative aspirate, inject 1 to 1.5 ml of local anesthetic (1% to 2% lidocaine or 0.25% to 0.5% bupivacaine) under fluoroscopic guidance. The patient should not feel any pain or paresthesia during injection. Remove the needle and place a sterile bandage.
Ganglionostomy of the sacral dorsal root ganglions (drgs) has been done by some that requires the creation of a burr hole through the lamina or the posterior sacrum. A curved-blunt tip needle can be successfully placed through the posterior sacral foramen at the superior aspect to stimulate and lesion with RFTC or pulsed electromagnetic frequency (pemf).
RADIOFREQUENCY OF THE SACRAL ROOTS (DRG)The goal is to position the tip of the needle directly adjacent to the DRG of the desired nerve
root. A sensory paresthesia should be felt in the desired dermatome at less the 1.0 V at 50-Hz stimulation. Ideal stimulation should be felt between 0.4 and 0.6 V. If stimulation is felt at less the 0.4 V, the tip of the needle is too close to the DRG, and if stimulation is felt at greater than 0.6 V, the tip is too far away from the DRG. Motor stimulation is then performed at 2 Hz. There should be a clear dissociation between motor And sensory stimulation; that is, the voltage required to see motor fasciculations at 2 Hz should be at least two times the voltage that produces sensory stimulation at 50 Hz. Thus, if good sensory stimulation at 50 Hz is noted at 0.5 V, the motor fasciculations at 2 Hz should not be seen at voltages less than 1.0 V. The point of dissociation defines the position of the DRG. If dissociation between sensory and motor stimulation cannot be obtained, the tip of the needle is not in alignment with the DRG, and lesioning at this point is not recommended.
Once the proper stimulation parameters have been achieved, inject 2 ml of local anesthetic with 40 mg of triamcinolone diacetate. Wait 3 to 5 minutes and then lesion at 67°C for 90 seconds with conventional radiofrequency. With pulsed radiofrequency is done at this site two or three times for 120 seconds and at 42°C.
Professor M. Omar Tawfik. MD October, 2003
22

Radiofrequency Lesions in Management of Pain
Professor M. Omar Tawfik. MD October, 2003
23