-
International Waldenstrom’s Macroglobulinemia Foundation: Hope,
Outreach, Support, Research
QUESTIONS & ANSWERS
Mission Statement:
To offer mutual support and encouragement to the Waldenstrom’s
macroglobulinemia community and others with an interest in the
disease.
To provide information and educational programs that address
patients’ concerns. To promote and support research leading
to better treatments, and ultimately, a cure.
Published by the International Waldenstrom’s Macroglobulinemia
Foundation This information has been provided by IWMF at no cost to
you. Please consider
joining and/or contributing to IWMF to enable us to continue to
provide materials like these to support research toward better
treatments and a cure for
Waldenstrom’s macroglobulinemia. You may join and/or contribute
at our website, www.iwmf.com or you may mail your contribution
to:
IWMF Business Office 6144 Clark Center Ave.
Sarasota, FL 34238
Ph: 941-927-4963 Fax: 941-927-4467
IWMF is a 501(c)(3) Tax Exempt Non-Profit Organization Fed ID #
54-1784426
-
FOREWORD
Questions and Answers is published by the International
Waldenstrom’s Macroglobulinemia Foundation (IWMF), a nonprofit
organization founded in 1994 by Arnold Smokler. The IWMF was
established to promote medical research on Waldenstrom’s
macroglobulinemia and to provide support to patients, their
families, and caregivers. Tax-deductible contributions are welcome
and appreciated. Information on how to contact the IWMF is provided
on the back of this booklet.
Questions and Answers was initially published in August 2003.
Mary Ann Foote, PhD, assisted with the writing of the original
manuscript. The IWMF gratefully acknowledges David Agus, MD, Morie
Gertz, MD, Robert Kyle, MD, and Alan Saven, MD, for their
thoughtful review of the original manuscript. The booklet was
revised in 2010 by Suzanne Herms and Guy Sherwood, MD, and reviewed
by Robert Kyle, MD. Copyright 2003 IWMF
-
1 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
TABLE OF CONTENTS
Introduction
.........................................................................2
What Is Waldenstrom’s Macroglobulinemia? ..................2
What Are Blood Cells? How Do They Change InWaldenstrom’s
Macroglobulinemia? .................................3
What Is The Prevalence Of Waldenstrom’sMacroglobulinemia?
...........................................................5
What Is The Prognosis For Waldenstrom’sMacroglobulinemia?
...........................................................6
Are There Any Known Risk Factors For DevelopingWaldenstrom’s
Macroglobulinemia? .................................7
What Are The Signs And Symptoms?
...............................8
How Is Waldenstrom’s MacroglobulinemiaDiagnosed And Monitored?
............................................12
How Is Waldenstrom’s Macroglobulinemia Treated?
...............................................................................14
What Are Clinical Trials? Are There Any ForWaldenstrom’s
Macroglobulinemia? ...............................25
What Are Some Of The Emerging Therapies? .............. 27
What Other Resources Are Available?
...........................29
Glossary
..............................................................................35
References...........................................................................42
-
2
INTRODUCTION
Questions and Answers is designed to address common questions
about Waldenstrom’s macroglobulinemia (WM) for people with the
disease, their families, friends, and others. Those who are newly
diagnosed may want to read the booklet from beginning to end,
whereas those who are more familiar with the disease may focus on a
specific question.
Answering questions about this disease requires the use of terms
that may not be familiar to some readers. Terms related to WM are
italicized the first time they are used and defined in the glossary
found at the end of this booklet. Should readers have other
questions not found in this booklet or seek further explanation on
a particular topic, they should direct their inquiries to a
healthcare professional.
WHAT IS WALDENSTROM’S MACRO-
GLOBULINEMIA?
Waldenstrom’s macroglobulinemia (WM) is a rare white blood cell
cancer defined by the World Health Organization (WHO) and the
Revised European American Lymphoma (REAL) classification as a
lymphoplasmacytic lymphoma, a type of non-Hodgkin’s lymphoma. It is
often compared with other white blood cell cancers, especially
chronic lymphocytic leukemia and multiple myeloma. A defining
characteristic of the disease is the presence of an elevated IgM
immunoglobulin protein, also referred to as an IgM paraprotein or
monoclonal IgM.
Dr. Jan Gosta Waldenström first described the disease that bears
his name in 1944. He described two patients who experienced
bleeding from the mouth, nose, and retina of the eye. They also
-
3 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
had enlarged lymph nodes and several abnormal laboratory values
including low hemoglobin, low platelet counts, and an increase in
an unknown protein which was later identified as the large (macro)
immunoglobulin IgM.
WHAT ARE BLOOD CELLS? HOW DO THEY
CHANGE IN WALDENSTROM’S
MACROGLOBULINEMIA?In order to understand this rare disease, one
needs to understand blood components, which are summarized briefly
in this section. More information on blood, blood components, and
blood tests can be found in the papers “Blood Tests” by Barb Hauser
and “Immunoglobulins” by Guy Sherwood, MD, available from the IWMF
at the foundation’s website www.iwmf.com.
Blood has both a liquid portion and a solid portion. The liquid
(plasma) portion of the blood contains proteins such as
immunoglobulins, clotting factors, hormones, and albumin, as well
as electrolytes such as sodium, chloride, potassium, calcium, and
magnesium. When clotting factors are removed from plasma, the
remaining liquid is called serum. The solid portion of the blood
contains blood cells such as red blood cells (erythrocytes), white
blood cells (leukocytes), and platelets (thrombocytes).
The different types of blood cells perform different functions.
Red blood cells deliver oxygen from the lungs to other areas of the
body. Hemoglobin is a large iron-containing protein found in red
blood cells and is the carrier molecule for oxygen. Platelets help
blood to clot. When a blood vessel is broken, platelets bind to the
broken blood vessel surface, clump together, and stop the bleeding.
Both red blood cells and platelets are found primarily in the
blood,
-
4
whereas some white blood cells are found not only in the blood
but also in other body tissues. The primary function of all white
blood cells is to eliminate foreign substances such as bacteria and
fungi from the body. Neutrophils, eosinophils, basophils,
monocytes, macrophages, T-lymphocytes, natural killer cells, and
B-lymphocytes are all different types of white blood cells.
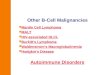
Red blood cells, platelets, and white blood cells develop from a
primitive blood cell called the hematopoietic stem cell. These stem
cells are unique because they are also able to produce other blood
stem cells. The process of blood cell development, called
hematopoiesis, is illustrated in Figure 1.
Hematopoiesis occurs primarily in the bone marrow, a spongy
tissue located inside the bones. Hematopoiesis occurs in all bones
at birth. By adulthood, however, it occurs only in the backbone
(vertebrae), ribs, skull, hip, shoulder, breastbone (sternum), and
the long bones (femur and humerus).
Figure 1. Hematopoiesis, the process of blood cell
differentiation.
-
5 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
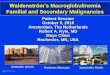
Normally, B-lymphocytes develop into plasma cells as shown in
Figure 2. The role of plasma cells is to secrete immunoglobulins,
which are proteins also referred to as antibodies, that are
produced when a foreign substance or antigen is detected in the
body. The immunoglobulins coat the foreign substance, such as a
bacterium, so that other types of white blood cells can eliminate
it. Five classes of immunoglobulins have been identified, IgA, IgD,
IgE, IgG, and IgM.
Figure 2. Plasma cell development.
In WM, the cancerous B-lymphocytes do not develop properly into
normal plasma cells but into a type of cancer cell referred to as a
lymphoplasmacytic cell. These cells invade the bone marrow and
other lymphoid organs, such as the spleen and lymph nodes, and make
and release increased amounts of IgM into the blood. This increased
release of IgM may result in thickening of the blood
(hyperviscosity).
WHAT IS THE PREVALENCE OF
WALDENSTROM’S MACROGLOBULINEMIA?WM is a rare cancer. Analyses of
new cancers reported in the United States show that blood cell or
hematologic cancers such as leukemias, lymphomas, and multiple
myeloma account for about 10% of all new cancers, and WM accounts
for only 1.4% of hematologic cancers or 0.1% of all cancers.1,2
These numbers mean that approximately 1,500 people in the United
States are diagnosed
-
6
with this disease each year.2 In comparison, lung cancer
accounts for 15%, breast cancer 13%, prostate cancer 13%, and colon
and rectal cancer 10% of all newly diagnosed cancers.1
WHAT IS THE PROGNOSIS FOR
WALDENSTROM’S MACROGLOBULINEMIA?The prognosis is variable.
Although the median survival was reported as 5-7 years in the older
literature,2 the survival time has been increasing steadily because
of better treatments, and many patients live for more than 20
years.
Several studies have attempted to determine characteristics or
prognostic factors that affect disease severity. The most recent
was an international study that developed the International
Prognostic Scoring System for Waldenstrom’s Macroglobulinemia
(ISSWM) for WM. This study did not include asymptomatic patients
who had not yet received treatment. Five adverse survival factors
were identified: advanced age (>65 years), hemoglobin level less
than or equal to 11.5 g/dL, platelet count less than or equal to
100 x 109/L, beta-2 microglobulin more than 3 mg/L, and serum
monoclonal IgM concentration more than 7.0 g/dL. Based on these
factors, patients were categorized into three groups. Low risk
patients at treatment presented with not more than one adverse
factor and age less than or equal to 65 years – these patients had
a 5-year survival rate of 87%. Intermediate risk patients had two
adverse factors or age older than 65 years and had a 5-year
survival rate of 68%. High risk patients had three or more adverse
factors and had a 5-year survival rate of 36%.3
-
7 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
ARE THERE ANY KNOWN RISK FACTORS
FOR DEVELOPING WALDENSTROM’S
MACROGLOBULINEMIA?A risk factor is anything that increases the
chances of developing a disease. The only risk factors that have
been identified in WM are male sex, increasing age, white race, and
a diagnosis of monoclonal gammopathy of undetermined significance
(MGUS) of IgM class.4
The risk is higher in men than in women, with the annual
age-adjusted incidence approximately twice as high in men as in
women.4,5,6 The incidence of the disease is also higher in older
people. The median age at diagnosis is 62 although patients as
young as 18 have been reported. The annual incidence increases
dramatically as age increases.6 Race appears to be a risk factor,
as the incidence is higher in whites than in blacks.4,5 Reliable
figures for other races are not available.
People with IgM MGUS have an increased risk of developing WM. In
one long-term study of IgM MGUS, the incidence of progression to WM
and other lymphoid malignancies was 10% at 5 years, 18% at 10
years, and 24% at 15 years.7
Several reports suggest a link between WM and genetic,
environmental, and viral factors. Research findings report an
element of familial susceptibility that is more significant than
with other B-lymphocyte cancers.8 Some evidence links the disease
to a deletion in part of chromosome 6, although this abnormality is
not present in all cases of WM.9 Environmental factors such as
radiation exposure and occupational exposure to leather, rubber,
paints, and dyes have also been implicated in some studies, as have
viral factors such as hepatitis C and human herpes virus
8.2,10,11,12 However, none of these factors has consistently been
determined to increase the risk.
-
8
WHAT ARE THE SIGNS AND SYMPTOMS?People with WM can have a wide
variety of signs and symptoms, the most common of which is fatigue,
although many patients present with no symptoms at all. Other signs
and symptoms are listed in Table 1. Most of these are attributable
to cancer cells that replace normal cells in the bone marrow and
secrete increased amounts of IgM.
Abnormal bleeding from gums and nose
Increased concentration of IgM
Decreased red blood cell count Neurological symptomsEnlarged
liver Visual impairmentEnlarged lymph nodes WeaknessEnlarged spleen
Weight lossFatigue Night sweats
Table 1. Common signs and symptoms of Waldenstrom’s
macroglobulinemia
There are several distinguishing features of WM, found in some,
but not all patients. These include hyperviscosity syndrome,
peripheral neuropathy, cryoglobulinemia, cold agglutinin disease,
and amyloidosis.
Hyperviscosity syndrome occurs in approximately 10-30% of
patients2 as a result of the increased IgM concentration, which
also ultimately results in an increased plasma volume. IgM
molecules are also large and contribute to the increase in serum
viscosity. Signs and symptoms of hyperviscosity include chronic
bleeding from the nose, gums, and, less commonly, the
gastrointestinal tract; headache; ringing in the ears (tinnitus);
dizziness (vertigo); impaired hearing; blurring or loss of vision;
distended, sausage-
-
9 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
shaped veins in the retina; and swelling of the optic disk at
the back of the eye (papilledema). In severe cases, heart failure,
sleepiness (somnolence), stupor, and coma can develop. Symptoms of
hyperviscosity occur most commonly at IgM concentrations greater
than 5,000 mg/dL; however, such concentrations are not always
associated with hyperviscosity.
Peripheral neuropathy (PN) is a commonly reported complication
of WM – the reported incidence varies but is generally about
20-30%. The clinical features of PN are predominantly sensory, with
abnormal sensations (paresthesias) such as burning, prickling,
itching, tingling, or numbness that are usually first noticed in
the feet. The paresthesias are symmetric, affecting both feet
equally, and slowly progress to the upper legs, hands, and arms.
Strength is often normal. The PN in WM is usually caused by the
targeting of specific antigens on the nerve coating (myelin) by the
circulating IgM, leading to nerve dysfunction.13 Symptoms can be
reduced with gabapentin (Neurontin), pregabalin (Lyrica),
amitriptyline (Elavil), opiate drugs, and others. These medications
mask the symptoms but do not slow the progression of PN. The
treatment of IgM-related neuropathy is directed toward the
reduction of circulating IgM, usually by either plasmapheresis or
rituximab-based therapy, both of which are further explained in the
section of this booklet entitled “How Is Waldenstrom’s
Macroglobulinemia Treated?”
Cryoglobulinemia (often referred to as cryo) literally means
“cold antibody in the blood” and refers to the physical and
chemical properties of the antibodies involved. Cryoglobulins
precipitate at temperatures below body temperature and then
re-dissolve upon warming. Cryo is most often due to unknown causes
but may in some cases be associated with an underlying disease such
as WM.
-
10
Frequently, the type of cryo associated with WM does not cause
symptoms until the concentration of antibody reaches high levels,
at which point it can produce a variety of symptoms because the
precipitated antibody physically obstructs smaller blood vessels.
When present, symptoms can include blueness of hands and feet from
the cold, Raynaud’s phenomenon (whiteness and numbness of the
fingers and toes from the cold), purpura (purple skin marks),
bleeding, ulcers, and gangrene of the fingers and toes. WM patients
should be tested for cryoglobulinemia at diagnosis, since it can
not only complicate treatment but can also affect the results of
other laboratory testing.
Cold agglutinin disease (CAD) is sometimes confused with
cryoglobulinemia because both conditions involve antibodies
(usually of the IgM-type) that react at lower temperatures.
However, the antibodies responsible for cold agglutinin disease are
specifically directed against proteins (antigens) found on one’s
own red blood cells. It is this characteristic that is responsible
for one of CAD’s primary manifestations: hemolytic anemia. Cold
agglutinins occur naturally in nearly everyone, but at low levels
that seldom cause problems. High concentrations can cause anemia
because red blood cells are destroyed faster than the bone marrow
can replace them. Clinical signs and symptoms of CAD vary according
to the severity of the disease. These may include Raynaud’s
phenomenon, painful fingers and toes, anemia, fatigue, shortness of
breath, jaundice, and dark urine caused by the presence of
hemoglobin. A few of these symptoms, such as Raynaud’s, are similar
to those of cryoglobulinemia because both conditions can affect the
circulation. Hemolytic anemia is not, however, a consequence of
cryoglobulinemia.
-
11 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Amyloidosis is a group of diseases caused by the buildup of an
abnormal protein, called amyloid, in various tissues and organs of
the body. The amyloid protein forms abnormal fibers that may injure
certain tissues and organs or interfere with their normal function.
The protein may be deposited in a localized area or systemically
(throughout the body). The most common tissues and organs involved
are the kidneys, heart, gastrointestinal tract, peripheral nerves,
and liver. Symptoms can vary widely, based on which tissues and
organs have the abnormal protein deposits. Clinical signs and
symptoms of amyloidosis may be vague, such as weakness, fatigue,
weight loss, shortness of breath, abnormal sensations in the feet,
enlarged liver and/or spleen, bleeding under the skin, and anemia.
More specific signs and symptoms might include swelling of the
extremities, an enlarged tongue, carpal tunnel syndrome, food
malabsorption, skin thickening, unexplained congestive heart
failure, and unexplained kidney failure.
Patients may also have kidney, gastrointestinal, eye, or skin
involvement. Bone lesions are uncommon and reported in less than 5%
of cases.2 Rarely, tumors with WM-like cells have been reported in
the spine, breast, extremities, palate, etc. Another unusual
complication of WM is Bing-Neel syndrome, which involves
infiltration of the central nervous system (brain and spinal cord)
by WM cells and/or IgM deposition, as well as hyperviscosity.
Complications of Bing-Neel syndrome may include mental
deterioration, confusion, visual disturbances, irritability,
personality changes, convulsions, and coma.
-
12
HOW IS WALDENSTROM’S
MACROGLOBULINEMIA DIAGNOSED
AND MONITORED?The diagnosis of WM is made upon demonstration of
bone marrow infiltration with lymphoplasmacytic lymphoma cells, the
presence of an IgM monoclonal protein regardless of its
concentration, and supporting immunophenotypic analysis (flow
cytometry or immunohistochemistry) that looks for specific surface
proteins, called cluster differentiation (CD) markers, on the
lymphoplasmacytic cells of the bone marrow.4 Each type of cancer,
including B-lymphocyte cancers such as WM, has its own identifying
pattern of CD markers, and this pattern helps to confirm the
diagnosis. The typical CD pattern for WM is CD19+, CD20+, CD5-,
CD10-, CD22+, CD23-, and CD79+ (+ means the marker is present on
the cell, whereas – means it is absent), although some variation
from this typical pattern can occur. Laboratory tests of blood,
serum, and urine and a bone marrow aspiration and biopsy are used
for these determinations. Imaging studies (X-rays, CT scans, and
PET scans) of the chest, abdomen, pelvis, and other areas may show
evidence of enlarged lymph nodes, enlarged spleen, or soft tissue
tumors.
In Table 2 common laboratory tests that may be used to diagnose
or monitor WM are listed, as well as normal reference values. Other
laboratory tests, such as metabolic panels and liver function
studies may also be performed.
It is important to realize that laboratory reference ranges are
not nationally standardized and therefore may vary slightly from
laboratory to laboratory. Units of measurement used for reporting
laboratory values may also vary. Generally speaking, patients
should follow the trends of their laboratory test results over
time.
-
13 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
All laboratory tests have an inherent degree of imprecision,
some more than others, and depend on proper specimen collection,
handling, and interpretation for accurate results. If a laboratory
test result is in doubt, it should be repeated.
More information on laboratory tests can be obtained from the
paper titled “Blood Tests” by Barb Hauser14 and from the IWMF
booklet, Medical Tests in Waldenstrom’s Macroglobulinemia Including
Glossary of Medical Terms Relating to Tests by Guy Sherwood,
MD.15
Blood Test Normal Value WM AbnormalityWhite blood cell (WBC)
count
3.5-6.1 million/ mL May be decreased
WBC differential Neutrophils 50%-70% of WBC count May be
decreased Bands 0%-4% of WBC count May be decreased Eosinophils
0%-7% of WBC count May be decreased Basophils
-
14
As mentioned above, a bone marrow aspiration and biopsy are
absolute requirements to confirm the diagnosis of WM. These
procedures typically involve inserting a needle into a bone and
removing a piece of bone and some bone marrow, usually from the
back of the pelvis (iliac crest). Evaluation of this material under
a microscope will demonstrate the lymphoplasmacytic cells
characteristic of WM. While a bone marrow aspiration and biopsy are
essential for diagnosis, they are generally not used for monitoring
because of their invasive nature, except in special circumstances
such as a clinical trials protocol.
HOW IS WALDENSTROM’S
MACROGLOBULINEMIA TREATED?There is no known cure for WM.
Initiating treatment early in the course of the disease in an
asymptomatic patient does not prolong survival; therefore,
treatment is delayed until the onset of symptomatic disease. Some
patients with increased amounts of IgM or increased numbers of
lymphoplasmacytic cells in the bone marrow (measured as % of bone
marrow infiltration) may remain stable and continue to be
asymptomatic for a long time. Such patients are considered to be on
“watch and wait,” which means that their disease status and their
health are monitored regularly for changes, sometimes for years,
before any treatment is initiated.
Signs and symptoms that may require the initiation of treatment
include the following: weakness, fatigue, fever, night sweats,
weight loss, bleeding from the nose or gums, blurred vision, bulky
(enlarged) lymph nodes, greatly enlarged liver or spleen,
hemoglobin less than 10 g/dL, platelets less than 100,000/µL,
hyperviscosity, severe peripheral neuropathy, amyloidosis, and
symptomatic cryoglobulinemia or cold agglutinin disease.
-
15 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Available treatment options include chemotherapy;
corticosteroids; biologic therapy; immunomodulatory drugs;
proteasome inhibitors; radiation; surgical and other procedures
such as plasmapheresis, splenectomy, or stem cell transplantation;
and newer emerging therapies. The booklet Treatment Options16,
written primarily for patients, is available through the IWMF. The
booklet Review of Therapy17, written for doctors and scientists by
Morie A. Gertz, MD, and also available from the IWMF, includes a
complete review of therapy options.
The success of a selected treatment is measured by the degree of
disease response to the therapy. “Progressive disease” is
characterized by an increase in serum monoclonal IgM of 25% or more
and confirmed by a second measurement, or by progression of
clinically significant signs or symptoms. “Stable disease” is
defined as either less than 25% reduction or a less than 25%
increase in serum monoclonal IgM without progression of lymph node
or organ enlargement or other clinically significant signs or
symptoms. A “minor response” is a reduction in serum monoclonal IgM
equal to or greater than 25%, but less than 50%, and no new signs
or symptoms of active disease. A “partial response” is a reduction
in serum monoclonal IgM equal to or greater than 50%, a 50%
decrease in lymph node or organ enlargement on physical examination
or on CT scan, and no new signs or symptoms of active disease. A
“complete response” is categorized by a disappearance of serum and
urine monoclonal IgM, absence of malignant cells in the bone
marrow, resolution of enlarged lymph nodes or organs confirmed by
CT scan, and no signs or symptoms of disease. Reconfirmation of
complete response is required six weeks later.18
-
16
Chemotherapy
One of the most common options used in the treatment of WM is
chemotherapy. In Table 3 selected drugs currently used in the
treatment of WM are listed. The two main classes of chemotherapy
are alkylating agents and nucleoside analogs. Alkylating agents
include chlorambucil, cyclophosphamide, and melphalan. Nucleoside
analogs include fludarabine, cladribine (also referred to as 2CdA),
and pentostatin.
Chlorambucil was historically the most common alkylating agent
used in treating WM. Chlorambucil has produced minor and partial
responses in 60-70% of patients; however, complete responses are
rare. Response to chlorambucil therapy occurs slowly and may take
from several months to more than one year. The drug is administered
orally either as low-dose, daily therapy or as pulse therapy, which
consists of a higher dose administered daily for 7 days and
repeated every 6 weeks. The optimal length of chlorambucil therapy
is unknown. Treatment is usually administered until the reduction
of IgM is maximal and at a stable (plateau) concentration.
Treatment is restarted as symptoms warrant. Maintenance therapy
with chlorambucil is not recommended because prolonged
administration is associated with an increased risk of developing
complications such as abnormal or defective formation of bone
marrow cells (myelodysplasia) or a secondary leukemia.
Alkylating agents have been used in varying combinations with
other drugs, such as nucleoside analogs, vincristine, doxorubicin,
corticosteroids, and/or rituximab.
-
17 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Generic Name (Brand Name)
Dosage Form Possible Side effects
Alkylating AgentsChlorambucil (Leukeran) Tablet Nausea,
vomiting, decreased
white blood cell and/or plate-let count, skin rashes
Cyclophosphamide(Cytoxan)
Infusion or tablet
Nausea, vomiting, decreased white blood cell and/or plate-let
count
Melphalan (Alkeran) Infusion or tablet
Decreased white blood cell and/or platelet count
Nucleoside AnaloguesFludarabine (Fludara) Infusion or
tabletDecreased white blood cell and/or platelet count, fatigue,
neurotoxicity, hemolytic anemia
Cladribine (Leustatin) Infusion Decreased white blood cell
and/or platelet count, fatigue, neurotoxicity
Pentostatin(Nipent)
Infusion Nausea, vomiting, skin rashes, decreased white blood
cell and/or platelet count, fatigue
Table 3. Selected chemotherapy agents used in the treatment of
Waldenstrom’s macroglobulinemia
The nucleoside analogs include fludarabine, cladribine, and
pentostatin. Compared with alkylating agents, nucleoside analogs
provide patients with response rates of 40-80%,2 but with a more
rapid onset of response. Therefore, fludarabine, cladribine, and
pentostatin may be the treatment of choice for people who have
serious complications and require rapid response. The nucleoside
analogs have also been effective in approximately 40% of people who
had disease progression on chlorambucil therapy.19 One of the most
common side effects with nucleoside analog therapy is suppression
of blood cell production by the bone marrow. This
-
18
side effect increases one’s chance of developing an infection.
When treatment ceases, blood cell production usually resumes. There
is a risk of developing myelodysplasia or secondary leukemia in WM
patients treated with nucleoside analogs. There may also be an
increased incidence of transformation to a more aggressive lymphoma
following treatment with these drugs. If autologous stem cell
transplantation is being considered, prior exposure to purine
nucleoside analogs is not advisable because of their effect on the
ability to procure hematopoietic stem cells.
Nucleoside analogs are often used in varying combinations with
other drugs, such as alkylating agents, corticosteroids, and/or
rituximab.
Corticosteroids
Although corticosteroids such as prednisone or dexamethasone are
rarely used alone in treating WM, they have been administered in
combination with other therapies. Corticosteroids or combination
alkylating agent-corticosteroid therapy may be beneficial in people
who also have or who develop selected hematologic complications
that are associated with WM (cryoglobulinemia, cold agglutinin
disease, thrombocytopenia).
Biologic Therapy
Biologic therapy is a treatment that causes activation of the
body’s own disease fighting systems. Biologic therapies for WM
include interferon, alemtuzumab, and rituximab and are listed in
Table 4.
Interferon, a hormone-like protein produced by white blood cells
to help the immune system fight infections, has been successful
in
-
19 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
treating a small number of patients,2 although it is seldom used
at present. Studies reported that responses occurred 3-6 months
after the start of therapy. Typical side effects included fever,
lethargy, anorexia (poor appetite), muscle and joint aches, and
bone marrow suppression. Low doses of interferon were better
tolerated.
Alemtuzumab (Campath) is a monoclonal antibody therapy that
targets the CD-52 antigen that is expressed on WM cells and on mast
cells, which are frequently found in association with WM cells in
the bone marrow. Initial results indicate that this treatment can
be helpful in WM, although toxicity is a problem. More studies are
needed.
Rituximab (Rituxan) is a monoclonal antibody therapy targeted
against the CD-20 antigen located on many lymphoid cancer cells, as
well as on normal B-lymphocytes, and is effective in treating
several types of lymphoma. Responses to rituximab therapy alone
have been reported in 40-75% of patients with WM, including those
who were previously treated with an alkylating or nucleoside analog
agent.20 Rituximab is now commonly used as a first-line treatment
in WM because it is less toxic than either alkylating agents or
nucleoside analogs; it has also been evaluated in combination with
these drugs, as well as with some of the emerging therapies. The
most typical side effects of rituximab occur during the first
infusion of the drug, when patients may experience chills or fever.
Subsequent infusions usually cause fewer side effects. If a WM
patient with high IgM and/or hyperviscosity elects to undergo
rituximab treatment, his physician needs to be aware of a
phenomenon known as rituximab “flare,” which causes a rapid but
temporary increase in IgM, potentially resulting in increased serum
viscosity or other IgM-associated complications.
-
20
Some studies have suggested that maintenance rituximab may
prolong response times and even overall survival in patients with
certain B-lymphocyte lymphomas. Although protocols vary, typical
maintenance consists of a single rituximab infusion every two or
three months for up to two years or more following the end of the
primary chemotherapy regimen. At present there are no studies that
confirm increased response times or overall survival for WM
patients.
There are several second and third generation monoclonal
antibodies similar to rituximab that also target the CD-20 antigen
on B-lymphocytes. As of 2010, a few of these, including ofatumumab
(Arzerra), are either still in clinical trials or have been
recently approved for some B-lymphocyte cancers; it remains to be
seen whether they will be more effective than rituximab or will
have fewer infusion-related side effects.
Generic Name (Brand Name)
Dosage Form
Possible Side effects
Interferon alfa (Roferon,Intron)
Injection Flu like symptoms, fever, nausea, vomiting, decreased
appetite, diar-rhea, dizziness, decreased blood counts
Alemtuzumab (Cam-path)
Infusion or Injection
Shortness of breath, chills, facial flushing, fatigue, fever,
headache, decreased blood pressure, nausea, vomiting, itching,
decreased blood counts
Rituximab (Rituxan) Infusion Shortness of breath, chills, facial
flushing, fatigue, fever, headache, decreased blood pressure,
nausea, vomiting, itching
Table 4. Selected biologic agents used in the treatment of
Waldenstrom’s macroglobulinemia
-
21 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Immunomodulatory Drugs
Immunomodulatory drugs kill tumor cells by four described
mechanisms of action: they starve the tumor cells by inhibiting the
development of blood vessels that feed them (anti-angiogenic
effect); they enhance the tumor killing properties of T-lymphocytes
and natural killer cells; they block some of the interactions
between tumor cells and other cells in the bone marrow environment;
and finally they appear to directly kill tumor cells by a mechanism
not yet fully understood. The best known immunomodulatory drug is
thalidomide (Thalomid) which was originally developed in the 1950s
as a sedative but was removed from the market when it was
discovered to be responsible for birth defects. It was subsequently
found to be effective in the treatment of multiple myeloma, a
disease closely related to WM. It has shown promise when used in
combination with other drugs, but its major side effects are
constipation and peripheral neuropathy. Several newer
thalidomide-type drugs have been developed, such as lenalidomide
(Revlimid) and pomalidomide (Actimid). These are expected to be as
effective as thalidomide but with fewer side effects.
Proteasome Inhibitors
Bortezomib (Velcade) is the first of a new class of drugs called
proteasome inhibitors. Proteasomes are large protein complexes
present in all cells that help regulate cell growth and death. When
proteasomes are inhibited with bortezomib, many types of cancer
cells, including those common to lymphoma and multiple myeloma,
undergo apoptosis (cell death). Normal non-cancerous cells appear
better able to tolerate the drug without significant difficulties.
Side effects such as peripheral neuropathy, temporary bone
marrow
-
22
suppression, and constipation have occurred with bortezomib.
Clinical trials using modified dosing schedules have greatly
reduced the incidence of peripheral neuropathy. Bortezomib has also
been combined with other therapies such as rituximab, leading to
better responses. Carfilzomib is a newer proteasome inhibitor
currently being evaluated in clinical trials, and oral proteasome
inhibitors are also being developed.
Radiation Therapy
Radiation therapy has been used in WM, primarily for the
selective and targeted reduction of enlarged lymph nodes and in the
uncommon instances of tumors developing in other sites such as the
spine. Total body irradiation is not used in the management of
WM.
Surgical and Other Procedures
Procedures that have been used include plasmapheresis,
splenectomy, and stem cell transplantation.
Plasmapheresis involves removal of blood from the body,
separation of the liquid (plasma) portion from blood, replacement
of plasma (usually with albumin and sodium chloride solutions), and
return of the remaining blood components to the body.
Plasmapheresis can be thought of as a form of dialysis where the
primary aim is the “filtering out” or removal of IgM from the
circulation. Plasmapheresis is widely used to reduce the symptoms
associated with hyperviscosity syndrome. In general, plasmapheresis
is initiated just prior to or concurrent with chemotherapy;
however, some patients have been treated successfully with only
-
23 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
plasmapheresis, particularly if they cannot tolerate more toxic
therapies. If performed alone, plasmapheresis must be repeated
frequently to maintain acceptable IgM levels because the procedure
has no effect on the growth and survival of WM cells.
Surgical removal of the spleen (splenectomy) has been effective
in reducing the IgM concentration for select cases after failure of
chemotherapy because the spleen is a major source of IgM-producing
cells. Splenectomy is usually considered only to relieve symptoms
of a significantly enlarged spleen and certain blood count
abnormalities, particularly the case of low platelets
(thrombocytopenia).
Stem cell transplants are feasible in WM. Preliminary data
suggest that a larger number of complete responses have been
obtained with stem cell transplant than with standard chemotherapy,
although there are serious side effects associated with
transplantation.
Autologous stem cell transplantation reinfuses a patient’s own
stem cells collected before he has undergone high-dose chemotherapy
to destroy the tumor cells in the bone marrow. Allogeneic stem cell
transplantation uses donor stem cells from either a family member
(usually) or an unrelated individual. A newer type of allogeneic
stem cell transplant, called non-myeloablative or “mini-allo”
transplant does not completely clear the recipient’s bone marrow
before infusion of the stem cells; it is believed that the donor
stem cells will recognize any remaining tumor cells in the marrow
as foreign and destroy them. Mini-allo transplant is less toxic
than a regular allogeneic transplant and recovery time tends to be
less.
The major toxicities of stem cell transplantation occur because
the patient’s immune system is severely depressed during the
procedure and for some time afterward. Because an allogeneic
transplant
-
24
uses donor stem cells, there is also a risk of serious
complications from graft vs. host disease (GVHD), which occurs when
the donor’s immune cells see the host’s cells as foreign and attack
them. Graft vs. host disease can be acute or chronic. Both forms
bring with them an increased risk of infections, either because of
the process itself or its treatment with immunosuppressive
drugs.
While autologous stem cell transplantation is used more
frequently in WM, allogeneic stem cell transplantation for WM is
usually recommended only in the context of a clinical trial or in
cases where aggressive disease is not responding to other
treatment.
Approach to Therapy
Initiation of therapy should not be based on IgM levels alone,
and asymptomatic patients should be monitored on a regular
basis.
Individual patient considerations need to be considered when
deciding on a first-line treatment – these include the presence of
low blood counts, need for rapid disease control, age, overall
general health, and possibility for future autologous stem cell
transplantation. Single-agent rituximab therapy may be the
preferred initial treatment for most patients with WM. Certain
patients with low-risk disease may be candidates either for
single-agent rituximab or for single-agent chlorambucil therapy
because of associated health problems. The presence of low blood
counts and relatively low levels of IgM may favor rituximab,
whereas slow progression and older age may favor the use of
chlorambucil. When rapid disease control is needed, the addition of
cyclophosphamide to rituximab or the combination of rituximab with
a nucleoside analog, with or without cyclophosphamide, may also be
appropriate.
-
25 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
The choice of therapy after relapse is also dependent on several
factors. Reuse of a first-line single agent therapy or combination
is reasonable if a patient achieved a response that lasted for 12
months or more; otherwise, use of an alternate single agent or
combination is recommended. It is clear, however, that combination
therapies using two or more agents are more effective than
single-agent therapies.
The use of stem cell transplantation in WM requires a more
extensive evaluation and selection of individual patients, focusing
primarily on patients with high-risk disease or on young patients
with aggressive disease.21
WHAT ARE CLINICAL TRIALS? ARE THERE
ANY FOR WALDENSTROM’S MACRO-
GLOBULINEMIA?Clinical trials are research studies designed to
answer questions about diseases and new ways to treat diseases.
Several different types of clinical trials for cancer are
available, including treatment, prevention, screening, and
quality-of-life or supportive care trials. Treatment trials are
designed to evaluate new treatments such as new drugs or new
combinations of drugs. Prevention trials are designed to evaluate
ways of lowering the risk of developing cancer. Screening trials
find the best way of diagnosing cancer. Finally, quality-of-life
and supportive care trials identify ways of improving the comfort
and quality of life of cancer patients.
Clinical trials for cancer treatment are conducted in four
phases. Phase I trials are the first step in testing a new
treatment in humans. Researchers evaluate what dosages are safe,
how new agents
-
26
should be administered (by mouth, infusion into a vein,
injection subcutaneously or into a muscle) and how often the drugs
are to be given to the patient. Researchers primarily monitor
harmful side effects. The dose of the new therapy or technique is
increased a little at a time. The highest dose with an acceptable
level of side effects is determined to be appropriate for further
testing. Phase I trials usually include only a limited number of
patients and are often carried out at a few large academic medical
centers.
Phase II trials attempt to determine whether the new agent or
technique works for a specific type of cancer and continue to study
its safety and effectiveness.
Phase III trials compare the treatment outcomes of patients
taking the new therapy with results of people taking standard
treatment. Participants are randomly assigned to the standard (also
called control) group or to the new treatment group. This method,
called randomization, helps to avoid bias and ensures that human
choices or other factors do not affect the study’s results. In most
cases, studies move into Phase III testing only after they have
shown promise in Phases I and II. Phase III trials often include
large numbers of participants.
Phase IV trials occur after a treatment has been approved and is
being marketed. The drug’s maker may study it further to evaluate
the side effects, risks, and benefits over a longer period of time
and in a larger number of people than in Phase III clinical trials.
Because of the small WM patient population, Phase III and Phase IV
trials for the disease are very uncommon.
Placebos or “sugar pills” are not normally used in cancer
trials. The details of the clinical trial, including the
advantages, disadvantages, and possible treatment-related side
effects, must be understood by
-
27 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
the participant before he or she enrolls in a clinical trial. A
person enrolled in a clinical trial can withdraw from the trial at
any time without penalty.
Cancer clinical trials change frequently. A trial will be
stopped after enough people are enrolled to answer the research
question. The results of one trial may lead to a new question that
necessitates a new trial. For example, a new drug may show promise
in one condition and merit testing in a related condition.
Therefore, it is important to obtain the most current information
from resources that are routinely updated. General information on
clinical trials and specific information on clinical trials
enrolling people with WM can be found on the IWMF website at
www.iwmf.com, at the National Cancer Institute’s Cancer Trials
website at www.cancer.gov/clinical_trials, or from the National
Institutes of Health website at www.clinicaltrials.gov.
WHAT ARE SOME OF THE EMERGING
THERAPIES?A number of new regimens and therapies are currently
being studied, a few of which will be covered here. It remains to
be seen how these will become part of the treatment protocol for WM
in the future.
Radioimmunotherapy combines a monoclonal antibody, such as
rituximab or similar agent, with a radioactive particle, called a
radioisotope. This radioisotope-antibody targets and binds to the
CD-20 antigen present on B-lymphocytes, delivering a dose of
radiation to the targeted cells. Two such radioimmunotherapy
treatments are called Zevalin and Bexxar. Very good results have
been achieved from using these treatments in certain lymphomas,
-
28
including a significant number of complete responses. The
difficulty in using these agents is that patients who have
extensive bone marrow involvement may not be able to receive them
without resulting in significant suppression of the bone marrow –
the radioactive particles also destroy surrounding normal bone
marrow cells.
Bendamustine (Treanda) shares characteristics of both an
alkylating agent and a nucleoside analog. Although it was developed
in Germany in the 1960s, it has only recently been approved for use
in chronic lymphocytic leukemia and in follicular lymphoma that is
resistant to treatment with rituximab. It is being used for WM by
some investigators, primarily in Europe.
There are several molecular signaling pathways in B-lymphocytes
that can influence cell growth and survival. Some of these may be
over- or under-expressed in malignant cells, and this abnormal
expression can impact the development and growth of malignant
cells. Several new agents that alter these signaling pathways,
among them enzastaurin, Everolimus (RAD001), perifosine, oblimersen
sodium (Genasense), and certain histone deacetylase inhibitors
(HDACs), are in the process of being tested in WM patients.
Vaccine therapy is currently in development for other types of
B-lymphocyte lymphomas. These lymphomas develop on their surfaces
certain molecules that distinguish them from healthy cells. A
vaccine is created specifically for an individual patient from the
patient’s own tumor cells and is designed to mobilize the patient’s
immune system to attack the malignant cells. A vaccine is typically
administered following treatment designed to minimize the disease.
After a rest period the vaccine is administered. The goal is to
prevent recurrence or at least to extend the response time.
-
29 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
WHAT OTHER RESOURCES ARE
AVAILABLE?In addition to this booklet, information on living
with cancer (and more specifically with WM) can be obtained from
several organizations and on the Internet. The following list is a
sampling of available resources. Information can also be obtained
from cancer treatment facilities and healthcare professionals.
Organizations
International Waldenstrom’s Macroglobulinemia Foundation
The International Waldenstrom’s Macroglobulinemia Foundation
(IWMF) is a nonprofit organization founded in 1994 by Arnold
Smokler. The IWMF provides numerous services for people with WM
including patient and caregiver support groups, dissemination of
information, and promotion of research. The IWMF distributes
information to members through newsletters, handbooks, annual
conferences, conference tapes, and the Internet. Membership in the
IWMF is based on voluntary contributions that support the
administration, outreach, and education programs of the
Foundation.
International Waldenstrom’s Macroglobulinemia Foundation 6144
Clark Center Avenue Sarasota, FL 34238 Telephone number:
941-927-4963 Email address: [email protected] Internet address:
www.iwmf.com
-
30
Waldenstrom’s Macroglobulinemia Foundation of Canada
The Waldenstrom’s Macroglobulinemia Foundation of Canada (WMF
Canada) is the Canadian chapter of the IWMF. Members of WMF Canada
are automatically also members of the IWMF. The group was formed in
order to support WM research, to provide support to patients and
caregivers, and to issue tax receipts for contributions that are
deductible for income tax purposes by Canadian taxpayers.
Waldenstrom’s Macroglobulinemia Foundation of Canada 260
Dalewood Drive Oakville, ON L6J 4P3 Canada Telephone number:
905-337-2455 Internet address: www.WMFC.ca
Lymphoma Research Foundation
The mission of the Lymphoma Research Foundation (LRF) is to
eradicate lymphoma and serve those touched by the disease.
Lymphoma Research Foundation 8800 Venice Blvd., Suite 207 Los
Angeles, CA 90034; and 115 Broadway, 13th Floor New York, NY 10006
Telephone numbers: CA 800-500-9976; and NY 800-235-6848 Internet
address: www.lymphoma.org
-
31 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
The Leukemia & Lymphoma Society
The mission of The Leukemia & Lymphoma Society (LLS) is to
cure leukemia, lymphoma, and myeloma and improve the lives of
patients and their families.
The Leukemia & Lymphoma Society 1311 Mamaroneck Avenue,
Suite 310 White Plains, NY 10605 Telephone number: 800-955-4572
Internet address: www.leukemia-lymphoma.org
American Cancer Society
The American Cancer Society (ACS) is a nationwide
community-based organization. The American Cancer Society provides
information on specific cancers and general information on coping
with a cancer diagnosis. Information is available both for people
with cancer and for their families and friends.
American Cancer Society 1599 Clifton Road NE Atlanta, GA 30329
Telephone number: 800-ACS-2345 Internet address: www.cancer.org
-
32
National Coalition for Cancer Survivorship
The National Coalition for Cancer Survivorship (NCCS) is a
patient-led organization dedicated to assuring quality cancer care
for all Americans. The NCCS works for people with all types of
cancer and their families. The NCCS provides information on living
with and surviving a cancer diagnosis.
National Coalition for Cancer Survivorship 1010 Wayne Avenue,
Suite 770 Silver Spring, MD 20910 Telephone number: 888-650-9127
Email address: [email protected] Internet address:
www.canceradvocacy.org
National Cancer Institute
The National Cancer Institute (NCI) is one part of the National
Institutes of Health. The National Cancer Institute is the federal
government’s principal agency for cancer research and training. The
National Cancer Institute provides information on many topics,
including specific types of cancer, prevention of cancer, genetic
predisposition to cancer, and coping with cancer.
NCI Public Inquiries Office 6116 Executive Boulevard Room 3036A,
MSC8322 Bethesda, MD 20892-8322 Telephone number: 800-422-6237
Internet address: www.cancer.gov
-
33 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Canadian Cancer Society
The Canadian Cancer Society is a community-based organization of
volunteers whose mission is the eradication of cancer and
enhancement of the quality of life of Canadians living with
cancer.
Canadian Cancer Society National Office Suite 200, 10 Alcorn
Ave. Toronto, Ontario M4V 3B1 Telephone number: 416-961-7223
Internet address: www.cancer.ca
European CanCer Organization
The European CanCer Organization (ECCO) is an umbrella
organization campaigning on political issues such as equitable
access to treatment and organizes a biennial series of congresses
for cancer researchers and healthcare professionals.
ECCO – the European CanCer Organisation Avenue E. Mounier 83
B-1200 Brussels Belgium Telephone number: +32 2 775 02 01 Internet
address: www.ecco-org.eu
-
34
The Cancer Council Australia
The Cancer Council Australia is a national, non-profit
organization which aims to promote cancer-control policies and to
reduce the illness caused by cancer in Australia.
Cancer Council Australia GPO Box 4708, Sydney NSW 2001 Level 1,
120 Chalmers St. Surry Hills NSW 2010 Telephone number: +61 2 8063
4100 Internet address: www.cancer.org.au
Internet Websites
www.cancerindex.org – This site was established in 1996 and
provides a directory of key websites for people with cancer and
their families and caregivers. Information is also provided for
healthcare professionals, scientists, and others interested in
learning about cancer.
www.nlm.nih.gov – The National Library of Medicine website
provides access to various types of health information for both
healthcare professionals and consumers. PubMed contains references
and abstracts from biomedical journals that can be searched for
information on specific diseases and treatments. Medline Plus has
excellent health information for consumers.
www.cancer.gov/clinical_trials and www.clinicaltrials.gov –
These two websites provide general and specific information on
clinical trials. Both sites can be searched for clinical trials
currently enrolling people with WM.
-
35 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
GLOSSARYAlbumin – the most abundant plasma protein, it is
produced in the liver and is important in regulating blood volume
and carrying molecules such as hormones, fatty acids, calcium, and
certain drugs.
Alkylating agent – a chemotherapeutic compound such as
chlorambucil or cyclophosphamide that damages DNA and blocks cell
division.
Amyloidosis – a group of diseases caused by the buildup of an
abnormal protein, called amyloid, in various tissues and organs of
the body. The amyloid protein forms abnormal fibers that may injure
certain tissues and organs or interfere with their normal
function.
Antibody – another name for immunoglobulin.
B-lymphocyte – a type of white blood cell that manufactures
immunoglobulin and develops into a plasma cell when a foreign
substance is detected.
Basophil – a type of white blood cell that is involved in
allergic reactions.
Beta-2 microglobulin – a protein found on all cells with a
nucleus; it is frequently elevated in people with multiple myeloma
and lymphoma.
Bing-Neel syndrome – a condition that involves infiltration of
the central nervous system (brain and spinal cord) by WM cells
and/or IgM deposition, as well as hyperviscosity; complications of
Bing-Neel syndrome may include mental deterioration, confusion,
visual disturbances, irritability, personality changes,
convulsions, and coma.
-
36
Chronic lymphocytic leukemia – the most common type of leukemia,
this is a cancer of B-lymphocytes that usually occurs in adults and
is characterized by increased numbers of B-lymphocytes in the
blood.
Cold agglutinin disease – a condition resulting from antibodies
(usually of the IgM-type) that react at lower temperatures; these
antibodies are specifically directed against proteins (antigens)
found on one’s own red blood cells and can cause anemia, among
other symptoms.
Cryoglobulinemia – a condition characterized by antibodies that
precipitate at temperatures below body temperature and then
re-dissolve upon warming; it is most often due to unknown causes
but may in some cases be associated with an underlying disease such
as WM; signs and symptoms are due to obstruction of small blood
vessels in the extremities and include whiteness, numbness,
bleeding, ulcers, and gangrene.
Doxorubicin – a drug used in cancer chemotherapy that blocks
cell division; it is known by the trade name Adriamycin.
Eosinophil – a type of white blood cell that is involved in
allergic reactions and is responsible for combating parasites.
Flow cytometry – a process in which an instrument uses a laser
beam to scatter light from cells as they pass through a liquid in
the instrument’s chamber; the laser beam light bounces off each
cell, is picked up by detectors, and provides information about the
cell’s characteristics, such as size and inner structure; flow
cytometers can also use antibodies tagged with fluorescent stains
that bind to specific antigens on the cell surfaces - in the case
of leukemias and lymphomas, these fluorescent-tagged antibodies
bind with and identify protein surface markers on the immune
cells.
-
37 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Follicular lymphoma – one of the most common indolent
(slow-growing) non-Hodgkin’s lymphomas, characterized by enlarged
lymph nodes.
Graft vs. host disease – a complication that can occur following
allogeneic stem cell transplant (using stem cells from a donor);
the donor’s immune cells see the recipient’s cells as foreign and
can make antibodies against them, causing a variety of
symptoms.
Hematopoiesis – the process of blood cell development.
Hemolytic anemia – anemia due to hemolysis, which is the
abnormal breakdown of red blood cells either in the blood vessels
or elsewhere in the body.
Hyperviscosity syndrome – occurs as a result of increased IgM
concentration; signs and symptoms include chronic bleeding from the
nose, gums, gastrointestinal tract, headache, ringing in the ears
(tinnitus), dizziness (vertigo), impaired hearing, blurring or loss
of vision, sausage-shaped veins in the retina, and swelling of the
optic disk at the back of the eye (papilledema).
IgM - an antibody that is produced by B-lymphocytes; it is the
largest antibody and the first one to appear in response to initial
exposure to antigen.
Immunoglobulin – a protein produced by B-lymphocytes and plasma
cells in response to a foreign substance or antigen; the classes of
immunoglobulins are IgA, IgD, IgE, IgG, and IgM; these are also
referred to as antibodies.
Immunohistochemistry – refers to the use of special stains to
identify antigens (eg. proteins) in the cells of a tissue section
for purposes of identification, exploiting the principle that
(labeled) antibodies bind specifically to antigens;
immunohistochemical staining is widely used in the diagnosis of
abnormal cells such as those found in cancerous tumors.
-
38
Immunophenotypic analysis – a method for dividing lymphomas and
leukemias into subgroups on the basis of differences in cell
surfaces and antigens. These differences are detected with
monoclonal antibodies and flow cytometry.
Leukemia – a cancer of the blood or bone marrow, characterized
by an abnormal number of circulating blood cells, usually white
blood cells; it is a broad term covering a spectrum of such
diseases.
Lymphocyte – a type of white blood cell, either B-lymphocyte,
T-lymphocyte, or natural killer cell.
Lymphoma – a cancer of the lymphocytes.
Lymphoplasmacytic – cancer cells which have characteristics of
both B-lymphocytes and plasma cells.
Macrophage – a type of white blood cell, found in the tissues,
that engulfs foreign substances and helps to stimulate the immune
response.
Maintenance therapy – a treatment given at regular intervals
after a disease has responded to previous treatment; maintenance
therapy is given in order to help prevent spread or recurrence of
the tumor.
Monoclonal – a group of cells, produced from a single ancestral
cell by repeated reproduction, that share the characteristics of
the original cell.
Monoclonal antibody therapy – the use of antibodies that
specifically bind to a target on cells in order to stimulate the
patient’s immune system to attack those cells.
Monoclonal gammopathy of undetermined significance (MGUS) – an
overproduction of one clone of B-lymphocytes or plasma cells that
produce an immunoglobulin; IgM MGUS is associated with an increased
risk of developing WM.
-
39 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Monocyte – a type of white blood cell that circulates in the
blood and can develop into a macrophage when it moves into
tissues.
Multiple myeloma – cancer of the plasma cells; most commonly the
cancerous clone produces immunoglobulin IgG, IgA, or only light
chains (kappa or lambda) of these immunoglobulins.
Myelodysplasia – a group of related disorders of the bone marrow
characterized by low numbers of abnormally developed blood cells;
myelodysplasia can precede the development of acute leukemia.
Natural killer cell – a type of lymphocyte that directly kills
tumor cells and virus-infected cells by enzymes contained in
granules found in its cytoplasm.
Neutrophil – the most abundant type of white blood cell and one
of the first responders to infection; it is the predominant cell in
pus.
Nucleoside analog – part of a larger class of anti-cancer drugs
termed antimetabolites, which act specifically on proliferating
cells; also known as purine analogs.
Paraprotein – another term for monoclonal immunoglobulin.
Peripheral neuropathy – a fairly common manifestation of WM,
usually caused by the targeting of antigens on the nerve coating
(myelin) by the circulating IgM; clinical features are
predominantly sensory, with abnormal sensations (paresthesias) such
as burning, prickling, itching, tingling, or numbness that are
symmetric and usually first noticed in the feet but can progress to
the hands and arms.
Plasma cell – a cell that develops from B-lymphocytes upon
recognition of a foreign substance or antigen; plasma cells secrete
antibodies to eliminate the foreign substance or antigen.
-
40
Plasmapheresis – a procedure that involves removal of blood from
the body, separation of the liquid (plasma) portion from blood,
replacement usually with albumin and sodium chloride solutions, and
return of the remaining blood components to the body.
Platelet – a type of blood cell that helps stop bleeding.
Prognosis – a prediction of the course of a disease and its
outcome.
Proteasome inhibitor – binds to the core of a cell structure
called a proteasome and blocks its enzyme activity, thus
interfering with its ability to degrade proteins; disruption of
this normal protein breakdown process allows certain proteins in
the cell to accumulate to the point where they can interfere with
cell reproduction and other functions and lead to cell death.
Red blood cell (RBC) – a type of blood cell that contains
hemoglobin and carries oxygen from the lungs to other areas of the
body.
Splenectomy – surgical removal of the spleen.
Stem cell transplantation – a procedure used to restore properly
functioning bone marrow by intentionally destroying the patient’s
diseased bone marrow through chemotherapy and/or radiation and
replacing it with stem cells derived from the patient or a
donor.
T-lymphocyte – a type of white blood cell that matures in the
thymus gland.
Thrombocytopenia – decrease in the number of platelets.
Transformation – the development of a more aggressive lymphoma
in a patient with an indolent or slow growing lymphoma; this may
occur over time as the cancerous B-lymphocytes acquire additional
mutations that cause the disease characteristics to change; some
studies suggest that certain chemotherapy treatments can also cause
transformation.
-
41 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
Vincristine – a drug used in cancer chemotherapy that blocks
cell division; it is known by the trade name Oncovin.
White blood cell (WBC) – a type of blood cell that eliminates
foreign substances or antigens from the body; B-lymphocytes,
basophils, eosinophils, macrophages, monocytes, neutrophils,
natural killer cells, and T-lymphocytes are types of white blood
cells.
-
42
REFERENCES1. American Cancer Society. Cancer Facts and Figures
2009.
www.cancer.org/downloads.
2. Dimopoulos MA, Kyle RA, Anagnostopoulos A, Treon SP.
Diagnosis and management of Waldenstrom’s macroglobulinemia. J Clin
Onc. 2005; 23:1564.
3. Morel P, Duhamel A, Gobbi P, Dimopoulos MA, Dhodapkar MV,
McCoy J, Crowley J, Ocio EM, Garcia-Sanz R, Treon SP, Leblond V,
Kyle RA, Barlogie B, Merlini G. International prognostic scoring
system for Waldenstrom macroglobulinemia. Blood 2009;
113:4163-4170.
4. Kyle RA, Treon SP, Alexanian R, et al. Prognostic markers and
criteria to initiate therapy in Waldenstrom’s macroglobulinemia:
consensus panel recommendations from the Second International
Workshop on Waldenström’s Macroglobulinemia. Semin Oncol 2003;
30(2):116-120.
5. Dimopoulos MA, Galani E, Matsouka C. Waldenstrom’s
macroglobulinemia. Hematol Oncol Clin North Am 1999;
13:1351-66.
6. Gertz MA, Fonseca R, Rajkumar SV. Waldenstrom’s
macroglobulinemia. Oncologist 2000; 5:63-7.
7. Kyle RA, Therneau TM, Rajkumar SV, Remstein ED, Offord JR,
Larson DR, Plevak MF, Melton LJ. Long-term follow-up of IgM
monoclonal gammopathy of undetermined significance. Blood 2003;
102:3759.
8. Khouri I, Sanchez FG, Deisseroth A. Leukemias. In: Devita
VTJ, Hellman S, Rosenberg SA, eds. Cancer: Principles and Practice
of Oncology. Philadelphia: Lippincott-Raven Publishers, 1997;
2285-96.
-
43 ~ Waldenstrom’s Macroglobulinemia - Questions and Answers
9. Schop RFJ, Kuehl WM, VanWier SA, Ahmann GJ, Price-Troska T,
Bailey RJ, Jalal SM, Qi Y, Kyle RA, Greipp PR, Fonseca R.
Waldenstrom macroglobulinemia neoplastic cells lack immunoglobulin
heavy chain locus translocations but have frequent 6q deletions.
Blood, 2002; 100(8):2996-3001.
10. Desikan KR, Dhodapkar MV, Barlogie B. Waldenstrom’s
macroglobulinemia. Curr Treat Options Oncol 2000; 1:97-103.
11. Krishnan K. Waldenstrom hypergammaglobulinemia. Vol. 2002:
www.emedicine.medscape.com/article/207097-overview.
12. McDermott MK, Bell EM. A review of Waldenstrom’s
macroglobulinemia. Clin J Oncol Nurs 1999; 3:107-11.
13. Levine T, Pestronk A, Florence J, et al. Peripheral
neuropathies in Waldenström’s macroglobulinemia J. Neurol.
Neurosurg. Psychiatry 2006; 77: 224-228.
14. Hauser B. Blood tests. Article available at
www.iwmf.com.
15. Sherwood G. Medical tests in Waldenstrom’s macroglobulinemia
including glossary of medical terms relating to tests. IWMF
2007.
16. Rude B. Waldenstrom’s macroglobulinemia: treatment options.
IWMF 2003. Sherwood G. Revision 2010.
17. Gertz MA. Waldenstrom’s macroglobulinemia: a review of
therapy. IWMF 2000. Revision 2008.
-
44
18. Kimby E, Treon SP, Anagnostopoulos A, Dimopoulos M,
Garcia-Sanz R, Gertz MA, Johnson S, LeBlond V, Fermand J-P, Maloney
DG, Merlini G, Morel P, Morra E, Nichols G, Ocio EM, Owen R, Stone
M, Blade Joan. Update on recommendations for assessing response
from the Third International Workshop on Waldenstrom’s
Macroglobulinemia. Clinical Lymphoma & Myeloma 2006;
6(5):380-383.
19. Alexanian R, Weber D. Recent advances in treatment of
multiple myeloma and Waldenstrom’s macroglobulinemia. Biomed
Pharmacother 2001; 55:550-2.
20. McKenna JA. Waldenstrom’s macroglobulinemia. Clin J Oncol
Nurs 2002; 6:283-6.
21. Dimopoulos MA, Gertz MA, Kastritis E, Garcia-Sanz R, Kimby
EK, LeBlond V, Fermand J-P, Merlini G, Morel P, Morra E, Ocio EM,
Owen R, Ghobrial IM, Seymour J, Kyle RA, Treon SP. Update on
treatment recommendations from the Fourth International Workshop on
Waldenstrom’s Macroglobulinemia. J Clin Onc 2009; 27(1):120-6.