-
8/16/2019 r1 DMCN 13163 Review
1/12
Online Proofing System Instructions
The Wiley Online Proofing System allows authors and proof
reviewers to review PDF proofs, mark corrections, respond
to queries, upload replacement figures, and submit these changes
directly from the PDF proof from the locally saved file
or while viewing it in your web browser.
1. For the best experience reviewing your proof in the
Wiley OnlineProofing System please ensure you are connected to the
internet.
This will allow the PDF proof to connect to the central Wiley
Online
Proofing System server. If you are connected to the Wiley
Online
Proofing System server you should see the icon with a green
check
mark above in the yellow banner.
2.
Please review the article proof on the following pages and mark
anycorrections, changes, and query responses using the Annotation
Tools
outlined on the next 2 pages.
3.
To save your proof corrections, click the “Publish Comments”
button appearing above in the yellow banner. Publishing your
comments saves your corrections to the Wiley Online Proofing
System server. Corrections don’t have to be marked in one
sitting,
you can publish corrections and log back in at a later time to
add
more before you click the “Complete Proof Review” button
below.
4.
If you need to supply additional or replacement files bigger
than
5 Megabytes (MB) do not attach them directly to the PDF
Proof,
please click the “Upload Files” button to upload files:
5.
When your proof review is complete and you are ready to submit
corrections to the publisher, please click
the “Complete Proof Review” button below:
IMPORTANT: Do not click the “Complete Proof Review” button
without replying to all author queries found on
the last page of your proof. Incomplete proof reviews will cause
a delay in publication.
IMPORTANT: Once you click “Complete Proof Review” you will not
be able to publish further corrections.
Connected Disconnected
Click Here
Click Here
-
8/16/2019 r1 DMCN 13163 Review
2/12
USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
Once you have Acrobat Reader open on your computer, click on the
Comment tab at the right of the toolbar:
This will open up a panel down the right side of the document.
The majority of
tools you will use for annotating your proof will be in the
Annotations section,pictured opposite. We’ve picked out some of
these tools below:
1. Replace (Ins) Tool – for replacing text.
Strikes a line through text and opens up a text
box where replacement text can be entered.
How to use it
Highlight a word or sentence.
Click on the Replace (Ins) icon in the Annotations
section.
Type the replacement text into the blue box that
appears.
2. Strikethrough (Del) Tool – for deleting t ext.
Strikes a red line through text that is to be
deleted.
How to use it
Highlight a word or sentence.
Click on the Strikethrough (Del) icon in the
Annotations section.
3. Add note to text Tool – for highlighting a section
to be changed to bold or italic.
Highlights text in yellow and opens up a text
box where comments can be entered.
How to use it
Highlight the relevant section of text.
Click on the Add note to text icon in the
Annotations section.
Type instruction on what should be changed
regarding the text into the yellow box thatappears.
4. Add sticky note Tool – for making notes at
specific points in the text.
Marks a point in the proof where a comment
needs to be highlighted.
How to use it
Click on the Add sticky note icon in the
Annotations section.
Click at the point in the proof where the comment
should be inserted.
Type the comment into the yellow box thatappears.
-
8/16/2019 r1 DMCN 13163 Review
3/12
USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
5. Attach File Tool – for inserting large amounts of
text or replacement figur es.
Inserts an icon linking to the attached file in the
appropriate place in the text.
How to use it
Click on the Attach File icon in the Annotations
section.
Click on the proof to where you’d like the attached
file to be linked.
Select the file to be attached from your computer
or network.
Select the colour and type of icon that will appear
in the proof. Click OK.
6. Drawing Markups Tools – for drawing
shapes, lines and freeform annotations on
proofs and commenting on these marks.Allows shapes, lines and
freeform annotations to be
drawn on proofs and for comment to be made on
these marks.
How to use it
Click on one of the shapes in the Drawing Markups
section.
Click on the proof at the relevant point and draw the
selected shape with the cursor.
To add a comment to the drawn shape, move the
cursor over the shape until an arrowhead appears.
Double click on the shape and type any text in the
red box that appears.
-
8/16/2019 r1 DMCN 13163 Review
4/12
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY ORIGINAL
ARTICLE
Evaluation of non-coding variation in GLUT1 deficiency
YU-CHI LIU1,2,* JIA WEI AUDREY LEE1,*
SUSANNAH T BELLOWS1 JOHN A DAMIANO1
SAUL A MULLEN1,3 SAMUEL F BERKOVIC1
MELANIE BAHLO2 INGRID E SCHEFFER1,3,4
MICHAEL S HILDEBRAND1 CLINICAL GROUP†1
1 Department of Medicine, Epilepsy Research Centre, Austin
Health, University of Melbourne, Heidelberg, Vic.; 2
Population Health and Immunity Division, The Walter
and Eliza Hall Institute, Parkville, Vic.; 3 Florey
Institute, Heidelberg, Vic.; 4 Department of
Paediatrics, University of Melbourne, Royal Children’s Hospital,
Parkville,
Vic., Australia.
Correspondence to Michael S Hildebrand, Epilepsy Research
Centre, 245 Burgundy St Heidelberg, Vic. 3084, Australia. E-mail:
[email protected]
*These authors contributed equally to this work.†Members of the
group are listed in Appendix A.
PUBLICATION DATA
Accepted for publication 14th April 2016.
Published online
ABBREVIATIONS
CSF Cerebrospinal fluid
GLUT-1 Glucose transporter-1
AIM Loss-of-function mutations in SLC2A1, encoding
glucose transporter-1 (GLUT-1), lead to
dysfunction of glucose transport across the
blood – brain barrier. Ten percent of cases with
hypoglycorrhachia (fasting cerebrospinal fluid [CSF] glucose
-
8/16/2019 r1 DMCN 13163 Review
5/12
deficiency, making it difficult to identify
genotype – pheno-type correlations, as emphasized by a
recent French study of 265 patients.12 Despite this molecular
diagnostic suc-cess, SLC2A1 mutations are not
detected in 10% of patients with 16y)
3.3 – 4.4 (age 50% of pairedserum glucose
levela
5 2.8 – 4.5
6 3.3 – 4.4
7 3.0 – 4.5
8 2.5 – 5.0
9 2.2 – 5.5
10 2.8 – 4.0
11 3.3 – 4.5
12 2.5 – 5.6
13 2.5 – 5.5
14 2.8 – 4.4
15 2.8 – 5.0
aOnly paired CSF and serum glucose levels were interpretable
for
this laboratory.
What this paper adds• Deep intronic SLC2A1
mutations may cause GLUT1 deficiency.
• Awareness of age-related cerebrospinal fluid (CSF)
glucose levels critical in
GLUT1 deficiency evaluation.
• Sequencing of SLC2A1 is worthwhile when
GLUT1 deficiency is suspected.
2 Developmental Medicine & Child
Neurology 2016
http://www.novocraft.com/http://www.novocraft.com/
-
8/16/2019 r1 DMCN 13163 Review
6/12
UCSC Genome Browser). PCR duplicates were removedusing
MarkDuplicates from Picard version 1.117
(http://broadinstitute.github.io/picard/; Broad Institute,
Cambridge,
MA, USA). Variant calling was performed with
GATK HaplotypeCaller (version v3.2 – 2) and variant
annotation
with ANNOVAR
(http://annovar.openbioinformatics.org/en/latest/; University of
Pennsylvania, Philadelphia, PA,USA). Variants were filtered
according to the following cri-teria: location in exonic or
splicing regions; mutation types(missense, stopgain/loss, coding
indels, or potential splicesite mutations); a minor allele
frequency ≤0.01 in the 1000Genomes dataset, Exome
Aggregation Consortium database,or the 6500 NHLBI-ESP exomes
dataset; and appearancein C; Fig. 1) and verifiedby Sanger
sequencing. This variant was not found in pub-licly available
databases including dbSNP, ExAC, the 1000Genomes and the 6500
NHLBI-ESP exomes dataset. Con-sidering its location within a splice
site, the potential effect of the mutation on the splicing
process was first evaluatedcomputationally. Splice-Site Analyzer
Tool software indi-cated that the mutation reduced the similarity
score of thesplice site to the consensus splice site sequence from
81.77to 69.29 (http://ibis.tau.ac.il/ssat/SpliceSiteFrame.htm;
Tel
Aviv University, Tel Aviv, Israel), predicting the
splicingmachinery may recognize an alternate splice site instead
of the mutated site.
Confirmation of SLC2A1 intron
retentionBecause SLC2A1 is expressed in lymphocytes, we
examinedthe effect of the mutation by extracting RNA from
venousblood of the proband and his unaffected mother.
Oligonu-cleotides were designed to amplify sequence from exon 5to
exon 8 (415 base pairs), and this size fragment wasamplified from
the cDNA of the mother who was homozy-gous wild-type c.972+5G (Fig.
2). However, when the
Non-Coding Variation in GLUT1 Deficiency Yu-Chi Liu et al.
3
http://broadinstitute.github.io/picard/http://broadinstitute.github.io/picard/http://annovar.openbioinformatics.org/en/latest/http://annovar.openbioinformatics.org/en/latest/http://www.ncbi.nlm.nih.gov/nuccore/NM_006516http://www.ncbi.nlm.nih.gov/genehttp://www.mrc-holland.com/http://ibis.tau.ac.il/ssat/SpliceSiteFrame.htmhttp://ibis.tau.ac.il/ssat/SpliceSiteFrame.htmhttp://www.mrc-holland.com/http://www.ncbi.nlm.nih.gov/genehttp://www.ncbi.nlm.nih.gov/nuccore/NM_006516http://annovar.openbioinformatics.org/en/latest/http://annovar.openbioinformatics.org/en/latest/http://broadinstitute.github.io/picard/http://broadinstitute.github.io/picard/
-
8/16/2019 r1 DMCN 13163 Review
7/12
T a b l e
I I :
P h e n o t y p e a n d f a s t i n g c e r e b r o s p
i n a l f l u i d ( C S F ) g l u c o s e r e s u l t s o f p a t i e n t s w i
t h n o v e l v a r i a n t s i n S L C 2 A 1
P r o b a n d
V a r i a n t
E p i l e p s y
s y n d r o m
e
S e i z u r e t y p e
A g e o f
o n s e t
D e v e l o p m e n t /
i n t e l l e c t
O t h e r
c l i n i c a l
f e a t u r e s
F a s t i n g C
S F
g l u c o s e l e v e l
( m m o l / L )
[ a g e a t t e
s t ]
L a b o r a t o r y
r e f e r e n c e
r a n g e
( m m o l / L )
A g e - s p e c i fi c
r e f e r e n c e
r a n g e
( L e e n
e t a l . ,
2 0 1 0 )
( m m o l / L )
E E G fi n
d i n g s
H e a d
c i r c u m f e r e n c e
( c e n t i l e )
F a m i l y 1 ,
I I : 1
A ( c . 9 7 2 + 5 G > C )
G L U T 1
e n c e p h a l o p a t h y
A t y p i c a l
a b s e n c e ,
n o n - c o n v u l s i v e
s t a t u s
e p i l e p t i c u s
4 y e a r s
D e l a y e d ,
r e g r e s s i o n ,
m o d e r a t e
i n t e l l e c t u a l
d i s a b i l i t y
A t a x i a ,
d y s a r t h r i a ,
h y p e r -
v e n t i l a t i o n
i n d u c e d
t e t a n y
1 . 9
[ 5 y ]
2 . 8 – 4 . 0
2 . 5 – 4 . 0
G e n e r a
l i z e d
s p i k e w a v e ,
p o l y s p
i k e
w a v e ,
f r e q u e
n t
m u l t i f o c a l
d i s c h a
r g e s
2 0 t h – 3 0 t h
F a m i l y 2 ,
I I : 1
B ( c . 1
9 – 4 2 0 C > T )
E p i l e p s y
w i t h
m y o c l o
n i c -
a t o n i c s
e i z u r e s
T o n i c / c l o n i c ,
M y o c l o n i c ,
D r o p a t t a c k s
3 y e a r s
N o r m a l
2 . 7
[ 3 y ]
2 . 8 – 5 . 0
2 . 5 – 4 . 0
G e n e r a
l i z e d
s p i k e w a v e ,
p o l y s p
i k e w a v e
5 0 t h – 6 0 t h
F a m i l y 3 ,
I I : 1
C ( c . 1
9 – 2 0 7 T > C )
E a r l y - o n
s e t
a b s e n c e
e p i l e p s y
A b s e n c e
1 2 m o n t h s
D e l a y e d
2 . 6
[ 1 6 m o ]
2 . 8 – 4 . 5
2 . 4 – 4 . 2
G e n e r a
l i z e d
s p i k e w a v e
4 0 t h – 5 0 t h
F a m i l y 4 ,
I I I : 1
E p i l e p t i c
e n c e p h a l o p a t h y
F o c a l m o t o r
s e i z u r e s ,
g e n e r a l i z e d
t o n i c c l o n i c
s e i z u r e s ,
s t a t u s
e p i l e p t i c u s
6 w e e k s
D e l a y e d ,
r e g r e s s i o n ,
s e v e r e
i n t e l l e c t u a l
d i s a b i l i t y
N o n - v e r b a l ,
c o m p l e x
m o v e m e n t
d i s o r d e r ,
b e h a v i o u r a l
i s s u e s
2 . 9
[ 2 y ]
3 . 5
[ 1 3 y ]
4 . 4
[ 1 4 y ]
3 . 0 – 5 . 0
2 . 4 – 4 . 2
G e n e r a
l i z e d
s l o w i n
g ,
n o d e fi
n i t e
e p i l e p t i f o r m
d i s c h a
r g e s
1 0 t h
4 Developmental Medicine & Child
Neurology 2016
-
8/16/2019 r1 DMCN 13163 Review
8/12
same amplification was performed for the proband,
the wild-type (415 base pairs) fragment and a larger
fragment (~ 570 base pairs) were observed (Fig. 2). These
resultsrevealed incorporation of intron 7 to 8 sequence in theRNA
produced by the mutant allele. This intron inclusionis predicted to
lead to a premature stop codon(p.S324+28*).
Screening for non-coding single nucleotide and copy
number variantsBased on the findings for Family 1, we searched
for non-coding mutations in promoter and intronic regions
of SLC2A1 in the 55 remaining probands by Sanger
sequenc-ing and multiplex-ligation-dependent probe
amplification.
Two novel single nucleotide variants in deep
intronicregions were identified by sequencing in three families(one
variant was found in two probands) (Fig. 1) but none
was found in the promoter regions. We also searched
forcopy number variants at the SLC2A1 locus by
multiplex-ligation-dependent probe amplification in the 55
remainingprobands, but none were found (data not shown).
Intronic variants reduce SLC2A1 mRNA
transcriptRNA from fresh venous blood was obtained from two
indi-
viduals from Family 4 with a deep intronic variant;
bloodsamples were not available for transcript analysis
fromFamilies 2 and 3. Real-time PCR studies using cDNA derived
from patient RNA revealed markedly reducedSLC2A1 mRNA
transcript in the proband (who carries
variant C) compared with her unaffected mother
(without variant C) (Fig. 3). The proband had around
half the
mRNA of her mother, consistent with near-failure of
tran-scription from one allele of SLC2A1.
Phenotypic analyses of patients with intronic variants The
three probands with intronic variants presented with arange of
phenotypes (Table II): epilepsy with myoclonic-atonic seizures
(Family 2), early-onset absence epilepsy
with developmental delay (Family 3), and
GLUT1encephalopathy with seizures, developmental delay
andregression, complex motor disorder (ataxia, dystonia,
andepisodic events), and progressive microcephaly (Family 4).
The CSF glucose levels (2.6 – 2.9mmol/L) of all
three
Controla b c
c.972+5 G>C c.19-420 C>T c.19-207 T>C
Control Control
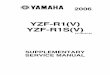
Figure 1:5 4Novel SLC2A1 non-coding variants in
families. Variant A is the splice site mutation identified by whole
exome sequencing in Family 1. Variant
B was found in Family 2, and variant C in Families 3 and 4.
587
M
o t h er –RT
M
o t h er +RT
P r o b an d –RT
P r o
b an d +RT
p U C 1 8 DNA H
a el l l l a d d er
MUT splice product (~570 bp)
WT splice product (415 bp)
458434
298
Figure 2: Transcript analysis in Family 1 confirms intron
retention. Reverse transcriptase PCR results showing inclusion of
intron 7 to 8 sequence in the
c.972+5G>C mutant transcript. A pUC18 DNA HaeIII ladder was
run. The wild-type fragments are 415 base pairs whereas the mutant
fragment is largerdue to retention of intron 7 to 8 sequence in the
transcript from one allele. No amplification is observed from the
minus reverse transcriptase (RT) con-
trol samples.
L O W
R E S O L U T I O N C O L O R F I G
C O L O R
Non-Coding Variation in GLUT1 Deficiency Yu-Chi Liu et al.
5
-
8/16/2019 r1 DMCN 13163 Review
9/12
probands were low according to laboratory-specific refer-ence
ranges; however, when compared with age-specificreference ranges,
the levels were within the normal range
(Table II).
3
The proband from Family 1 has trialled theketogenic diet,
however they found it difficult to imple-ment because the patient
refused food. Seizures in pro-bands of Families 3 and 4 have been
well controlled onanti-epileptic medication. The proband from
Family 4 hassevere intellectual disability and is severely
restricted dueto autistic features and behavioural problems. A
modified
Atkins or ketogenic diet is now being considered in
thesepatients.
DISCUSSION A critical issue is the variation in the
definition of normalCSF glucose levels in different laboratories
(Table I).3,10
Yang et al.10 note that the normal range for CSF
glucosehas never been properly defined, and this has led to
con-siderable confusion about the lower limits of normal CSFglucose
in patients whose presentation falls within theGLUT1 phenotypic
spectrum.5,6,9 This is further compli-cated by the need for
age-specific reference ranges asclearly delineated by Leen et al.3
When reviewing theseranges for the probands of Families 2 to
4 with intronic
variants, it is notable that all would be defined as
havingnormal fasting CSF glucose for age in contradistinction
totheir laboratory-specific ranges (Table II). The proband
of Family 4 had three CSF glucose test results, which
interestingly show marked variability (2.9, 3.3,
4.4). Although testing should be performed in the fasting
state,it is possible that adequate fasting is not always
achievedand could result in pre-analytical error. The abnormalmRNA
transcript levels found in one proband is highly suggestive of
GLUT1 deficiency, implying that the morerecent parameters
suggesting that CSF glucose lower than3.3mmol/L are more
appropriate to consider for investiga-tion of this treatable
disease. Even so, 52 of our 56 patientsdid not have mutations, and
it remains unclear if theirCSF glucose level reflects normal
physiological variationor GLUT1 deficiency. Although genetic
heterogeneity may also underlie GLUT1 deficiency, our
sequencing of related transporters GLUT3 and
MCT1 – 4 did not identify mutations.14
Sequencing of SLC2A1 intronic and promoter
sequencesrevealed a novel de novo single nucleotide splice site
muta-tion in the proband of Family 1 by whole exome analysis,and
novel deep intronic variants in the probands of Fami-lies 2, 3, and
4 (Fig. 1). SLC2A1 splice site mutations have
been reported in GLUT1 deficiency with abnormal splic-ing of the
mRNA transcripts in some cases3,13,15,16
(Table SIII, online supporting information). These splicesite
mutations have been found 1 to 3 base pairs from
theintron – exon boundary, whereas our mutation was 5
basepairs from the boundary (Table SIII). Our transcript stud-ies
showed that the de novo splice site mutation led to dis-ruption of
the original donor splice site and utilization of acryptic splice
site further into the intron, resulting inintron inclusion in the
transcript (Fig. 2). This transcript islikely to lead to
translation of aberrant protein due to apremature stop codon, and
consequent GLUT1 trans-
porter deficiency.Here we show that deep intronic variants can
also alterSLC2A1 transcription and are likely to lead to
GLUT1deficiency (Fig. 3). To add further support for
thepathogenicity of these variants, functional studies such
aserythrocyte 3-O-methyl-d-glucose uptake assays could
beconsidered. Recurrent, novel variant C (c.19 – 207
T>C),found in Families 3 and 4, is predicted by the Encode
pro-
ject (http://www.genome.ucsc.edu/ENCODE/;
StanfordUniversity, Stanford, CA, USA) to be in a region enrichedin
H3K27Ac, H3K4me1, and H3K4me3 histone markingscharacteristic of
active enhancer elements.17 Alteration of these
epigenetic modifications has the potential to change
chromatin structure and de-regulate gene transcription.18
For example, binding of transcription factors to
intronicenhancer elements has been found to regulate, through
his-tone modifications, CFTR expression in cystic fibrosis.19
In silico predictions suggest that variant B
(c.19 – 428C> T), found in Family 2, lies within
a gene region
where DNA-dependent RNA polymerase II subunit
A (POLR2A) – the largest subunit of RNA
polymerase II – binds. Therefore, variant B could
affect POLR2A bindingand enhancer interaction, leading to altered
transcriptionof SLC2A1. This type of effect is not
unprecedented inepilepsy as a deep intronic variant in a pseudoexon
was
1.2
SLC2A1 mRNA
1
Mother
Proband
0.8
0.6
R e l a t i v e m R N A
0.4
0.2
0
Figure 3: Real-time PCR analysis reveals reduced
transcript due to deep
intronic mutation. Real-time PCR results showing reduction of
SLC2A1
mRNA transcript in blood due to the presence of variant C in the
proband
from Family 4 compared with her unaffected mother who does not
carry
the variant.
C O L O R
6 Developmental Medicine & Child
Neurology 2016
http://www.genome.ucsc.edu/ENCODE/http://www.genome.ucsc.edu/ENCODE/
-
8/16/2019 r1 DMCN 13163 Review
10/12
discovered that altered the expression of ALDH7A1
inpyridoxine-dependent epilepsy.20 However, we could
not determine the effect of this variant, because blood
samplesfrom suitable family members were unavailable for
tran-script analysis.
A molecular diagnosis was not found for most of ourcohort
with low CSF glucose levels according to current clinical
laboratory reference ranges, despite examination of SLC2A1
coding and non-coding regions. Part of the expla-nation may
be that we did not sequence introns 1 and 2comprehensively because
of their large size (~ 15 and 12megabases, respectively), and
there may be other distantly located non-coding sites
important for SLC2A1 regulation.
Our findings suggest that, in a patient with clinical
andlaboratory features of GLUT1 deficiency, and a normalresult from
standard sequencing of SLC2A1, specific stud-ies looking
for smaller intragenic, or contiguous copy number variants and
structural variants, should be per-formed, followed by sequencing
of intronic regions.
A C K N O W L E D G E M E N T S We thank the patients and
their families for participation in this
study. Elena Aleksoska (Epilepsy Research Centre) is
acknowl-
edged for performing genomic DNA extractions. This study was
supported by a National Health and Medical Research Council
(NHMRC) Program Grant (628952) to SFB and IES, a Practi-
tioner Fellowship (1006110) to IES and a Career
Development
Fellowship (1063799) to MSH. MB was supported by an
NHMRC Senior Research Fellowship (1002098) and NHMRC
Program Grant (1054618). This work was also supported by
Vic-
torian State Government Operational Infrastructure Support
and
Australian Government NHMRC IRIISS funding to MB and
YL.
Authors report grant funds that contributed to this
project as out-
lined above. IES discloses payments from UCB Pharma, Eisai,
GSK, Athena Diagnostics, and Transgenomics for lectures and
educational presentations, and a patent for SCN1A
testing held by
Bionomics Inc. licensed to various diagnostic companies. SFB
dis-
closes payments from UCB Pharma, Novartis Pharmaceuticals,
Sanofi-Aventis, and Jansen Cilag for lectures and educational
pre-
sentations, and a patent for SCN1A testing held by
Bionomics
Inc. licensed to various diagnostic companies.
S U P P O R T I N G I N F O R M A T I O N
The following additional material may be found online:
Table SI: Oligonucleotides used in this study. Table
SII: Exome coverage statistics.
Table SIII: Reported SLC2A1 splice site
mutations.
REFERENCES
1. Simpson IA, Carruthers A, Vannucci SJ. Supply and
demand in cerebral energy metabolism: the role of
nutrient transporters. J Cereb Blood Flow Metab
2007; 27 :
1766 – 91.
2. De Vivo DC, Trifiletti RR, Jacobson RI, Ronen GM,
Behmand RA, Harik SI. Defective glucose transport
across the blood-brain barrier as a cause of
persistent
hypoglycorrhachia, seizures, and developmental delay.
N
Engl J Med 1991; 325:
703 – 09.
3. Leen WG, Klepper J, Verbeek MM, et al. Glucose
transporter-1 deficiency syndrome: the expanding clini-
cal and genetic spectrum of a treatable disorder.
Brain
2010; 133: 655 – 70.
4. Pearson TS, Akman C, Hinton VJ, Engelstad K, De
Vivo DC. Phenotypic spectrum of glucose transporter
type 1 deficiency syndrome (Glut1 DS). Curr
Neurol
Neurosci Rep 2013; 13: 342.
5. Arsov T, Mullen SA, Damiano JA, et al. Early onset
absence epilepsy: 1 in 10 cases is caused by GLUT1
deficiency. Epilepsia 2012; 53:
e204 –
07. doi:10.1111/epi.12007.
6. Arsov T, Mullen SA, Rogers S, et al. Glucose trans-
porter 1 deficiency in the idiopathic generalized epilep-
sies. Ann Neurol 2012; 72 :
807 – 15.
7. Mullen SA, Marini C, Suls A, et al. Glucose transporter
1 deficiency as a treatable cause of myoclonic astatic epi-
lepsy. Arch Neurol 2011; 68:
1152 – 55.
8. Suls A, Dedeken P, Goffin K, et al. Paroxysmal exer-
cise-induced dyskinesia and epilepsy is due to mutations
in SLC2A1, encoding the glucose transporter GLUT1.
Brain 2008; 131: 1831 – 44.39. Suls A,
Mullen SA, Weber YG, et al. Early-onset
absence epilepsy caused by mutations in the glucose
transporter GLUT1. Ann Neurol 2009; 66:
415 – 19.
10. Yang H, Wang D, Engelstad K, et al. Glut1
deficiency
syndrome and erythrocyte glucose uptake assay. Ann
Neurol 2011; 70:
996 – 1005.
11. Klepper J, Scheffer H, Elsaid MF, Kamsteeg EJ, Lefer-
ink M, Ben-Omran T. Autosomal recessive inheritance
of GLUT1 deficiency syndrome. Neuropediatrics
2009;
40: 207 – 10.
12. Hully M, Vuillaumier-Barrot S, Le Bizec C, et al. From
splitting GLUT1 deficiency syndromes to overlapping
phenotypes. Eur J Med Genet 2015; 58:
443 – 54.
13. Wang D, Kranz-Eble P, De Vivo DC. Mutational anal-
ysis of GLUT1 (SLC2A1) in Glut-1 deficiency syn-
drome. Hum Mutat 2000; 16:
224 –
31.14. Hildebrand MS, Damiano JA, Mullen SA, et al. Glucose
metabolism transporters and epilepsy: only GLUT1 has
an established role. Epilepsia 2014; 55:
e18 – 21.
15. Hashimoto N, Kagitani-Shimono K, Sakai N, et al.
SLC2A1 gene analysis of Japanese patients with glucose
transporter 1 deficiency syndrome. J Hum
Genet 2011;
56: 846 – 51.
16. Woo SB, Lee KH, Kang HC, Yang H, De Vivo DC,
Kim SK. First report of glucose transporter 1
deficiency
syndrome in Korea with a novel splice site mutation.
Gene 2012; 506 : 380 – 82.
17. Heintzman ND, Stuart RK, Hon G, et al. Distinct and
predictive chromatin signatures of transcriptional pro-
moters and enhancers in the human genome. Nat
Genet
2007; 39: 311 – 18.
18. Gupta J, Kumar S, Li J, Krishna Murthy Karuturi R,
Tikoo K. Histone H3 lysine 4 monomethylation
(H3K4me1) and H3 lysine 9 monomethylation
(H3K9me1): distribution and their association in regu-
lating gene expression under hyperglycaemic/hyperinsu-
linemic conditions in 3T3 cells. Biochimie 2012;
94:
2656 – 64.
19. Paul T, Li S, Khurana S, Leleiko NS, Walsh MJ. The
epigenetic signature of CFTR expression is co-ordinated
via chromatin acetylation through a complex intronic
element. Biochem J 2007; 408:
317 – 26.
20. Milh M, Pop A, Kanhai W, et al. Atypical
pyridoxine-dependent epilepsy due to a pseudoexon in ALDH7A1.
Mol Genet Metab 2012; 105:
684 – 86.
Non-Coding Variation in GLUT1 Deficiency Yu-Chi Liu et al.
7
http://dx.doi.org/10.1111/epi.12007http://dx.doi.org/10.1111/epi.12007http://dx.doi.org/10.1111/epi.12007http://dx.doi.org/10.1111/epi.12007
-
8/16/2019 r1 DMCN 13163 Review
11/12
APPENDIX A:CLINICAL GROUP
The following authors are clinicians who provided
patientsfor this study: Monique M. Ryan, Department of Neurol-ogy,
Royal Children’s Hospital, and Department of Paedi-atrics,
University of Melbourne, Royal Children’s Hospital,Parkville,
Victoria; Richard J. Leventer, Department of
Neurology, Royal Children’s Hospital; Department of
Pae-diatrics, University of Melbourne, Royal Children’s Hospi-tal;
and Murdoch Children’s Research Institute, RoyalChildren’s
Hospital, Parkville, Victoria; Jeremy L. Free-man, Department of
Neurology, Royal Children’s Hospi-tal, Parkville, Victoria; Mark T.
Mackay, Department of Neurology, Royal Children’s Hospital,
and Department of
Paediatrics, University of Melbourne, Royal Children’sHospital,
Parkville, Victoria; Michael Hayman, Depart-ment of Neurology,
Royal Children’s Hospital, and Mur-doch Children’s Research
Institute, Royal Children’sHospital, Parkville, Victoria; Victoria
Rodriguez-Casero,Department of Neurology, Royal Children’s
Hospital,Parkville, Victoria; Gopi Subramanian, Paediatric
Neurol-ogy Unit, John Hunter Children’s Hospital, New
LambtonHeights, NSW; Richard Webster, TY Nelson Department of
Neurology and Neurosurgery, The Children’s Hospitalat Westmead,
Sydney, NSW, Australia. Lynette G. Sadleir,Department of
Paediatrics, School of Medicine and HealthSciences, University of
Otago, Wellington, New Zealand.
8 Developmental Medicine & Child
Neurology 2016
-
8/16/2019 r1 DMCN 13163 Review
12/12
Author Query Form
Journal: DMCN Article: 13163
Dear Author,
During the copy-editing of your paper, the following queries
arose. Please respond to these by marking up yourproofs with the
necessary changes/additions. Please write your answers on the query
sheet if there is insufficient space on the page proofs.
Please write clearly and follow the conventions shown on the
attached corrections sheet.If returning the proof by fax do not
write too close to the paper’s edge. Please remember that illegible
mark-upsmay delay publication.
Many thanks for your assistance.
Query reference Query Remarks
1 AUTHOR: Please confirm that given names (red) and
surnames/family names (green) have been identified
correctly.
2 AUTHOR: Please provide city location for the manufacturer
“Genotek
Inc”.
3 AUTHOR: References [8] and [10] are identical. Hence,
reference [10] isdeleted and rest of the references is renumbered.
Please check.
4 AUTHOR: Figure 1 has been saved at a low resolution of 173
dpi. Pleaseresupply at 600 dpi. Check required artwork
specifications at
http:// authorservices.wiley.com/bauthor/illustration.asp
5 AUTHOR: If you would like the figures in your article to
appear ascolour in print, please complete the Colour Work Agreement
form (including payment information) and post/courier to
Customer Services(OPI); otherwise, we will publish the figures in
colour for the online
version for free. The form can be requested from the
Production Editor at [email protected].