Embed Size (px)
Citation preview

11
Call 844-ASPiRA1(844-277-4721)
Quick Reference Guide

2
Table of Contents
Contact Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Welcome to ASPiRA LABS! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Specimen Requirements and Ordering Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
How To Order OVA1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Frequently Asked Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Collection and Shipping Instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Test Requisition Form Example . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Test Report Example . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Billing Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Patient Welcome/Billing Letter Example . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21

3
Contact Information
ASPiRA LABS can be reached by the following:
Phone
1 .844 .ASPiRA1 (1 .844 .277 .4721)
support@aspiralab .com
Fax
Laboratory: 512 .869 .4114
Website
www .aspiralab .com
www .OVA-1 .com
Account informationFor quick reference, please note your account number and name:

4
Welcome to ASPiRA LABS!
Dear Valued Customer,
I want to personally thank you for providing ASPiRA LABS with the opportunity to assist you in the care of your gynecology patients through our OVA1® testing service . At ASPiRA LABS, we pride ourselves on being at the forefront of ovarian cancer research and we have a passion for assisting in the delivery of relevant and timely care to your patients .We believe our passion will become evident to you in the level of service that we provide .
Providing you with the highest quality diagnostic results is a responsibility that we take very seriously and we are honored that you have chosen us to do so . You can trust the results that ASPiRA LABS provides and take comfort in the knowledge that OVA1 testing is FDA cleared and ASPiRA LABS is certified by Clinical Laboratory Improvement Amendments (CLIA), which means that we adhere to the highest standards in the clinical laboratory industry .
Our entire team of business and laboratory professionals is looking forward to working with you . It is important to all of us that you receive exceptional service, so please don’t hesitate to contact me, at any time, with any comments or concerns that you may have .
Sincerely,
Herbert A. Fritsche
Herbert A . Fritsche, Ph .D .Laboratory Director Cell: 713 .542 .0831Email: hfritsche@vermillion .com

5
ASPiRA LABS is led by medical director Herbert A . Fritsche Jr, Ph .D . Prior to his tenure at ASPiRA LABS, Dr . Fritsche was a professor of biochemistry and clinical chemistry section chief in the Department of Pathology and Laboratory Medicine at The University of Texas M .D . Anderson Cancer Center in Houston . Dr . Fritsche holds doctorate and masters degrees in chemistry from Texas A&M University, and a bachelor of science degree in chemistry from the University of Houston .
Dr . Fritsche serves as associate editor for the International Journal of Biological Markers and section editor for the Archives of Pathology and Laboratory Medicine, among other numerous editorships currently and over the years . In addition he is a member of more than a half dozen industry editorial boards such as Cancer Molecular Biology, Tumor Biology and Diagnostic Oncology . He has been recognized by the American Association for Clinical Chemistry with its Presidential Citation; the Morton K . Schwartz Award for Research and Accomplishments in Cancer Diagnostics; and the Annual National Award for Outstanding Contributions in Education . In 1999, he received the Distinguished Scientist Award from the Clinical Ligand Assay Society, where he also served as president .
Dr . Fritsche has been on numerous national committees and Boards during his career, including for the American Association for Clinical Chemistry, Eastman Kodak and SmithKline Beecham Clinical Laboratories . He is a member of, and has held leadership positions in, the American Association for Clinical Chemistry, the International Society for Oncodevelopmental Biology and Medicine, Clinical Ligand Assay Society and the National Academy of Clinical Biochemistry . He has published more than 100 articles on topics related to his field of expertise.
Herbert A . Fritsche, Ph .D .
Herbert A . FritscheASPiRA LABS Medical Director
5
ASPiRA LABS is led by medical director Herbert A . Fritsche Jr, Ph .D . Prior to his tenure at ASPiRA LABS, Dr . Fritsche was a professor of biochemistry and clinical chemistry section chief in the Department of Pathology and Laboratory Medicine at The University of Texas M .D . Anderson Cancer Center in Houston . Dr . Fritsche holds doctorate and masters degrees in chemistry from Texas A&M University, and a bachelor of science degree in chemistry from the University of Houston .
Dr . Fritsche serves as associate editor for the International Journal of Biological Markers and section editor for the Archives of Pathology and Laboratory Medicine, among other numerous editorships currently and over the years . In addition he is a member of more than a half dozen industry editorial boards such as Cancer Molecular Biology, Tumor Biology and Diagnostic Oncology . He has been recognized by the American Association for Clinical Chemistry with its Presidential Citation; the Morton K . Schwartz Award for Research and Accomplishments in Cancer Diagnostics; and the Annual National Award for Outstanding Contributions in Education . In 1999, he received the Distinguished Scientist Award from the Clinical Ligand Assay Society, where he also served as president .
Dr . Fritsche has been on numerous national committees and Boards during his career, including for the American Association for Clinical Chemistry, Eastman Kodak and SmithKline Beecham Clinical Laboratories . He is a member of, and has held leadership positions in, the American Association for Clinical Chemistry, the International Society for Oncodevelopmental Biology and Medicine, Clinical Ligand Assay Society and the National Academy of Clinical Biochemistry . He has published more than 100 articles on topics related to his field of expertise.
Herbert A . Fritsche, Ph .D .
Herbert A . FritscheASPiRA LABS Medical Director

6
Specimen Requirementsand Ordering Information
Specimen Requirements
• 2 .2 mL refrigerated serum; 1 .1 mL minimum
• Fresh serum stored at +2 to +8°C can be used up to 8 days
• Lipemic samples or frozen samples that are turbid after thawing must be clarified by centrifugation (10 minutes at ~15,000 x g) prior to testing. Lipemic samples that cannot be clarified should not be used. For testing, the clarified portion of the sample must be used, and must be drawn through the supernatant lipid layer .the supernatant lipid layer .the supernatant lipid layer
• The OVA1 test is for use with serum only . Plasma and other sample types are not acceptable for testing and will be discarded .
• Do not use serum specimens that are heat-inactivated or stabilized with azide .
• Serum specimens must be completely coagulated and, after centrifugation, must not contain any particles or traces of fibrin.
OVA1 Ordering Information
To order the OVA1 test, please complete a provided test requisition form and ship the form and the serum specimen according to the instructions included in this quick-reference guide .
CPT Code†:
81503: Oncology (ovarian), biochemical assays of five proteins (CA-125, apoliproprotein A1, beta-2 microglobulin, transferrin, and pre-albumin), utilizing serum, algorithm reported as a risk score
Reference ICD-10 Codes††:R19 .03 Right lower quadrant abdominal swelling, mass and lumpR19 .04 Left lower quadrant abdominal swelling, mass and lump
† The CPT codes provided are based on AMA guidelines and are for informational purposes only . CPT coding is the sole responsibility of the billing party . Please direct any questions regarding coding to the payor being billed .
†† This is provided for informational purposes only and is not a guarantee of coverage . It is the provider’s responsibility to determine the appropriate codes .

7
How To Order OVA1
Partnering reference laboratory
In-office phlebotomy
Quest Patient Service Center (PSC) / draw
station
Use ASPiRA test kitSubmit requisition
Reporting
Average turnaround time of 24-48 hrs from receipt
In-hospital phlebotomy

8
Frequently Asked Questions
Q Does blood have to be spun down? Yes, once the sample has been allowed to clot for 30 minutes, it must be centrifuged at 1000-1300 x g for 10-15 minutes.
Q What is your turnaround time? Our guaranteed turnaround time is 4 days, but we strive to provide results faster than that and we are frequently able to do so. On average, we have reported results 24-48 hrs from receipt.
Q How will results be reported? Resultswillbefaxedtothesecurefaxnumberthatwehaveonfileforeachofourclients.
Results is available via secure web portal for participating customers. To learn more and sign up for the web portal, please call 1-844-ASPiRA1 (1.844.277.4721).
Q Is ASPiRA LABS open weekends? We receive samples on Saturdays, but we are closed on Sundays. The laboratory’s normal days of operation are Monday through Friday.
Q When does the kit expire? The only perishable items within the kit are SST tubes. These tubes are generally good for several years, but please check the expiration date on the SST tube itself.
Q Is CA125II a biomarker in OVA1 testing? CA125IIisoneofthefivebiomarkerswhosebloodlevelsareusedtocomputetheOVA1
score, but it is not approved by the FDA to be used as a stand-alone test for assessing risk of malignancy in adnexal masses.
Q If we draw on a Friday, and FedEx will not come by the end of the day, what should we do? Store the serum specimen at +2 to +8°C over the weekend and set up a FedEx pick up for the following Monday.
Q How long can a serum specimen be stored and under what conditions?Serum specimens can be stored at +2 to +8°C for up to 8 days.
Q What is the number to call for FedEx sample pickup? Please call 1-800-GO-FEDEX to schedule a pickup if there is not a regular FedEx pickup at your location.
Q What is your billing policy or who can I speak to regarding billing questions?Please see our billing policy in this Quick Reference Guide. Please call 1-844-ASPiRA1 (1.844.277.4721).
Q Can I get the CA-125 value when I order an OVA1 test?Yes, physicians who would like a patient’s CA-125 value for the purpose of monitoring ovarian cancer can contact ASPiRA LABS at 1-844-ASPiRA1 (1.844.277.4721).

9
Q I received a biohazard bag with test requisition forms . How do I submit a sample with this? AsanofficethatusestheQuestcouriernetwork,yourphlebotomistcandrawandplace
the specimen in the provided biohazard bags along with a fully completed test requisition form. This submission can now be picked up by the courier network (e.g., via lock-box) and delivered to ASPiRA LABS.
Q How do I get the test requisition forms? If you are submitting a sample to a reference laboratory (e.g., Quest), please contact
your local ASPiRA LABS or reference laboratory representative or call 1-844-ASPiRA1 (1.844.277.4721).Wewillhelpsupplyrequisitionformstoyouroffice(s).
If you are submitting a sample directly to ASPiRA LABS, please visit www.trf.vermillion.com for a unique printable test requisition form. Alternatively, you can contact your local ASPiRA LABS oor call 1-844-ASPiRA1 (1.844.277.4721). We will help supply requisition forms to your office(s).
Q Where can I find the nearest Quest Patient Service Center (PSC) or reference laboratory draw center? The nearest Quest PSC can be located at the following web link - https://secure.
questdiagnostics.com/hcp/psc/jsp/SearchLocation.do. Alternatively, you may contact your local ASPiRA LABS representative or call 1-844-ASPiRA1 (1.844.277.4721).
If you are looking for another reference laboratory draw center, please contact your local ASPiRA LABS representative or call 1-844-ASPiRA1 (1.844.277.4721) for the most up-to-date information. If there are no partnering reference laboratories near you, ASPiRA LABS can send you test kits with pre-paid shipping labels for FedEx pick-up.
For future reference, please note the phlebotomy centers near you:

10
Sample Collection with an ASPiRA Test Kit
Preparation• When you receive the transport kit, remove coolant pack from kit and place into freezer 24 hours prior to use .• Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the shipping and
handling instructions .• Fill out the patient name and date of birth on each of the 6 barcoded labels provided . Apply one barcode label to
each of the tubes, and one barcode label to each copy of the Test Requisition Form . The 6th barcode label will be returned with the sample .
• Complete collection date and phlebotomist initials on the ASPiRA requisition (top right corner) .• Complete the Test Requisition Form including the following: collection date and time, patient’s first and last name,
patient’s DOB, last four (4) digits of the patient’s SSN, practitioner’s name and signature, ICD-9 or ICD-10 codes, and patient’s billing information .
• Note: Missing or incomplete test requisition information will delay processing and extend turnaround time . Specimens not properly identified will not be accepted by the laboratory.
5x
Step 1
• Draw 8 .5 mL of the patient’s blood by performing a standard venipuncture procedure using the Serum Separation Transport Tube (Tiger Top Tube) .
• Mix the blood in the tube by inverting 5 times .Place a barcode label on the Serum Separation Transport Tube (Tiger Top Tube) to identify and label the sample .
• Place tube in an upright position and allow the blood to clot for 30 minutes, but no longer than 2 hours .
Step 2
• Document the time and date of blood draw on the top right-hand section of the Test Requisition Form .
• Record the phlebotomist’s initials .
Step 3
• Once the sample has completed clotting, centrifuge 1000-1300 x g for 10-15 minutes .
• After separation, serum should be stored at 2-8°C

11
3 Steps to Sample Shipping and Handling
Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the instructions below.
STEP 1 • Place the Serum Separator Tube and Serum
Transport Tube into the biohazard bag with absorbent pad. Remove the excess air and seal the bag along the zippered track.
Fold the Test Requisition Form into quarters and place in the side pocket of the biohazard bag along with the 6th barcode label.
Place the biohazard bag into the foil pouch. Remove the adhesive liner, fold the flap, and seal the foil pouch.
•
• FOLD
STEP 2 • Remove the lid from the foam cooler. Place one
frozen coolant pack at in the bottom of the foam cooler.
Place the foil pouch with the enclosed Serum Separator Tube and Serum Transport Tube on top of the coolant pack, ensuring the foil pouch is pushed down securely into the foam cooler.
Place the second coolant pack on top of the foil pouch, ensuring the contents are packed in the foam cooler to allow the lid to be placed firmly.
•
•
STEP 3 • Place the lid on the foam cooler ensuring the lid is
completely closed.
• Close the kit box and affix the Shipping Label provided to the outside of the kit box.
• Contact FedEx online or call 1-800-463-3339 to schedule a pick up. Kits may also be dropped off at a FedEx shipping location.
ASPiRA LABS | aspiralab.com 101 Cooperative Way, Suite 220 Georgetown, TX 78626 [email protected] (844) ASPiRA1 / (844) 277.4721 Fax: (512) 869.4114
To receive additional specimen transport kits: Call (844) ASPiRA1 / (844) 277.4721
and ask for catalog No. 1212.
CSS003
Sample Shipping and Handling (Single Specimen Test Kit)• Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the instructions below .
Step 1
• Place the Serum Separator Tube into the biohazard bag with absorbent pad . Remove the excess air and seal the bag along the zippered track .
• Fold the Test Requisition Form into quarters and place in the side pocket of the biohazard bag along with the 6th barcode label .
• Place the biohazard bag into the foil pouch .Remove the adhesive liner, fold the flap, and seal the foil pouch .
Step 2
• Remove the lid from the foam cooler .Remove the lid from the foam cooler .Remove the lid from the foam cooler Place one frozen coolant pack at in the bottom of the foam cooler .cooler .cooler
• Place the foil pouch with the enclosed Serum Separator Tube and Serum Transport Tube on top of the coolant pack, ensuring the foil pouch is pushed down securely into the foam cooler .pushed down securely into the foam cooler .pushed down securely into the foam cooler
• Place the second coolant pack on top of the foil pouch, ensuring the contents are packed in the foam cooler to allow the lid to be placed firmly.
Step 3
• Place the lid on the foam cooler ensuring the lid is completely closed .
• Close the kit box and affix the Shipping Label provided to the outside of the kit box .
• Contact FedEx online or call 1-800-463-3339 to schedule a pick up . Kits may also be dropped off at a FedEx shipping location .
FOLD
3 Steps to Sample Shipping and Handling
Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the instructions below.
STEP 1 • Place the Serum Separator Tube and Serum
Transport Tube into the biohazard bag with absorbent pad. Remove the excess air and seal the bag along the zippered track.
Fold the Test Requisition Form into quarters and place in the side pocket of the biohazard bag along with the 6th barcode label.
Place the biohazard bag into the foil pouch. Remove the adhesive liner, fold the flap, and seal the foil pouch.
•
• FOLD
STEP 2 • Remove the lid from the foam cooler. Place one
frozen coolant pack at in the bottom of the foam cooler.
Place the foil pouch with the enclosed Serum Separator Tube and Serum Transport Tube on top of the coolant pack, ensuring the foil pouch is pushed down securely into the foam cooler.
Place the second coolant pack on top of the foil pouch, ensuring the contents are packed in the foam cooler to allow the lid to be placed firmly.
•
•
STEP 3 • Place the lid on the foam cooler ensuring the lid is
completely closed.
• Close the kit box and affix the Shipping Label provided to the outside of the kit box.
• Contact FedEx online or call 1-800-463-3339 to schedule a pick up. Kits may also be dropped off at a FedEx shipping location.
ASPiRA LABS | aspiralab.com 101 Cooperative Way, Suite 220 Georgetown, TX 78626 [email protected] (844) ASPiRA1 / (844) 277.4721 Fax: (512) 869.4114
To receive additional specimen transport kits: Call (844) ASPiRA1 / (844) 277.4721
and ask for catalog No. 1212.
CSS003
3 Steps to Sample Shipping and Handling
Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the instructions below.
STEP 1 • Place the Serum Separator Tube and Serum
Transport Tube into the biohazard bag with absorbent pad. Remove the excess air and seal the bag along the zippered track.
Fold the Test Requisition Form into quarters and place in the side pocket of the biohazard bag along with the 6th barcode label.
Place the biohazard bag into the foil pouch. Remove the adhesive liner, fold the flap, and seal the foil pouch.
•
• FOLD
STEP 2 • Remove the lid from the foam cooler. Place one
frozen coolant pack at in the bottom of the foam cooler.
Place the foil pouch with the enclosed Serum Separator Tube and Serum Transport Tube on top of the coolant pack, ensuring the foil pouch is pushed down securely into the foam cooler.
Place the second coolant pack on top of the foil pouch, ensuring the contents are packed in the foam cooler to allow the lid to be placed firmly.
•
•
STEP 3 • Place the lid on the foam cooler ensuring the lid is
completely closed.
• Close the kit box and affix the Shipping Label provided to the outside of the kit box.
• Contact FedEx online or call 1-800-463-3339 to schedule a pick up. Kits may also be dropped off at a FedEx shipping location.
ASPiRA LABS | aspiralab.com 101 Cooperative Way, Suite 220 Georgetown, TX 78626 [email protected] (844) ASPiRA1 / (844) 277.4721 Fax: (512) 869.4114
To receive additional specimen transport kits: Call (844) ASPiRA1 / (844) 277.4721
and ask for catalog No. 1212.
CSS003

12
Step 1• Complete collection date and phlebotomist initials on ASPiRA
Req (top right corner) . Place SST tube into the biohazard bag with absorbent pad and seal .
• Fold ASPiRA requisition into quarters and place in the side pocket of biohazard bag along with the barcode label
Step 2• Remove lid from the foam cooler .Remove lid from the foam cooler .Remove lid from the foam cooler Place biohazard bag with SST
tube in the bottom of cooler .tube in the bottom of cooler .tube in the bottom of cooler• Up to three specimens can be shipped together in a kit .• Place one frozen coolant pack on top of the specimen(s) .
Step 3• Place lid on foam cooler, ensure it is completely closed .• Close the kit box and affix the prepaid shipping label to the
outside of the kit box .
• Contact FedEx online or call 1-800-463-3339 to schedule a pick up . Kits may also be dropped off at a FedEx shipping location .
FOLD
Sample Shipping and Handling (Multiple Specimen Test Kit)• Note: Store serum sample at 2-8 degrees Celsius until the sample can be packaged following the instructions below .

13
∙ ∙ ∙ ∙ ∙ ∙ ∙
OVA1117522
ACME Laboratories, Inc. 100123 N. Main Street Suite B
Sometown PA 18903
111-222-5555 111-222-6666 111-222-6666
[ ] Dr. Pepsi-Cola[ ] Dr. Smith[ ] Dr. Joey[ ] Dr. Caffeine[ ] Dr. Brown[ ] Dr. Spock[ ] Dr. Phil[ ] Dr. Pepper
[ ] Dr. Doctor[ ] Dr. White
ACM1418658
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Name__________________DOB___________________
OVA1117522
Test Requisition Form Example
Fill ICD-9/10 code
Complete patient insurance information
Complete all details and check menopausal status
Check ordering physician and ensure accuracy
Date and initial
*Complete all required areas of the test requisition form; information marked in*Complete all required areas of the test requisition form; information marked in red may cause delays if incomplete may cause delays if incomplete **Please complete the Advance Beneficiary Notice (ABN) form on the back side for medicare patients
Check test requested
Patient and provider signature
Help further research by providing additional information and consent

14
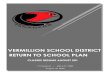
Test Report Example: Pre-menopausal
0 1 2 3 4 6 7 8 9 10
OVA1 Premenopausal Cutoff
R E F E R E N C E R A N G E
LOWER LIKELIHOOD OF
OVARIAN MALIGNANCY
HIGHER LIKELIHOOD OF
OVARIAN MALIGNANCY
5.0
N=0 N=13
N=88 N=126 N=80 N=42
N=26
N=21
N=28
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1-1.9 2-2.9 3-3.9 4-4.9
OVA1 Score
5-5.9 6-6.9 7-7.9 8-8.9 9-10
Pre-Menopausal Malignancy Rate
Jane Doe
7.8 Elevated Risk of Ovarian Malignancy
Sample Report
• The OVA1 test score is reported as a single numeric score on a scale of 0-10 .
• The cutoff threshold for a premenopausal patient is 5 .0, and 4 .4 for a postmenopausal patient .
• Scores greater than or equal to these thresholds indicate a higher likelihood of malignancy. Patients with a higher likelihood of malignancy may benefit from consultation with the gynecologic oncologist .

15
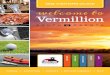
Test Report Example: Post-menopausal
N=0 N=11N=96
N=137
N=30
N=18
N=19 N=35
0%
20%
40%
60%
80%
100%
1-1.9 2-2.9 3-4.3 4.4-5.9 6-6.9 7-7.9 8-8.9 9-10
Post-Menopausal Malignancy Rate
OVA1 Score
0 1 2 3 4 5 6 7 8 9 10
OVA1 Postmenopausal Cutoff
R E F E R E N C E R A N G E
LOWER LIKELIHOOD OF
OVARIAN MALIGNANCY
HIGHER LIKELIHOOD OF
OVARIAN MALIGNANCY
4.4
Jane Doe
3.2 Low Risk of Ovarian Malignancy
Sample Report
• Risk of malignancy was reported as below 1 .4% for premenopausal women and 3 .3% for postmenopausal women based on Bristow et al .’s clinical validation study .

16
Billing Policy
Overview
ASPiRA LABS recognizes that some patients will need assistance in order to access OVA1 testing and will work with patients to facilitate access and to reach a satisfactory resolution regarding patient responsibility .
• We will seek positive coverage decisions with all insurance providers, including Medicare, to provide appropriate coverage for patients
• If a claim is denied, we will appeal the patient’s insurance carrier on behalf of the patient to assist in claims reimbursement
• We offer a generous financial assistance program to all patients in accordance with applicable laws
• Only after exhausting all other options will we seek fair reimbursement from the patient as required
Insurance Claim Requirements
Billing Patient’s Health Insurance – Laboratory tests are offered nationally and may be covered by the patient’s insurance . All patients are encouraged to contact their insurance carrier to understand and confirm their specific insurance coverage prior to testing. In order for ASPiRA LABS to file a claim directly with a patient’s health insurance plan we require the following:
• A completed test requisition form with diagnosis codes and patient history information supporting the medical necessity of testing and authorizing ASPiRA LABS to bill the patient’s health insurance plan
• An enlarged copy of patient’s health insurance plan card (front and back) with each test requisition
• When required by the patient’s health insurance plan, a prior authorization approval number
Insurance Coverage and Patient Payments
ASPiRALABSisaMedicareapprovedproviderandOVA1haspositiveMedicarecoveragethroughNovitas and is FDA cleared.
Contracted Insurance – There are hundreds of insurance plans in the United States, some of which may be contracted with ASPiRA LABS . ASPiRA LABS bills all insurances . If the patient’s health insurance plan is contracted with ASPiRA LABS, it will usually pay for most, and possibly all, of the charges for services provided to the patient . ASPiRA LABS will bill the patient for any deductible, coinsurance, or required amount after receipt of the explanation of benefits (EOB).
Non contracted health insurance carriers may still cover all or some portion of the bill for the provided testing services. Patient financial responsibility for any applicable deductible, co-insurance and co-payments will still apply .
Denied Claims and Appeals
A patient’s health insurance carrier can deny payment for treatment or medical services for many reasons .If the claim is denied, ASPiRA LABS will immediately formally appeal the claim to the insurance company .

17
Additionally, ASPiRA LABS can offer tools and resources to help patients throughout the appeal process .We offer various discounts and financial assistance when insurance denies payment. Please see the payment assistance program section below .
Payment Assistance Programs for Patients with No Insurance Coverage
Programs are available for patients who are not covered by any health insurance . These programs are only offered individually and cannot be combined in any form or fashion . ASPiRA LABS will work with the patient to determine their eligibility for each program .
Immediate Pay Discounts – A discount is extended to those patients who are self-pay or uninsured if payment is received within 7 days of the date of service . The patient should contact us to determine their discounted amount . We offer the following options to obtain this discount:
• Send payment with the sample or test requisition; we accept money orders, personal checks or cashier checks if payment is received with the sample or test requisition .
Payment Plan
Please call our billing department to arrange a payment plan for up to 4 monthly installments .
Financial Assistance Program
Patients who are uninsured may be eligible for financial assistance under the ASPiRA LABS Financial Assistance Program (FAP) . The patient must complete the FAP Application or contact the ASPiRA LABS billing department to determine eligibility for the FAP .billing department to determine eligibility for the FAP .billing department to determine eligibility for the FAP The patient will be required to submit proof of eligibility for these programs to verify income and number of dependents . Financial Assistance Programs cannot be combined with other Payment Assistance Programs except for the Payment Plan option .
The following information serves as a preliminary guide to help determine if the patient qualifies for FAP, but please see the FAP application for specific documentation requirements:
• The patient must be a U .S . resident or citizen
• If the patient is eligible for federal food stamps, qualifies for State Medical Assistance, or is eligible for the Hill-Burton Program, they automatically qualify
• In the event that the patient does not automatically qualify due to the participation in one of the above listed programs, the patient will need to submit proof of gross income for the patient and spouse (e .g ., W-2) as well as the number of dependents
ASPiRA LABS is committed to working with the patient to help determine if they qualify for financial assistance. Once we receive a request for financial assistance, and review income, we will promptly notify the patient and will discuss costs. If the patient qualifies for assistance, but has already received a bill, we will indicate the portion of the bill that will be deducted due to the application of the FAP credit .

18
Billing: Common QuestionsQ Do you accept Medicare patients?
Yes, Medicare and any supplemental insurance (if applicable) are accepted and will be billed. Patients are responsible for any applicable deductible and co-pay as stipulated by their plan(s) and not covered by Medicare or the supplemental policy, as required by federal law. Co-payment is usually 20% of Medicare allowable for anatomic pathology.
Q What does it mean if the patient’s health insurance is contracted with you?ASPiRA LABS accepts as payment in full the payer’s contracted allowed amount for testing services. Patients are responsible for any applicable deductible, co-insurance and co-pay as directedbytheExplanationofBenefits(EOB).Patientswillnotberesponsibleforthedifference between our list price and the payer’s contracted allowable amount, except when services are denied under provisions of the patient’s plan.
Q What does it mean if the patient’s health insurance is not contracted with you?ASPiRA LABS will make every effort to work with non-contracted health insurance carriers to minimize the out-of-pocket expense to the patient. If ASPiRA LABS is considered to be outofnetworkbythepayer,wewillhonorthepatient’sOUT-of-networkbenefitswhenprovidedwithcleardocumentationindicatingthepatient’sOUT-of-networkbenefits.Thepatient will be responsible for any applicable deductible, co-insurance and co-payments not coveredbythepayer’sOUT-of-networkbenefits.
Q What happens if the patient does not have insurance or chooses to pay out of pocket?The patient will be billed at a discounted rate and is responsible for the billed amount. However, at no time will the billed amount be less than the Medicare allowed amount. Patients may contact ASPiRA LABS at 1-844-ASPiRA1 (1.844.277.4721).
Q What is your billing process? Note:AllMedicareclaimsandinsuranceclaimsarefiledelectronicallytotheextentthattheinsuranceplanisabletoacceptelectronicclaims.Claimsarefileddaily.
1.Fivedaysaftertheclaimisfiled,aninitialletterwillbesenttothepatientinformingthemthattheirlabworkhasbeenfiledtoinsuranceandaskingthepatienttonotifyusiftheinsurance information is incorrect.
2. After insurance has paid the claim, the patient will be responsible for any applicable deductible, co-insurance and co-payments per their plan. If insurance denies the claim, we will appeal the denial and only after all appeal attempts have been exhausted will the patient be billed.
If you have any billing questions, please call 1-844-ASPiRA1 (1.844.277.4721)

19
Application for Economic Hardship
ASPiRA LABS | aspiralab.com 12117 Bee Caves Rd. Building III, Suite 100 Austin, Texas 78738
[email protected] (844) ASPiRA1 / (844) 277.4721 Fax: (512) 869.4114
Please send completed form with the test requisition or fax it at the time of sample collection to: 512.869.4114
PATIENT INFORMATION
Last Name: Middle Initial: First:
Birth date: Social Security #: Home phone: ( )
Street address:
City: State: Zip:
STATEMENT OF MEDICAL NECESSITY
I have determined the ordered OVA1 test is medically indicated for the above named patient.
CERTIFICATION OF ECONOMIC HARDSHIP The above patient has no medical insurance and I have established to my satisfaction that this patient’s existing financial resources are not sufficient to cover the cost of the OVA1 test. I am requesting that he/she be included in the ASPiRA LABS Uninsured Patient Program. To the best of my knowledge, this patient’s household income falls below 250% of the Poverty Level as established by the U.S. Department of Health and Human Services. I will also provide comparable discounted and/or waived fee arrangements to this patient for a substantial portion of my services. Physician Signature: Medical License Number:
Print Physician Name: Institution/Clinic:
ADDITIONAL INFORMATION
This completed form must be received with the specimen kit, or notify that it will be received separately no later than 72 hours of test requisition and submission. Direct any questions about this program, including questions pertaining to patients who may have extenuating circumstances, to our billing representative at phone number 888.403.6673. Note: This form does not replace the official test requisition form, which must accompany the specimen kit in order for testing to be initiated. Accepted for ASPiRA LABS by:
Name: Signature: Date:
APPLICATION FOR ECONOMIC HARDSHIP

20
Financial Assistance Plan Application
ASPiRA LABS | aspiralab.com 12117 Bee Caves Rd. Building III, Suite 100 Austin, Texas 78738
[email protected] (844) ASPiRA1 / (844) 277.4721 Fax: (512) 869.4114
Please send completed form to the address below or fax it to: 512.869.4114
PATIENT INFORMATION (PLEASE PRINT) Patient’s last name: First: Middle: q Mr.
q Mrs.
q Miss q Ms.
Marital status (circle one)
Single / Mar / Div / Sep / Wid
Birth date: Age Sex Best time to contact you: Best contact no.: / / q M q F ( ) Street address: Social Security #: Home phone no.: ( ) P.O. box: City: State: ZIP Code:
FINANCIAL INFORMATION Current annual household gross income $ Number of household members dependent on the income stated above (including the applicant) Number of dependents currently attending college Annual tuition costs for the dependents listed above (please provide documentation) Monthly mortgage, rent or property tax payment (please provide documentation) $ Monthly car payments (please provide documentation) $ Annual medical expenses not including the current bill for (Insert test name) $ In order to be considered for this program, the following documents should be supplied (*denotes required item):
□ This application form completed and SIGNED* □ A copy of your most recent tax return and/or the past 2 years W-‐2’s for all wage earners* □ Verification of mortgage/rent/property tax payment □ Verification of monthly car payments □ Verification of medical expenses □ Verification of tuition expenses □ Copy of any information provided by your insurance company related to the reimbursement of (Insert test name)
APPLICATION DECLARATION
I attest that the information provided is complete and accurate. I agree that at any time during my enrollment ASPiRA LABS may request additional documents to authenticate the statements made on my application. I understand that ASPiRA LABS reserves the right to change or discontinue this program at any time. Patient/Guardian Signature Date
FINANCIAL ASSISTANCE PLAN APPLICATION

21
Patient Welcome/Billing Letter Example
Dear Patient:
At your physician’s request, ASPiRA LABS has performed a highly specialized laboratory analysis, OVA1®
to provide important information that will contribute to how your doctor manages your treatment decisions . ASPiRA is privileged to play an active role in your care . We will continue to work with you through the reimbursement process to ensure your insurance company makes the appropriate payment on your behalf .
This letter is to let you know that we will be submitting a bill to your insurance company for payment for OVA1® testing that your physician ordered on your behalf. You should receive an Explanation of Benefits (EOB) from your insurance company that includes its initial payment policy for this procedure . An EOB is not a bill . Here is an example of an EOB:
Provider Explanation of Benefits
PRODUCT MEM . ID PATIENT NAME PAT REL PATIENT
ACCOUNTMEMBER
NAMECONTROL NUMBER
DATE RECEIVED PROVIDER OF SERVICE
CHOYC+ 12345 Jane Doe EE XXXXX Jane Doe 6/23/14 ASPIRA LABS
SERVICE DETAIL
PATIENT NAME
DATES OF SERVICE
DESCRIPTION OF SERVICE
AMOUNT CHARGED
NOT COVERED
PROV ADJ DISCOUNT
AMOUNT ALLOWED
DEDUCT/COPAY
PAID TO PROVIDER
AMT CD
PATIENT RESP .
Jane Doe 6/23/14 81503 XXX .XX XX .XX XX .XX XX .XX XX .XX XX .XX
This letter is simply to inform you that the reimbursement process often takes a significant amount of time to complete and your insurance company may ask for more information from you or your doctor .time to complete and your insurance company may ask for more information from you or your doctor .time to complete and your insurance company may ask for more information from you or your doctorNo action is required of you at this time .
Our Customer Service team is available to assist you in compiling this information for submission to your insurer .insurer .insurer We will keep you updated throughout this process . If you have questions regarding an EOB or any correspondence from your insurance company, please call our Reimbursement Specialists toll-free at 1-844-aspira1 (1-844-277-4721) or contact us via email at support@aspiralab .com .
The ASPiRA LABS Customer Service Team
12117 Bee Caves Rd . • Building III, Suite 100 • Austin, TX 78738

22
Notes:

23
Notes:

ASPiRA LABS // aspiralab .com12117 Bee Caves Rd . Building III, Suite 100
Austin, TX 78738
- - - - -
[email protected](844) ASPiRA1 // (844) 277-4721 // Fax: (512) 869-4114
Its in the earlier e-mail I sent you.
V3 .11 .2015