Embed Size (px)
Citation preview
Plus & Materials Only Plans
G R O U P S 2 +
Vision CareQuality
for Groups Big and Small

Offer your group clients a fully insured vision plan that provides one of the greatest valuesin the vision care industry. Employees receive complete vision care coverage for apremium that is very affordable.
Groups have the option of selecting a complete vision solution that provides coverage forexams and optical materials; or opt for a plan design which only covers frames andlenses, or contact lenses for each plan period.
The Avesis Vision Plan offer a generous vision carebenefit for your employee groups and their dependents.Members receive the greatest value if they receiveservices from in-network providers.
Avesis Vision Groups
Covered employees have the option of utilizing anational network of over 30,000 providers. Membersmay choose between independent optometrists andophthalmologists as well as national and regional retailvision centers.
An Expansive Provider Network
You can offer the Avesis Vision Plan with a lowparticipation requirement of only 2 enrolled employees.There are no pre-existing exclusions, and rates areguaranteed up to 24 months.
Simple Underwriting
Groups can take advantage of forefront advancements in online plan administration andindividual benefit research. Plan administrators have tools which simplify the billing andenrollment process. Additionally, members have access to important plan informationsuch as provider data, eligibility dates, and more.
Technology
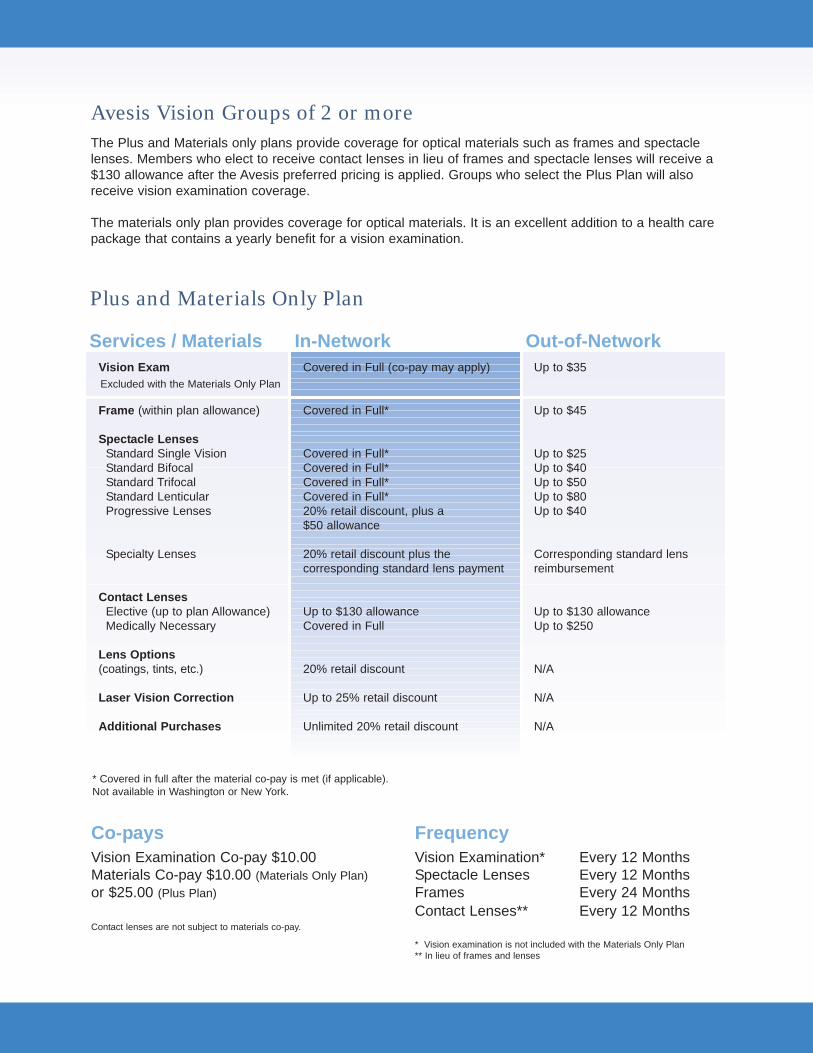
The Plus and Materials only plans provide coverage for optical materials such as frames and spectaclelenses. Members who elect to receive contact lenses in lieu of frames and spectacle lenses will receive a$130 allowance after the Avesis preferred pricing is applied. Groups who select the Plus Plan will alsoreceive vision examination coverage.
The materials only plan provides coverage for optical materials. It is an excellent addition to a health carepackage that contains a yearly benefit for a vision examination.
Vision Exam
Frame (within plan allowance)
Spectacle LensesStandard Single VisionStandard BifocalStandard TrifocalStandard LenticularProgressive Lenses
Specialty Lenses
Contact LensesElective (up to plan Allowance)Medically Necessary
Lens Options(coatings, tints, etc.)
Laser Vision Correction
Additional Purchases
Covered in Full (co-pay may apply)
Covered in Full*
Covered in Full*Covered in Full*Covered in Full*Covered in Full*20% retail discount, plus a $50 allowance
20% retail discount plus thecorresponding standard lens payment
Up to $130 allowanceCovered in Full
20% retail discount
Up to 25% retail discount
Unlimited 20% retail discount
Up to $35
Up to $45
Up to $25Up to $40Up to $50Up to $80Up to $40
Corresponding standard lensreimbursement
Up to $130 allowanceUp to $250
N/A
N/A
N/A
In-NetworkServices / Materials
Co-pays Frequency
Avesis Vision Groups of 2 or more
Out-of-Network
* Covered in full after the material co-pay is met (if applicable).Not available in Washington or New York.
Excluded with the Materials Only Plan
Vision Examination* Every 12 MonthsSpectacle Lenses Every 12 MonthsFrames Every 24 MonthsContact Lenses** Every 12 Months
* Vision examination is not included with the Materials Only Plan** In lieu of frames and lenses
Vision Examination Co-pay $10.00Materials Co-pay $10.00 (Materials Only Plan)or $25.00 (Plus Plan)
Contact lenses are not subject to materials co-pay.
Plus and Materials Only Plan
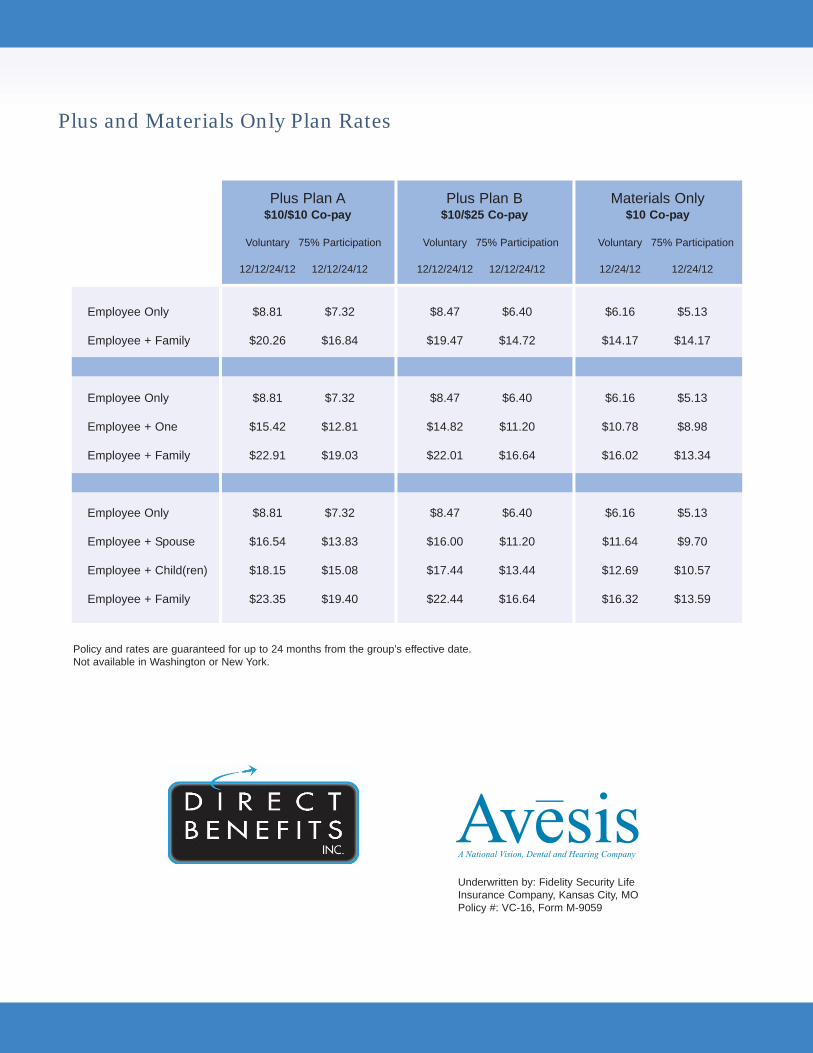
Underwritten by: Fidelity Security LifeInsurance Company, Kansas City, MOPolicy #: VC-16, Form M-9059
Voluntary 75% Participation Voluntary 75% Participation Voluntary 75% Participation
12/12/24/12 12/12/24/12 12/12/24/12 12/12/24/12 12/24/12 12/24/12
Employee Only $8.81 $7.32 $8.47 $6.40 $6.16 $5.13
Employee + Family $20.26 $16.84 $19.47 $14.72 $14.17 $14.17
Employee Only $8.81 $7.32 $8.47 $6.40 $6.16 $5.13
Employee + One $15.42 $12.81 $14.82 $11.20 $10.78 $8.98
Employee + Family $22.91 $19.03 $22.01 $16.64 $16.02 $13.34
Employee Only $8.81 $7.32 $8.47 $6.40 $6.16 $5.13
Employee + Spouse $16.54 $13.83 $16.00 $11.20 $11.64 $9.70
Employee + Child(ren) $18.15 $15.08 $17.44 $13.44 $12.69 $10.57
Employee + Family $23.35 $19.40 $22.44 $16.64 $16.32 $13.59
Plus Plan A$10/$10 Co-pay
Plus Plan B$10/$25 Co-pay
Materials Only$10 Co-pay
Policy and rates are guaranteed for up to 24 months from the group’s effective date.Not available in Washington or New York.
Plus and Materials Only Plan Rates
Limitations: This plan is designed to cover eye examinations and corrective eyewear. It is alsodesigned to cover visual needs rather than cosmetic options. Should the member select options thatare not covered under the plan, as shown in the schedule of benefits, the member will pay adiscounted fee to the participating Avesis provider. Benefits are payable only for services receivedwhile the group and individual member’s coverage is in force.
Exclusions: There are no benefits under the plan for professional services or materials connectedwith and arising from: 1) Orthoptics of vision training; 2) Subnormal vision aids and any supplementaltesting; 3) Plano (non-prescription) lenses, sunglasses; 4) Two pair of glasses in lieu of bifocal lenses;5) Any medical or surgical treatment of eye or support structures; 6) Replacement of lost or brokenlenses, contact lenses or frames, except when the member is normally eligible for services; 7) Any eyeexamination or corrective eyewear required by an employer as a condition of employment; 8) Servicesor materials provided as a result of Workers Compensation Law, or similar legislation, required by anygovernmental agency whether Federal, State or subdivision thereof.
Limitations: This plan is designed to cover corrective eyewear. It is also designed to cover visualneeds rather than cosmetic options. Should the member select options that are not covered under theplan, as shown in the schedule of benefits, the member will pay a discounted fee to the participatingAvesis provider. Benefits are payable only for expenses incurred while the group and individualmember’s coverage is in force.
Exclusions: There are no benefits under the plan for professional services or materials connectedwith and arising from: 1) Orthoptics of vision training; 2) Subnormal vision aids and any supplementaltesting; 3) Plano (non-prescription) lenses, sunglasses; 4) Two pair of glasses in lieu of bifocal lenses;5) Any medical or surgical treatment of eye disease or injury; 6) Replacement of lost or broken lenses,contact lenses or frames, except when the member is normally eligible for services; 7) Any correctiveeyewear required by an employer as a condition of employment; 8) Services or materials provided asa result of Workers Compensation Law, or similar legislation, required by any governmental agencywhether Federal, State or subdivision thereof; 9) Any vision examination.
PLUS PLAN LIMITATIONS AND EXCLUSIONS
MATERIALS ONLY PLAN LIMITATIONS AND EXCLUSIONS
325 Cedar Street, Suite 800 Saint Paul, MN 55101 • ph 651-649-3503 800-620-5010 fax 651-649-3502 • www.directbenefits.com
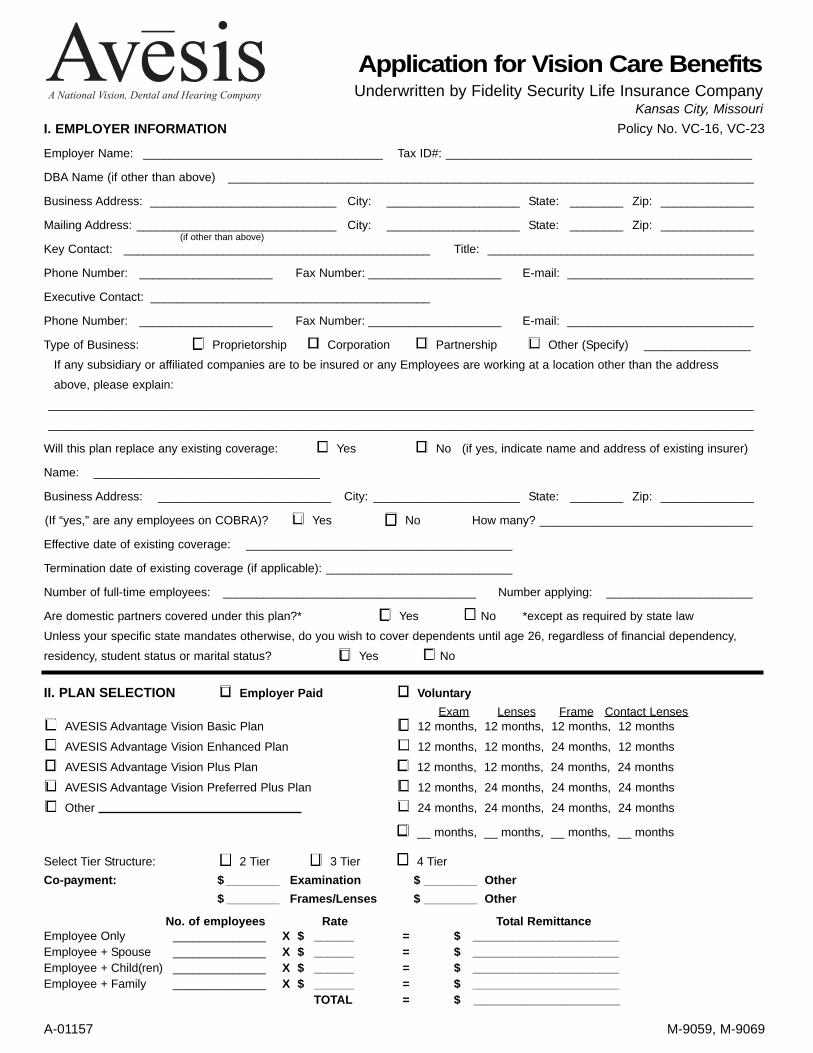
I. EMPLOYER INFORMATION
Employer Name: ____________________________________ Tax ID#: ______________________________________________
DBA Name (if other than above) _______________________________________________________________________________
Business Address: ____________________________ City: ____________________ State: ________ Zip: ______________
Mailing Address: ______________________________ City: ____________________ State: ________ Zip: ______________
Key Contact: ______________________________________________ Title: ________________________________________
Phone Number: ____________________ Fax Number: ____________________ E-mail: ____________________________
Executive Contact: __________________________________________
Phone Number: ____________________ Fax Number: ____________________ E-mail: ____________________________
Type of Business: Proprietorship Corporation Partnership Other (Specify) ________________
If any subsidiary or affiliated companies are to be insured or any Employees are working at a location other than the address
above, please explain:
__________________________________________________________________________________________________________
__________________________________________________________________________________________________________
Will this plan replace any existing coverage: Yes No (if yes, indicate name and address of existing insurer)
Name: __________________________________
Business Address: __________________________ City: ______________________ State: ________ Zip: ______________
(If “yes,” are any employees on COBRA)? Yes No How many? ________________________________
Effective date of existing coverage: ________________________________________
Termination date of existing coverage (if applicable): ____________________________
Number of full-time employees: ______________________________________ Number applying: ______________________
Are domestic partners covered under this plan?* Yes No *except as required by state law
Unless your specific state mandates otherwise, do you wish to cover dependents until age 26, regardless of financial dependency,
residency, student status or marital status? Yes No
II. PLAN SELECTION Employer Paid VoluntaryExam Lenses Frame Contact Lenses
AVESIS Advantage Vision Basic Plan 12 months, 12 months, 12 months, 12 months
AVESIS Advantage Vision Enhanced Plan 12 months, 12 months, 24 months, 12 months
AVESIS Advantage Vision Plus Plan 12 months, 12 months, 24 months, 24 months
AVESIS Advantage Vision Preferred Plus Plan 12 months, 24 months, 24 months, 24 months
Other 24 months, 24 months, 24 months, 24 months
__ months, __ months, __ months, __ months
Select Tier Structure: 2 Tier 3 Tier 4 TierCo-payment: ( ) Split $ ________ Examination $ ________ Other
$ ________ Frames/Lenses $ ________ Other
No. of employees Rate Total RemittanceEmployee Only ______________ X $ ______ = $ ______________________Employee + Spouse ______________ X $ ______ = $ ______________________Employee + Child(ren) ______________ X $ ______ = $ ______________________Employee + Family ______________ X $ ______ = $ ______________________
TOTAL = $ ______________________
(if other than above)
Application for Vision Care BenefitsUnderwritten by Fidelity Security Life Insurance Company
Kansas City, Missouri
A-01157 M-9059, M-9069
Policy No. VC-16, VC-23
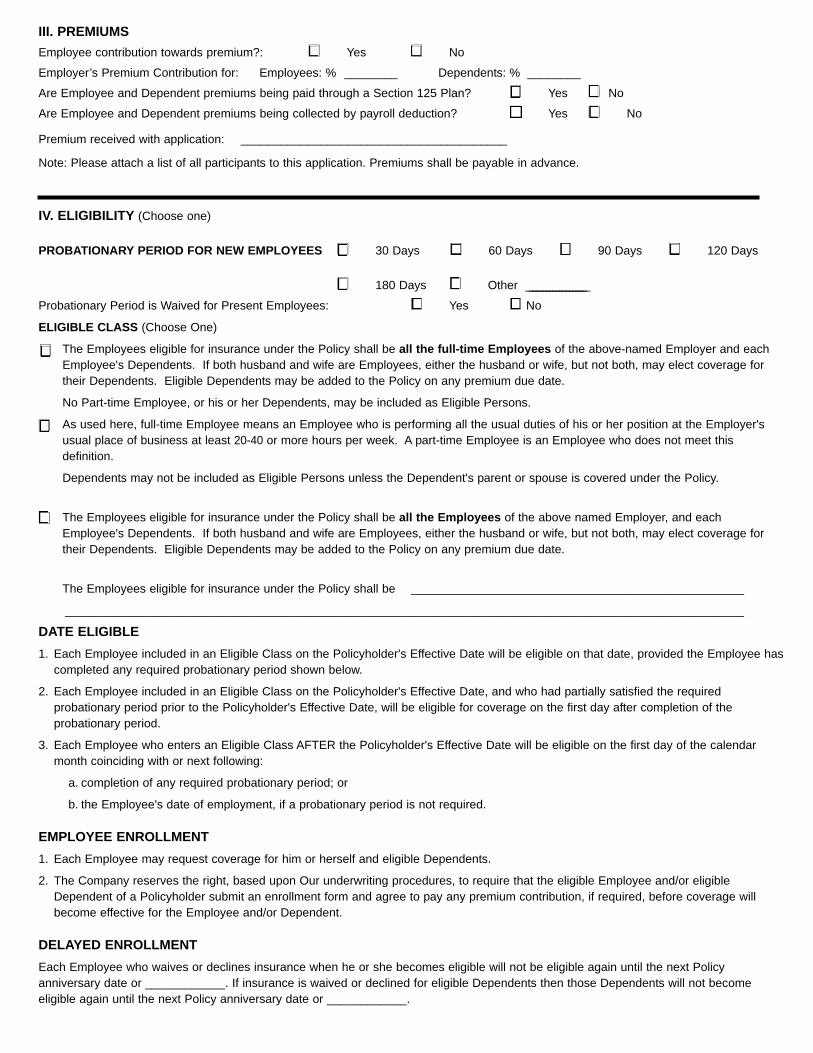
III. PREMIUMSEmployee contribution towards premium?: Yes No
Employer’s Premium Contribution for: Employees: % ________ Dependents: % ________
Are Employee and Dependent premiums being paid through a Section 125 Plan? Yes No
Are Employee and Dependent premiums being collected by payroll deduction? Yes No
Premium received with application: ________________________________________
Note: Please attach a list of all participants to this application. Premiums shall be payable in advance.
IV. ELIGIBILITY (Choose one)
PROBATIONARY PERIOD FOR NEW EMPLOYEES 30 Days 60 Days 90 Days 120 Days
180 Days Other __________________
Probationary Period is Waived for Present Employees: Yes No
ELIGIBLE CLASS (Choose One)
The Employees eligible for insurance under the Policy shall be all the full-time Employees of the above-named Employer and eachEmployee's Dependents. If both husband and wife are Employees, either the husband or wife, but not both, may elect coverage fortheir Dependents. Eligible Dependents may be added to the Policy on any premium due date.
No Part-time Employee, or his or her Dependents, may be included as Eligible Persons.
As used here, full-time Employee means an Employee who is performing all the usual duties of his or her position at the Employer'susual place of business at least 20-40 or more hours per week. A part-time Employee is an Employee who does not meet thisdefinition.
Dependents may not be included as Eligible Persons unless the Dependent's parent or spouse is covered under the Policy.
The Employees eligible for insurance under the Policy shall be all the Employees of the above named Employer, and eachEmployee's Dependents. If both husband and wife are Employees, either the husband or wife, but not both, may elect coverage fortheir Dependents. Eligible Dependents may be added to the Policy on any premium due date.
The Employees eligible for insurance under the Policy shall be __________________________________________________
______________________________________________________________________________________________________
DATE ELIGIBLE 1. Each Employee included in an Eligible Class on the Policyholder's Effective Date will be eligible on that date, provided the Employee has
completed any required probationary period shown below.
2. Each Employee included in an Eligible Class on the Policyholder's Effective Date, and who had partially satisfied the requiredprobationary period prior to the Policyholder's Effective Date, will be eligible for coverage on the first day after completion of theprobationary period.
3. Each Employee who enters an Eligible Class AFTER the Policyholder's Effective Date will be eligible on the first day of the calendarmonth coinciding with or next following:
a. completion of any required probationary period; or
b. the Employee's date of employment, if a probationary period is not required.
EMPLOYEE ENROLLMENT1. Each Employee may request coverage for him or herself and eligible Dependents.
2. The Company reserves the right, based upon Our underwriting procedures, to require that the eligible Employee and/or eligibleDependent of a Policyholder submit an enrollment form and agree to pay any premium contribution, if required, before coverage willbecome effective for the Employee and/or Dependent.
DELAYED ENROLLMENTEach Employee who waives or declines insurance when he or she becomes eligible will not be eligible again until the next Policyanniversary date or ____________. If insurance is waived or declined for eligible Dependents then those Dependents will not becomeeligible again until the next Policy anniversary date or ____________.
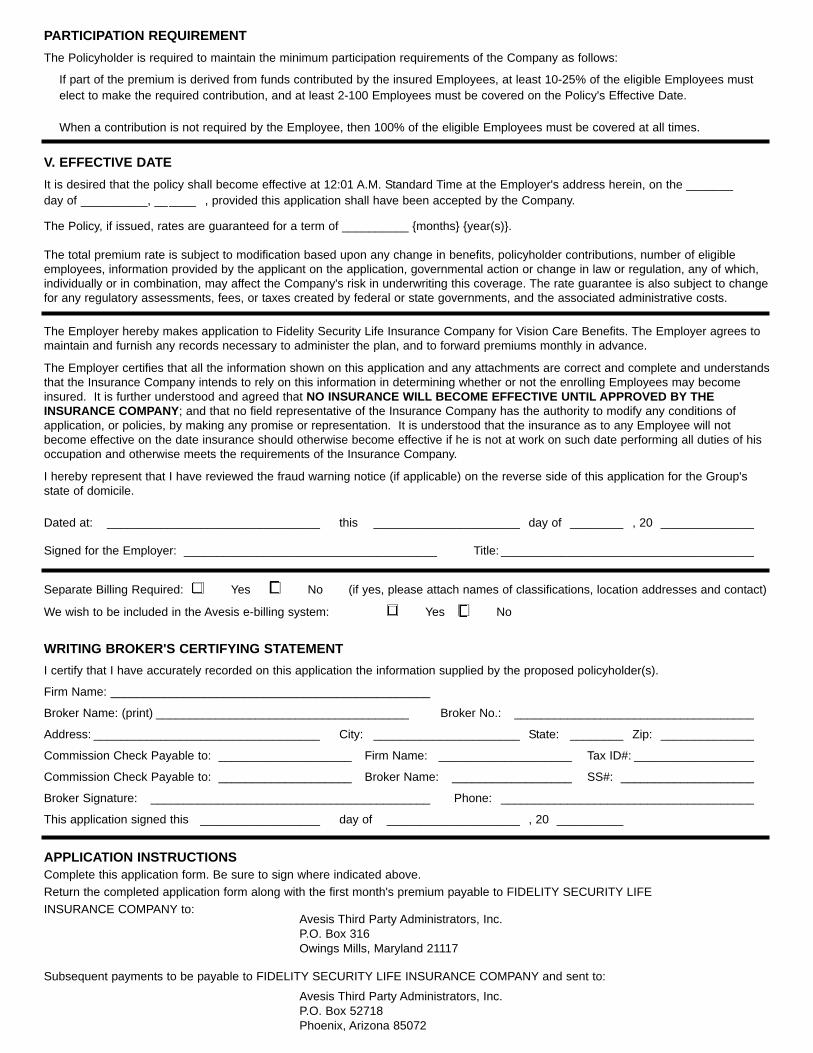
PARTICIPATION REQUIREMENTThe Policyholder is required to maintain the minimum participation requirements of the Company as follows:
If part of the premium is derived from funds contributed by the insured Employees, at least 10-25% of the eligible Employees mustelect to make the required contribution, and at least 2-100 Employees must be covered on the Policy's Effective Date.
When a contribution is not required by the Employee, then 100% of the eligible Employees must be covered at all times.
V. EFFECTIVE DATEIt is desired that the policy shall become effective at 12:01 A.M. Standard Time at the Employer's address herein, on the _______ day of __________, ______ , provided this application shall have been accepted by the Company.
The Policy, if issued, rates are guaranteed for a term of __________ {months} {year(s)}.
The total premium rate is subject to modification based upon any change in benefits, policyholder contributions, number of eligibleemployees, information provided by the applicant on the application, governmental action or change in law or regulation, any of which,individually or in combination, may affect the Company's risk in underwriting this coverage. The rate guarantee is also subject to changefor any regulatory assessments, fees, or taxes created by federal or state governments, and the associated administrative costs.
The Employer hereby makes application to Fidelity Security Life Insurance Company for Vision Care Benefits. The Employer agrees tomaintain and furnish any records necessary to administer the plan, and to forward premiums monthly in advance.
The Employer certifies that all the information shown on this application and any attachments are correct and complete and understandsthat the Insurance Company intends to rely on this information in determining whether or not the enrolling Employees may becomeinsured. It is further understood and agreed that NO INSURANCE WILL BECOME EFFECTIVE UNTIL APPROVED BY THEINSURANCE COMPANY; and that no field representative of the Insurance Company has the authority to modify any conditions ofapplication, or policies, by making any promise or representation. It is understood that the insurance as to any Employee will notbecome effective on the date insurance should otherwise become effective if he is not at work on such date performing all duties of hisoccupation and otherwise meets the requirements of the Insurance Company.
I hereby represent that I have reviewed the fraud warning notice (if applicable) on the reverse side of this application for the Group'sstate of domicile.
Dated at: ________________________________ this ______________________ day of ________ , 20 ______________
Signed for the Employer: ______________________________________ Title: ______________________________________
Separate Billing Required: Yes No (if yes, please attach names of classifications, location addresses and contact)
We wish to be included in the Avesis e-billing system: Yes No
WRITING BROKER'S CERTIFYING STATEMENTI certify that I have accurately recorded on this application the information supplied by the proposed policyholder(s).
Firm Name: ________________________________________________
Broker Name: (print) ______________________________________ Broker No.: ____________________________________
Address: __________________________________ City: ______________________ State: ________ Zip: ______________
Commission Check Payable to: ____________________ Firm Name: ____________________ Tax ID#: __________________
Commission Check Payable to: ____________________ Broker Name: __________________ SS#: ____________________
Broker Signature: __________________________________________ Phone: ______________________________________
This application signed this __________________ day of ____________________ , 20 __________
APPLICATION INSTRUCTIONSComplete this application form. Be sure to sign where indicated above.Return the completed application form along with the first month's premium payable to FIDELITY SECURITY LIFE INSURANCE COMPANY to:
Avesis Third Party Administrators, Inc.P.O. Box 316Owings Mills, Maryland 21117
Subsequent payments to be payable to FIDELITY SECURITY LIFE INSURANCE COMPANY and sent to:
Avesis Third Party Administrators, Inc.P.O. Box 52718Phoenix, Arizona 85072
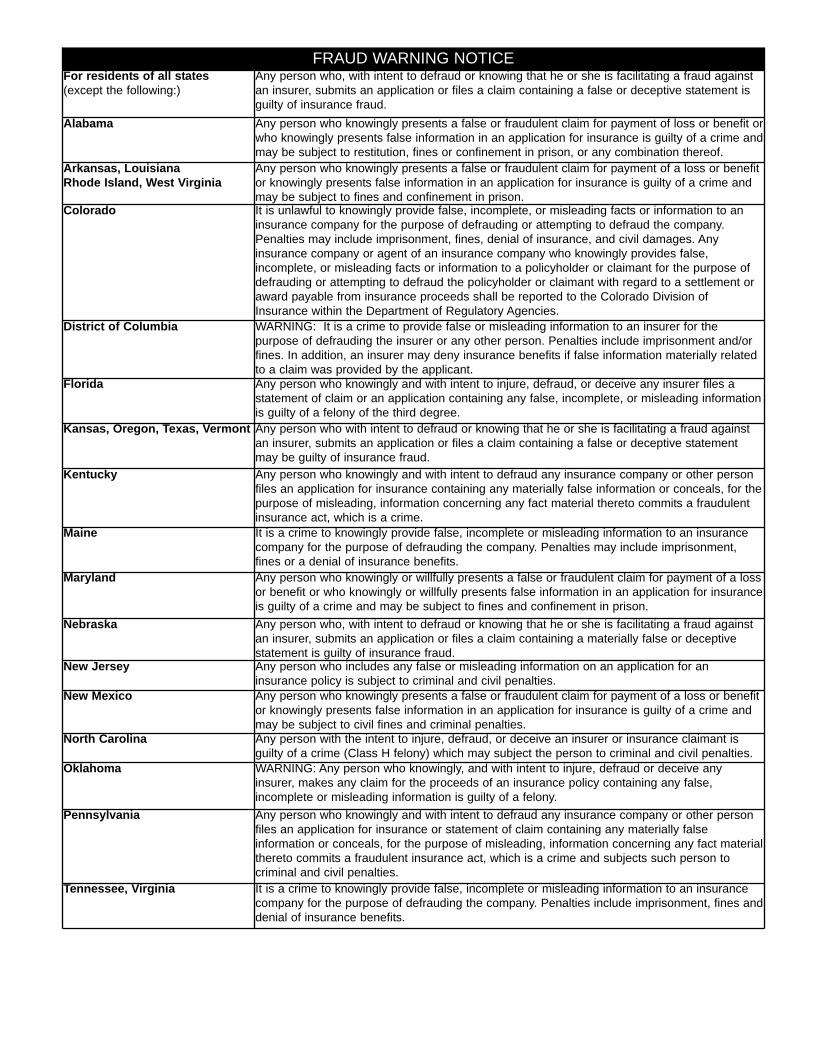
FRAUD WARNING NOTICEFor residents of all states(except the following:)
Any person who, with intent to defraud or knowing that he or she is facilitating a fraud againstan insurer, submits an application or files a claim containing a false or deceptive statement isguilty of insurance fraud.
Alabama Any person who knowingly presents a false or fraudulent claim for payment of loss or benefit orwho knowingly presents false information in an application for insurance is guilty of a crime andmay be subject to restitution, fines or confinement in prison, or any combination thereof.
Arkansas, Louisiana Rhode Island, West Virginia
Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefitor knowingly presents false information in an application for insurance is guilty of a crime andmay be subject to fines and confinement in prison.
Colorado It is unlawful to knowingly provide false, incomplete, or misleading facts or information to aninsurance company for the purpose of defrauding or attempting to defraud the company.Penalties may include imprisonment, fines, denial of insurance, and civil damages. Anyinsurance company or agent of an insurance company who knowingly provides false,incomplete, or misleading facts or information to a policyholder or claimant for the purpose ofdefrauding or attempting to defraud the policyholder or claimant with regard to a settlement oraward payable from insurance proceeds shall be reported to the Colorado Division ofInsurance within the Department of Regulatory Agencies.
District of Columbia WARNING: It is a crime to provide false or misleading information to an insurer for thepurpose of defrauding the insurer or any other person. Penalties include imprisonment and/orfines. In addition, an insurer may deny insurance benefits if false information materially relatedto a claim was provided by the applicant.
Florida Any person who knowingly and with intent to injure, defraud, or deceive any insurer files astatement of claim or an application containing any false, incomplete, or misleading informationis guilty of a felony of the third degree.
Kansas, Oregon, Texas, Vermont Any person who with intent to defraud or knowing that he or she is facilitating a fraud againstan insurer, submits an application or files a claim containing a false or deceptive statementmay be guilty of insurance fraud.
Kentucky Any person who knowingly and with intent to defraud any insurance company or other personfiles an application for insurance containing any materially false information or conceals, for thepurpose of misleading, information concerning any fact material thereto commits a fraudulentinsurance act, which is a crime.
Maine It is a crime to knowingly provide false, incomplete or misleading information to an insurancecompany for the purpose of defrauding the company. Penalties may include imprisonment,fines or a denial of insurance benefits.
Maryland Any person who knowingly or willfully presents a false or fraudulent claim for payment of a lossor benefit or who knowingly or willfully presents false information in an application for insuranceis guilty of a crime and may be subject to fines and confinement in prison.
Nebraska Any person who, with intent to defraud or knowing that he or she is facilitating a fraud againstan insurer, submits an application or files a claim containing a materially false or deceptivestatement is guilty of insurance fraud.
New Jersey Any person who includes any false or misleading information on an application for aninsurance policy is subject to criminal and civil penalties.
New Mexico Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefitor knowingly presents false information in an application for insurance is guilty of a crime andmay be subject to civil fines and criminal penalties.
North Carolina Any person with the intent to injure, defraud, or deceive an insurer or insurance claimant isguilty of a crime (Class H felony) which may subject the person to criminal and civil penalties.
Oklahoma WARNING: Any person who knowingly, and with intent to injure, defraud or deceive anyinsurer, makes any claim for the proceeds of an insurance policy containing any false,incomplete or misleading information is guilty of a felony.
Pennsylvania Any person who knowingly and with intent to defraud any insurance company or other personfiles an application for insurance or statement of claim containing any materially falseinformation or conceals, for the purpose of misleading, information concerning any fact materialthereto commits a fraudulent insurance act, which is a crime and subjects such person tocriminal and civil penalties.
Tennessee, Virginia It is a crime to knowingly provide false, incomplete or misleading information to an insurancecompany for the purpose of defrauding the company. Penalties include imprisonment, fines anddenial of insurance benefits.
TO BE COMPLETED BY THE EMPLOYEEEmployee Last Name Employee First Name MI
Date of Birth Social Security Number Sex
Street Address Apartment No.
City State Zip Code
TO BE COMPLETED BY THE EMPLOYER
New Enrollment AddDependent(s)
ChangeAddress PhoneName COBRA
Cancel CoveragePolicy HolderDependent(s)
Reason for Change Employment StatusQualifying Event: (PLEASE STATE) ___________________________________________
Requested Effective Date Date of Employment
AVESIS ADVANTAGE VISION CARE EMPLOYEE ENROLLMENT FORMUnderwritten by Fidelity Security Life Insurance Company Kansas City, Missouri Policy No. VC-16/VC-23
MACY C. O’BRIEN SCHOOL DISTRICT #90 & PINAL COUNTY SPECIAL EDUCATION12345-123401900
I authorize deductions from my earnings at the required contributions towards the cost of the coverage.
Signature Date
A-00713 M-9059/M-9069/M-9086
Dependent Name Date of Birth
Spouse /Domestic Partner
Child
Child
Child
Child
Child
Child
Male Female
Do you wish to cover your eligible dependents? Yes NoIf yes, complete the following:
I would like to cover additional eligible dependents (PLEASE LIST ON A SECOND ENROLLMENT FORM)
--//
-
//
//
//
//
//
//
//
//
PLEASE PRINT LEGIBLY
//01/12 - R03
//
FIRST LAST

Vision Examination
FRAMES
SPECTACLE LENSES
Contact Lenses
LASIK Surgery
Additional Discounts
Group Details
Benefit Frequency
Co-Pays
Rates
Out-of-NetworkReimbursement
www.avesis.com
Progressive LensesAre discounted up to 20% off retail inaddition to a $50 allowance
Lens Options, Non-Covered Itemsand Additional PurchasesAre discounted up to 20% off retail
Specialty LensesAre discounted up to 20% off retail in additionto the corresponding standard lens allowance
LASIK Surgery5% - 25% off retail
In-Network Benefits
Ask your vision care provider aboutthe premium No-Glare lens
AND
*
**
Vision ExamSpectacle LensesFramesContact Lenses
Effective Date:Group Number:Plan #:
Vision ExaminationMaterials
ExamStandard Single VisionStandard BifocalStandard TrifocalStandard LenticularProgressiveSpecialty Lenses
FrameContact Lenses (Elective)Contact Lenses (Med. Necessary)LASIK Surgery
Corresponding StandardLens Reimbursement
Up to:
Every:
Your vision exam is covered in full after a co-pay.
Medically necessary contact lenses are covered in full (prior authorization is required)
Your vision health is an important part of complete wellness. Avesis is pleased topresent your vision benefits which are designed to give you and your covered familymembers the care, value and service to help maintain good vision and overall health.
AVESIS NEW BUSINESS CHECKLIST
Please confirm that the following is submitted with all new cases:
Completed Employer Application
o Contact Direct Benefits for state specific applications for:
CA, DE, FL, HI, IL, KY, ME, NH, NV, OR, VT
Completed Employee Enrollment Forms (or Census Enrollment)
First Months Premium, payable to Fidelity Security
Producer Licensing Forms (if not previously contracted)
After all required forms are completed and signed, send all original forms to:
Direct Benefits, Inc. 325 Cedar Street, Suite 800
St Paul, MN 55101 651-649-3503 | 1-800-620-5010
Submission Date:
New Group Information should be postmarked no later than the end of the month to be effective by the first of the following month.





























