Embed Size (px)
DESCRIPTION
Radio Seminar
Citation preview
Metastatic Calcifications By Farah Aiman Ahmad Nurulazam
Metastatic Calcifications � Is when minerals precipitate into normal tissues as
a result of higher serum calcium and phosphate levels in certain conditions *
� Occurs bilaterally and symmetrically
Heterotopic Bone � Mineral is deposited in soft tissue (well organized)
� Formed in an abnormal location (extraskeletal)
Ossification of the Stylohyoid Ligament
� Usually downward (from base of skull)
� Bilaterally
� Rare cases ( ossifications at lesser horn of the hyoid and fewer in central of the ligament)
Clinical Features � Palpation over tonsil (hard, pointed)
� Minor patients have symptoms/Most of them symptomless
� Symptoms of this disease is termed as Eagle Syndrome : 1)Classic Eagle Syndrome
2) Carotid Artery Syndrome
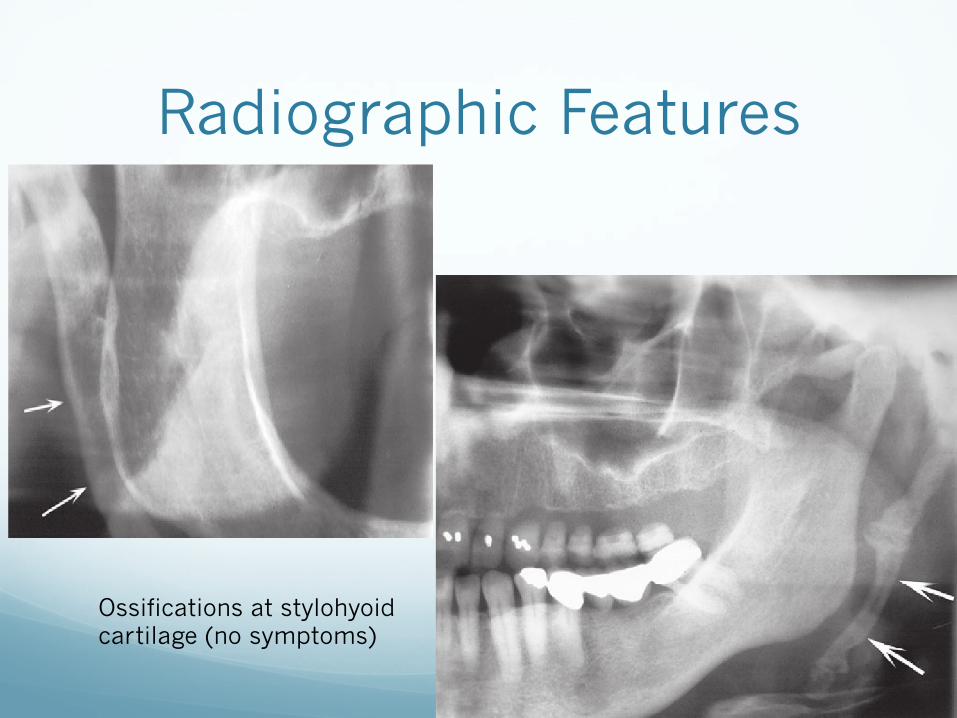
Radiographic Features
Ossifications at stylohyoid cartilage (no symptoms)
� Incidental in panoramic RG, 18% examined showed 30mm calcification of stylohyoid ligament
� Calcifications of the in individuals of any age
� LOCATION: Panoramic- linear ossifications extends forward from mastoid process and cross post-inf aspect of ramus towards hyoid bone. Hyoid bone parallel (roughly) to/ superimposed on post aspect of inferior cortex mandible
� SHAPE: long, tapering, thin radiopaque process (thicker at base) projects downwards and forward. Length- 0.5-2.5cm. Irregularity may be seen at outer surface. Farther the radiopaque ossified ligaments extend toward the hyoid bone then it will be interupted by radiolucent jointlike junctions (PSUEDOARTICULATIONS)
� INTERNAL STRUCTURE: Homogenous RO, outer cortex
Differential Diagnosis/ Management
� TMJ DYSFUNCTION: symptoms alike
� MANAGEMENT: � Asymptomatic : NO Rx
� Symptomatic: vague symptoms- conservative approach of reassurance – steroid/lidocaine injections into tonsillar fossa
� Persistent/Intense pain- stylohyoidectomy
Osteoma Cutis � Rare ossification soft tissue in skin
� 85% cases are due to long duration acne, developing scar, chronic inflammatory dermatosis
� Histologically: dense viable bone in dermis or subcutaneous tissue
� Found in diffuse scleroderma, replaced altered collagen in dermis and subcutaneous septa
Clinical Features � Anywhere/ Face (COMMON SITE)
� Intraoral (Tongue*)- osteoma mucosae or osseous choristoma
� No visible changes. Colour changes occasionally appear yellowish white
� Large lesion can be palpated
� Needle inserted to one of the papules will feel stonelike resistance
� Numerous in some patients (dozens to hundreds) –multiple osteoma cutis
Radiographic Features � LOCATION: cheek and lips regions. May
superimposed with tooth root or alveolar process (appearance of dense bone).
� PERIPHERY AND SHAPE: smoothly outlined, RO, washer shaped image. Single or multiple usually small (0.1 to 5cm)
� INTERNAL STRUCTURE: � homogenously RO but usually has RL center (normal
fatty marrow) DONUT APPEARANCE. � Snow flake like RO- calcified cystic scar
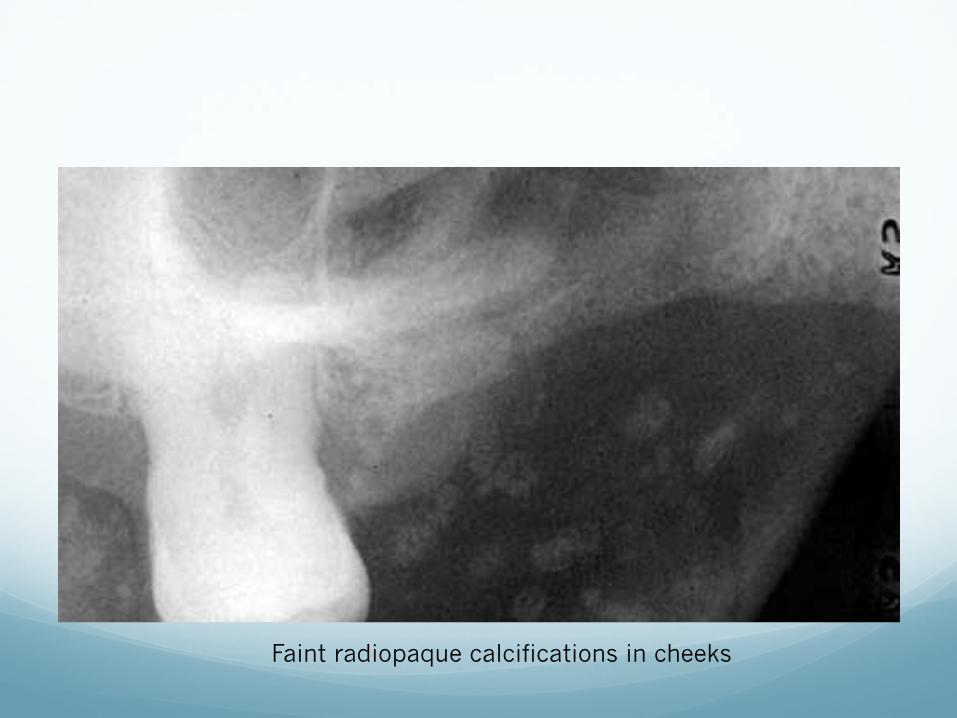
Faint radiopaque calcifications in cheeks
Differential Diagnosis � Myositis ossificans
� Calcinosis cutis
� Osteoma mucosae
� MANAGEMENT: NO RX. Removed for cosmetics reasons. � Resurface skin with ERB-Ytrium- Aluminum- Garnet
laser + Tretinoin cream successful in multiple miliary osteoma cutis
� Needle microincision-extirpation (good cosmetic results)
Myositis Ossificans � Fibrous tissue + heterotopic bone within the
interstitial tissue of muscle, associated tendons and ligaments
� Secondary destruction and atrophy to fibrous tissue and bone interdigitate and separate the muscle fibers.
� Localized and Progressive
Localized (Traumatic) Myositis Ossificans
� Synonyms: Posttraumatic myositis ossificans and solitary myositis
� From acute/ chronic trauma or from heavy muscular strain caused by occupations and sports
� From multiple injections (from dental anesthetic)
� Skeletal muscle limited capacity for regeneration after significant physical trauma.
Clinical Features � At any age can develop in either sex ( most often young
men)
� Site: � Trauma remains swollen, tender and painful � Overlying skin red and inflamed � Opening jaws difficult –(muscle of mastication)
� The localized lesion may enlarge slowly, will stop growing
� Fixed/ freely movable on palpation
� 2 to 3 weeks area of ossifications becomes apparent in the tissue , a firm intramuscular mass can be palpated
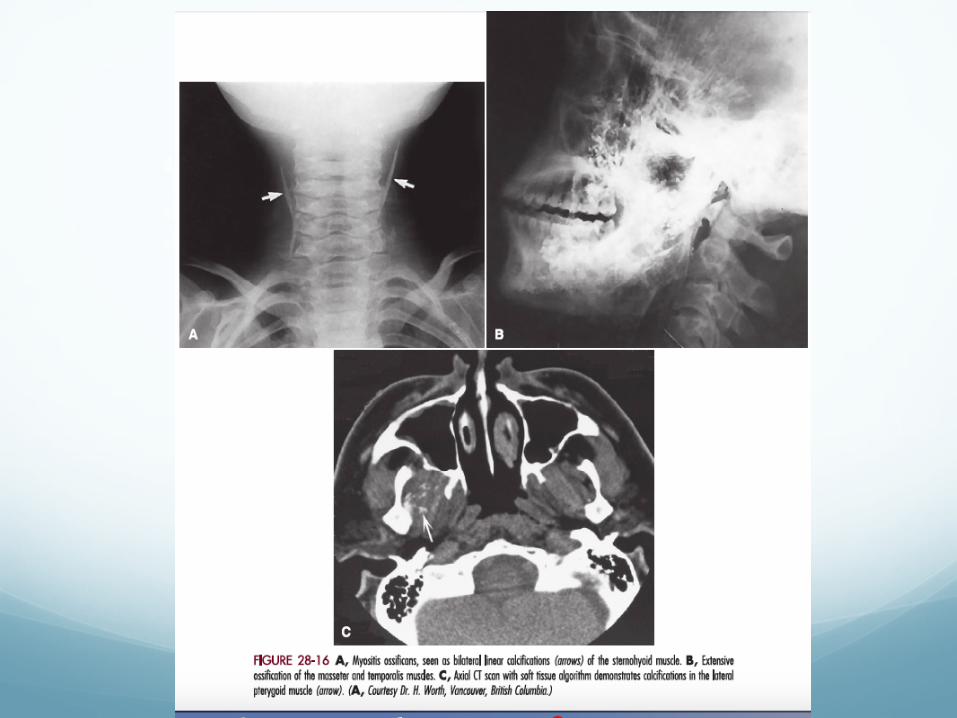
Radiographic Features � LOCATION:
� muscles of the head and neck and muscles of mastication � RL band can be seen between the area of ossification and adjacent bone. � Heterotopic bone - long axis of the muscle
� PERIPHERY AND SHAPE: � periphery is more RO than the internal structure. � Variation in shape from irregular oval to linear streaks (pseudotrabeculae)
running same direction as normal muscle fibers
� INTERNAL STRUCTURE: varies within time. � 3rd-4th week after injury- homogenously radiopacity � 2 months- delicate lacy or feathery radiopacity internal structure develops.
Indicates the formation of bone-not a normal- appearing trabecular pattern. � 5-6 months- denser, well defined and mature fully � After that, lesion may shrink

Differential Diagnosis � Ossification of the stylohyoid ligament and other
soft tissue calcification
� Bone forming tumours-osteogenic sarcoma > tumor is contiguous with the adjacent bone. Have signs of destruction of bone
� MANAGEMENT: � Rest and limitation to diminish extent of the calcific
deposit � Surgical excision of entire calcified mass with
intensive physiotherapy to minimize postsurgical scarring *
Progressive Myositis Ossificans
� Rare hereditary disease ( Autosommal Dominant transmission)
� Spontaneous mutation (less common)
� >Males and symptoms from early infancy
� Within interstitial tissue of muscles, tendons, ligaments and fascia
� Muscles atrophy
Clinical features � Most cases starts in muscles of neck and upper back and moves
to the extremities
� Soft tissue swelling, tender and painful, redness and heat
� Firm mass remains
� Striated muscles affected (heart and diaphragm)
� Limited to extensive
� Petrified Men- advance stage of the disease
� 3rd decade- process arrest
� 3rd to 4th decade- mostly patient died
� Premature death- respiratory embarassment or from initiation of muscles of mastication
Radiographic Features � Similar to limited form
� Oriented along long axis of muscles involved
� Osseous malformation at muscle attachment (mandibular condyles)
Differential Diagnosis � Initial stage – Rheumatoid Arthritis
� Calcinosis- deposits of calcium salts will resorb
� MANAGEMENT: NO AFFECTIVE RX � Traumatized and ulcerated nodules should be excised � Interference of respiration or respiratory infection
occurs, supportive therapy needed





























