Embed Size (px)
Citation preview

ACADEMIC EMERGENCY MEDICINE • July 1999, Volume 6, Number 7 715
Radial Head Subluxation: ComparingTwo Methods of Reduction
JULIA MCDONALD, MD, CHRISTINE WHITELAW, MD,L. JANE GOLDSMITH, PHD
Abstract. Objectives: To determine whether reduc-tion of radial head subluxation (RHS) is more suc-cessful using pronation and flexion (PF) vs the morewidely used supination and flexion (SF) method.Methods: Prospective study in a tertiary care chil-dren’s hospital ED from August 1996 through Decem-ber 1997. Inclusion criteria included age <7 yearswith an upper-extremity injury. Exclusion criteria in-cluded neurologic impairment, congenital malforma-tion, or obvious bony deformity or edema. Patientswere randomized to receive either PF or SF. Reduc-tion was considered successful if the child used theinjured arm. Both the physician and the parent ratedthe child’s pain during the procedure using a descrip-tive ordinal scale, from 0 (no pain) to 3 (severe pain).Results: 148 patients were enrolled; 13 were ex-cluded. Success was achieved on the first attempt in
53/67 (80%, 95% CI = 0.67 to 0.88) of patients receiv-ing PF and in 47/68 (69%, 95% CI = 0.57 to 0.80)of those receiving SF (p = 0.186). For those injuringthe left arm, 29/41 (71%, 95% CI = 0.54 to 0.84) weresuccessfully reduced using SF, while 33/37 (89%, 95%CI = 0.75 to 0.97) were successfully reduced using PF(p = 0.044). Physicians perceived PF to be less pain-ful than SF (p = 0.013). There was no significantpain score difference rated by parents. Conclusions:
Both PF and SF can be used with success to reduceRHS. For left arm injuries, PF should be attemptedfirst, since it may decrease the need for further treat-ment. PF may be less painful, particularly for firstreduction attempts. Key words: radial head sublux-ation; nursemaid’s elbow. ACADEMIC EMERGENCYMEDICINE 1999; 6:715–718
RADIAL head subluxation (RHS), commonlyreferred to as nursemaid’s elbow, is a fre-
quent injury among children less than 7 years ofage. The typical mechanism of injury is longitudi-nal traction applied to an extended arm, which canoccur when pulling a child at the wrist to preventa fall, picking him or her up after a fall, pullingthe arm through a tight sleeve, or swinging a childby the arms. Subsequently, the child cries out inpain and refuses to use the arm. Any attempts atpassive movement are met with resistance. No ob-vious bony deformity or edema is present, and ten-derness is minimal. Typically, RHS is reduced us-ing a rapid supination of the forearm, followed byflexion or extension. However, there are isolatedreports in the medical literature that describe apronation method of reduction.1–4 This method isperformed by rapidly hyperpronating the forearmfollowed by flexion. Only one recent study by Ma-
From the Department of Pediatrics, University of Louisville,Louisville, KY (JM, CW) and the Statistical Consulting Center,University of Louisville, Louisville, KY (LJG).Received September 21, 1998; revision received February 19,1999; accepted February 24, 1999. Presented as a poster at theSAEM annual meeting, Chicago, IL, May 1998.Address for correspondence and reprints: J. McDonald, MD,Pediatric Emergency Medicine, 571 South Floyd Street, Lou-isville, KY 40202. Fax: 502-629-5991; e-mail:[email protected]
cias et al. has compared the success rates of thesetwo methods.4
METHODS
Study Design. This was a prospective, random-ized study to determine whether reduction of RHSis more successful using rapid pronation and flex-ion or the more widely used rapid supination andflexion method. We also attempted to determinewhich method was less painful, and whether therate of success was dependent on the arm injured.This study was approved by the hospital’s institu-tional review board, with parents or guardians giv-ing written prospective consent for enrollment.
Study Population and Site. Subjects were re-cruited from the ED of a tertiary care children’shospital from July 1996 through December 1997.All children less than 7 years old presenting to theED with a complaint of an upper-extremity injury,and who were refusing to use the injured arm,were considered for enrollment. Exclusion criteriaincluded: history of neurologic impairment, con-genital bony malformation, and obvious bony de-formity or edema.
Study Protocol. Patients were randomized to re-ceive either the rapid supination method or therapid pronation method at the time of enrollment.

716 RADIAL HEAD SUBLUXATION McDonald et al. • RADIAL HEAD SUBLUXATION
TABLE 1. Characteristics of Each Treatment Group
Pronation Supination
Age—range 5 months–6 years 3 months–5 years
Sex (p = 0.67)Female 37 40Male 30 28
Handedness (p = 0.55)Left 37 41Right 30 27
Randomization was performed using a blockedrandomization list generated by computer. Therandomization was designed so that the trial wasbalanced after every ten patients, thus ensuringbalance over time. The physician then attemptedto reduce the subluxation using the assignedmethod.
Measurements. Although the patients may havebeen evaluated by residents in pediatrics, emer-gency medicine (EM), internal medicine, or familymedicine, or senior medical students, a pediatricEM attending physician or fellow performed or su-pervised all reductions. Prior to the start of thestudy, physicians received a brief inservice on per-forming both reduction maneuvers. In addition,printed instructions on both methods of reductionwere provided on the enrollment forms. A reduc-tion was considered successful if the subject usedthe injured arm to reach for a piece of candy or afavorite toy. If the child did not use the injured armwithin 30 minutes after the reduction attempt, thephysician repeated the maneuver using the samemethod of reduction. If the child was still not usingthe injured arm 30 minutes following the secondattempt, the alternative method of reduction wasattempted. Both the physician performing the ma-neuver and the parent accompanying the childrated the perceived amount of pain the child ex-perienced during each reduction by documentingtheir assessments of the child’s pain immediatelyfollowing each reduction attempt. A descriptive or-dinal scale demarcated with 0 (no pain), 1 (littlepain), 2 (quite a lot of pain), to 3 (very bad pain)was used. Parent scoring sheets were illustratedwith descriptive drawings of facial expressions.5
Data Analysis. Prior to patient enrollment, itwas estimated that 142 subjects would be requiredto detect with 80% power an increase from 70% to90% success rate with p < 0.05. The success of thereduction was analyzed with a chi-squared test,Fisher’s exact test, and stepwise logistic regres-sion. Analysis of the pain scale ratings was per-formed using the Mann-Whitney U test. A p-value< 0.05 was considered significant.
RESULTS
One hundred forty-eight children were enrolled inthe study (Table 1). Thirteen subjects were ex-cluded: six were found to have a fracture, two spon-taneously reduced while being enrolled, in twocases the study protocol was not followed, and datawere missing for three cases.
On the first attempt, 47/68 (69%, 95% CI = 0.57to 0.80) patients undergoing supination had a suc-cessful reduction, as did 53/67 (79%, 95% CI = 0.67to 0.88) patients undergoing the pronation method.The difference was not statistically significant (p =0.186).
In cases of unsuccessful reduction, the prona-tion method was more successful than the supi-nation method on the second attempt. While onlyfour of 21 patients had a successful reduction usingthe supination method (19%, 95% CI = 0.54 to0.42), nine of 14 reductions involving the pronationmethod were successful (64%, 95% CI = 0.35 to0.87) (p = 0.009). For those patients requiring athird attempt, 13 of 17 initially assigned the su-pination method had success with the pronationmethod (76%, 95% CI = 0.50 to 0.93), and three offive patients initially assigned the pronationmethod were successfully reduced by the supina-tion method (75%, 95% CI = 0.19 to 0.99) (p =1.000).
Of the six patients who never reduced, fourwere in the supination group, and two were in thepronation group. Two of four in the supinationgroup spontaneously reduced after leaving the ED.The other two failed to follow up with their pri-mary care physician as instructed, but were notseen on subsequent visits for upper-extremityproblems. Neither of the two patients in the pro-nation group followed up with their primary carephysician.
Fifty-seven children injured the right arm and78 children injured the left arm. Of those injuringthe right arm, 18/27 (67%, 95% CI = 0.46 to 0.83)were successfully reduced using the supinationmethod and 20/30 (67%, 95% CI = 0.47 to 0.83)were successfully reduced using the pronationmethod (p = 1.000). For those injuring the left arm,however, pronation was more effective (33/37 suc-cessful 89%, 95% CI = 0.75 to 0.97) than supination(29/41 successful, 71%, 95% CI = 0.54 to 0.84) (p =0.044). In an assessment of success of reductionusing logistic regression, while neither the sided-ness of the injury nor the method of reduction byitself was significant, the interaction of the arminjured (right vs left) with the method of reduction(supination vs pronation) yielded a statisticallysignificant association (p = 0.009). This logistic re-gression using the interaction of sidedness andmethod supports the subgroup analysis described

ACADEMIC EMERGENCY MEDICINE • July 1999, Volume 6, Number 7 717
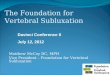
Figure 1. Degree of pain as perceived by physicians.
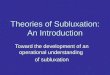
Figure 2. Degree of pain as perceived by parents.
above, in which the right-sided injuries showed nostatistically significant difference. Left-sided inju-ries, however, favored pronation.
On first reduction attempts, physicians per-ceived the pronation method of reduction to be sig-nificantly less painful than the supination method(p = 0.013). For second and third reduction at-tempts, however, there was no statistically signif-icant difference in the degree of pain as perceivedby physicians (p = 0.145 and p = 0.594, respec-tively) (Fig. 1). Parental perceptions of the painduring reduction were similar for the two groupson all three attempts (p = 0.169, p = 0.168, and p= 0.667, respectively) (Fig. 2).
DISCUSSION
Although the pronation method of reduction waselaborately described in J. Hutchinson’s paper in1885, and further described in his paper in theBritish Medical Journal in 1886, little has sincebeen written about this method.1,2 During the sameperiod, multiple articles describing the supinationmethod of reduction were published.6–9 Despitethese early articles reporting success with bothmethods, most of the current textbooks in both pe-diatrics and orthopedics describe the supinationmethod as the preferred method of reduction. Inclinical practice, however, many practitionersanecdotally report better success using the prona-tion method. A recent report by Macias et al. ad-vocated the pronation technique as a more suc-cessful method of reduction when compared withthe supination method.4 This study did not differ-entiate success between the left and the right arm,however, and did not attempt to assess pain.
We found no significant difference in the suc-cess rate of the two methods in our study exceptwhen a second attempt at reduction was required,with the pronation method being more successful.On third reduction attempts, when patientscrossed over to the alternative method, we foundthe two methods to be equally successful.
In our study, as in previous studies, the left armis more frequently injured.10–15 As the majority ofinvestigators performing reduction maneuverswere right-handed, the supination maneuverseems a more natural movement for the examinerwhen the patient’s left arm is injured; however, wefound the pronation method to be more successfulin performing reductions of subluxations involvingthe left arm.
Radial head subluxation reduction involvessome degree of pain for the patient. Assuming thatsuccess rates for the two methods may be equal,our study sought to determine whether one methodof reduction is less painful than the other, andwould hence be preferable. Lyver reported that pa-
tients experienced less anxiety using the pronationmethod of reduction.3 Nichols also stated that chil-dren complain less with the pronation method.12
Our study supports this trend as demonstrated bythe lower pain scores recorded by investigators forthe pronation method on first attempts at reduc-tion. A significant difference in pain was not seenon subsequent attempts. This may be due to asmaller ability to detect a difference. Parents de-tected no difference in pain between the two meth-ods, although their pain scores had more variationwhen compared with those of the physicians.
LIMITATIONS AND FUTURE QUESTIONS
Limitations of our study in assessing pain includethe use of an ordinal pain scale. A greater differ-ence in pain might have been detected if a contin-uous scale had been used. The scale we used wasa modified version of a known scale developed byWong and Baker.5 Although this modified versionhas not been tested to be as accurate as the origi-nal version, the version we used is one that hasbeen adopted by our institution for the nursing

718 RADIAL HEAD SUBLUXATION McDonald et al. • RADIAL HEAD SUBLUXATION
staff to assess children’s pain in all clinical situa-tions.
Because blinding to the method of reductionwas impossible, physician bias in recording painassessment was possible. No attempt was made toassess the patient’s pain by self-report due to thepatient’s young age. Although a core group of prac-titioners to assess the children’s pain both beforeand during reduction would have been ideal, lim-iting the reductions to a small group would haveresulted in less experience for our residents andmedical students. Since physicians from a varietyof specialties are faced with having to reduce RHS,our study design more closely emulates the situa-tion present in most EDs.
Bias could also have been introduced because ofthe subjective endpoint. However, most of the cur-rent textbooks in pediatrics, EM, and orthopedicsdescribe spontaneous movement as an indicationof a successful reduction.
The reason for the difference in successful re-duction with each method between the right andleft arm is not clear. Further biomechanical studiesare needed to definitely determine why the pro-nation method works better than the supinationmethod for left arm injuries.
CONCLUSIONS
Both the pronation and supination methods can beused for reduction of RHS with equal success. Wefound the pronation method to be more successfulif the left arm is injured. Physicians perceived the
pronation method as subjectively less painful forthe child. For the above reasons, we offer the pro-nation method as a substitute for the supinationmethod, or an alternative when the supinationmethod is not successful.
References
1. Hutchinson J. On certain obscure sprains of the elbow oc-curring in young children. Ann Surg. 1885; 2:91–8.2. Hutchinson J. Partial dislocation of the head of the radiuspeculiar to children. Br Med J. 1886; 1:9–10.3. Lyver MB. Radial head subluxation [letter]. J Emerg Med.1990; 8:154–5.4. Macias CG, Bothner J, Wiebe R. A comparison of supina-tion/flexion to hyperpronation in the reduction of radial headsubluxations. Pediatrics. 1998; 102:e10.5. Wong DL, Baker CM. Pain in children: comparison of as-sessment scales. Pediatr Nurs. 1988; 14:9–17.6. Poinsot G. Dislocation of the head of the radius downwardby elongation. NY Med J. 1885; 441:8–11.7. Lindeman SH. Partial dislocation of the head of the radiuspeculiar to children. Br Med J. 1885; 2:1058–9.8. Cushing HW. Subluxation of the radial head in children.Boston Med Surg J. 1886; 114:77–80.9. Van Arsdale WW. On subluxation of the head of the radiusin children with a resume of 100 consecutive cases. Ann Surg.1889; 9:401–23.10. Salter RB, Zaltz C. Anatomic investigations of the mech-anism of injury and pathologic anatomy of ‘‘pulled elbow’’ inyoung children. Clin Orthop. 1971; 77:134–3.11. Quan L, Marcuse EK. The epidemiology and treatment ofradial head subluxation. Am J Dis Child. 1985; 139:1194–7.12. Nichols HH. Nursemaid’s elbow: reducing it to simpleterms. Contemp Pediatr. 1988; 5(May):50–7.13. Amir D, Frankl U, Pogrund H. Pulled elbow and hyper-mobility of joints. Clin Orthop. 1990; 257(Aug):94–9.14. Magill HK, Aitken AP. Pulled elbow. Surg Gynecol Obstet.1954; 98:753–6.15. Schunk JE. Radial head subluxation: epidemiology andtreatment of 87 episodes. Ann Emerg Med. 1990; 19:1019–23.