Embed Size (px)
Citation preview

C
CtlqrgGitaurcoPtsi
taE
a
Int. J. Radiation Oncology Biol. Phys., Vol. 63, No. 1, pp. 5–24, 2005Copyright © 2005 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/05/$–see front matter
doi:10.1016/j.ijrobp.2005.03.047
RITICAL REVIEW
RADIATION PNEUMONITIS AND PULMONARY FIBROSIS INNON–SMALL-CELL LUNG CANCER: PULMONARY FUNCTION,
PREDICTION, AND PREVENTION
VIVEK MEHTA, M.D.
Department of Radiation Oncology, Swedish Cancer Institute, Seattle, WA
Although radiotherapy improves locoregional control and survival in patients with non–small-cell lung cancer,radiation pneumonitis is a common treatment-related toxicity. Many pulmonary function tests are notsignificantly altered by pulmonary toxicity of irradiation, but reductions in DLCO, the diffusing capacity ofcarbon monoxide, are more commonly associated with pneumonitis. Several patient-specific factors (e.g. age,smoking history, tumor location, performance score, gender) and treatment-specific factors (e.g. chemotherapyregimen and dose) have been proposed as potential predictors of the risk of radiation pneumonitis, but thesehave not been consistently demonstrated across different studies. The risk of radiation pneumonitis also seemsto increase as the cumulative dose of radiation to normal lung tissue increases, as measured by dose–volumehistograms. However, controversy persists about which dosimetric parameter optimally predicts the risk ofradiation pneumonitis, and whether the volume of lung or the dose of radiation is more important. Radiationoncologists ought to consider these dosimetric factors when designing radiation treatment plans for all patientswho receive thoracic radiotherapy. Newer radiotherapy techniques and technologies may reduce the exposureof normal lung to irradiation. Several medications have also been evaluated for their ability to reduce radiationpneumonitis in animals and humans, including corticosteroids, amifostine, ACE inhibitors or angiotensin IItype 1 receptor blockers, pentoxifylline, melatonin, carvedilol, and manganese superoxide dismutase-plasmid/liposome. Additional research is warranted to determine the efficacy of these medications and identify
nonpharmacologic strategies to predict and prevent radiation pneumonitis. © 2005 Elsevier Inc.ncwrai
lsaaFrppptpa
bIAt
INTRODUCTION
linical treatment guidelines recommend the use of radio-herapy in patients with locally advanced non–small-cellung cancer (NSCLC), good performance status, and ade-uate pulmonary function (1). Conventionally fractionatedadiotherapy for NSCLC consists of 1.8–2.0 Gy fractionsiven once daily for 5 days each week to a total dose of 60y or more. This treatment strategy is associated with
mproved locoregional control and survival (2), but radia-ion-induced lung toxicity such as radiation pneumonitisnd pulmonary fibrosis is common. Radiation pneumonitissually develops in the first few weeks to months afteradiotherapy is initiated and consists of symptomatichanges such as cough, shortness of breath, and fever, withr without changes in pulmonary function tests (PFTs).ulmonary fibrosis is the permanent scarring of lung tissue
hat occurs more gradually (over months to years) in re-ponse to the initial tissue injury and leads to permanentmpairment of oxygen transfer.
Reprint requests to: Vivek Mehta, M.D., Department of Radia-ion Oncology, Swedish Cancer Institute, 1221 Madison St., Se-ttle, WA 98104. Tel: (206) 386-2323; Fax: (206) 363-5907;-mail: [email protected] by a grant from MedImmune Oncology, Inc. The
uthor receives research support, has served on the speaker’s A
5
The incidence of moderate to severe radiation pneumo-itis ranges from roughly 10% to 20% with radiotherapy orhemoradiotherapy (3), but its reported incidence has variedidely in clinical studies for several reasons. The type of
adiotherapy and the presence or absence of neoadjuvant,djuvant, concurrent, or consolidation chemotherapy maynfluence the risk of radiation pneumonitis.
Underreporting of radiotherapy-induced pneumonitis isikely, particularly in retrospective studies, because the non-pecific symptoms of acute pneumonitis (shortness of breathnd cough, with or without mild fever) may be erroneouslyttributed to another cardiovascular or respiratory disorder.urthermore, patients may be asymptomatic but still haveadiographic evidence of radiation pneumonitis, and thisopulation is not reported in retrospective analyses. Even inrospective trials that include acute toxicity end points,atients are not always assessed for the presence of radia-ion pneumonitis (4, 5). Finally, some analyses includeatients who expire early (i.e., before it is reasonable tossume they could have developed radiation pneumonitis) in
ureau, and has served as a consultant for MedImmune Oncology,nc.cknowledgment—Jonathan N. Latham, Pharm.D., provided edi-
orial assistance.Received Dec 6, 2004, and in revised form Mar 14, 2005.
ccepted for publication Mar 16, 2005.

ti
atlmbasuttsptmmmdom
tausdtrrnarl
t
psaefumidspttp
g1imoobsNseap
hrlh
C
R
S
�E
Nb
6 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
he denominator of patients “at risk,” thereby artificially reduc-ng the true estimated incidence of radiation pneumonitis.
The morbidity and mortality directly attributable to radi-tion-induced lung toxicity are difficult to distinguish fromhe clinical consequences of NSCLC itself and the under-ying cardiorespiratory conditions in these patients. Theajor consequence of radiation pneumonitis is shortness of
reath, which leads to diminished quality of life and reducedctivities of daily living. These are particularly importantequelae in patients with locally advanced lung cancer, whosually undergo treatment to reduce symptoms rather thano increase life span. Mild to moderate symptomatic radia-ion pneumonitis may resolve with symptomatic treatmentuch as inhaled corticosteroid therapy (6). Severe radiationneumonitis is associated with significantly lower survivalhan mild or absent radiation pneumonitis (7), and theortality rate associated with severe radiation pneumonitisay approach 50% (8). Consequently, one analysis deter-ined that 2.3% of all patients who received thoracic ra-
iotherapy or chemoradiotherapy for advanced cancer diedf radiation pneumonitis (9), corresponding to approxi-ately 1 in 43 patients.Emerging clinical evidence suggests that identifying pa-
ients at risk of radiation pneumonitis, modifying radiother-py treatment to minimize doses to normal lung tissue, andsing radioprotective therapy may reduce the incidence andeverity of radiation pneumonitis, potentially increasing theose of radiotherapy that can be administered to NSCLCumors. The objective of this review was to briefly summa-ize recent findings that might influence how practicingadiation oncologists predict and prevent radiation pneumo-itis. The pathophysiology, etiology, and radiographic di-gnosis of radiation pneumonitis are not discussed in thiseview, and the reader is referred to other papers for excel-ent summaries of these topics (10–13).
This review begins with a summary of clinical studieshat evaluated the correlations between PFTs and radiation
Table 1. Toxicity
Criteria 1
TCAE Asymptomatic; radiographicfindings only
Symptomatiinterfering
TOG/EORTC(LENT-SOMA)
Asymptomatic or mildsymptoms (dry cough),with radiographic findings
Moderately(severe co
WOG (33) Asymptomatic or symptomsnot requiring steroids,with radiographic findings
Initiation ofin steroids
Abbreviations: CTCAE � Common Terminology Criteria for ARadiation Therapy Oncology Group; EORTC � European Organ
ffects on Normal Tissues-Subjective, Objective, Management anNote: Data from Cancer Therapy Evaluation Program, Commo
IH, DHHS, December 12, 2003 (http://ctep.cancer.gov/reporting
idity Scoring Criteria (http://www.rtog.org/members/toxicity/acute.htmlneumonitis, because these tests are frequently used asurrogate end points for the presence and severity of radi-tion pneumonitis. The next sections describe studies thatvaluated patient-specific and treatment-specific risk factorsor radiation pneumonitis, with particular attention to these of dose–volume histograms (DVHs) and various dosi-etric parameters that are used to estimate risk; this section
s followed by a brief review of potential biochemicaletection markers for radiation pneumonitis. The remainingections of the review describe how the risk of radiationneumonitis might be influenced by evolving radiotherapyreatment strategies; also discussed is preliminary evidencehat cytoprotective medications might reduce radiationneumonitis.
PULMONARY FUNCTION MEASURES AFTERRADIATION THERAPY
Major determinants of gas exchange in the lung includeas movement (measured by forced expiratory volume ins [FEV1]), lung capacity (measured by forced vital capac-
ty [FVC]), and diffusion of gases (measured by carbononoxide diffusing capacity [DLCO]). However, the severity
f pneumonitis usually is defined according to the presencer absence of symptoms such as cough and shortness ofreath, as well as the treatment that is required for theseymptoms (Table 1), rather than on the basis of PFTs.onetheless, extensive research has evaluated the relation-
hip between PFTs and the radiographic and symptomaticvidence of radiation pneumonitis in an attempt to use PFTss markers or predictors for the incidence and severity ofneumonitis.In patients undergoing lung resection, several studies
ave suggested that changes in postoperative PFTs areelated to the amount of perfused lung resected. Over theast several decades, investigators at different institutionsave attempted to correlate changes in PFTs after radiother-
for pneumonitis
3 4 5
ADLSymptomatic;
interfering withADL; O2 indicated
Life-threatening;ventilatorysupport indicated
Death
maticever)
Severely symptomatic Severe respiratoryinsufficiency;continuousoxygen/assistedventilation
Death
reasered
O2 required Assisted ventilationnecessary
Death
Events; ADL � activities of daily living; O2 � oxygen; RTOGfor the Research and Treatment of Cancer; LENT-SOMA � Late
lytic Scales; SWOG � Southwest Oncology Group.inology Criteria for Adverse Events, Version 3.0, DCTD, NCI,
ml); Radiation Therapy Oncology Group, Acute Radiation Mor-
criteria
2
c; notwith
symptough, f
or increqui
dverseizationd Anan Term/ctc.ht
); and Ref. 33.

ahcptmbswafidcd7ssabs
DpowRl
sge1aGdGmFt
asocSat71tmr0tw
R
C
C
A
RSADG
M
c
w
7Radiation pneumonitis in NSCLC ● V. MEHTA
py to percentage of perfused lung irradiated. Recently, itas become apparent that changes in regional perfusion areorrelated only weakly with global changes in PFTs. In onerospective study, 53 patients (36 of these patients werereated for lung cancer) underwent postradiotherapy treat-ent evaluations that included studies of regional perfusion
y single photon emission computed tomography perfusioncans (SPECT) and PFTs (14). Most of the patients whoere treated for lung cancer received 40–45 Gy using
nterior and posterior fields, followed by off-cord obliqueelds to approximately 66 Gy in fractions of 1.8–2.0 Gyaily. Thirteen patients received 1.25 Gy twice daily to thelinical target volume and 1.6 Gy twice daily to the grossisease (minimum 6-h interfraction interval) to a total of3.6 Gy. Among all patients, regardless of tumor type, aignificant but modest correlation was found between theum of changes in regional perfusion (measured by SPECT)nd changes in FEV1 (r � 0.40, p � 0.001). The correlationetween regional perfusion and DLCO was smaller and non-ignificant (r � 0.16, p � 0.24).
Although the correlation between regional perfusion andLCO was smaller than the correlation between regionalerfusion and FEV1 in that study, the opposite is usuallybserved; DLCO is affected more by local lung dysfunction,hereas FEV1 is influenced more by gross obstructions.eported reductions in FEV1 after photon radiotherapy for
ung cancer were 12% or less from baseline in numerous
Table 2. Mean changes in pulmonary functio
Reference No. Dose/fraction,* G
ubenstein et al., 1988 (15) 22 50–61/1.8–2.0 q.d.
hoi et al., 1990 (16)Lobectomy 49 54/1.8 q.d.Pneumonectomy 22 54/1.8 q.d.
hoi and Kanarek, 1994 (17)Group A† 80 58/NRGroup B† 33 59/NRGroup C† 22 58/NR
bratt and Willcox, 1995(18)
51 50–55/2.5 q.d., or45–48/3.0 q.d.
obert et al., 1999 (19) 43 60/2.0 q.d.unyach et al., 2000 (20) 54 66/2.0 q.d.llen et al., 2003 (21) 43 76.9/2.1 q.d.e Jaeger et al., 2003 (22) 82 70/2.0 q.d.opal et al., 2003 (23) 100 70.95/2.15 q.d., or
63/1.8–2.0 q.d. � CT,69.6/1.2 b.i.d. � CT
iller et al., 2003 (24) 13§ NR
Abbreviations: DLCO � diffusing capacity of carbon monoxide iapacity; q.d. � once daily; b.i.d. � twice daily; NR � not repor
* Reported as the median dose or range of radiotherapy doses.† Group A: patients with FEV1 �50% predicted at baseline; Gro
ith �10% shift of ventilation or perfusion to the uninvolved sid‡ Reported as the change in the ratio of FEV1:vital capacity.§ Number of patients with 2 years of disease-free survival and
� Annual rate of decline after 1 year.tudies, whereas reductions in DLCO were usually 13% orreater from baseline in those studies (Table 2) (15–24). Forxample, a retrospective study was performed on data from00 patients in 5 trials where patients received radiotherapylone (2.15 Gy fractions to a total median dose of 70.95y), or sequential or concurrent chemoradiotherapy (once-aily fractions of 1.8–2.0 Gy or twice-daily fractions of 1.2y) (23). That study determined that the median posttreat-ent values for DLCO, total lung capacity (TLC), and FEV1/VC were 74%, 94%, and 100% of baseline values, respec-
ively.In fact, many patients experience improvement in PFTs
fter radiotherapy, probably because reductions in tumorize lead to reduced lung obstruction. In one prospective,bservational study of 82 patients with inoperable lungancer, PFTs, computed tomography (CT) scans, andPECT lung perfusion scans were performed at baselinend 3–4 months after three-dimensional conformal radio-herapy (3D-CRT) consisting of 70 Gy in 35 fractions over
weeks (22). DLCO and FEV1 were reduced by a mean of4% and 6% from baseline, respectively, but 21% of pa-ients had improvements in DLCO, and 38% had improve-ents in FEV1. Multivariate analysis revealed that tumor
eduction was correlated with improvement in FEV1 (p �.02), and it tended to reduce DLCO (p � 0.05). Notably,hese associations were independent of whether the tumoras located centrally or peripherally in the lung.
during photon radiotherapy for lung cancer
Follow-up,months DLCO FEV1 TLC
2–6 NR �2% NR6–12 NR �12% NR�12 NR �10% NR
12 NR �1.1% �3.8%12 NR �0.6% �2.0%
12 �27% �19% to �20% �13%12 �11% �1% to �8% 0%12 NR �4% to �7% �21%
6 (n � 42) �14% �2% �7%12 (n � 22) �13% �3% �8%
5–6 �20% �9.2% �11%1.5 �5.7% �0.1% �7.2%
6.2 (median) �13% �1% NR3–4 �14% �6% NRNR �26% �6%‡ 0%
38 (median) �3.5%� �7%� NR
ung; FEV1 � forced expiratory volume in 1 s; TLC � total lungT � chemotherapy.
atients with FEV1 �50% predicted at baseline; Group C: patientse lung, regardless of FEV1 at baseline.
-up pulmonary function tests.
n tests
y
or
n the lted; C
up B: pe of th
follow

frcdd1(Aar(i(atarfcd�
aDataarp
bsDu
ratm1�dfdtGotasecsd
P
t
B
SJLBMY
RQR
H
R
C
8 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
Long-term survival rates are generally poor for NSCLC, soew studies have evaluated the long-term effects of thoracicadiotherapy on PFTs (Table 2). An early study of PFThanges after radiotherapy for lung cancer reported only a 2%ecrease from baseline 2–6 months after radiotherapy, a 12%ecrease from baseline 6–12 months after radiotherapy, and a0% decrease from baseline �12 months after radiotherapy15). Changes in DLCO and TLC were not reported in that study.
subsequent study of conventional adjuvant radiotherapyfter lobectomy or pneumonectomy in a total of 71 patientseported little or no worsening of FEV1 after 12 months�1.1% and �0.6%, respectively), and only slight reductionsn TLC (�3.8% and �2.0%, respectively) over that period16). Significant worsening of DLCO from baseline was reportedt 6 months (�14%) and 12 months (�13%) in one prospec-ive study of 51 patients, of whom 42 provided 6-month datand 22 provided 12-month data (18). Despite the use of highadiotherapy fractions in that study (50–55 Gy in 2.5 Gyractions or 45–48 Gy in 3 Gy fractions), only modest de-reases were reported in PFTs at 6 and 12 months: FVCecreased by �6% and �5%, TLC decreased by �7% and8%, and FEV1 decreased by �2% and �3%, respectively.Acute impairment of lung capacity resulting from radiother-
py may resolve initially and then worsen chronically, whereasLCO impairment progresses after radiotherapy, even in the
bsence of tumor recurrence. A prospective study with long-erm follow-up was performed in 128 patients with unresect-ble lung cancer, of which 13 patients had disease-free survivalnd follow-up PFTs for at least 2 years after definitive thoracicadiotherapy (24). Median values for FEV1 and FVC in thoseatients decreased at 6 months, returned to approximately
Table 3. Clinical factors that may influence the rate of symptomAdapted from
Author No. Incr
rooks et al., 1986 (26) 80 Chemothe
chaake-Koning et al., 1992 (27) 331eremic et al., 1996 (28) 131ee et al., 1996 (29) 79 Chemotheyhardt et al., 1998 (30) 461 Concurrenonson et al., 1998 (31) 83 Smokingamada et al., 1998 (32) 60 Tumor loc
Concurrenobert et al., 1999 (19) 43 Chemotheuon et al., 1999 (33) 608obnett et al., 2000 (34) 148 Women
Low KPSernando et al., 2001 (35) 201
ancati et al., 2003 (36) 84
laude et al., 2004 (37) 96 Age
Abbreviations: KPS � Karnofsky performance status.
aseline values by 12 months, and then decreased progres-ively by 7% and 9.5% annually thereafter. Median values forLCO decreased progressively but gradually throughout follow-p, with an annual rate of decline of 3.5% after 1 year.
Measurable decreases in DLCO may also occur at even lowadiation doses. In the retrospective analysis describedbove that included 5 trials of radiotherapy or chemoradio-herapy (23), 44 of 100 patients had three-dimensional treat-ent planning and PFTs available for analysis. For every
% increase in the volume of normal lung tissue receiving20 Gy, total lung capacity decreased by 0.8%, and DLCO
ecreased by 1.3%. The same group of investigators per-ormed a separate analysis of 26 of these patients andetermined that a pronounced decrease in DLCO occurs whenhe local dose of radiotherapy to normal tissue exceeds 13y (25), based on mathematical modeling. This effect wasbserved regardless of whether patients received daily frac-ions of 2.15 Gy or twice-daily fractions of 1.2 Gy. Theuthors further noted that Grade 2 or higher pulmonaryymptoms typically accompanied DLCO loss of �30%, soven small doses of radiation to normal tissue may havelinically significant effects on lung function. Therefore,trategies are needed to predict and prevent the severity ofamage to normal lung tissue.
PREDICTING RISK OF RADIATIONPNEUMONITIS
atient characteristicsSeveral studies were conducted to identify clinical factors
hat predict the occurrence or severity of radiation pneumonitis
iation pneumonitis in patients with non–small-cell lung cancer.do et al. (32)
risk No change in risk Decreased risk
AgeKPSChemotherapyChemotherapy
otherapyChemotherapy Surgery
otherapy
AgeChemotherapy timingTumor siteAgeTumor location
Smoking
AgeChemotherapy
Surgery
GenderKPSSmokingSurgeryChemotherapy
atic radHernan
eased
rapy
rapyt chem
ationt chemrapy

(d
wmctpftsrtpmp(sw
erswbetoni
pvr(pnrpcc0ldfm(en
igraroc
pcns�ihnsip
C
aptoraGbrrao(Nanri�acaprrrgt
rppcGartps1bm
9Radiation pneumonitis in NSCLC ● V. MEHTA
19, 26–37). Unfortunately, much of the evidence for indepen-ent risk factors was inconsistent and inconclusive (Table 3).
For example, there is conflicting evidence regardinghether tumor location influences the risk of radiation pneu-onitis. A retrospective analysis of 60 patients with lung
ancer who received chemotherapy plus conventional radio-herapy reported that 28% of patients had Grade �2 radiationneumonitis (32). Radiation pneumonitis was more commonor irradiation of the lower lobe (70%) than for irradiation ofhe middle or upper lobes of the lung (20%). Another retro-pective analysis of 137 patients who received conventionaladiotherapy and 7 patients who received hyperfractionatedwice-daily radiotherapy reported that the risk of radiationneumonitis was comparable for patients with upper-lobe tu-ors (8% crude risk of severe radiation pneumonitis) com-
ared with those who had middle- or lower-lobe tumors (9%)34). However, the latter study did not evaluate the risk ofevere radiation pneumonitis separately for just those patientsith lower-lobe tumors.Age is another potential risk factor for which conflicting
vidence has been published. One recent study reported thatadiation pneumonitis was more common, but not moreevere, in elderly patients who received 3D-CRT (37),hereas another study reported the opposite (more severeut not more common) in elderly patients who receivedither conventional radiotherapy with etoposide and cispla-in or hyperfractionated radiotherapy alone (38). In severalther studies, older patients tended to have radiation pneumo-itis more often than younger patients, but age was not anndependent risk factor for radiation pneumonitis (26, 34–36).
Pulmonary dysfunction before radiotherapy may predis-ose patients for radiation pneumonitis (7, 31, 36). A PaO2
alue of �80 was independently associated with severeadiation pneumonitis more often than a higher PaO2 value19% vs. 5%, p � 0.034) in a retrospective analysis of 191atients with lung cancer (7), but other measures of pulmo-ary function before irradiation did not predict the risk ofadiation pneumonitis. Another retrospective study of 84atients with lung cancer determined that the presence ofhronic obstructive pulmonary disease before 3D-CRT in-reased the risk of radiation pneumonitis 4.82-fold (p �.026) (36). A prospective study with 12 months of fol-ow-up data in 135 patients with unresectable lung canceretermined that patients with good pretreatment pulmonaryunction (FEV1 �50% predicted) experienced larger decre-ents in PFTs than patients with poor function at baseline
FEV1 �50% predicted) (Table 2) (17); however, the pres-nce or absence of symptoms of radiation pneumonitis wasot reported in that study.Despite evidence that preexisting pulmonary dysfunction
ncreases the risk of radiation pneumonitis, one study sug-ested that ongoing smoking may in fact protect againstadiation pneumonitis in patients with NSCLC (35). Theuthors noted that this finding was consistent with similaresults in patients who received thoracic radiotherapy forther tumor types (39). In another study, 83 patients re-
eived definitive radiotherapy (median dose, 54 Gy; most matients received fractions of 1.8–2.0 Gy daily) for lungancer. The development of radiation pneumonitis was sig-ificantly more common among patients with a history ofmoking than among those who never smoked (31), but10% of the patients in that study had no history of smok-
ng, potentially confounding the results. It is possible that aistory of smoking increases the risk of radiation pneumo-itis as a result of preexisting lung damage, but activemoking somehow protects the lungs from radiotherapy-nduced damage. Further study is needed to elucidate thearadoxical role of smoking in radiation pneumonitis.
hemotherapySeveral treatment-specific factors also have been evalu-
ted for their potential influence on the risk of radiationneumonitis. As noted in Table 3, chemotherapy increasedhe risk of radiation pneumonitis in some studies, but not inthers. A randomized trial of 331 patients with NSCLCandomly assigned patients to treatment with radiotherapylone (total of 60 Gy given in a split-course fashion of 30y in 10 daily fractions of 3 Gy with a 3-week rest periodetween courses), radiotherapy plus weekly cisplatin, oradiotherapy plus daily cisplatin (27). The incidence ofadiotherapy injury on chest films was not greater with theddition of weekly cisplatin (50% overall, 23% Grade 3–4)r daily cisplatin (65%, 34%) than with radiotherapy alone70%, 30%). In a subsequent study of 131 patients withSCLC, carboplatin and etoposide were added to radiother-
py (69.6 Gy delivered in twice-daily doses of 1.2 Gy), ando increased acute or late bronchopulmonary toxicity waseported (28). However, an analysis of 5 clinical trialsncluding 461 patients with NSCLC concluded that Grade
3 late lung toxicity was significantly more commonmong patients who received induction plus concurrentisplatin-based chemotherapy with conventional radiother-py (incidence, 21%) or concurrent chemotherapy with hy-erfractionated radiotherapy (20%) than among those whoeceived only induction chemotherapy before conventionaladiotherapy (10%) (29). The authors noted that the greaterisk of severe toxicity might have influenced some oncolo-ists to make chemotherapy dosing alterations to reduceoxicity, thereby reducing efficacy as well.
The use of taxane chemotherapy may also influence theisk of radiation pneumonitis. The incidence of Grade �2ulmonary toxicity was 70% in a Phase I/II study of 24atients with NSCLC who were treated with paclitaxel/isplatin concurrently with conventional radiotherapy (60y given in 2.0 Gy fractions over 6 weeks) (19). Based oncomparison of these findings to those in a literature
eview, the authors concluded that paclitaxel-based chemo-herapy might be associated with a slightly higher risk ofulmonary toxicity. However, a subsequent retrospectivetudy of potential risk factors for radiation pneumonitis in44 patients with lung cancer, including 37 with paclitaxel-ased chemotherapy and 102 with nonpaclitaxel-based che-otherapy (5 patients had unknown chemotherapy regi-
ens), found that the risk of radiation pneumonitis was not
imwmps2n
cic3GtwvagstarlAwmtacarvcrptiotT(oorod
twco0ntcw
lbotb(srp1artacmmtliDiiww
D
i
FopwrpiJop(
10 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
ncreased significantly with the use of paclitaxel-based che-otherapy (10% vs. 8%, p � 0.59) (34). In that study,omen were more likely than men to have radiation pneu-onitis (15% vs. 4%, p � 0.01), and the risk of radiation
neumonitis was greater among patients with performancetatus of 1 than those with performance status of 0 (16% vs.%), but other studies found that these clinical factors wereot predictive of risk (32, 36).
Other chemotherapeutic agents for the treatment of lungancer that may increase the risk of radiation pneumonitisnclude mitomycin C, gemcitabine, irinotecan, and do-etaxel. In a retrospective study of 84 patients who receivedD-CRT for lung cancer, the 6-month actuarial rates ofrade �2 radiation pneumonitis were 31.2% among pa-
ients who received mitomycin C and 10.6% among thoseho did not (36), whereas vinca alkaloids (vinorelbine orindesine) and gemcitabine were not independently associ-ted with increased risk of radiation pneumonitis. However,emcitabine was used by only 8 (10%) patients in thattudy, and the dose of gemcitabine was not noted. In con-rast, in a prospective study of 27 patients with locallydvanced NSCLC, all of whom received gemcitabine withadiotherapy, Grade 3 radiation pneumonitis was the dose-imiting toxicity at a dose of 450 mg/m2 once weekly (40).nother prospective study found that radiation pneumonitisas a dose-limiting toxicity for gemcitabine at a dose of 50g/m2 twice-weekly with concurrent radiotherapy in pa-
ients with locally advanced NSCLC (41). A retrospectivenalysis of 60 patients who received chemotherapy withonventional radiotherapy for lung cancer determined thatny use of irinotecan tended to increase risk of Grade �2adiation pneumonitis overall, albeit nonsignificantly (41%s. 21%) (32). Among the patients who received concurrenthemotherapy in that analysis, the incidence of Grade �2adiation pneumonitis was significantly higher among thoseatients who received irinotecan (56%) compared withhose who did not (14%). Another prospective, nonrandom-zed study was performed to evaluate the efficacy and safetyf combining weekly docetaxel with conventional radio-herapy for the treatment of lung cancer in 32 patients (42).he response rate to the combination was 91%, but 15
47%) patients developed Grade �3 radiation pneumonitis,f which 6 (19%) had fatal pulmonary toxicity. In response,ther investigators reported also that they observed severeadiation pneumonitis in 3 of 7 patients in their pilot studyf concurrent treatment with conventional radiotherapy andocetaxel (43).
As noted above, timing of chemotherapy may influencehe risk of radiation pneumonitis. The analysis of 60 patientsho received concurrent or sequential chemotherapy with
onventional radiotherapy (32) determined that the overalldds ratio of Grade �2 radiation pneumonitis was 1.42 (p �.30) for regimens that included irinotecan vs. those that didot; the odds ratio increased to 2.67 (p � 0.038) when justhose patients who received concurrent chemotherapy wereonsidered. Likewise, the pooled analysis of 461 patients
ith NSCLC in 5 trials determined that the incidence of 5ate-effect lung toxicity was higher for concurrent platinum-ased chemotherapy with conventional radiotherapy (21%)r concurrent platinum-based chemotherapy with hyperfrac-ionated radiotherapy (20%) than for sequential platinum-ased chemotherapy and conventional radiotherapy (10%)30). However, a subsequent analysis of 144 patients at aingle center failed to confirm these results (34); the crudeisk of Grade �3 radiation pneumonitis was 7% amongatients who received concurrent chemoradiotherapy and1% among those who received sequential chemoradiother-py. Another retrospective analysis of 100 patients whoeceived conventional radiotherapy or 3D-CRT concludedhat the use of any chemotherapy is predictive of lower DLCO
fter radiotherapy (p � 0.029), and the use of concurrenthemotherapy reduces the diffusing capacity of the lungore than sequential chemotherapy (p � 0.028), but che-otherapy does not influence the severity of lung obstruc-
ion or restriction (23). Furthermore, the volume of normalung that is exposed to a specific dose of irradiation (Vdose)s associated with changes in DLCO (See “Predicting risk:ose–volume histograms,” below). Combined, these find-
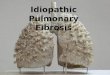
ngs may explain why the correlation between Vdose and thencidence of radiation pneumonitis is stronger for patientsho receive chemoradiotherapy than among those patientsho receive only radiotherapy (Fig. 1) (44).
ose–volume histogramsThe dose schedule and dose intensity of radiotherapy
nfluence the risk of toxicity. A pooled analysis of 1,911
ig. 1. Incidence of Grade �2 radiation pneumonitis as a functionf the relative lung volume irradiated to more than 20 Gy (V20) ofatients treated with radiotherapy alone (open circles, n � 382) orith chemoradiotherapy (closed circles, n � 71) (44). Patients
eceiving chemotherapy had a sharper increase in risk of radiationneumonitis as the volume of normal lung exposed to 20 Gyncreased. Reprinted with permission from Seppenwoolde Y, Deaeger K, Lebesque JV. In regard to Tsujino et al. Predictive valuef dose-volume histogram parameters for predicting radiationneumonitis after concurrent chemoradiation for lung cancerIJROBP 2003;55:110–115). Int J Radiat Oncol Biol Phys 2003;
6:1208–1209 (44).
pddmd(Grr
mlapaddncdsptoa
udm(wGppp4sn
a12pwc2l3nppawuAp2rwapTw1powaC1iuVo
FdVa
A
G
H
C
11Radiation pneumonitis in NSCLC ● V. MEHTA
atients in 24 studies who received conventional chemora-iotherapy for lung cancer determined that higher totaloses of radiotherapy increased the risk of radiation pneu-onitis; incidences were 6% for total doses �45 Gy, 9% for
oses of 45 to 54 Gy, and 12% for doses of at least 55 Gy3). Greater individual fraction size of radiotherapy (�2.67y once daily) and the use of once-daily vs. twice-daily
adiotherapy were also associated with increased risk ofadiation pneumonitis in those studies.
The most consistent predictor of pneumonitis is the cu-ulative dose of radiotherapy that is administered to normal
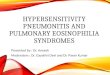
ung tissue, but it can be difficult to assess these dosesccurately. The use of 3D-CRT for NSCLC results in com-lex dose distribution patterns within the lung, so multiplelgorithms were created to simplify assessment of 3D doseistribution. A DVH commonly is calculated from the ra-iotherapy treatment plan to estimate the percentage of theormal lung tissue that will be exposed to a particularumulative dose of radiotherapy (Fig. 2). On this two-imensional representation, the horizontal axis represents apecific radiation dose. The vertical axis represents theroportion of the lung volume that will receive more thanhis dose of radiation. V20, V30, and V40 are the percentagesf the total volume of lung that receive �20 Gy, �30 Gy,nd �40 Gy, respectively.
Several studies have demonstrated that higher Vdose val-es (i.e., exposure of larger volumes of lung to a specificose) are associated with increased risk of radiation pneu-onitis in patients receiving radiotherapy for lung cancer
Table 4). In one study (45), 31 patients with lung cancerere treated with 3D-CRT (median total dose, 70.2 Gy).rade �3 radiation pneumonitis occurred in 38% (3/8) ofatients with V25 values of �30% and in only 4% (1/23) ofatients with V25 values of �30%; the single fatality due toulmonary toxicity occurred in a patient with a V25 value of9%. Of the dosimetric parameters evaluated in anothertudy of 99 patients with NSCLC (46), only V20 was sig-ificantly associated with risk of Grade �2 pneumonitis
ig. 2. Hypothetical dose–volume histogram describing three-imensional radiotherapy dose distribution for normal lung tissue.
and V represent the percent volume of the lungs exposed to
p20 30
t least 20 Gy or at least 30 Gy, respectively.
fter 3D-CRT, and the actuarial incidences were 0%, 7%,3%, and 36% among patients with V20 values of �22%,2%–31%, 32%–40%, and �40%, respectively. All fatalneumonitis occurred in patients who received 3D-CRTith a V20 of �35%, and all high-grade pneumonitis oc-
urred in patients with a V20 of �32%. A DVH analysis of01 patients who received conventional radiotherapy forung cancer found that mean V20, V30, and V40 values were4.7%, 29.9%, and 24.4% among patients in the pneumo-itis group (n � 39) and 28.7%, 23.8%, and 20.2% amongatients in the nonpneumonitis group (n � 162); all com-arisons between groups were statistically significant. Innother study (47), V20, V25, and V30 were all associatedith increased risk of Grade �2 pneumonitis after contin-ous hyperfractionated accelerated radiotherapy (CHART).mong the 2 patients with pneumonitis and 30 withoutneumonitis, values for V20, V25, and V30 were 42% vs.3.5%, 38% vs. 21%, and 31% vs. 17.2%, respectively. Aetrospective study of 71 patients with lung cancer whoere followed for �3 months, without locoregional failure,
fter conventionally fractionated radiotherapy found that 20atients developed Grade �2 radiation pneumonitis (48).he mean V20 values according to severity of pneumonitisere 20.1%, 22.0%, 26.3%, 27.0%, and 34.5% for Grade 0,, 2, 3, and 5, respectively. Overall, Grade �2 radiationneumonitis was more common in patients with V20 valuesf �26% than in those with V20 values of �25%, and V20
as predictive of Grade �2 pneumonitis on multivariatenalysis. In a prospective analysis of 90 patients after 3D-RT for NSCLC (37), the threshold values of 18% for V20,3% for V30, and 10% for V40 were all associated withncreased risk of radiation pneumonitis (any severity) onnivariate and multivariate analyses. The cutoff values for
20 and V30 were also predictive of Grade �2 pneumonitisn univariate analyses, but multivariate analyses were not
Table 4. Incidence of radiation pneumonitis according to Vdose
in patients treated with radiotherapy for lung cancer
ReferenceSeverity ofpneumonitis Vdose
Observedrate
rmstrong et al.,1995 (45)
Grade �3 V25 �30% 38%V25 �30% 4%
raham et al.,1999 (46)
Grade �2 V20 �22% 0%V20 22%–31% 7%V20 32%–40% 13%V20 �40% 36%
ernando et al.,2001 (34)
Grade �1 V30 �22% 6%V30 22%–31% 24%V30 32%–40% 18%V30 �40% 29%
laude et al.,2004 (36)
Grade �1 V10 �33% 53%V20 �18% 56%V30 �13% 56%V40 �10% 56%V50 �5% 53%
erformed for these associations.

M
mN3b7ilppapw((rvaNedfNi(rGpGNrpopbpni
N
ctmmocrcnstanmi
wuCoaacwp2rtcmhwt(rr(g
wb�pt20sNNsrN�
cdat(mclmapedlapwa
12 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
ean lung dose (MLD or NTDmean)Data from the DVH can also be used to calculate theean biologic lung dose (MLD or NTDmean). An analysis ofTDmean values in 540 patients at 5 centers who receivedD-CRT for lung cancer (n � 399), lymphoma (n � 78),reast cancer (n � 59), and other tumor types reported that3 patients had Grade �2 radiation pneumonitis (49). Thenvestigators determined that an NTDmean of 30.5 Gy wasikely to result in pneumonitis in approximately 50% ofatients (NTD50). Other studies at individual institutionsrovided further evidence of a relationship between NTDmean
nd risk of radiation pneumonitis. A random sample of 46atients with lung cancer was analyzed retrospectively, ofhich 9 developed symptomatic radiation pneumonitis
NTDmean � 23.8 Gy) and 37 did not (NTDmean � 20.1 Gy)50). In a subsequent study of 201 patients, most of whomeceived 2 Gy daily to a total dose of �60 Gy, NTDmean
alues were 20.66 Gy in the pneumonitis group (n � 39)nd 16.98 Gy in the nonpneumonitis group (n � 162) (35).ine (18.4%) of 49 patients at another institution experi-
nced Grade �3 radiation pneumonitis during a 3D-CRTose-escalation trial (70.2–81 Gy total dose in 1.8 Gy dailyractions), and the risk of pneumonitis was correlated withTDmean values for the total lung (p � 0.04) and for the
psilateral lung (p � 0.03), but not for the contralateral lungp � 0.30) (51). Investigators from several centers in Franceecently reported that 40 (44%) of 90 evaluable patients hadrade �1 radiation pneumonitis and 7 (8%) had Grade �2neumonitis within 6 weeks after 3D-CRT for NSCLC (2y daily to a median total dose of 66 Gy) (37). TheTDmean values were 13 Gy for patients with Grade �1
adiation pneumonitis and 10 Gy for those without anyneumonitis. NTDmean was associated with a 1.11 relative riskf any severity of pneumonitis on multivariate analysis, and itredicted risk of Grade �2 pneumonitis on univariate analysis,ut multivariate analyses were not performed for the latter endoint (37). However, the risk of Grade �2 radiation pneumo-itis was not associated with NTDmean on multivariate analysisn 2 other studies described above (36, 46).
ormal-tissue complication probability (NTCP)Another dosimetric parameter, the normal-tissue compli-
ation probability (NTCP), is based on the assumption thathe probability of pulmonary complications follows a sig-oidal dose–response relationship. This approach usesathematical models based on the tolerance dose for whole-
rgan irradiation and the steepness of the dose–responseurve to calculate the probability of pulmonary damageesulting from irradiation (52, 53). Correlations betweenalculated NTCP values and the risk of radiation pneumo-itis in lung cancer patients were documented by severaltudies. Among 42 lung cancer patients who underwent 3Dreatment planning in one study, the NTCP average valuesmong all 84 lungs were 73% for the patients with pulmo-ary complications and 25% for the patients without pul-onary complications (54). Another study reported signif-
cant differences in NTCP values for patients with and m
ithout Grade �2 radiation pneumonitis (19.6% vs. 12.0%)sing the Lyman algorithm for both lungs combined (35).ombining or separating the lungs may influence the abilityf NTCP to predict pneumonitis risk. When the ipsilateralnd contralateral lungs were evaluated separately in anothernalysis of 46 lung cancer patients, most of whom receivedonventional radiotherapy, the NTCP in the ipsilateral lungas 37.0% vs. 20.2% among patients with and withoutneumonitis using the Lyman algorithm and 39.8% vs.2.8% using the Kutcher algorithm (50). However, similaresults were not obtained in that study when the lungs werereated as a paired organ. Another study of 146 patients whoompleted 3D-CRT combined with chemotherapy deter-ined that the mean NTCP value for the ipsilateral lung was
igher in the group with pneumonitis (66.0%) vs. the groupithout pneumonitis (26.4%), but average NTCP values for
he lung as a paired organ were not significantly different55). Furthermore, in a study of 49 NSCLC patients whoeceived 3D-CRT, NTCP was correlated with pneumonitisisk in the lower lobe but not in the upper lobe of the lungNTCP values in the pneumonitis and nonpneumonitisroups were not reported) (51).Conversely, the ability of NTCP to accurately predict
hich patients will experience radiation pneumonitis haseen evaluated in a few studies. Using an NTCP value of12% for both lungs combined as a cutoff, a study of 31
atients who received 3D-CRT for lung cancer determinedhat the incidence of Grade �3 radiation pneumonitis was9% among the patients with an NTCP value of �12% and% among the patients with an NTCP value of �12%; aingle fatality in that study occurred in a patient with anTCP value of 85% (45). Another study evaluated theTCP values for the ipsilateral and contralateral lungs
eparately, with a cutoff value of 30% (50). The observedates of pulmonary toxicity were 13% for patients with anTCP of �30% and 29% for those with an NTCP of30%.Early studies of NTCP parameters did not use density
orrection algorithms to account for inhomogeneity in theose of radiation delivered (52, 56). Subsequent studiesttempted to improve accuracy by incorporating reduc-ion algorithms such as the equivalent path length model49, 54, 57), parallel functional subunit models (58, 59),odels that included baseline perfusion (60), or complex
onvolution-superposition algorithms (61, 62). An ana-ytical comparison of two DVH reduction models deter-ined that they provided identical results (63). In other
nalyses, the more complex algorithms were found torovide more accurate estimates of radiation dose deliv-red, resulting in a lower estimate of actual irradiationose to normal tissue and a lower TD50 value (61, 62). Asong as the correct TD50 value was used, the simplerlgorithms and the more complex algorithms had similarredictive power for radiation pneumonitis. In otherords, the risk of radiation pneumonitis associated withspecific course of treatment in a specific patient re-
ained approximately the same with different reduction
am
S
arNrpidNmVtbnwmiw�mrdbt
iivtcp
“
ile3cdnVrBdpn
rcfdl
13Radiation pneumonitis in NSCLC ● V. MEHTA
lgorithms, although the values of the dosimetric esti-ates changed.
electing a dosimetric parameterAlthough several dosimetric parameters are available to
ssess risk, none has been conclusively identified as supe-ior to the others. Tight correlations between V20 andTDmean were reported in two studies of 99 patients who
eceived 3D-CRT for NSCLC (r � 0.942) (46) and 32atients who received CHART (r � 0.98) (47). A multivar-ate analysis of 90 patients who received conventional ra-iotherapy for NSCLC demonstrated a correlation betweenTDmean and Grade �1 radiation pneumonitis that re-ained statistically significant when cutoff values for V20,
30, and V40 were substituted for NTDmean (37). Collec-ively, these results suggest that either V20 or NTDmean cane used with similar reliability to predict radiation pneumo-itis risk. However, of these dosimetric variables, only V20
as associated with the risk of Grade �2 radiation pneu-onitis on multivariate analysis in one of those studies (46);
t was not significant in another of those studies (47), and itas not evaluated as an independent risk factor for Grade2 radiation pneumonitis in the third study (37). Further-ore, despite excellent correlations between dosimetric pa-
ameters among 43 patients who received 3D-CRT (medianose, 73.9 Gy) in another study, no correlation was foundetween the DVH parameters and changes in PFTs, leadinghe authors to conclude that additional efforts are needed to
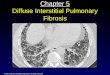
Fig. 3. Logistic regression analyses for V10, V20, V30, apatients with lung cancer who received 3D-CRT (52–70increases for V40 compared with the lower levels of expto a large region was safer than a large dose to a little reBaier K, Flentje M. A little to a lot or a lot to a little? Aparameters of the lung in patients with lung cancer tr
2003;179:548–556 (65).dentify DVH parameters that accurately predict risk of lungnjury and radiation pneumonitis (21). Indeed, a recent re-iew of published studies that evaluated DVH parameters forhe prediction of radiation pneumonitis reached similar con-lusions and noted that the ideal DVH metric for radiationneumonitis risk prediction has not yet been identified (64).
A lot to a little or a little to a lot”A controversial area of predicting radiation pneumonitis
s the determination of whether to give “a lot to a little or aittle to a lot” (25, 65). In one study, 18 of 49 patients (37%)xperienced Grade �2 radiation pneumonitis after receivingD-CRT to a total dose of up to 70 Gy in 2 Gy fractions, inombination with paclitaxel and carboplatin (65). The totalose and MLD were both correlated to the risk of pulmo-ary toxicity. Furthermore, logistic regression curves for
10, V20, V30, and V40 demonstrated sharper increases inisk of radiation pneumonitis for higher doses (Fig. 3).ased on these findings, the authors concluded that a littleose (e.g. 10 Gy) to a large volume of normal lung wasreferable to a large dose (e.g. 40 Gy) to a small volume oformal lung.However, a recent evaluation was performed for dosimet-
ic parameters and DLCO values in 26 patients with lungancer who were treated with 3D-CRT alone (2.15 Gy dailyractions) or with hyperfractionated 3D-CRT (1.2 Gy twiceaily) plus concurrent cisplatin (25). Significant changes inung function occurred with small changes in radiation dose.
of the ipsilateral and total lung, based on data from 492 Gy fractions) with paclitaxel and carboplatin. Sharper(V10–V30) led the authors to conclude that a little dosef normal lung tissue. Reprinted from Willner J, Jost A,lysis of pneumonitis risk from dose–volume histogramwith 3-D conformal radiotherapy. Strahlenther Onkol
nd V40
Gy inosuregion on ana
eated

Tracctibnlaapsms�vr
Cf
cdiamstatpcs
dl
B
maddfpsna(ap
tplptpwncfptdppmmttk
(rwGb
FiRJp(
14 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
he loss of DLCO was estimated to be 0% for areas thateceived �10 Gy, 72% for those that received 10–20 Gy,nd 90% for those that received �20 Gy. These findings areonsistent with previous results suggesting that V20 is aritical predictive factor for radiation pneumonitis. Addi-ional mathematical modeling revealed a sharp loss in DLCO
n normal lung exposed to as little as 13 Gy, which is wellelow the level previously considered the cutoff for pulmo-ary toxicity. They concluded from these findings that “aittle dose to a lot of lung could be much worse than a lot to
little.” Data from 63 patients treated with 3D-CRT atnother institution (51) demonstrated that complicationrobability curves rise steeply above MLD of 10 Gy, furtherupporting the need to limit widespread irradiation of nor-al lung tissue, even with this low dose. All of these data
uggest that “a little to lot” is safe only if it is limited to10 Gy. Clinically, the safest approach is to limit both the
olume of normal lung that is irradiated and the amount ofadiation that it receives.
ombining dosimetric, clinical, and location-relatedactors to predict risk
A recent analysis attempted to consolidate dosimetric,linical, and location-related risk factors into a single pre-ictive model for radiation pneumonitis (66). The studyncluded 200 patients with �6 months of follow-up datafter 3D-CRT for the definitive treatment of NSCLC. The 4ost significant risk factors on multivariate logistic-regres-
ion modeling were (in decreasing order of significance):he use of concurrent chemotherapy, the generalized equiv-lent uniform dose, V60, and tumor location at the base ofhe lung. Therefore, the ability to predict risk of radiationneumonitis seems to be strongest when several dosimetric,linical, and location-related factors are combined into aingle model rather than when a single factor is used to
ig. 4. The cytokine cascade of pulmonary toxicity–-cell-cellnteraction and control of gene expression by growth factors.eprinted with permission from Rubin P, Johnston CJ, Williams
P, et al. A perpetual cascade of cytokines postirradiation leads toulmonary fibrosis. Int J Radiat Oncol Biol Phys 1995;33:99–109
t67).
istinguish between patients with high risk and those withow risk.
iochemical detection markersPneumonitis usually does not appear until at least 2–3onths after radiotherapy, by which time the damage has
lready been done and cannot be reversed. Because ofifficulties in predicting which patients will experience ra-iation pneumonitis, biochemical markers have been soughtor the early detection of pulmonary damage. Although therecise target of radiation-induced pulmonary damage istill unknown, it has been proposed that radiation pneumo-itis and the ensuing pulmonary fibrosis may be the result ofcytokine cascade that is triggered by irradiation (Fig. 4)
67). Because these cytokines are thought to be key medi-tors of lung toxicity, many of them have been examined asotential early markers for radiation pneumonitis (Table 5).In one study, several cytokines were evaluated as poten-
ial markers for radiation pneumonitis based on data for 24atients who underwent thoracic radiotherapy, provided ateast 12 months of clinical follow-up, and provided seriallasma specimens before, during, and up to 12 weeks afterhoracic radiotherapy (68, 69). Six patients had Grade 1neumonitis, and 13 had Grade 2 pneumonitis. Comparedith the patients who did not experience radiation pneumo-itis, those patients who did have pneumonitis had signifi-antly higher levels of interleukin-1� and interleukin-6 be-ore, during, and after radiotherapy (p � 0.05). Levels of therofibrotic cytokines basic fibroblast growth factor andransforming growth factor (TGF)-�1 were not appreciablyifferent between the patients with and without radiationneumonitis. Nor were there significant differences betweenatients with and without pneumonitis with respect to che-okines and adhesion molecule markers—monocyte che-otactic protein–1, L-selectin, and E-selectin. Therefore,
he profibrotic cytokines and chemokines were not predic-ive of radiation pneumonitis, but the inflammatory cyto-ines were.Serum levels of soluble intercellular adhesion molecule
sICAM)-1 may also be useful for the early identification ofadiation pneumonitis. In one prospective study, 30 patientsere treated with hyperfractionated radiotherapy (1.5–1.6y twice daily), and blood samples for sICAM-1 were takenefore, midway, and after radiotherapy. Twelve (40%) pa-
Table 5. Potential early-detection markers forradiation pneumonitis
Markers
Interleukins IL-1� and IL-6 (68, 69)Soluble intracellular adhesion molecule (SICAM)-1 (70)Cytokeratin 19 fragment (CYFRA 21-1) (74)Serum mucin-like glycoprotein antigen KL-6 (72)Exhaled nitric oxide (75)Pulmonary surfactant protein D (71)Transforming growth factor (TGF)-�1 (77–79, 81, 82)
ients had radiation pneumonitis. Serum levels of sICAM-1

wnggtttsdtit
apwotdritmw(otp
ipcapfpfwmppvCwwdnCdf
poctaa
cwsti3rcm
mtptlg(mav
rprTntatdbanoibascepbppptabppTa
psa
15Radiation pneumonitis in NSCLC ● V. MEHTA
ere elevated significantly at baseline in both the pneumo-itis and nonpneumonitis groups. sICAM-1 levels rose pro-ressively during and after radiotherapy in the pneumonitisroup but not in the nonpneumonitis group, reaching statis-ical significance at the end of radiotherapy (70). Althoughhis serum marker was associated with pneumonitis, the facthat levels did not separate until the end of radiotherapyuggests that it has limited utility as a guide for treatmentecisions; it is too late to alter the radiotherapy by the timehis marker appears, and at this point, there is no provenntervention that can alter the course of the ensuing radia-ion pneumonitis.
Other potential markers for radiation pneumonitis havelso emerged in clinical studies. A prospective study ofatients with lung, breast, or esophageal cancer who under-ent thoracic radiotherapy determined that elevated levelsf serum pulmonary surfactant protein D has strong sensi-ivity (74%) and positive predictive value (68%) for theetection of radiation pneumonitis (71). When patients whoeceive conventional radiotherapy have at least a 1.5-foldncrease in serum mucin-like glycoprotein antigen (KL-6),hey are significantly more likely to have radiation pneu-onitis (72). Similar results have been obtained in patientsho receive a single high dose of stereotactic radiotherapy
73). Three of 16 patients treated with this strategy devel-ped radiation pneumonitis, and all 3 had increases in KL-6o a level of �500 IU, whereas none of the patients withoutneumonitis demonstrated this change in KL-6.Cytokeratin 19 is a subtype of a cytoskeletal structure that
s expressed in bronchial epithelial cells, among other sim-le epithelial cell types, so it was proposed that levels ofytokeratin 19 fragment (CYFRA 21–1) might be elevateds a marker for pulmonary damage in patients with radiationneumonitis (74). Blood samples from 16 smokers withocal Grade 1 pneumonitis (n � 10) or diffuse Grade 3–4neumonitis (n � 6) were compared with blood samplesrom 10 smokers without pneumonitis. CYFRA 21–1 levelsere significantly higher among patients with focal pneu-onitis than those without pneumonitis (1.74 vs. 1.0 ng/mL,� 0.02), and they were elevated much further among
atients with diffuse pneumonitis (30.9 ng/mL, p � 0.002s. other cohorts). Follow-up blood samples determined thatYFRA 21–1 levels increased further among patientshose pneumonitis worsened and decreased in a patientho improved with steroid therapy. Because of the largeifference between patients with focal and diffuse pneumo-itis in that analysis, it remains to be determined whetherYFRA 21–1 is a reliable marker for early pulmonaryamage that can be used to alter treatment plans and avoidurther damage to normal lung.
Exhaled levels of nitric oxide were evaluated in 29atients who received conventional radiotherapy (n � 8)r combined chemoradiotherapy (n � 21) for lung can-er, and were compared to levels from 11 healthy con-rols and 10 patients with asthma (75). Before radiother-py, exhaled nitric oxide levels were significantly higher
mong patients with lung cancer than among healthy pontrol subjects, but substantially lower than in patientsith asthma. Overall, conventional radiotherapy was as-
ociated with reductions in exhaled nitric oxide levels inhe patients with lung cancer. However, 5 patients had anncrease in exhaled nitric oxide to a level that was at least-fold greater than baseline, and 3 of these 5 patients hadadiation pneumonitis. The authors noted that thehanges appeared late in the treatment course, so earlierarkers for pulmonary damage were needed.The transmembrane endothelial cell protein thrombo-odulin is an endogenous anticoagulant that is released into
he circulation by inflammation. A prospective study of 17atients before, during, and after 3D-CRT determined thathrombomodulin levels decreased significantly from base-ine during the first week of 3D-CRT in the nonpneumonitisroup (n � 8), but not in the pneumonitis group (n � 9)76). Therefore, thrombomodulin might serve as an earlyarker for pulmonary damage at a time when the radiother-
py plan can still be adjusted, if desired, potentially pre-enting pulmonary damage.Several studies evaluated the utility of measuring se-
um levels of TGF-�1 as an early-detection marker. Ailot study in 27 patients who received conventionaladiotherapy for Stage III NSCLC determined that meanGF-�1 levels remained significantly elevated aboveormal in the 9 patients with radiation pneumonitis, buthey were unchanged or declined toward normal levelsmong the other patients (77). Another study of 73 pa-ients with lung cancer who were treated with 3D-CRTemonstrated that reduction of TGF-�1 levels belowaseline by the end of radiotherapy was more commonmong patients who did not develop radiation pneumo-itis (78). A decrease from baseline to a value at the endf 3D-CRT that was within normal limits had 90% pos-tive predictive value for identifying patients who woulde free of radiation pneumonitis. TGF-�1 levels werelso measured from bronchoalveolar lavage samples in atudy of 11 patients who received 3D-CRT for lungancer (79). Bronchoalveolar levels were significantlylevated in areas of the lung that were irradiated com-ared with nonirradiated areas, and greater increases inronchoalveolar TGF-�1 levels occurred at 1 month inatients with radiation pneumonitis than in those withoutneumonitis. A retrospective study of 104 lung canceratients, most of whom underwent 3D-CRT, determinedhat TGF-�1 levels independently predicted risk of radi-tion pneumonitis on multivariate analysis, and the com-ination of TGF-�1 with V30 further improved predictiveower (80). The incidence of symptomatic radiationneumonitis at 1 year was 14% among patients whoseGF-�1 levels decreased during radiotherapy and 26%mong patients whose TGF-�1 levels increased.
However, these results were not confirmed by a recentrospective study that evaluated plasma TGF-�1 levels,ymptoms of radiation pneumonitis, and CT scans (tossess both MLD and radiographic evidence of radiation
neumonitis) in 68 patients with NSCLC (81). Multivar-
ioMslroldtAwitdnlablls
CR
rssGCtt5torrtr1rpWswtdvmCgprb
pmptotrcm
fmrwpcbwne(dtCoacrnfitr
T
cretiwdj�twt(pmGit
16 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
ate analysis revealed that although persistent elevationsf TGF-�1 after 3D-CRT were associated with increasedLD, which in turn was correlated with radiographic and
ymptomatic evidence of radiation pneumonitis, TGF-�1evels themselves were not independent predictors foradiation pneumonitis. Another recent prospective studyf 46 patients with NSCLC also concluded that plasmaevels of TGF-�1 during the course of conventional ra-iotherapy had weak, if any, predictive power for radia-ion pneumonitis, particularly at later time points (82).lthough a reduction in TGF-�1 by Week 3 of treatmentas predictive of radiation pneumonitis, the confidence
ntervals were large, which led the authors to concludehe trend was not consistent enough to warrant safeecision-making in a clinical setting. A potential expla-ation for these contradictory findings is that TGF-�1evels are elevated locally at the site of radiation injury,s demonstrated by bronchoalveolar lavage studies (79),ut TGF-�1 does not pass through the vascular endothe-ium into the general circulation, so increases in plasmaevels are not commensurate with increases in lung tis-ue.
PREVENTING RADIATION PNEUMONITIS
ontinuous Hyperfractionated Acceleratedadiotherapy (CHART)Just as the choice of chemotherapy seems to influence
isk of radiation pneumonitis, the choice of radiotherapytrategy is likely to influence risk. Aggressive radiotherapytrategies such as CHART (54 Gy total in 36 fractions of 1.5y, given three times daily over 12 consecutive days),HARTWEL (60 Gy in 40 fractions of 1.5 Gy, given three
imes daily excluding weekends), or escalated hyperfrac-ionated accelerated radiotherapy (EHART; 66 Gy total in0 fractions over 5 weeks, 5 days/week, using escalatedwice-daily fractions of 1.2–1.5 Gy) may influence the riskf pulmonary toxicity compared with standard fractionatedadiotherapy (83, 84). In a post hoc analysis of data from aandomized comparison of CHART or conventional radio-herapy in 563 patients with NSCLC, the incidence ofadiation pneumonitis requiring treatment at 6 months was1.0% in the CHART arm and 9.2% in the conventionaladiotherapy arm (85). The predicted incidence of radiationneumonitis requiring treatment at 6 months with CHART-EL therapy was 12.8% (83). However, the incidences of
ymptomatic radiation pneumonitis in the CHART studyere 19% in the conventionally treated group and 10% in
he CHART group, and the frequency of radiographicallyetermined radiation pneumonitis was also higher with con-entional therapy (65% vs. 56%) (85). Significant improve-ent in local control and survival was also observed withHART vs. conventional radiotherapy. These findings sug-est that despite a small increase in the risk of radiationneumonitis requiring treatment, the risk of symptomatic oradiographic pneumonitis may be reduced, and the overall
enefit:risk ratio seems to favor CHART. rIn a nonrandomized, single-arm study of EHART, 8% ofatients developed acute radiation pneumonitis requiring treat-ent, and another 32% developed Grade 1–2 acute radiation
neumonitis (84). The lack of a standard fractionated radio-herapy group in the latter study precluded a direct comparisonf these incidences across different treatment strategies. Fur-hermore, the benefits of hyperfractionated radiotherapy withespect to locoregional tumor control (HR � 0.78, CHART vs.onventional radiotherapy) (83) may outweigh the risk ofoderate to severe radiation pneumonitis.The combination of induction chemotherapy with hyper-
ractionated radiotherapy may be particularly toxic to nor-al lung tissue. In a pilot study, 2 of 3 patients who
eceived the initial regimen of vinorelbine and carboplatinith CHART (54 Gy in 36 fractions over 12 days) died ofulmonary fibrosis, leading the authors to conclude that theombination had unacceptable lung toxicity (86). The com-ination of the same CHART regimen with concurrenteekly paclitaxel resulted in Grade �3 radiation pneumo-itis in 10 of 20 patients in another study (87). The accel-rated hyperfractionated treatment strategy in CHARTWELdiscontinuing CHART on weekends) may increase theose intensity to the tumor while still allowing normal lungissues the opportunity to repair. A comparative study ofHARTWEL plus chemotherapy vs. CHARTWEL alonebserved no cases of Grade �3 radiation pneumonitismong the 37 patients who received the chemoradiotherapyombination, and only 1 case among the 76 patients whoeceived CHARTWEL alone (88). Further studies areeeded to determine whether induction chemotherapy be-ore hyperfractionated radiotherapy provides sufficient clin-cal benefit to offset the potential increase in pulmonaryoxicity and to directly compare the tolerability of chemo-adiotherapy with CHARTWEL or CHART.
hree-dimensional conformal radiotherapy (3D-CRT)The evidence for reduced lung toxicity with 3D-CRT
ompared with conventional radiotherapy is equivocal. Oneecent Phase I/II trial reported that only 1 of 62 patientsxperienced Grade �2 radiation pneumonitis when all pa-ients received 3D-CRT combined with paclitaxel and plat-num treatment (89). In another recent study of 18 patientsho received high-dose 3D-CRT (92.4 or 102.9 Gy total inaily fractions of 2.1 Gy), of which only 1 received neoad-uvant chemotherapy, none of the patients developed Grade
2 radiation pneumonitis (90). Another recent dose-findingrial reported that of 50 patients who received chemotherapyith conventional radiotherapy, followed by boost irradia-
ion with 3D-CRT to a total radiotherapy dose of 60–78 Gymedian, 75 Gy), only 1 patient had Grade 3 radiationneumonitis (91). The incidence of Grade 2 radiation pneu-onitis was not reported separately, but 36% of patients hadrade 1–2 toxicity, so it is not possible to compare the
ncidence of Grade �2 radiation pneumonitis in that studyo the rates reported in other studies of 3D-CRT. In fact, the
ates of Grade �2 radiation pneumonitis after 3D-CRT
w3
swtsnorpNchwrr
rllrGwsupwweaca
I
is1
tet3fssttlmttot
tgatS(utbttd
B
dspw(fw
GSHHB
RWWCN
follow
17Radiation pneumonitis in NSCLC ● V. MEHTA
ere as high as 37% in other clinical studies (Table 6) (20,5, 37, 46, 65, 90, 92–94).The general trend toward lower rates in more recent
tudies suggests that 3D-CRT technique may be improvingith additional clinical research and experience. Alterna-
ively, it may simply reflect a trend to smaller daily fractionize, smaller treatment field sizes, or closer attention toormal lung dose. Or perhaps, this trend might be the resultf increased use of preventive measures (See “Preventingadiation pneumonitis: Radioprotection,” below). For exam-le, one group reported that when it treated 54 patients withSCLC by splitting each target tumor into a cranial and
audal segment, treating these segments separately withigh-dose 3D-CRT (�80 Gy total) and providing patientsith prednisone prophylaxis, only 1 patient had Grade �3
adiation pneumonitis, and this patient inadvertently had noteceived the prednisone regimen (95).
Other potential contributors to variations in the reportedates of radiation pneumonitis in studies of 3D-CRT forung cancer include differences between the patient popu-ations studied or the methods that were used to diagnoseadiation pneumonitis. For example, the highest rate ofrade �2 radiation pneumonitis among these studies (37%)as reported by a prospective study that specifically as-
essed radiation pneumonitis using CT scans, clinical eval-ation, and PFTs before and 6 weeks after 3D-CRT in 54atients with NSCLC (20). In another study of 19 patientsho received 3D-CRT for NSCLC, 7 patients had a CT scanithin 3 months, and all of these patients had radiographic
vidence of radiation pneumonitis in the small area directlyround the tumor (94), although the authors noted that thesehanges were less extensive than those expected to occurfter conventional radiotherapy.
ntensity-modulated radiotherapy (IMRT)Compared with conventional radiotherapy, the use of
ntensity-modulated radiotherapy (IMRT) reduces the expo-ure of normal lung tissue to irradiation by approximately
Table 6. Incidence of radiation pneumonitis in
Study No.Once-dailyfractions
raham et al., 1999 (46) 99 2.0 Gyunyach et al., 2000 (20) 54 2.0 Gyayman et al., 2001 (92) 104 2.1 Gyernando et al., 2001 (35) 201 2.0 Gyhatnagar et al., 2002 (93) 46 1.8 Gy
osenman et al., 2002 (89) 62 2.0 Gyillner et al., 2003 (65) 49 2.0 Gyu et al., 2003 (91) 50 †
laude et al., 2004 (37) 90 2.0 Gyarayan et al., 2004 (90) 18 2.1 Gy
* Data presented as Grade 3/Grade 1–2.† Conventional radiotherapy (42 Gy in 21 daily fractions) was
0% to 20% at the same time that it increases the dose to the a
arget lung tumor (96–98). This emerging technique wasvaluated in a prospective, nonrandomized trial of 41 pa-ients with recurrent NSCLC who had previously undergoneD-CRT (99). Use of IMRT (63 Gy total in 35 dailyractions of 1.8 Gy) in these patients was associated withignificantly greater target conformity and 10% less expo-ure of normal lung tissue to irradiation. The authors usedhe DVH techniques described previously to determine thathe estimated risk of radiation pneumonitis was significantlyower with IMRT than 3D-CRT (9% vs. 36% using oneodel and 7% vs. 13% using another). Prospective, con-
rolled, long-term outcomes studies are needed to confirmhis preliminary evidence that IMRT might reduce the riskf radiation pneumonitis compared with conventional radio-herapy or 3D-CRT.
One evolving form of IMRT, known as helical tomo-herapy, uses technology similar to a spiral CT scan. Theantry is rotated 360° around the patient, who is movedxially (100). Treatment plans for 3D-CRT and helicalomotherapy were compared for 5 sample patients withtage III NSCLC in a simulated dose-escalation experiment101). The effective uniform dose of the gross tumor vol-me was comparable for the two treatment strategies, buthe tomotherapy approach was estimated to reduce the V20
y 22% and the NTDmean by 30%. Although limited accesso these machines and the lack of clinical evidence reducehe clinical implications at present, it is possible that theseevices may be used increasingly in the future.
oost radiotherapyConcomitant boost radiotherapy, which combines low
oses of radiotherapy to large regions and higher doses inmaller fields encompassing the gross tumor, was shown torovide superior response to conventional radiotherapyithout increasing Grade �3 lung toxicity in one study
102). When cisplatin/etoposide was combined with hyper-ractionated accelerated radiotherapy (1.5 Gy b.i.d. for 3eeks) and a small-volume boost of 20 Gy to the tumor in
ed clinical studies of 3D-CRT for lung cancer
otal dose,Gy
Chemotherapyuse
Grade �2 radiationpneumonitis
60–74 42% 14%66 24% 37%
63–102.9 24% 6.7%26–86.4 60% 17%30–68.4 67% Acute: 2%/9%*
Late: 0%/15%*60–74 100% 1.6%52–70 98% 37%69–78 100% 2%/36%*46–72 25% 7.8%.4 or 102.9 6% 0%
ed by 3D-CRT boost of 27–36 Gy in daily 3-Gy fractions.
select
T
92
nother study of patients with locally advanced NSCLC,

o(rfc
S
tltwGpwrmoprt
P
ettttwpateI2ra6rpwrlAsoa(
C
icrfo
�Glsu�iwftTtFamuo
R
taepeomcimccwpp
hnisesawa
ncrtholdcm
18 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
nly 1 case of Grade �3 radiation pneumonitis was reported103). Similarly low rates of radiation pneumonitis wereeported in a study of conventional radiotherapy to 42 Gyollowed by 3D-CRT boost therapy to 69–78 Gy with aombination regimen of chemotherapy (91).
ingle-dose stereotactic radiotherapyPreliminary evidence suggests that single-dose stereotac-
ic radiotherapy may also be effective for the treatment ofung cancer, yet have a low risk of pulmonary toxicity. Thisreatment modality was used successfully in 18 patientsith Stage I NSCLC who were given a single dose of 19–26y (104). No patient had symptoms of Grade �2 radiationneumonitis, but the authors noted that lung function testsere not performed regularly during follow-up. In a sepa-
ate study of 28 patients with primary lung cancer or lungetastases who were treated with high-dose (30–40 Gy
ver 3–4 fractions) stereotactic 3D-CRT, only 1 patient hadrogressive disease (105). All patients developed Grade 1adiation pneumonitis within 3 months, but none had symp-omatic or serious late complications.
roton radiotherapyBecause the highest radiation dose is delivered upon
ntry into the body with conventional radiotherapy, anotherreatment alternative to improve delivery of irradiation toumors involves the use of particle-beam therapy with pro-ons, which are subject to less dispersion before reaching thearget (106). A prospective Phase I/II study of 24 patientsith medically inoperable NSCLC evaluated the use ofroton irradiation alone in 10 patients (51 cobalt Gy equiv-lent total, in 10 fractions), and photon irradiation (45 Gyotal, in 25 fractions) plus proton boost (28.8 cobalt Gyquivalent total, given daily during the last 3 weeks) (107).n the latter cohort (photon radiotherapy with proton boost),
patients developed symptomatic radiation pneumonitisequiring treatment, and scheduled evaluations of dyspneand pulmonary function revealed significant worsening after
to 12 months. In contrast, none of the patients whoeceived only proton irradiation had symptomatic radiationneumonitis, and pulmonary function and dyspnea were notorsened over time. Another study of 14 patients who
eceived proton irradiation for NSCLC reported a similarack of pulmonary toxicity with long-term follow-up (108).
larger study of 51 patients with NSCLC reported that theeverity of acute radiation pneumonitis was Grade 2 in 6%f patients and Grade 3 in 2% after proton irradiation withmedian total dose of 76 Gy and a median fraction of 3 Gy
109).
arbon-ion radiotherapyA heavy ion medical accelerator was constructed in Japan
n 1993, and 81 patients with NSCLC were treated witharbon-ion irradiation using this device (110). Total dosesanged from 59.4 to 95.4 Gy equivalents, given in 18ractions over 6 weeks or with a more dose-intense schedule
f 9 fractions over 3 weeks. Eight (10%) patients had Grade m2 radiation pneumonitis, including 3 (4%) patients withrade 3 severity. Grade 2 radiation pneumonitis was dose-
imiting at 79.2 Gy equivalents for the more dose-intensechedule and 95.4 Gy equivalents for the less intense sched-le. Multivariate analysis determined that the risk of Grade2 radiation pneumonitis was reduced by respiratory-gated
rradiation and increased by the use of irradiation portalsith opposing fields. In a separate analysis of the 52 patients
rom this population who completed pulmonary functionests at 6 and 12 months after irradiation (111), FEV1 andLC decreased by �7% from baseline at each follow-up
est, but other pulmonary function tests (such as DLCO andVC) were not significantly different from baseline valuesfter 6 and 12 months. Although carbon-ion radiotherapyay have low risk of severe pulmonary toxicity despite the
se of high doses of irradiation, the technology is availablenly to a limited number of patients.
adiotherapy selection: Clinical considerationsThe available clinical evidence suggests that many fac-
ors may influence the risk of radiation pneumonitis, but thevailable methods for predicting which patient will experi-nce radiation pneumonitis are far from perfect. Identifyingatients at low risk of radiation pneumonitis may permitscalation of radiotherapy to improve response, but thepposite is not true. Patients at high risk of radiation pneu-onitis are unlikely to have their radiotherapy dose de-
reased simply to prevent pulmonary toxicity. Adequaterradiation of the tumor is essential to the success of treat-ent. It has been shown that interrupting radiotherapy be-
ause of toxicity significantly reduces overall survival, lo-oregional control, and metastasis-free survival in patientsith NSCLC (112). Therefore, reducing radiotherapy torevent radiation pneumonitis may not be an option in mostatients.Furthermore, reducing radiation doses in patients at
igher risk does not necessarily prevent radiation pneumo-itis. A dose-escalation study of 3D-CRT in patients withnoperable NSCLC reported that 15% of patients who werecheduled to receive a cumulative dose of 70.2 Gy experi-nced severe or fatal radiation pneumonitis (113). Althoughubsequent patients were given a reduced dose of radiother-py if they had an NTCP of 25% or greater, 2 of 4 patientsho received a reduced dose still experienced severe radi-
tion pneumonitis.The use of 3D-CRT or IMRT may limit the irradiation of
ormal lung tissue while maintaining similar or improvedoverage of the tumor, but it requires precise targeting of theadiation beams. Patients may be immobilized by placinghem in a specially designed cradle, but unlike patients withead-and-neck cancer or prostate cancer, the thoracic regionf patients with lung cancer cannot be completely immobi-ized, because of respiration. To address this problem, theeep-inspiration breath-hold technique may be used to in-rease the dose of radiotherapy that is administered safely toedium-to-large NSCLC tumors (114). The use of confor-
al radiotherapy in conjunction with the deep-inspiration
bmd
R
iadgitmrwsrsttfw
powibbdpamtird
nAmisdadwt
ppfiRopp(imrwowtacptinctfiw
A
A
W
K
19Radiation pneumonitis in NSCLC ● V. MEHTA
reath-hold technique has been shown to decrease the treat-ent margins that are required, thereby increasing the total
ose of radiotherapy that can be given safely (115).
adioprotectionAn emerging alternative to prevent radiation pneumonitis
s to allow the normal lung tissue to be irradiated but to alsodminister medications with cytoprotective activity to re-uce the severity of radiation damage. A case report sug-ested that the use of broad-spectrum prophylaxis withmmunomodulating therapy such as corticosteroids or aza-hioprine does not seem to protect against radiation pneu-onitis (116). However, one of the trials described above
eported no cases of Grade �3 radiation when prednisoneas given before high-dose radiotherapy; 1 case was ob-
erved, but it occurred in a patient who inadvertently did noteceive the corticosteroid therapy (95). Because of theafety issues inherent in the long-term use of broad-spec-rum immunomodulating therapy for prophylaxis, agentshat are well tolerated and that selectively protect lung tissuerom radiation-induced pulmonary damage would beelcome.Amifostine is an aminothiol with broad-spectrum cyto-
rotection that may reduce the incidence of acute toxicitiesf thoracic radiotherapy, including radiation pneumonitis,ithout protecting tumors (Table 7) (117–120). Initial stud-
es demonstrated that adjusting amifostine doses on theasis of body surface area and administering them dailyefore radiotherapy or chemoradiotherapy significantly re-uced the incidence of severe radiation pneumonitis com-ared to no cytoprotective therapy (117, 118). Later studieschieved similar results using a flat dose of amifostine 500g administered i.v. 2–4 times weekly between hyperfrac-
ionated, twice-daily doses of radiotherapy (119). However,n a large randomized Phase III study of patients whoeceived chemotherapy in addition to hyperfractionated ra-iotherapy, administration of amifostine 4 times weekly did
Table 7. Incidence of radiation pneumonitis in randomizedchemoradiothe
Reference No. Radiation dose Chemothe
ntonadou et al.,2001 (117)
146 55–60 Gy at2.0 Gy q.d.
None
ntonadou et al.,2003 (118)
73 55–60 Gy at2.0 Gy q.d.
Concurrent wor C
erner-Wasik et al.,2003 (120)
242 69.6 Gy at1.2 Gy b.i.d.
Induction P �concurrent
omaki et al., 2004(119)
62 69.6 Gy at1.2 Gy b.i.d.
Concurrent CDays 1, 8,
Oral etoposidDays 1–5, 829–33, 36–
Abbreviations: P � paclitaxel; C � platinum (carboplatin or ci
* Severity of pneumonitis based on National Cancer Institute Commoot reduce the incidence of radiation pneumonitis (120).mifostine administered with radiotherapy may protect nor-al lung parenchyma and prevent the decline in DLCO seen
n patients treated with radiotherapy (21). In that study,ignificant decreases in DLCO were observed when the lungose exceeded 13 Gy in patients treated with radiotherapylone. When compared to patients who received amifostineuring the radiotherapy course, patients without amifostineere not observed to have the same degree of DLCO reduc-
ion until the lung dose exceeded 36 Gy.The ACE inhibitor captopril contains a thiol and has been
roposed as a potential cytoprotective agent for radiationneumonitis. Captopril protected against pneumonitis andbrosis in rats (121), and it is being evaluated by theadiation Therapy Oncology Group in humans; the resultsf the Radiation Therapy Oncology Group study are stillending. However, a retrospective analysis of lung canceratients who received ACE inhibitors during radiotherapyusually for hypertension management) concluded that ACEnhibitor therapy did not reduce the risk of radiation pneu-onitis significantly (122). Of the 213 eligible patients
eceiving 3D-CRT for lung cancer with curative intent, 26ere receiving ACE inhibitors (usually for the managementf hypertension) during 3D-CRT, and the remaining 187ere not, but there were no significant differences between
he treatment groups for any demographic or clinical char-cteristics at baseline. ACE inhibitor therapy did not de-rease, and instead tended to increase, the risk of radiationneumonitis (15% vs. 12%), and radiation pneumonitisended to occur earlier in the patients who received ACEnhibitors. It has been suggested that the sulfhydryl compo-ent that is present in captopril may be responsible forytoprotection, but animal studies concluded that the angio-ensin II receptor was also a key contributor to radiationbrosis, based on preliminary evidence of cytoprotectionith an angiotensin II type 1 receptor blocker (123).Several other treatments may prove to be effective for
f amifostine treatment in patients receiving radiotherapy orr lung cancer
Amifostine dose Effect on pneumonitis*
340 mg/m2 q.d. 15 min.before radiotherapy
2 Grade 2� from 43% to9% 2 months afterradiotherapy
300 mg/m2 q.d. beforeradiotherapy orchemoradiotherapy
2 Grade 3� from 56% to19% duringchemoradiotherapy
2;C
500 mg i.v. 4�/wkbetween b.i.d.fractions
No change
500 mg i.v. 1st, 2ndday each week beforechemo and 1stradiotherapy fraction
2 Grade 3� from 16% to0% duringchemoradiotherapy
).
trials orapy fo
rapy
eekly P
C �weekly
on29, 36e
–12,40
splatin
n Toxicity Criteria.
raflrcm(p
tcd2smtntcpdHmt
huprp
qardnpfabtrar
utrctbctfdtsmpertt
20 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
adioprotection in patients who receive thoracic radiother-py. In a preliminary placebo-controlled study of pentoxi-ylline in patients with lung or breast cancer, significantlyower toxicity scores and greater diffusing capacity andegional perfusion were observed in the patients who re-eived pentoxifylline (124). Animal and human studies withelatonin suggested that it has radioprotective activity
125), but controlled studies of melatonin are needed inatients who receive thoracic radiotherapy for lung cancer.Animal studies have identified other potential radiopro-
ective agents that have not been evaluated in controlledlinical trials. Injection of the antihypertensive agent carve-ilol several days before and after a single radiation dose of0 Gy in rats significantly reduced the inflammatory re-ponse to irradiation (126). Intratracheal gene therapy withanganese superoxide dismutase-plasmid/liposome pro-
ected normal lung tissue in mice from irradiation, but didot protect Lewis lung carcinoma tumors, suggesting selec-ive radioprotection (127). As the biochemical factors thatontribute to radiation pneumonitis are elucidated, futurereventive treatments may target the cytokine cascade toirectly inhibit the development of radiation pneumonitis.owever, because many of these biochemical factors haveyriad responsibilities, it may be difficult to inhibit radia-
ion pneumonitis without considerable side effects.
CONCLUSIONS
Although the existence and risk of radiation pneumonitisave been recognized for many years, there are still manynanswered questions about the incidence, consequences,rediction, and prevention of this common toxicity of tho-acic radiotherapy for NSCLC. Symptomatic radiation
neumonitis is associated with clinically significant se- iREFEREN
6. Magana E, Crowell RE. Radiation pneumonitis successfully
uelae, and it may occur at much lower doses of radiother-py than previously suspected, particularly as patientseceive increasingly aggressive radiotherapy and chemora-iotherapy regimens. Newer conformal radiotherapy tech-iques may reduce, but not eliminate, the risk of radiationneumonitis. Several studies have evaluated clinical riskactors for radiation pneumonitis, but these studies have notrrived at a clear consensus. The major risk factor seems toe the radiation dose that is administered to normal lungissue surrounding tumors. The use of dosimetric data de-ived from DVH and reduction algorithms may providedditional information regarding risk, but no ideal dosimet-ic parameter has been identified.
Serum levels of several biochemical markers may besed to identify radiation pneumonitis in early stages, buthese markers are of questionable benefit if they do notesult in radiotherapy dose reduction. Patients with lo-ally advanced NSCLC are unlikely to interrupt radio-herapy that has a potential risk of radiation pneumonitis,ecause doing so would probably worsen treatment suc-ess and outcomes. Controlled trials indicate that selec-ive radioprotection with the cytoprotective agent ami-ostine may enable patients to receive their scheduledoses of radiotherapy with reduced risk of pulmonaryoxicity. Preliminary clinical and preclinical evidenceuggests that ACE inhibitors, carvedilol, pentoxifylline,elatonin, or gene therapy may also reduce radiation
neumonitis. Further studies are needed to confirm thefficacy and safety of these agents for prevention ofadiation pneumonitis and to evaluate how radioprotec-ive therapy influences outcomes, including tumor con-rol, survival, quality of life, and activities of daily living
n patients with NSCLC.CES
1. Pfister DG, Johnson DH, Azzoli CG, et al. American Societyof Clinical Oncology treatment of unresectable non–small-cell lung cancer guideline: Update 2003. J Clin Oncol 2004;22:330–353.
2. Clinical practice guidelines for the treatment of unresectablenon–small-cell lung cancer. Adopted on May 16, 1997 by theAmerican Society of Clinical Oncology. J Clin Oncol 1997;15:2996–3018.
3. Roach M 3rd, Gandara DR, Yuo HS, et al. Radiation pneu-monitis following combined modality therapy for lung can-cer: Analysis of prognostic factors. J Clin Oncol 1995;13:2606–2612.
4. Senzer N. A phase III randomized evaluation of amifostine instage IIIA/IIIB non-small cell lung cancer patients receivingconcurrent carboplatin, paclitaxel, and radiation therapy fol-lowed by gemcitabine and cisplatin intensification: Prelimi-nary findings. Semin Oncol 2002;29:38–41.
5. Leong SS, Tan EH, Fong KW, et al. Randomized double-blind trial of combined modality treatment with or withoutamifostine in unresectable stage III non–small-cell lung can-cer. J Clin Oncol 2003;21:1767–1774.
treated with inhaled corticosteroids. South Med J2003;96:521–524.
7. Inoue A, Kunitoh H, Sekine I, et al. Radiation pneumonitis inlung cancer patients: A retrospective study of risk factors andthe long-term prognosis. Int J Radiat Oncol Biol Phys 2001;49:649–655.
8. Wang JY, Chen KY, Wang JT, et al. Outcome and prognos-tic factors for patients with non–small-cell lung cancer andsevere radiation pneumonitis. Int J Radiat Oncol Biol Phys2002;54:735–741.
9. Ohe Y. Treatment-related death from chemotherapy and tho-racic radiotherapy for advanced cancer. Panminerva Med2002;44:205–212.
10. Movsas B, Raffin TA, Epstein AH, et al. Pulmonary radia-tion injury. Chest 1997;111:1061–1076.
11. Abid SH, Malhotra V, Perry MC. Radiation-induced andchemotherapy-induced pulmonary injury. Curr Opin Oncol2001;13:242–248.
12. Abratt RP, Morgan GW. Lung toxicity following chest irra-diation in patients with lung cancer. Lung Cancer 2002;35:103–109.
13. Werner-Wasik M, Yu X, Marks LB, et al. Normal-tissue
toxicities of thoracic radiation therapy: Esophagus, lung, and
21Radiation pneumonitis in NSCLC ● V. MEHTA
spinal cord as organs at risk. Hematol Oncol Clin North Am2004;18:131–160, x–xi.
14. Fan M, Marks LB, Lind P, et al. Relating radiation-inducedregional lung injury to changes in pulmonary function tests.Int J Radiat Oncol Biol Phys 2001;51:311–317.
15. Rubenstein JH, Richter MP, Moldofsky PJ, et al. Prospectiveprediction of post-radiation therapy lung function usingquantitative lung scans and pulmonary function testing. Int JRadiat Oncol Biol Phys 1988;15:83–87.
16. Choi NC, Kanarek DJ, Grillo HC. Effect of postoperativeradiotherapy on changes in pulmonary function in patientswith stage II and IIIA lung carcinoma. Int J Radiat OncolBiol Phys 1990;18:95–99.
17. Choi NC, Kanarek DJ. Toxicity of thoracic radiotherapy onpulmonary function in lung cancer. Lung Cancer 1994;10:S219–S230.
18. Abratt RP, Willcox PA. The effect of irradiation on lungfunction and perfusion in patients with lung cancer. Int JRadiat Oncol Biol Phys 1995;31:915–919.
19. Robert F, Childs HA, Spencer SA, et al. Phase I/IIa study ofconcurrent paclitaxel and cisplatin with radiation therapy inlocally advanced non–small cell lung cancer: Analysis ofearly and late pulmonary morbidity. Semin Radiat Oncol1999;9:136–147.
20. Sunyach MP, Falchero L, Pommier P, et al. Prospectiveevaluation of early lung toxicity following three-dimensionalconformal radiation therapy in non–small-cell lung cancer:Preliminary results. Int J Radiat Oncol Biol Phys 2000;48:459–463.
21. Allen AM, Henning GT, Ten Haken RK, et al. Do dose-volume metrics predict pulmonary function changes in lungirradiation? Int J Radiat Oncol Biol Phys 2003;55:921–929.
22. De Jaeger K, Seppenwoolde Y, Boersma LJ, et al. Pulmo-nary function following high-dose radiotherapy of non–small-cell lung cancer. Int J Radiat Oncol Biol Phys 2003;55:1331–1340.
23. Gopal R, Starkschall G, Tucker SL, et al. Effects of radio-therapy and chemotherapy on lung function in patients withnon–small-cell lung cancer. Int J Radiat Oncol Biol Phys2003;56:114–120.
24. Miller KL, Zhou SM, Barrier RC, Jr., et al. Long-termchanges in pulmonary function tests after definitive radio-therapy for lung cancer. Int J Radiat Oncol Biol Phys 2003;56:611–615.
25. Gopal R, Tucker SL, Komaki R, et al. The relationshipbetween local dose and loss of function for irradiated lung.Int J Radiat Oncol Biol Phys 2003;56:106–113.
26. Brooks BJ Jr., Seifter EJ, Walsh TE, et al. Pulmonary tox-icity with combined modality therapy for limited stage small-cell lung cancer. J Clin Oncol 1986;4:200–209.
27. Schaake-Koning C, van den Bogaert W, Dalesio O, et al.Effects of concomitant cisplatin and radiotherapy on inoper-able non–small-cell lung cancer. N Engl J Med 1992;326:524–530.
28. Jeremic B, Shibamoto Y, Acimovic L, et al. Hyperfraction-ated radiation therapy with or without concurrent low-dosedaily carboplatin/etoposide for stage III non–small-cell lungcancer: A randomized study. J Clin Oncol 1996;14:1065–1070.
29. Lee JS, Scott C, Komaki R, et al. Concurrent chemoradiationtherapy with oral etoposide and cisplatin for locally advancedinoperable non–small-cell lung cancer: Radiation TherapyOncology Group protocol 91–06. J Clin Oncol 1996;14:1055–1064.
30. Byhardt RW, Scott C, Sause WT, et al. Response, toxicity,failure patterns, and survival in five Radiation Therapy On-cology Group (RTOG) trials of sequential and/or concurrent
chemotherapy and radiotherapy for locally advanced non–small-cell carcinoma of the lung. Int J Radiat Oncol BiolPhys 1998;42:469–478.
31. Monson JM, Stark P, Reilly JJ, et al. Clinical radiationpneumonitis and radiographic changes after thoracic radia-tion therapy for lung carcinoma. Cancer 1998;82:842–850.
32. Yamada M, Kudoh S, Hirata K, et al. Risk factors of pneu-monitis following chemoradiotherapy for lung cancer. Eur JCancer 1998;34:71–75.
33. Quon H, Shepherd FA, Payne DG, et al. The influence of ageon the delivery, tolerance, and efficacy of thoracic irradiationin the combined modality treatment of limited stage smallcell lung cancer. Int J Radiat Oncol Biol Phys 1999;43:39–45.
34. Robnett TJ, Machtay M, Vines EF, et al. Factors predictingsevere radiation pneumonitis in patients receiving definitivechemoradiation for lung cancer. Int J Radiat Oncol Biol Phys2000;48:89–94.
35. Hernando ML, Marks LB, Bentel GC, et al. Radiation-induced pulmonary toxicity: A dose-volume histogram anal-ysis in 201 patients with lung cancer. Int J Radiat Oncol BiolPhys 2001;51:650–659.
36. Rancati T, Ceresoli GL, Gagliardi G, et al. Factors predictingradiation pneumonitis in lung cancer patients: A retrospec-tive study. Radiother Oncol 2003;67:275–283.
37. Claude L, Perol D, Ginestet C, et al. A prospective study onradiation pneumonitis following conformal radiation therapyin non–small-cell lung cancer: Clinical and dosimetric fac-tors analysis. Radiother Oncol 2004;71:175–181.
38. Schild SE, Stella PJ, Geyer SM, et al. The outcome ofcombined-modality therapy for stage III non–small-cell lungcancer in the elderly. J Clin Oncol 2003;21:3201–3206.
39. Johansson S, Bjermer L, Franzen L, et al. Effects of ongoingsmoking on the development of radiation-induced pneumo-nitis in breast cancer and oesophagus cancer patients. Ra-diother Oncol 1998;49:41–47.
40. van Putten JW, Price A, van der Leest AH, et al. A Phase Istudy of gemcitabine with concurrent radiotherapy in stageIII, locally advanced non–small cell lung cancer. Clin CancerRes 2003;9:2472–2477.
41. Blackstock AW, Lesser GJ, Fletcher-Steede J, et al. Phase Istudy of twice-weekly gemcitabine and concurrent thoracicradiation for patients with locally advanced non–small-celllung cancer. Int J Radiat Oncol Biol Phys 2001;51:1281–1289.
42. Onishi H, Kuriyama K, Yamaguchi M, et al. Concurrenttwo-dimensional radiotherapy and weekly docetaxel in thetreatment of stage III non–small cell lung cancer: A goodlocal response but no good survival due to radiation pneu-monitis. Lung Cancer 2003;40:79–84.
43. Dincbas FO, Atalar B, Koca S. Two-dimensional radiother-apy and docetaxel in treatment of stage III non–small celllung carcinoma: No good survival due to radiation pneumo-nitis. Lung Cancer 2004;43:241–242.
44. Seppenwoolde Y, De Jaeger K, Lebesque JV. In regard toTsujino, et al. Predictive value of dose-volume histogramparameters for predicting radiation pneumonitis after concur-rent chemoradiation for lung cancer. (IJROBP 2003;55:110–115). Int J Radiat Oncol Biol Phys 2003;56:1208–1209;author reply 1209.
45. Armstrong JG, Zelefsky MJ, Leibel SA, et al. Strategy fordose escalation using 3-dimensional conformal radiationtherapy for lung cancer. Ann Oncol 1995;6:693–697.
46. Graham MV, Purdy JA, Emami B, et al. Clinical dose-volume histogram analysis for pneumonitis after 3D treat-ment for non–small cell lung cancer (NSCLC). Int J RadiatOncol Biol Phys 1999;45:323–329.
47. Jenkins P, D’Amico K, Benstead K, et al. Radiation pneu-
monitis following treatment of non–small-cell lung cancer
22 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
with continuous hyperfractionated accelerated radiotherapy(CHART). Int J Radiat Oncol Biol Phys 2003;56:360–366.
48. Tsujino K, Hirota S, Endo M, et al. Predictive value ofdose-volume histogram parameters for predicting radiationpneumonitis after concurrent chemoradiation for lung cancer.Int J Radiat Oncol Biol Phys 2003;55:110–115.
49. Kwa SL, Lebesque JV, Theuws JC, et al. Radiation pneu-monitis as a function of mean lung dose: An analysis ofpooled data of 540 patients. Int J Radiat Oncol Biol Phys1998;42:1–9.
50. Oetzel D, Schraube P, Hensley F, et al. Estimation of pneu-monitis risk in three-dimensional treatment planning usingdose-volume histogram analysis. Int J Radiat Oncol BiolPhys 1995;33:455–460.
51. Yorke ED, Jackson A, Rosenzweig KE, et al. Dose-volumefactors contributing to the incidence of radiation pneumonitisin non–small-cell lung cancer patients treated with three-dimensional conformal radiation therapy. Int J Radiat OncolBiol Phys 2002;54:329–339.
52. Lyman JT, Wolbarst AB. Optimization of radiation therapy,III: A method of assessing complication probabilities fromdose-volume histograms. Int J Radiat Oncol Biol Phys 1987;13:103–109.
53. Kutcher GJ, Burman C. Calculation of complication proba-bility factors for non-uniform normal tissue irradiation: Theeffective volume method. Int J Radiat Oncol Biol Phys1989;16:1623–1630.
54. Martel MK, Ten Haken RK, Hazuka MB, et al. Dose-volumehistogram and 3-D treatment planning evaluation of patientswith pneumonitis. Int J Radiat Oncol Biol Phys 1994;28:575–581.
55. Lee SW, Choi EK, Lee JS, et al. Phase II study of three-dimensional conformal radiotherapy and concurrent mitomy-cin-C, vinblastine, and cisplatin chemotherapy for Stage IIIlocally advanced, unresectable, non–small-cell lung cancer.Int J Radiat Oncol Biol Phys 2003;56:996–1004.
56. Burman C, Kutcher GJ, Emami B, et al. Fitting of normaltissue tolerance data to an analytic function. Int J RadiatOncol Biol Phys 1991;21:123–135.
57. Marks LB, Munley MT, Bentel GC, et al. Physical andbiological predictors of changes in whole-lung function fol-lowing thoracic irradiation. Int J Radiat Oncol Biol Phys1997;39:563–570.
58. Niemierko A, Goitein M. Modeling of normal tissue re-sponse to radiation: The critical volume model. Int J RadiatOncol Biol Phys 1993;25:135–145.
59. Yorke ED, Kutcher GJ, Jackson A, et al. Probability ofradiation-induced complications in normal tissues with par-allel architecture under conditions of uniform whole or par-tial organ irradiation. Radiother Oncol 1993;26:226–237.
60. Seppenwoolde Y, Engelsman M, De Jaeger K, et al. Opti-mizing radiation treatment plans for lung cancer using lungperfusion information. Radiother Oncol 2002;63:165–177.
61. Seppenwoolde Y, Lebesque JV, de Jaeger K, et al. Compar-ing different NTCP models that predict the incidence ofradiation pneumonitis. Normal tissue complication probabil-ity. Int J Radiat Oncol Biol Phys 2003;55:724–735.
62. De Jaeger K, Hoogeman MS, Engelsman M, et al. Incorpo-rating an improved dose-calculation algorithm in conformalradiotherapy of lung cancer: Re-evaluation of dose in normallung tissue. Radiother Oncol 2003;69:1–10.
63. Kwa SL, Theuws JC, Wagenaar A, et al. Evaluation of twodose-volume histogram reduction models for the predictionof radiation pneumonitis. Radiother Oncol 1998;48:61–69.
64. Rodrigues G, Lock M, D’Souza D, et al. Prediction ofradiation pneumonitis by dose-volume histogram parametersin lung cancer—a systematic review. Radiother Oncol 2004;
71:127–138.65. Willner J, Jost A, Baier K, et al. A little to a lot or a lot to alittle? An analysis of pneumonitis risk from dose-volumehistogram parameters of the lung in patients with lung cancertreated with 3-D conformal radiotherapy. Strahlenther Onkol2003;179:548–556.
66. Hope AJ, El Naqa I, Bradley JD, et al. Radiation pneumo-nitis/fibrosis risk based on dosimetric, clinical, and location-related factors [Abstract]. Int J Radiat Oncol Biol Phys2004;60:S204.
67. Rubin P, Johnston CJ, Williams JP, et al. A perpetual cas-cade of cytokines postirradiation leads to pulmonary fibrosis.Int J Radiat Oncol Biol Phys 1995;33:99–109.
68. Chen Y, Williams J, Ding I, et al. Radiation pneumonitis andearly circulatory cytokine markers. Semin Radiat Oncol2002;12:26–33.
69. Chen Y, Rubin P, Williams J, et al. Circulating IL-6 as apredictor of radiation pneumonitis. Int J Radiat Oncol BiolPhys 2001;49:641–648.
70. Ishii Y, Kitamura S. Soluble intercellular adhesion mole-cule-1 as an early detection marker for radiation pneumoni-tis. Eur Respir J 1999;13:733–738.
71. Sasaki R, Soejima T, Matsumoto A, et al. Clinical signifi-cance of serum pulmonary surfactant proteins A and D forthe early detection of radiation pneumonitis. Int J RadiatOncol Biol Phys 2001;50:301–307.
72. Goto K, Kodama T, Sekine I, et al. Serum levels of KL-6 areuseful biomarkers for severe radiation pneumonitis. LungCancer 2001;34:141–148.
73. Hara R, Itami J, Komiyama T, et al. Serum levels of KL-6 forpredicting the occurrence of radiation pneumonitis after stereo-tactic radiotherapy for lung tumors. Chest 2004;125:340–344.
74. Fujita J, Ohtsuki Y, Bandoh S, et al. Elevation of cytokeratin19 fragment (CYFRA 21–1) in serum of patients with radi-ation pneumonitis: Possible marker of epithelial cell damage.Respir Med 2004;98:294–300.
75. Koizumi M, Yamazaki H, Toyokawa K, et al. Influence ofthoracic radiotherapy on exhaled nitric oxide levels inpatients with lung cancer. Jpn J Clin Oncol 2001;31:142–146.
76. Hauer-Jensen M, Kong FM, Fink LM, et al. Circulatingthrombomodulin during radiation therapy of lung cancer.Radiat Oncol Investig 1999;7:238–242.
77. Vujaskovic Z, Groen HJ. TGF-beta, radiation-induced pul-monary injury and lung cancer. Int J Radiat Biol 2000;76:511–516.
78. Anscher MS, Kong FM, Andrews K, et al. Plasma transform-ing growth factor �1 as a predictor of radiation pneumonitis.Int J Radiat Oncol Biol Phys 1998;41:1029–1035.
79. Barthelemy-Brichant N, Bosquee L, Cataldo D, et al. In-creased IL-6 and TGF-�1 concentrations in bronchoalveolarlavage fluid associated with thoracic radiotherapy. Int J Ra-diat Oncol Biol Phys 2004;58:758–767.
80. Fu XL, Huang H, Bentel G, et al. Predicting the risk ofsymptomatic radiation-induced lung injury using both thephysical and biologic parameters V30 and transforminggrowth factor �. Int J Radiat Oncol Biol Phys 2001;50:899–908.
81. De Jaeger K, Seppenwoolde Y, Kampinga HH, et al. Signif-icance of plasma transforming growth factor-� levels inradiotherapy for non–small-cell lung cancer. Int J RadiatOncol Biol Phys 2004;58:1378–1387.
82. Novakova-Jiresova A, Van Gameren MM, Coppes RP, et al.Transforming growth factor-beta plasma dynamics and post-irradiation lung injury in lung cancer patients. RadiotherOncol 2004;71:183–189.
83. Bentzen SM, Saunders MI, Dische S. From CHART to
CHARTWEL in non-small cell lung cancer: Clinical radio-
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
23Radiation pneumonitis in NSCLC ● V. MEHTA
biological modelling of the expected change in outcome.Clin Oncol (R Coll Radiol) 2002;14:372–381.
84. Chen GY, Jiang GL, Qian H, et al. Escalated hyperfraction-ated accelerated radiation therapy for locally advanced non-small cell lung cancer: A clinical phase II trial. RadiotherOncol 2004;71:157–162.
85. Saunders M, Dische S, Barrett A, et al. Continuous hyper-fractionated accelerated radiotherapy (CHART) versus con-ventional radiotherapy in non–small-cell lung cancer: A ran-domised multicentre trial. CHART Steering Committee.Lancet 1997;350:161–165.
86. Kirkbride P, Hatton M, Lorigan P, et al. Fatal pulmonaryfibrosis associated with induction chemotherapy with carbo-platin and vinorelbine followed by CHART radiotherapy forlocally advanced non–small cell lung cancer. Clin Oncol (RColl Radiol) 2002;14:361–366.
87. Oral EN, Bavbek S, Kizir A, et al. Preliminary analysis of aphase II study of paclitaxel and CHART in locally advancednon–small cell lung cancer. Lung Cancer 1999;25:191–198.
88. Saunders MI, Rojas A, Lyn BE, et al. Dose-escalation withCHARTWEL (continuous hyperfractionated accelerated ra-diotherapy week-end less) combined with neo-adjuvant che-motherapy in the treatment of locally advanced non–smallcell lung cancer. Clin Oncol (R Coll Radiol) 2002;14:352–360.
89. Rosenman JG, Halle JS, Socinski MA, et al. High-doseconformal radiotherapy for treatment of stage IIIA/IIIB non–small-cell lung cancer: Technical issues and results of aphase I/II trial. Int J Radiat Oncol Biol Phys 2002;54:348–356.
90. Narayan S, Henning GT, Ten Haken RK, et al. Resultsfollowing treatment to doses of 92.4 or 102.9 Gy on a phaseI dose escalation study for non–small cell lung cancer. LungCancer 2004;44:79–88.
91. Wu KL, Jiang GL, Liao Y, et al. Three-dimensional confor-mal radiation therapy for non–small-cell lung cancer: Aphase I/II dose escalation clinical trial. Int J Radiat OncolBiol Phys 2003;57:1336–1344.
92. Hayman JA, Martel MK, Ten Haken RK, et al. Dose esca-lation in non–small-cell lung cancer using three-dimensionalconformal radiation therapy: Update of a phase I trial. J ClinOncol 2001;19:127–136.
93. Bhatnagar A, Flickinger JC, Bahri S, et al. Update on resultsof multifield conformal radiation therapy of non–small-celllung cancer using multileaf collimated beams. Clin LungCancer 2002;3:259–264.
94. Koenig TR, Munden RF, Erasmus JJ, et al. Radiation injuryof the lung after three-dimensional conformal radiation ther-apy. AJR Am J Roentgenol 2002;178:1383–1388.
95. Wurstbauer K, Deutschmann H, Sedlmayer F, et al. Non–small-cell lung cancer: Dose escalation by target splittingwith asymmetric collimation. Clin Lung Cancer 2001;3:151–153.
96. Dirkx ML, Essers M, van Sornsen de Koste JR, et al. Beamintensity modulation for penumbra enhancement in the treat-ment of lung cancer. Int J Radiat Oncol Biol Phys 1999;44:449–454.
97. Dirkx ML, Heijmen BJ. Beam intensity modulation for pen-umbra enhancement and field length reduction in lung cancertreatments: A dosimetric study. Radiother Oncol 2000;56:181–188.
98. van Sornsen de Koste J, Voet P, Dirkx M, et al. An evalu-ation of two techniques for beam intensity modulation inpatients irradiated for stage III non–small cell lung cancer.Lung Cancer 2001;32:145–153.
99. Murshed H, Liu HH, Liao Z, et al. Dose and volume reduc-
tion for normal lung using intensity-modulated radiotherapyfor advanced-stage non–small-cell lung cancer. Int J RadiatOncol Biol Phys 2004;58:1258–1267.
00. Mackie TR, Balog J, Ruchala K, et al. Tomotherapy. SeminRadiat Oncol 1999;9:108–117.
01. Scrimger RA, Tome WA, Olivera GH, et al. Reduction inradiation dose to lung and other normal tissues using helicaltomotherapy to treat lung cancer, in comparison to conven-tional field arrangements. Am J Clin Oncol 2003;26:70–78.
02. Sun LM, Leung SW, Wang CJ, et al. Concomitant boostradiation therapy for inoperable non–small-cell lung cancer:Preliminary report of a prospective randomized study. Int JRadiat Oncol Biol Phys 2000;47:413–418.
03. Pottgen C, Eberhardt W, Bildat S, et al. Induction chemo-therapy followed by concurrent chemotherapy and definitivehigh-dose radiotherapy for patients with locally advancednon–small-cell lung cancer (stages IIIa/IIIb): A pilot phaseI/II trial. Ann Oncol 2002;13:403–411.
04. Hof H, Herfarth KK, Munter M, et al. Stereotactic single-dose radiotherapy of stage I non–small-cell lung cancer(NSCLC). Int J Radiat Oncol Biol Phys 2003;56:335–341.
05. Lee SW, Choi EK, Park HJ, et al. Stereotactic body framebased fractionated radiosurgery on consecutive days for pri-mary or metastatic tumors in the lung. Lung Cancer 2003;40:309–315.
06. Suit H. The Gray Lecture 2001: Coming technical advancesin radiation oncology. Int J Radiat Oncol Biol Phys 2002;53:798–809.
07. Bonnet RB, Bush D, Cheek GA, et al. Effects of proton andcombined proton/photon beam radiation on pulmonary func-tion in patients with resectable but medically inoperablenon-small cell lung cancer. Chest 2001;120:1803–1810.
08. Satoh H, Okumura T, Yamashita YT, et al. Proton irradiationfor non–small cell lung cancer. Arch Intern Med 1998;158:1379–1380.
09. Shioyama Y, Tokuuye K, Okumura T, et al. Clinical evalu-ation of proton radiotherapy for non–small-cell lung cancer.Int J Radiat Oncol Biol Phys 2003;56:7–13.
10. Miyamoto T, Yamamoto N, Nishimura H, et al. Carbon ionradiotherapy for stage I non–small cell lung cancer. Ra-diother Oncol 2003;66:127–140.
11. Kadono K, Homma T, Kamahara K, et al. Effect ofheavy-ion radiotherapy on pulmonary function in stage Inon–small cell lung cancer patients. Chest 2002;122:1925–1932.
12. Jeremic B, Shibamoto Y, Milicic B, et al. Impact of treat-ment interruptions due to toxicity on outcome of patientswith early stage (I/II) non–small-cell lung cancer (NSCLC)treated with hyperfractionated radiation therapy alone. LungCancer 2003;40:317–323.
13. Rosenzweig KE, Mychalczak B, Fuks Z, et al. Final report ofthe 70.2-Gy and 75.6-Gy dose levels of a phase I doseescalation study using three-dimensional conformal radio-therapy in the treatment of inoperable non-small cell lungcancer. Cancer J 2000;6:82–87.
14. Yorke ED, Wang L, Rosenzweig KE, et al. Evaluation ofdeep inspiration breath-hold lung treatment plans with MonteCarlo dose calculation. Int J Radiat Oncol Biol Phys 2002;53:1058–1070.
15. Rosenzweig KE, Hanley J, Mah D, et al. The deep inspira-tion breath-hold technique in the treatment of inoperablenon–small-cell lung cancer. Int J Radiat Oncol Biol Phys2000;48:81–87.
16. Kwok E, Chan CK. Corticosteroids and azathioprine do notprevent radiation-induced lung injury. Can Respir J 1998;5:211–214.
17. Antonadou D, Coliarakis N, Synodinou M, et al. Random-
ized phase III trial of radiation treatment �/� amifostine in
1
1
1
1
1
1
1
1
1
1
24 I. J. Radiation Oncology ● Biology ● Physics Volume 63, Number 1, 2005
patients with advanced-stage lung cancer. Int J Radiat OncolBiol Phys 2001;51:915–922.
18. Antonadou D, Throuvalas N, Petridis A, et al. Effect ofamifostine on toxicities associated with radiochemo-therapy in patients with locally advanced non–small-celllung cancer. Int J Radiat Oncol Biol Phys 2003;57:402–408.
19. Komaki R, Lee JS, Milas L, et al. Effects of amifostine onacute toxicity from concurrent chemotherapy and radiother-apy for inoperable non–small-cell lung cancer: Report of arandomized comparative trial. Int J Radiat Oncol Biol Phys2004;58:1369–1377.
20. Werner-Wasik M, Scott C, Movsas B, et al. Amifostine asmucosal protectant in patients with locally advanced non–small cell lung cancer (NSCLC) receiving intensive che-motherapy and thoracic radiotherapy (RT): Results of theRadiation Therapy Oncology Group (RTOG) 98 – 01study. Int J Radiat Oncol Biol Phys 2003;57:S216.
21. Ward WF, Lin PJ, Wong PS, et al. Radiation pneumonitisin rats and its modification by the angiotensin-convertingenzyme inhibitor captopril evaluated by high-resolutioncomputed tomography. Radiat Res 1993;135:81– 87.
22. Wang LW, Fu XL, Clough R, et al. Can angiotensin-con-
verting enzyme inhibitors protect against symptomaticradiation pneumonitis? Radiat Res 2000;153:405–410.
23. Molteni A, Moulder JE, Cohen EF, et al. Control ofradiation-induced pneumopathy and lung fibrosis by an-giotensin-converting enzyme inhibitors and an angiotensinII type 1 receptor blocker. Int J Radiat Biol 2000;76:523–532.
24. Ozturk B, Egehan I, Atavci S, et al. Pentoxifylline in pre-vention of radiation-induced lung toxicity in patients withbreast and lung cancer: A double-blind randomized trial. IntJ Radiat Oncol Biol Phys 2004;58:213–219.
25. Vijayalaxmi, Reiter RJ, Tan DX, et al. Melatonin as a radio-protective agent: A review. Int J Radiat Oncol Biol Phys2004;59:639–653.
26. Jonsson OE, Bjermer L, Denekamp J, et al. Perivascular cellprotection in vivo and increased cell survival in vitro by theantihypertensive agent carvedilol following radiation. Eur JCancer 1999;35:1268–1273.
27. Guo H, Epperly MW, Bernarding M, et al. Manga-nese superoxide dismutase-plasmid/liposome (MnSOD-PL)intratracheal gene therapy reduction of irradiation-inducedinflammatory cytokines does not protect orthotopic Lewis
lung carcinomas. In Vivo 2003;17:13–21.