Embed Size (px)
Citation preview
R vd Berg3 Feb 2012
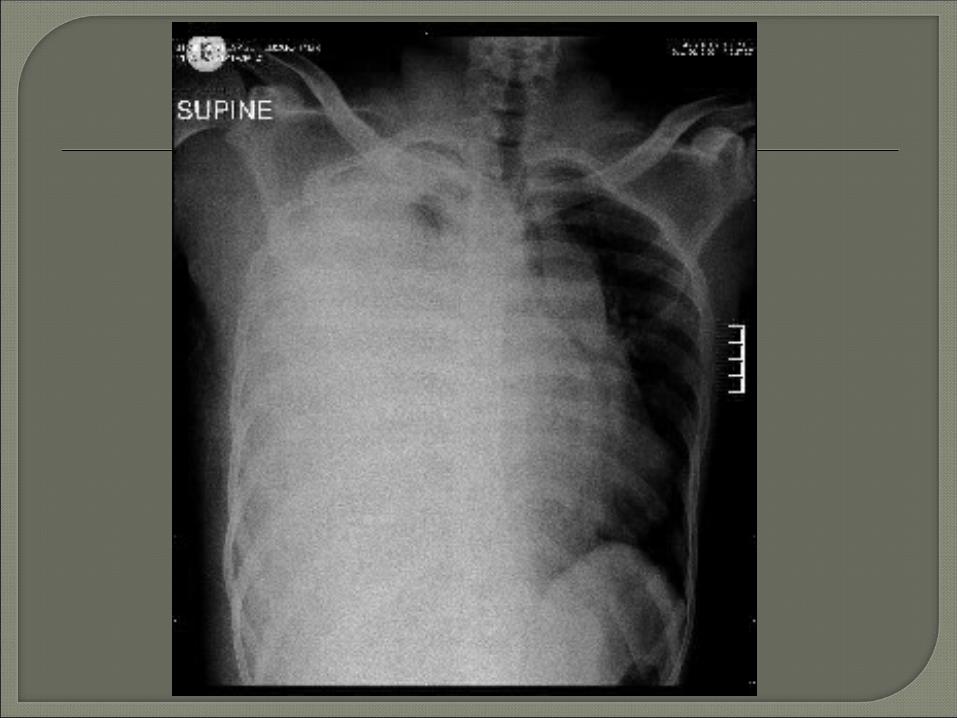
25 year old male HIV Seen 1/12 ago with a right pleural
effusion Started on TB-treatment Now presents with a mediastinal
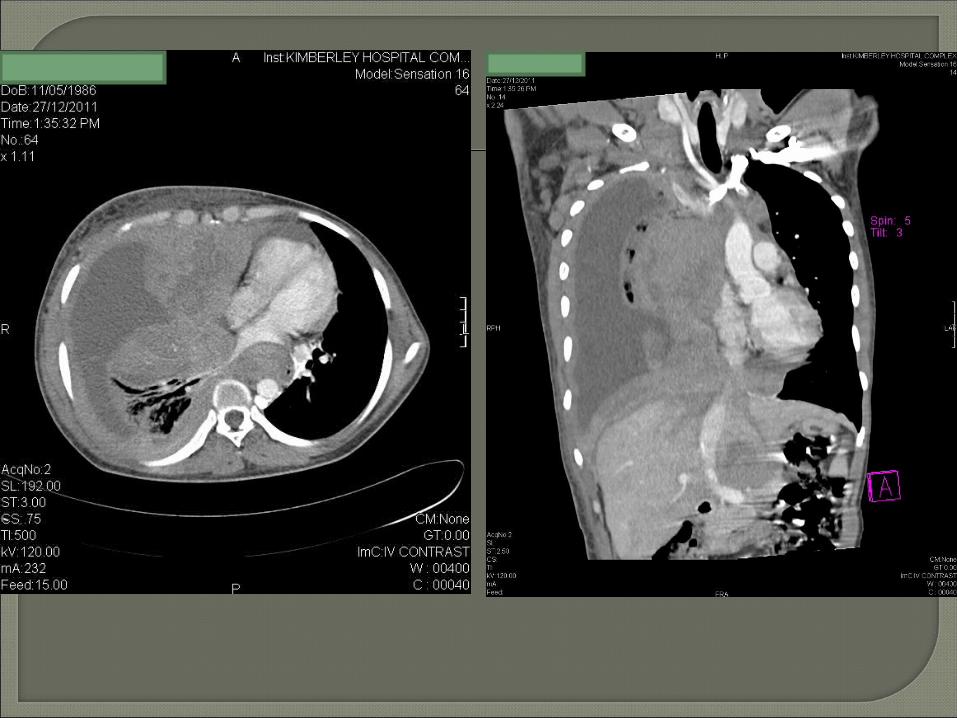
mass & right pleural effusion For CT chest ? Lymphoma
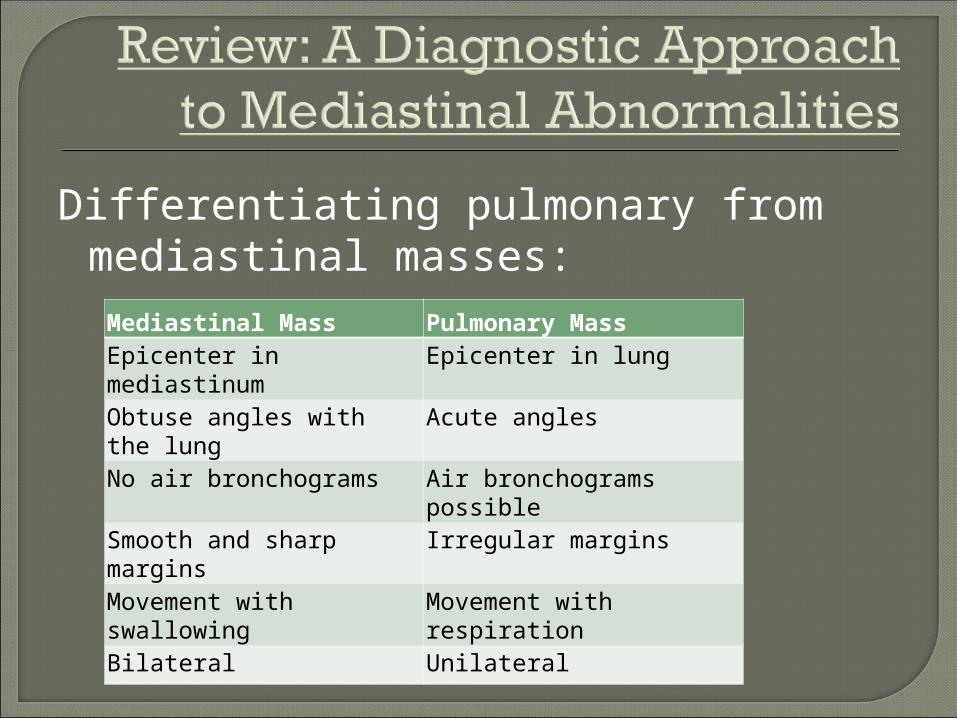
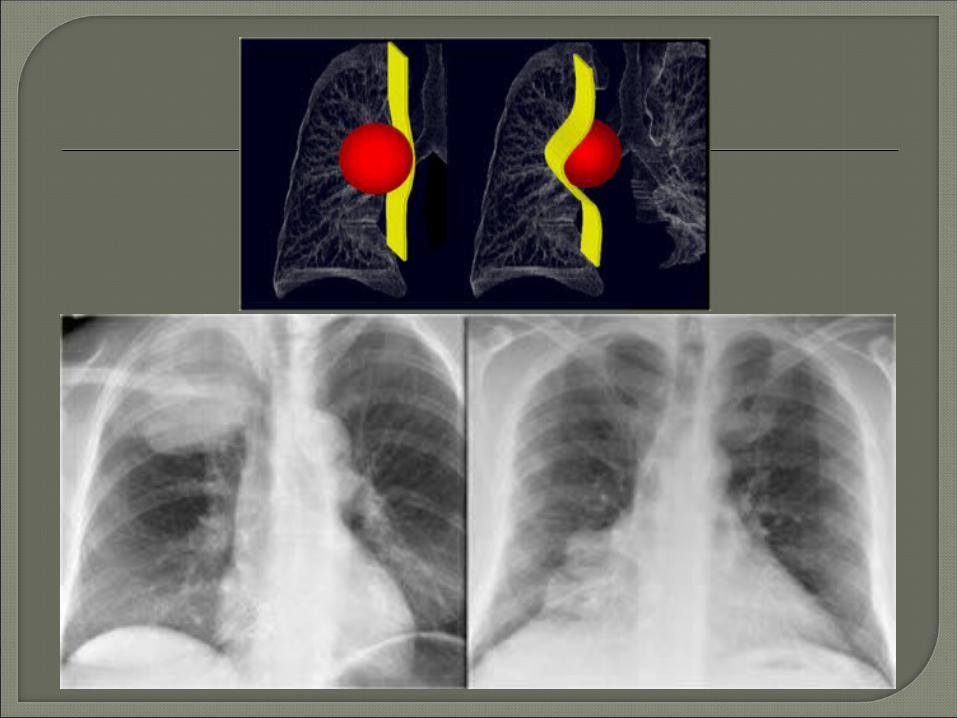
Differentiating pulmonary from mediastinal masses:
Mediastinal Mass Pulmonary MassEpicenter in mediastinum Epicenter in lungObtuse angles with the lung
Acute angles
No air bronchograms Air bronchograms possible
Smooth and sharp margins
Irregular margins
Movement with swallowing
Movement with respiration
Bilateral Unilateral
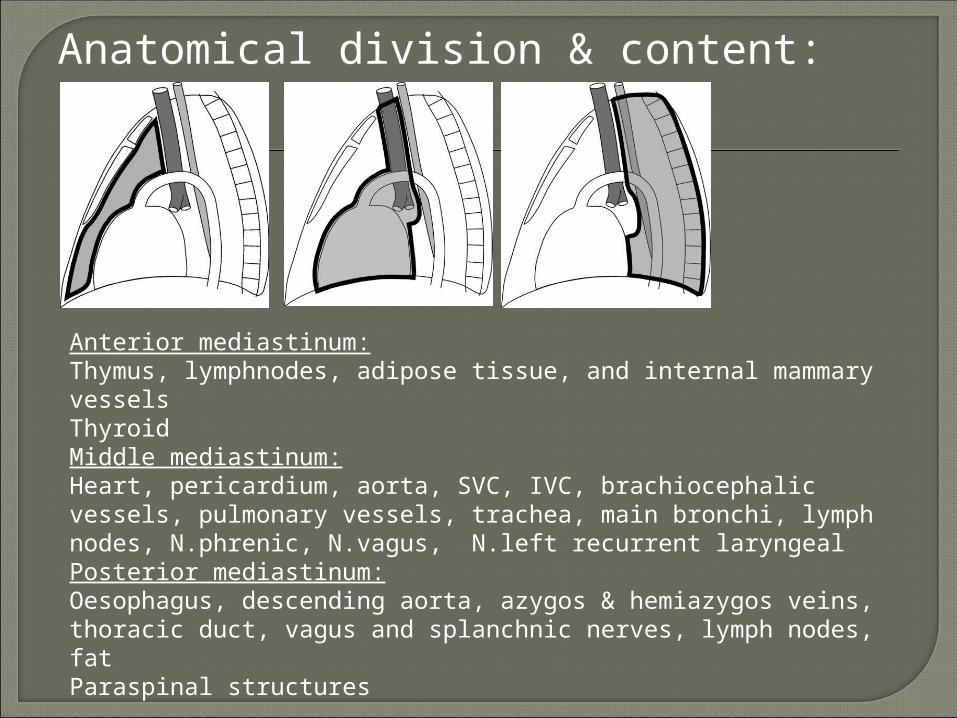
Anatomical division & content:
Anterior mediastinum:Thymus, lymphnodes, adipose tissue, and internal mammary vesselsThyroidMiddle mediastinum:Heart, pericardium, aorta, SVC, IVC, brachiocephalic vessels, pulmonary vessels, trachea, main bronchi, lymph nodes, N.phrenic, N.vagus, N.left recurrent laryngealPosterior mediastinum:Oesophagus, descending aorta, azygos & hemiazygos veins, thoracic duct, vagus and splanchnic nerves, lymph nodes, fatParaspinal structures
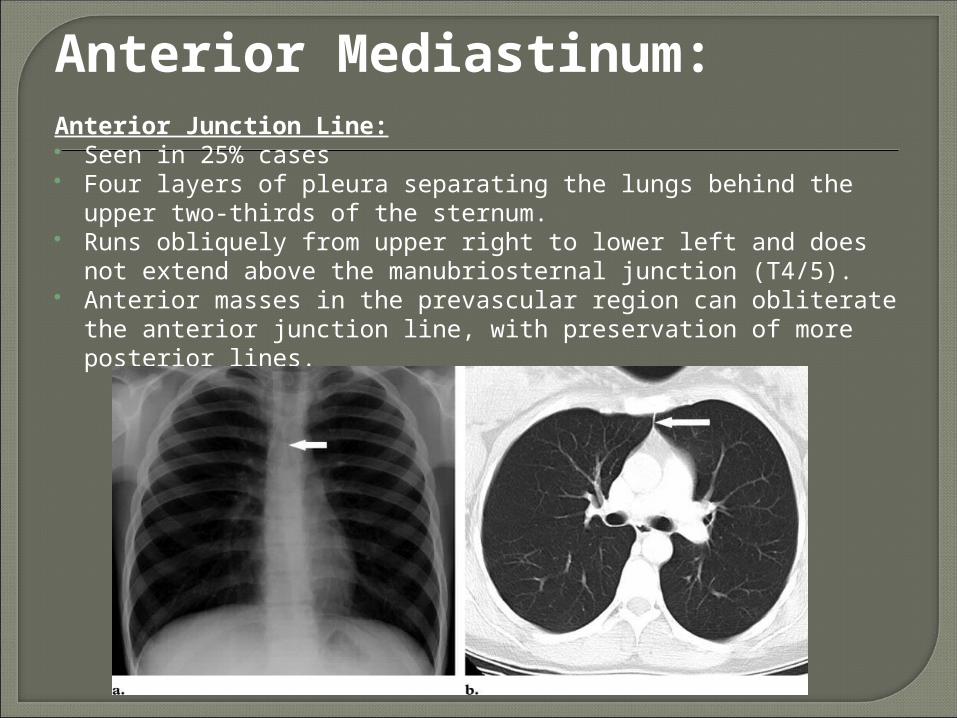
Anterior Mediastinum:Anterior Junction Line: Seen in 25% cases Four layers of pleura separating the lungs behind the upper
two-thirds of the sternum. Runs obliquely from upper right to lower left and does not
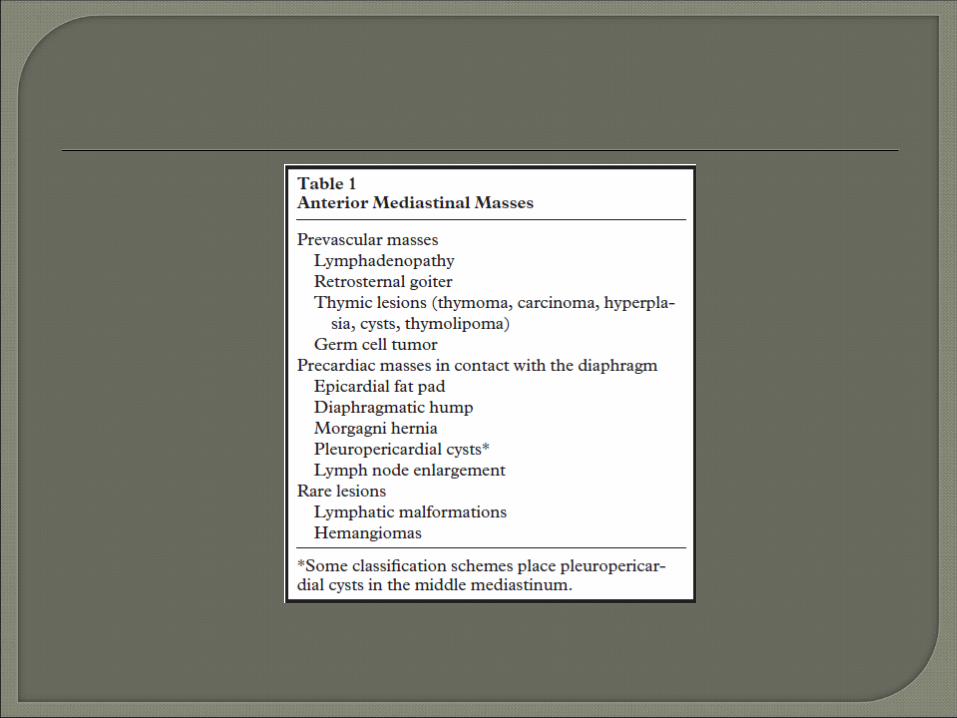
extend above the manubriosternal junction (T4/5). Anterior masses in the prevascular region can obliterate the
anterior junction line, with preservation of more posterior lines.
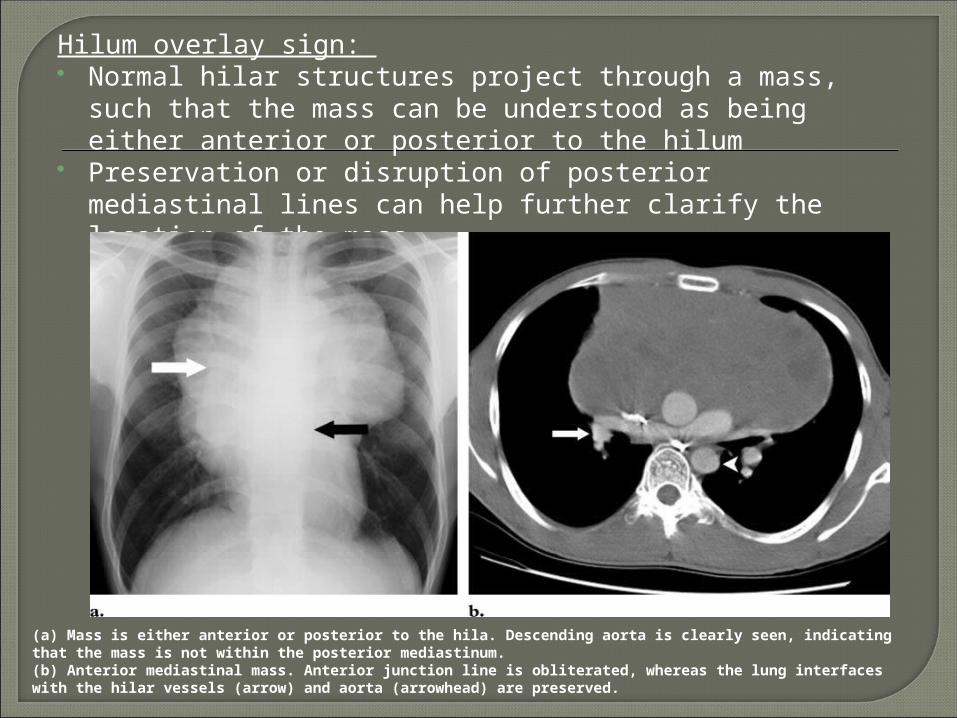
Hilum overlay sign: Normal hilar structures project through a mass, such that
the mass can be understood as being either anterior or posterior to the hilum
Preservation or disruption of posterior mediastinal lines can help further clarify the location of the mass
(a) Mass is either anterior or posterior to the hila. Descending aorta is clearly seen, indicating that the mass is not within the posterior mediastinum.(b) Anterior mediastinal mass. Anterior junction line is obliterated, whereas the lung interfaces with the hilar vessels (arrow) and aorta (arrowhead) are preserved.
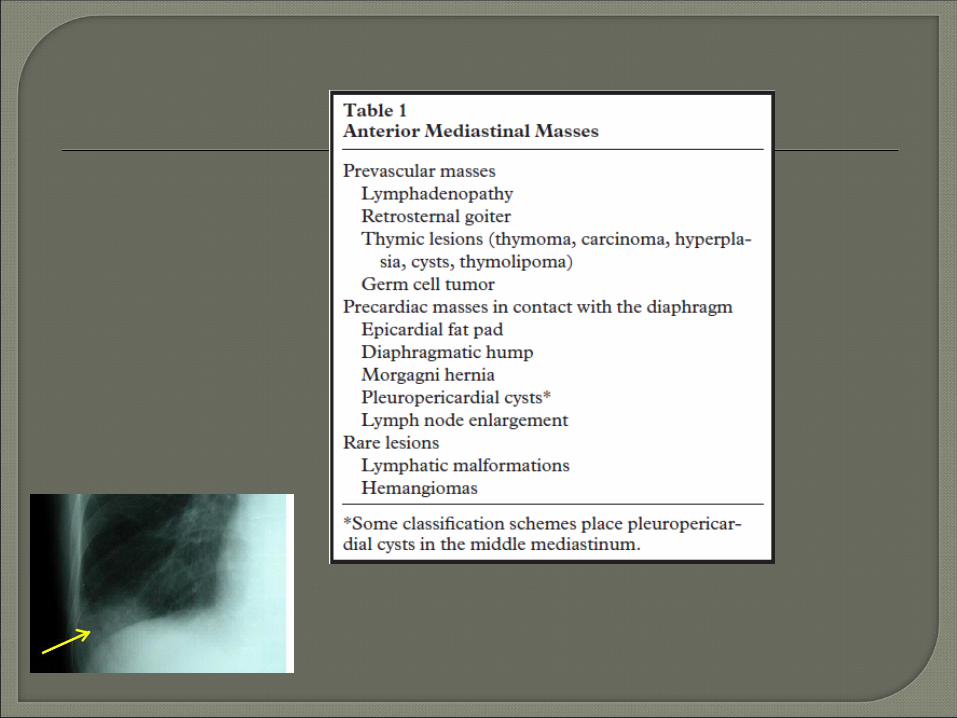
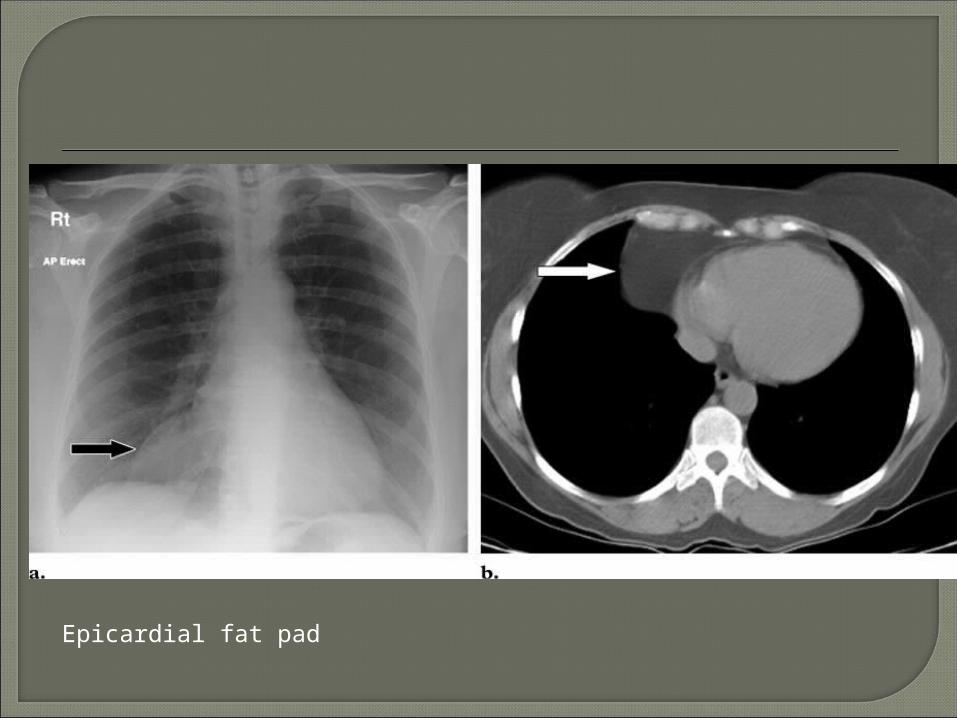
Epicardial fat pad
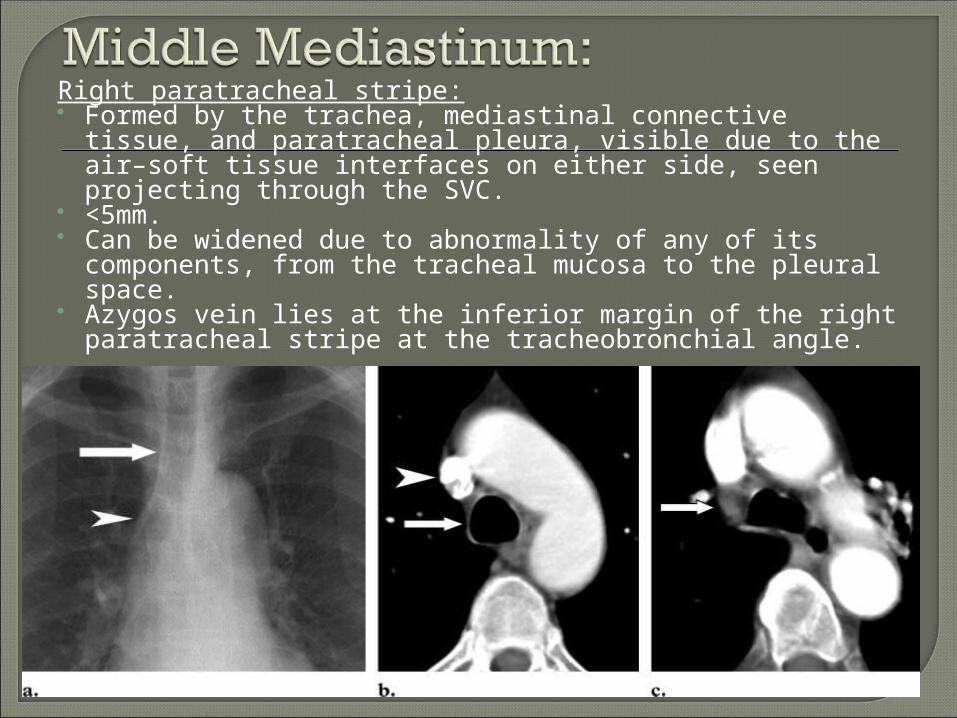
Right paratracheal stripe: Formed by the trachea, mediastinal connective tissue,
and paratracheal pleura, visible due to the air–soft tissue interfaces on either side, seen projecting through the SVC.
<5mm. Can be widened due to abnormality of any of its
components, from the tracheal mucosa to the pleural space.
Azygos vein lies at the inferior margin of the right paratracheal stripe at the tracheobronchial angle.
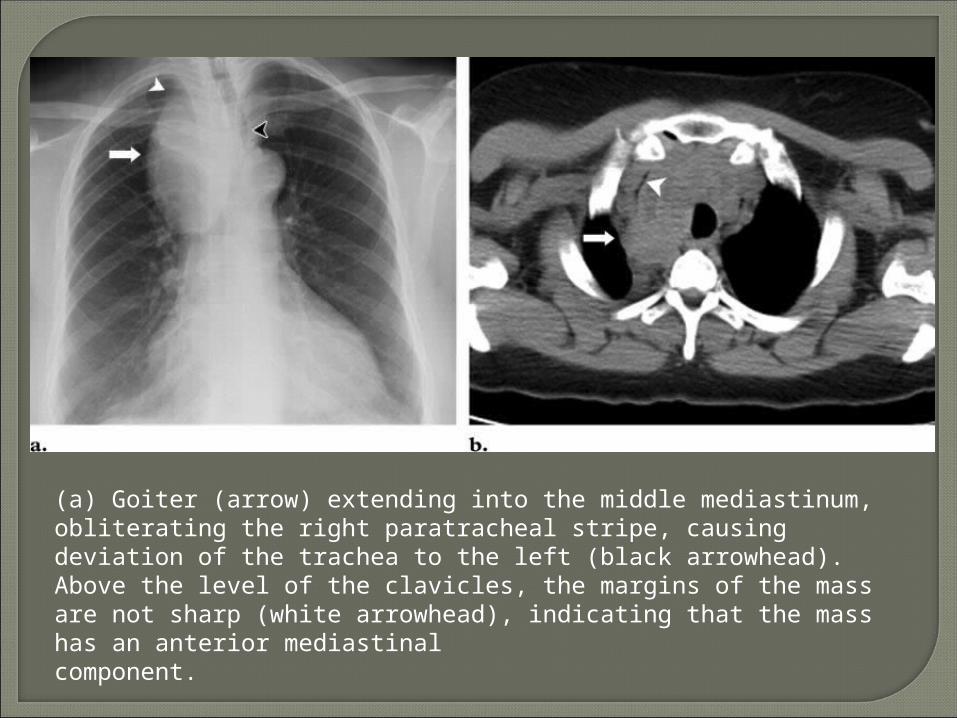
(a) Goiter (arrow) extending into the middle mediastinum, obliterating the right paratracheal stripe, causing deviation of the trachea to the left (black arrowhead). Above the level of the clavicles, the margins of the mass are not sharp (white arrowhead), indicating that the mass has an anterior mediastinalcomponent.
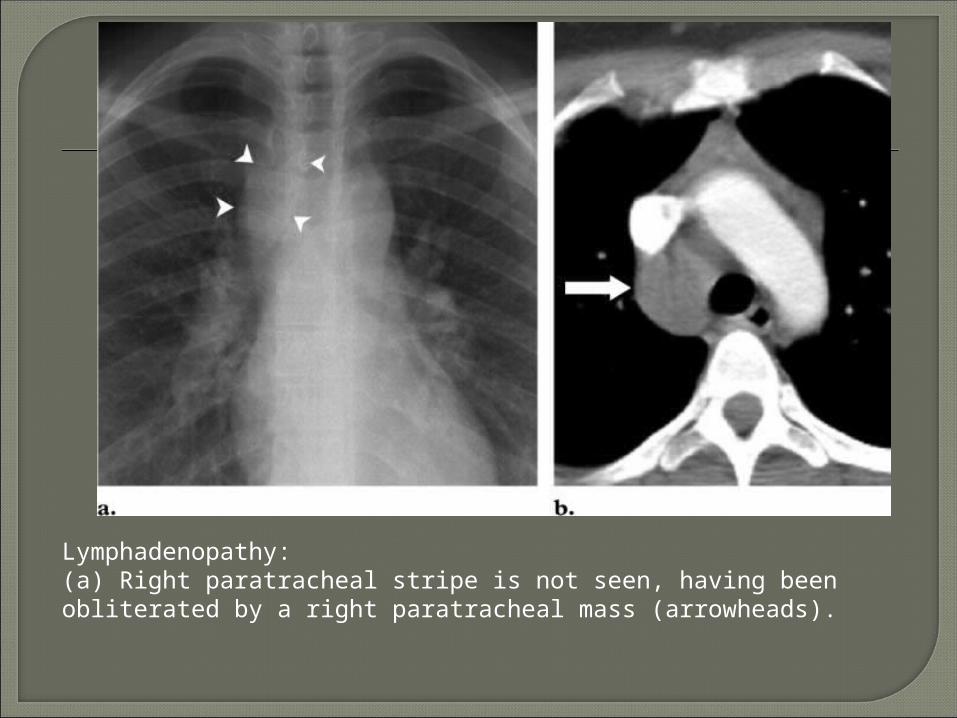
Lymphadenopathy:(a) Right paratracheal stripe is not seen, having been obliterated by a right paratracheal mass (arrowheads).
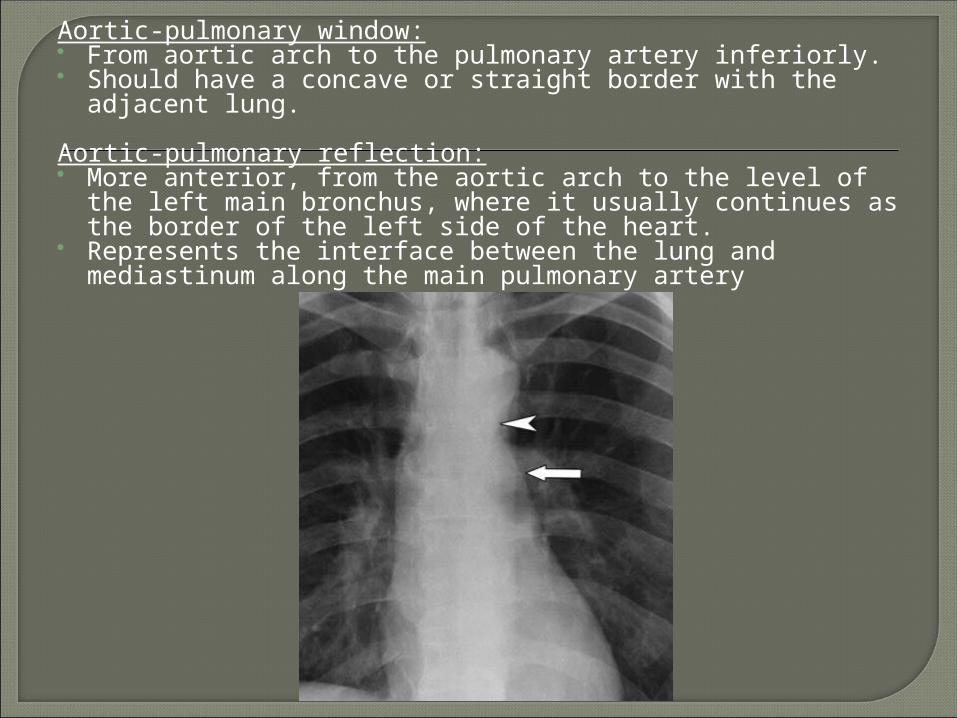
Aortic-pulmonary window: From aortic arch to the pulmonary artery inferiorly. Should have a concave or straight border with the adjacent
lung.
Aortic-pulmonary reflection: More anterior, from the aortic arch to the level of the left
main bronchus, where it usually continues as the border of the left side of the heart.
Represents the interface between the lung and mediastinum along the main pulmonary artery
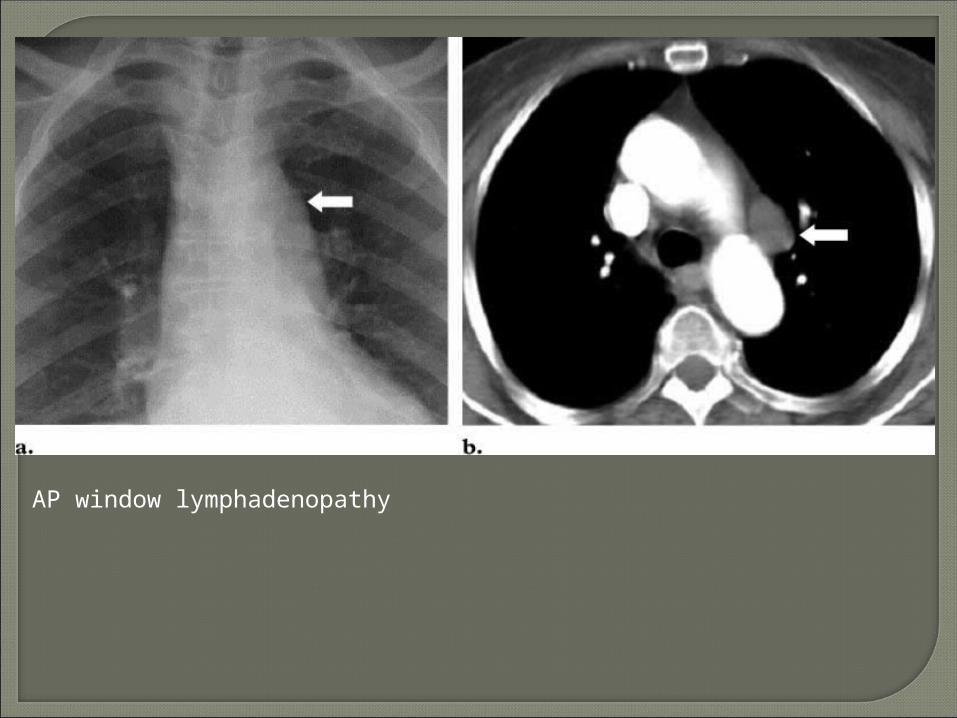
AP window lymphadenopathy

Aneurysm of the aortic arch
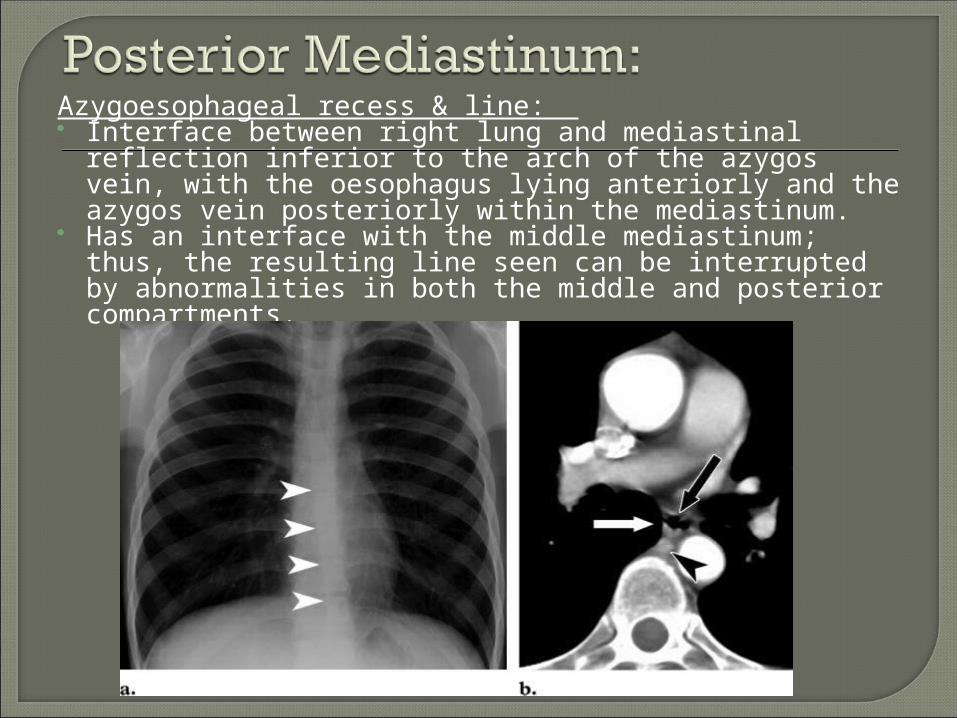
Azygoesophageal recess & line: Interface between right lung and mediastinal reflection
inferior to the arch of the azygos vein, with the oesophagus lying anteriorly and the azygos vein posteriorly within the mediastinum.
Has an interface with the middle mediastinum; thus, the resulting line seen can be interrupted by abnormalities in both the middle and posterior compartments.
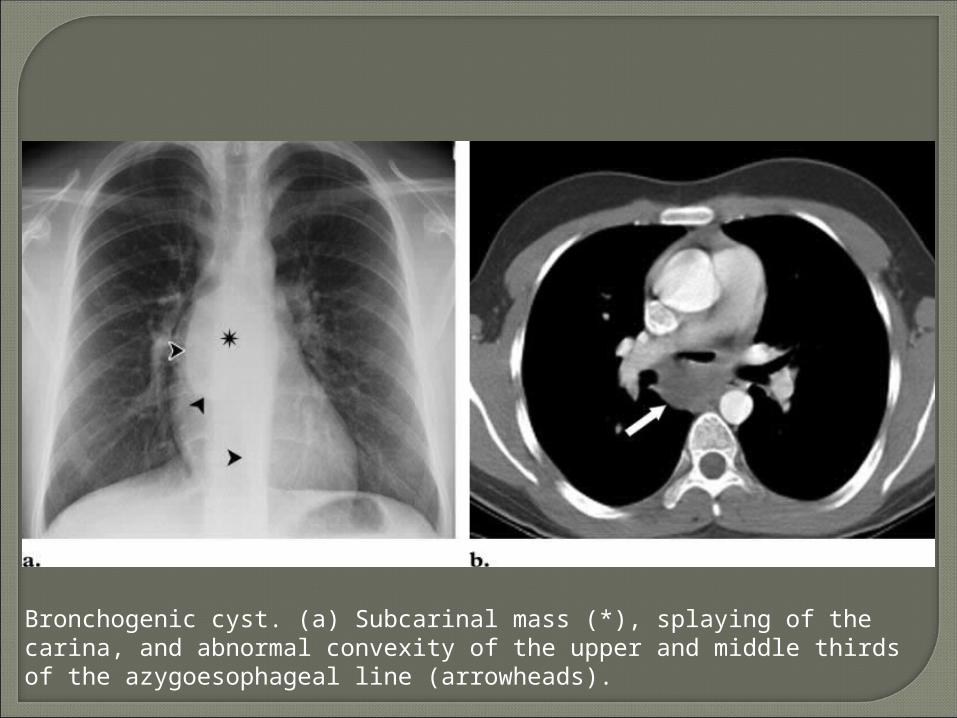
Bronchogenic cyst. (a) Subcarinal mass (*), splaying of the carina, and abnormal convexity of the upper and middle thirds of the azygoesophageal line (arrowheads).
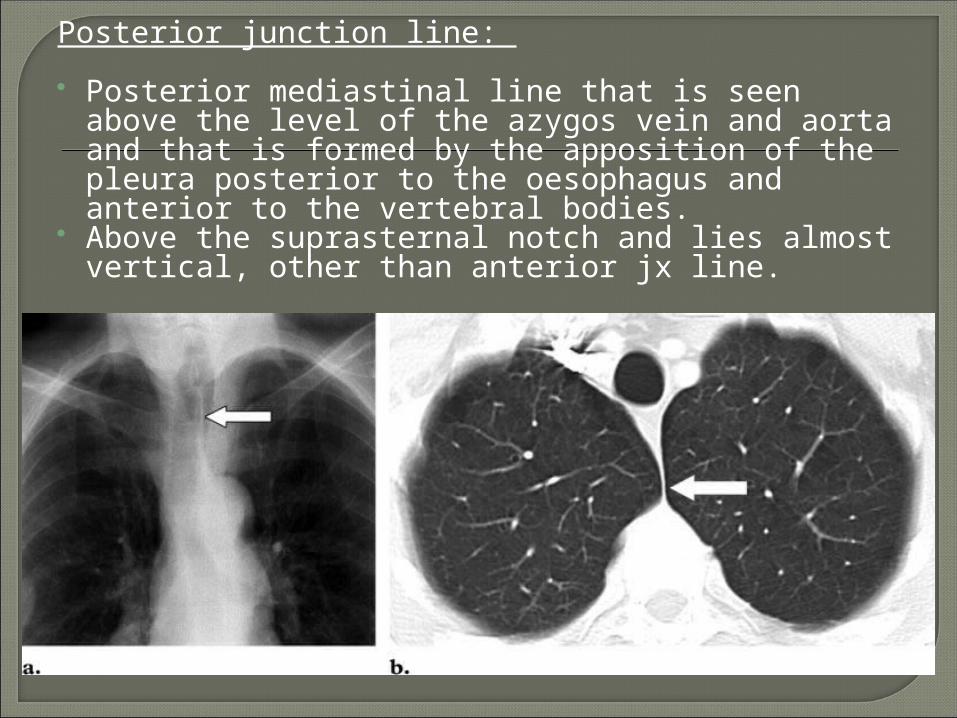
Posterior junction line:
Posterior mediastinal line that is seen above the level of the azygos vein and aorta and that is formed by the apposition of the pleura posterior to the oesophagus and anterior to the vertebral bodies.
Above the suprasternal notch and lies almost vertical, other than anterior jx line.
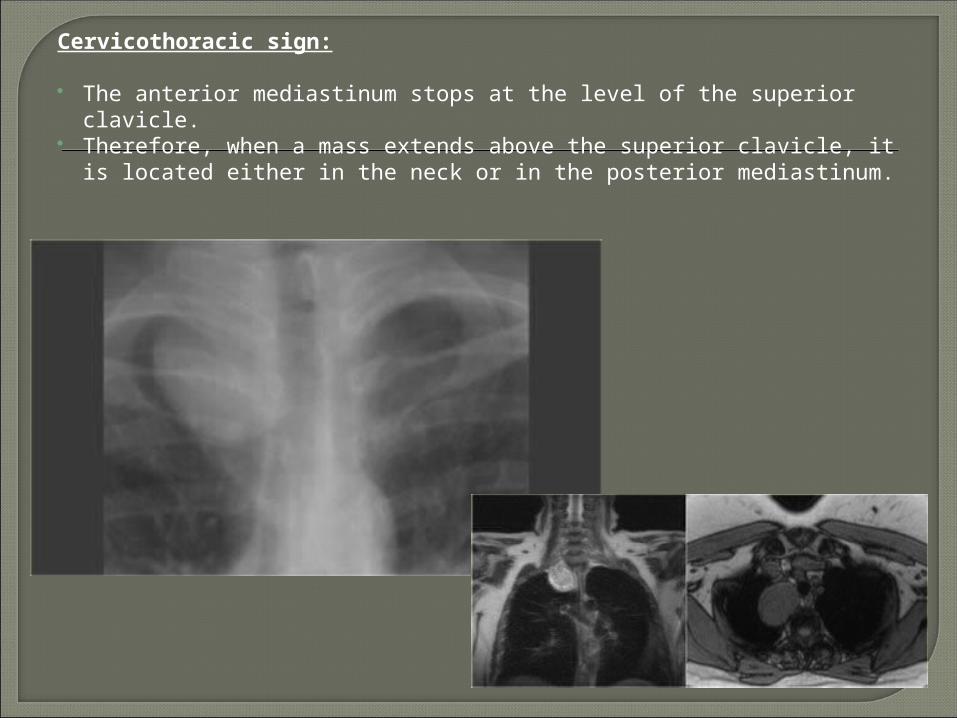
Cervicothoracic sign:
The anterior mediastinum stops at the level of the superior clavicle.
Therefore, when a mass extends above the superior clavicle, it is located either in the neck or in the posterior mediastinum.
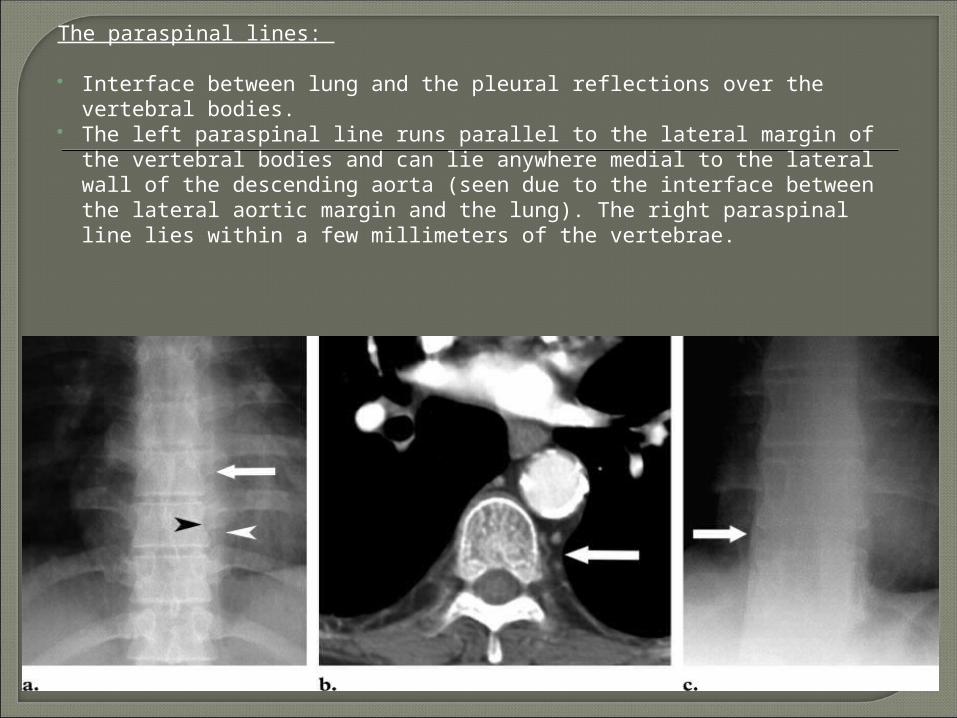
The paraspinal lines:
Interface between lung and the pleural reflections over the vertebral bodies.
The left paraspinal line runs parallel to the lateral margin of the vertebral bodies and can lie anywhere medial to the lateral wall of the descending aorta (seen due to the interface between the lateral aortic margin and the lung). The right paraspinal line lies within a few millimeters of the vertebrae.
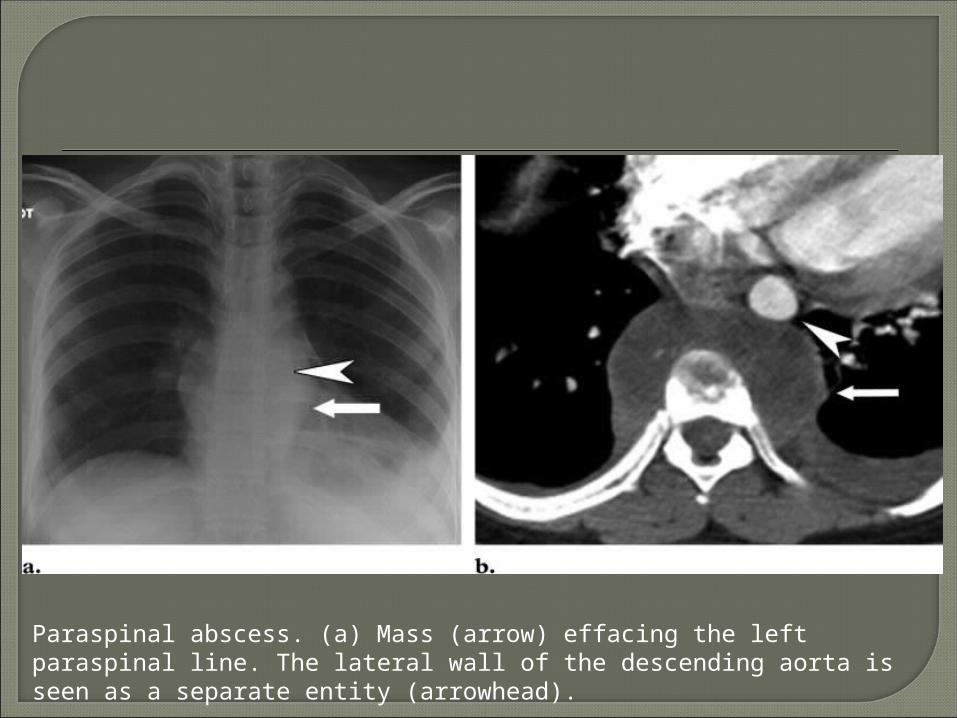
Paraspinal abscess. (a) Mass (arrow) effacing the left paraspinal line. The lateral wall of the descending aorta is seen as a separate entity (arrowhead).
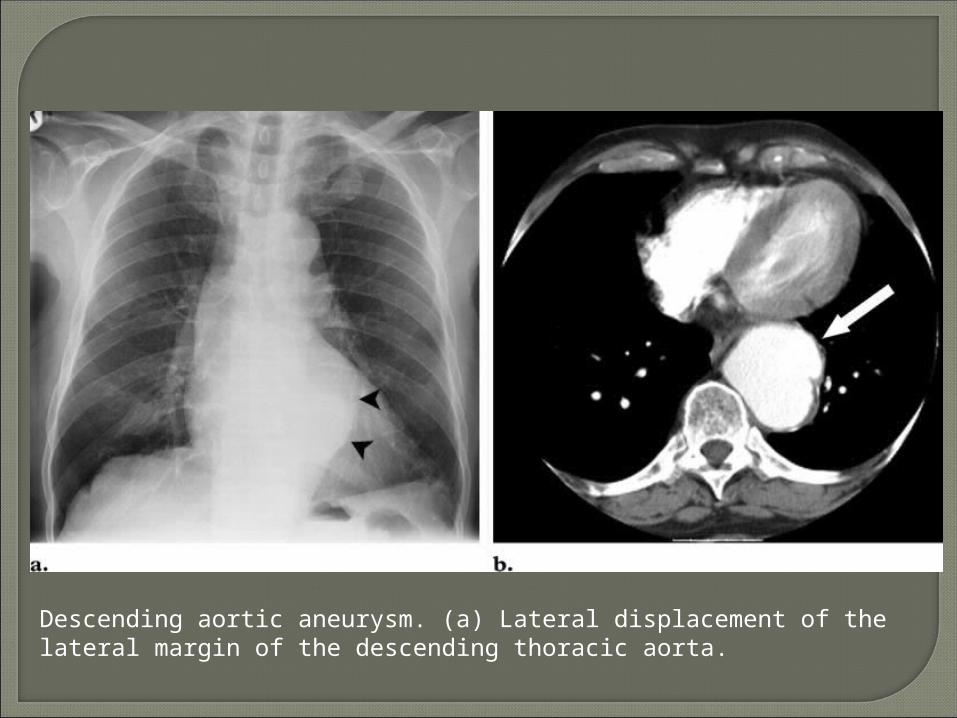
Descending aortic aneurysm. (a) Lateral displacement of the lateral margin of the descending thoracic aorta.
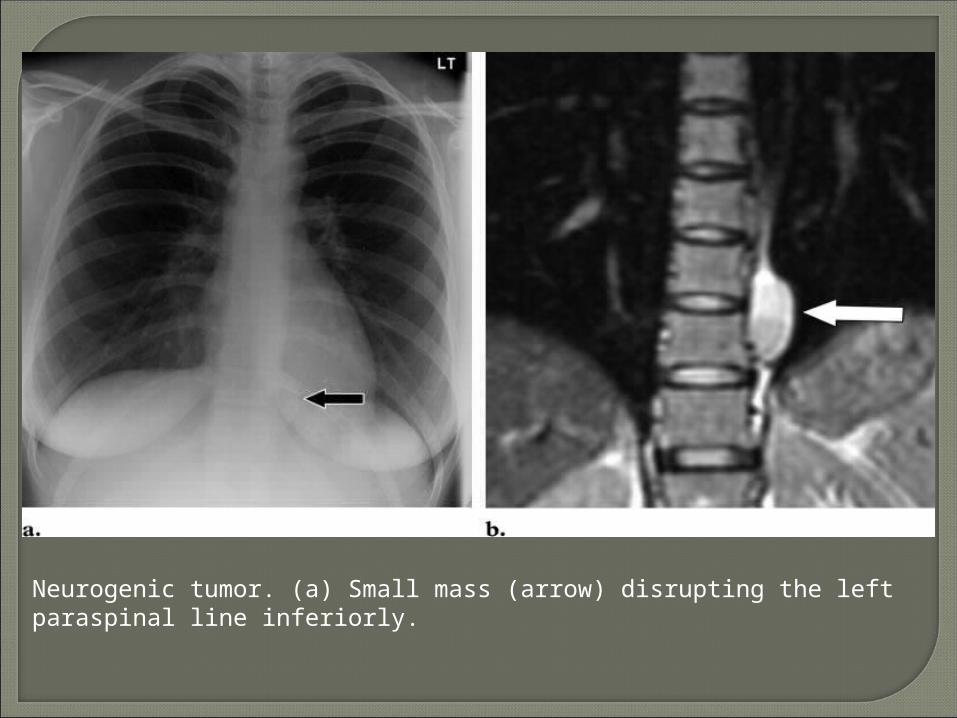
Neurogenic tumor. (a) Small mass (arrow) disrupting the left paraspinal line inferiorly.
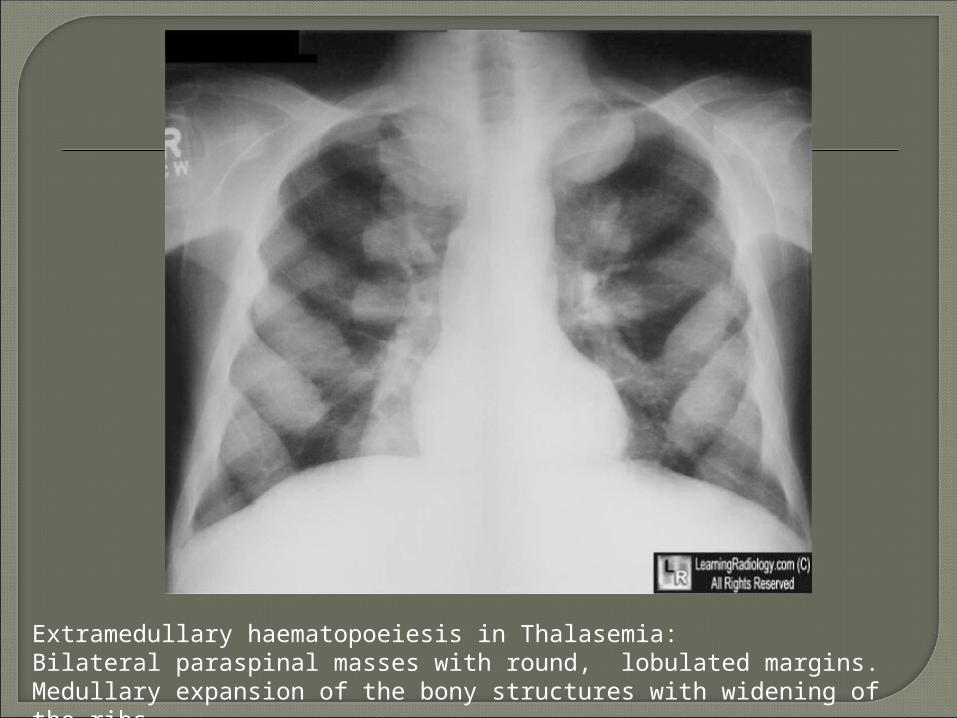
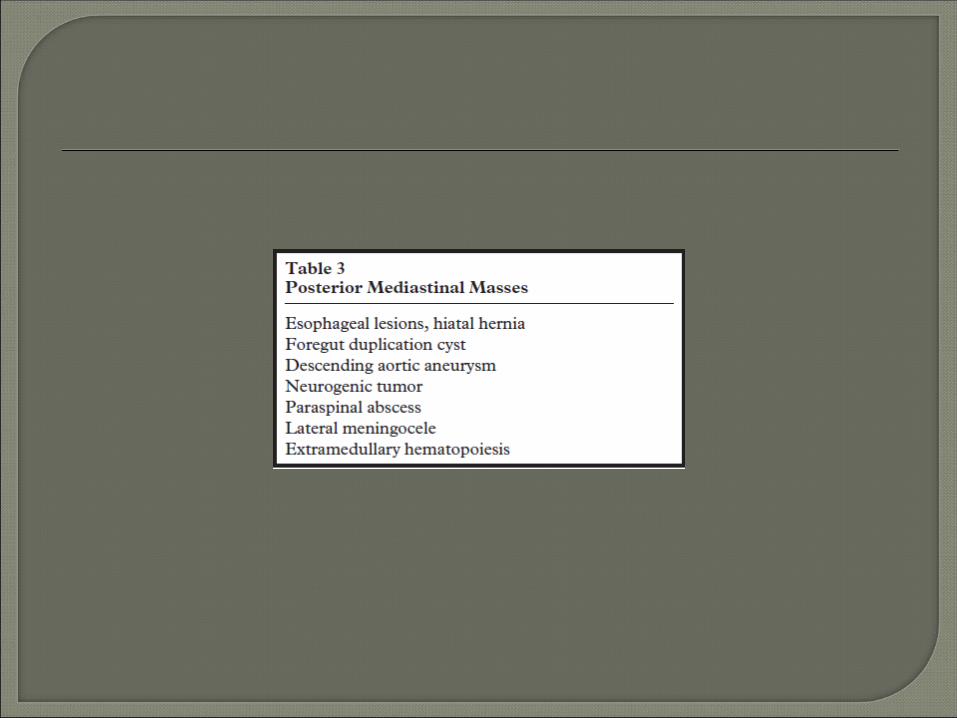
Extramedullary haematopoeiesis in Thalasemia:Bilateral paraspinal masses with round, lobulated margins.Medullary expansion of the bony structures with widening of the ribs.
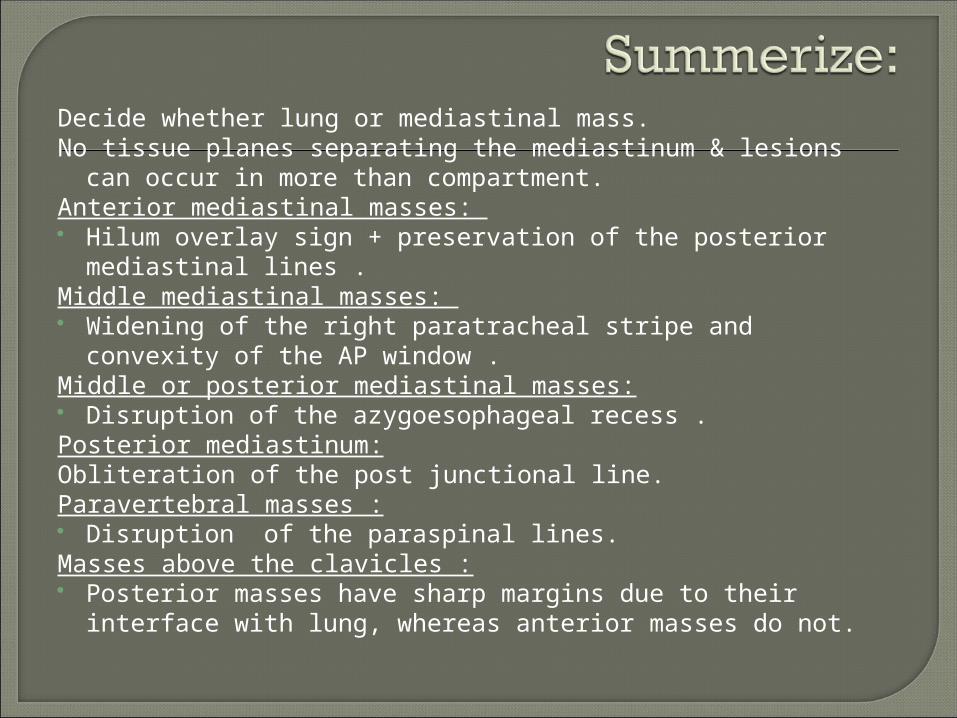
Decide whether lung or mediastinal mass.No tissue planes separating the mediastinum & lesions can
occur in more than compartment.Anterior mediastinal masses: Hilum overlay sign + preservation of the posterior mediastinal
lines . Middle mediastinal masses: Widening of the right paratracheal stripe and convexity of the
AP window .Middle or posterior mediastinal masses: Disruption of the azygoesophageal recess . Posterior mediastinum:Obliteration of the post junctional line.Paravertebral masses : Disruption of the paraspinal lines.Masses above the clavicles : Posterior masses have sharp margins due to their interface
with lung, whereas anterior masses do not.
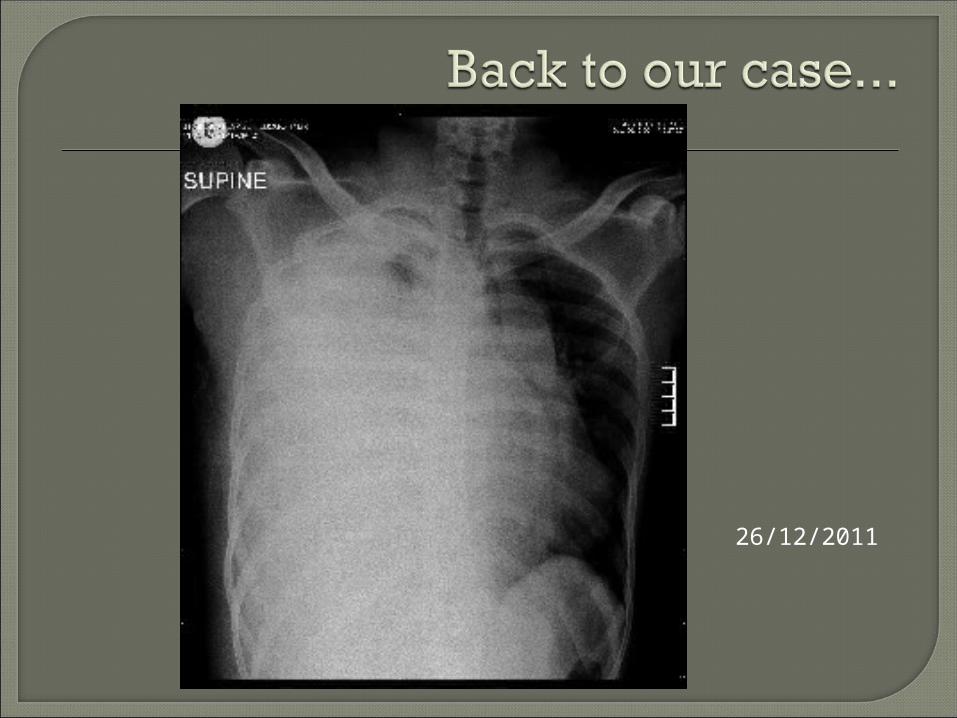
26/12/2011

14/11/2011 (42 days earlier)
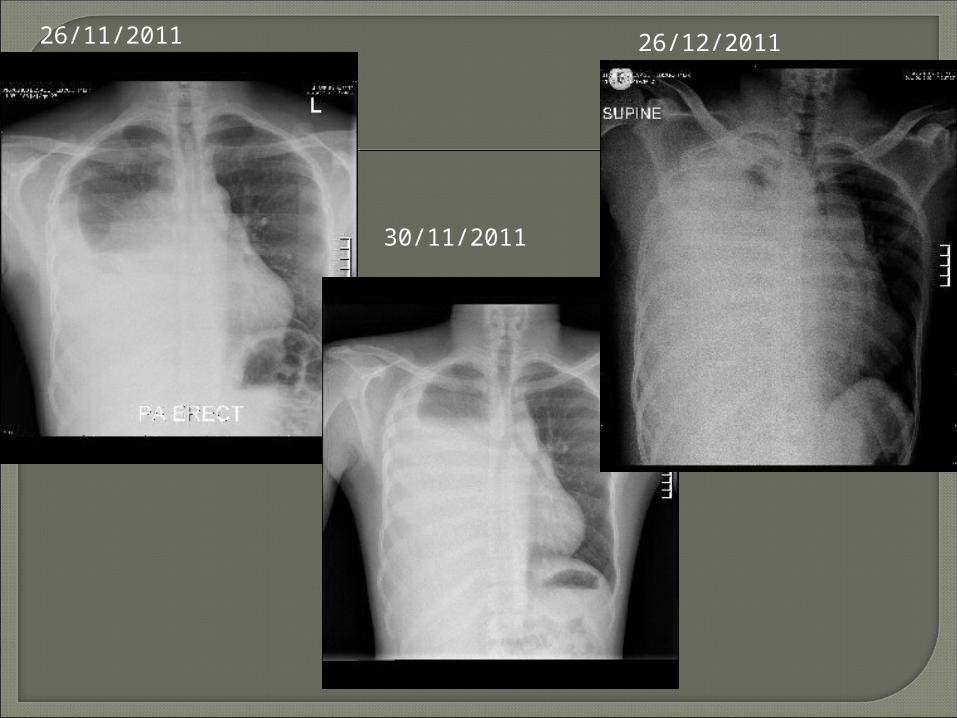
26/11/2011
30/11/2011
26/12/2011
A Diagnostic Approach to Mediastinal Abnormalities, Whitten CR et al, Radiographics, May 2007, p.657-671
Mediastinal Masses : localize and characterize, Bhalla S, Hazewinkel M and Smithuis R, 2007, www.radiologyassistant.nl
Some radiographs from www.learningradiology.com
Primer of Diagnostic Imaging, Weissleder, et al, 4th ed, 2007.