Embed Size (px)
Citation preview
Clinica Chimica Acta 269 (1998) 13–20
Quantitative ELISA for platelet m-calpain: aphenotypic index for detection of carriers of
Duchenne muscular dystrophy
a a b bTajamul Hussain , D.V. Narayan Kumar , C. Sundaram , S. Mohandas ,a ,*M.P.J.S. Anandaraj
aInstitute of Genetics and Hospital for genetic diseases, Begumpet, Hyderabad 500 016, India
bNizam’s Institute of Medical Sciences, Panjagutta, Hyderabad, India
Received 28 May 1997; received in revised form 22 August 1997; accepted 3 September 1997
Abstract
In order to measure the amount of m-calpain in platelets from Duchenne muscular dystrophy(DMD) patients, carriers and controls, an enzyme linked immunosorbent assay (ELISA) has beendeveloped using polyclonal antibodies raised against m-calpain (Calcium dependent neutralprotease), purified from human placenta. Compared to controls a nine-fold increase in the level ofm-calpain was observed in all 25 DMD patients and eight obligate carrier mothers studied. Serumcreatine kinase (SCK) values of four of these obligate carriers were found to be overlapping withthat of normal values, limiting its usefulness. Since calpain levels were found to be raised in allDMD patients and obligate carriers, the estimation of calpain in all female relatives of the onesaffected with DMD (with or without raised serum CK) would prove a facile index. Populationscreening for carrier females using this cost and labour effective index may help in assessing thecarrier status and counselling the at risk families. 1998 Published by Elsevier Science B.V.
Keywords: m-Calpain; DMD; Carrier detection; Platelets; ELISA; Serum CK
1. Introduction
Duchenne muscular dystrophy (DMD), the most common of the childhooddystrophies, is inherited as an x-linked recessive disorder. In the absence of
*Corresponding author.
0009-8981/98/$19.00 1998 Published by Elsevier Science B.V. All rights reserved.PII S0009-8981( 97 )00189-7
14 T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20
effective treatment for DMD, genetic counselling acquires great importance forwomen at risk of being carriers of this condition. The assessment of the risk of awoman being a carrier is done by serum creatine kinase estimation and DNAanalysis.
Detection rate of serum CK in obligate carriers lies in the neighbourhood of66% unlike in mothers of simplex cases where it is lower than in obligatecarriers [1,2]. Skewed distribution at higher values and substantial overlapbetween populations make it difficult to interpret SCK results. Although DNAanalysis by various molecular techniques provides direct and reliable infor-mation in deciding the carrier status, it can be labour intensive especially theanalysis of such a vast gene as dystrophin and at times complex, makinginterpretation difficult.
Striking alterations in intracellular calcium and membrane abnormalities aresome of the early changes observed in muscle [3] and non muscle cells such asplatelets [4,5], lymphocytes [6,7], erythrocytes [8,9] and fibroblasts [10] ofDMD patients. Whereas in obligate carriers the observed increase in calcium isintermediary [4]. The muscle and non muscle cells of DMD patients and carriersare therefore subjected to the consequences of the enhanced calcium. Theincreased calcium affects the cellular processes that are calcium sensitive anddependent. One such calcium dependent enzyme is calpain, an intracellular nonlysosomal thiol protease. Calpain exists in two isoforms namely milli and microcalpains (m-calpain, m-calpain) which require for activation, milli molar andmicro molar concentrations of calcium respectively. Calpain is implicated inmuscle degradation [11,12]. Increase in Calpain was first reported in muscle andthis has been attributed to an increase in intracellular calcium [13,14].
Our estimation of m-calpain (also known as m-CANP) by direct activity assay[14] and by semi quantitative dot immunoblot [15] showed an elevation ofm-calpain in platelets of DMD patients and carriers.
In order to assess the status of calpain in platelets of DMD patients andcarriers, and to establish the m-calpain assessment as a phenotypic index, a rapidand cost effective ELISA has been developed.
2. Materials and methods
2.1. Isolation of platelets
Blood samples (10 ml) using Heparin as anti coagulant were collected from25 DMD patients (6–12 years of age), eight obligate carriers (25–45 years ofage) and 18 probable carriers (19–40 years of age). Blood samples were alsocollected from eight healthy boys of 5–15 years of age and from 14 healthyfemales of 25–40 years of age as age and sex matched controls. Blood samples
T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20 15
were collected at the hospital, avoiding the transportation of the samples whichmight affect the platelets. Individuals suspected of DMD were studied byclinical examination, pedigree analysis, EMG, muscle biopsy analysis and serumCK estimation. Obligate and probable carriers were categorized by their detailedfamily history. Obligate carriers are defined as those mothers that have one ortwo affected sons and a relative with DMD in the female line of inheritance.Obligate carrier status was thus established only by the detailed family pedigree.Platelets from the blood samples were isolated on Ficoll hypaque using gradientcentrifugation method [16] and the washed cells were sonicated using Imecosonicator. Cell lysis was completed with eight, 15 sec bursts with intermittentcooling on ice. Protein concentration of lysates was estimated by Lowry’smethod [17] using BSA as standard.
2.2. Purification of m-calpain
m-calpain was purified to homogeneity from human placenta, according to themethod of Shastri and Anandaraj [18]. The purified enzyme was homogeneousin nature as judged by denaturing polyacrylamide gel electrophoresis (PAGE).Active subunit of the enzyme was electroeluted and the integrity of the subunitwas established by PAGE.
2.3. Raising antisera against m-calpain
Antesera was raised against purified m-calpain in male albino rabbits and IgGfraction of the antisera was obtained by affinity chromatography on proteinA-sepharose column [19].
2.4. Enzyme linked immunosorbant assay (ELISA)
The method described for quantitation of platelet m-calpain is an indirect-noncompetitive ELISA with antigen immobilized on the solid phase microtitre plate(NUNC Kamtrup, Denmark), amplified with a alkaline phosphatase labelledsecond antibody. Optimum assay conditions were determined by initial doseresponse study. Wells were coated with 100 ml of antigen solution (plateletlysate or purified m-calpain) diluted in carbonate buffer (14 mM Na CO and 462 3
mM NaHCO pH 9.2) at 48C overnight. A rank of wells in each plate was filled3
with carbonate buffer as blank. Plate was washed three times with PBS-T (137mM Na Co ; 2.7 mM KCl; 8.1 mM Na HPO and 1.5 mM KH PO pH 7.42 3 2 4 2 4
and 0.1% Tween-20) at 5 min intervals. Blocking of non specific binding siteswas done with: 3% BSA (dissolved in PBS pH 7.4) for 2 h at room temperature.After washing three times with PBS-T, 100 ml of specific antibodies (1:2000dilution in 1% BSA/PBS) were added and the plate was incubated for 3 h at
16 T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20
room temperature. After rinsing three times at 5 min interval with PBS-T, 100ml alkaline phosphatase conjugated second antibody (1:1000 diluted in 1%,BSA/PBS) was added. The plate was further incubated for 2 h at roomtemperature. Excess second antibody was removed by washing five times at 5min interval with PBS-T. The bound peroxidase was detected by the addition of100 ml of substrate solution (10 mg of p-nitro phenyl phosphate (pNPP) in 10ml diethanolamine (pH 9.5) containing 0.5 mM MgCl and the reaction was2
allowed to develop for 10 min at room temperature. The reaction was stopped byadding 100 ml of stop solution (0.1 M EDTA) and the absorbance was measuredat: 409 nm wavelength.
2.5. Estimation of Serum CK activity
Serum samples from 50 healthy females of 19–45 years of age wereprocessed for SCK estimation in order to establish the upper reference cut offpoint for control population. Normal reference values in females were estab-lished by cumulative frequency plots, where the 97.5th percentile of the CKnormal reference interval was selected as the cut off point [20]. SCK was alsoestimated in eight obligate and 18 probable carriers of DMD. 20 ml of serumwas mixed with 1 ml of working solution containing creatine phosphate, ADP,glucose, hexokinase, NADP and Glucose-6-phosphate dehydrogenase. TheSerum Creatine Kinase enzyme is assayed by quantitating the ATP generatedwhen ADP is phosphorylated by creatine phosphate. The generated ATP byphosphorylation of ADP is indirectly measured by converting glucose toglucose-6-phosphate and its further oxidation to gluconate-6-phosphate. Thegeneration of gluconate-6-phosphate requires the reduction of NADP toNADPH, which process is monitored by change in absorption at 340 nm. Meanabsorbance increase per minute (D /min) was determined. Serum CK activity(IU/ l) 5 D /min 3 8199.
2.6. Preparation of standards for ELISA
m-calpain standards were prepared with serial dilution (7.5 ng–60 ng/ml) incarbonate buffer. Statistical analysis was done by student’s t-test.
3. Results
The standard curve for purified m-calpain was obtained by the ELISAprocedure detailed in materials and methods. Linear response was observed inthe range of 7.5 ng–60 ng/ml.
Similarly m-calpain was quantitated in platelets from patients, obligate
T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20 17
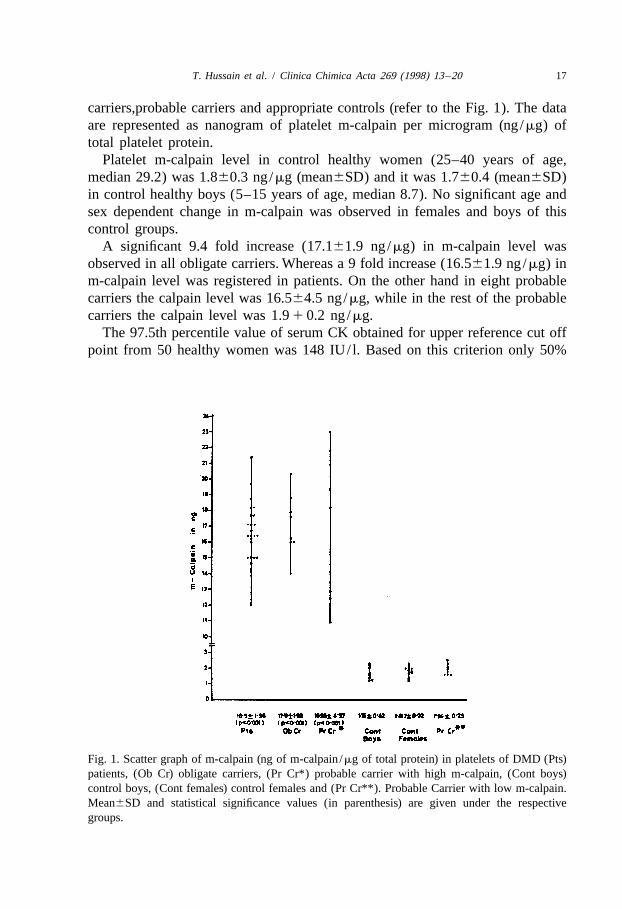
carriers,probable carriers and appropriate controls (refer to the Fig. 1). The dataare represented as nanogram of platelet m-calpain per microgram (ng/mg) oftotal platelet protein.
Platelet m-calpain level in control healthy women (25–40 years of age,median 29.2) was 1.860.3 ng/mg (mean6SD) and it was 1.760.4 (mean6SD)in control healthy boys (5–15 years of age, median 8.7). No significant age andsex dependent change in m-calpain was observed in females and boys of thiscontrol groups.
A significant 9.4 fold increase (17.161.9 ng/mg) in m-calpain level wasobserved in all obligate carriers. Whereas a 9 fold increase (16.561.9 ng/mg) inm-calpain level was registered in patients. On the other hand in eight probablecarriers the calpain level was 16.564.5 ng/mg, while in the rest of the probablecarriers the calpain level was 1.9 1 0.2 ng/mg.
The 97.5th percentile value of serum CK obtained for upper reference cut offpoint from 50 healthy women was 148 IU/ l. Based on this criterion only 50%
Fig. 1. Scatter graph of m-calpain (ng of m-calpain /mg of total protein) in platelets of DMD (Pts)patients, (Ob Cr) obligate carriers, (Pr Cr*) probable carrier with high m-calpain, (Cont boys)control boys, (Cont females) control females and (Pr Cr**). Probable Carrier with low m-calpain.Mean6SD and statistical significance values (in parenthesis) are given under the respectivegroups.
18 T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20
i.e. four of the eight obligate carriers and 22% i.e. four of the eighteen probablecarriers exceeded this cut off point.
4. Discussion
Many of the studies on serum CK in obligate carriers show that inapproximately 30% subjects, the values overlap that of controls [1,2]. The use ofCK test depends on how strictly the control reference range is interpreted asvalues for serum CK activities differ from one laboratory to another and severalfactors such as genetic makeup, age and pregnancy are reported to influence thesame. The change in CK activity with age, the skewed distribution and thesubstantial overlap between control and carrier population limit its use in carrierdetection.
In an ever increasing efforts to precisely diagnose DMD carriers or the foetusat risk, DNA analysis has been emphasized. Relatively large size of the gene andhigh frequency of recombination and mutation events within the dystrophinlocus, continue to pose difficulties in the genetic counselling of DMD carriersand renders the conclusions of molecular analysis less clear cut. Therefore,application of DNA technology to new mutations can at time be very complexespecially when carriers are non-informative for polymorphism. Hence aphenotypic index can be economic and simplifies the carrier detection pro-cedures.
Only 50% of obligate carriers and 22%, probable carriers in the present studyshow CK values higher than the upper reference value of normal controls, whichunderlines the inadequacy of CK test for carrier detection. On the other hand allthe obligate carrier mothers and patients showed elevated calpain levels notoverlapping with controls (refer to Fig. 1). This indicates the usefulness ofcalpain as a phenotypic index in identifying the true carriers. The polarisation ofpossible carriers distinctly into high and low calpain groups (refer to Fig. 1) is apossible reflection of true status with respect to presence of DMD gene. Thisdistinct polarisation further establishes the discriminatory power of calpain indifferentiating carriers from non carriers.
Haldane [21] estimated the rate of spontaneous mutation of the gene forhaemophilia on the assumption that the number of genes lost by the failure ofaffected males to reproduce must equal the number of new mutations if the poolof defective genes is to remain stable. Since one third of the X-chromosomes inpopulation occur in males, and DMD is genetically lethal, one third of genes forthis disorder are lost with each generation. Under the assumption that themutation rates in males and females were equal, one third of the males affectedwith the disorder have been thought to be the result of new mutations.
Out of 19 mothers studied (refer to the Fig. 1) eight are obligate carriers based
T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20 19
on family history and whose calpain values were also found elevated. Theremaining 11 cases who are the mothers of simplex cases, revealed that in onlysix cases the values of calpain were as high as in the obligate carrier mothersand in the remaining six cases the values were found to be in the control range.If Calpain values were applied to detect carrier females, at most only five of the25 cases appear to represent new mutations. Applying the Haldane’s formulam 5 (1 2 f ) u /(u 1 v), where u and v are the mutation rates in females andmales and f the fitness, which is taken to be zero as affected males in DMD failto reproduce and m is the proportion of affected males with new mutations.Setting m 5 5/25 5 0.2. The value of 0.2 is lower than value of 0.33 prom-ulgated by Haldane, which indicates that majority of affected males are born tocarrier females. Such a value, being less than 0.3, was also made by Pickard etal. [7] and Bucher et al. [22]. However the number of patients and carriersobserved in our study is small and therefore subject to random errors.
Incidentally we also confirmed the calpain results by multiplex PCR (data notshown). All the patients who exhibited the DNA deletion mutations were alsofound positive for the calpain test.
Our earlier studies on a few Limb girdle [14] and Becker muscular dystrophycases have shown intermediary platelet calpain activities. These observedintermediary calpain ranges could be exploited in differential diagnosis of thesemyopathies.
Since the calpain test is simple, cost effective and could be performed fromeasily accessible blood sample, it is well suited for routine and wide spread use.
References
[1] Dreyfus JC, Schapira F, Demos J, Schapira G. The value of serum enzyme determinations inthe identification of dystrophic carriers. Ann NY Acad Sci 1986;138:304.
[2] Gruemer HD, Miller WG, Chinchilli VM et al. Prediction of carrier status in Duchennedystrophy by creatine kinase measurement. J Clin Pathol 1985;84:655–8.
¨ ´[3] Bodensteiner JB, Engel AG. Intracellular calcium accumulation in Duchenne dystrophy andother myopathies. A study of 567 000 muscle fibres in 114 biopsies. Neurology1978;28:439–45.
[4] Bonadonna G, Zatti M. Platelet intracellular calcium in patients with Duchenne musculardystrophy. Clin Chim Acta 1988;49:11–122.
[5] Bonadonna G, Corradine P, Lechi C, De Grandis D, Zatti M. Decreased A 23187-inducedplatelet aggregation in Duchenne muscular dystrophy. Muscle Nerve 1984;7:493.
[6] Nicholson GA, Sugars J. Decreased A 23187 induced Chemiluminescence in Duchennemuscular dystrophy granulocytes. J Neurol Sci 1982;56:11–66.
[7] Pickard NA, Gruemer HD, Verrill HL et al. Systemic membrane defect in the proximalmuscular dystrophies. New Engl J Med 1978;229:841–6.
[8] Dise CA, Goodman DBP, Lake WC, Hodson A, Rasmussen H. Enhanced sensitivity tocalcium in Duchenne muscular dystrophy. Biochem Biophys Res Commun 1977;79:1285–92.
20 T. Hussain et al. / Clinica Chimica Acta 269 (1998) 13 –20
[9] Metheson DW, Howland JL. Erythrocyte deformation in human muscular dystrophy. Science1974;184:165–6.
21[10] Fingerman E, Campise J, Pardee AB. Defective Ca -metabolism in Duchenne musculardystrophy: effects on cellular and viral growth. Proc Natl Acad Sci (USA) 1984;81:7517–621.
21[11] Busch WA, Stromer MH, Gikk DE, Suzuki A. Ca -specific removal of Z-lines from rabbitskeletal muscle. J Cell Biol 1972;52:367–81.
21[12] Dayton WR, Goll DE, Zeece MG, Robson RM, Reville WJ. A Ca -activated proteasepossibly involved in myofibrillar protein turnover. Purification from porcine muscle. .Biochemistry 1975;15:2150–8.
[13] Kar NC, Pearson CM. A Calcium activated neutral protease in normal and dystrophic humanmuscle. Clin Chim Acta 1975;73:293–7.
[14] Rabbani N, Moses L, Anandavalli TE, Anandaraj MPJS. Calcium activated neutral proteasefrom muscle and platelets of Duchenne muscular dystrophy. Clin Chim Acta 1984;143:163–8.
[15] Jagadeesh G, Shailaja B, Lavanya M, Kusuma Kumari C, Anjaneyulu A, Anandaraj MPJS.Importance of monitoring calcium and calcium related properties in carrier detection forDuchenne muscular dystrophy. Indian J Med Res 1994;99:283–8.
[16] Phillips DR, Agin PP. Platelet plasma membrane glycoproteins. J Biol Chem 1977;252:2121.[17] Lowry OH, Rosenbrough NJ, Farr A, Randall RJ. Protein measurement with folin phenol
reagent. J Biol Chem 1981;193:255–75.[18] Shastri R, Anandaraj MPJS. A low calcium requiring calcium activated neutral proteinase
from human placenta. Biochem Biophys Acta 1986;873:260–6.[19] Tijssen P. Laboratory Techniques in Biochemistry and Molecular Biology. In: Burdon RH,
Van Knippenberg PH, editors. Practice and Theory of Enzyme Immuno assays, Elsevier,Amsterdam, 1985;15:105–113.
[20] Gruemer HD, Miller WG, Chinchilli VM et al. Are reference limits for serum CreatineKinase valid in detection of the carrier state for Duchenne muscular dystrophy?. Clin Chem1984;30:724–30.
[21] Haldane JBS. The rate of spontaneous mutation of human gene. J Genet 1935;31:31726.[22] Bucher K, Ionasescu V, Hanson J. Frequency of new mutants among boys with Duchenne
muscular dystrophy. Am J Med Genet 1980;7:27–46.





























