Embed Size (px)
Citation preview
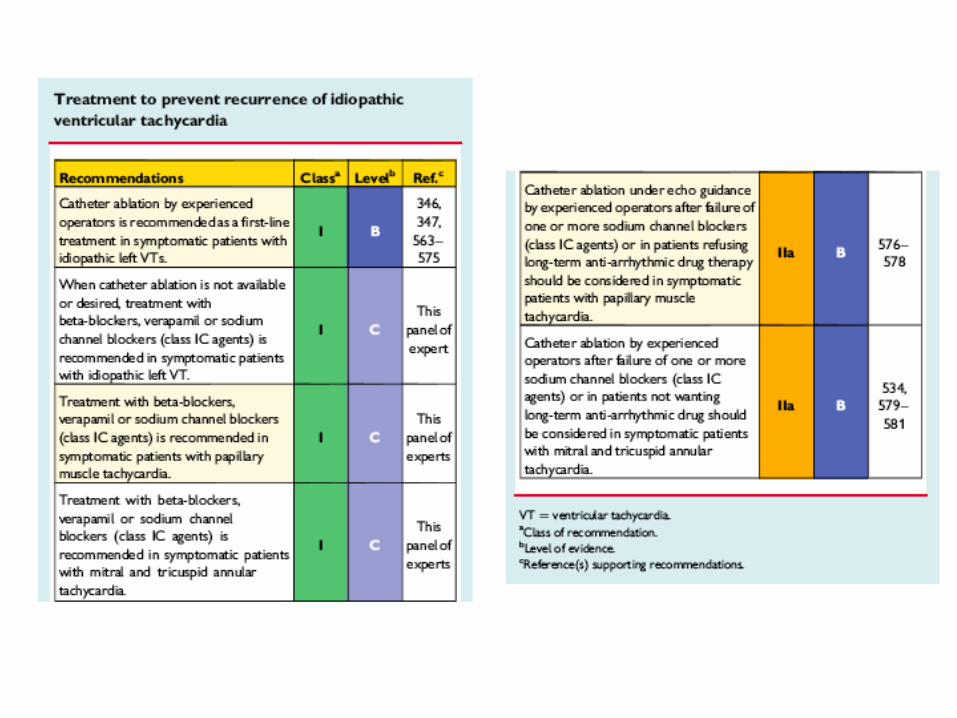
Quando procedere all’ablazione della tachicardia ventricolare
rinunciando al defibrillatore
Leonardo Calo’
Direttore U.O.C. Cardiologia
Policlinico Casilino -Roma
DISCLOSURE INFORMATION
No conflict of interest

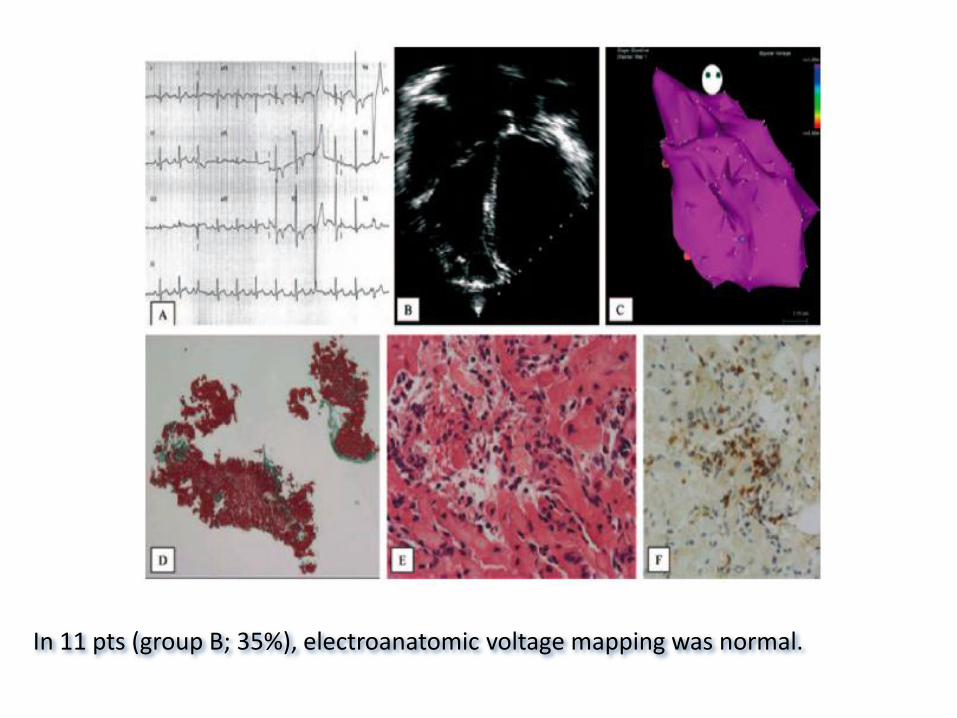
In 11 pts (group B; 35%), electroanatomic voltage mapping was normal.
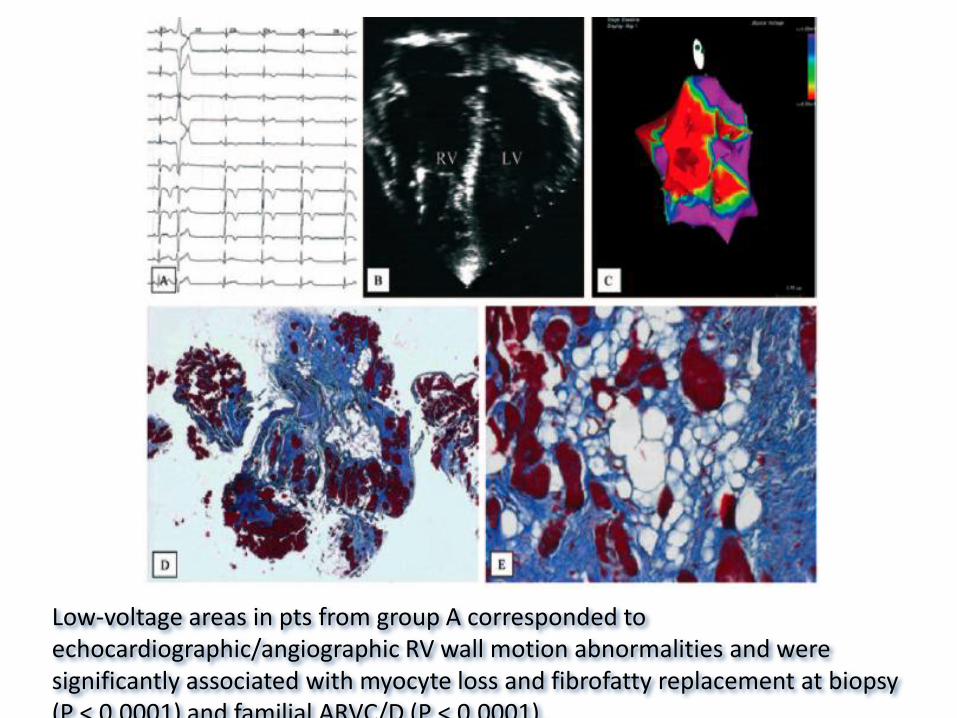
Low-voltage areas in pts from group A corresponded to echocardiographic/angiographic RV wall motion abnormalities and were significantly associated with myocyte loss and fibrofatty replacement at biopsy (P < 0.0001) and familial ARVC/D (P < 0.0001).
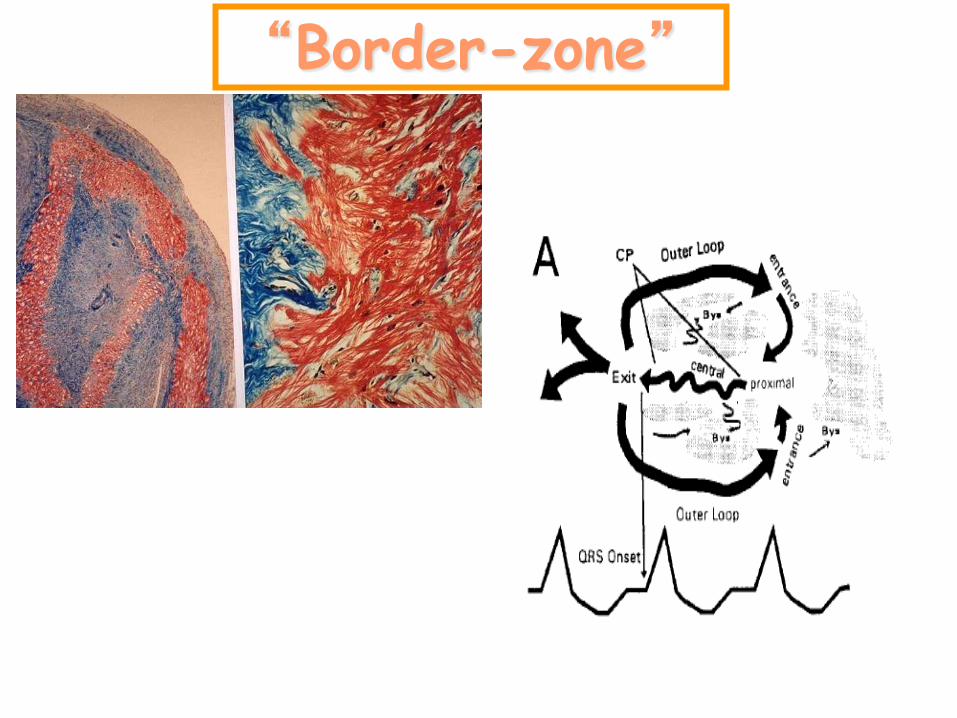
“Border-zone”
I
Abld
I
Abld
I
Abld
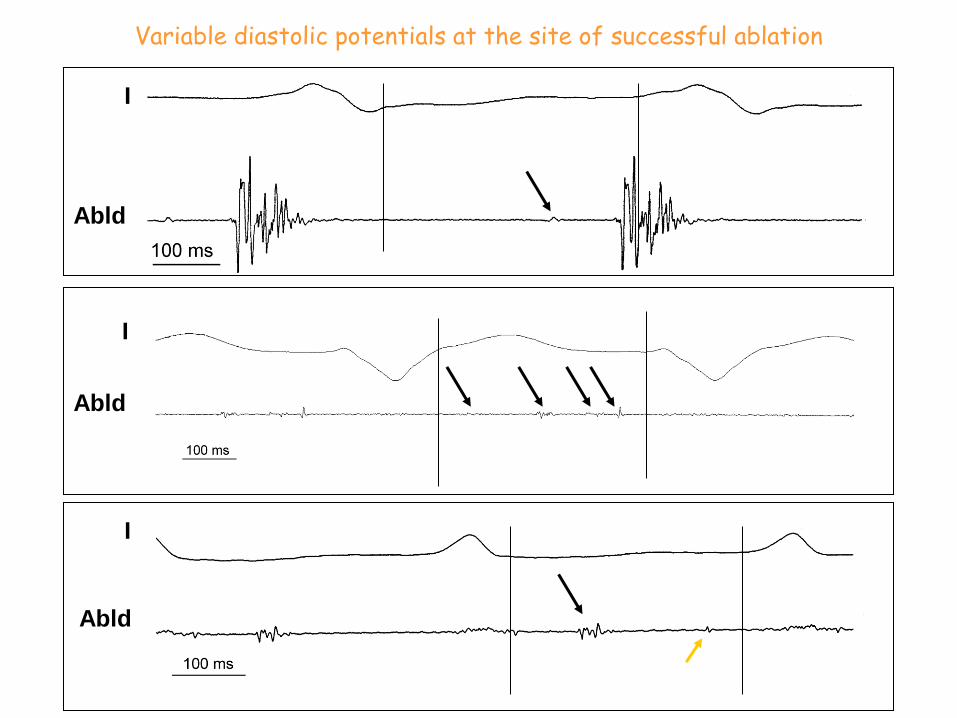
Variable diastolic potentials at the site of successful ablation
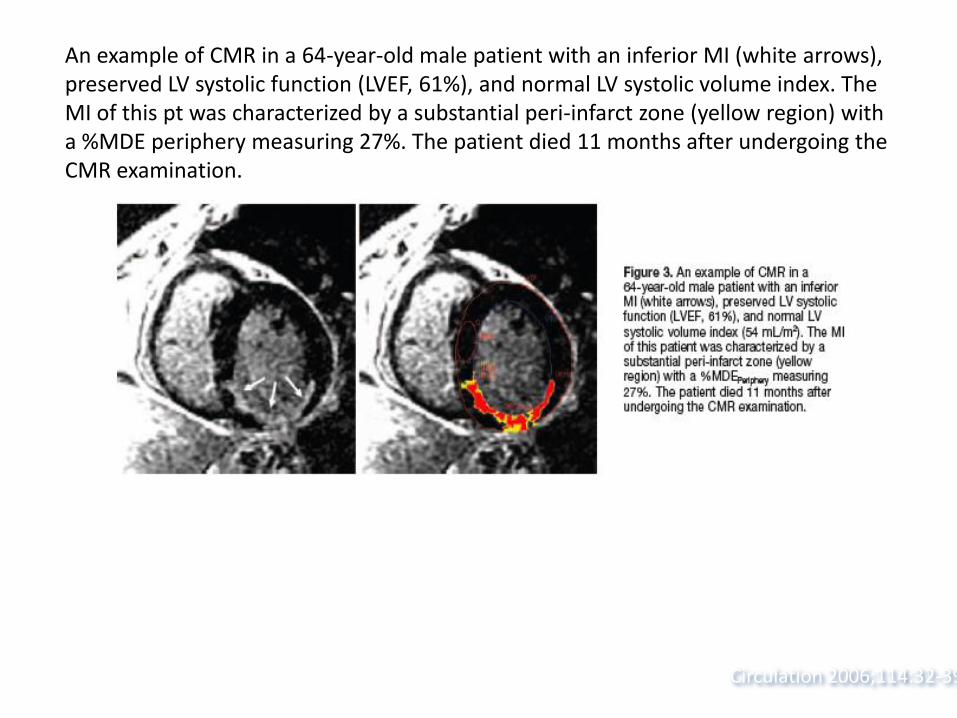
Circulation 2006;114:32-39
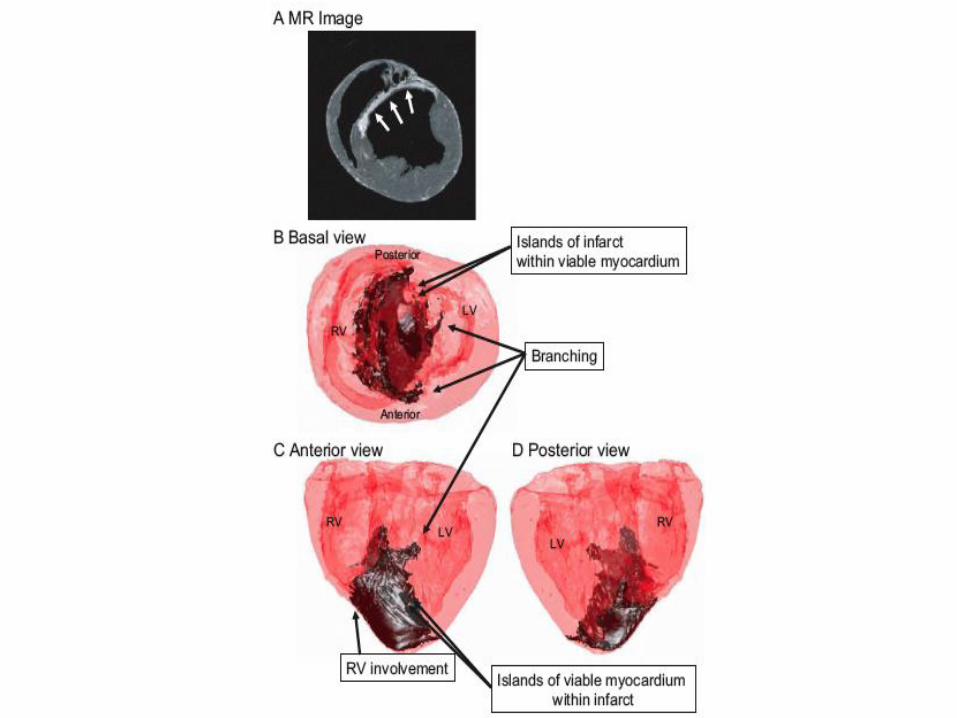
An example of CMR in a 64-year-old male patient with an inferior MI (white arrows), preserved LV systolic function (LVEF, 61%), and normal LV systolic volume index. The MI of this pt was characterized by a substantial peri-infarct zone (yellow region) with a %MDE periphery measuring 27%. The patient died 11 months after undergoing the CMR examination.
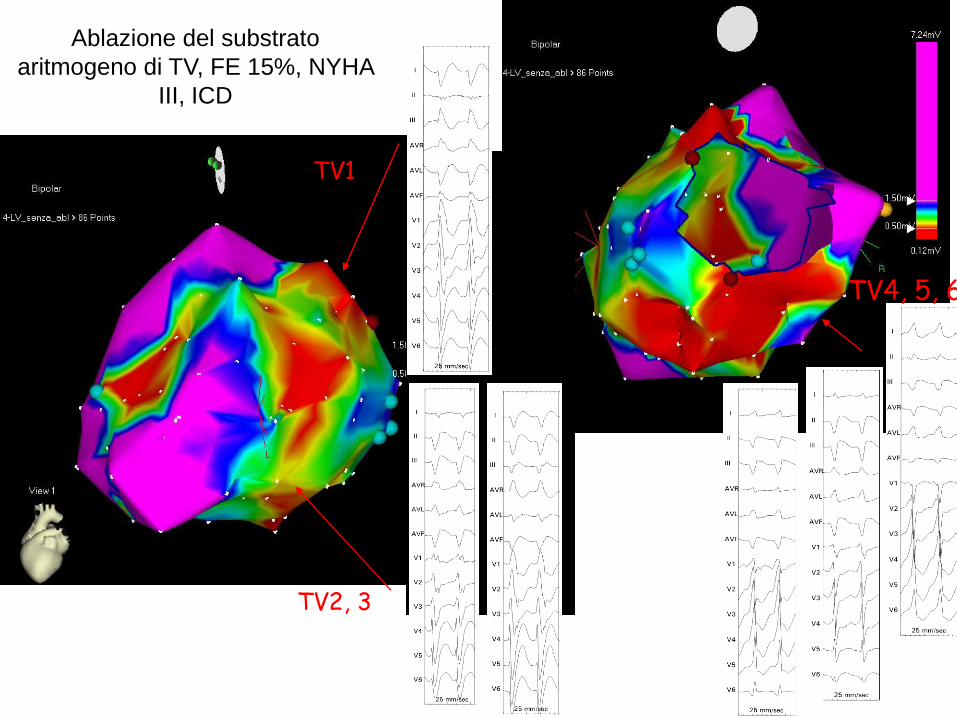
TV1
TV2, 3
TV4, 5, 6
Ablazione del substrato
aritmogeno di TV, FE 15%, NYHA
III, ICD

Con isoproterenolo
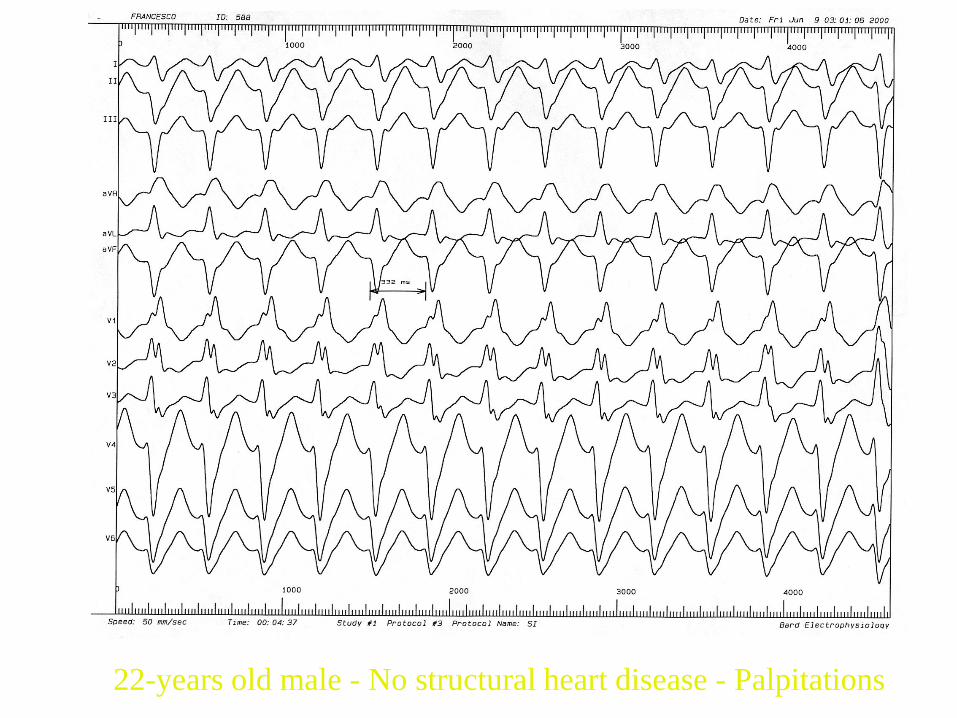
22-years old male - No structural heart disease - Palpitations
* * *
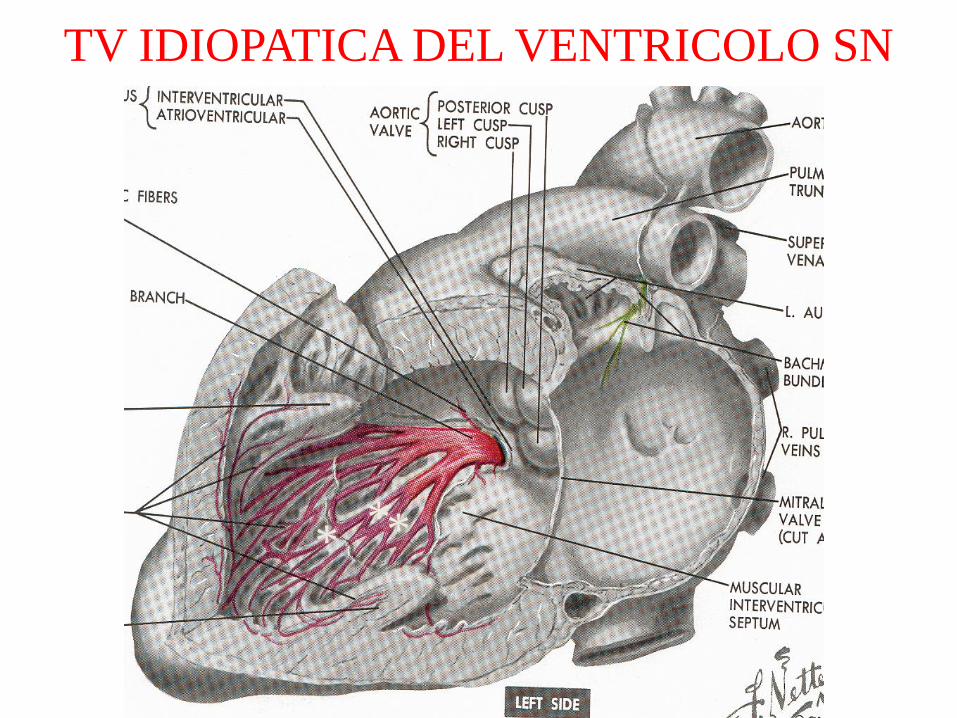
TV IDIOPATICA DEL VENTRICOLO SN
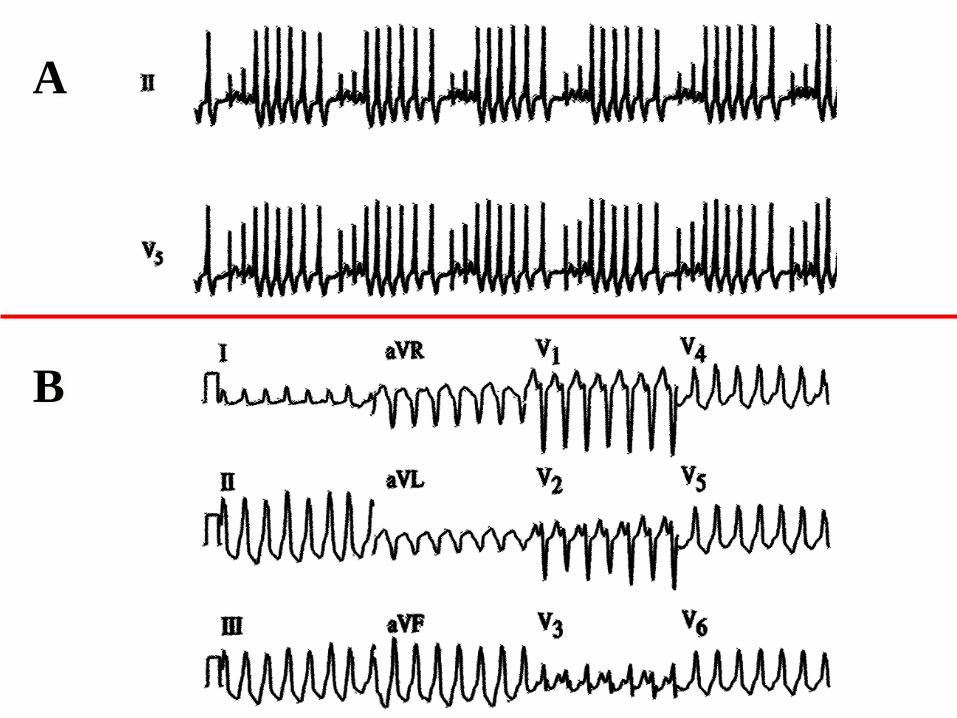
A
B
* *
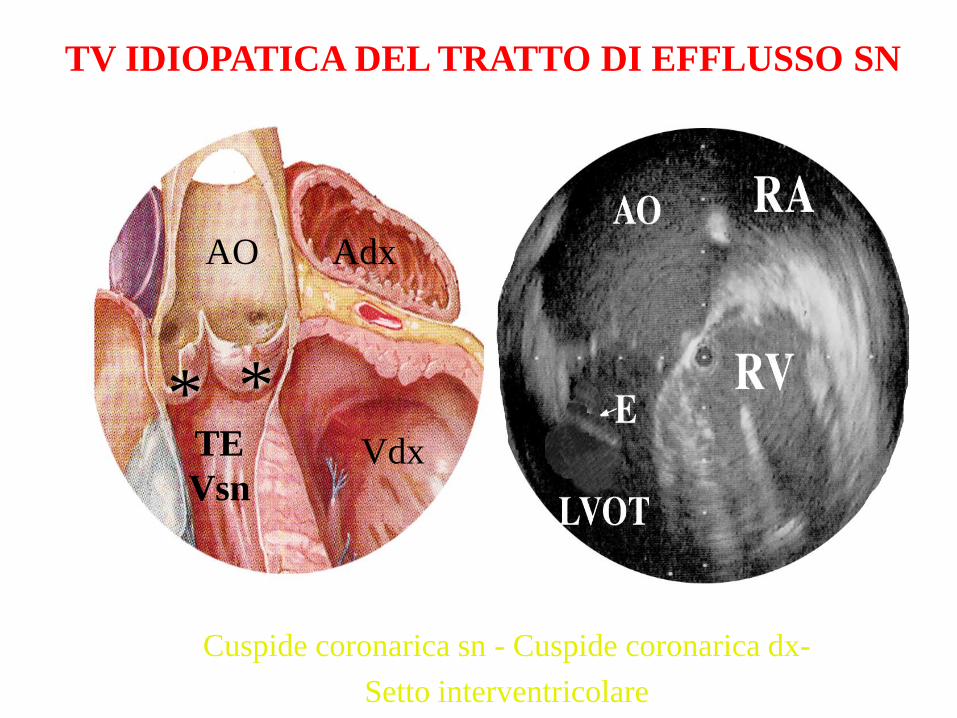
AO Adx
Vdx TE
Vsn
TV IDIOPATICA DEL TRATTO DI EFFLUSSO SN
Cuspide coronarica sn - Cuspide coronarica dx-
Setto interventricolare
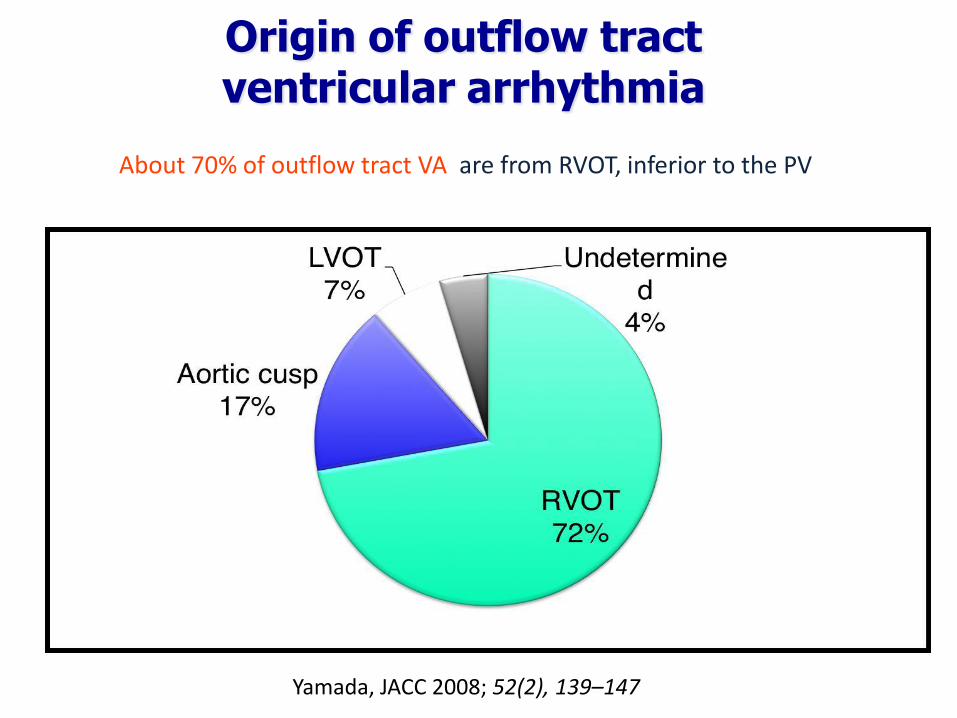
Origin of outflow tract ventricular arrhythmia
Yamada, JACC 2008; 52(2), 139–147
About 70% of outflow tract VA are from RVOT, inferior to the PV
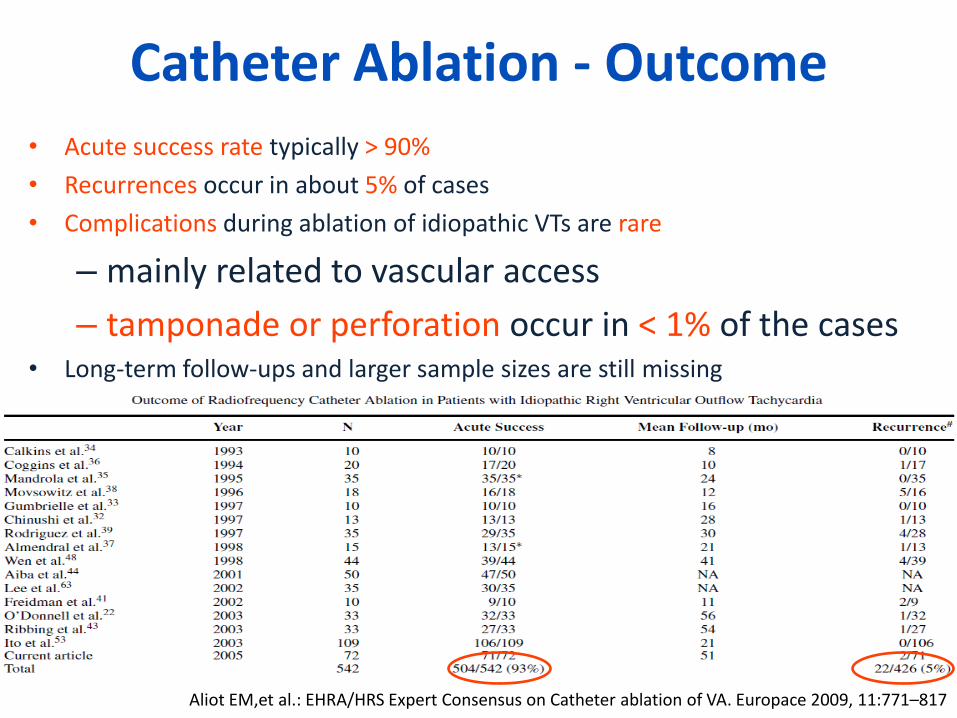
Catheter Ablation - Outcome
Aliot EM,et al.: EHRA/HRS Expert Consensus on Catheter ablation of VA. Europace 2009, 11:771–817
• Acute success rate typically > 90%
• Recurrences occur in about 5% of cases
• Complications during ablation of idiopathic VTs are rare
– mainly related to vascular access
– tamponade or perforation occur in < 1% of the cases • Long-term follow-ups and larger sample sizes are still missing


Tachycardia-Related Cardiomyopathy
• TCM is caused by very frequent runs of VT as well as PVCs
• The threshold of ectopy needed to result in TCM has been evaluated by many authors:
– Yarlagadda et al. PVC > 17,000 daily
– Takemoto et al. PVC > 20% daily
– Baman et al. PVC > 24% daily
– Hasdemir et al. PVC > 16% daily
– Niwano et al. PVC > 31,268 daily
• Thus, patients likely need to have > 10,000 PVCs daily over a substantial period (≈4 years) to cause TCM
• TCM is uncommon and occurred in 5-6% of patients
Eric N. Prystowsky et al. J Am Coll Cardiol 2012;59:1733–44
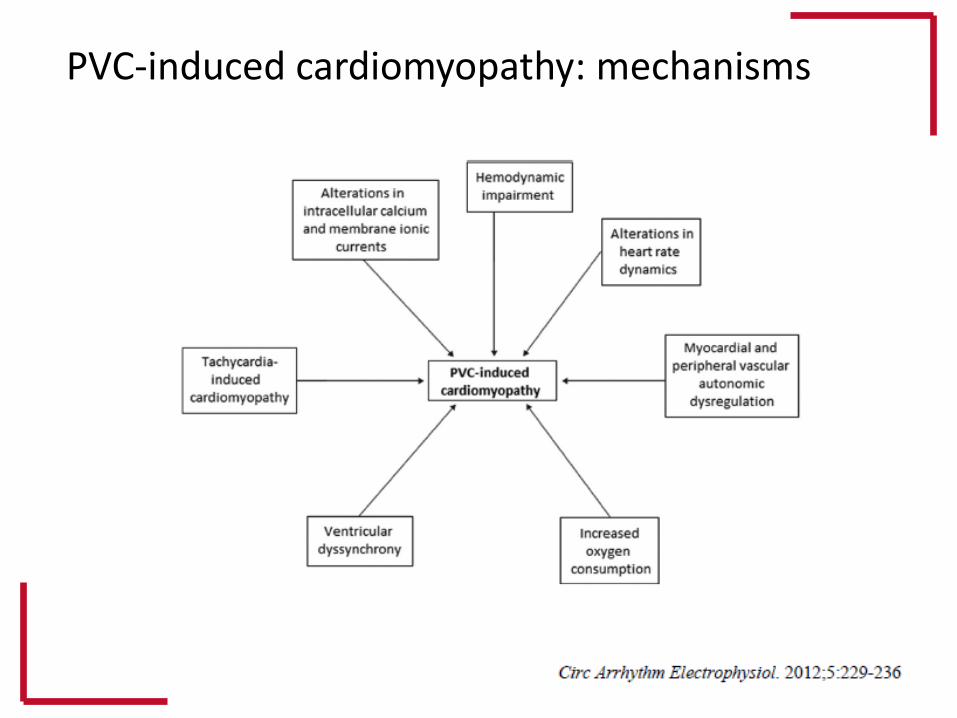
PVC-induced cardiomyopathy: mechanisms
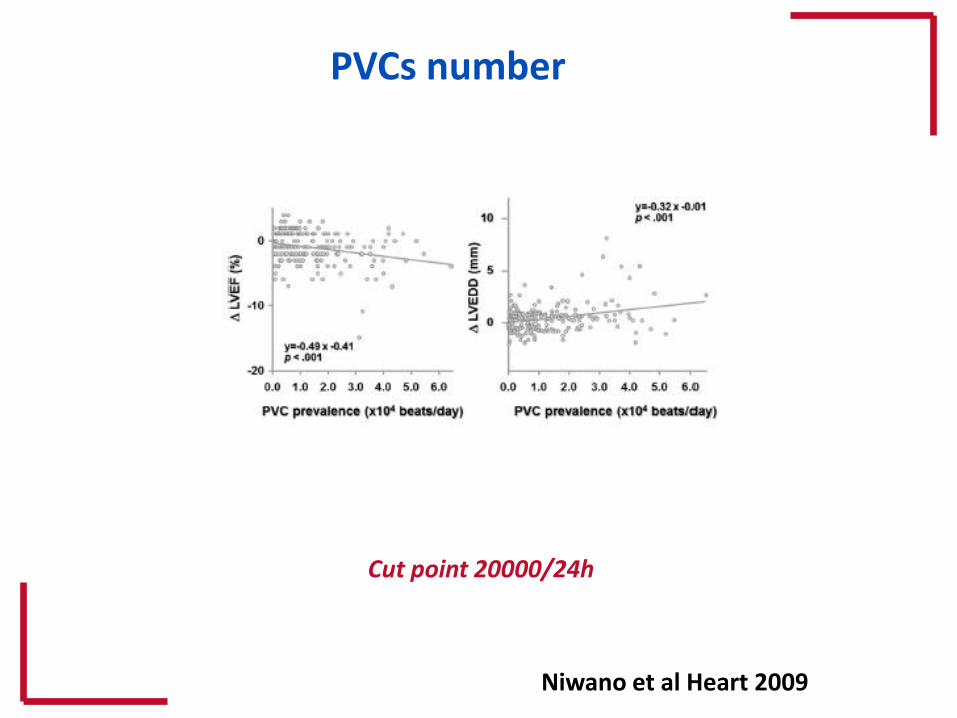
Niwano et al Heart 2009
Cut point 20000/24h
PVCs number
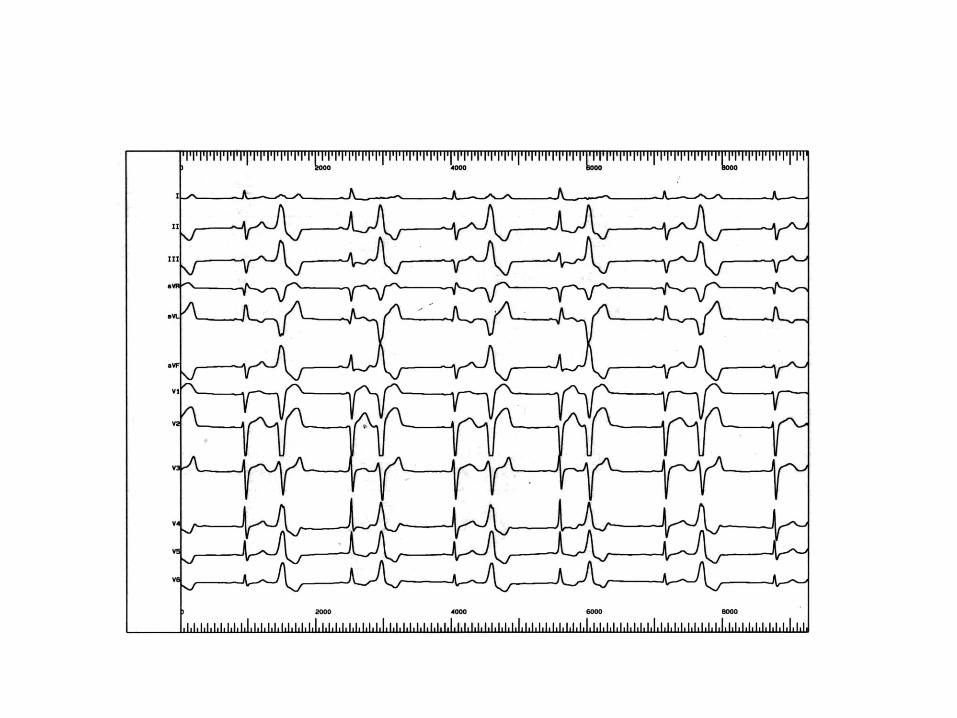
Case 1
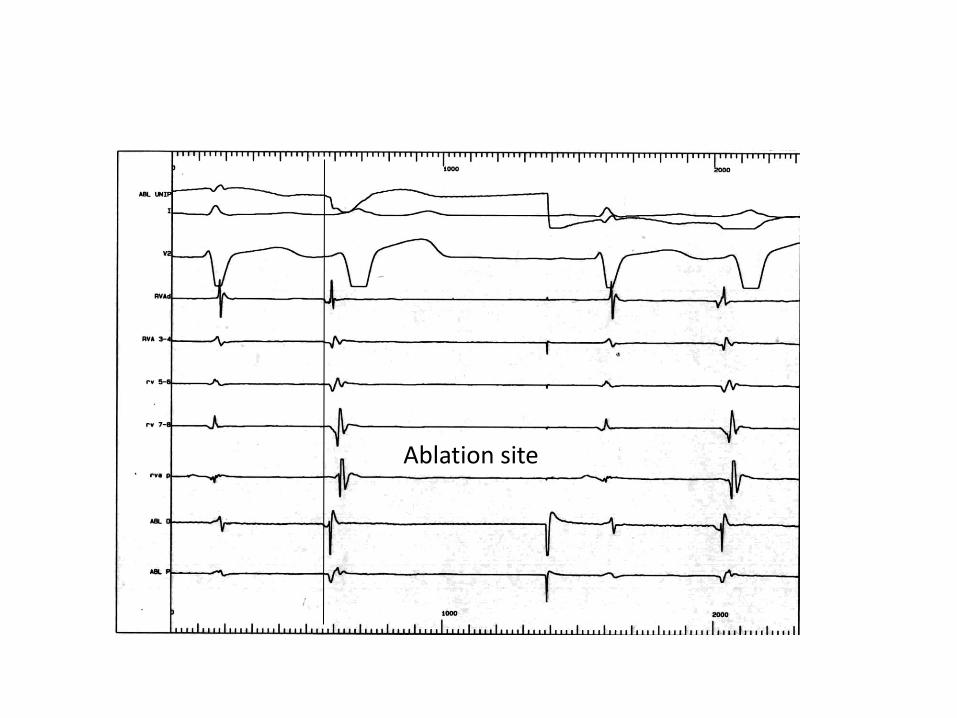
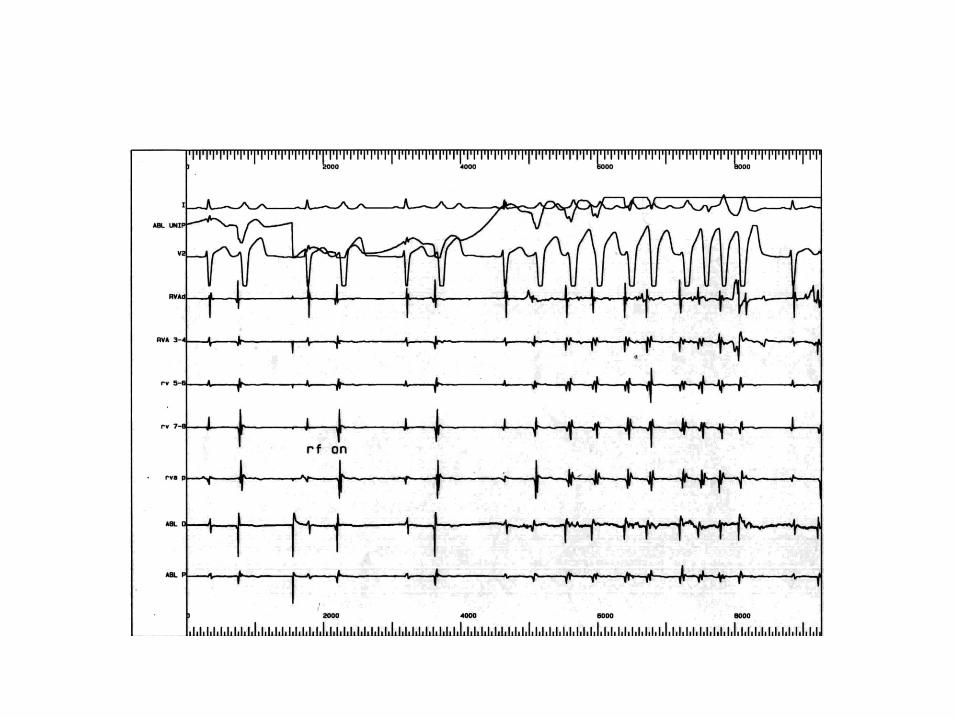
Ablation site
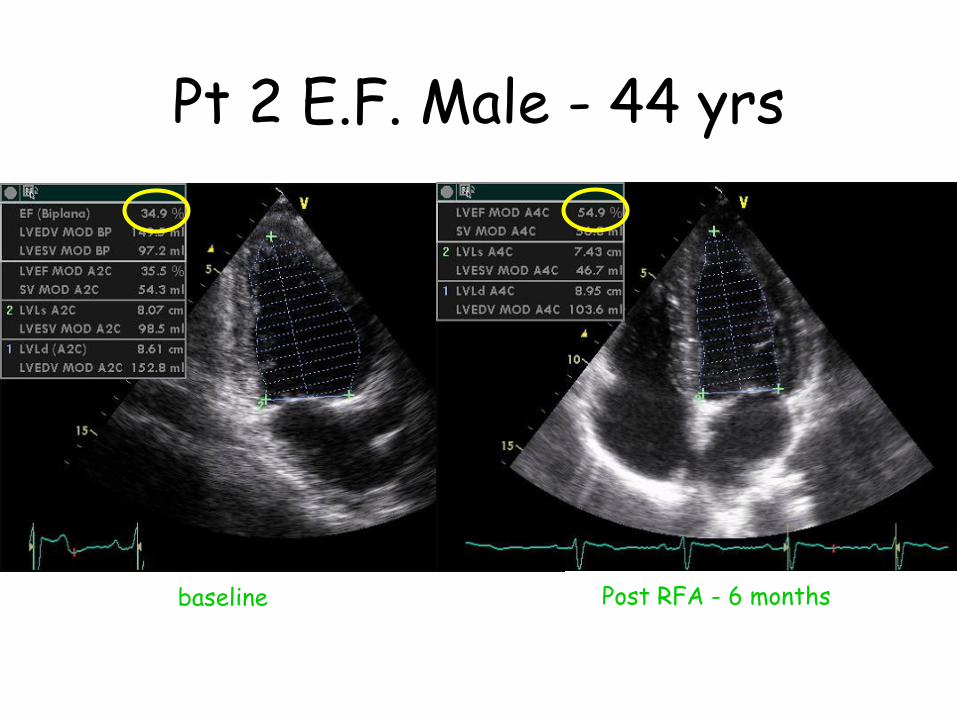
Pt 2 E.F. Male - 44 yrs
baseline Post RFA - 6 months
Case 2
Medical history
M.A. 59 years old female
Hypercholesterolemia; no other risk factors
Highly symptomatic for palpitations since several months
NYHA class II
Echo: Mitral valve prolapse with mild regurgitation; EF 46%; LVED 56 mm
On therapy with betablockers: persistence of symptoms
Holter: sinus rhythm; 34000 PVCs (two morphologies; one highly predominant); couplets; frequent runs of NSVT
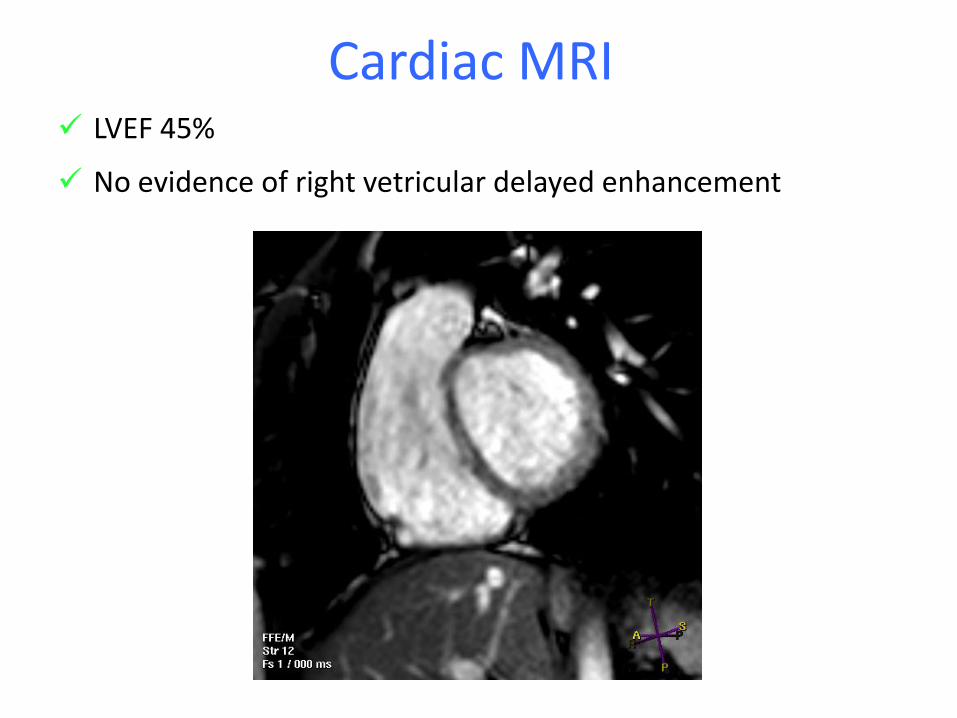
Cardiac MRI LVEF 45%
No evidence of right vetricular delayed enhancement
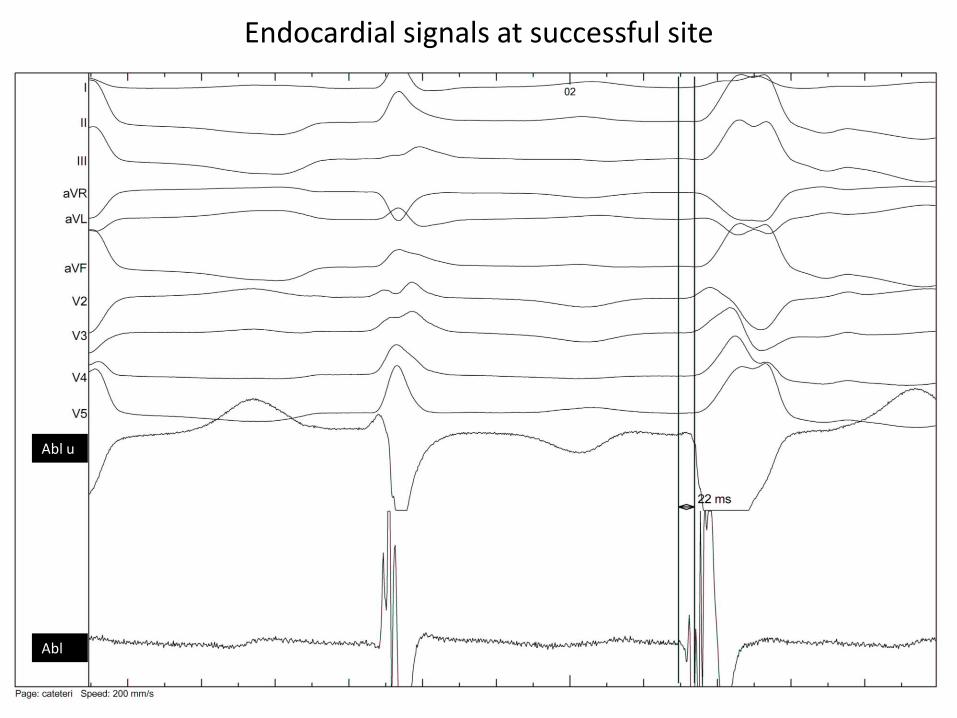
Abl u
Abl
Endocardial signals at successful site
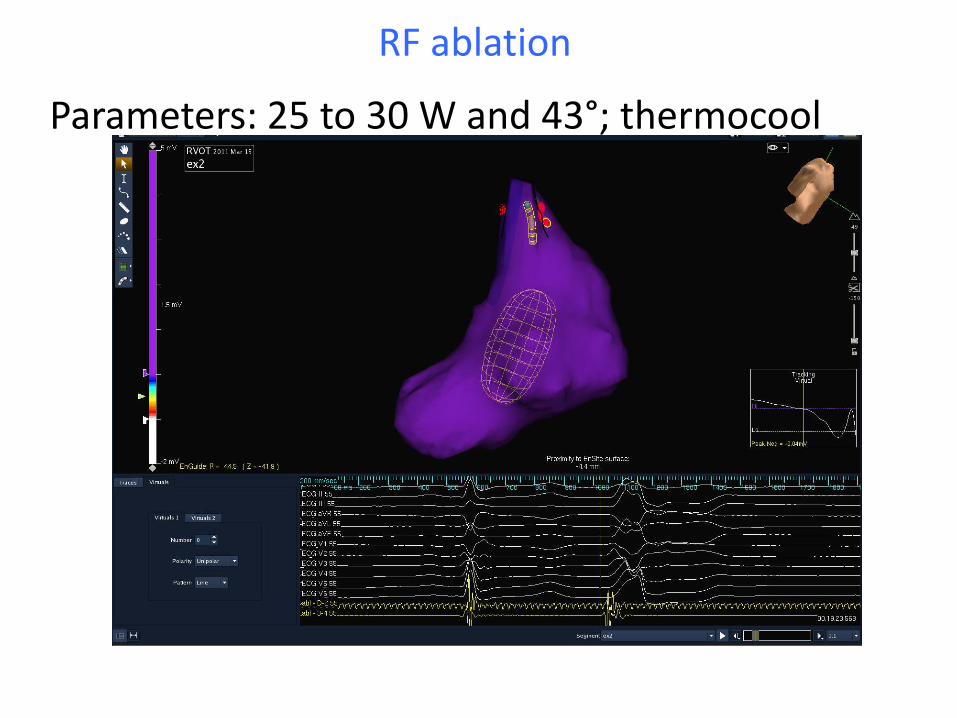
RF ablation
Parameters: 25 to 30 W and 43°; thermocool
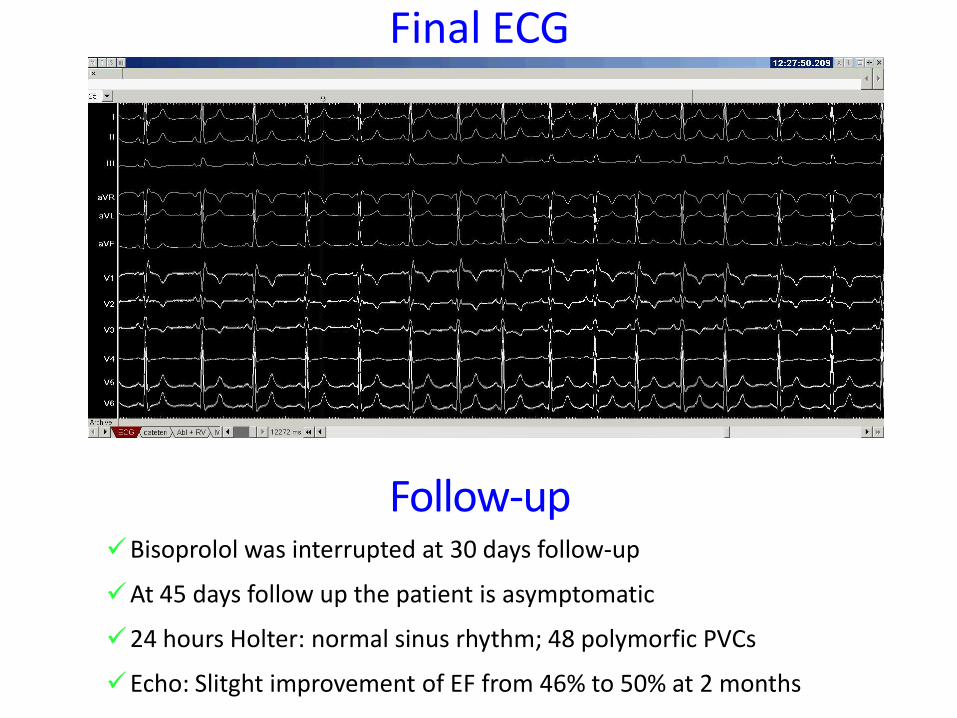
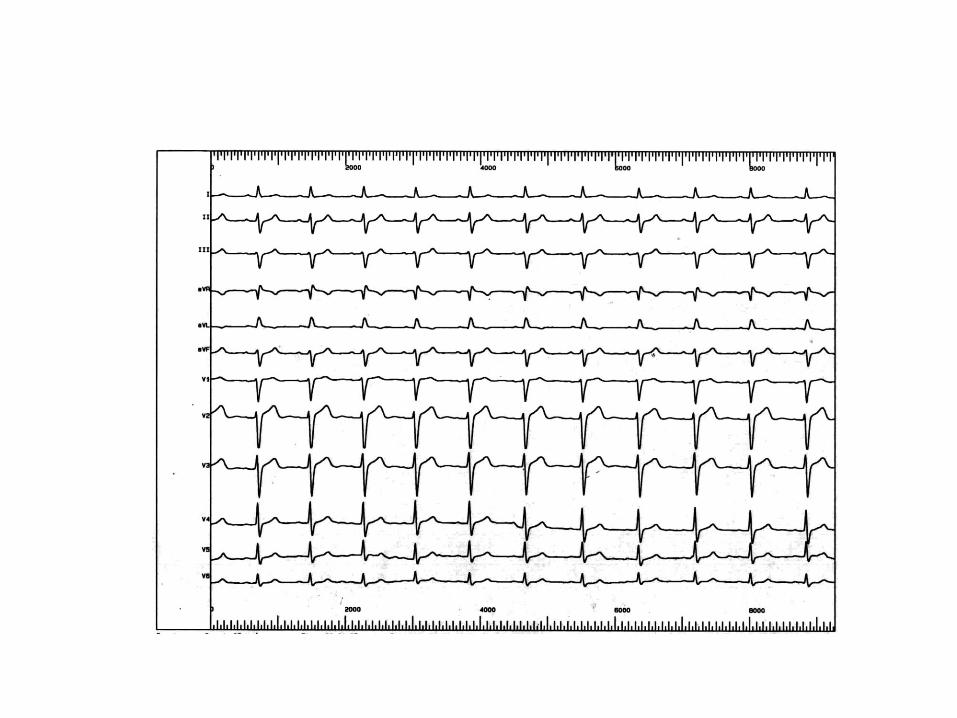
Final ECG
Follow-up Bisoprolol was interrupted at 30 days follow-up
At 45 days follow up the patient is asymptomatic
24 hours Holter: normal sinus rhythm; 48 polymorfic PVCs
Echo: Slitght improvement of EF from 46% to 50% at 2 months
Case 3
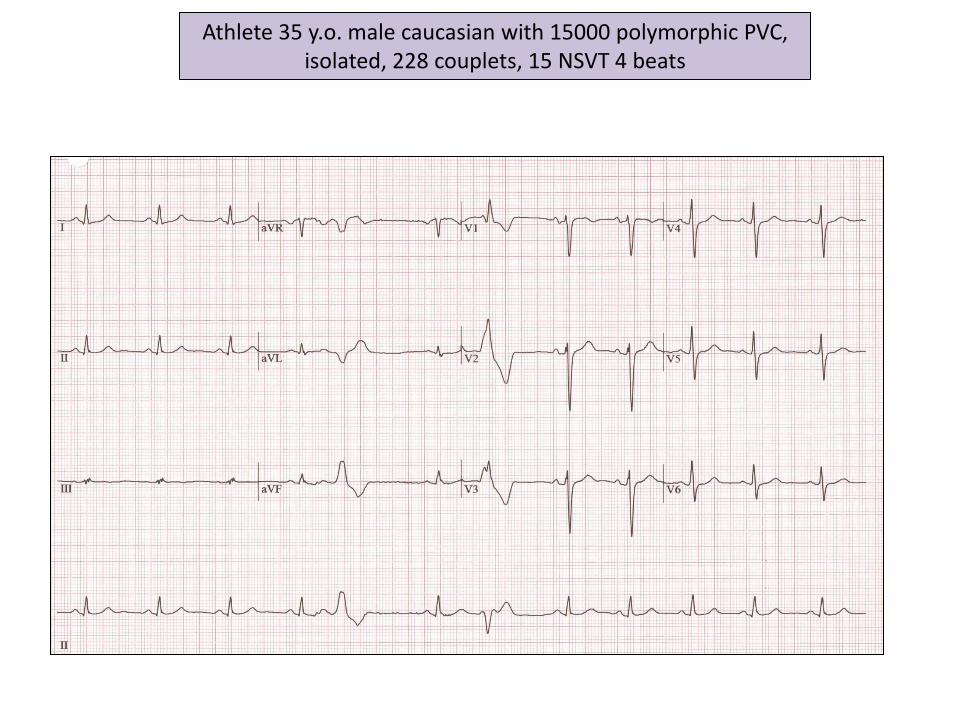
Athlete 35 y.o. male caucasian with 15000 polymorphic PVC, isolated, 228 couplets, 15 NSVT 4 beats
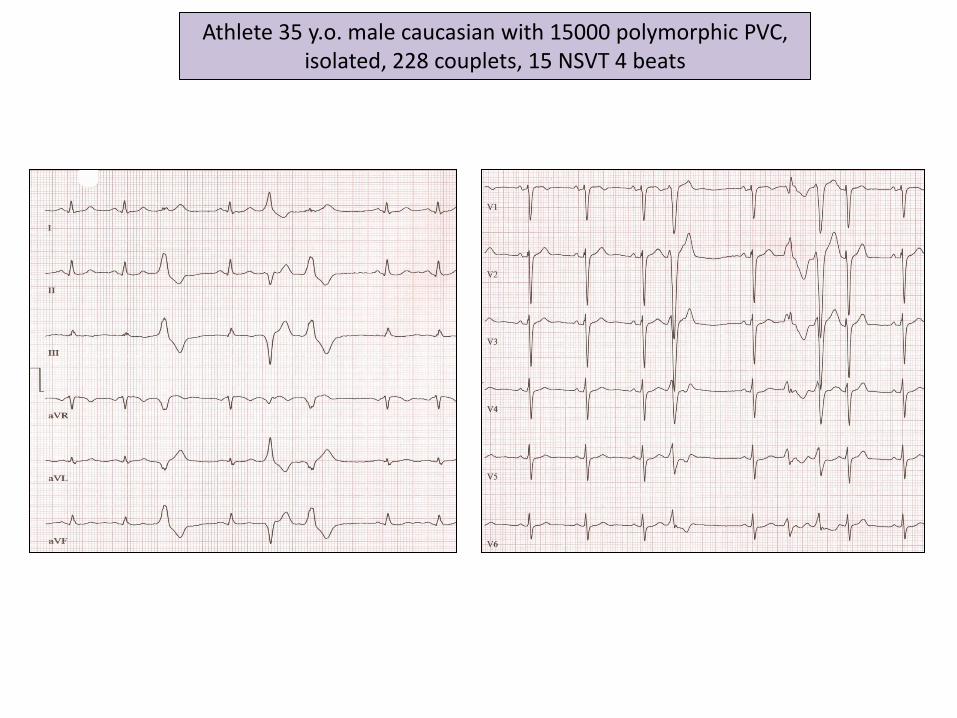
Athlete 35 y.o. male caucasian with 15000 polymorphic PVC, isolated, 228 couplets, 15 NSVT 4 beats
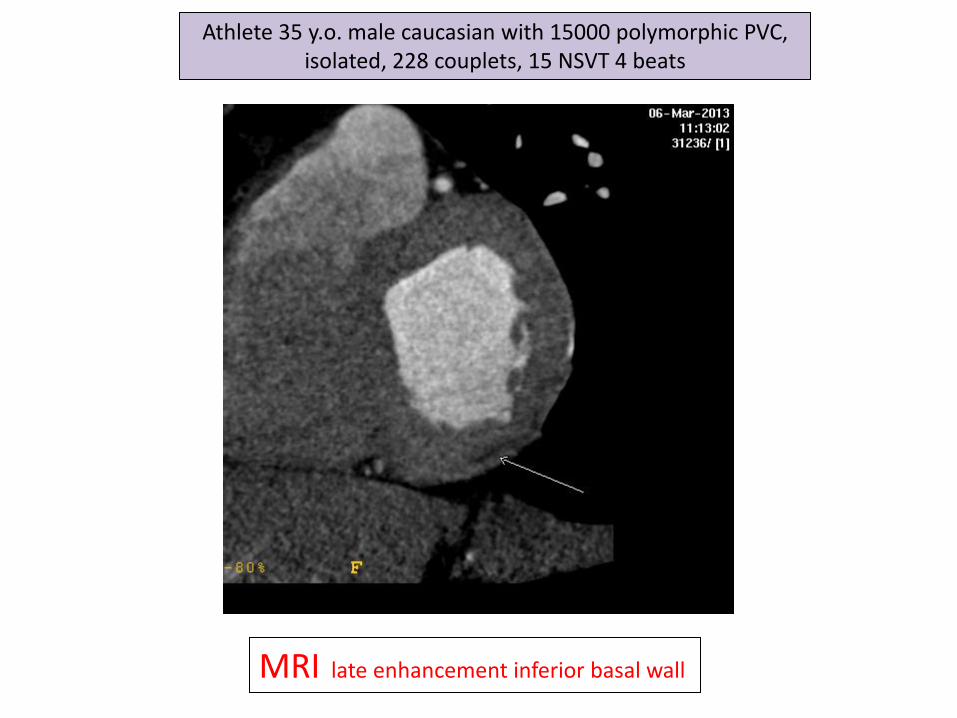
MRI late enhancement inferior basal wall
Athlete 35 y.o. male caucasian with 15000 polymorphic PVC, isolated, 228 couplets, 15 NSVT 4 beats
Case 4
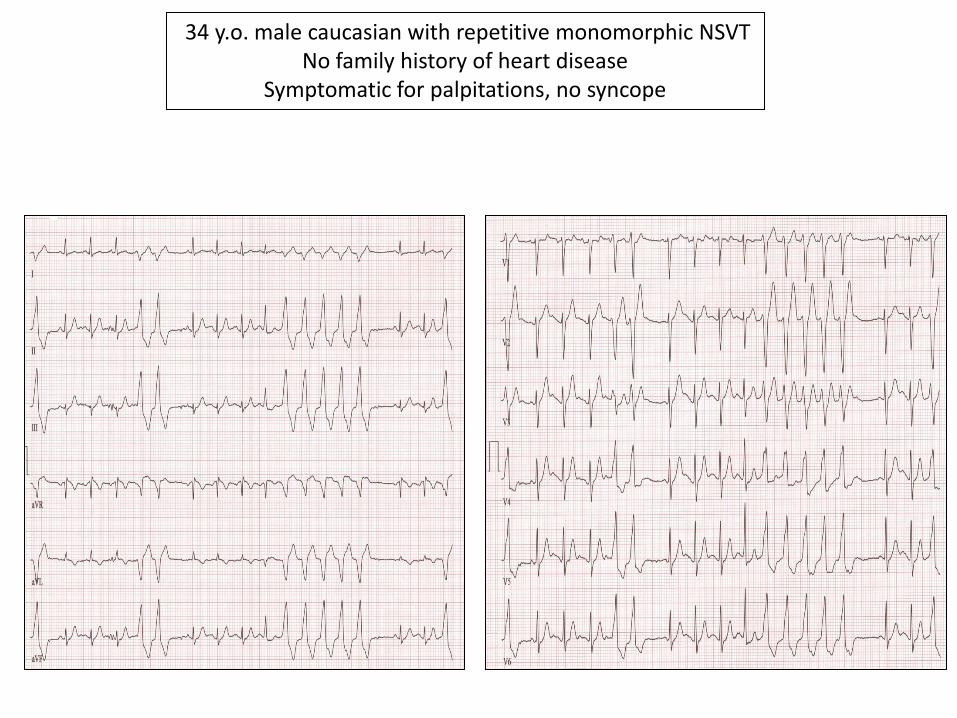
34 y.o. male caucasian with repetitive monomorphic NSVT No family history of heart disease
Symptomatic for palpitations, no syncope
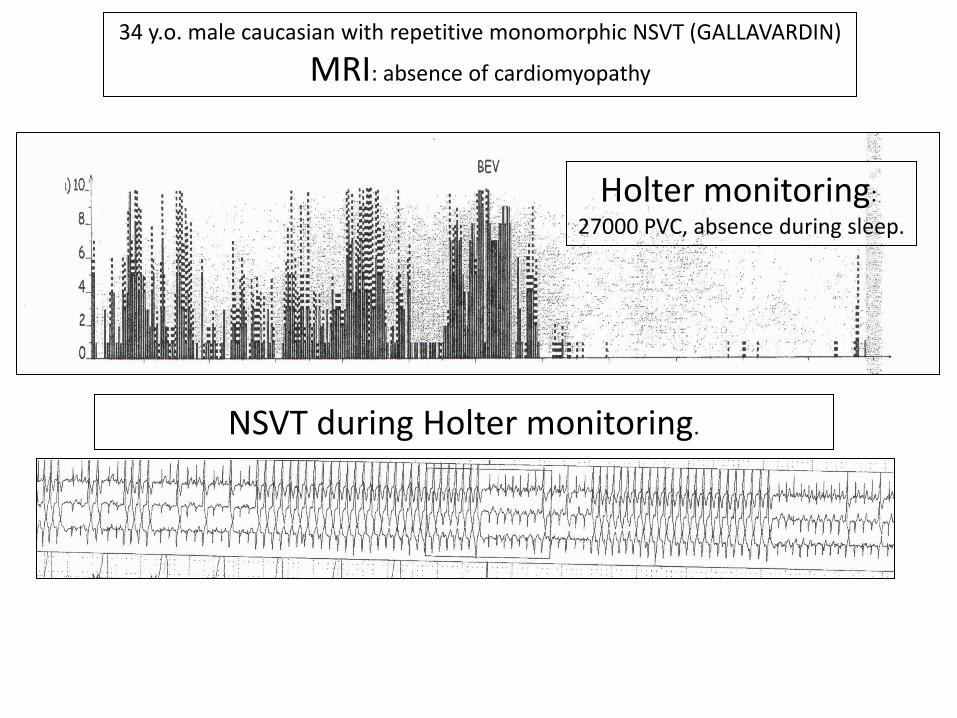
34 y.o. male caucasian with repetitive monomorphic NSVT (GALLAVARDIN)
MRI: absence of cardiomyopathy
Holter monitoring:
27000 PVC, absence during sleep.
NSVT during Holter monitoring.
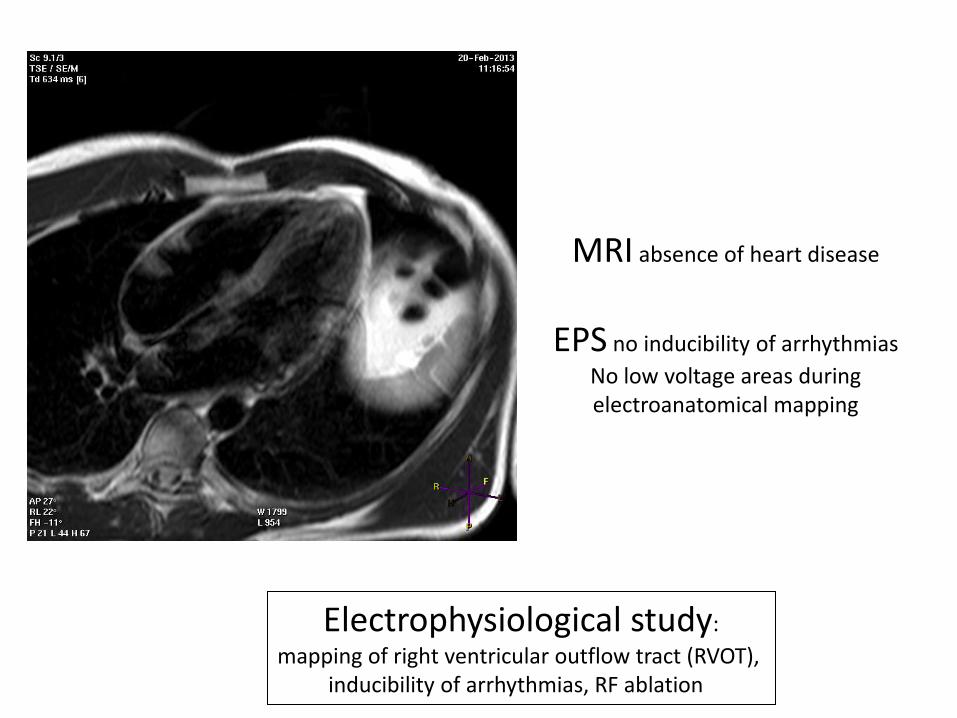
MRI absence of heart disease
EPS no inducibility of arrhythmias
No low voltage areas during electroanatomical mapping
Electrophysiological study:
mapping of right ventricular outflow tract (RVOT), inducibility of arrhythmias, RF ablation
Case 5

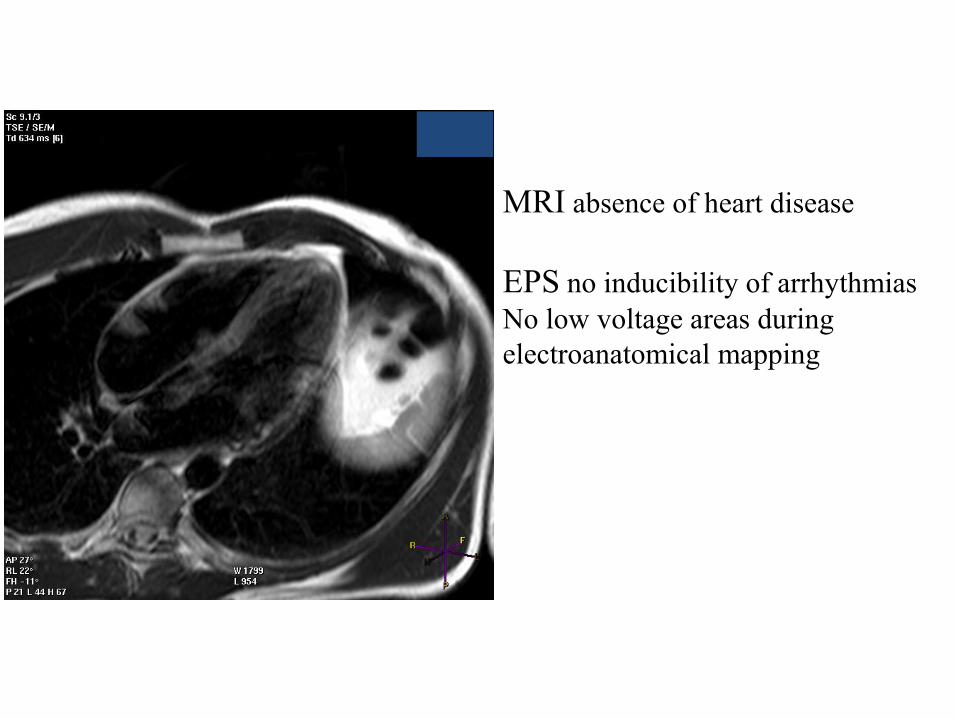
MRI absence of heart disease
EPS no inducibility of arrhythmias
No low voltage areas during
electroanatomical mapping