Embed Size (px)
Citation preview
R. Siebert
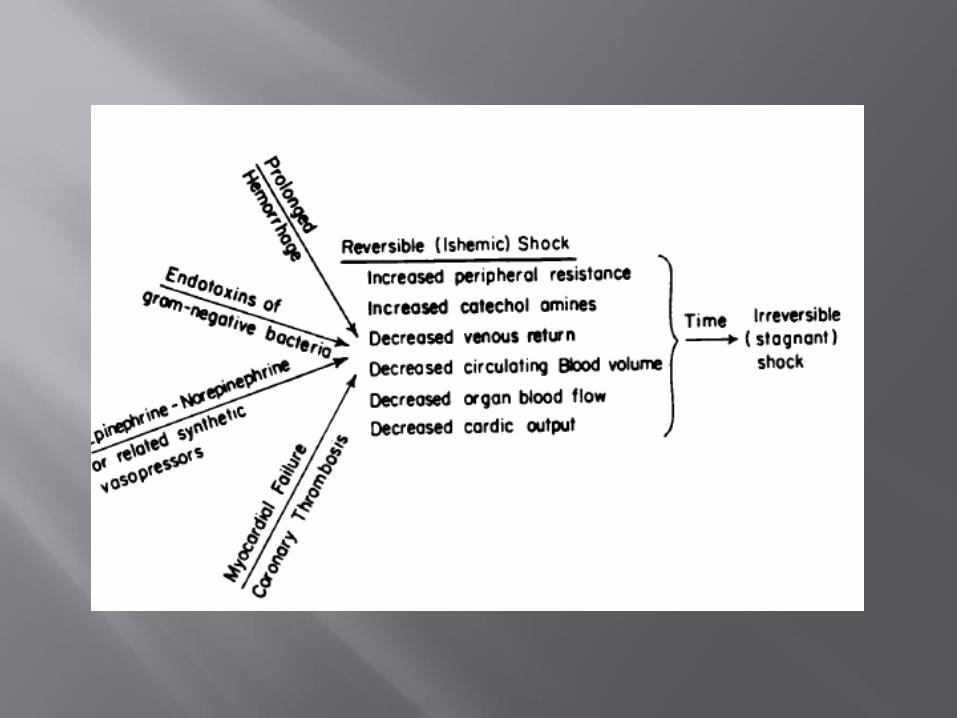
Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure and perfusion with progressive organ failure and death despite any heroic attempts to resuscitate the patient.
Pre-terminal event
Made retrospectively – end result in all forms of shock
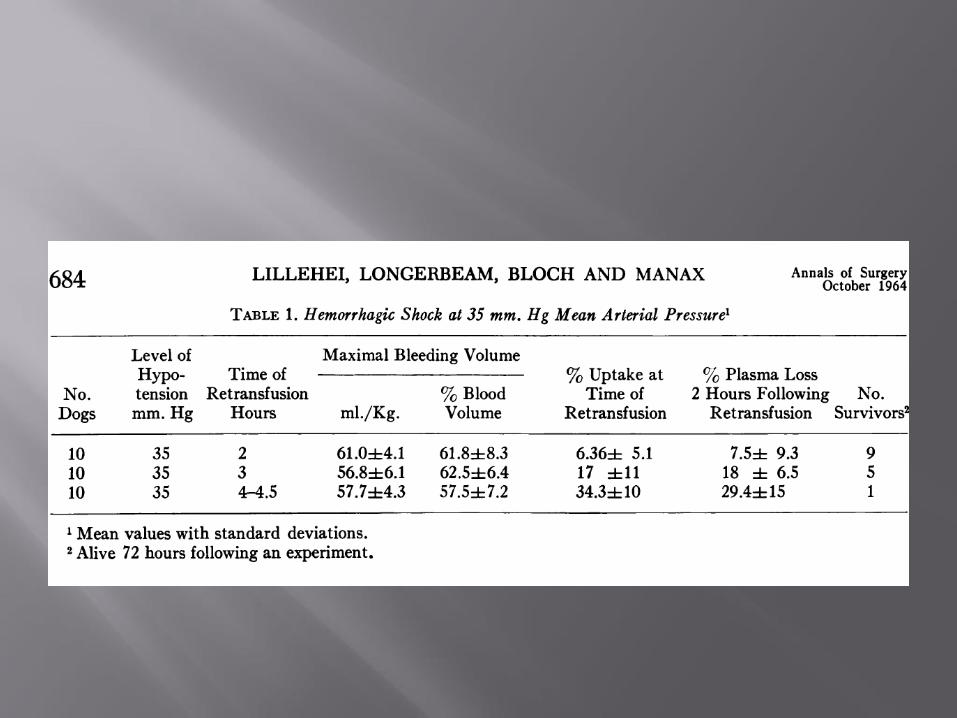
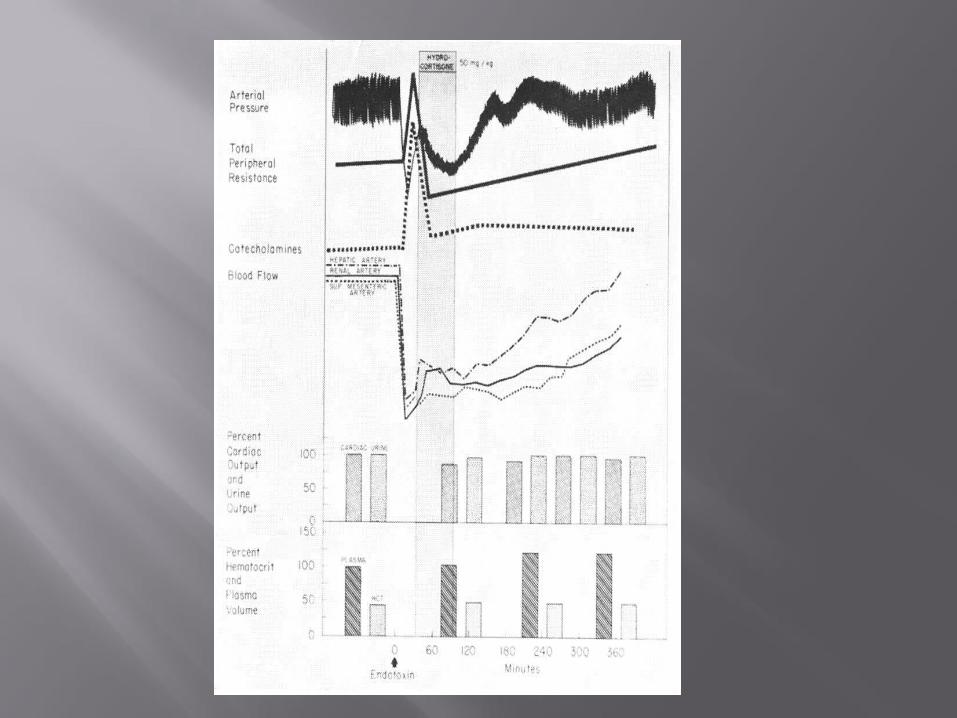
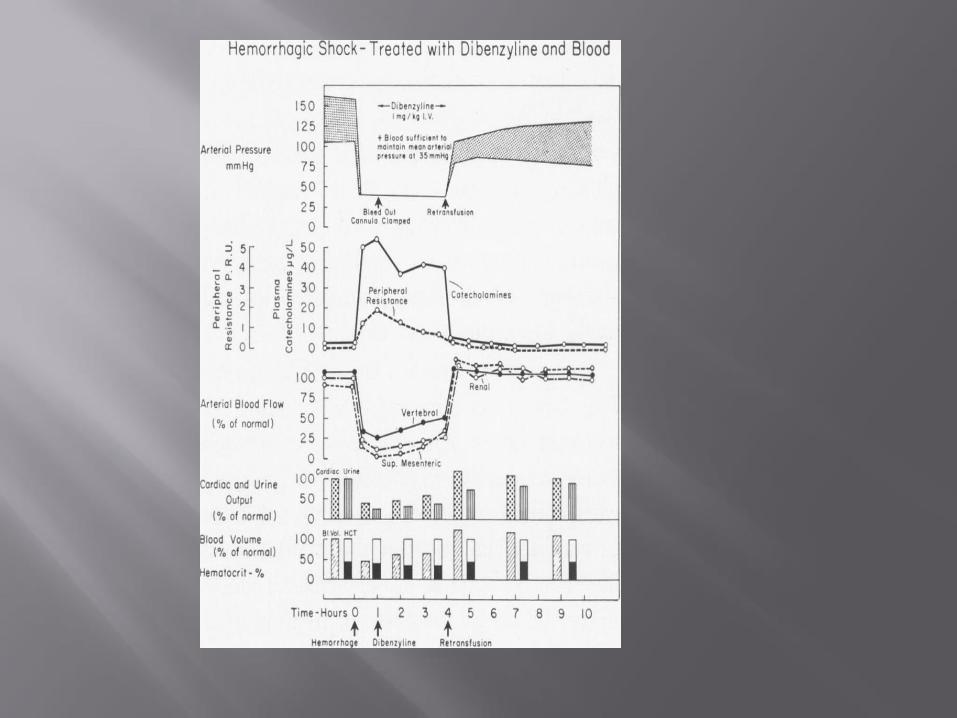
Classical article – The nature of irreversible shock – Lillehei et el – Annals of Surgery , October 1964
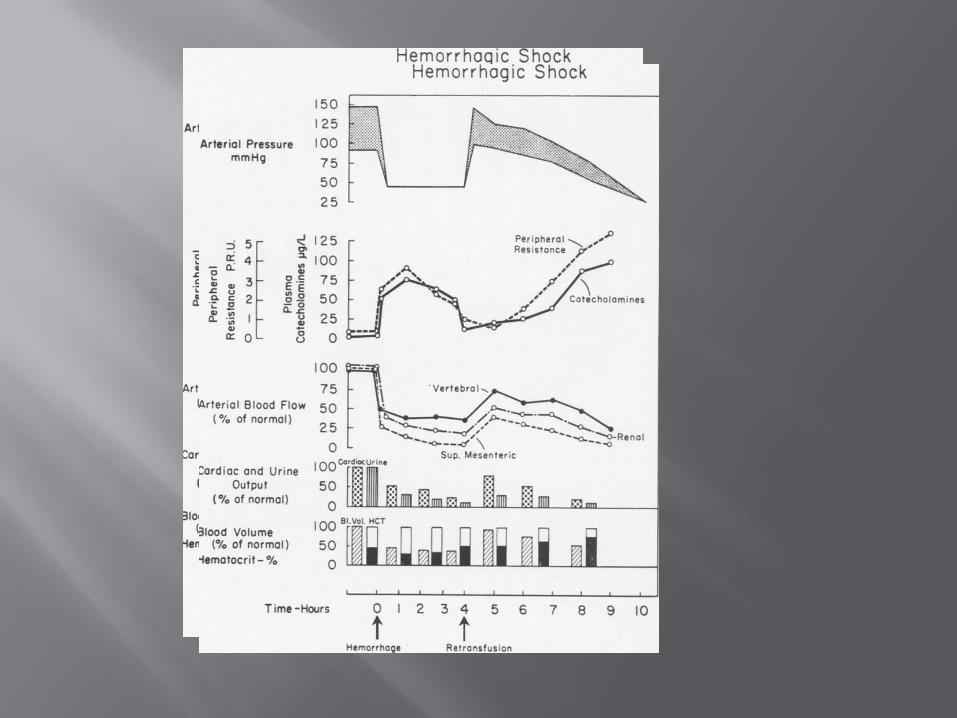
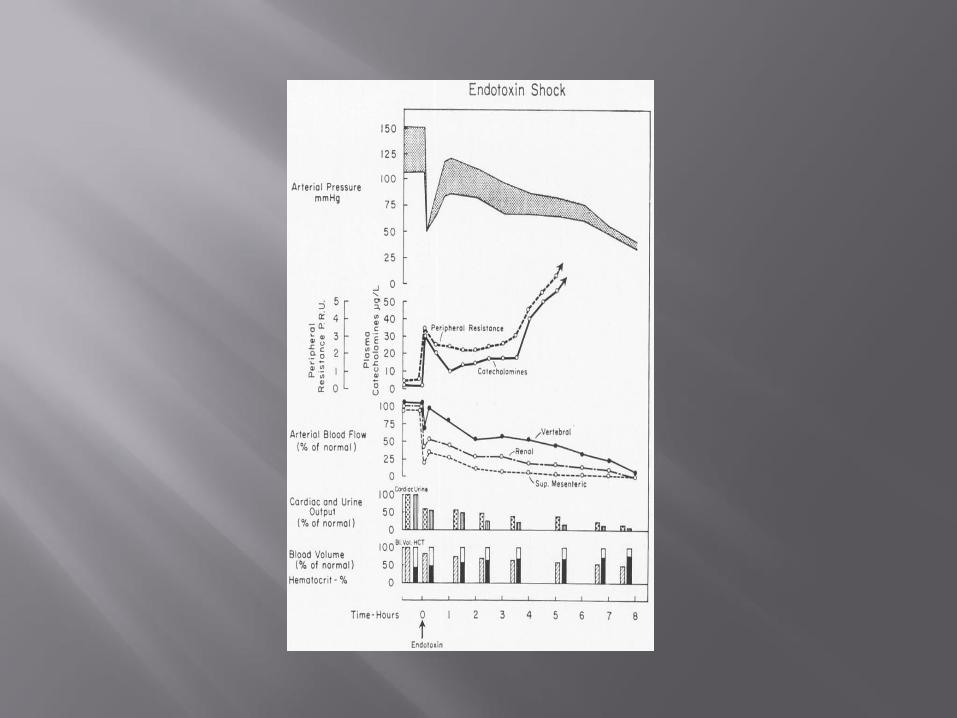
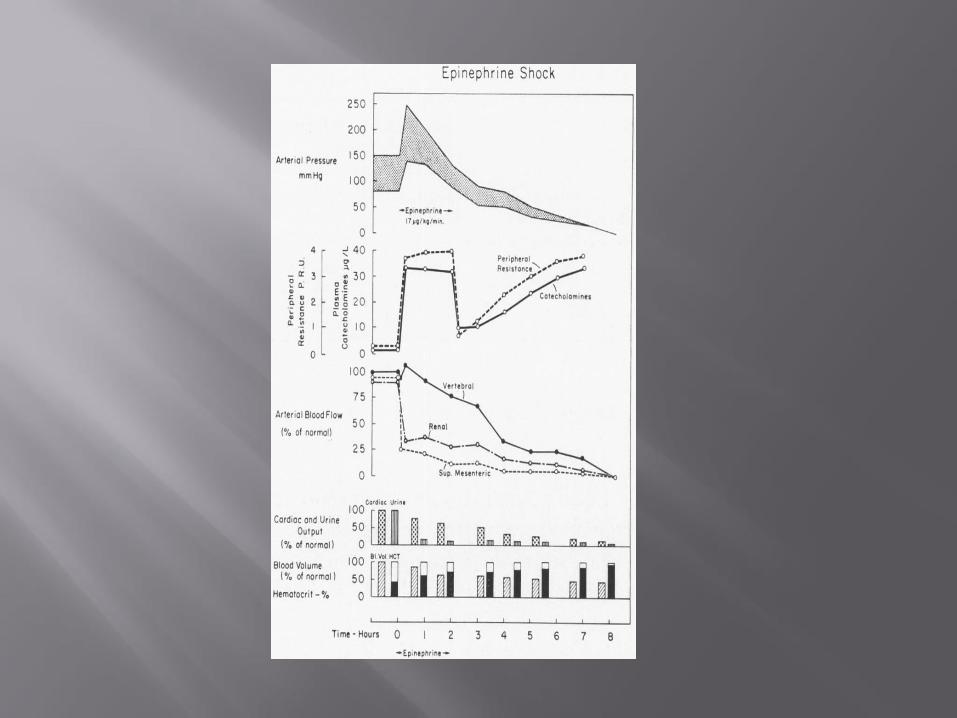
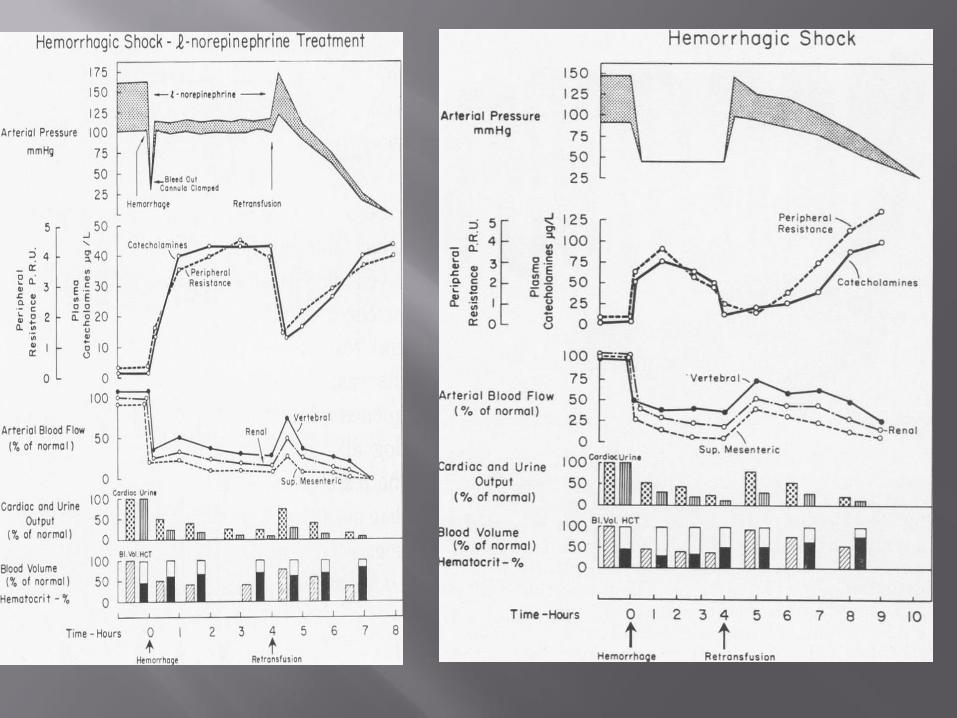
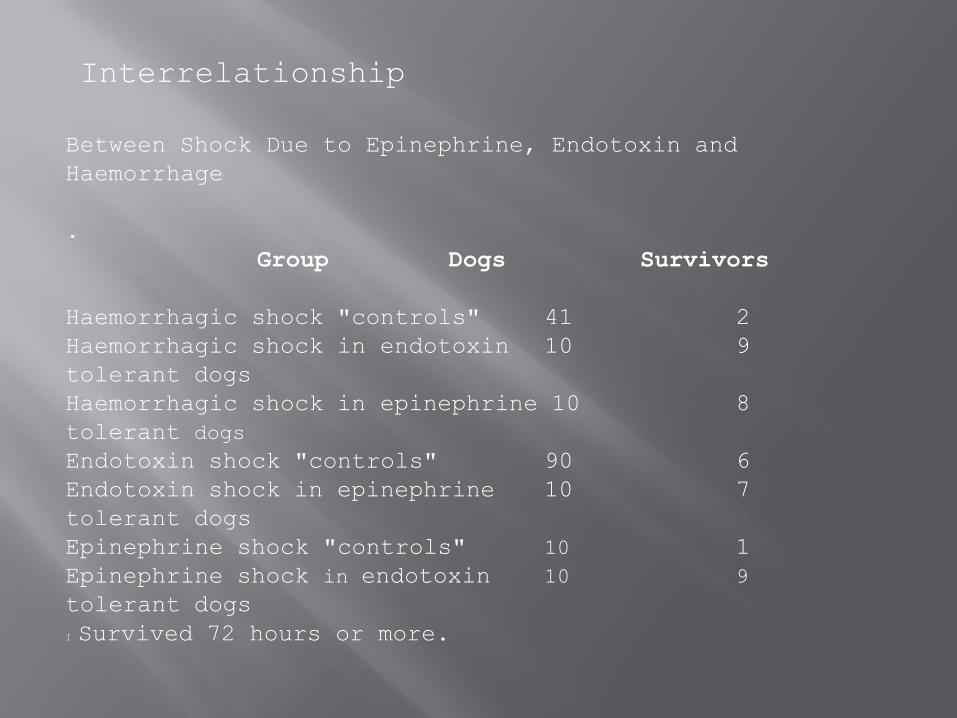
Interrelationship
Between Shock Due to Epinephrine, Endotoxin and
Haemorrhage
.
Group Dogs Survivors
Haemorrhagic shock "controls" 41 2
Haemorrhagic shock in endotoxin 10 9
tolerant dogs
Haemorrhagic shock in epinephrine 10 8
tolerant dogs
Endotoxin shock "controls" 90 6
Endotoxin shock in epinephrine 10 7
tolerant dogs
Epinephrine shock "controls" 10 1
Epinephrine shock in endotoxin 10 9
tolerant dogs
I Survived 72 hours or more.
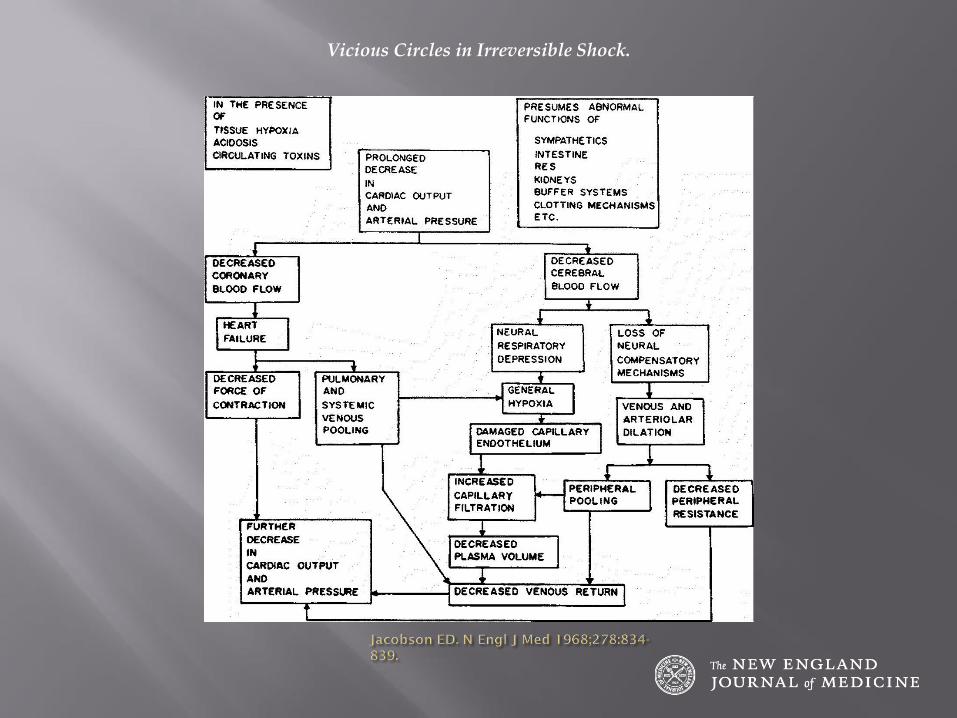
Vicious Circles in Irreversible Shock.
Impaired oxidative metabolism and oxygen debt (Crowel et al 1964) with increased venous C02 due to decreased CO2 clearance and increased formation of anaerobically derived acids
DO2 decreased and once maximum O2 extraction is reached anaerobic metabolism and hyperlactenemia suffice
ATP generation impaired by lack of oxygen , increased NO and peroxynitrate and superoxide
Inflammatory mediators ( TNF , Endotoxins , free radicals ) inhibit mitochondrial function
Tissue hypoxia : inhibition of cellular oxidative metabolism : cardiac , renal , splanchnic etc. and accumulation if intracellular CO2.
Abnormal mitochondrial function
Endothelial injury with micro vascular thrombosis , decreased capillary density and increased capillary permeability
Reperfusion injury with induction of apoptosis and necrosis of injured cells
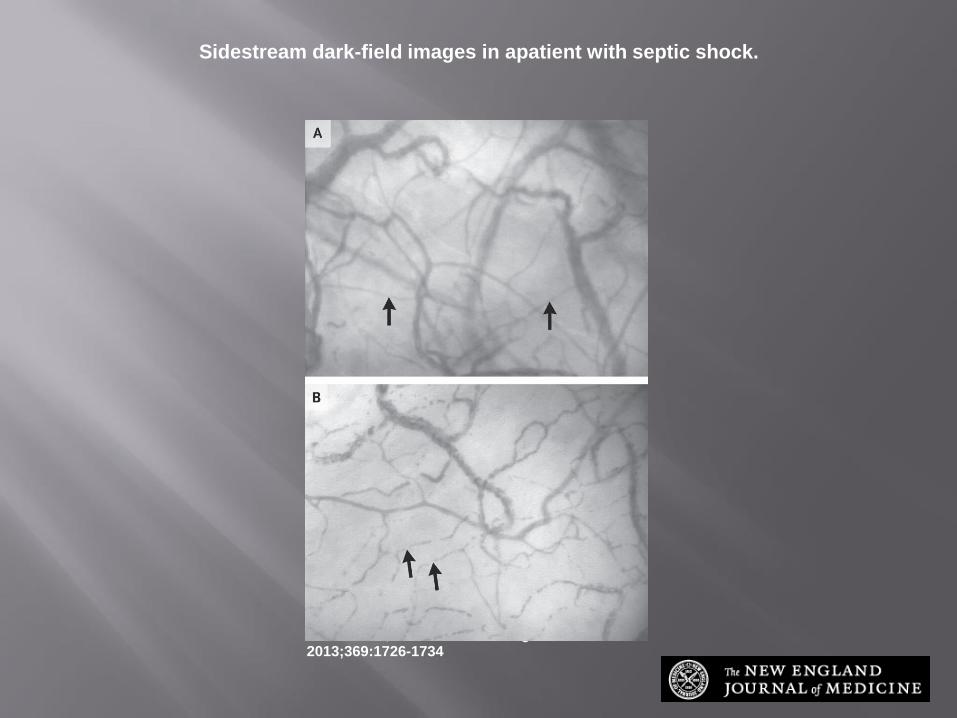
Sidestream dark-field images in apatient with septic shock.
Vincent J-L, De Backer D. N Engl J Med 2013;369:1726-1734
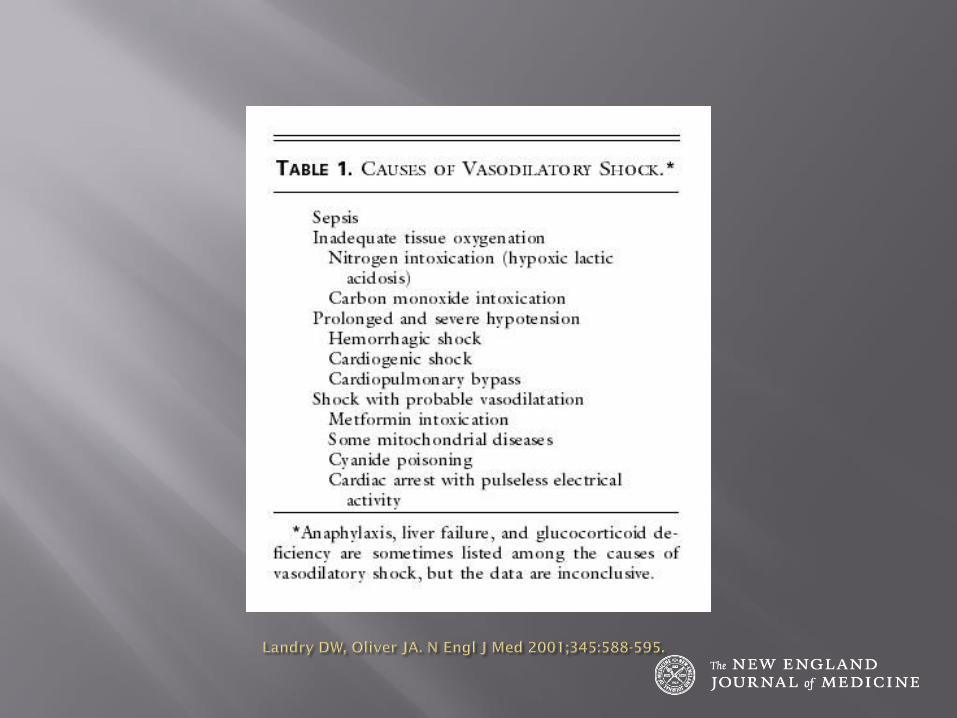
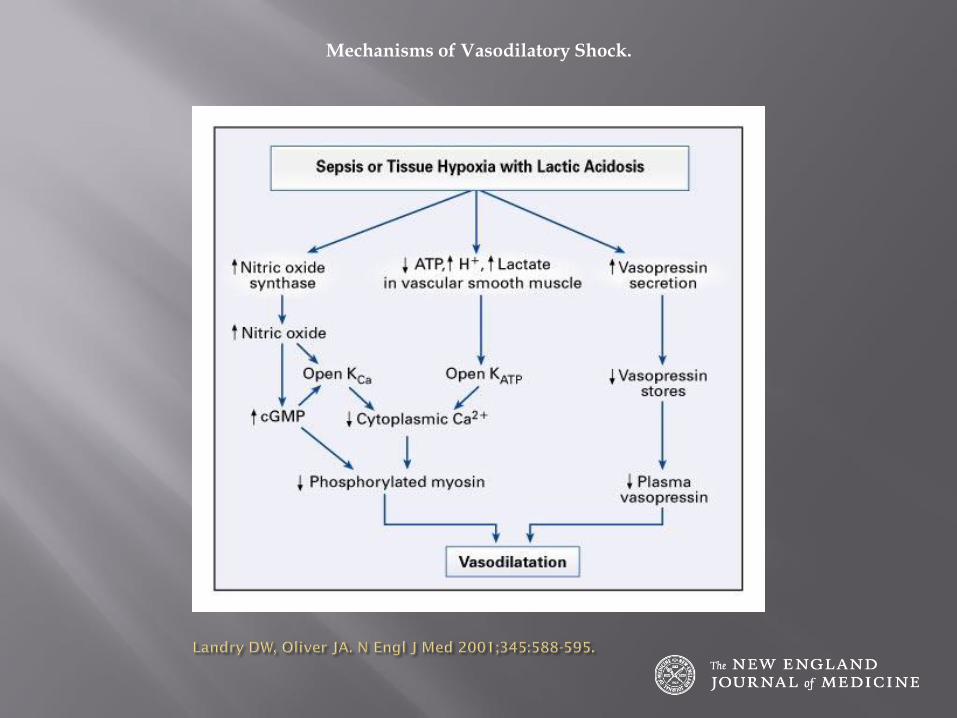
Mechanisms of Vasodilatory Shock.
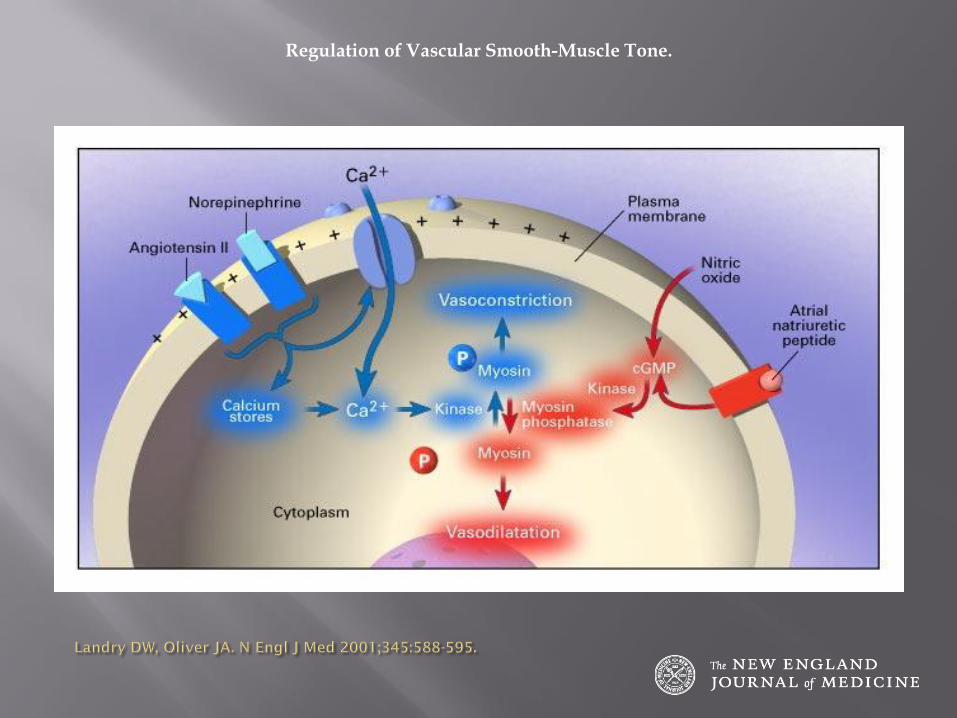
Regulation of Vascular Smooth-Muscle Tone.
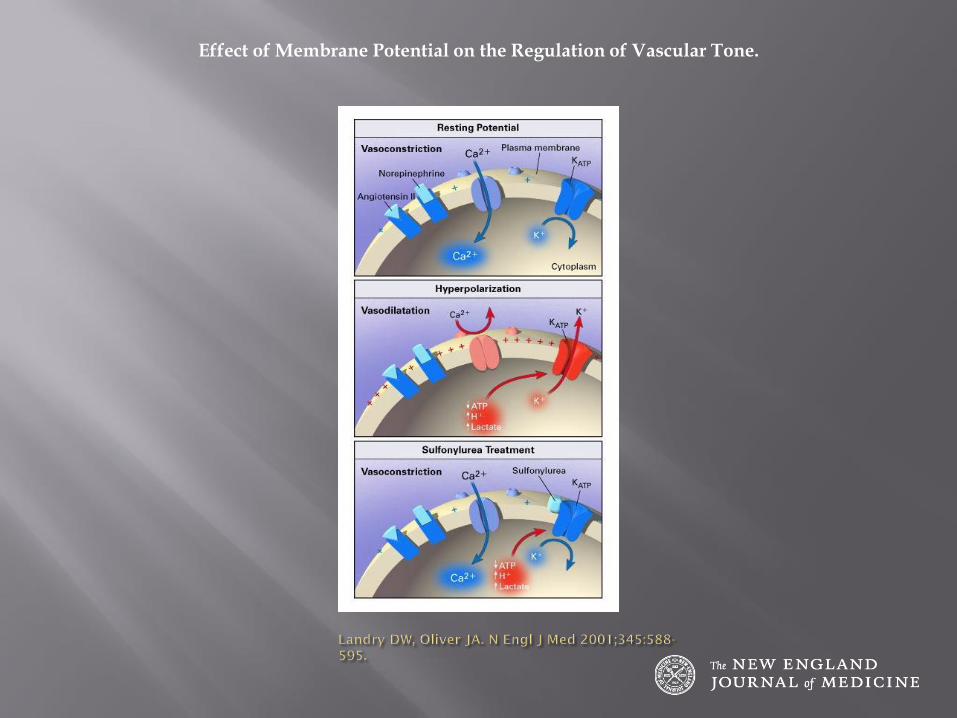
Effect of Membrane Potential on the Regulation of Vascular Tone.
Determine the type of circulatory shock.
Hyperdynamic vs hypodynamic shock
Use hemodynamic parameters and clinical information
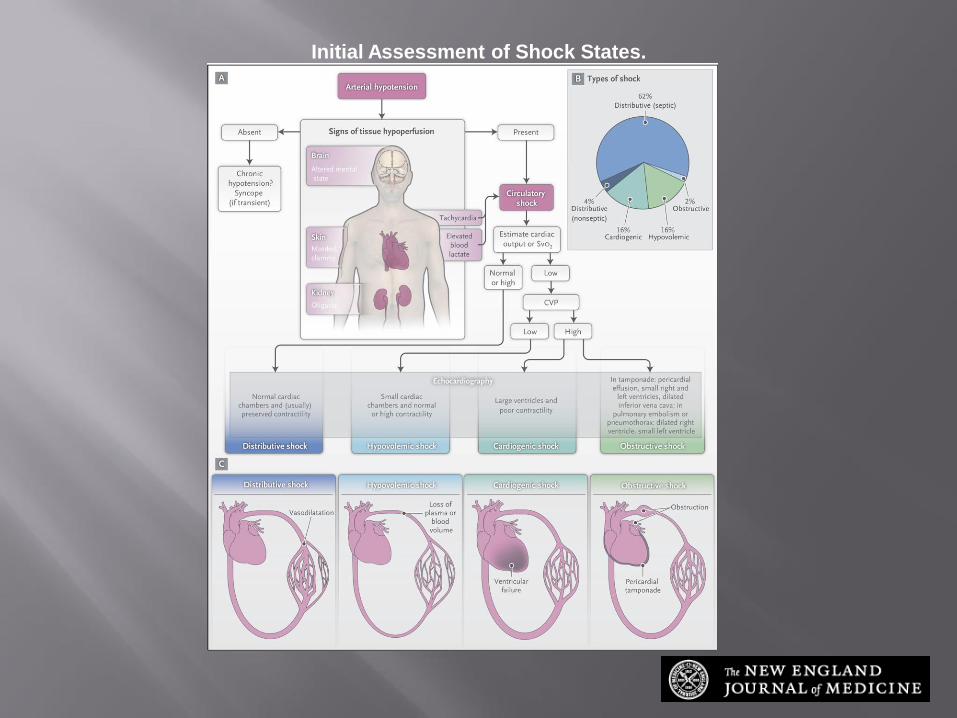
Initial Assessment of Shock States.
Vincent J-L, De Backer D. N Engl J Med 2013;369:1726-1734
Distributive shock
Cardiogenic shock
Hypovolemic shock
Obstructive shock
increased OR Normal CO ,
decreased SVR ,
SVO2 normal or increased ( shunting )
PAWP : Normal or decreased
Clinically ( warm shock)
Cardiogenic shock
Hypovolemic shock
Obstructive shock
The difficult one ( Cardiac tamponade , tension pneumothorax , abdominal compartment syndrome , Massive PE)
CO decreased
PAWP normal or increased
SVR increased
SV02 ( increased )
Decreased CO
Increased PAWP
Increased SVR
Decreased Sv02
( The obvious or difficult one )
CO , PAWP , SvO2 all decreased
SVR increased
Associated with irreversible shock
A useful mnemonic to describe the important components of resuscitation is the VIP rule :
ventilate (oxygen administration), infuse (fluid resuscitation), and pump (administration of vasoactive agents).
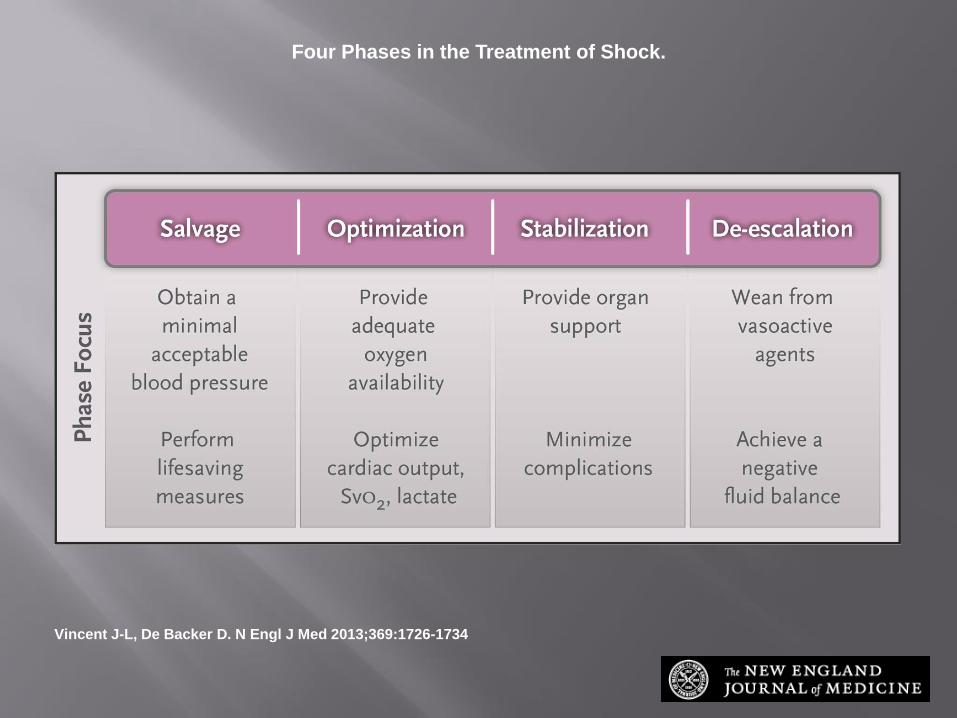
Four Phases in the Treatment of Shock.
Vincent J-L, De Backer D. N Engl J Med 2013;369:1726-1734
Early goal directed treatment in the first 6 hours. ( VIP Treatment )
Review diagnosis when not responding
Optimize Hb , electrolytes and pH ,
Optimize ventilation
Decreased sedatives dose
Use correct inotropes/vasopressor for hemodynamics and Vasopressin + hydrocortisone( hyperdynamic (septic)shock)
Consider ECMO , Aortic balloon counter pulsation
Scv02
PsvC02-PaC02
Lactate clearance
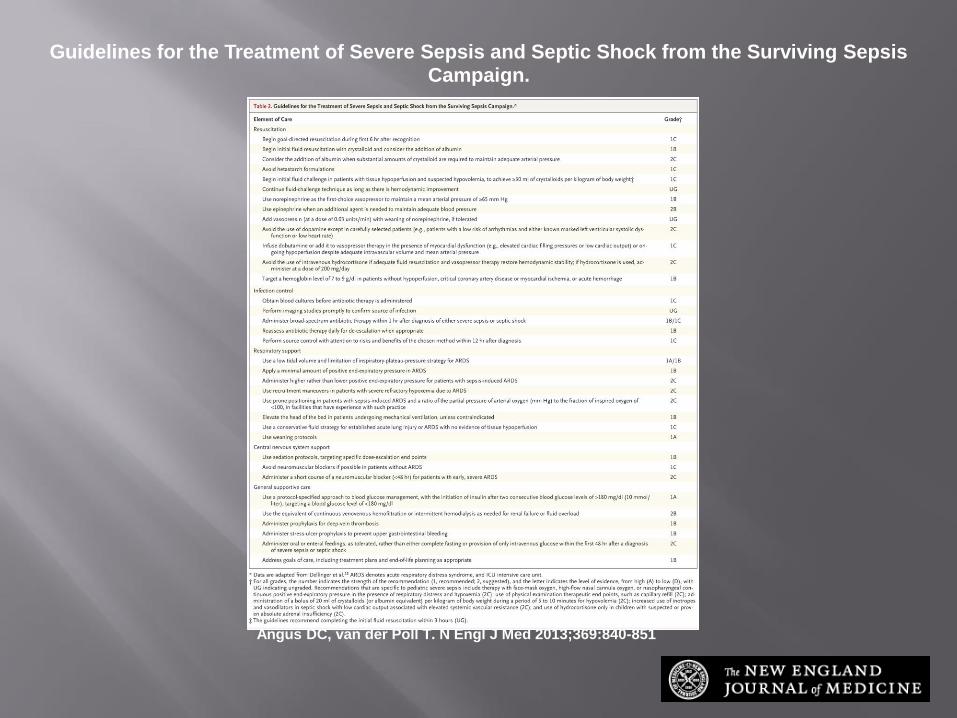
Guidelines for the Treatment of Severe Sepsis and Septic Shock from the Surviving Sepsis Campaign.
Angus DC, van der Poll T. N Engl J Med 2013;369:840-851
Medical history i.e. , myocardial infarction , hemorrhage , pulmonary embolism , cardiac tapenade.
Hemodynamic parameters
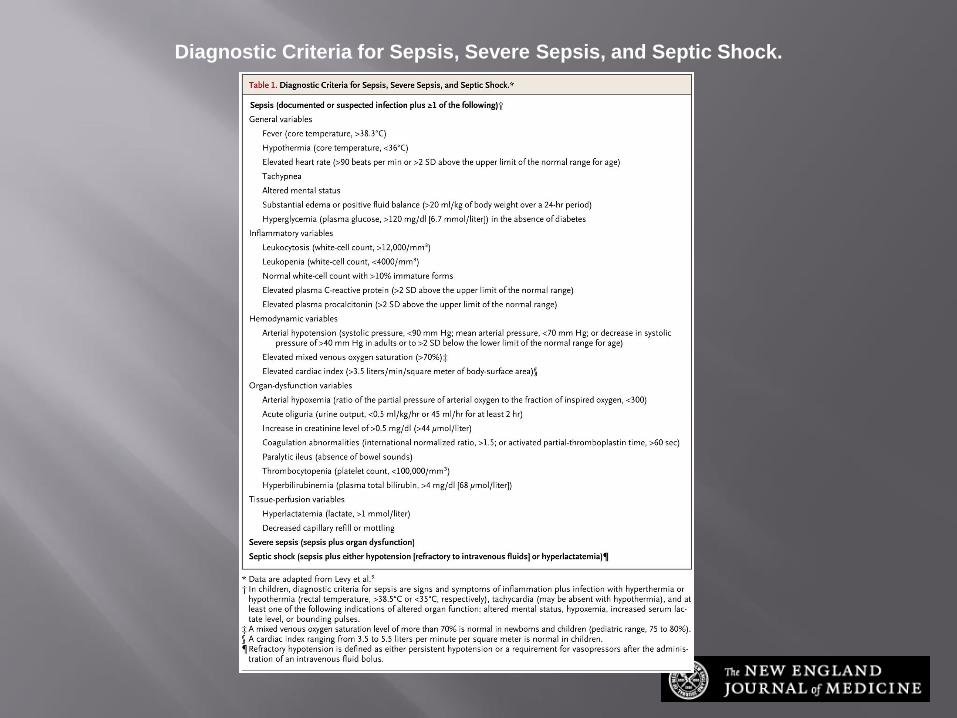
Diagnostic Criteria for Sepsis, Severe Sepsis, and Septic Shock.
Angus DC, van der Poll T. N Engl J Med 2013;369:840-851
Inability to contain and treat the cause for shock or define the mechanism of shock leading to irreversible damage on a cellular level and cell death after prolonged hypotension with decreased perfusion.
Impaired oxidative metabolism and oxygen debt (Crowel et al 1964) with increased venous C02 due to decreased CO2 clearance and increased formation of anaerobically derived acids
DO2 decreased and one maximum O2 extraction is reached anaerobic metabolism and hyperlactenemia
ATP generation impaired by lack of oxygen , increased NO and peroxynitrate and superoxide
Inflammatory mediators ( TNF , Endotoxins , free radicals ) inhibit mitochondrial function
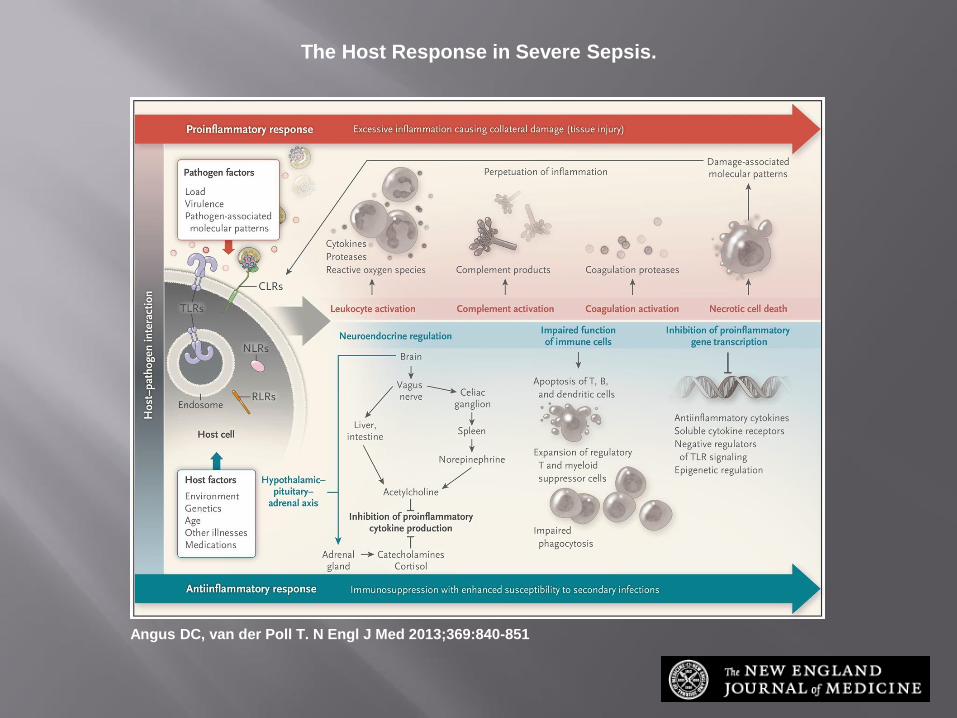
The Host Response in Severe Sepsis.
Angus DC, van der Poll T. N Engl J Med 2013;369:840-851
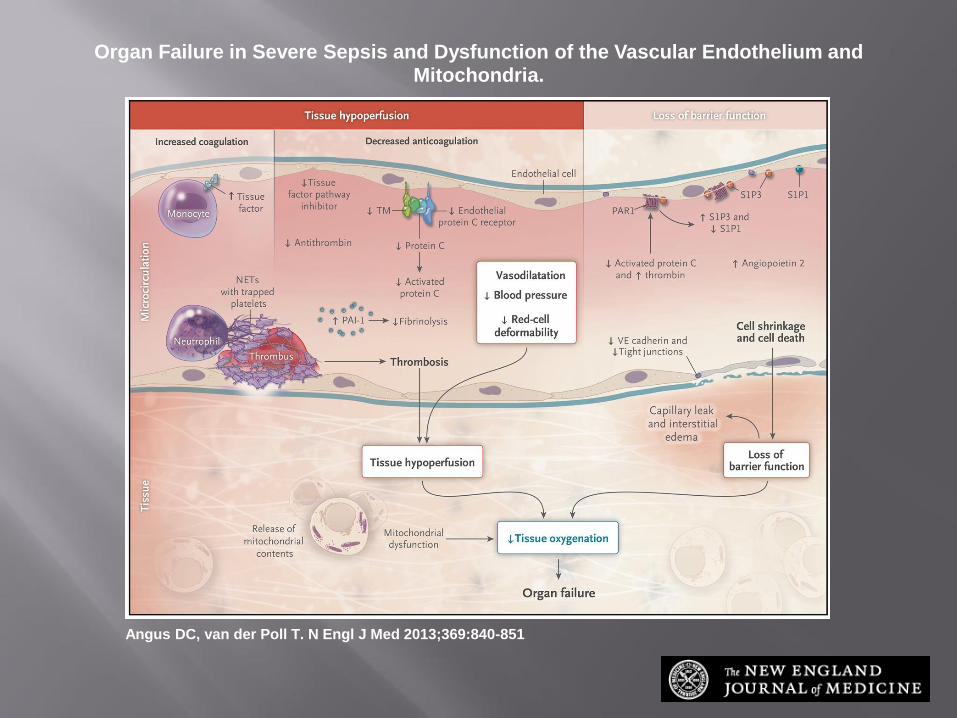
Organ Failure in Severe Sepsis and Dysfunction of the Vascular Endothelium and Mitochondria.
Angus DC, van der Poll T. N Engl J Med 2013;369:840-851
Impaired oxygen metabolism
Organ failure Ischamic injury with loss of membrane integrity
Inflammatory mediators released
Endothelial cell dysfunction
Reperfusion injury : during ischemia : ATP metabolized to hypoxanthine xanthine dehydrogenase -> Xanthine oxidase ->reperfusion -> superoxide formed -> cellular injury and membrane damage
Induction of apoptosis

Clinical Summary of 15 Patients with Refractory Hypotension.
The term "irreversible shock" in the dog signifies a form of death that is inevitable after certain early manifestations, including hemorrhage from the gut, the acceptance of large amounts of blood without maintained blood-pressure restoration, portal hypertension and hepatic-outflow obstruction. There was no evidence for this sequence in any of these patients, including those who died.
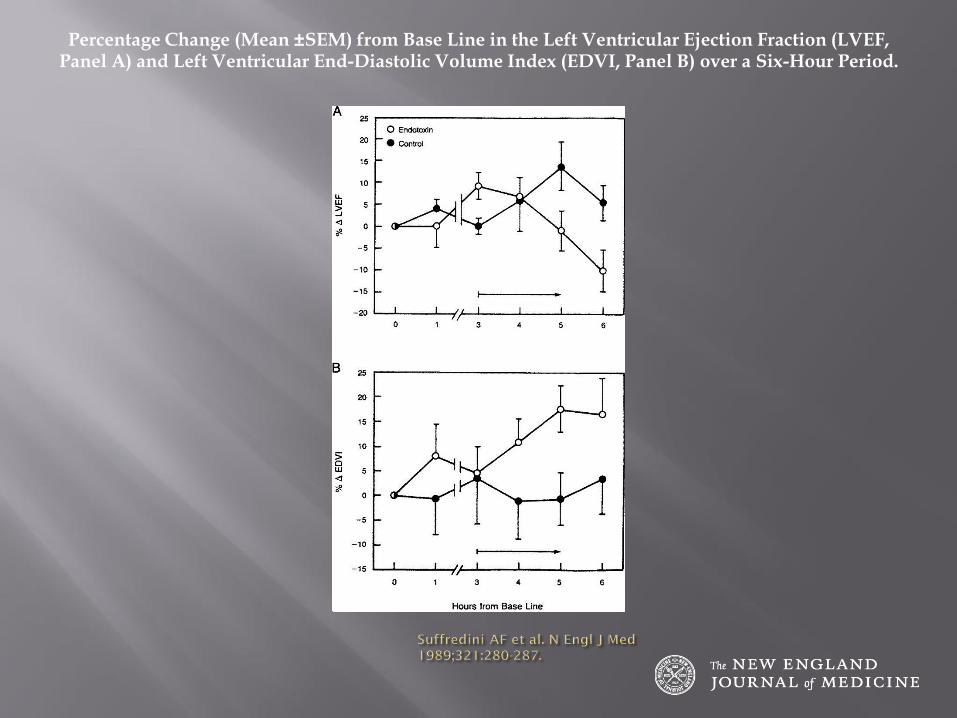
Percentage Change (Mean ±SEM) from Base Line in the Left Ventricular Ejection Fraction (LVEF, Panel A) and Left Ventricular End-Diastolic Volume Index (EDVI, Panel B) over a Six-Hour Period.
Can Resuscitation Jeopardize Survival?George Lister, M.D., and J. Julio Pérez Fontán, M.D.N Engl J Med 2004; 350:1708-1709April 22, 2004DOI: 10.1056/NEJMp048055





























