Embed Size (px)
Citation preview

Hindawi Publishing CorporationNursing Research and PracticeVolume 2011, Article ID 613589, 8 pagesdoi:10.1155/2011/613589
Research Article
Quality of Life in People with Type 2 Diabetes inRelation to Deprivation, Gender, and Age in a NewCommunity-Based Model of Care
Grace Lindsay,1 Kathryn Inverarity,2 and Joan R. S. McDowell3
1 NHS Greater Glasgow and Clyde Acute Division, Nursing, Midwifery and Community Health School, Glasgow Caledonian University,Govan Mbeki Building, Glasgow G4 0BA, UK
2 Golden Jubilee National Hospital, Beardmore Street, Clydebank G81 4HX, UK3 College of Medical, Veterinary and Life Sciences, School of Medicine, Nursing and Health Care, University of Glasgow,57-61 Oakfield Avenue, Glasgow G12 8LW, UK
Correspondence should be addressed to Grace Lindsay, [email protected]
Received 8 December 2010; Revised 22 February 2011; Accepted 14 April 2011
Academic Editor: Barbara Resnick
Copyright © 2011 Grace Lindsay et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objectives. To evaluate changes in health related quality of life (HRQL) for individuals with Type 2 diabetes following theintroduction of a new community-based model of care. Methods. A survey method was used in which HRQL, Problems AreasIn Diabetes (PAID) and demographics were assessed before and 18 months after introducing the new service. Results. OverallHRQL and PAID scores were lower than published levels in individuals with diabetes but remained stable during the transitionto the new model of care except for the bodily pain domain and deteriorating PAID scores for older patients. Four domains ofSF36 health showed deterioration in the highest socio-economic groups. Deterioration was also observed in males, most notablymental health, in patients aged 54 years or less, 75 years or more and patients from socio-economic groups 1 and 2. HRQL waslowest at baseline and follow-up in socio-economic groups 6 & 7. Low levels of distress in patients across all deprivation categorieswas observed but remained stable over the transition. Conclusions. HRQL and distress associated with diabetes remained stablefollowing the introduction of the new community-based model of care except for deterioration in the bodily pain domain anddeteriorating PAID scores for older patients. Relevance for Practice. (i) Health related quality of life assessment is practical andacceptable to patients. (ii) In clinical governance terms it is good practice to monitor the impact of change in service delivery onthe health of the patients in your care. (iii) Screening with health related quality of life tools such as generic and disease specifictools could help identify health problems otherwise undetected within current clinical care. Systematic identification of the mostvulnerable groups with Type 2 diabetes should allow care to be better targeted.
1. Introduction
The increasing incidence of Type 2 diabetes globally is chal-lenging to health care systems. Within the United Kingdom(UK), different models of care are proposed to cope with thischallenge.
In 2003, the Scottish Executive Health Departmentawarded £2.3 million to Greater Glasgow Health Board(GGHB), now defunct but at the time the largest HealthBoard in Scotland, to undertake a service redesign [1]aimed at meeting the requirements of policy documents,providing a service that is more accessible to people with
Type 2 diabetes and consequently reducing morbidity andmortality associated with diabetes. An integrated model ofcare was proposed with general practitioners (GPs) based inprimary care taking the lead role rather than hospital-basedconsultants in secondary care. Patients would be referred tosecondary care based on clinical need.
All members of the multiprofessional primary healthcare team were required to undergo accredited diabeteseducation. General Practices provided information technol-ogy (IT) and data management systems to support anannual review of clinical parameters and management ofdiabetes and risk factors. Additional new posts were created

2 Nursing Research and Practice
Table 1: Comparisons of key differences in approaches between the secondary care focussed model of care to a community model of carefor patients with Type 2 diabetes.
Parameter Previous New model
Setting of diabetes care Hospital based (secondary care) General practitioner surgery (Primary care)
Access to care Mixed community/secondary care Community
Structure IT systemsIT systems to support annual review, recall, andmanagement systems introduced
Care providedAnnual Screening and review of clinicalparameters
Annual screening and review of clinical parametersFollowup appointments for management of clinicalparameters; greater empowerment of self-care
Laboratory results sent onto GP withrecommendations for action
GP receives laboratory results directly and actsaccordingly
Recommendations to GP for change inprescriptions
GP alters prescriptions and initiates necessary therapies
Review by dietitian, podiatrist, and diabetesspecialist nurse at annual review that mayrequire considerable waiting times
Review by dietitian, podiatrist, and practice nurse atannual review as part of a one stop shop so no waitingbetween professionals
Management of diabetes and related riskfactors
Management of diabetes, related risk factors within aholistic context
Referral to specialist services as required forexample, renal physicians
Referral to specialist services as required for example,renal physicians
Educational preparationStaff have significant clinical expertise indiabetes with or without recognisedqualifications
Staff all required to undertake a credit-ratedqualification in diabetes
Retinal screening Secondary care National level directed
in community nursing, dietetics and podiatry to support theservice redesign.
The new model of care was based on the chroniccare model [2]. This model focuses on six evidence-basedareas of practice associated with improved outcomes in themanagement of patients with a chronic disease, namely, thecommunity, the health care system, the design of the deliverysystem, the decision support system, the clinical informationsystems, and self-management support. The chronic caremodel [2] also suggests that informed and motivated patientsin conjunction with prepared proactive teams can producebetter care and improved outcomes [3]. This was a centraltenet of the move to the new model of care. Key differencesbetween the new and previous model are presented inTable 1.
Diabetes and its management can have a considerableimpact on people’s lives [4, 5], for example, feelings of iso-lation, codependency, experience of loss, overuse of defencemechanisms, and loss of freedom, all of which could haveconsequences for the optimal management of the condition.
The literature on the impact of a range of interventionsto improve care for people with diabetes has producedconflicting findings. Some features of diabetes care and itsmanagement regimen have been shown to reduce HRQL[6]. On the other hand, specific improvements in qualityof life have been reported when care was associated withregular clinical review (at least twice a year), continuity ofcare, education by the Diabetes Nurse and satisfaction witheducation [5]. Davies et al. [7] also found positive changeson depression scores, greater understanding of diabetes,
perceived personal responsibility and weight loss following astructured education programme with 12-month followup.However, other authors who have evaluated specific educa-tional interventions found that blood glucose monitoring oreducational courses [8] had no impact on HRQL.
HRQL is increasingly taken into account within healthcare provision as a measure of the effectiveness of care [9].As part of a larger study, it was considered important toinclude not only clinical markers of effective service whichare reported elsewhere [10], but also any potential impact onHRQL.
This study was conducted to evaluate a new model of carefor people with Type 2 diabetes and reports on the generalhealth status and disease-specific health of individuals beforeand after the change in service delivery.
1.1. Aims of This Study. The aim of the study is to assessHRQL for people within a defined geographical area whoare experiencing a change in service delivery for theirdiabetes care management. Patterns of changes in HRQLwere examined in relation to different age groups, gender,and socioeconomic deprivation categories.
2. Materials and Methods
2.1. Study Design. The before and after design of the studyused validated and reliable questionnaires at baseline andfollowup 18 months after the implementation of the new ser-vice [10–13]. Two questionnaires were used as recommended

Nursing Research and Practice 3
in the literature [14]. Ethics permission was acquired fromGGHB Primary Care Research Ethics Committee.
2.1.1. Questionnaires
(a) Demographic Information. Demographic details (age,sex, and postcode) were collected from the health care ITsystem and used to estimate socioeconomic status using anupdated version of the Carstairs deprivation scores [15].The deprivation score is based on vital statistics collectedby UK Government surveys and is a number from 1 to 7calculated from indicators such as lack of car ownership,male unemployment, postcode, and overcrowding, with 1denoting the most affluent and 7 the most socioeconomicallydeprived.
(b) General Health Status. The health experiences of partic-ipants in the four weeks prior to assessment was measuredusing the SF-36 questionnaire [11]. The questionnaire itselfconsists of thirty-six questions measuring eight domains ofhealth, namely, “physical functioning,” “role limitation dueto physical” health problems, “bodily pain,” “general health,”“energy and vitality,” “social functioning,” “mental health,”and “role limitations due to mental” health problems. Eachdomain provides a score from 0 to 100 with zero indicatingthe worst health status and 100 the best. The questionnaireis based on a WHO definition of health, which states thathealth is not only defined by the absence of disease andinfirmity, but also by the presence of physical, mental,and social well-being [16]. The domains themselves weredeveloped in consultation with health professionals ratherthan patients. The scales were scored using a Likert’s methodof summated ratings. Each item was assumed to havea linear relationship with the score for its domain. Theeight scales of the SF-36 questionnaire have been shown tohave high internal consistency (Cronbach Alpha 0.76–0.86).Content validity (the extent to which SF-36 comprehensivelymeasured health status) and criterion validity (the extentto which SF-36 correlated with existing measures of health)were established during this developmental stage. The SF-36health assessment questionnaire has been reported as validand reliable in normal populations as well as diabetes patientgroups [14, 17, 18].
(c) Diabetes Specific Emotional Distress. The problem areasin diabetes (PAID) questionnaire is a reliable and valid toolto determine diabetes specific emotional distress [12, 13, 18].It consists of 20 items measuring emotional adjustment toliving with diabetes. These items are further constructedaround the goals of treatment, family support, worry aboutcomplications, and eating and drinking. Each item is scoredon a 5-point Likert scale according to the degree to which theindividual perceives that it as a problem. Total scores varybetween 0 and 100 with a higher score indicating greateremotional distress associated with diabetes.
2.2. Participants. At the time of the study, the primary carestructure within GGHB was based on 14 local health care
cooperatives (LHCCs), each of which was a functional unitfor the delivery of care in a defined geographical area. Thestudy was conducted within one LHCC with 14 GP practicesand a registered patient population of 63,028 patients ofwhom 1,402 people were diagnosed with Type 2 diabetes.
Every third person on each general practitioner’s (GP)register with Type 2 diabetes was invited to take part inthe study (n = 576). These individuals were sent a lettervia their GP to inform them of the study, the nature ofany participation and a written informed consent sheetgranting permission to access their clinical records pertainingto diabetes care.
Consenting individuals were sent the SF-36 and thePAID questionnaires with instructions for their completiontogether with stamped addressed envelopes for their returnat two time points. The questionnaires were completed in thefirst instance at the commencement of the new community-based model of care (2004) and again 18 months later (2006).
2.2.1. Data Presentation and Analysis. Data are presentedas mean ± standard deviation and median (interquartilerange) for nonparametric distributions. Differences in theoutcome variables were tested by comparison of baselineand follow-up data using χ2 tests for categorical variablesand Students’ t-tests or Mann-Whitney tests for continuousvariables (dependent upon data distribution) using ArcusQuickstat Biomedical software (Addison Wesley Longmantrading as Research Solutions). The sample size allowedsufficient statistical power to detect a 10% change in the SF-36 scores with a confidence level of 90% and a P value of .05.
3. Results
A total of 136 people were recruited to the study. Paired datafor the questionnaire responses at baseline, and followup wasavailable on 65% (n = 88) of the participants.
Demographic details (age, gender, deprivation category,and ethnic origin) of the participants and the populationgroup from which they were selected are presented in Table 2.Proportions (and mean/standard deviation for age) arecalculated for the LHCC Type 2 diabetes population and forthe sample of 136 participants. A Chi-squared test of equalproportions was used to compare our sample against theremaining LHCC patients. Significant differences are shownin bold. There is evidence of a difference in the distributionsof age category, deprivation category, and ethnic originbetween our sample and the rest of the LHCC. Unfortunatelythis means that it is not possible to state that the sample isrepresentative of the full LHCC patient group at the time.
Scores from the SF-36 and the PAID questionnaires arepresented in Tables 3, 4, and 5. Comparisons are made for thewhole group between the SF-36 as applied to other diabeticpatient groups and this sample (Table 3). Thereafter, SF-36and PAID results are presented by gender, age categories andby deprivation category (Tables 4 and 5).
3.1. SF-36 General Trends. Overall, the general health of thestudy group was similar to that of other published results on

4 Nursing Research and Practice
Table 2: Comparison of patient demographic details between the research sample and the local health cooperative (LHCC) population ofpatients with Type 2 diabetes∗.
Patient numbers with Type 2diabetes in the LHCC and theresearch sample
Total patient population in theLHCC with Type 2 diabetes
Research sampleLHCC patient population withType 2 diabetes (excludingresearch sample)
P-value
Total Number 1402 136 1266 —
Gender .10
Female 662 (47%) 55 (40%) 607 (48%)
Male 740 (53%) 81 (60%) 659 (52%)
Mean age (SD dev) in years 63.76 (13.59) 65.38 (11.96) 63.57 (13.75) .08
Age Category .003
<55 yrs 346 (25%) 28 (21%) 318 (25%)
55–64 yrs 324 (23%) 23 (17%) 303 (24%)
65–74 yrs 415 (30%) 56 (41%) 357 (28%)
>74 yrs 317 (23%) 29 (21%) 288 (23%)
Deprivation category .007
1 38 (3%) 3 (2%) 35 (3%)
2 260 (19%) 27 (20%) 233 (18%)
3 160 (11%) 26 (19%) 134 (11%)
4 252 (18%) 32 (24%) 220 (17%)
5 85 (6%) 8 (6%) 77 (6%)
6 187 (13%) 11 (8%) 176 (14%)
7 420 (30%) 29 (21%) 391 (31%)
Grouped dep cat .001
1 and 2 268 (21%) 30 (22%) 268 (21%)
3, 4 & 5 431 (34%) 66 (49%) 431 (34%)
6 & 7 567 (45%) 40 (29%) 567 (45%)
Ethnic origin <.001
Asian 254 (18%) 8 (6%) 246 (19%)
Other 1148 (82%) 128 (94%) 1020 (81%)∗
Chi Squared statistics were used to compare differenced in frequencies.
larger samples but tended towards reduced levels at followup.There was no evidence of “floor” or “ceiling” effects; that is,the scaling was sensitive at the extremes of the scales andcould detect changes in states of very poor health and verygood health. The “physical function,” “bodily pain,” “rolelimitation physical,” “role limitation mental,” and “socialfunction” scores were all better than other published resultsfor people with diabetes at the beginning of the change inservice delivery, but there was a lowering of these scoresover the course of the study. Scores in “general health,”“energy/vitality,” and “mental health” commenced at a lowerlevel and remained lower (Table 3). However, scores for thewhole group showed no statistically significant change at theP < .05 level after implementation of the new model of care,except in the “bodily pain” domain (P = .02).
There were no differences between genders with theexception of a deteriorating mental health score for males.The oldest group showed more deterioration in SF-36scores across “physical function,” “role limitation due tophysical function,” “energy and vitality,” and “bodily pain”(4 domains), whereas the youngest group showed more
deterioration in “role limitation due to physical function,”“social function,” and “general health” (3 domains). Therewas also a statistically significant deterioration in “physicalfunction,” “role limitation due to physical function,” “energyand vitality,” “bodily pain,” and “general health” (5 domains)for people in the highest socioeconomic groups (dep cat 1& 2) with the scores for those in the other socioeconomicgroups remaining stable (Table 4). HRQL was lower for allgroups at baseline in socioeconomic groups 6 & 7 andremained so at follow-up assessment.
The middle years of 55–74 appear to be the mostsettled with no extremes in results. There was no evidenceof improvement in SF-36 health domains. Any statisticallysignificant changes across the whole group or within thepatient subgroups examined were deterioration in healthstatus.
3.2. PAID Scores. The results from this questionnaire weresimilar both before and after the implementation of thenew community-based model of care (Figure 1). Scoresindicated that there was sensitivity to different levels of

Nursing Research and Practice 5
Table 3: Health-related quality of life scores: SF-36 by whole group and by gender before and 18 months after introduction of the newcommunity model of care for people with Type 2 diabetes compared with other diabetic population groups (12).
SF-36 domains SF 36 scores (9) Whole group Males Females
n 541 88 52 36
Baseline/followup B F B F B F
Physical function 67.775 versus 70 75 versus 78 73 versus 63
P = .10 P = .24 P = .25
Role limitation physical 56.875 versus 50 100 versus 75 50 versus 25
P = .08 P = .20 P = .24
Role limitation mental 75.688 versus 100 100 versus 100 67 versus 100
P = .86 P = .82 P = .60
Social function 82.089 versus 78 89 versus 78 78 versus 78
P = .07 P = .08 P = .48
Mental health 76.872 versus 70 75.4 versus 71.2 66.1 versus 67.7
P = .18 P = .02 P = .46
Energy/vitality 55.751 versus 49 54.1 versus 49.9 47.5 versus 47.4
P = .21 P = .09 P = .97
Bodily pain 68.570 versus 63.9 72.5 versus 67.4 67.3 versus 59.0
P = .02 P = .12 P = .08
General health 56.154.8 versus 51.7 55.8 versus 51.1 53.4 versus 52.6
P = 0.13 P = .09 P = .80
Table 4: Health-related quality of life scores: SF-36 before and 18 months after introduction of the new community model of care for peoplewith Type 2 diabetes by age groupings and deprivation category. Statistical comparisons of baseline and follow-up data, when these data arenot normally distributed, are based on the Mann-Whitney-Wilcoxon rank test.
SF-36 domains Age <55 yearsAge 55–64
yearsAge 65–74
yearsAge >74 years Dep cat 1&2
Dep cat 3,4 & 5
Dep cat 6 & 7
n 15 17 39 17 24 41 23
Baseline/followup B F B F B F B F B F B F B F
Physical function75 versus 80
(55–100)75 versus 80
(43–90)75 versus 70
(50–90)65 versus 45
(45–78)75 versus 75 75 versus 75 50 versus 45
P = .06 P = .19 P = .40 P < .001 P = .04 P = .23 P = .64
Role limitation physical100 versus 50
(0–100)100 versus 100
(13–100)50 versus 50
(0–100)50 versus 0(13–100)
100 versus 50 100 versus 100 25 versus 0
P = .045 P = .29 P = .51 P = .013 P = .01 P = .92 P = .57
Role limitation mental100 versus 33
(0– 100)100 versus 100
(46–100)67 versus 100
(33–100)100 versus 67
(17–100)100 versus 100 75 versus 100 57 versus 33
P = .57 P = .46 P = .81 P = .52 P = .80 P = .25 P = .22
Social function89 versus 67
(33–100)89 versus 78
(56–100)89 versus 89
(67–100)78 versus 67
(62–95)100 versus 89 89 versus 89 67 versus 56
P = .006 P = .54 P = .71 P = .10 P = .06 P = .88 P = .11
Mental health59.5 versus
56.366.8 versus
67.575.3 versus
73.678.6 versus
74.881.0 versus
77.570.7 versus
70.663.3 versus
60.0
P = .41 P = .71 P = .47 P = .13 P = .06 P = .96 P = .35
Energy/vitality41.7 versus
41.352.4 versus
52.452.1 versus
51.257.7 versus
46.862.7 versus
54.451.1 versus
50.240.2 versus
40.7
P = .92 P = 1.00 P = .73 P = .04 P = .02 P = .74 P = .93
Bodily pain68.3 versus
57.966.1 versus
68.170.4 versus
65.376.5 versus 62
79.3 versus67.6
70.5 versus67.3
60.9 versus54.2
P = .19 P = .74 P = .18 P = .03 P = .03 P = .35 P = .30
General health50.3 versus
41.452.3 versus
55.856.7 versus
54.056.8 versus
51.564.1 versus
55.155.6 versus
53.643.6 versus
44.7
P < .001 P = .48 P = .46 P = .13 P = .02 P = .40 P = .83

6 Nursing Research and Practice
Table 5: Health-related quality of life scores: PAID questionnaires before and 18 months after introduction of community model of care forpeople with Type 2 diabetes.
DomainWholegroup
Males FemalesAge <55
yearsAge 55–64
yearsAge 65–74
yearsAge >74
yearsDep cat 1 &
2Dep cat 3,
4 & 5Dep cat 6 &
7
n 88 52 36 15 17 39 17 24 41 23
Baseline/followup
B F B F B F B F B F B F B F B F B F B F
PAID13 versus
1312 versus
1313 versus
1325 versus
2316 versus
1310 versus
116 versus 9 9 versus 9
13 versus14
14 versus13
P = .14 P = .17 P = .55 P = .86 P = .39 P = .045 P = .02 P = .11 P = .44 P = .54
∗∗∗
25
20
15
10
5
0
Baseline
PAD
scor
e
(Age)
Followup
<55 >7456–65 66–74
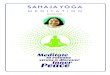
Figure 1: Baseline PAID score and follow-up PAID score versusage. ∗statistically significant difference with P = .045. ∗∗statisticallysignificant difference with P = .020.
distress associated with diabetes and were slightly lowerthan other published data for people with diabetes [13,18] in respect of lower and unchanged levels of distressfollowing the introduction of the new community-basedservice. However, scores were generally low (less distress),but were relatively higher in younger participants (Table 5)and exhibited statistically significant deterioration in patientsaged 65 years or more (Figure 1).
4. Discussion
In the study group, no major differences were observed inthe pattern of HRQL and PAID scores both by comparisonwith other published assessment [11] or over the timeframeof the introduction of the new service except in respectof a deterioration in the “bodily pain” domain of SF-36which was due to other conditions unrelated to diabetes.However, a tendency towards lowering of health status overthe period of the study (see results section) emerged. Dataon the presence of other medical conditions was noted inparticipants’ accounts of their health, for example, presenceof arthritis, but this was not confirmed by checking medicalrecords.
An earlier study [19] showed no gender differences withthe PAID questionnaire. This is further supported in thepresent study using the PAID and SF-36 questionnaires
with the only exception being in respect of mental healthfor males. However, mental health scores were higher atbaseline for male participants and higher than womenoverall. Nevertheless, the statistically significant result is thatthe mental health of males deteriorated during the period ofthe study, whereas that of females was stable.
This result contrasts with other work examining depres-sion and diabetes which found no differences in levelsof depression between men and women living with thecondition [20]. This effect was observed only with the totalgroup and was not obvious in analyses by age group ordeprivation category. This was a surprise finding. Men areknown to be less proactive than women in accessing healthcare facilities; nevertheless, there is no obvious reason whythere should be such a deterioration in their mental healthover this 18-month period.
A meta-analyses of studies examining links betweendepression in diabetes demonstrated a relationship withhyperglycaemia [21] and with an increased risk for com-plications [22]. People at elevated risk for depression canbe identified through the medical history and clinicalpresentation and by asking depression-specific questionsor through the use of depression screening tools. Peoplewith a history of depression, anxiety disorder, mental healthtreatment, substance abuse, or smoking are at heightenedrisk for depression, as are women and those with a familyhistory of depression or mental health treatment. People whohave multiple complications are more likely to be depressed,especially when those complications include neuropathy,impotence, or cardiovascular disease [22].
The older age group (>74years) experienced a greaterdeterioration in health scores than younger groups. This mayreflect a group of people who are living with increased frailtygenerally but appear to have less psychosocial related healthissues. By contrast, the youngest age group (<55years) hadvarious deteriorations in health scores and, moreover, hadthe lowest, energy, and vitality scores for all age groups. Apotential explanation for this observation is that people atthis stage of life have many competing demands on time, forexample, employment, commitments to children, and ageingparents although the study provides no supporting evidence.
Interestingly, the deterioration in health status as mea-sured by the SF 36 questionnaire was statistically significantin deprivation categories 1 & 2 for various domains (Table 4).It is not clear why scores in this group decreased but the

Nursing Research and Practice 7
outcome are scores that are similar to participants fromdeprivation categories 3, 4, and 5. By implication this placesthis group of people at higher risk of increased mortality andmorbidity associated with increased levels of socioeconomicdeprivation. It would appear that those in deprivationcategories 1 & 2 are experiencing HRQL issues as if they livedin a lower deprivation category. This was a surprise finding,implying that the more articulate, educated people are justas much in need of support as those from a more deprivedbackground.
It has been reported in the literature that diabetes dis-proportionately affects socially and materially disadvantagedindividuals [23]. Higher levels of retinopathy, heart disease,and HbA1c and less health checks for the quality indicatorsof diabetes care have been reported leading to increasedmortality and morbidity [24]. Our findings are similar inthat we found the lowest levels of health scores in participantsfrom the areas of highest socioeconomic deprivation. Forparticipants from deprivation categories 3, 4, 5, and 6 & 7there was a general deterioration in scores, but the trendwas not statistically significant. This pattern of HRQL changediffers from reports examining the impact of a range ofinterventions including diabetes education and behaviouralmodification (15 studies), pharmacotherapy (11 studies),and surgery (7 studies) in that these interventions generallydemonstrated improvement in HRQL although the magni-tude of effect varied [25]. Our evaluation is different in therespect that it assesses differences in two models of routineclinical care and as such the fundamental principles of caremay not be radically changed compared with the testing ofan additional focussed intervention. Recommendations havebeen made to develop further focussed strategies aimed atreducing inequalities of health outcomes for people withdiabetes from areas of socioeconomic disadvantage [24].
It is interesting to note that PAID scores were at thelower level of distress severity compared with the genericSF-36 health domains where some domains were less than50% of the possible optimal score. The statistically significantdeterioration in scores in the older-age groups (Figure 1)could be related to the fact that these people had livedwith the condition for a longer period of time and maybe experiencing some of the wider pathological effects ofdiabetes. Alternatively, people newly diagnosed with diabetesin that age group may find the impact of diabetes greater thanyounger people. This conclusion, however, must be treatedwith caution, as it is based on the difference between just oneindividual.
A review of assessment and measurement of quality oflife in people with Type 2 diabetes [26] acknowledged thatthere are many other variables that impact on quality of life,for example, demographics, comorbidities and psychosocialfactors. The effect of daily ongoing monitoring of diet,exercise, medication management, and glucose monitoringto achieve as closely as possible a nondiabetic metabolic statewas recognized as having a major impact on peoples’ lives.New models of service delivery, such as that described here,can best support care management and are likely to improveHRQL.
Using both the SF-36 and PAID questionnaires allowsinsight into the impact of diabetes to health alone and aholistic assessment of overall health status. These question-naires provide appropriate tools to evaluate a service thatis moving from a specialist model to enhanced generalistcommunity-based model of care, the latter being noted byparticipants to be important to them [27]. Because thegeneral health scores were disproportionately lower than thedisease-specific scores, it could be argued that a general,holistic health care context is more fitting for these patient’shealth care needs.
5. Conclusions
In the group studied, HRQL and distress associated withdiabetes remained stable following the introduction of achange in the delivery of care from a hospital-based setting toa community model of care. The only statistically significantdeterioration in HRQL was in bodily pain and was identifiedas due to other health conditions and unrelated to diabetes.
Although it is recognised that many factors impact onHRQL it is noteworthy that for particular age groups, peoplefrom socioeconomic groups 1 & 2 and males had significantdeterioration in certain domains of their HRQL. The reasonsfor these findings are beyond the scope of this study but willform the basis for further investigation. In agreement withthe literature, it was noted that HRQL was lowest at baselinein socioeconomic groups 6 & 7 and remained so at follow-upassessment.
The study confirms the value of measuring HRQLfor people with diabetes, living with a chronic long-termcondition, to identify changes in status as a mechanismfor understanding wider health issues and developing indi-vidualised strategies to improve care. The HRQL measureshave been shown to identify subgroups of people whosehealth may be particularly affected by the impact of diabetesmellitus. Assessment of HRQL could be integrated intoannual review assessments.
Acknowledgments
The authors wish to acknowledge Dr. Malcolm Brown andGraham Bowman. This study was commissioned and fundedby Shawlands Local Health Care Cooperative, Glasgow,Scotland.
References
[1] Scottish Executive, Scottish Diabetes Framework, Scottish Exec-utive, Edinburgh, UK, 2001.
[2] E. Wagner, E. A. Coleman, T. B. Eilertsen et al., “What willit take to improve care for chronic illness?” Effective ClinicalPractice, vol. 4, no. 2, pp. 2–4, 2001.
[3] M. L. Parchman, J. A. Pugh, C. P. Wang, and R. L. Romero,“Glucose control, self-care behaviours, and the presence of thechronic care model in primary care clinics,” Diabetes Care, vol.30, pp. 2849–2854, 2007.

8 Nursing Research and Practice
[4] (SIGN) Scottish Intercollegiate Guideline Network, SIGNGuideline, vol. 116, Management of Diabetes SIGN, Edin-burgh, UK, 2010.
[5] J. Hanninen, J. Takala, and S. Keinanen-Kiukaanniemi, “Goodcontinuity of care may improve quality of life in Type 2diabetes,” Diabetes Research and Clinical Practice, vol. 51, no.1, pp. 21–27, 2001.
[6] R. R. Rubin and M. Peyrot, “Quality of life and diabetes,”Diabetes/Metabolism Research and Reviews, vol. 15, no. 3, pp.205–218, 1999.
[7] M. J. Davies, S. Heller, T. C. Skinner et al., “On behalf of theDiabetes Education and Self Management for ongoing andNewly Diagnosed Collaborative Effectiveness of the diabeteseducation and self management for ongoing and newlydiagnosed (DESMOND) programme for people with newlydiagnosed type 2 diabetes: cluster randomised controlledtrial,” British Medical Journal, vol. 336, pp. 491–495, 2008.
[8] T. A. Deakin, J. E. Cade, R. Williams, and D. C. Green-wood, “Structured patient education: the Diabetes X-PERTProgramme makes a difference,” Diabetic Medicine, vol. 23, no.9, pp. 944–954, 2006.
[9] C. D. Jenkins, R. T. Jono, B. A. Stanton, and C. A. Stroup-Benham, “The measurement of health-related quality of life:major dimensions identified by factor analysis,” Journal ofSocial Science and Medicine, vol. 31, no. 8, pp. 925–931, 1990.
[10] G. Lindsay, J. McDowell, and K. McPhail, An Evaluation ofthe Impact of the Glasgow Diabetes Project for Healthcare forPatients with Type 2 Diabetes, University of Glasgow Press,2006.
[11] J. E. Ware, K. K. Snow, A. S. Kosinski, and B. Gandek, SF-36:Health Survey Manual and Interpretation Guide, Nimrod Press,Boston, Mass, USA, 1993.
[12] G. W. Welch, A. M. Jacobson, and W. H. Polonsky, “Theproblem areas in diabetes scale: An evaluation of its clinicalutility,” Diabetes Care, vol. 20, no. 5, pp. 760–767, 1997.
[13] G. Welch, K. Weinger, B. Anderson, and W. H. Polonsky,“Responsiveness of the problem areas in diabetes question-naire,” Diabetic Medicine, vol. 20, no. 1, pp. 69–72, 2003.
[14] A. M. Jacobson, M. De Groot, and J. A. Samson, “Theevaluation of two measures of quality of life in patients withtype I and type II diabetes,” Diabetes Care, vol. 17, no. 4, pp.267–274, 1994.
[15] P. McLoone, Carstairs Scores for Scottish Postcode Sectors fromthe 1991 & 2001 Census, MRC Social & Public Health ResearchUnit, University of Glasgow, Scotland, UK, 2004.
[16] Constitution of the World Health Organisation, Handbookof Basic Documents, World Health Organisation, Palais desNations, Geneva, Switzerland, 5th edition, 1952.
[17] C. Jenkinson, A. Coulter, and L. Wright, “Short form 36 (SF36) health survey questionnaire: Normative data for adults ofworking age,” British Medical Journal, vol. 306, no. 6890, pp.1437–1440, 1993.
[18] W. H. Polonsky, B. J. Anderson, P. A. Lohrer et al., “Assessmentof diabetes-related distress,” Diabetes Care, vol. 18, no. 6, pp.754–760, 1995.
[19] C. West and J. McDowell, “Diabetes related distress in type 2diabetes,” British Journal of Community Nursing, vol. 7, no. 12,pp. 606–613, 2002.
[20] A. Engum, A. Mykletun, K. Midthjell, A. Holen, and A. Dahl,“Depression and diabetes: a large population-based studyof sociodemographic, lifestyle, and clinical factors associated
with depression in type 1 and type 2 diabetes,” Diabetes Care,vol. 28, no. 8, pp. 1904–1909, 2005.
[21] M. De Groot, R. Anderson, K. E. Freedland, R. E. Clouse,and P. J. Lustman, “Association of depression and diabetescomplications: a meta-analysis,” Psychosomatic Medicine, vol.63, no. 4, pp. 619–630, 2001.
[22] P. J. Lustman, L. S. Griffith, R. E. Clouse et al., “Effectsof nortiptyline on depression and glucose regulation indiabetes: results of a double-blind, placebo-controlled trial,”Psychosomatic Medicine, vol. 59, pp. 241–250, 1997.
[23] A. F. Brown, S. L. Ettner, J. Piette et al., “Socioeconomicposition and health among persons with diabetes mellitus: aconceptual framework and review of the literature,” Epidemi-ologic Reviews, vol. 26, pp. 63–77, 2004.
[24] X. Zhang, S. L. Norris, F. M. Chowdhury, E. W. Gregg, and P.Zhang, “The effects of interventions on health-related qualityof life among persons with diabetes: a systematic review,”Medical Care, vol. 45, no. 9, pp. 820–834, 2007.
[25] A report by the All Parliamentary Group for Diabetes andDiabetes UK, “Diabetes and the disadvantaged: reducinghealth inequalities in the UK,” World Diabetes Day, 2006.
[26] R. R. Rubin and M. Peyrot, “Quality of life and diabetes,”Diabetes/Metabolism Research and Reviews, vol. 15, no. 3, pp.205–218, 1999.
[27] J. R. S. McDowell, K. McPhail, G. Halyburton, M. Brown, andG. Lindsay, “Perceptions of service redesign by adults livingwith type 2 diabetes,” Journal of Advanced Nursing, vol. 65, no.7, pp. 1432–1441, 2009.

Submit your manuscripts athttp://www.hindawi.com
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Breast CancerInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
HematologyAdvances in
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
ScientificaHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PediatricsInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Advances in
Urology
HepatologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
InflammationInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgery Research and Practice
Current Gerontology& Geriatrics Research
Hindawi Publishing Corporationhttp://www.hindawi.com
Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
NursingResearch and Practice
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
HypertensionInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Prostate CancerHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Surgical OncologyInternational Journal of























![Short circuit followup[1]](https://img.pdfslide.us/doc/110x75/556264fad8b42ae87d8b4ffa/short-circuit-followup1.jpg)