Embed Size (px)
Citation preview

Radiobiological aspects of IORT with
Intrabeam Carsten Herskind, Ph.D.
Dept. of Radiation Oncology, Universitätsmedizin Mannheim (UMM)
Medical Faculty Mannheim, Heidelberg University, D-68167 Mannheim, Germany
e-mail: [email protected]
TARGIT Symposium, Herlev Hospital, 21st January 2015

Very large dose fractions in radiotherapy
Hypofractionated HDR Brachytherapy
Radiosurgery, Stereotactic Body/Ablative Radiotherapy (SBRT/SABR)
Intraoperative Radiotherapy (IORT)
IORT with
50 kV X-rays
IORT with electrons

3
A Novel Mobile Device for Intraoperative Radiotherapy (IORT) U. Kraus-Tiefenbacher Onkologie 2003; 26:596-5998
The INTRABEAM Intraoperative Device low-energy X-rays: 30-50 kV

Characteristics of IORT with Intrabeam X-rays Differences from External Beam RadioTherapy
Low-energy X-rays (50 kV vs 6 MV)
point source: intensity decreases with distance ( 1/dist2)
stronger energy absorption (attenuation), less penetration most of the dose is deposited in a small volume radiation quality: enhanced relative biologic effectiveness (RBE)
Lower dose rate
Repair of damage during protracted irradiation (20-50 min)
Single dose, no fractionation dose must be reduced
Effect on residual tumour cells ? Sparing of late-reacting normal tissue (NT) ?
No delay between surgery and RT
No repopulation of tumour cells during wound healing (~ 5 weeks)

5
Radiation quality: ionisation density
Linear Energy Transfer (LET):
Mean energy deposited per track length
- measured in keV/µm
10-40 keV photons: 4-6 keV/µm
i.e. an order of magnitude lower
than
Heavy particles: high-LET
typically 50-200 keV/µm
photon
scattered
photon
electron
-particle
~1000 tracks/Gy
3-4 tracks/Gy
Photons, electrons: low-LET
typically 0.2-2 keV/µm
Adapted from Goodhead, Health Phys (1988)

Low-energy X-rays deposit
a larger proportion of their
dose in electron track ends
Electron track ends (<1 keV):
Schematic electron track produced by 50 kV X-rays
Schematic electron track produced by 6 MV X-rays
10 keV electron
LET=2.3 keV/µm
Distance (nm) H. Nikjoo,
IFMBE Proceedings, Springer 2009
Goodhead, in Meyn, Withers,1980
Goodhead et al., Int J Radiat Biol., 1993
Herskind, Wenz, Transl. Cancer Res. 2014

Target molecule: DNA
http://en.wikipedia.org/wiki/File:ADN_animation.gif
Double helix ( 2.3 nm)
Sugar-phosphate backbone:
deoxyribose-phosphate
Base pairing: A T, T A
C G, G C

Induction and repair of DNA damage
e¯
OH OH
OH
OH For low LET:
~25% direct action
ionisation directly in DNA
~75% indirect action
via aqueous free radicals (OH)
Double-strand breaks ~ 40 per Gy
Single-strand breaks ~ 1000 per Gy
Base damage ~ 3000 per Gy
Lethal lesions ~ 0.5 per Gy
very efficient repair of most lesions
Residual, complex damage is important

9
Relative Biologic Effectiveness (RBE)
Cell survival curves
Su
rviv
ing
Fra
cti
on
(S
F)
Low LET High LET
Unirradiated Irradiated
RBE: Dref(MeV photons)/Dtest
RBE = ratio of physical doses
producing same effect
Dref = RBE Dtest M.C. Joiner in: Joiner & van der Kogel (Eds)„
Basic Clinical Radiobiology, 4th ed., 2009
Hall & Giaccia„ Radiobiology for the Radiologist, 7th ed., 2012 50kV X-rays
Clonogenic survival: surviving fraction (SF)

Su
rviv
ing
Fra
cti
on
(S
F)
Low LET High LET Quadratic component:
Reparable lesions
Linear component:
Irreparable lethal lesions
-ln(SF)= D+ D2
Shape of the survival curve: Linear-Quadratic
(2nd-order polynomial)
Various
biophysical
models Repairable
lesions
Cell death
Survival
Irreparable
lesions
repair
Damage fixation
Misrepair/no repair

Dose (Gy)
0 2 4 6 8 10 12 14 16
SF
1e-5
1e-4
1e-3
1e-2
1e-1
1e+0
1e+1
G=1.0
G=0.5
G=0.1
RBE for protracted irradiation with 50 kV X-rays
Dose (Gy)
0 5 10 15 20 25 30
SF
1e-10
1e-9
1e-8
1e-7
1e-6
1e-5
1e-4
1e-3
1e-2
1e-1
1e+050 kV acute
50 kV, G=0.5
Ref, acute
Repair during
irradiation
RBEacute
RBEprotracted
Radiation quality affects .
Continuous production and
repair of sublesions affects .
Lea-Catcheside time factor
-ln[SF(D)] = D+G(T) D2
continuous
protracted
acute
Split dose irrad.

12
Experimental determination of RBE in tumour-bed phantom in vitro
Spherical breast applicator (4.0 cm diam.):
RBE=1.35 [c.i. 1.2;1.5] in 8 mm distance from
applicator surface (2.0 cm from source)
Liu et al.(2013), Int J Radiat Oncol Biol Phys 85:1127-33

13
Anz. Fraktionen
0 10 20 30 40
SF
1e-8
1e-7
1e-6
1e-5
1e-4
1e-3
1e-2
1e-1
1e+0
2 Gy/Fx
4 Gy/Fx
D2=
48 Gy
D1=
62 Gy
no. of fractions Dosis (Gy)
0 2 4 6 8 10 12
SF
0.001
0.01
0.1
1
Einzeitdosis
2 Gy/Fx
4 Gy/Fx
single dose
Effect of fraction size on the surviving fraction (SF) in the Lin.-Quadr. model: SF = exp[-( d+ d2)]
L-Q model for fractionation:
-ln(SF) = -n ln(SF(d) = n ( d+ d2) = D+ dD
D: total dose (Gy)
n: number of fractions
d: Fraction size (Gy)
: lin. coefficient (Gy-1)
: quadr. coeff. (Gy-2)
Total dose, D [Gy]

0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 20 40 60 80 100
P (
en
dp
oin
t)
Total dose (Gy)
d=2 Gy
d=3 Gy
d=6 Gy
Single dose
Is the L-Q model for isoeffective fractionation valid
for dose fractions >8-10 Gy ?
YES: Brenner et al.
Mechanistic basis
Several mech. models lead to L-Q
Good fit of SF up to 15 Gy
Works well for late reacting tissue
NO: Kirkpatrick et al.
Linear slope of SF at high doses
Mechanistic basis is not all
Effects of stroma, vasculature
Different cell kill modes at high doses
Subpopul. cancer stem-like cells
?
Semin. Radiat. Oncol. 18, 2008

EQD2=10Gy
0 20 40 60 80 100 120 140 160
Local con
trol
0
20
40
60
80
100
Single (liver)
3 Fx. (liver)
Single (lung)
3 Fx. (lung)
3 Fx. (lu./liv.)
Very large dose fractions have proved efficient in stereotactic body radiotherapy (SBRT)
Herskind, Wenz (2014):
Transl. Cancer Res. 3:3-17
Data from studies reviewed in Siva et al. (2010), J Thorac Oncol 5:1091-9
and Hoyer et al. (2012), Radiother Oncol 82:1047-57
Doses converted to equivalent dose given in 2 Gy/fx (EQD2) using the L-Q model

16
Modelling the biological effect of tumour bed
irradiation with Intrabeam
DoseINTRABEAM Doseref Biol. effect
RBE
Clinical
dose-response
fract. L-Q
model
Single-dose Single-dose
Strategy:

17
Total dose (EQD2: Gy)
0 20 40 60 80 100
TC
P
0.0
0.2
0.4
0.6
0.8
1.0
30% foci
small tumours
solid tumours
Dose response for different types of targets
The number of tumour cells matters
Modified after Herskind et al.: WC2009
IFMBE Proceedings 25/III, Springer, 2009.

18
EQD2
0 20 40 60 80
local
tum
ou
r c
on
tro
l0.5
0.6
0.7
0.8
0.9
1.0
conv. fract.
w/o repop.
Distance from applicator (mm)
0 5 10 15 20 25
Do
se (
Gy)
1
10
100
Dphys
(50 kV)
Disoeff
(ref.)
EQD2 (ref.)
RBE
Fractionation
Modelling the risk of recurrence (breast)
DoseINTRABEAM Doseref Biol. effect
RBE Dose-response
EQD2ref
fract.
L-Q
model Herskind et al. Int J
Radiat Oncol Biol
Phys 72 (2008)

For IORT, the probability of recurrence
increases as the absorbed dose decreases
with depth in the tumour bed. For external
beam RT, the probability is constant.
20 Gy single dose at the
applicator surface
Equivalent Dose EQD2= 67.8-73.0 Gy
Exceeds 50 Gy given in a standard
course of external beam radiotherapy
Sphere of equivalence in relation to excised
tumour plus 10 mm margin. The relative
dose and probability of recurrence are
given on the y-axis as function of distance.
Risk of Local Recurrence:
- “Sphere of Equivalence”

20
Clinical dose-response: Therapeutic window of complication-free tumour control
0.0
0.5
1.0
0 20 40 60 80 100
Dose (Gy)
Pro
ba
bil
ity
Tumour
control (TC)
Normal tissue
complication
complication-
free TC
Holthusen 1936
Small dose fractions widen the therapeutic window by
protecting the normal tissue relative to the tumor cells

The curves are displaced away from
the applicator surface and the
displacement is greater for the
larger diameters. ED50 is reached at
5.9-7.8 mm. The risk becomes
negligible at larger distances (lung)
For different applicator diameters the
probability of developing subcutaneous
fibrosis is the same. This end point
requires higher doses than pneumonitis,
the volume at risk for developing fibrosis is
smaller than that for pneumonitis
Herskind et al., Radiat. Res. 163 (2005)
Modelling calculations including the effect of recovery
Late effect probability after a single high dose
Pneumonitis Subcutaneous Fibrosis Pneumonitis Subcutaneous Fibrosis

Estimated extent of late reaction
under different assumptions for RBE
Pneumonitis is limited to ~ 10-12 mm distance even if RBE = 1.5
Thus the thorax wall offers sufficient protection of the lung
Subcutaneous Fibrosis Pneumonitis
Herskind et al., Radiat. Res. 163 (2005)

23
Electron IORT (uniform) : 21 Gy
50 kV IORT
(non-uniform):
max 20 Gy x RBE
Radiosurgery (e.g. brain, liver, lung)
i
v(i)/Vk
5022 1)(D(i)/NTDNTDP1
High doses may be
tolerated if the irradiated
volume is small:
Does not apply to serial
tissues !
Limiting the volume of irradiated normal tissue
1-p probability without necrosis
V total volume of brain
NTD2(i) normalised total dose à 2 Gy/fx
v(i) volume receiving NTD2(i)
NTD2(D50) NTD inducing 50% risk of necrosis
Flickinger,
IJROBP 17, 1989
Volume effect
Nairz et al., Strahlenther.
Onkol. 6, 2006

24
Radiobiological aspects of high single doses
Cellular response to large single doses Influence of radiation quality, dose protraction
Effects on DNA repair, genomic instability
Non-targeted (cohort) effects
Influence of the stroma, micromilieu Microvasculature, platelets, endothelial cells
Microenvironment, cytokines
Immunological effects Release and presentation of tumour-associated antigens (TAA)

Non-targeted effects in medium-transfer experiments
Conditioned medium (CM) from irradiated cells
(2 Gy) induces DNA DSB repair foci ( H2AX)
Burdak-Rothkamm et al. Oncogene 26 (2007); Cancer Res 68
(2008)
15 Gy CM induces H2AX foci
over many hours in MCF7
breast cancer cells and reduces
colony formation. Veldwijk et al., PLoS One 9(1) 2013

26
Role of microvascular endothelial cell apoptosis for
tumour growth and radiation-induced growth delay
Acid sphingomyelinase (asmase) ceramide endothelial apoptosis
Garcia-Barros et al., Science 300, 2003
Ch‘ang et al., Nat. Med. 11, 2005
Truman et al., PLoS One. 5, 2010
Induction of
ceramide
synthase
20 Gy 10 Gy 15 Gy MCA/129
asmase-/-
mice
w.t.
mice

27
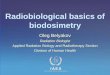
Radiation-induced clotting of blood platelets: Thrombus formation
Maeda et al., PLoS One 7 (2012)
D=30 Gy
Dorsal Skin Fold Window Chamber
Red blood cells
Platelets

Micromilieu – Cytokines in Wound Fluid
MCF-7 in MATRIGEL
MDA-MB 231
PRE-Sera WF UNTR.
WF TARGIT
PRE Sera
WF UNTR
WF TARGIT
NIH CM
SFM PRE Sera
Irradiation with
a high single
dose changes
cytokine profile
in wound fluid
Invasion assay
Transwell
chemotaxis
assay
Belletti et al., Clin. Cancer Res. 14, 2008

29
Immunological effects
Irradiation of large volumes of blood and tissue is
immunosuppressive (kills lymphocytes)
However
IR also induces an inflammatory environment
Cytokines (IL1 , IL-6, TNF- ), chemokines
Endothelial adhesions molecules: ICAM-1, E-selectin, P-selectin
attracts antigen presenting cells (APC)
recruits T-cells to tumour

Immunological effects
IL-1, IL-6, TNF
Hs proteins
Chemokines
Adhesion mol.
Demaria, Formenti, Int.J.Radiat.Biol. 83, 2007
Demaria et al., IJROBP 63, 2005
Lugade et al., J. Immunol. 174, 2005
Herskind et al., Strahlenther. Onkol.
180, 2004; 174 suppl.3, 1998
antigen presenting cells (APC)
(dendritic cells, macrophages)
CD8+ T-cell
MHC-I
stromal cells Tumour-draining
lymph node
Tumour
cell
death
antigens
+ „danger“ signals
Homing: e.g. CCL5
ICAM-1, E-, P-selectin
tumour cells
IR
Activation
CD4+ (Th1) IL-2
IL-12
MHC-II
MHC-I

Overview: model of biological effects versus dose
Dose range
3-6 Gy > 8-10 Gy 25-30 Gy
Repair saturation Increased irreparable damage
Non-targeted effects
Decreased
prolif./invas.
Increased CIN Increased cell death, release of
Tumour-Associated
Antigens
Endothelial
apoptosis
Cells
Stroma,
micro-
milieu,
systemic
Cytokines
Antigen
presentation Thrombus
formation
Targeted/non-targeted effects

SUMMARY: single large dose vs. fractionation
Biophysics; L-Q formalism
RBE is increased for 50 kV X-rays; dose dependence not verified
L-Q model for fx. is a reasonable approximation up to ~15-20 Gy
Biological effects on residual tumour cells
IORT eliminates tumour cell repopulation before ext.beam RT
Sphere of Equivalence: high dose at applicator surface
Minimize NT volume to counter smaller therapeutic window !
Biological effects of high doses per fraction
Cellular radiation response (repair quality, non-targeted effects)
Effects of irradiated stroma (vascular effects, cytokines)
Immunological effects (increased antigen presentation)

33
Acknowledgements
Lab:
Miriam Bierbaum
Juliane Bradl, M.Sc.
Linda Hartmann, Ph.D.
Anne Kirchner
Junqi Liu, M.D.
Xiaolei Liu, M.Sc.
Patrick Maier, Ph.D.
Marlon Veldwijk, Ph.D.
Previous members
Qi Liu, Ph.D.
Lin Ma, Ph.D.
Nicole Roth
Bo Zhang, Ph.D.
Clinic, Physics:
F. Giordano, M.D.
U. Kraus-Tiefenbacher, M.D.
F. Schneider, Ph.D.
E. Sperk, M.D.
V. Steil, head physicist
Director: Prof. F. Wenz, M.D.

34
References
Herskind C, Steil V, Kraus-Tiefenbacher U, Wenz F (2005). Radiobiological aspects of intraoperative radiotherapy (IORT) with isotropic low-energy X rays for early-stage breast cancer. Radiat. Res., 163, 208-15
Herskind C, Schalla S, Hahn EW, Höver K-H, Wenz F (2006). Influence of different dose rates on cell recovery and RBE at different spatial positions during protracted conformal radiotherapy. Radiat. Protection Dosimetry 122 (Nos.1-4) 498-505
Herskind C, Griebel J, Kraus-Tiefenbacher U, Wenz F (2008). Sphere of equivalence – a novel target volume concept for intraoperative radiotherapy using low-energy x rays. Int. J. Radiat. Oncol. Biol. Phys. 72:1575-81
Herskind C, Wenz F (2009). Is there more to intraoperative radiotherapy (IORT) than physical dose ? Int J Radiat Oncol Biol Phys 74:976-977
Herskind C, Ma L, Liu Q, Wenz F (2009). Biological Effect of Single, Very Large Dose Fractions as used in Intraoperative Radiotherapy (IORT), O. Dössel and W.C. Schlegel (Eds.): WC2009, IFMBE Proceedings 25/III, Springer, 18-21
Herskind C, Wenz F (2010). Radiobiological comparison of hypofractionated accelerated partial breast irradiation (APBI) and single-dose intraoperative radiotherapy (IORT) with 50 kV x rays. Strahlenther. Onkol. 186:444-51
Liu Q, Schneider F, Ma L, Wenz, F, Herskind C (2013). Relative Biologic Effectiveness (RBE) of 50 kV X-rays Measured in a Phantom for Intraoperative Tumor-Bed Irradiation. Int J Radiat Oncol Biol Phys. 85:1127-33
Veldwijk MR, Zhang B, Wenz F, Herskind C (2014) The biological effect of large single doses: a possible role for non-targeted effects in cell inactivation. PLoS One 9:e84991
Herskind C, Wenz F. (2014). Radiobiological aspects of intraoperative tumour-bed irradiation with low-energy X-rays (LEX-IORT). Transl Cancer Res 3:3-17

35
Replacing multiple fractions of conventional RT with
a single large dose
multiple fx single dose
Therapeutic window narrower (NT ?)
4 R‘s of radiotherapy
Repair less (tumour/NT ?)
Redistribution none (resistant cells ?)
Reoxygenation none (hypoxic cells ?)
Repopulation none (tumour/NT ?)
The biological effect of high doses per fraction
may differ from the effect of 2 Gy daily fractions