Embed Size (px)
Citation preview
Queensland News
ADVANCINGVETERINARY SCIENCE
Australian Veterinary AssociationOctober 2009
Australian Veterinary AssociationOctober 2009
INSIDE THIS ISSUE:INSIDE THIS ISSUE:• President’s Word
•Whistle While You Work
• Three papers on Infection Control in Veterinary Practice
• “Ciao” from Rome
•HeV REVIEW
•Workplace Health & Safety visits to veterinary Clinics in Queensland
• Voice Picking Technology In Veterinary Warehousing
•Update from James Cook University
• AVA PetPEP to go National
•Honorary Editor’s Note
• In Memoriam: Alister Rodgers
• SHORT BITS…
The Publisher, The Australian Veterinary Association Queensland Division, does not hold itself responsible for the statements made in AVA Qld News by contributors or advertisers. Unless so stated, material in AVA Qld News does not reflect the endorsement, official attitude or position of the Australian Veterinary Association or the Honorary Editor. Advertisers are responsible for complying with the Trade Practices Act 1974 as amended.
The Australian Veterinary Association Queensland Division Garden City Office Park Building 3, 2404 Logan Road
EIGHT MILE PLAINS QLD 4113
Tel: 07 3423 1844 Fax: 07 3423 1505
Email: [email protected]
Bruce Pott
Jodie Wilson
Bob Rees
Tony Thelander
Andrew Easton, Patricia Clarke, Sue Fowkes, Carmel Kerwick, Robert Hedlefs & Michael O’Donoghue
Malcolm McLennan & Jon Hill
David Paxton
Michael O’Donoghue (Convenor), Phil Summers, Sue Fowkes, Sue Lapham & Patricia Clarke
Robert Cassidy (Convenor), Andrew Tribe, Ray Barbero, David Lovell & Laurie Dowling
John Odlum
Malcolm McLennan
Robert Hedlefs
President
President Elect
Honorary Treasurer
Honorary Secretary
Committee Members
Invited Executive Members
Honorary Newsletter Editor
Veterinary Education
Animal Welfare
Rep. on Body Corporate – AVA House
Historian
Policy Councillor
AVA QLD DIVISION EXECUTIVE, STANDING & SUB-COMMITTEES & OTHER HONORARY POSITIONS 2009

AVA Queensland News - October 2009
1
The American philosopher and historian Thomas Khun is famous for his publication “The structure of scientific revolutions”. He argued that scientific change is a strictly rational process, a process that has influenced economists, historians, sociologists and philosophers.
Very recently the veterinary profession in this country has been confronted with bitter experiences of what an exotic disease and a relatively new emerging infectious disease can do to our community, to individuals and to families within our profession.
Khun also said that scientists tend to resist research that might signal the development of a new paradigm and that there is a need to sweep present thinking away with new ideas.
It would be fortunate if these new ideas could include a fresh approach to researching the process of hendra virus (HeV) disease in bats, horses and people. At the moment it has reached a stage of boring repetitiveness.
Unfortunately for our scientists, fresh thinking and research requires focus and funding. It is therefore necessary for the profession and all equine stakeholders to lobby politicians regularly.
The AVA has produced a template for this purpose. These templates need to be available to the public via practice waiting rooms, stock feed outlets, stock and station agents and veterinary students
We have previously commented on the success of Infection Control workshops held throughout the state. Unfortunately our interstate colleagues have the misconception that HeV is only a Queensland phenomenon.
There has to be a culture change in how our profession approaches every disease process. Professor Rick Speare from the Anton Brienl Centre for Tropical Health at James Cook University reminded attendees at the Infection Control workshop in Townsville that everyone in the health industries can be presented with all the facts and figures on managing infections in practice. However, if they don’t believe in the principles of Infection Control then we have not moved forward.
Even when there is “belief”, there can be moments in the busy schedule of a veterinarian’s daily routine that cause us to drop our guard and become exposed, only temporarily, but just long enough, to compromise our safety.
Please take this message seriously: a culture change for managing risks of infection is a must for veterinarians and related personnel.
Past events have produced some blips on the radar screens at Workplace Health and Safety Queensland and, by law, they have to respond. Consequently practice audits have already begun in central Queensland. These audits will begin in a constructive manner but future non-compliance will initiate a more regulatory approach.
Your Queensland Division executive has been working closely with officers from WHSQ to ensure a positive result for practitioners from the audits. There are always some downsides to any audit situation. However, we believe there will be positive outcomes for every practice.
Dr Bill Perry and his North Queensland Branch committee are to be congratulated on a successful meeting at an attractive location on the Mackay Marina. The educational segment was inspirational. A big thank you to the speakers who so generously gave of their time.
The NQ Branch continues to engage veterinary nurses. This is a great initiative that always brings many benefits back to the practice. I must remind practice principals that the information nurses receive from these meetings far outweighs your investment.
President’s Word
Dr Bruce Pott - President
AVA Queensland News - October 2009
2
President’s Word Continued from pg. 1
Newly elected NQ Branch president Dr Tess Guilfoyle will no doubt maintain the quality of these programs. Do yourself a favour and pencil in the NQ conference for 2010.
I trust you will notice some new advertising associated with this issue of Queensland News. Merial Australia has provided some valuable financial input. Merial Australia was formed in 1997 from the joint venture of MSD, Agvet and Rhone Merieux. The company has invested in university internships, human breast cancer research and a wide range of veterinary parasite related products that we value and dispense on a daily basis. Thank you, Merial Australia.
While on a brief trip to Brisbane recently one could not help but notice through the dust haze, all the jacaranda trees in magnificent bloom. The Queensland AVA executive and staff take this opportunity to wish all veterinary student AVA members and their classmates success in their forth coming examinations.
All the best for now.
Dr Bruce Pott President
Whistle While You Work The following three papers provide basic information on infection control. In the year nine of the new millennium, it may seem like going back to the future to revisit hand washing, but it remains an essential component of infection control. Hand washing needs to be thorough, and this means washing for about as long as it takes to whistle or sing Happy Birthday or Twinkle Little Star. ‘Hot’ members of the profession might like use other songs. Here is a Calypso example for free:
Wash, wash the hands, Wash, wash the hands;
It really is no pain, To wash and wash again!
Considering Infection Control in Veterinary Practice Dr Sue Fowkes BVSc, DipEd, BED
Contents summary• Why do we need infection control now? (I’ve been ok for the past 30 years);• Elements of successful infection control – per Queensland Health and Commonwealth Health and Ageing
Infection Control Guidelines;• Principles of infection control
♦ Standard precautions♦ Additional precautions♦ Risk assessment♦ Routine practices essential for effective infection control.
Why do we need infection control?• To protect self• To protect staff• To protect owners• To protect patient• To meet legal obligations.
AVA Queensland News - October 2009
3
We don’t want THIS sad news from the AVA President: “Dear Members, I have been shocked and saddened by the tragic death of xyz state member, Dr Jane Doe, as a result of contracting xyz virus. “ – something our current national President has had to write.Recent documented infections in veterinary personnel show that there is ample evidence of emerging zoonotic diseases:• Hendra virus• Monkey pox (never been seen in the United States, except in non-human primates in captivity, until 2003
outbreak)• Multi drug resistant E.coli• Cryptosporidiosis• Methicillin resistant Staphylococcus aureus (MRSA)• Dermatophytosis• Cat associated sporotrichosis.
The areas of greatest risk are:• Injury to the health of veterinarians, their staff and their families;• Economic effects of workplace legislation;• Loss of professional reputation;• Injury to the health of clients and the community at large, with resultant civil suits and loss of professional
reputation.
What are potentially infectious materials????? Following are extracts from the Veterinary Surgeons Board of Queensland letter to the Queensland Division of AVA following the Board’s investigation into a case of Hendra virus:
…horses to humans. While hendra virus remains a sporadic disease of horses, and would not normally be expected to be a likely occurrence in a veterinary clinic premise, its consequences demand stringent new standards.
The Board recommends that all veterinary surgeons are mindful of potential risks to themselves and to others who may come into contact with potentially infectious materials.
Biosecurity and your risk• Veterinarians are at higher risk of contracting infections from animals – as they often are the first to
encounter potentially infected animals;• Veterinarians are ten times more likely to have been exposed to Q Fever than the general population;• Twenty-five percent of affected humans in an outbreak of Monkey Pox in USA were veterinarians;• Numbers of older veterinary practitioners are infected with Brucella abortus;• Standardised infection control guides or procedures are not generally or widely implemented in veterinary
hospitals;• Practice owners may be liable if staff or clinic workers become infected.
In 2005 a survey in the USA found that veterinarians:• did not use appropriate personal protective equipment;• did not engage in protective behaviour to reduce zoonotic disease transmission. Are Australian vets any better? Biosecurity breakdowns happen in Australia and affect veterinarians: for example, Hendra virus infection in veterinarians and infections with Australian Bat Lyssavirus.
The veterinarian undertook a high-risk procedure, taking less than optimal precautions. She was a relatively recent graduate and her training may not have adequately impressed upon her the need to undertake such procedures with due care.
...those working in animal health also must accept that recently emerged zoonotic viruses (e.g., HeV and Australian bat lyssavirus) necessitate appropriate working procedures and personal protective equipment in veterinary practice (MJA, 2006,185: 562).
AVA Queensland News - October 2009
4
Elements of successful infection controlSuccessful infection control involves five elements as described in the Commonwealth Infection Control Guidelines:• Applying basic infection control strategies;• Identifying infection control strategies in specialized settings;• Managing specific infectious agents;• Developingeffectiveworkpractices that prevent transmission of infectious agents;• Adopting quality management systems.
Principlesofinfectioncontrol
Just bear in mind that anything can be a hazard – it is important to identify and evaluate risks:• Basic measures for infection control (standardandadditionalprecautions);• Identifying hazards & minimising risk;• Identify who is at risk;• Identify who is responsible;• Routine practices essential for effective infection control:
Aseptic techniqueHandling of sharpsReprocessing equipmentUse of antibioticsUse of antiseptics and disinfectants.
Basic measures for infection control (standard and additional precautions)• Standard precautions are work practices required to achieve a basic level of infection control and are
recommended for the treatment and care of allpatients;• Additional precautions are recommended for patients knownorsuspected to be infected or colonised
with disease agents that cause infections and that may not be contained by standard precautions alone.
Standard precautions include • Aseptic technique – including appropriate use of skin disinfectants;• Personal hygiene practices – especially hand washing;• Use of personal protective equipment;• Appropriate handling and disposal of sharps and other clinical waste;• Appropriate reprocessing of reusable equipment;• Environmental controls
♦ Design & maintenance of premises♦ Cleaning.
Standard precautions are recommended• for the care and treatment ofallpatients, regardless of their perceived or confirmed infectious status;• when handling blood (even dried blood), and all other body fluids, secretions and excretions;• and to protect non-intact skin and mucous membranes;
because infectious patients may not show any signs or symptoms of infection that may be detected in a routine history and medical assessment.
Additional precautions should be applied when there is a risk of:• Airborne transmission of respiratory secretions;• Droplet transmission of respiratory secretions.
The additional precautions need to be tailored to the specific infectious agent involved and its mode of transmission, and may include:• Isolation• Cohorting• Special ventilation
Continued from pg. 3
AVA Queensland News - October 2009
5
• Additional personal protective equipment • Dedicated patient equipment• Restricted movement of patients and staff (and clients).
Droplet transmission involves contact of the conjunctivae or the mucous membranes of the nose or mouth of a susceptible animal with large-particle droplets (larger than 5 μm in size) containing microorganisms generated from an animal who has a clinical disease or is a carrier of the disease.
Droplets are generated from the source animal primarily during coughing, sneezing, vocalising, and performance of certain veterinary procedures such as suctioning and bronchoscopy.
Transmission of large-particle droplets requires close contact between source and recipient persons because droplets do not remain suspended in the air and generally travel only short distances (usually 3 feet or less).
Special air handling and ventilation are not required to prevent droplet transmission because droplets do not remain suspended in the air.
Airborne transmission of an infectious agent by particles, dust, or droplet nuclei suspended in the air does require special air handling and ventilation.
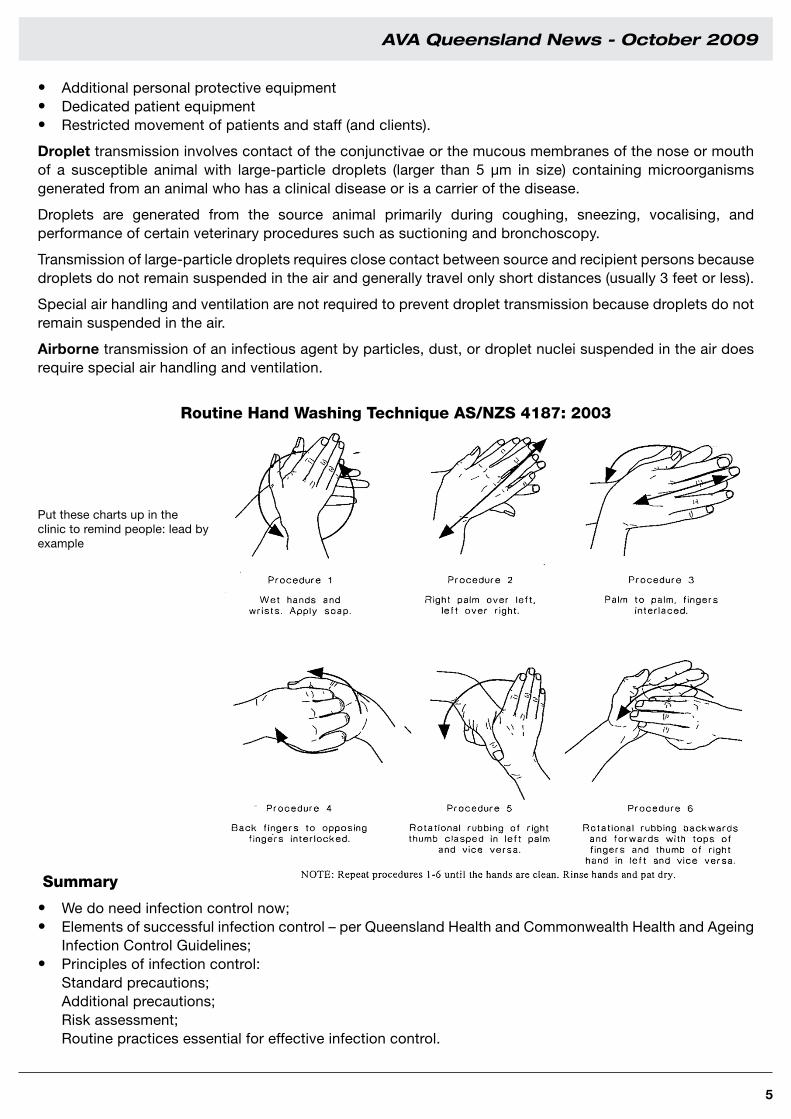
Routine Hand Washing Technique AS/NZS 4187: 2003
Put these charts up in the clinic to remind people: lead by example
Summary
• We do need infection control now;• Elements of successful infection control – per Queensland Health and Commonwealth Health and Ageing
Infection Control Guidelines;• Principles of infection control:
Standard precautions;Additional precautions;Risk assessment;Routine practices essential for effective infection control.
AVA Queensland News - October 2009
6
Infection Control Plan• General principles• Engineering required• Administrative protocols• Personal protective equipment (PPE)• Hurdles
Poor mentorshipLack of a culture of safetyDifficulty of implementation.
General PrinciplesEvery animal is an infection risk and requires standard precautions.
Sick animals may be a higher risk and require additional precautions if droplet and aerosol transmission is suspected.
Animals with specific signs are considered high risk and will require appropriate additional precautions.
Some procedures are very high risk and will require appropriate additional precautions.
Administrative protocols• Registration of veterinary practices• Veterinary Surgeons Board (VSB) requirements• Standing Infection Control Committee at each
practice• Legal requirements from VSB??• Incident reporting• Sharing of information (AVA???)• Newsletters• Training role• Public/client education role.
Veterinary Precautions• Hand Hygiene• Use of protective clothing• Use a surgical mask• Use of gloves DOESN’T NEGATE HAND
HYGIENE• Hand washing is the single most important
measuretoreducetherisk ( keep finger nails short )
• Running water while washing hands is very important
• Moisturizing soaps smell nice, preserve skin integrity and most importantly encourage
compliance• Alcoholic hand gel is an excellent alternative
to soap and water BUT WILL NOT WORK IF HANDS ARE GROSSLY CONTAMINATED!
Standard precautions• Correct handling of all sharps• Safe handling of clinical waste• Appropriate reprocessing of all equipment• Follow correct procedures for cleaning and
spills• Proper handling of laundry.
Additional precautions
Standard precautions plus:• Use of goggles and face protection• Use of P2/N95 respirator or Powered air
purifying respirator • Use of caps, gowns• Use of disinfectant foot baths• Patient isolation• Practice protocols• Animal outside clinic• Increase host defences• Decrease host susceptibility.
Disposal of Waste
Hazard: excretions may infect humans and other animals• Within clinic• At the animal’s home• At waste disposal site.
How would risk be minimised in each case?
Who should cover the costs?
Cleaning Procedures
Hazard: aerosol and physical dispersion of infectious material• Hosing is a high risk procedure• Run off needs to be monitored/treated/disposed• Some droplet formation always occurs• Pathogens may become aerosolised.
Follow world standards.
Infectious Disease Control in Veterinary PracticeDr Andrew Easton BVSc MACVSc CMAVA
AVA Queensland News - October 2009
7
The Infectious Disease Control Kit• Overalls• Gloves• Surgical mask• P2/N95 mask• Goggles/Face shield• Cap• Ground Sheet• Shoe covers• Sanitising wipes.
Hierarchy of Cases
Hazards: humans transmit infectious agents, eg, veterinarians, veterinary nurses, stable hands, students, owners.
Always examine or carry out husbandry activities on admitted animals in a sequence from the healthy to the unhealthy.
Consider whether a colour coding system should be used on individual stalls and or record slates.
Use infection control strategies between animals – always.Visitors
Hazards:
Humans become infected from ill animals
Humans transmit pathogens between animals
Humans bring pathogens into facility.
Visitors adhere to same protocol as staff.
Visitors sign an agreement to do this prior to entry.
Free Ranging Vectors
Rodent control • sealed feed rooms• remove spilt or uneaten feed.
Eliminate nesting sites for rodents and birds.
Vector control• remove mosquito breeding sites• Insect screening• pest control annual reduction program.• hospital pen/cage/stall security• native animals possums/macropods/reptiles.
Incident Management: Sharps injury
Hazard: if it occurs and is not reported, and appropriate prophylactic measures are not taken, the conditions causing/contributing to the injury may then not be rectified.
Conclusion
AVA needs to develop a strategy to ensure veterinarians are recognised for their contribution to public safety by minimising the risk of zoonotic animal diseases in the community.
Practice managers/Principals should promote safe work habits for employee health.
There should be client education on infection control, including risks of zoonosis.
Question: Are the medical practitioners we consult at the cutting edge of awareness of zoonoses and emerging infectious diseases when they consider differential diagnoses?
Infectious Disease Control in Veterinary Practice Dr Robert Hedlefs, AVA Policy Councillor (Queensland Division)
Veterinary Obligations
1. LegislativeWorkplace Health and Safety Act 1995 Veterinary Surgeons Act 1936
2. EthicalAVA Code of Conduct AVA Code of Practice Australian Council of Professions ethics statement
3. PracticalconsiderationsEstablishing an Infection Control Committee
AVA Queensland News - October 2009
8
Continued from pg. 7
1. LegislativeObligations♦ Legally binding with prescribed penalties♦ Provide a safe workplace♦ Protection of animals under your “care”♦ Protection of clients and community♦ Need to demonstrate compliance if required.
RegistrationofVeterinarySurgeons♦ Veterinary Surgeons Act requirements for registration: 18A (4) (b): shall be subject to such terms and conditions or restrictions as are prescribed and specified.
RegistrationofVeterinaryPractices♦ Veterinary Surgeons Act requirements for registration of premises: 25G (1): The board may impose on the approval conditions the board decides, equipment used or intended to be used; hygiene practices or safe storage of drugs, qualifications or skills required of persons.
WorkplaceHealthandSafetyAct♦ Veterinarians must fulfil their obligations under the Workplace Health and Safety Act 1995. Obligation extends to clients, staff and family. Obligation rests on you at visits to a client’s property if you are conducting veterinary work.
WorkplaceHealthandSafetyAct:RiskManagementCodeofPractice2007♦ Five step process for identification and management of hazards and risk;♦ Personal protective equipment is not the prime focus, all strategies must be considered and utilised.
HistoryofAdoptionbyVets♦ Health (Drugs and Poisons) Regulations: veterinarians targeted for failure to record and store as prescribed; ♦ Radiation Safety Act: veterinarians provided many examples of poor practice;♦ Infection control: are we going to follow the trend??
2. EthicalObligationsAVACodeofConduct♦ Used by Veterinary Surgeons’ Board to assess conduct and frames the usual or community expectations of the profession; ♦ Reflects the consensus position of the profession towards animals, community and colleagues;♦ Not legally binding but a useful indicator of accepted practice.
AVAQueenslandDivisionCodeofPracticeforInfectionControl♦ Five principles to assess and manage risk;♦ Closely follow Health system;♦ Standard precautions and additional measures;♦ Must become a habit;♦ Must be continuously reviewed;♦ Accepted by VSB as a guideline for best practice.
AustralianCouncilofProfessionsethicsstatement♦ A profession is a disciplined group of individuals who adhere to high ethical standards;♦ Uphold themselves to, and are accepted by the public as possessing special knowledge and skills derived from research, education and training at a high level; ♦ Are prepared to exercise this knowledge and these skills in the interest of others.
3. PracticalConsiderationsInfectionControlCommitteesneedtobeestablishedbyveterinarypractices
AVA Queensland News - October 2009
9
Most otitis externa treatments require two doses a day…
With Mometamax®, it’s just one daily dose.Mometamax® is proven to alleviate clinical signs of otitis externa in dogs and only requires once-daily administration.
To help ensure your clients and their dogs receive convenient, safe and effi cacious treatment against otitis externa, prescribe the simple once-daily treatment, Mometamax®.
Contact your local Territory Manager directly or on 1800 033 461
MOMETAMAX® ONCE DAILY • NEW MOMETAMAX® ONCE DAILY • NEW MOMETAMAX® ONCE DAILY • NEW MOMETAMAX®
♦ Demonstrated adoption of practices after due consideration of risks to clients, patients, staff, community and self; ♦ Documented and used, role models followed;♦ Discussed and developed, owned by all members of the practice.Does the Veterinary Surgeons Act already imply the need for such formal requirements for registration of persons and premises? Need to consider compliance with Occupational Health and Safety in regard to possible offences and subsequent action by Veterinary Surgeons’ Board. The AVA and VSB agree: ♦ The profession should develop a suitable standard for infection control;♦ The standard is acceptable to the profession and conforms to legislative requirements;♦ The standard will be used to assess individuals if required.
4. Summarycomments♦ Veterinary Surgeons Act requires veterinarians to have standards of hygiene at their workplace;♦ Primary considerations are underpinned by the Work Place Health and Safety Act. The Veterinary Surgeons Act supports these considerations; ♦ AVA is trying to achieve the recommendations of the Perkins report in respect of infection control practices by veterinarians. ♦ The Veterinary Surgeons Board has expressed a desire to work with Biosecurity Queensland and the AVA to develop infection control practices that will be used as a benchmark; ♦ An Infection Control workplace based plan should encompass hygiene management; standard infection control procedures; high risk procedures; demonstrated commitment to infection control practices and monitoring of infection control programs.
“Ciao” from RomeDr Ian Douglas
The Newsletter Editor has asked me to write a little for you about the recent change in life-direction that I have taken.
At the end of August my wife and I travelled to Rome to take up a two-year contract with the UN’s Food and Agriculture Organization. I spent a wonderful six months here in mid-2008, relieving in the staff position that I now hold.
But first, a disclaimer. I am not the “Ian Douglas” that some people think I am. I have a namesake (I have sadly never met him) who is doing some great work by all reports with “Vets Beyond Borders” – also overseas but with an entirely different approach.
In Rome, I am managing the Crisis Management Centre for Animal Health (CMC). The CMC is just three years old having been set up as an initiative of a number of international agencies, but notably the USDA, to be a ‘rapid response’ unit. So we constantly monitor animal health intelligence and, when a disease ‘hot spot’ occurs, within a few days of receiving an invitation from a country, we select, brief, task and insert a team of experts to

AVA Queensland News - October 2009
10
provide initial advice and some limited but key funds into the disease response.
In its short history of operation, the CMC has organised some 36 missions to around 25 different countries, spanning from Mexico to Morocco - Nepal to Fiji. Many of these are to address highly pathogenic avian influenza outbreaks but we have also addressed foot and mouth disease, Rift Valley fever, PPR (peste de petits ruminants), bovine brucellosis, Teschen disease and PRRS (porcine reproductive and respiratory syndrome) of pigs, and rabies.
The work is challenging but satisfying. I have a small (around a dozen people) team of very bright people with a wide variety of skills and interact with many more here at the Rome headquarters of FAO and in the many field centres.
As a pre-requisite to be on staff here, I needed to have two languages of English, French or Spanish. Although I just scrape by on the French (and some would query my English), I do have to work regularly in French – largely reading mission reports and correspondence. Fortunately all of my staff are ‘able’ in at least three languages, and often fluent. I know one of my people speaks five languages fluently. I am determined to expand my currently limited Italian as well.
FAO is situated in central Rome, about 800 metres from the Colosseum and directly opposite the Circus Maximus (Circo Massimo). My apartment is in the inner suburb of Colosseo and I walk to work in less than 15 minutes. My office window overlooks a forest and gardens, but the roof-top restaurants and terraces in the huge building complex provide some of the best views of Rome, with the Forum in the foreground and St Peter’s dome shining in the distance.
And the lifestyle? Well!! Very different to Queensland but very enjoyable. We have quite a number of friends here now and there is a regular flow of dinners and evenings at bars – for coffee or wine. We are lovers of Italian food and they do it very well here, with literally thousands of restaurants and food outlets to choose from. Last time we were here we concentrated on Rome itself, its monuments and history, it delightful walks and hidden treasures. This time, as we become more settled, we will probably buy a car and attack the country-side (and other countries) on weekends and time off.
It is an absolute delight meeting and working with so many people from so many different cultures. My colleagues here really take a global approach and have amazing knowledge of geography and of the veterinary situation. They take a true “world view” and travel extensively to many destinations, many of which most Australians would be terrified to even think of visiting. We work in a number or war zones and security is part and parcel of the job considerations.
It surprises me how many Australians are working around the world, either working directly for international agencies or as consultants. Familiar names keep coming up. And they are generally very highly regarded, and found to be hard working, resourceful and diplomatic.
I am also aware that many Queensland vets have a soft spot for Italy. So, perhaps I will see you strolling down Viale Aventino one of these days.
CiaodaRomae la bocca della Lupa
(the latter - an Italian expression of good luck – “the mouth of the wolf”)
Continued from pg. 9
HeV REVIEWThisupdatewaspreparedbyDrsJoEdmondstonandHumeField
Research Update: Hendra VirusOverview
Hendra virus was first isolated in 1994 from an outbreak of disease in a racing stable located in the northern Brisbane suburb of Hendra less than 10km from the city centre. The outbreak resulted in death of a horse trainer and 13 horses and left a stable hand seriously ill. A further seven horses with evidence of exposure to the virus were humanely destroyed to avoid possible further spread of the disease. Subsequent incidents from the north of Queensland in Cairns to the New South Wales border at Murwillimbah have led to the deaths

AVA Queensland News - October 2009
of a further three people and 21 horses. Despite these periodic and ongoing incidents, Hendra remains one of the world’s rarest diseases.
Scientific evidence suggests that Hendra virus is carried by flying foxes. Under unknown but rare circumstances, the virus spills over from these bats to susceptible horses, killing over 70% of the horses it infects. Under even rarer circumstances, the virus spreads to humans who have had very close contact with Hendra infected horses. While there is strong evidence to support this mode of transmission (bat-to-horse-to-human) there is no evidence of bat-tohuman, human-to-human, or human-to-horse transmission of the virus.
Since Hendra virus was first isolated, significant progress has been made in understanding the virus, where it originates in nature, and how to detect infection and past exposure. Shortly after the September 1994 outbreak, researchers isolated and characterised the virus, developed laboratory tests to detect infection in both humans and animals, and identified the likely source of the virus. Processes have been put in place to reduce the likelihood of outbreaks based on the knowledge obtained from these studies.
While there have been significant gains in knowledge about Hendra, much remains to be learnt. Ongoing studies address the nature of the infection in bats including how and where infection occurs, how Hendra persists in bat populations, and how the virus is transmitted to horses and subsequently to humans. As new technologies are developed, better laboratory tests will be designed to detect and monitor past and current infections. And future research will be directed towards developing better outbreak prevention and control, and potential vaccines and treatments.
Hendra virus incidents
Since 1994, there have been 12 identified incidents of Hendra virus infection in horses. In each of these incidents the first confirmed cases (known as the index cases) were housed in paddocks or yards, not stalls or stables. Six incidents were single horse events, with infection identified in the index case alone. Two incidents involved the infection of one or more companion horses after close contact with the index case. The remaining four incidents involved both horses and humans. After close contact with infected horses, three people developed an influenza-like illness and recovered. Another four people died from influenza-like illnesses and encephalitis (inflammation of the brain).
The incubation period (time from
11
Hendra is a notifiable disease and suspected infections must be reported to the Emergency Animal Disease Hotline on: 1800 675 888. Signs to suggest horses may be infected with Hendra virus include acute onset, increased body temperature, increased heart rate, and rapid progression to death associated with either respiratoryor neurological signs. See Guidelines for veterinarians handling potential Hendra Virus infection in horses.Download available on:http://www.dpi.qld.gov.au/cps/rde/dpi/hs.xsl/4790_13371_ENA_HTML.htm
Incident 3:Gordonvale, October 2004. A veterinarian tested positive for Hendra virus after performing a post mortem on a horse that died suddenly. While no samples were available from the horse for testing, the clinical and post mortem signs were consistent with Hendra virus infection.
Incident 1:Mackay, August 1994. Not recognised until the death of the farmer who had assisted his veterinarian wife with an autopsy of two horses that died of unknown causes. The farmer appeared full recovered after hospitalisation but relapsed and died 13 months later. Retrospective testing showed the horses were infected with Hendra.
Incident 2:Hendra, September 1994. Resulted in the death of a horse trainer, 13 of his horses, and caused severe febrile illness in a stable-hand. The trainer had very close physical contact sick horses, as did the stable hand.
Incident 4:Redlands, June 2008. A veterinarian and veterinary nurse at the Redlands Veterinary Clinic were infected after close direct contact with infected horses. The veterinarian tested positive for Hendra virus and died in August after spending several weeks in intensive care. The veterinary nurse also spent several weeks in intensive care but was later discharged.
Incident 5:Cawarral, August 2009. A Queensland veterinarian died in September after being exposed to Hendra. Infection has been confirmed in two horses that died recently and another had to be destroyed after returning a positive test. The incident was discovered after a property manager and a local veterinarian alerted Biosecurity Queensland with the dead of a horse suffering from respiratory distress.
Figure 1: Details of all Hendra virus incidents associated with human cases.
AVA Queensland News - October 2009
12
Continued from pg. 11
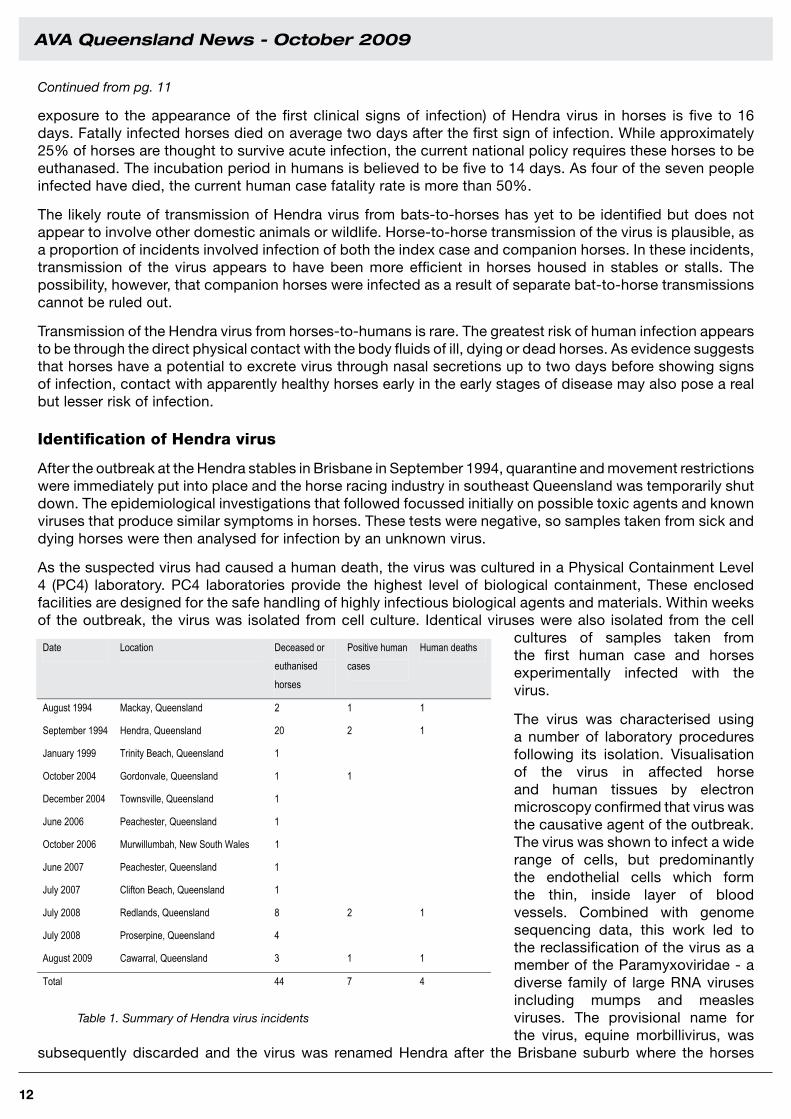
Date Location Deceased or euthanisedhorses
Positive human cases
Human deaths
August 1994 Mackay, Queensland 2 1 1
September 1994 Hendra, Queensland 20 2 1
January 1999 Trinity Beach, Queensland 1
October 2004 Gordonvale, Queensland 1 1
December 2004 Townsville, Queensland 1
June 2006 Peachester, Queensland 1
October 2006 Murwillumbah, New South Wales 1
June 2007 Peachester, Queensland 1
July 2007 Clifton Beach, Queensland 1
July 2008 Redlands, Queensland 8 2 1
July 2008 Proserpine, Queensland 4
August 2009 Cawarral, Queensland 3 1 1
Total 44 7 4
Table 1. Summary of Hendra virus incidents
exposure to the appearance of the first clinical signs of infection) of Hendra virus in horses is five to 16 days. Fatally infected horses died on average two days after the first sign of infection. While approximately 25% of horses are thought to survive acute infection, the current national policy requires these horses to be euthanased. The incubation period in humans is believed to be five to 14 days. As four of the seven people infected have died, the current human case fatality rate is more than 50%.
The likely route of transmission of Hendra virus from bats-to-horses has yet to be identified but does not appear to involve other domestic animals or wildlife. Horse-to-horse transmission of the virus is plausible, as a proportion of incidents involved infection of both the index case and companion horses. In these incidents, transmission of the virus appears to have been more efficient in horses housed in stables or stalls. The possibility, however, that companion horses were infected as a result of separate bat-to-horse transmissions cannot be ruled out.
Transmission of the Hendra virus from horses-to-humans is rare. The greatest risk of human infection appears to be through the direct physical contact with the body fluids of ill, dying or dead horses. As evidence suggests that horses have a potential to excrete virus through nasal secretions up to two days before showing signs of infection, contact with apparently healthy horses early in the early stages of disease may also pose a real but lesser risk of infection.
Identification of Hendra virus
After the outbreak at the Hendra stables in Brisbane in September 1994, quarantine and movement restrictions were immediately put into place and the horse racing industry in southeast Queensland was temporarily shut down. The epidemiological investigations that followed focussed initially on possible toxic agents and known viruses that produce similar symptoms in horses. These tests were negative, so samples taken from sick and dying horses were then analysed for infection by an unknown virus.
As the suspected virus had caused a human death, the virus was cultured in a Physical Containment Level 4 (PC4) laboratory. PC4 laboratories provide the highest level of biological containment, These enclosed facilities are designed for the safe handling of highly infectious biological agents and materials. Within weeks of the outbreak, the virus was isolated from cell culture. Identical viruses were also isolated from the cell
cultures of samples taken from the first human case and horses experimentally infected with the virus.
The virus was characterised using a number of laboratory procedures following its isolation. Visualisation of the virus in affected horse and human tissues by electron microscopy confirmed that virus was the causative agent of the outbreak. The virus was shown to infect a wide range of cells, but predominantly the endothelial cells which form the thin, inside layer of blood vessels. Combined with genome sequencing data, this work led to the reclassification of the virus as a member of the Paramyxoviridae - a diverse family of large RNA viruses including mumps and measles viruses. The provisional name for the virus, equine morbillivirus, was
subsequently discarded and the virus was renamed Hendra after the Brisbane suburb where the horses
AVA Queensland News - October 2009
13
For more details about PC4 laboratories (also known as BSL4) seehttp://www3.niaid.nih.gov/topics/BiodefenseRelated/Biodefense/PublicMedia/labtour/
For more details about the PC4 laboratory at CSIRO AAHL where the Hendra virus is handled see:http://www.csiro.au/resources/psd6
Nipah virus emerged in pigs and humans in Malaysia. Since then over 470 known human infections and over 240 deaths have been linked to outbreaks of Nipah in Malaysia, Singapore, Bangladesh and India. Pteropid bats are thought to be the natural reservoirs of the virus. There have been no reported outbreaks in Australia.
For more details about Nipah see:www.who.int/mediacentre/factsheets/fs
Artificially coloured Hendra virus electron micrograph Courtesy AAHL Biosecurity Microscopy Facility.
were stabled in the September 1994 outbreak. Rapid molecular tests to detect the virus were developed using the sequence data.
Further molecular analysis showed this virus was sufficiently different from existing paramyxoviruses to warrant the creation of a new genus within the family. This new genus, the Henipaviruses, now includes Hendra virus and Nipah virus which both have genomes up to 15% larger than other paramyxoviruses. In addition to a number of unique molecular characteristics, these viruses are distinguished from other members of the Paramyxoviridae family by their ability to infect a broad range of species and fatally infect both animals and humans.
Serological studies confirmed that horses and humans affected in the outbreaks had been exposed to Hendra virus. Serum antibodies are formed in response to viral infection. By immunoelectronmicroscopy, Hendra virus was shown to be neutralised with antibodies from the blood of symptomatic horses and humans, confirming these animals had been exposed to the virus. Serum neutralisation tests showed the growth of the virus in cell culture could be halted by these antibodies.
Reservoir hosts
After isolating Hendra and developing a number of specific diagnostic tests for the virus, extensive investigations looked for the source of the virus in nature. Early research focussed on animals present in the locations of index cases found no evidence of Hendra virus infection. The search was then broadened to include sick or injured wildlife in temporary captivity. A total of 168 animals (from more than 16 species of rodents, marsupials, birds, amphibians, and insects) returned negative antibody tests. Retrospective investigations of diagnostic laboratory records and stored specimens from horses failed to identify any sign of previous infection.
A multidisciplinary task group reviewed the available laboratory and epidemiological data for clues to which animal or animals may harbour the virus in nature. Flying foxes were targeted for further investigation because they fulfilled the criteria of the possible viral reservoir host. They were present in both of the locations of the incidents at Hendra and Mackay, were capable of moving between and/or had overlapping populations spanning these two locations, and could plausibly have had indirect contact with horses at both locations. By early 1996, sampling of sick or injured flying foxes in temporary captivity showed that several species of Australian flying foxes had antibodies to Hendra virus. Broader serological surveillance revealed antibodies to the virus in all four mainland pteropid species – the black, grey headed, little red and spectacled flying foxes. The theory that the risk of bat-to-human transmission of the virus is low was supported when wildlife carers in close and regular contact with sick and injured bats showed no evidence of Hendra virus infection.
Further sampling throughout eastern Queensland involving over 5000 sera samples collected from 46 species (including 34 species of wildlife) found no evidence of antibodies in species other than the horses and humans involved in incidents and flying foxes. No domestic animals tested have shown any signs of Hendra virus infection.
AVA Queensland News - October 2009
14
Continued from pg. 13
Pteropus bats, also known as flying foxes or fruit bats, are mammals and members of the Pteropididae bat family. They have the largest body of all bats. Four species of these mammals are native to mainland Australia; the little red flying fox (Pteropus scapulatus), black flying fox (Pteropus alecto), grey-headed flying fox (Pteropus poliocephalus) and spectacled flying fox (Pteropus conspicullatus).
For further information about flying foxes see:http://www.dse.vic.gov.au/dse/nrenpa.nsf/FID/-BAA86C6B029BC723CA256BF2001E4069?O
Sampling bat saliva, Photo: Dr. Andrew Breed
Ongoing research supports the theory that flying foxes are the natural reservoir of the virus. In September 1996, live Hendra virus was isolated from a grey-headed flying fox euthanised after becoming tangled and injured in a wire fence. This bat had recently aborted twin foetuses and virus was also isolated from a pooled sample of tissue collected from the foetuses. A third viral isolate was obtained from the lung of a foetus collected from a black flying-fox which had been euthanised for spinal injuries. It has been detected periodically in urine samples collected under flying fox roosts. Surveys of 1043 flying foxes in Queensland between 1996 and 1998 showed evidence of exposure to Hendra virus in 47% of the bats sampled. Similar frequencies have since been observed in samples taken from flying foxes across mainland Australia. Antibodies have also been detected in archived blood samples taken from flying foxes in the 1980s.
The high frequency of Hendra antibodies observed in flying foxes suggests transmission of the virus between these bats is efficient. Flying fox camps often consist of thousands of bats roosting together in the canopy of trees. In these dense roosts, bats excrete urine and faeces throughout the day and a fine mist of urine is commonly observed. Under these conditions, and given their regular grooming activities, transmission from one bat to another in the roost is highly plausible.
It is less clear if Hendra virus is maintained within flying fox colonies as an acute or ongoing infection. Computer modelling of flying fox populations suggests that Hendra virus does not persist as a constant endemic infection in discrete populations of bats, but persists throughout the range of flying foxes in a pulsing pattern. In this pattern of infection, a nomadic individual or small group of bats from an infected colony may make contact with a colony of flying foxes susceptible to infection either because they have not yet been exposed to the virus or their immunity has waned. These nomadic bats then introduce (or reintroduce) the virus to bats within the susceptible colony, resulting in an increase (or pulse) of infection followed by a period of waning immunity.
Little red flying foxes may play a key role in this pattern of pulsing endemicity of Hendra infection, making them a possible key reservoir of the virus. A rapid decline in immunity to Hendra virus was observed between seasons during a study sampling flying foxes over two years from 2004. Periods of waning immunity may correspond to times when these bats are susceptible to infection. This is in contrast to two other Australian flying fox species. Both the grey-headed and spectacled flying foxes appear to develop long lived immunity to the virus.
The exact mechanics of Hendra virus transmission from flying foxes to horses is not known as no virus has been isolated from flying foxes during incidents. However transmission of the virus to horses is thought to be through the ingestion of grass or partially eaten fruit contaminated with bat urine, saliva or other bodily fluids. The timing of Hendra virus infection in horses may then be linked to the pattern of pulsing endemicity in flying foxes. A period of the peak virus excretion may follow the introduction of infection to a susceptible bat colony. This period is likely to correspond increased risk of exposure and infection of susceptible horses in the vicinity.
AVA Queensland News - October 2009
15
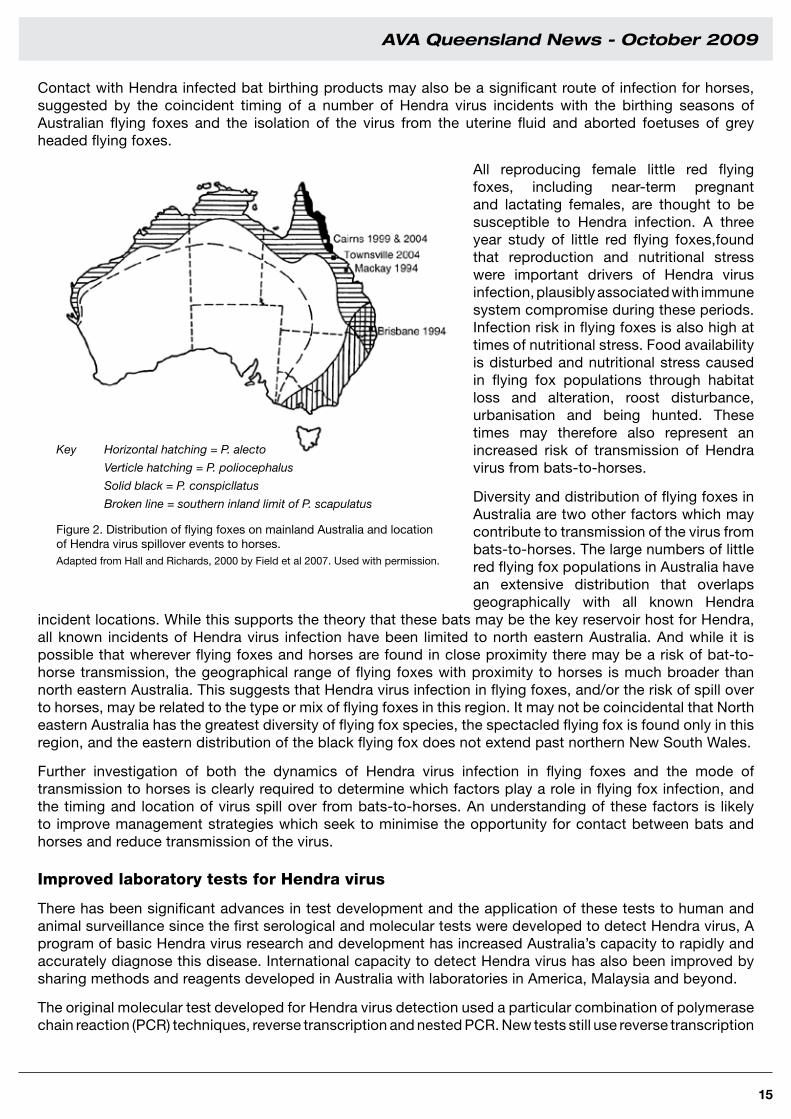
Key Horizontal hatching = P. alecto
Verticle hatching = P. poliocephalus
Solid black = P. conspicllatus
Broken line = southern inland limit of P. scapulatus
Figure 2. Distribution of flying foxes on mainland Australia and location of Hendra virus spillover events to horses.Adapted from Hall and Richards, 2000 by Field et al 2007. Used with permission.
Contact with Hendra infected bat birthing products may also be a significant route of infection for horses, suggested by the coincident timing of a number of Hendra virus incidents with the birthing seasons of Australian flying foxes and the isolation of the virus from the uterine fluid and aborted foetuses of grey headed flying foxes.
All reproducing female little red flying foxes, including near-term pregnant and lactating females, are thought to be susceptible to Hendra infection. A three year study of little red flying foxes,found that reproduction and nutritional stress were important drivers of Hendra virus infection, plausibly associated with immune system compromise during these periods. Infection risk in flying foxes is also high at times of nutritional stress. Food availability is disturbed and nutritional stress caused in flying fox populations through habitat loss and alteration, roost disturbance, urbanisation and being hunted. These times may therefore also represent an increased risk of transmission of Hendra virus from bats-to-horses.
Diversity and distribution of flying foxes in Australia are two other factors which may contribute to transmission of the virus from bats-to-horses. The large numbers of little red flying fox populations in Australia have an extensive distribution that overlaps geographically with all known Hendra
incident locations. While this supports the theory that these bats may be the key reservoir host for Hendra, all known incidents of Hendra virus infection have been limited to north eastern Australia. And while it is possible that wherever flying foxes and horses are found in close proximity there may be a risk of bat-to-horse transmission, the geographical range of flying foxes with proximity to horses is much broader than north eastern Australia. This suggests that Hendra virus infection in flying foxes, and/or the risk of spill over to horses, may be related to the type or mix of flying foxes in this region. It may not be coincidental that North eastern Australia has the greatest diversity of flying fox species, the spectacled flying fox is found only in this region, and the eastern distribution of the black flying fox does not extend past northern New South Wales.
Further investigation of both the dynamics of Hendra virus infection in flying foxes and the mode of transmission to horses is clearly required to determine which factors play a role in flying fox infection, and the timing and location of virus spill over from bats-to-horses. An understanding of these factors is likely to improve management strategies which seek to minimise the opportunity for contact between bats and horses and reduce transmission of the virus.
Improved laboratory tests for Hendra virus
There has been significant advances in test development and the application of these tests to human and animal surveillance since the first serological and molecular tests were developed to detect Hendra virus, A program of basic Hendra virus research and development has increased Australia’s capacity to rapidly and accurately diagnose this disease. International capacity to detect Hendra virus has also been improved by sharing methods and reagents developed in Australia with laboratories in America, Malaysia and beyond.
The original molecular test developed for Hendra virus detection used a particular combination of polymerase chain reaction (PCR) techniques, reverse transcription and nested PCR. New tests still use reverse transcription
AVA Queensland News - October 2009
16
Continued from pg. 15
The enzyme linked immunosorbent assay or ELISA measures antibody concentrations in serum samples by immobilising a known amount of inactivated virus (antigen) onto the bottom of a well in an ELISA plate. This viral antigen is then used to capture and quantify specific antibodies present in the samples.
For a more detailed description of ELISAtests see:
http://en.wikipedia.org/wiki/ELISA
but the innovation of real time PCR makes the test much faster, requiring significantly less viral material. Further refinements allow these tests to distinguish Hendra virus from Nipah virus which is important for disease control and prevention.
A number of Hendra virus isolates have been fully sequenced. Prior to 2006, the gene sequence of these viral isolates were virtually identical, irrespective of the species from which they were recovered, the location of the incident, or the time of recovery. In more recent incidents, genetic differences have been detected between the isolates and those sequenced previously. While it is possible the virus may be changing, it is more likely that flying foxes have carried this virus for a long time and over the years variants have evolved. As more isolates are identified and sequenced, the likelihood of detecting these variants increases, hence the observed differences. These genetic variations could explain the range of clinical symptoms observed in infected horses across the 11 incidents. However, recent experimental studies suggest these variations are more likely due to differences in the route of Hendra infection or the system that is first compromised in an infected horse.
Molecular tests for Hendra are fast, accurate and sensitive, but they are only effective in detecting virus when it is present at the time of testing. As viruses usually disappear in infected individuals a few days after infection, PCR tests are ineffective in the longer term. Antibodies, however, are detectable long after infection, so serological assays are effective in detecting viral exposure over long periods.
While the serum neutralisation test remains the gold standard for detection of an antibody response to Hendra virus infection, other serological tests have been developed that do not use live Hendra virus either directly in the assay or in the preparation of the assay reagents. Enzyme linked immunosorbent assays (ELISAs) developed shortly after the serological studies of the September 1994 outbreak have been particularly useful for serological surveillance. Early in the development of these ELISAs, non-containment laboratories performed the assays using virus that had been cultured and irradiated for safe use. However, preparation of the viral reagents for use in the ELISA still required cell culture-based growth of the virus in a PC4 laboratory. A number of recombinant Hendra virus antigens have subsequently been developed for use in these tests. Production of antigen using these methods provides test reagents that are robust, specific, and affordable. Importantly, they can be also be produced and used in non-PC4 environments.
More recently, another serological assay using bead-based flow cytometry has been developed to detect and differentiate antibodies against Hendra virus and Nipah virus in a single test. Also using recombinant antigens, this test represents a significant advance in serological capability in Australia.
Despite significant advances in laboratory testing for Hendra virus, viral isolation in cell culture remains an important diagnostic tool, especially in a new case or outbreak when isolation of the virus is sought for absolute confirmation of the disease. Despite advances in technology that allow for Hendra tests to be developed and performed independent of PC4 facilities, the virus remains classified as a PC4 pathogen because of its high case fatality rate in humans and lack of effective vaccine or therapy.
Disease Control & Animal Management
Control of Hendra virus infection has focussed on strategies for managing infected horses. When Hendra virus infection has been confirmed, the premises involved are quarantined and the disease investigated. Measures are put into place to care for the animals on the premises, to reduce the risk of transmission to people and other horses, to disinfect the environment, and safely dispose of infected horses that die or are euthanised.
Other management strategies are used to reduce the opportunity for contact between bats and horses, to monitor horses and other species for evidence of infection, and improve biosecurity in areas at risk of infection.
Studies suggest that at least 290 plant species worldwide rely on large populations of flying foxes for propagation.
AVA Queensland News - October 2009
Flying foxes infected with Hendra virus show no clinical signs and appear to be unaffected by the virus. It has been suggested that the immune system of bats is special, and allows them to sustain viral infections in the absence of overt disease. This has yet to be established.
Work is ongoing to learn more about bats’ immune systems.
17
Significant effort has also been made to improve awareness of Hendra virus, particularly for veterinarians, horse handlers and wildlife carers.
The indiscriminate or targeted killing of flying foxes is not considered as an effective Hendra virus management strategy. As these bats are nomadic, culling may create a niche that other bats fill, possibly increasing rather than decreasing the number of flying foxes in the target area. Culling could also contribute to altering the ecology of the region as flying foxes play a key role in the pollination and seed dispersal for a large number of plants. And while flying foxes remain relatively conspicuous in some areas, many of their current populations are in rapid decline and require protection.
Experimental models
The key to understanding Hendra viruses may lie in studying suitable animal models of the disease. Early experimental infections of horses and bats conducted with virus isolated from the September 1994 outbreak confirmed that this virus was the agent responsible for the outbreak. Further experimental infections have also been undertaken to study replication of the virus, antibody development, virus shedding, transmission, and pathogenesis.
Hendra virus has an affinity for endothelial cells and infection in horses causes inflammation of the blood vessels (vasculitis) throughout the body. The spectrum of respiratory and neurological clinical signs observed in various infected horses is thought to be a consequence of this vasculitis in different body systems. So the organ or system where the greatest vascular damage lead to the first clinical signs linked to these observed in this horse. The detection of viral genetic material in the blood, nasal secretions and a wide range of body tissues of infected horses indicates that by the time a horse shows clinical signs of infection the virus is widespread throughout the body. Most virus is shed from these horses when they are sickest, suggesting that this is the time when transmission is most likely. However, studies have also shown that a horse can potentially excrete the virus through nasal/naso-pharyngeal secretions at least two days prior to the appearance of clinical signs.
Experimentally infected flying foxes develop a viraemia (where the virus enters into the blood stream) then excrete the virus in their urine, faeces and saliva for approximately one week. But unlike horses, there is no indication of illness in these bats.
Experimental infections have also been performed to preclude certain animals as carriers of the disease. Mice, rats, rabbits, chickens, and dogs do not develop disease following inoculation with the virus. In contrast, cats and guinea pigs are highly susceptible. The cat has been the preferred choice for experimental studies of Hendra virus infection. Experimentally infected cats develop symptoms of Hendra virus that closely resemble the lethal respiratory disease in humans and horses and they are easier to manage under PC4 conditions than large domestic animals such as horses. However ferrets are now becoming the preferred animal model because of their ease of handing. While the susceptibility of cats to experimental infection raises the possibility that cats may play a role in the transmission of this virus to horses, no evidence of natural infection has ever been found in cats.
Horses, bats and cats have also been used to examine possible routes of virus transmission between susceptible animals. In these laboratory studies, the virus shows low levels of transmissibility under most circumstances. Attempts to recreate transmission have been largely unsuccessful in cats-to-cats, cats-tohorses, bats-to-bats, bats-to-horses, horses-to-horses and horses-to-cats.
Further studies have shown that the virus does not survive for extended periods after excretion from infected animals. There has been very little virus detected in urine collected from the floor of horse stalls containing horses with high levels of virus in their bladder urine, and research into persistence of the virus under various environmental conditions suggests the virus is highly sensitive to temperature and dessication. These results suggest that natural transmission is likely to require close contact with an infected animal or exposure to contaminated material shortly after excretion.

AVA Queensland News - October 2009
Continued from pg. 17
18
Vaccines and Therapy
There are currently no vaccines or drugs for preventing or treating Hendra virus infection. Development of these agents has been hampered by a lack of knowledge about the initial sites and duration of virus replication following infection and issues associated with funding vaccine development for a rare disease. However, a number of vaccines and drugs are in the pipeline and it is likely that animal models will be particularly useful in both the development and testing of these new therapeutic agents.
The proteins involved in Hendra virus infection have also been studied in detail as these proteins may provide clues to blocking infection. Viral proteins, which have been crystallised and their structures and genomic sequences determined, could possibly be used to reduce infection by preventing viral entry into cells. Because both attachment to cells and fusion are critical steps for infection, therapeutic agents that block either process could be used as antiviral drugs. To date, the most extensively characterised novel therapeutic agents for Hendra target the host cell protein that binds the virus, ephrin B2.
Advances have also been made in the development of possible Hendra virus vaccines. While inactivated viruses have been used as the basis for a number of other commonly used vaccines, it is unlikely that this type of vaccine will ever be developed for Hendra because of the risk, albeit remote, of infection. However, vaccine trials have been initiated that use recombinant viral antigens. These antigens represent only a small fraction of the virus, but may be sufficient to stimulate an immune response and protect against infection with the live virus. If successful, this vaccine could be administered without any risk of infection.
Conclusions
Despite the recent emergence of Hendra virus and the difficulties associated with researching a virus carried by flying foxes, there have been significant advances in understanding this virus and the disease it causes. The virus has been fully characterised and monitoring sequence changes in isolates is ongoing. The species that are susceptible to infection have been determined and how the virus infects the cells of these species (and the symptoms it causes) has been well documented. The viral reservoir in nature has been identified and measures have been taken of the prevalence of flying foxes exposed to this virus. A suite of laboratory tests have been developed for detection of the virus during incidents and for surveillance, and these tests can now be performed in a number of national and international laboratories. And the analysis of experimental infections continues, yielding new data to be used to improve management of the disease and to develop novel vaccines and therapies.
Hendra virus research, however, is challenging and complicated and much remains to be learnt. Research continues into understanding the behaviour of the virus in flying foxes in the wild and what factors cause the virus to spill over from these bats to horses and subsequently to humans. Significant questions remain concerning how and when the virus is transmitted and whether any domestic animals or wildlife other than flying foxes are involved in the disease cycle. Research that addresses these questions will lead to a
AVA Queensland News - October 2009
19
better understanding of how to predict and prevent incidents and how best to manage them when, and if, they occur. Ultimately it is hoped that future research will lead to the development of a vaccine to prevent the disease, and/or a treatment that will stop the disease in infected individuals.
Resources
Further information about Hendra virus can be found at the following websites:
General articles:
Hendra Virus Feature Article - CSIRO Australian Animal Health Laboratory (AAHL) http://www.csiro.au/science/Hendra-Virus.html
Hendra Virus Overview – Queensland Primary Industries and Fisheries (QPIF) http://www.dpi.qld.gov.au/cps/rde/dpi/hs.xsl/4790_11127_ENA_HTML.htm
Hendra Virus Disease and Nipah Virus Encephalitis Fact Sheet- Centres for Disease Control and Prevention (CDC) http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/nipah.htm
Information for the community, veterinarians and horse owners:
Hendra Virus. Important Community Information- Queensland Health http://www.dpi.qld.gov.au/documents/Biosecurity_GeneralAnimalHealthPestsAndDiseases/HendraVirusCommunity.pdf
Guidelines for Veterinarians Handling Potential Hendra Virus Infection in Horses – QPIF http://www.dpi.qld.gov.au/cps/rde/dpi/hs.xsl/4790_13371_ENA_HTML.htm
Hendra Virus. Important Information for Horse Owners – QPIF http://www.dpi.qld.gov.au/documents/Biosecurity_GeneralAnimalHealthPestsAndDiseases/Hendra-virus-horseowner-guidelines.pdf
Hendra Virus Infection – Queensland Health http://access.health.qld.gov.au/hid/InfectionsandParasites/ViralInfections/hendraVirusInfection_fs.asp
Hendra Research:
Research into Hendra Virus. The Story So Far – QPIF http://www.dpi.qld.gov.au/cps/rde/dpi/hs.xsl/4790_11599_ENA_HTML.htm
Hendra Virus. The Initial Research – QPIF http://www.dpi.qld.gov.au/cps/rde/dpi/hs.xsl/4790_11112_ENA_HTML.htm
Flying Foxes Information:
Consortium for Conservation Medicine The Henipavirus Ecology Collaborative Research Grouphttp://www.henipavirus.org/
Bat Care Brisbane http://www.bats.org.au/
Flying Foxes - Victorian Department of Sustainability & Environment http://www.dse.vic.gov.au/DSE/nrenpa.nsf/LinkView/C330BE1115AF2EAACA256BF2001CF9DB16C869C35CA02BB14A256DEA00247222
The Action Plan for Australian Bats – Australian Government Department of the Environment, Water, Heritage and the Arts http://www.environment.gov.au/biodiversity/threatened/publications/action/bats/index.html
Australian Bats – Australian Museum http://australianmuseum.net.au/Australian-bats
© 2009 Australian Biosecurity CRC for Emerging Infectious Disease. Prepared by Dr Jo Edmondston and Dr Hume Field.
AVA Queensland News - October 2009
20
Workplace Health & Safety visits to veterinary Clinics in QueenslandCourtesy Patricia Coward, Principal Adviser (Occupational Health), Workplace Health and Safety Queensland
Improving workplace health and safety reduces the human and financial cost of workplace injury and illness. The Workplace Health and Safety Act 1995 aims to prevent work-caused death, injury and illness in Queensland. To this end, Workplace Health and Safety Queensland (WHSQ) inspectors will be visiting a number of horse–related businesses in Queensland in 2009-2010, with a focus on businesses that provide veterinary services to horses. This intervention is in response to continuing incidents of Hendra virus in Queensland and the potential for those who handle horses to be exposed to this rare but serious disease.
WHSQ inspectors will assess how employers are managing Hendra virus risks. This will involve a desktop audit of Hendra virus risk management strategies, including policies and procedures, staff training and provision of personal protective equipment, and may also include a walk-through survey of the veterinary clinic. Workplace health and safety guidance to assist with preparation for these visits is available in the Queensland Primary Industries and Fisheries Guidelines for veterinarians handling potential Hendra virus infection in horses( h t t p : / / w w w. d p i . q l d . g o v. a u / c p s / rd e / d p i /hs.xsl/27_2900_ENA_HTML.htm) and the WHSQ Hendra virus safety alert for veterinarians(http://www.deir.qld.gov.au/workplace/publications/alerts/hendra_virus/index.htm).
All WHSQ inspectors carry photo identification and will identify themselves on arrival. Advance notice of a visit is not required but is often given to ensure minimal business disruption. Inspectors have a number of powers including gathering information, making enquiries, examining and copying documents and requiring persons to give reasonable help. Depending on the circumstances, an inspector may give advice or take enforcement action such as giving a verbal direction or issuing notices. There is an appeal process if you disagree with a decision made by an inspector. More information on inspector visits is available in What to expect when an inspector calls (http://www.deir.qld.gov.au/workplace/resources/pdfs/inspector_calls.pdf).
WHSQ will consult with key stakeholders at all stages of the intervention, including the Australian Veterinary Association, Equine Veterinarians Australia, Queensland Primary Industries and Fisheries and Queensland Health. The findings from the workplace visits will be shared with key stakeholders in a decoded form that does not identify individual veterinary practices, with the aim of informing future strategies for Hendra virus risk management.
WHSQ also provides a free advisory service to small businesses employing fewer than 20 workers. Small Business Advisers are able to provide free group coaching for industry groups or small groups of businesses with a common interest.
For more information and advice about WHSQ and its services, phone 1300 369 915 or visit www.worksafe.qld.gov.au
WORK SAFE. HOME SAFE.
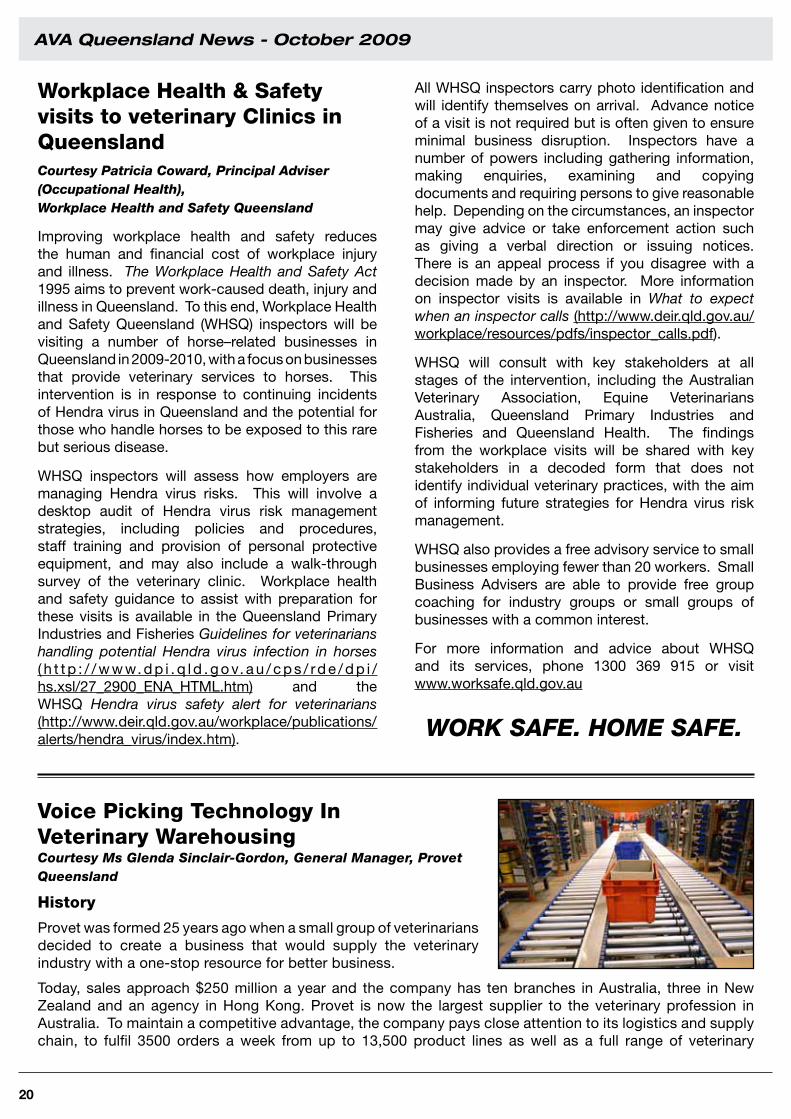
Voice Picking Technology In Veterinary WarehousingCourtesy Ms Glenda Sinclair-Gordon, General Manager, Provet Queensland
History
Provet was formed 25 years ago when a small group of veterinarians decided to create a business that would supply the veterinary industry with a one-stop resource for better business.
Today, sales approach $250 million a year and the company has ten branches in Australia, three in New Zealand and an agency in Hong Kong. Provet is now the largest supplier to the veterinary profession in Australia. To maintain a competitive advantage, the company pays close attention to its logistics and supply chain, to fulfil 3500 orders a week from up to 13,500 product lines as well as a full range of veterinary
AVA Queensland News - October 2009
21
Update from James Cook UniversityKylie Francis, Senior AVA JCU Representative
Semester 2 at the JCU Vet School certainly kicked off with a bang! While first years were having their first introductory anatomy classes, second years were learning introductory pathology, parasitology and virology. The fourth years had an intensive week of exotic animals, focussing on birds and reptiles, and the third years saw some serious sheep production on their week long trip to Longreach. The week consisted of 7 property visits to learn about different sheep production systems, two trips out to the DPI Research Station and some demonstrations at the Longreach Agricultural College. The trip was thoroughly enjoyed by all, highly informative, and made somewhat more colourful by the local pubs and bus trips. A big thanks to all the staff involved for making the week possible and enjoyable.
On a social side, the third years recently celebrated their half-way dinner. A fantastic night was had by all at the Reef Museum. The night wouldn’t have been made possible without the hard work of the committee or the generous support of Merial who sponsored the evening.
Congratulations must go to Ellie McKenna for her fantastic effort in Endurance Riding on the weekend. Ellie competed in Mackay at the State Championships, riding 160km over the weekend. Ellie rode extremely well and finished 8th, allowing her to qualify for the next level of competition. Well done Ellie, we are all very proud.
instruments and equipment needed in modern practices.
When Provet planned a new South East Queensland warehouse strategically located in the Brisbane suburb of Northgate, its management realised the facility would need to use a high degree of automation, so design engineers began working with Provet on a voice picking conveyor system for the new facility. The large purpose-built facility in Northgate opened in 2006.
Operation of the system
A conveyor delivers totes to the appropriate pick faces but can bypass the non-active zones. The majority of picking is managed by voice terminals, of which there are 10 in the operation. Receipt and put away is managed via radio frequency terminals. Orders arrive via EDI, phone and fax and are uploaded to the warehouse management system (WMS). The WMS then downloads the orders to PickDIRECTOR, which determines the priority and release of orders. It also allows tracking of orders and carton contents.
Different coloured totes determine the priority of orders. Up to 250 orders – or around 1000 cartons – are processed per day. Urgent orders such as medical supplies are despatched the same day, while all other orders are despatched next day. The warehouse staff members have embraced the new technology and it has had a major impact on the workplace.
With the previous paper-based system, pickers spent a lot of time walking to collect the orders. In contrast, with the new system, the orders are taken to the picker, so productivity has certainly increased. Picking accuracy has also increased and although there is still the occasional human error, wrong product or wrong tote, accuracy is up around 99%. With the previous system, every order had to be double checked; this isn’t necessary with the voice picking system.
AVA Queensland News - October 2009
22
AVA PetPEP to go NationalMark FraserEducation Project Officer PetPEP (Pets & People Education Program)
The AVA is currently looking at streamlining and organising a national offering for their AVA PetPEP community education program. Presently South Australia and Queensland are extremely pro-active in their respective states and the AVA PetPEP message is spreading.
In consultation with both these states and key stakeholders around the country, we have come up with a core of key messages that will reflect the future content and direction of the program.
The key messages are : Responsible pet ownership, Safety around animals, Healthy living (pets and animals), Welfare of animals, Animals and the community.
Connecting veterinarians with the community is a key element of the AVA strategic plan, and the key messages need to address and reflect this aspect.
Currently I am creating content based around the key messages and updating the AVA PetPEP website, which is a crucial platform in communicating with the community at large.
Presently heavily involved with schools, the national format is looking further afield into community groups and other relevant target audiences.
As part of the new national focus, the importance of training and resources will also form a large part of the revamped program.
As for myself, I come from an education, multimedia and journalism background and am enjoying the challenge…although my three month contract seems to be passing all too quickly.
If you have any queries or comments please feel free to contact me at: [email protected]
Honorary Editor’s NoteInfection control …
There is a tide in the affairs of men,
(And of women too, it may now be said),
Which, taken at the flood, leads on to fortune;
Omitted, all the voyage of their life
Is bound in shallows and in miseries.
In such a full sea are we now afloat,
And we must take the current as it serves,
Or lose our ventures.
-DrWilliamShakespeare
Doctor Bill’s style may be whimsical but his message is clear, just as is the message of our President in this issue of Queensland News. We can show our mettle by grasping the nettle. Veterinarians always faced the dangers of zoonoses with a degree of stoic fatalism, but the mourned loss of two of our Members to Hendra virus in an interval of only a few months is a tragedy to which we must all react constructively. This issue focuses on infection control techniques which veterinarians must consider. There is also a comprehensive situation report on research into Hendra virus. Many will have seen this report as an Internet file, but they,
and Members who are not in that information loop, will, I hope, find hard copy useful.
One of the many factors in the transmission of Hendra virus is the probable role of flying foxes. At the Infection Control workshop in Townsville 30 August, Dr Jim Pollock told me that, due to pressure on habitat, the fruit bats are now in tobacco fields, where they come into contact with Ixodes holocyclus. Resultant maternal mortalities mean that a single agency might handle 4 to 5 hundred orphaned pups a season. This seems a high zoonotic risk for carers and veterinarians. I might have misunderstood what Jim said during a hurried coffee break, so mean to obtain more information for a forthcoming issue of Queensland News. You will remember that Dr Janine Barrett provided a summary on Bat Lyssavirus for the 2007 Winter edition.
… and a little pontification
On the matter of representative membership, there has been concern voiced in other forums that not all veterinarians are members of the Australian Veterinary Association. During the discussion at the Strategic Planning meeting on 29 August, where one of the objectives is to grow the membership, I realized that I may have been putting the cart before the horse in my own thinking. Rather than about those who are not members, I should be pleased that so many veterinarians actually are members
AVA Queensland News - October 2009
23
In Memoriam: Alister RodgersWe record with great sadness the passing of AVA member Dr Alister Rodgers, who was infected with Hendra virus and died 2 September 2009. Dr Rodgers had treated sick horses at Cawarral near Rockhampton. Our condolences go to Dr Rodgers’ wife Linda, to his family, and friends and colleagues at Rockhampton Veterinary Clinic. Dr Rodgers’ funeral was held at St Paul’s Cathedral, Rockhampton on Thursday 10 September 2009.
and that the Association is an institutionally and financially creditable organization. The reasons people study veterinary science might be quite different to the reasons they wish to associate in a professional society. The reason I studied veterinary science, for example, was that my father, who was something of a cynic after serving in the War, admired the seeming nonchalance with which the unions then held Australian industry to ransom. He dreamed of me becoming a wharfie. When it became clear that I would never have the required physique, he sighed and recommended I take up a profession. Animals seemed less threatening than people, hence BVSc Queensland 1966 instead of, say, a medical or teaching degree. The reason I joined the AVA that year, and have remained a member ever since, is quite different. I wanted to be a vet among vets. Other veterinary graduates might see themselves as researchers, microbiologist, teachers, adventurers, mothers or whatever, and so not wish to join. We don’t have to angst too much about it. Sure, some may find the cost of joining absolutely or relatively too expensive, but those cases can be handled piece-meal.
In that Strategic Planning meeting on 29 August, doodling away, I tried to imagine the people who had begun to see the need for an Australian Veterinary Association at all, a 100 years ago. Even though these founders might have had conflicting personal priorities and ambitions, it seemed to me that they must have shared and respected certain views:
• That their interests were of local, national and international relevance;
• That incuriosity was anathema;
• That facts were the essence of understanding;
• That human beings were the stewards of other animals;
• That animal disease and suffering were their adversaries;
• That geographic isolation needed to be managed.
• It seemed to me that these self-respecting founders would have come together naturally because of their perceptions of:
• Rampant disease and suffering in animals;
• Ignorance, cruelty and abuse of animals;
• Lack of scientific thinking;
• Lack of activity by governments and the community;
• Lack of communication and coordination with likeminded persons here and abroad.
It seems to me that these issues remain sharp edged and can be sensed at branch and divisional meetings in Queensland. The issues endure as reasons why the Australian Veterinary Association will continue to attract self-respecting new members now.
Axel Munthe wrote about the lack of cohesion in the medical profession in the late 1800s in Europe. In The Story of San Michele he railed against lack of fundamental knowledge and public gullibility, and the resultant quackery rampant in his profession. In an outbreak of cholera in Naples he went almost insane with frustration at his own inadequacy and at municipal stupidity. In the foreword to the 47th impression of his book he wrote: Surely a medical man, like every other human being, has the right to laugh at himself now and then to keep up his spirits, maybe even to laugh at his colleagues if he is willing to stand the risk. But he has no right to laugh at his patients. I like to think that the founders of our own Association had the same sense of proportion, and I hope that they would be satisfied that we still have our eye on the ball.
Continued from pg. 22
AVA Queensland News - October 2009
24
SHORT BITS…• Congratulations to Dr Ron Glanville, Chief Veterinary Officer and President of the South East
Queensland Branch, who has received the 2009 Equine Veterinarians Australia award for leading the team which eradicated Equine Influenza in Queensland during 2007/8. Equine Influenza was first diagnosed in August 2007. Dr Glanville was pleased to accept the award on behalf of the 1,000+ members of the eradication task force in Queensland. Dr Bruce Christie, Chief Veterinary Officer NSW, was a joint recipient of the award. The cool calm confidence of Dr Glanville and his senior colleagues certainly helped the team weather some fairly fraught and confusing months.
• The Minster for Primary Industries, the Hon. Tim Mulherin, has reiterated the Government’s support for the phasing out of mulesing of sheep by December 2010. Mr Mulherin points out in a press statement that alternative practices such as breeding resistance to fly strike and the use of anti-fly strike clips are more humane than mulesing. The lobby group Agforce has recognized that mulesing is outdated and would damage Australia’s reputation for exemplary animal welfare practices, as well as access to markets for Australian wool, according to Sheep and Wool President Mr Brent Finlay.
• Working with cattle can be fatal. Dr Sue Fowkes draws our attention to a five year survey (2003-2008) of 21 cattle related deaths in people in four US states. Risk factors were being an older male, working in enclosed areas with cattle and/or moving, herding, loading or feeding them. Death was caused mainly by blunt trauma to the head or chest. Ten of the fatalities were caused by individual bulls, 6 by individual cows, and 5 by multiple cattle. Sixteen were caused directly by the animal while 5 were secondary actions due to movement of the animals. One fatality was due to an injection of antibiotic (tilmicosin phosphate) in the victim’s pocket when the cow knocked him down. The authors comment on the need for cattle handling facilities to be designed to optimize safety.
• Ouch! In the April 2009 issue, Ms Naiomi Pham provided an article in Queensland News on the occupational health dangers of scalpel blades and ampoules in veterinary practice. Our profession seems quite prone to needlestick and sharps injuries, particularly those of us who are in small or mixed practice, women, less experienced and working hard and long hours. A survey by Peter Leggat, Derek Smith and Richard Speare published on 28 August 2009 in the Journal of Occupational Medicine and Toxicology showed that 75 percent of 664 participants were exposed to at least one NSI in the past 12 months and in 60 percent of cases the sharps may have been contaminated. The researchers recommend further study of why veterinarians are at high risk and to determine their attitudes to NSI. Thanks to Dr Andrew Easton for this sobering information.
• The Chief Veterinary Officer advises on 26 August 2009 that Human Swine Influenza H1N1 was confirmed in sick pigs at Dalby. The piggery has 370 sows and a total of 3,000 pigs. Pigs in one shed containing sows, weaners and porkers showed signs of inappetance, high temperatures and coughing. The infection spread rapidly to the other pigs. Two staff members developed signs of influenza. The closest other piggery is 15 kilometers away and it appears transmission was from people to pigs. The piggery was placed in quarantine.
• This issue contains an update on Hendra virus which was prepared in September by the Australian Biosecurity Cooperative Research Centre for Emerging Infectious Disease. The authors are Drs Jo Edmondston and Hume Field. Since that update was written, Hendra virus was also diagnosed in a horse at Bowen. The horse was euthanased on 3 September 2009 after showing signs of abdominal pain and grinding its teeth, before collapsing. The attending veterinarian, Dr Tim Annand, had attended the AVA Queensland Division Infection Control workshop in Townsville 30 August 2009.
Good news. Vets can access mortgage finance of up to 100% of the purchase price of their owner occupied practice premises. A refreshing change in the current climate we think you’ll agree.
As a specialist financier Investec Experien is committed to providing innovative financial solutions to healthcare professionals. We understand that purchasing your own rooms has the potential to be a profitable long-term business strategy for you and we’re here to help.
Our commercial mortgage products are designed to suit your cash flow, ensuring minimal difference between renting and buying. In addition, all of our products combine the benefits of competitive interest rates, dedicated expert finance consultants and a quick and easy approval process.
The future is in your hands. Call now.
1300 131 141 Australia wideNSW QLD SA VIC WA
Commercial Property Finance • Asset Finance • Deposit Facilities • Goodwill & Practice Purchase Loans • Home Loans • Income Protection & Life Insurance • Professional OverdraftInvestec Experien Pty Limited ABN 94 110 704 464 (Experien). Investec Bank (Australia) Limited ABN 55 071 292 594 (Investec Bank). All finance is subject to our credit assessment criteria. Terms and conditions, fees and charges apply. Deposit products are issued by Investec Bank. Before making any decision to invest in these products, please contact Experien, a division of Investec Bank, for a copy of the Product Disclosure Statement and consider whether these products suit your personal financial and investment objectives and circumstances. We reserve the right to cease offering these products at any time without notice. Income Protection/Life Insurance is distributed by Experien Insurance Services Pty Ltd (Experien Insurance Services) which is an authorised representative of Financial Wisdom Limited AFSL 231138 (AR No.320626). Experien Insurance Services is part owned by Investec Experien Pty Ltd.
Exper ien
Experien is a subsidiary of Investec Bank
Plan to own your practice premises? We’re with you 100%
Exper ien
Join AVA... and see the difference!The vision of the Australian Veterinary Association is for a global community that respects and values the benefits of enhanced animal health, welfare and production.
The Queensland Division mission is to be the state organisation representing and serving the interests of the veterinary profession in Queensland to act and speak with a single voice on matters of importance to our members. Why not spread the word about the benefits of AVA membership to your non member colleagues?
AVAmembershipprovides:
• Substantial discounts for AVA annual conference registration
• Subscription to the monthly Australian Veterinary Journal
• AVA eLine – monthly electronic newsletter
• Access to AVA Online, our extensive website
• A special bond with your professional peers
• Access to local branches and Special Interest Groups (SIGs)
• Pets & People Education Program
• Practice Rewards
• Practices of Excellence Award in community service
• Accredited Microchip Centres
• National Cattle Pregnancy Diagnosis Scheme
• Hospital Accreditation Scheme
• New Graduate Friendly Practice Scheme
• AVA Vet Ed – Continuing Education Scheme
TheAVAalsoprovidesfreetelephonehelplines:
• HR Advisory Service
• Telephone Counselling Service
• Accounting, Finance and Superannuation Helpline
• Legal Helpline
Withaddedbenefitssuchas:
◊ GE Money CareCredit Client Finance Plans
◊ Manchester Unity Health Insurance
◊ British Veterinary Association Journals – In Practice and The Veterinary Record
◊ New Zealand Veterinary Association Journals – NZVJ and VetScript
◊ Diners Club
◊ Mitsubishi Motors Australia
◊ Qantas Club
◊ Car rental with Thrifty, Hertz and Avis
For more information contact AVA member services on 1300 137 309
or email [email protected]

Recommend HeaRtgaRd30® PlusDogs love it. Their owners love you for it.
†When used as recommended. 1.Data on file.Merial Australia Pty Ltd, Level 6, 79 George Street, Parramatta NSW 2150. ABN 53 071 187 285. ®HEARTGARD30 is a registered trademark of Merial. ©2009 Merial Limited. All rights reserved. HTGD-09-006. H&T MCA0471/QN
HEARTGARD30® is the safe† and effective monthly heartworm treatment that dogs actually enjoy. That’s because it’s a great-tasting meaty treat made from real beef. What’s more, HEARTGARD30 PLUS also provides protection against roundworm and hookworm.
No wonder HEARTGARD30 protects more dogs around the world than any other heartworm treatment.1