Embed Size (px)
DESCRIPTION
Â
Citation preview

Quality Strategy 2014-17

Page 2 of 41
Foreword
When I first came to Phoenix Futures in 2007, it was
clear to me that the charity needed to focus on quality
and growth. I wanted to do this without compromising
the passion of our staff and the spirit of peer-led
services, which is in our very roots. Over the last 7
years we have steadily improved the quality of what
we do. For example, in our residential Therapeutic
Community services we have a manual which is linked
to the evidence, and which helps both staff and service
users to know what they need to do and why. Our
work to improve quality has been recognised during
the last few years, for instance through achieving the
prestigious accreditations of Recognised for Excellence
– at 4 star level – in 2013; and Investors In People Gold
in 2014, and also through awards such as Third Sector’s
Best Employer in 2012. Whilst these are pleasing, they
are not the pinnacle of what we seek to achieve. We
have high ambitions for people in recovery, and we will
keep on improving what we do so that we can help
them. Our aim is to become the best, but not the
biggest, charity in our field. We owe that to the people
we exist for – our service users – past, present, and
future.
Karen Biggs,
Chief Executive

Page 3 of 41
Contents
1. Introduction 4
2. Our Quality Management System 5
3. Our Clinical Governance Framework 6
4. Our approach to risk and risk management 7
5. Our safety arrangements 9
6. Our information governance framework 11
7. Our performance information 12
8. Our service users – experts in recovery 13
9. Ensuring our effectiveness 14
10. Our culture of excellence and customer care 16
11. Our sustainability 17
12. Action plan 20
Appendix A – our Clinical Governance Framework 26
Appendix B – Our Integrated Governance arrangements 39
Page 4 of 41
1. Introduction
As the Corporate plan says “We are experts in recovery. We derive our expertise from our history our staff and our service users”. This strategy sets out how we apply this expertise and is divided into the following sections:
Our Quality Management System
Our Clinical Governance Framework
Our approach to risk and risk management
Our safety arrangements
Our information governance framework
Our performance information
Our service users – experts in recovery
Ensuring our effectiveness
Our culture of excellence and customer care
Integrated governance We set ourselves ambitious targets in the 2010-13 Quality Strategy and we excelled against these. Examples of what we achieved include:
Generating improvement against the EFQM Model and achieving 4 star Recognised for Excellence a year ahead of plan
We are a safer organisation to be in, with range of staff qualified to NEBOSH General Certificate and IOSH Managing Safely levels
We comprehensively revised all our policies and consolidated them into Policy manuals which contain all our policies in one place, and which are more easily updated in line with legislation and best practice.
We developed further our information systems and conducted a systems review to look at long term options.
We adopted the Outcomes Star as an extra tool for measuring outcomes
We produced our first Social Return On Investment report, for our Family service.
We have invested further in our Quality Department and now have a full time researcher who is affiliated to the University of Stirling as a Visiting Fellow.
We made it easier for people to feed back to us their compliments, complaints, and satisfaction
We continued our detailed internal audits, which have driven continuous improvement in our local services
National and local impact reports have been produced, in various formats including a podcast
Despite gaining various accreditations and winning various awards over the life of the last corporate strategy, we are not resting on our laurels; we will continue to approach every aspect of what we do with the passion which makes Phoenix Futures unique. Phoenix Futures recently embarked on a group structure, and all subsidiaries will be supported with the same arrangements as described herein, unless there are good reasons to the contrary. At the time of writing (June 2014), Foundation 66 is the first and only subsidiary charity in our group structure.

Page 5 of 41
2. Our Quality Management System
We have adopted the EFQM Excellence Model as our Quality Management System. We use it to assess the organisation as a whole, and we have been accredited to the Excellence Model under the Recognised for Excellence scheme, for which we achieved a 4 star rating in 2013. We also are accredited to Investors In People, relating to business excellence through people; and to CHAS for Health and Safety; and we see these as fitting within the wide umbrella of the Model in “People” and “People Results”, and “Partnerships and Resources” respectively. We see the Excellence Model as:
A framework to help us continuously improve
A way to benchmark ourselves against other organisations in a measurable way
A community where we can share good practice
More flexible and non-prescriptive than other Quality Management Systems available
The Model (pictured above) provides a generic framework of nine criteria which are applicable to any business. Excellent results with respect to performance, customers, people and society are achieved through leadership driving policy and strategy, people, partnership and resources and processes. We have used it to identify areas for improvement which are aligned with planning processes, particularly the Corporate Plan 2014-17 What we will do:
1. We will self-assess against the Model in November 2014, led by trained EFQM Assessors. 2. We will invite another external assessment under Recognised for Excellence in April 2015,
and gain 4 or 5 stars. 3. We will improve our process management in our support services, in line with ISO 9001
standards.
Page 6 of 41
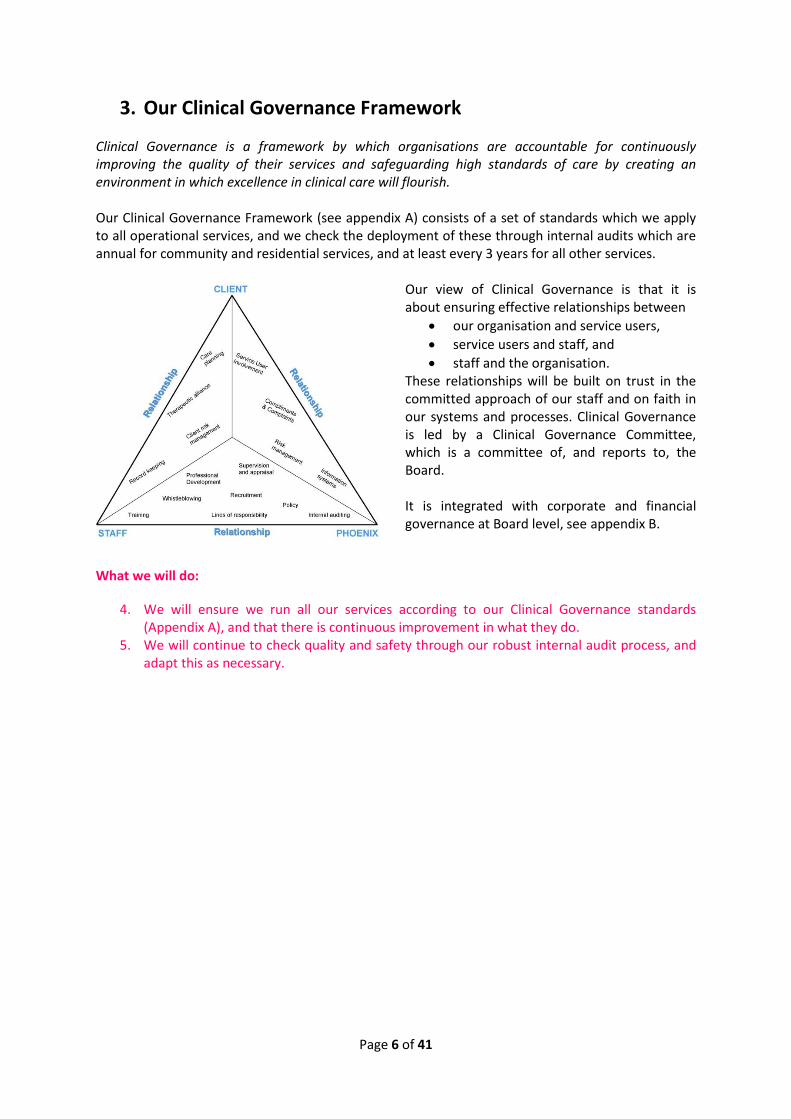
3. Our Clinical Governance Framework
Clinical Governance is a framework by which organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish. Our Clinical Governance Framework (see appendix A) consists of a set of standards which we apply to all operational services, and we check the deployment of these through internal audits which are annual for community and residential services, and at least every 3 years for all other services.
Our view of Clinical Governance is that it is about ensuring effective relationships between
our organisation and service users,
service users and staff, and
staff and the organisation. These relationships will be built on trust in the committed approach of our staff and on faith in our systems and processes. Clinical Governance is led by a Clinical Governance Committee, which is a committee of, and reports to, the Board. It is integrated with corporate and financial governance at Board level, see appendix B.
What we will do:
4. We will ensure we run all our services according to our Clinical Governance standards (Appendix A), and that there is continuous improvement in what they do.
5. We will continue to check quality and safety through our robust internal audit process, and adapt this as necessary.

Page 7 of 41
4. Our approach to risk and risk management
How we manage risk All risks posed to our business will be managed appropriately and proactively. We are committed to maintaining an open and responsive approach to risk management which involves staff, stakeholders, and service users. We keep a corporate risk register and an operational risk register, and these are presented to the Board via the Audit & Control Committee and Clinical Governance Committee respectively each year and used in planning processes. We identify risks through:
Staff through supervision and the line management structure
H&S accident reporting, including trends
Whistle-blowing policy which is promoted annually by our HR department
Serious Incidents reported through our Serious Incidents procedure
Media scanning We approach risk management on the supposition that it is best to manage risk at the lowest appropriate level, but at the same time that serious risks will be escalated appropriately. We choose staff who have the ability to dynamically assess risk, and we provide NVQ 3 and 4 level training on risk assessment at managerial level, and safer working practices at staff level. At a local level, we ensure corporately that each local service does a general risk assessment for its premises and regular activities. This is checked by holding a corporate copy and through review by the Quality & Performance Department. We also ensure that each service does appropriate risk assessments on an extraordinary basis such as activities / trips. Each client is risk assessed and an appropriate risk management plan put into place. Our On Call policy and processes ensures that there is always a first stage on-call for applicable services, plus a second stage on-call manned by a member of the Senior Management Team, and both are on a 24/7/365 basis. This enables us to support staff and highlight any risks to appropriate people very quickly. How we record and learn from Serious Incidents Phoenix Futures has a clear process for Serious Incidents. Staff complete a Serious Incident form within 2 hours of such incident occurring. This is graded by severity according to our risk matrix, and lodged with our Quality and Performance Department. Serious Incidents are escalated to senior managers as applicable by severity and nature. Serious Incidents are aggregated quarterly and discussed at both the H&S Committee and Clinical Governance Committee. How we approach safeguarding adults and children Safeguarding means protecting people’s health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It is fundamental to creating high-quality health and social care. We have high standards for safeguarding for our staff. We vet and re-vet staff effectively, and train them up to the standards we expect in our policy and in the law We have effective policies and processes which guide our staff in the event of incidents, and we monitor various items as part of our Clinical Governance Framework (see appendix).
Page 8 of 41
What we will do:
6. We will ensure a wider involvement in the compilation and dissemination of the Risk Registers, ensuring our culture is that of a proportionate approach to risk
7. We will move our Serious Incidents into a more comprehensive information system so that the process is more automated
8. We will continue to improve our approach to safeguarding vulnerable adults and children, particularly in terms of the deployment of training.

Page 9 of 41
5. Our safety arrangements
Safety is the basic building block of offering any service. We will prioritise safety and where we work in partnership with other agencies will ensure we are satisfied with their arrangements. We will be renowned by our stakeholders and by our insurers for being a safe steward of people’s health and safety. In 2013 we registered successfully with the Contractors Health and Safety Assessment Scheme (CHAS). Our approach centres around creating an identity for staff and service users which is that of someone who takes safety seriously and who takes action whenever they see a hazard. Our by-line is “Think treatment, Think safety”. We also have a more specialist identity for those within our regional and local structure. The identity is designed to be fun – it is based around a series of hats and signified in practice with coloured lanyards:
The Safety Champion (white hat) reports directly into a member of the [national] Health & Safety Committee; and they also liaise closely with the Locality Manager. This structure allows us to address safety concerns quickly and with sufficient backing. Decisions are guided by a comprehensive Health and Safety Policy available to staff through printed form and on our intranet site. Our Health and Safety Committee meets every quarter and is chaired by the Chief Executive. It reports to the Clinical Governance Committee of the Board. It oversees the English and Scottish National Forums for Health and Safety, which is where the white hats regularly meet every 6 months to determine their strategic direction. On a regional basis, white hats meet those under their charge within their region. What we will do:
9. Continue to extend NEBOSH and IOSH qualifications amongst staff, in order to gain competent advice corporately and locally
10. Continue to maintain our registration with CHAS annually 11. Review the dynamism of our Health and Safety arrangements, and how we engage our
staff in them better, using learning gained from the ECETT European knowledge exchange scheme
A safety identity
“Safety Champion”
Region
“Safety Keeper”
Service
First Aider Fire Warden

Page 10 of 41
12. Become affiliated to a national H&S membership organisation 13. We will achieve compliance to BS25999 around business continuity 14. We will ensure we have proactive corporate response to emerging events, through
extending our use of alerts such as Met Office weather alerts.
Page 11 of 41
6. Our Information Governance framework
Information Governance ensures necessary safeguards for, and appropriate use of, client and personal information. The Quality Department leads on Information Governance for the organisation. Our approach centres around the use of the NHS Information Governance toolkit as our framework, but in order to become even better we will seek to achieve BS27000 accreditation. What we will do:
15. Continue our use of the NHS Information Governance toolkit, reporting this to the Clinical
Governance Committee, and be majority level 3 by 2017.
16. Achieve BS27000 accreditation
Page 12 of 41
7. Our performance information
Phoenix Futures is committed to flexibility in light of commissioning requirements, and to that end we operate several operational information systems. In the majority of our services we have been using Janus for the last 5 years, which is a bespoke system which we developed in partnership with a software supplier. Using the Information Systems review held in autumn 2013, and the input of our staff user group, we are committed to migrating from Janus to a proprietary solution which will better fit the needs of our growing organisation and the increasingly complex national data set. We will use this solution alongside other proprietary systems which we already use. We will invest in robust systems to monitor our performance, and in expert staff to analyse and present the data emerging from the systems.
What we will do:
17. We will implement a system or systems to be our main database(s) of choice, replacing
Janus.
18. We will ensure the integration of information systems between operational systems, and
between operational systems and finance/HR systems
19. We will review our KPIs and align them in a hierarchy which shows how we are meeting the
goals of the corporate plan.
20. We will ensure all staff are well trained not only in our systems but also in the principles of
performance management, and are well briefed about their role in this
Page 13 of 41
8. Our service users – experts in recovery
We believe that service users are “experts by experience”. Phoenix Futures was founded in 1970 on the principle of addicts helping addicts – peer support. We continue to deliver services based on high levels of service user input – for example, our Therapeutic Communities within prisons and in residential rehabs across the UK, or peer mentoring services. Peer support and delivery is a traditional area of strength for Phoenix Futures and we will expand on this where we can. We involve service users in evaluating our services in many ways, such as through our Service User Satisfaction Survey or through interviewing them at internal audits. As our service users are experts by experience, we believe there is more potential to refine our approaches and involve our clients more in the evaluation of our services. At a national level we are re-launching our Service User Council, and investing in dedicated support from two paid co-ordinators. This development will be key in ensuring that our service users are fully represented across all levels of the organisation including in decisions made at the Clinical Governance Committee. What we will do:
21. Apply our new framework for peer mentoring and expand this in the delivery of services.
22. Work with SMART Recovery to review the quality and consistency of meetings
sponsored by Phoenix Futures
23. Develop a new model for a Service User Council and put resources in place to support
this, ensuring that there is representation of service user views at our Clinical
Governance Committee
24. Relaunch mystery shopping, to be led by service users themselves in liaison with the
Service User Council
25. Investigate ways to further involve service users or ex-service users in our audit process
26. Ensure we give service users better and more systematic ways to evaluate our
programmes as they leave our services
27. Continue to expand our provision of volunteering opportunities and hold regular
volunteer conferences
28. Achieve the Investors In Volunteers national accreditation

Page 14 of 41
9. Ensuring our effectiveness
Basing our interventions on research We have employed a dedicated researcher, based in our Quality and Performance Department, and we undertake project based research. The aim of this is to ensure that our services operate according to the evidence base, and also to help add to the evidence base for existing and new interventions – examples of this include ongoing work such as the national TRACER research for which we are the largest single contributor. We are also investigating new avenues such as the Justice Data Lab to look at reoffending rates from our Prison TC programmes. We also offer opportunities to researchers at undergraduate and postgraduate level from outside Phoenix, to access clients and staff in research which is ethical and agreed by our Clinical Governance Committee. We also commission research where this is needed, for example we commissioned a Social Return on Investment report which showed that our National Specialist Family Service returned social value of £3.54 [check figure] for every £1 spent. We do not limit our evaluation to “traditional” measures of drug and alcohol treatment. Our pioneering Phoenix Plus model focuses on building Recovery Capital. We evaluate how we add Recovery Capital, for example we know that 1 in 5 clients did any paid or voluntary work in the month before coming to Phoenix; but this rose to 3 in 5 clients in the month after treatment. Innovation Innovation has always been a cornerstone of Phoenix Futures’ approach to recovery. During the life of the last Corporate Plan, we launched a Fundraising and Innovation Team, to take forward ideas in a structured way. One innovation that has been running for nearly 20 years in Phoenix Futures is our Recovery Through Nature programme (formerly Conservation Therapy). This unique programme adds value through taking groups of service users into natural environments and achieving tasks such as repairing walls and footpaths, building bird hides, digging ponds etc. It encourages service users to stay 50% longer, and makes them around 45% more likely to complete their programme successfully. As with many truly pioneering organisations, they press ahead with such innovation and ahead of the evidence, and then the evidence catches up. We have a full literature surrounding RTN now and we are committed to expanding its delivery. Other more recent innovations have been the Phoenix Forest, which is an ongoing project which plants a tree for every service user who graduates from one of our structured treatment services; and the Voyage of Recovery, which was a sailing voyage around the coast of the UK in 2012. We now have an ongoing system which helps our staff put their innovative ideas into action – the Fundraising and Innovation Team – which awards grants internally, and helps staff gain fundraising for their ideas. Linking theory and practice Over the last few years, we have become much more explicit at linking theory and practice. For example, we have a detailed manual for our Therapeutic Communities which sets out what we do and why we do it, based on the wide ranging and long standing evidence base for TCs which has built up over nearly 100 years. We have been expanding our use of such manuals and our goal is that eventually all our programmes will have them.

Page 15 of 41
What we will do:
29. We will expand our use of longitudinal research, and ensure to this end that follow-up is built into our systems from the very start of a client’s contact with us.
30. We will continue to increase the robustness of our research and publicise it more. 31. We will review our use of outcomes measures, looking particularly at the Recovery Capital
measures 32. We will continue to deliver Recovery Through Nature, expand on its use, and look at new
models and new areas of delivery for it. 33. We will continue to seek adaptations to programmes, and new programmes, through the
Fundraising and Innovation Team. 34. We will continue to expand our use of manualised programmes 35. We will demonstrate our value to public health through local and national impact reporting
Page 16 of 41
10. Culture of excellence and customer care
Over a number of years there has been a growing culture of excellence in Phoenix Futures, driven from the top, with an unwavering belief that quality is critical. Our staff believe in what we do. We are nurturing a subculture of customer care. The first step in customer care is in knowing our customers. To this end we know more about our clients than ever before, through our “Footprints” surveys. These focus on giving us a snapshot of the complexity of problems our clients face and we will continue to refine and deploy this valuable resource. For example, from this we know that
25% of our clients have been in care, compared to 1% of the UK population.
21% of our clients are homeless or temporary homeless when they come to us.
We have a well developed compliments and complaints process, and we get an average of nearly 4 compliments to every complaint on an overall corporate basis. We want to ensure that complaints are resolved more locally and meaningfully for our complainants, and have started to make changes to this effect. Our customers are not just our service users; they are also the people and bodies who pay for our services. We have piloted commissioner and funder feedback and we will continue to develop this so we can ensure they are happy with the services we provide for them. What we will do:
36. We will ensure we resolve complaints for the complainants locally where possible, following up on a sample basis to ensure this is achieved
37. We will continue to operate our Footprints survey and refine this process 38. We will continue to celebrate World Quality Day and to seek other ways of promoting
quality within and outside Phoenix Futures

Page 17 of 41
11. Our sustainability
We believe that delivering services in a way that is environmentally sustainable is important. We have a sustainability strategy and action plan. The Head of Procurement is responsible for ensuring Phoenix Futures and Foundation66 meets the highest standards in environmental management in all our business activities, leading on development of organisation’s environmental agenda and the implementation of the organisation’s Environmental Policy and Action Plan. Our environmental management system and Environmental Policy Statement and Action Plan have been developed to ensure we continue to operate at an equivalent level to ISO 14001/EMAS or equivalent. Phoenix Futures’ and Foundation66 Environmental Policy and Action Plan sets out the relevant environmental regulations and legislation relating to our business operations with which we will comply. These include but are not limited to: • Control of Pollution (Amendment) Act 1989 • Environmental Protection Act 199 • Controlled Waste Regulations 1992 SI 588 • Controlled Waste (Amendment) Regulations 1993 SI 566 • Environmental Protection (Duty of Care) Regulations 1991 SI 2839 • Environmental Protection (Duty of Care) (England) (Amendment) Regulations 2003 SI 63 • Hazardous Waste (England and Wales) Regulations 2005 SI 894 Our overarching environmental objective is to reduce both organisation’s carbon footprint as we recognise the environmental impact our services have. We regularly monitor each service’s gas/electricity/water usage and aim to reduce the gas and electricity consumption of all Phoenix Futures services by at least 5% per annum. Our central procurement department manages an automated data collection system that will monitor monthly the energy usage of the sites used for delivering this contract, allowing us to benchmark our success against existing monthly usage data. We will ensure waste is recycled where possible, or disposed of responsibly/ethically. Through our central procurement department we ensure services use a wide range of recycled and ethical products including nearly 100% all paper used, recycled printer cartridges, and environmentally-friendly stationary. Phoenix Futures will also continue to recycle all company-owned mobile phones/BlackBerrys internally or via donated to organisations such as Macmillan Cancer Care. We will continue to reduce organisational travel incurred by promoting video conferencing, online courses, increased local rather than central training sessions and public or carbon neutral transport to reduce impact where travel is necessary. supports environmental research and initiatives through Recovery through Nature, our pioneering conservation therapy programme, which runs in all of our residential services as well as many of our community services. Last year through this project, we provided 30,000 volunteer hours to improving local natural areas including by rebuilding dry-stone walls, building bird hides, planting forests and rebuilding paths. Phoenix Futures has also planted two Phoenix Forests in partnership with the Woodland Trust (England) and John Muir Trust (Scotland). Through the initiative, a tree is planted for every person who graduates from one of our recovery programmes. In January 2011, we planted 737 trees with a further 974 planted in 2012 and 2,294 planted in 2013, thus making a significant contribution to

Page 18 of 41
offsetting our carbon footprint. In ten years’ time, there will be at least 10,000 trees reaching maturity in the Phoenix Forest, helping the Woodland Trust with its development of the site, which will ultimately host 600,000 trees. Each acre of trees absorbs 327 tonnes of CO2 during its lifetime of 100 years (one tonne per tree). Phoenix Futures and Foundation66 take a number of actions to minimise the impact of disposal of broken or out of date PCs and computer equipment: - Stripping and re-modelling the PC by the IT department for a fraction of the cost of replacing a PC and then re-using it. - Breaking the PC into component parts and selling these on ebay at a profit, re-investing the money into the organisation. - Giving PCs to specialist recycling companies if deemed the most practical solution by the IT department. The IT department centrally monitors the money that is raised from selling PCs and reinvests it towards initiatives which support our corporate social responsibility objectives. For example, in 2012 they raised £660 from selling old IT equipment that they donated to Phoenix Futures’ Voyage of Recovery. We recycle company-owned mobile phones and BlackBerrys internally or donate them to charities for re-selling or recycling of parts. Through our central procurement department we purchase Fairtrade coffee, tea and sugar. Working towards our organisational goal to decrease travel and reduce the associated environmental impact, through changes already implemented, we have seen organisational travel reduce by over 30% in 2011-2012 compared to 2008-2009. To reduce the organisation’s carbon footprint, Phoenix Futures is investing in biomass (wood pellet) boilers at our largest energy consuming residential services, based in Hampshire and the Wirral. These boilers will provide hot water and heating to up to 32 service users each and will replace the existing fossil fuel boiler, thus considerably reducing the carbon emissions of these two sites. The biomass boiler recently installed at our Wirral residential service has been accepted into Ofgem’s Renewable Heat Incentive scheme. Our residential sites (often the biggest producers of waste across our operations) have been able to consistently recycle 50% of their waste through the introduction of 1,100 litre mixed recycling bins which cater for all paper and cardboard, metal cans, aluminum, steel, plastics, bottles, shrink-wrap and bubble wrap. Organizational waste disposal is continually monitored through monthly reporting to ensure best practice. After reviewing our printer cartridge arrangements last year, our central procurement team took the opportunity to move our contracts to a new supplier which recycles a greater volume of cartridges than the supplier with whom our contract was previously held. This has led to a 37% reduction in our annual spend on printer cartridges and a demonstrable reduction in environmental impact as a result. Our central procurement function has designed an automated data collection system that ensures that the gas and electricity usage of each Phoenix Futures and Foundation66 site is monitored on a monthly basis, providing up-to-date, accurate usage data for the entire organisation. This allows Phoenix Futures and Foundation66 to benchmark our progress in meeting environmental targets,
Page 19 of 41
such as the new initiatives we are currently introducing to reduce our gas and electricity usage by at least 5% per annum. Additionally, it enables IT systems to quickly identify any monthly usage anomalies for a particular site and investigate accordingly. Our Phoenix Forest has offset the organisation’s CO2 production by up to 55% per year.
What we will do:
36. Deliver against the standards set out in our new procurement policy launched in 2014
Page 20 of 41
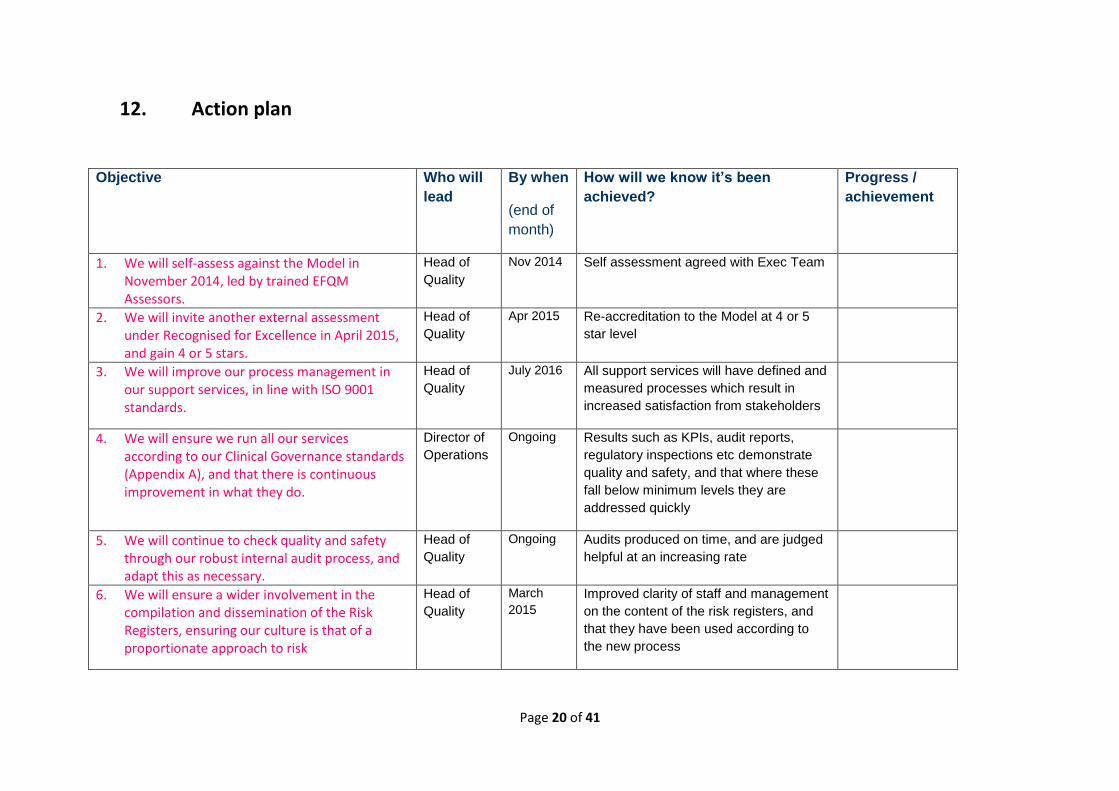
12. Action plan
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
1. We will self-assess against the Model in November 2014, led by trained EFQM Assessors.
Head of
Quality
Nov 2014 Self assessment agreed with Exec Team
2. We will invite another external assessment under Recognised for Excellence in April 2015, and gain 4 or 5 stars.
Head of
Quality
Apr 2015 Re-accreditation to the Model at 4 or 5
star level
3. We will improve our process management in our support services, in line with ISO 9001 standards.
Head of
Quality
July 2016 All support services will have defined and
measured processes which result in
increased satisfaction from stakeholders
4. We will ensure we run all our services according to our Clinical Governance standards (Appendix A), and that there is continuous improvement in what they do.
Director of
Operations
Ongoing Results such as KPIs, audit reports,
regulatory inspections etc demonstrate
quality and safety, and that where these
fall below minimum levels they are
addressed quickly
5. We will continue to check quality and safety through our robust internal audit process, and adapt this as necessary.
Head of
Quality
Ongoing Audits produced on time, and are judged
helpful at an increasing rate
6. We will ensure a wider involvement in the compilation and dissemination of the Risk Registers, ensuring our culture is that of a proportionate approach to risk
Head of
Quality
March
2015
Improved clarity of staff and management
on the content of the risk registers, and
that they have been used according to
the new process
Page 21 of 41
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
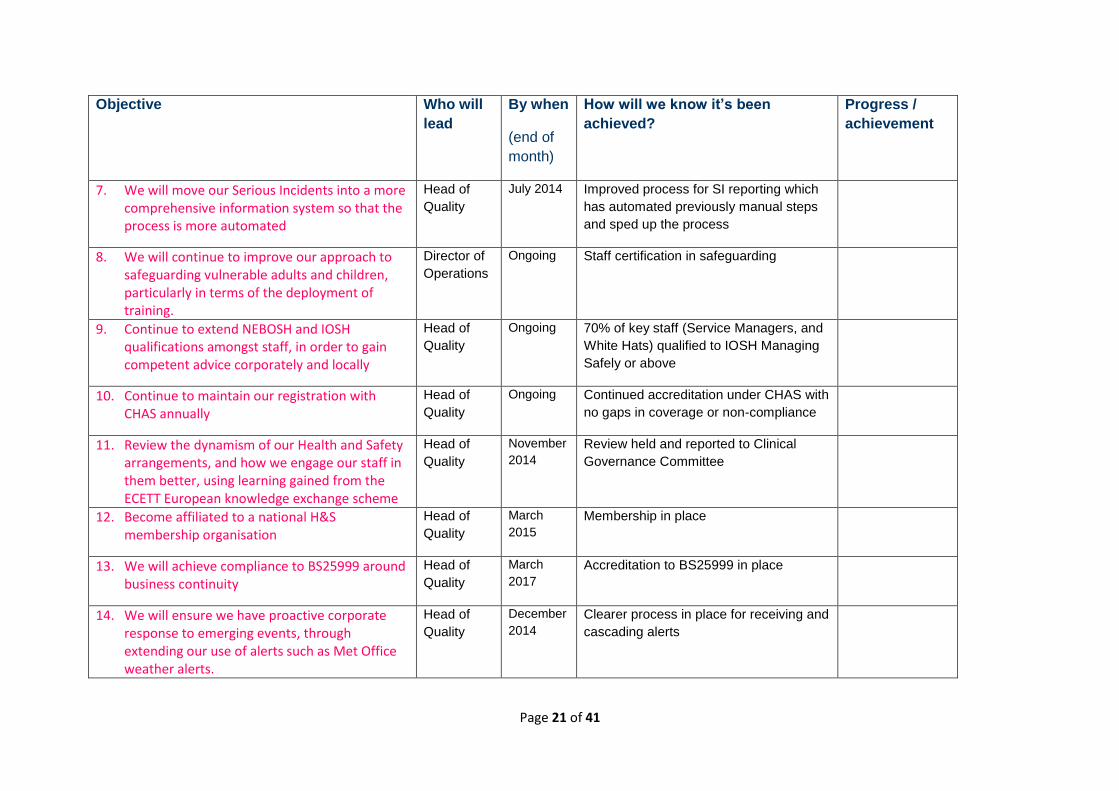
7. We will move our Serious Incidents into a more comprehensive information system so that the process is more automated
Head of
Quality
July 2014 Improved process for SI reporting which
has automated previously manual steps
and sped up the process
8. We will continue to improve our approach to safeguarding vulnerable adults and children, particularly in terms of the deployment of training.
Director of
Operations
Ongoing Staff certification in safeguarding
9. Continue to extend NEBOSH and IOSH qualifications amongst staff, in order to gain competent advice corporately and locally
Head of
Quality
Ongoing 70% of key staff (Service Managers, and
White Hats) qualified to IOSH Managing
Safely or above
10. Continue to maintain our registration with CHAS annually
Head of
Quality
Ongoing Continued accreditation under CHAS with
no gaps in coverage or non-compliance
11. Review the dynamism of our Health and Safety arrangements, and how we engage our staff in them better, using learning gained from the ECETT European knowledge exchange scheme
Head of
Quality
November
2014
Review held and reported to Clinical
Governance Committee
12. Become affiliated to a national H&S membership organisation
Head of
Quality
March
2015
Membership in place
13. We will achieve compliance to BS25999 around business continuity
Head of
Quality
March
2017
Accreditation to BS25999 in place
14. We will ensure we have proactive corporate response to emerging events, through extending our use of alerts such as Met Office weather alerts.
Head of
Quality
December
2014
Clearer process in place for receiving and
cascading alerts
Page 22 of 41
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
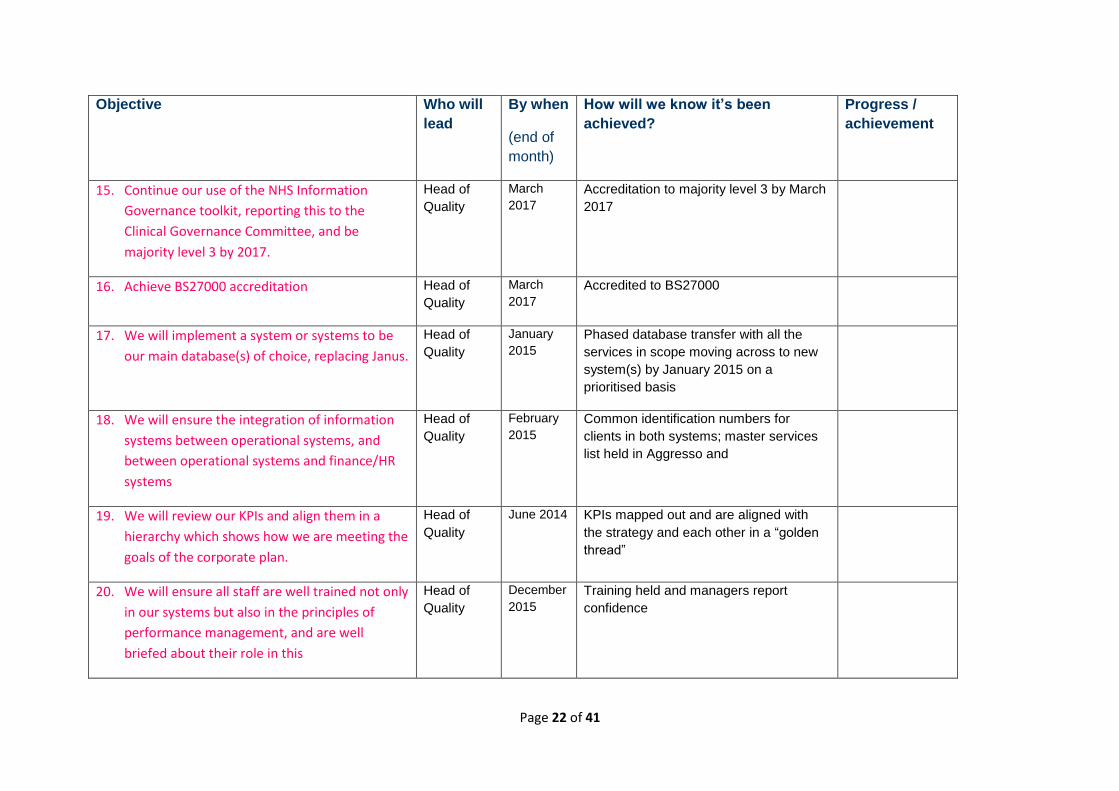
15. Continue our use of the NHS Information
Governance toolkit, reporting this to the
Clinical Governance Committee, and be
majority level 3 by 2017.
Head of
Quality
March
2017
Accreditation to majority level 3 by March
2017
16. Achieve BS27000 accreditation Head of
Quality
March
2017
Accredited to BS27000
17. We will implement a system or systems to be
our main database(s) of choice, replacing Janus.
Head of
Quality
January
2015
Phased database transfer with all the
services in scope moving across to new
system(s) by January 2015 on a
prioritised basis
18. We will ensure the integration of information
systems between operational systems, and
between operational systems and finance/HR
systems
Head of
Quality
February
2015
Common identification numbers for
clients in both systems; master services
list held in Aggresso and
19. We will review our KPIs and align them in a
hierarchy which shows how we are meeting the
goals of the corporate plan.
Head of
Quality
June 2014 KPIs mapped out and are aligned with
the strategy and each other in a “golden
thread”
20. We will ensure all staff are well trained not only
in our systems but also in the principles of
performance management, and are well
briefed about their role in this
Head of
Quality
December
2015
Training held and managers report
confidence

Page 23 of 41
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
21. Apply our new framework for peer mentoring
and expand this in the delivery of services.
Head of
Marketing
and
Comms
July 2014 Peer mentoring policy in place and being
used in increasing number of services
22. Work with SMART Recovery to review the
quality and consistency of meetings sponsored
by Phoenix Futures
Head of
Quality
March
2015
Review held and plans in place to
improve coverage / quality where
necessary
23. Develop a new model for a Service User Council
and put resources in place to support this,
ensuring that there is representation of service
user views at our Clinical Governance
Committee
Head of
Marketing
and
Comms
March
2015
Service User Council in place and
functioning effectively, with service user
views being represented at the Clinical
Governance Committee.
24. Relaunch mystery shopping, to be led by
service users themselves in liaison with the
Service User Council
Head of
Quality
March
2015
Mystery shopping producing results
which are reported back to Clinical
Governance Committee
25. Investigate ways to further involve service
users or ex-service users in our audit process
Head of
Quality
August
2015
Methodology approved by Clinical
Governance Committee and
arrangements in place
26. Ensure we give service users better and more
systematic ways to evaluate our programmes
as they leave our services
Head of
Quality
October
2015
Pilot taken place and reported back to
Clinical Governance Committee

Page 24 of 41
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
27. Continue to expand our provision of
volunteering opportunities and hold regular
volunteer conferences
Director of
Operations
Ongoing Increasing number of volunteers;
conferences held at least once per year
28. Achieve the Investors In Volunteers national
accreditation
Director of
Operations
March
2016
Accreditation in place
29. We will expand our use of longitudinal research, and ensure to this end that follow-up is built into our systems from the very start of a client’s contact with us.
Head of
Quality
Ongoing Follow up consent in place by July 2014;
clear proposals to this to the Clinical
Governance Committee by December
2014
30. We will continue to increase the robustness of our research and publicise it more.
Head of
Quality
Ongoing Presence of research on website;
Increase in amount of research that is
published in academic circles.
31. We will review our use of outcomes measures, looking particularly at the Recovery Capital measures
Director of
Operations
March
2015
Pilot of REC CAP carried out; clear
message delivered across the
organisation in terms of outcome
measures
32. We will continue to deliver Recovery Through Nature, expand on its use, and look at new models and new areas of delivery for it.
Head of
Quality
Ongoing Continued success of RTN and
expansion in sites by 10%
33. We will continue to seek adaptations to programmes, and new programmes, through the Fundraising and Innovation Team.
Chief
Executive
Ongoing Reporting back from Fundraising and
Innovation Team to Board

Page 25 of 41
Objective Who will
lead
By when
(end of
month)
How will we know it’s been
achieved?
Progress /
achievement
34. We will continue to expand our use of manualised programmes
Director of
Operations
Ongoing Manuals in place for all prison based
services by March 2016, and for all
community services by March 2017
35. We will demonstrate our value to public health
through local and national impact reporting
Head of
Quality
Sept 2014
and Sept
every year
National impact report, and local impact
reports, produced and distributed
36. We will ensure we resolve complaints for the complainants locally where possible, following up on a sample basis to ensure this is achieved
Head of
Quality
Ongoing Sample to indicate 90+% satisfaction with
our process
37. We will continue to operate our Footprints survey and refine this process
Head of
Quality
Ongoing Reports produced from each survey
which are helpful to senior staff and our
researcher, and to external agencies
38. We will continue to celebrate World Quality Day and to seek other ways of promoting quality within and outside Phoenix Futures
Head of
Quality
Ongoing Engagement with World Quality Day and
quality initiatives improves both within
and outside the organisation.
39. Deliver against the standards set out in our new procurement policy launched in 2014
Head of
Procure-
ment
Ongoing Continuation of trends in environmental
sustainability results

Page 26 of 41
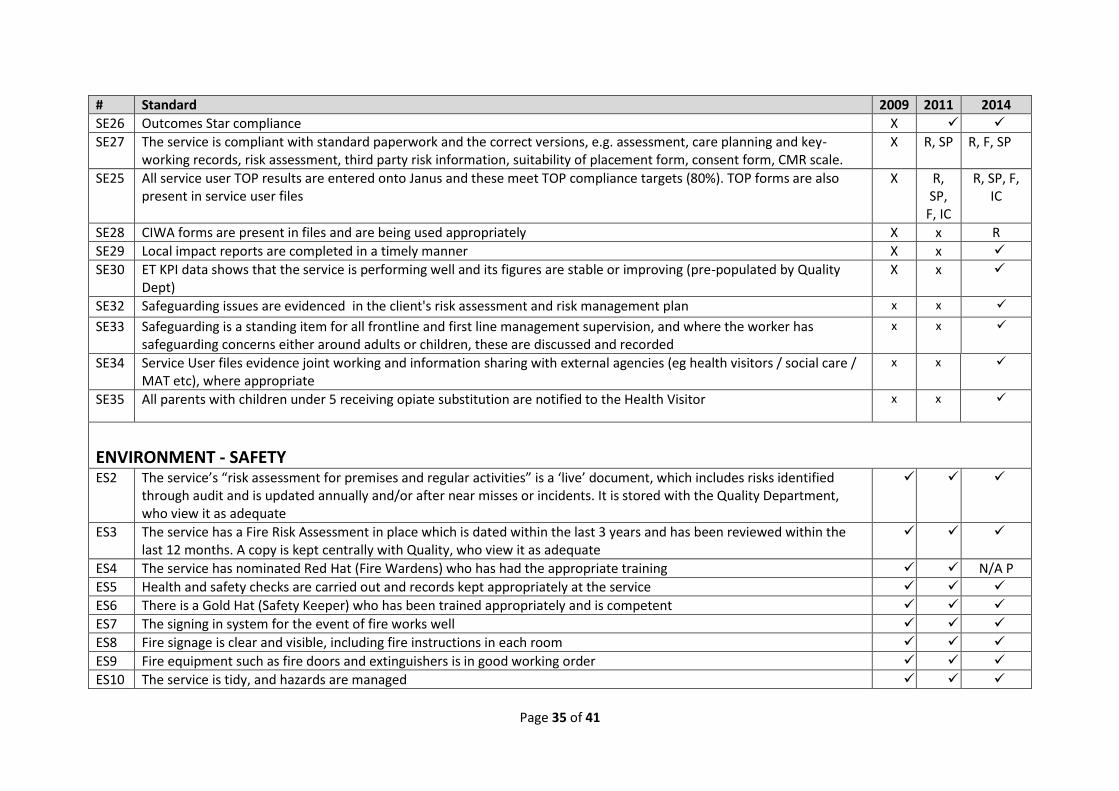
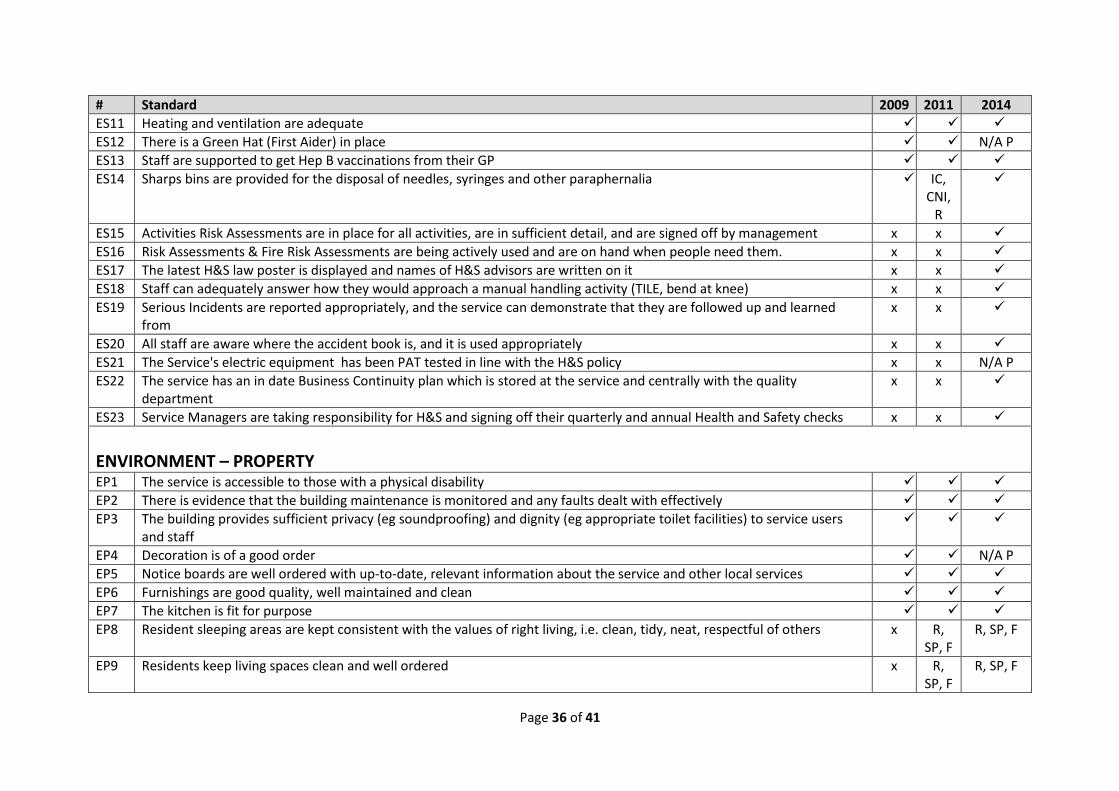
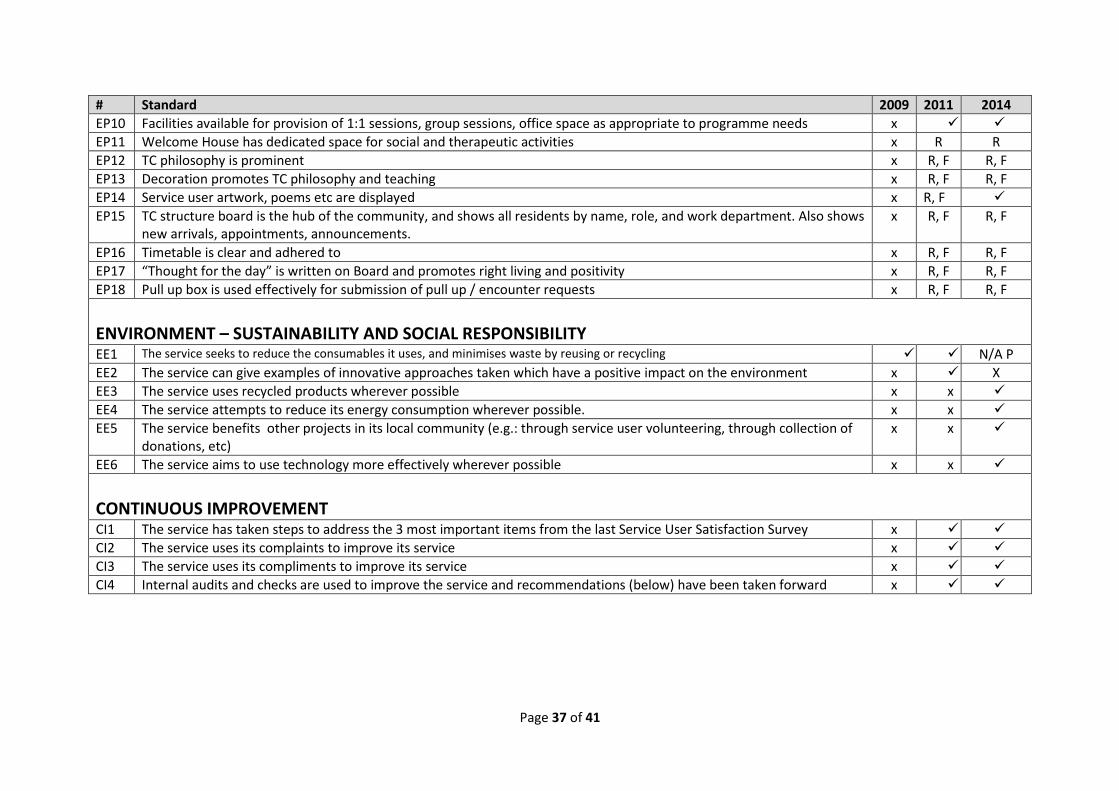
Appendix A - Phoenix Futures Clinical Governance Framework (2014 version)
These standards form our Clinical Governance framework, as set out in our Quality Strategy 2014-17, and are what we audit ourselves against in our annual
Internal Audit cycles. The standards were originally derived from external standards such as CQC, Care Inspectorate [Scotland], Ofsted, HSE, NICE guidelines
etc. They will be indexed to these standards over the course of the 2014-17 Quality Strategy, so we can demonstrate how our standards ensure we measure
and meet external standards.
The aim of this list is to keep a consolidated record of all our Clinical Governance standards and be able to track how they have adapted over time. We have
reviewed them periodically since our Framework was established, and this is indicated in the tables. Reviews of the standards have looked at: regulatory
changes; emergent best practice; how clear the wording is; whether the standards are necessary; whether they represent too much of a burden on services
and auditors; whether they duplicate each other; and how effectively they are being used in the audits themselves. The standards and changes are agreed
by the Clinical Governance Committee.
All standards have a single code which consists of two letters and two numerals. The purpose of this is to enable quick reference and better analysis. The
codes do not necessarily correspond to the order of the standards, as sometimes we have decided to move a standard to a more meaningful section of the
audit. The code is derived from the following Clinical Governance structure, where Governance, Service Users, Environment, and Continuous Improvement
are the four main themes, and beneath these are groups of standards:
Theme Governance Service Users Environment
Continuous
Improvement
Policy Staff Stakeholders Outcomes Experience Harm Reduction
and Infection
Control
Evidence Safety Property Sustainability
and Social
Responsibility
Code
letters
GP GS GE SO SX SH SE ES EP EE CI
The main table below shows the standards and which years they have been present in our framework. Here are three examples:
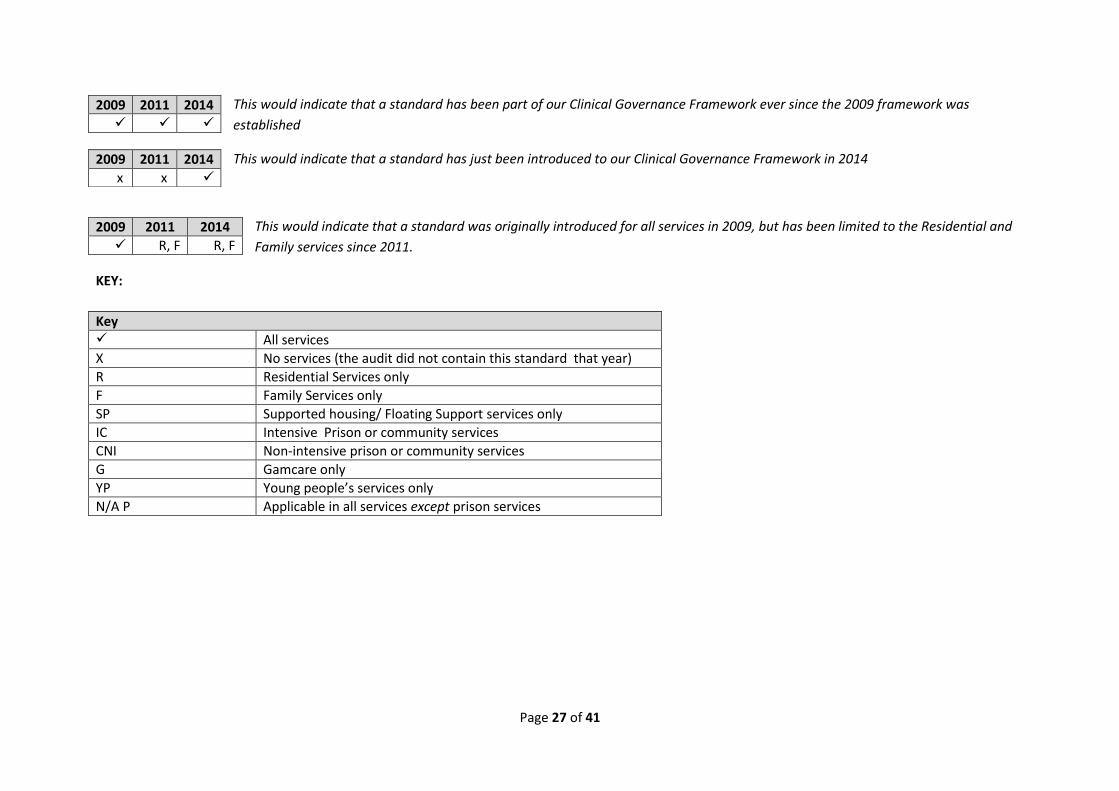
Page 27 of 41
This would indicate that a standard has been part of our Clinical Governance Framework ever since the 2009 framework was
established
This would indicate that a standard has just been introduced to our Clinical Governance Framework in 2014
This would indicate that a standard was originally introduced for all services in 2009, but has been limited to the Residential and
Family services since 2011.
KEY:
2009 2011 2014
2009 2011 2014
x x
2009 2011 2014
R, F R, F
Key All services
X No services (the audit did not contain this standard that year)
R Residential Services only
F Family Services only
SP Supported housing/ Floating Support services only
IC Intensive Prison or community services
CNI Non-intensive prison or community services
G Gamcare only
YP Young people’s services only
N/A P Applicable in all services except prison services

Page 28 of 41
# Standard 2009 2011 2014
GOVERNANCE – POLICY GP1 Staff know where to find policy and procedures and are made aware when these have been updated
GP58 The Service has a corporate policy folder which is up-to-date (see schedule issued by Quality department for latest versions)
x x
GP2 Volunteers and agency staff receive the same information as in GP1
GP3 The 'Our Promise' poster [Service User Charter] is prominent and staff can outline at least 3 of the principles
GP4 Staff can describe the Adult or Child Protection procedure x
GS2 Staff can describe what professional boundaries are and why they are important
GP5 Staff can describe how they work within the Data Protection & Confidentiality policy x
GP7 The service operates to the Confidentiality and Data Protection Policy especially in terms of file retention, archiving, and destruction
GP60 Computers are not left unlocked when staff leave their desks x x
GP61 Service Users are not able to gain access to staff areas independently x x
GP62 Confidential data (including client names and details) is tidied away and not within sight of Service Users (e.g.: on desks) x x
GP8 There are suitable lone working procedures in place locally to complement the overall policy
GP9 Staff show service users ways to make a Compliment or Complaint locally and corporately
GP10 The service has a local protocol known by staff which sets out emergency numbers
ES1 The service ensures that no drugs or alcohol are brought, used or supplied on the premises
GP15 Sanctions and privileges are proportionately linked to behaviour and can demonstrate a learning experience x R
GP16 The programme is delivered in accordance with the manual/ model x R, F, SP, CI
R, F, SP, CI
GP17 Activities are planned as a core part of the programme and are fun for service users; and service users are involved in planning them
x R, F, SP, CI
GP18 The Service involves Service Users in delivering and promoting the Service x
GP19 The service is focussed on education opportunities and helping service users with their employability x
GP20 The service can demonstrate innovative ways of involving service users in promoting services x x
GP21 The service can demonstrate innovative ways of involving service users in consultation x x
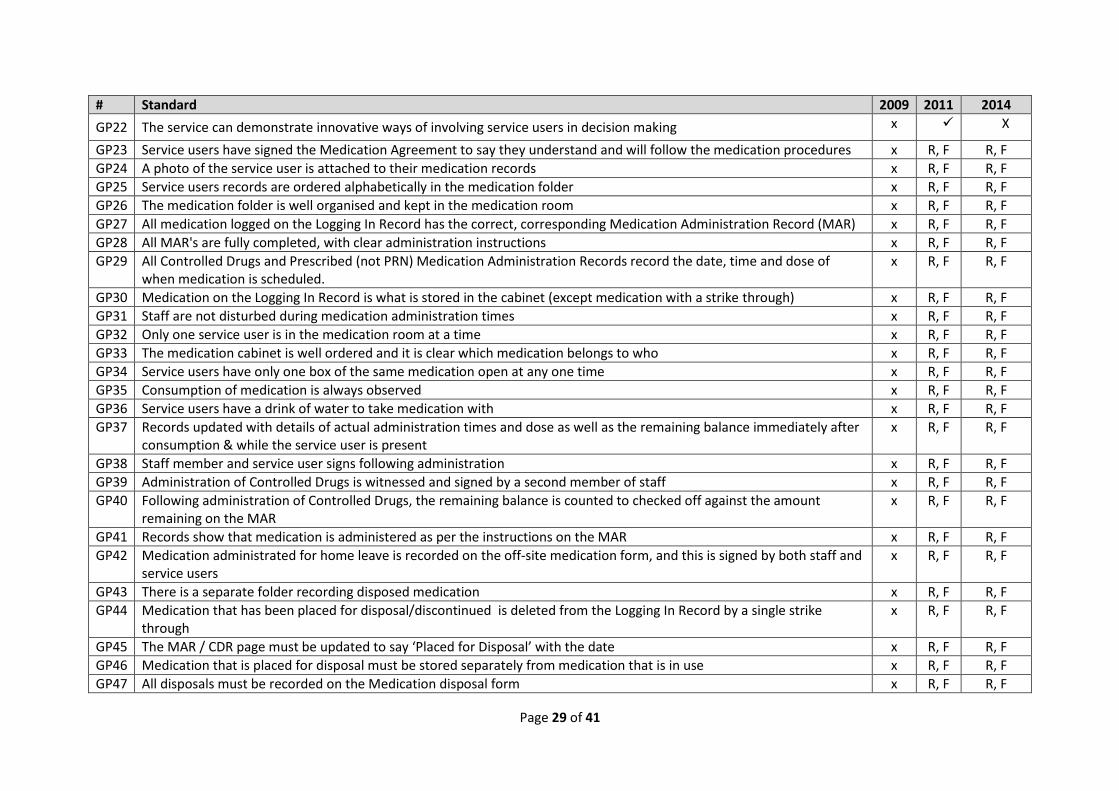
Page 29 of 41
# Standard 2009 2011 2014
GP22 The service can demonstrate innovative ways of involving service users in decision making x X
GP23 Service users have signed the Medication Agreement to say they understand and will follow the medication procedures x R, F R, F
GP24 A photo of the service user is attached to their medication records x R, F R, F
GP25 Service users records are ordered alphabetically in the medication folder x R, F R, F
GP26 The medication folder is well organised and kept in the medication room x R, F R, F
GP27 All medication logged on the Logging In Record has the correct, corresponding Medication Administration Record (MAR) x R, F R, F
GP28 All MAR's are fully completed, with clear administration instructions x R, F R, F
GP29 All Controlled Drugs and Prescribed (not PRN) Medication Administration Records record the date, time and dose of when medication is scheduled.
x R, F R, F
GP30 Medication on the Logging In Record is what is stored in the cabinet (except medication with a strike through) x R, F R, F
GP31 Staff are not disturbed during medication administration times x R, F R, F
GP32 Only one service user is in the medication room at a time x R, F R, F
GP33 The medication cabinet is well ordered and it is clear which medication belongs to who x R, F R, F
GP34 Service users have only one box of the same medication open at any one time x R, F R, F
GP35 Consumption of medication is always observed x R, F R, F
GP36 Service users have a drink of water to take medication with x R, F R, F
GP37 Records updated with details of actual administration times and dose as well as the remaining balance immediately after consumption & while the service user is present
x R, F R, F
GP38 Staff member and service user signs following administration x R, F R, F
GP39 Administration of Controlled Drugs is witnessed and signed by a second member of staff x R, F R, F
GP40 Following administration of Controlled Drugs, the remaining balance is counted to checked off against the amount remaining on the MAR
x R, F R, F
GP41 Records show that medication is administered as per the instructions on the MAR x R, F R, F
GP42 Medication administrated for home leave is recorded on the off-site medication form, and this is signed by both staff and service users
x R, F R, F
GP43 There is a separate folder recording disposed medication x R, F R, F
GP44 Medication that has been placed for disposal/discontinued is deleted from the Logging In Record by a single strike through
x R, F R, F
GP45 The MAR / CDR page must be updated to say ‘Placed for Disposal’ with the date x R, F R, F
GP46 Medication that is placed for disposal must be stored separately from medication that is in use x R, F R, F
GP47 All disposals must be recorded on the Medication disposal form x R, F R, F
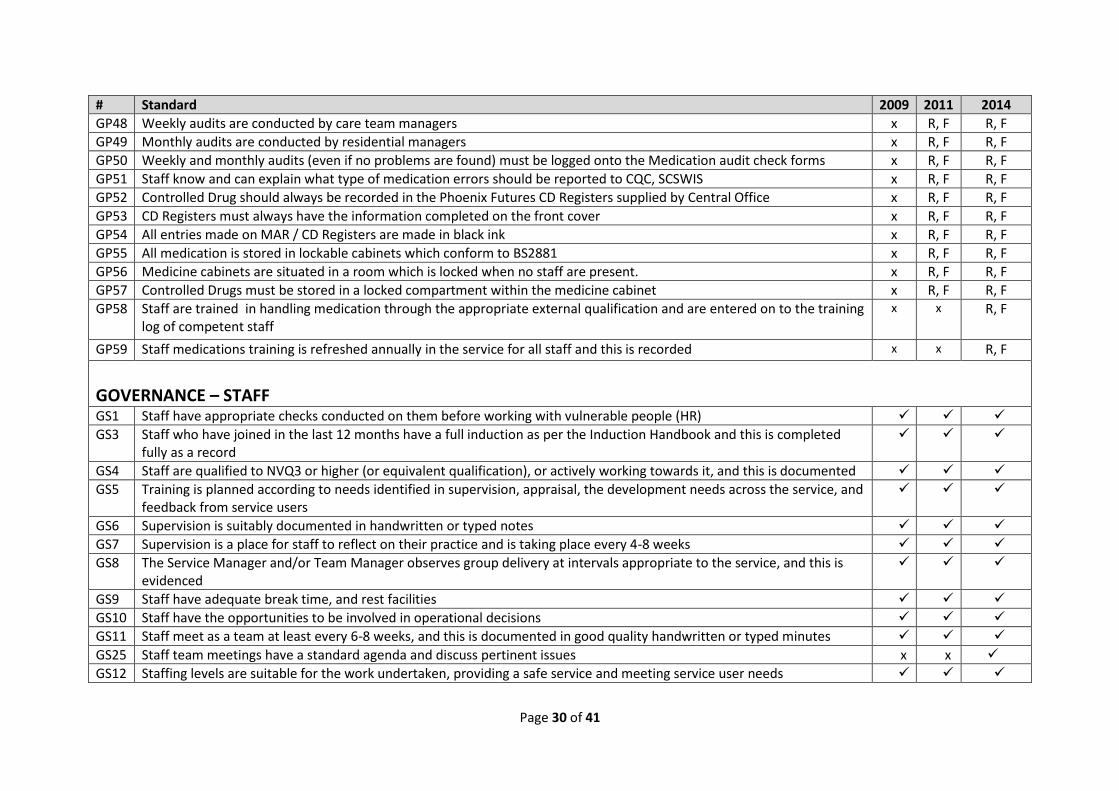
Page 30 of 41
# Standard 2009 2011 2014
GP48 Weekly audits are conducted by care team managers x R, F R, F
GP49 Monthly audits are conducted by residential managers x R, F R, F
GP50 Weekly and monthly audits (even if no problems are found) must be logged onto the Medication audit check forms x R, F R, F
GP51 Staff know and can explain what type of medication errors should be reported to CQC, SCSWIS x R, F R, F
GP52 Controlled Drug should always be recorded in the Phoenix Futures CD Registers supplied by Central Office x R, F R, F
GP53 CD Registers must always have the information completed on the front cover x R, F R, F
GP54 All entries made on MAR / CD Registers are made in black ink x R, F R, F
GP55 All medication is stored in lockable cabinets which conform to BS2881 x R, F R, F
GP56 Medicine cabinets are situated in a room which is locked when no staff are present. x R, F R, F
GP57 Controlled Drugs must be stored in a locked compartment within the medicine cabinet x R, F R, F
GP58 Staff are trained in handling medication through the appropriate external qualification and are entered on to the training log of competent staff
x x R, F
GP59 Staff medications training is refreshed annually in the service for all staff and this is recorded x x R, F
GOVERNANCE – STAFF GS1 Staff have appropriate checks conducted on them before working with vulnerable people (HR)
GS3 Staff who have joined in the last 12 months have a full induction as per the Induction Handbook and this is completed fully as a record
GS4 Staff are qualified to NVQ3 or higher (or equivalent qualification), or actively working towards it, and this is documented
GS5 Training is planned according to needs identified in supervision, appraisal, the development needs across the service, and feedback from service users
GS6 Supervision is suitably documented in handwritten or typed notes
GS7 Supervision is a place for staff to reflect on their practice and is taking place every 4-8 weeks
GS8 The Service Manager and/or Team Manager observes group delivery at intervals appropriate to the service, and this is evidenced
GS9 Staff have adequate break time, and rest facilities
GS10 Staff have the opportunities to be involved in operational decisions
GS11 Staff meet as a team at least every 6-8 weeks, and this is documented in good quality handwritten or typed minutes
GS25 Staff team meetings have a standard agenda and discuss pertinent issues x x
GS12 Staffing levels are suitable for the work undertaken, providing a safe service and meeting service user needs

Page 31 of 41
# Standard 2009 2011 2014
GS13 Staff are offered Hep B vaccinations
GS14 Staff were involved in the self-assessment process of the audit x
GS15 Staff know who their Gold Hat is in their service, and their White Hat where appropriate too x
GS16 Staff know who their regional and local E&D representatives are?
x x
GS17 Staff know who their Saturn and Titans (regional and local Janus reps) are?
x x
GS18 Staff know how to report serious incidents and accidents internally x
GS19 Staff are visible in the service, not hidden in offices x
GS20 Staff and volunteers are clearly differentiated from service users in all services through lanyards and/or name badges, and also where possible through a staff photo board
GS21 Management shows clear and consistent leadership and vision for where the service is going
GS22 Staff have received the necessary training from the local safeguarding children board x x
GS23 The service has made referrals appropriately into the local safeguarding teams for adults or children X x
GS24 Volunteers have a comprehensive local induction
GOVERNANCE – STAKEHOLDERS
GE2 The service completes its returns and notifications for its regulator(s) e.g. Care Inspectorate, CQC
GE3 Where a regulator makes requirements or recommendations, these are done within the requisite timescale
GE4 The service tries to build positive relationships with its immediate neighbours
GE5 The service works well in partnership with other agencies, and this is documented in client case notes etc
GE6 The service provides referrers with information so that they make appropriate referrals
GE8 The service works within the multi-agency local safeguarding arrangements for adults and children to ensure protection from abuse
GE9 The data submitted to NDTMS (England) or SDMD (Scotland) is relevant, timely, complete and accurate
GE12 The service maintains effective relations with support services and other Phoenix Futures services
GE17 Staff members have been given the opportunity to visit other Phoenix Futures Services x x
GE13 The service promotes the organisation as appropriate
GE14 Care Managers and other professionals are invited to care plan reviews x R, F
GE15 Families and significant others are invited to care plan reviews x R, F
GE18 Letters are sent to the family of each resident upon admission x x R, F

Page 32 of 41
# Standard 2009 2011 2014
GE16 Managers should know the types of incidents that must be reported to CQC/Care Inspectorate, and can cite a couple x R, F R, F
GE19 Recent regulatory visits and results have been positive and the service is compliant with regulatory standards x x R, F
SERVICE USERS – OUTCOMES SO1 Service users are retained in the service for appropriate lengths of time
SO2 There is evidence of success, eg discharge rates, appropriate to the type of service
SO9 TOP shows positive change for service users x R, F, IC
R, F, IC
SO10 Outcomes Star shows positive change for service users x
SO11 Service users have access to local Recovery Networks and are supported to do so by the service x
SO12 The service celebrates the achievements of its service users i.e. certificates for phase/stage completions, annual Graduation ceremonies and My Recovery Day
x R, F, IC
SO13 Janus is used to produce departure reports/progress reports x R, F R, F, IC
SO14 Waiting times are effectively managed and where targets apply these are met. x
SO15 The Service has positive outcomes for Gambling Addiction x x G
SERVICE USERS - EXPERIENCE SX21 Is Phoenix Futures meeting the promises it makes in Our Promise? x
SX23 What do you think about the groups? x
SX24 What do you think about the range of Activities? x
SX25 How often do you have key-works? x
SX26 Do you feel you are involved in planning your care and setting your goals? x
SX27 Have others you would like to involved had input into your care and goals? x
SX28 Do you understand the purpose of the Welcome House? Did it meet this purpose for you? x R
SX29 Are you working towards a qualification, or is there a plan for that to happen x
SX30 Are you being supported to look at options for when you leave here, as appropriate? x
SX31 How are you involved in the running of the service? x
SX32 How are you involved in the recovery of your peers? x
SX33 What involvement did you have in assessing the service as part of the self-assessment process? x

Page 33 of 41
# Standard 2009 2011 2014
SERVICE USERS – HARM REDUCTION & INFECTION CONTROL SH1 Literature is available on reducing harm and risks of overdose
SH2 Packs containing harm reduction information are distributed at important times i.e. to those leaving in planned and unplanned ways
SH3 Harm reduction is addressed within key-working or drop-in/outreach sessions, eg. advice on safer injecting, safer sex advice, sharing needles/syringes, issuing condoms etc
SH4 Harm reduction work is written in support/ care plans
SH5 The service promotes Hep B vaccination for service users
SH6 The service promotes Hep C testing for service users
SH7 Services have a needle stick pack for the disposal of sharps which meets with the requirements set out in the H&S policy x
SH8 Staff who provide care have received suitable and sufficient information, training and supervision in preventing and controlling the risks of infection.
x x
SH9 The service has made a suitable and sufficient assessment of the risks to each service user with respect to prevention and control of infection.
x x
SH10 The cleaning arrangements detail the standards of cleanliness required on each part of the premises and there are scheduled cleans and deep cleans
x x
SH11 The service has adequate provision of suitable hand washing facilities and antimicrobial hand rubs. These are clearly signposted in key areas such as bathrooms and kitchens, and hand washing advice is given eg through posters.
x x
SERVICE USERS - EVIDENCE SE1 Service users have a full assessment of need, including parental responsibility
SE2 Risks to the client and others are identified at assessment which is a separate document/ in its own separate section from the main assessment
SE3 Support / Care plans address the needs and risks identified at assessment
SE4 Service users have a support / care plan in place by the end of their 2nd appointment / 2nd one-to-one
SE5 Support / Care plans have clear goals, timescales, and indicate responsibility for actions
SE6 Support / Care plans are reviewed at an appropriate period
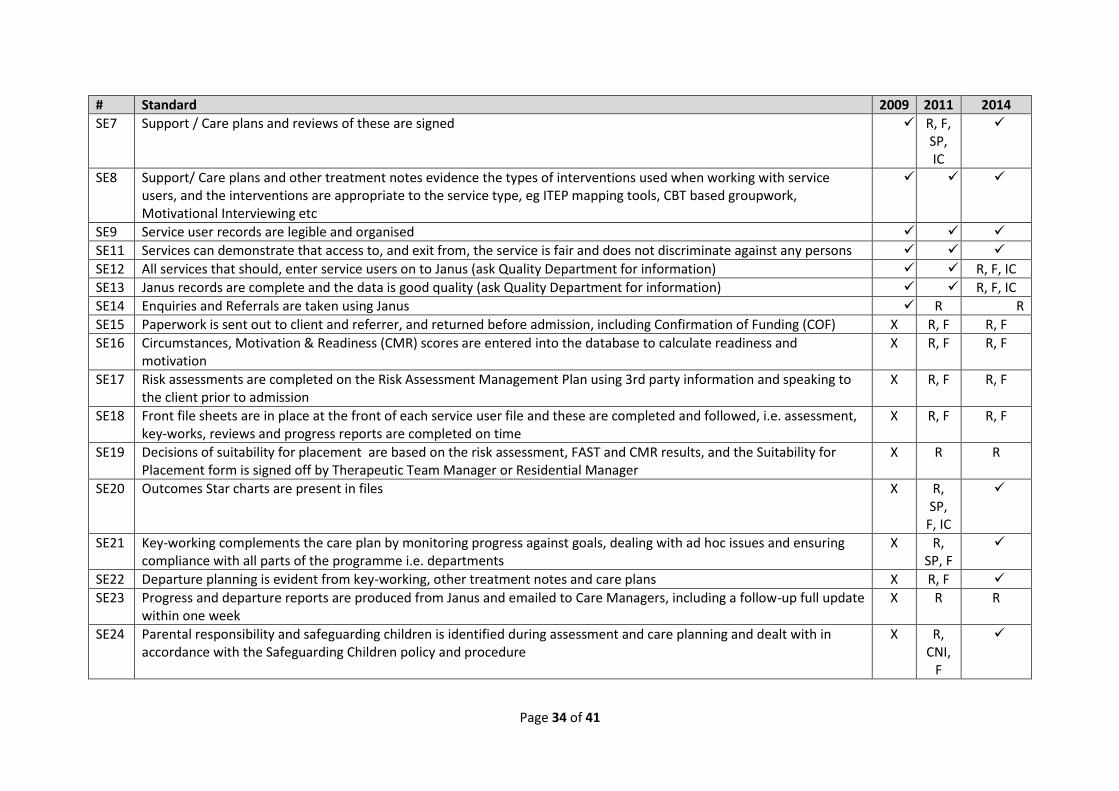
Page 34 of 41
# Standard 2009 2011 2014
SE7 Support / Care plans and reviews of these are signed R, F, SP, IC
SE8 Support/ Care plans and other treatment notes evidence the types of interventions used when working with service users, and the interventions are appropriate to the service type, eg ITEP mapping tools, CBT based groupwork, Motivational Interviewing etc
SE9 Service user records are legible and organised
SE11 Services can demonstrate that access to, and exit from, the service is fair and does not discriminate against any persons
SE12 All services that should, enter service users on to Janus (ask Quality Department for information) R, F, IC
SE13 Janus records are complete and the data is good quality (ask Quality Department for information) R, F, IC
SE14 Enquiries and Referrals are taken using Janus R R
SE15 Paperwork is sent out to client and referrer, and returned before admission, including Confirmation of Funding (COF) X R, F R, F
SE16 Circumstances, Motivation & Readiness (CMR) scores are entered into the database to calculate readiness and motivation
X R, F R, F
SE17 Risk assessments are completed on the Risk Assessment Management Plan using 3rd party information and speaking to the client prior to admission
X R, F R, F
SE18 Front file sheets are in place at the front of each service user file and these are completed and followed, i.e. assessment, key-works, reviews and progress reports are completed on time
X R, F R, F
SE19 Decisions of suitability for placement are based on the risk assessment, FAST and CMR results, and the Suitability for Placement form is signed off by Therapeutic Team Manager or Residential Manager
X R R
SE20 Outcomes Star charts are present in files X R, SP,
F, IC
SE21 Key-working complements the care plan by monitoring progress against goals, dealing with ad hoc issues and ensuring compliance with all parts of the programme i.e. departments
X R, SP, F
SE22 Departure planning is evident from key-working, other treatment notes and care plans X R, F
SE23 Progress and departure reports are produced from Janus and emailed to Care Managers, including a follow-up full update within one week
X R R
SE24 Parental responsibility and safeguarding children is identified during assessment and care planning and dealt with in accordance with the Safeguarding Children policy and procedure
X R, CNI,
F
Page 35 of 41
# Standard 2009 2011 2014
SE26 Outcomes Star compliance X
SE27 The service is compliant with standard paperwork and the correct versions, e.g. assessment, care planning and key-working records, risk assessment, third party risk information, suitability of placement form, consent form, CMR scale.
X R, SP R, F, SP
SE25 All service user TOP results are entered onto Janus and these meet TOP compliance targets (80%). TOP forms are also present in service user files
X R, SP,
F, IC
R, SP, F, IC
SE28 CIWA forms are present in files and are being used appropriately X x R
SE29 Local impact reports are completed in a timely manner X x
SE30 ET KPI data shows that the service is performing well and its figures are stable or improving (pre-populated by Quality Dept)
X x
SE32 Safeguarding issues are evidenced in the client's risk assessment and risk management plan x x
SE33 Safeguarding is a standing item for all frontline and first line management supervision, and where the worker has safeguarding concerns either around adults or children, these are discussed and recorded
x x
SE34 Service User files evidence joint working and information sharing with external agencies (eg health visitors / social care / MAT etc), where appropriate
x x
SE35 All parents with children under 5 receiving opiate substitution are notified to the Health Visitor x x
ENVIRONMENT - SAFETY ES2 The service’s “risk assessment for premises and regular activities” is a ‘live’ document, which includes risks identified
through audit and is updated annually and/or after near misses or incidents. It is stored with the Quality Department, who view it as adequate
ES3 The service has a Fire Risk Assessment in place which is dated within the last 3 years and has been reviewed within the last 12 months. A copy is kept centrally with Quality, who view it as adequate
ES4 The service has nominated Red Hat (Fire Wardens) who has had the appropriate training N/A P
ES5 Health and safety checks are carried out and records kept appropriately at the service
ES6 There is a Gold Hat (Safety Keeper) who has been trained appropriately and is competent
ES7 The signing in system for the event of fire works well
ES8 Fire signage is clear and visible, including fire instructions in each room
ES9 Fire equipment such as fire doors and extinguishers is in good working order
ES10 The service is tidy, and hazards are managed
Page 36 of 41
# Standard 2009 2011 2014
ES11 Heating and ventilation are adequate
ES12 There is a Green Hat (First Aider) in place N/A P
ES13 Staff are supported to get Hep B vaccinations from their GP
ES14 Sharps bins are provided for the disposal of needles, syringes and other paraphernalia IC, CNI,
R
ES15 Activities Risk Assessments are in place for all activities, are in sufficient detail, and are signed off by management x x
ES16 Risk Assessments & Fire Risk Assessments are being actively used and are on hand when people need them. x x
ES17 The latest H&S law poster is displayed and names of H&S advisors are written on it x x
ES18 Staff can adequately answer how they would approach a manual handling activity (TILE, bend at knee) x x
ES19 Serious Incidents are reported appropriately, and the service can demonstrate that they are followed up and learned from
x x
ES20 All staff are aware where the accident book is, and it is used appropriately x x
ES21 The Service's electric equipment has been PAT tested in line with the H&S policy x x N/A P
ES22 The service has an in date Business Continuity plan which is stored at the service and centrally with the quality department
x x
ES23 Service Managers are taking responsibility for H&S and signing off their quarterly and annual Health and Safety checks x x
ENVIRONMENT – PROPERTY EP1 The service is accessible to those with a physical disability
EP2 There is evidence that the building maintenance is monitored and any faults dealt with effectively
EP3 The building provides sufficient privacy (eg soundproofing) and dignity (eg appropriate toilet facilities) to service users and staff
EP4 Decoration is of a good order N/A P
EP5 Notice boards are well ordered with up-to-date, relevant information about the service and other local services
EP6 Furnishings are good quality, well maintained and clean
EP7 The kitchen is fit for purpose
EP8 Resident sleeping areas are kept consistent with the values of right living, i.e. clean, tidy, neat, respectful of others x R, SP, F
R, SP, F
EP9 Residents keep living spaces clean and well ordered x R, SP, F
R, SP, F
Page 37 of 41
# Standard 2009 2011 2014
EP10 Facilities available for provision of 1:1 sessions, group sessions, office space as appropriate to programme needs x
EP11 Welcome House has dedicated space for social and therapeutic activities x R R
EP12 TC philosophy is prominent x R, F R, F
EP13 Decoration promotes TC philosophy and teaching x R, F R, F
EP14 Service user artwork, poems etc are displayed x R, F
EP15 TC structure board is the hub of the community, and shows all residents by name, role, and work department. Also shows new arrivals, appointments, announcements.
x R, F R, F
EP16 Timetable is clear and adhered to x R, F R, F
EP17 “Thought for the day” is written on Board and promotes right living and positivity x R, F R, F
EP18 Pull up box is used effectively for submission of pull up / encounter requests x R, F R, F
ENVIRONMENT – SUSTAINABILITY AND SOCIAL RESPONSIBILITY EE1 The service seeks to reduce the consumables it uses, and minimises waste by reusing or recycling N/A P
EE2 The service can give examples of innovative approaches taken which have a positive impact on the environment x X
EE3 The service uses recycled products wherever possible x x
EE4 The service attempts to reduce its energy consumption wherever possible. x x
EE5 The service benefits other projects in its local community (e.g.: through service user volunteering, through collection of donations, etc)
x x
EE6 The service aims to use technology more effectively wherever possible x x
CONTINUOUS IMPROVEMENT CI1 The service has taken steps to address the 3 most important items from the last Service User Satisfaction Survey x
CI2 The service uses its complaints to improve its service x
CI3 The service uses its compliments to improve its service x
CI4 Internal audits and checks are used to improve the service and recommendations (below) have been taken forward x

Page 38 of 41
Note
Some standards have further guidance points in order to interpret them, and this is made available to managers and auditors.
Summary of changes for 2014 version:
Added Changed Removed Number of standards proposed in 2014 version (after all additions, removals and changes)
Governance – Policy 6 6 4 56
Governance – Staff 4 3 2 22
Governance – Stakeholders 2 2 1 14
Service Users – Outcomes 1 0 0 9
Service Users – Experience 0 2 0 12
Service Users – Harm Reduction and Infection Control
4 2 0 11
Service Users – Evidence 7 1 0 33
Environment – Safety 9 2 0 22
Environment – Property 0 1 0 18
Environment – Sustainability and Social Responsibility
4 0 1 5
Continuous Improvement 0 0 0 4
TOTAL 37 19 8 206
The total number of standards is 206; however, not all of these apply to every service. The service type which has the most standards is Residential.
The net effect of the changes is 29 more standards in the 2014 version. However, not all of these apply to every service.
Page 39 of 41
Appendix B - Our approach to Integrated Governance
Principles of integrated governance
Phoenix Futures adopts the following principles in order to maintain and demonstrate integration of
our governance arrangements.
1. Entity a. We are one organisation with subsidiaries as agreed by the board b. All subsidiaries will have clearly defined mandates c. We will as a group have signed agreements for all contractual partnerships we enter
into, setting out accountabilities. d. We will as a group not enter into partnerships or arrangements with other bodies, or
form new bodies, which are not legally constituted, aware of their responsibilities, and easy to identify.
2. Accountability a. The Executive Team is formed of 5 Executive Directors and forms the “controlling
mind”: Chief Executive Officer, Director of Finance, Director of Business Development, Director of Resources, and Director of Operations
b. Scotland will be accountable to a committee of the Board and the main Board.
3. Stakeholders a. Phoenix Futures is regulated by the Care Quality Commission, the Care Commission
for Scotland, the Homes and Communities Agency and Ofsted. b. As part of our operation of the EFQM Excellence Model we consider our impact on
society. c. We have a formal Corporate Social Responsibility approach.
4. Governance and management a. Phoenix Futures has a clear Purpose and Values, and these are communicated
through corporate roadshows and literature. Our corporate workplan is developed and agreed by the Board.
b. Information Governance in Phoenix Futures is controlled by a Data Protection Working Group, and the named Caldicott Guardian equivalent (for our non NHS organisation) is the Head of Quality and Performance
c. We will continue to use the NHS Information Governance toolkit and will achieve as a minimum Level 2 on every standard, with an ambition to also reach Level 3 on at least 3 standards by March 2017
d. We commit to producing schedules of performance information to be produced for Operational, Financial, IT, and HR information.
5. The Board and constructive challenge a. Phoenix Futures will adopt the Board etiquette outlined in section 6.5 of the HQIP Good
Governance Handbook

Page 40 of 41
6. Delegation and reservation a. The Board delegates powers to the Audit and Control Committee, Clinical
Governance Committee, and the Remuneration Committee. The areas of responsibility are outlined below for the two main committees.
b. These Committees have the information they need in order to monitor the work of Phoenix Futures
c. The Board oversees a Corporate Workplan and a workplan for the Executive Team, with which all other departmental and individual workplans are aligned.
7. Openness and transparency a. Board members will declare conflicts of interest. b. The Quality and Performance department will seek to make more performance
information available to staff on how their service is performing, except where commercial or service user interest means it should be restricted.
c. Phoenix Futures will be open with the organisations it partners with, by providing information where possible and appropriate, and by developing partnership agreements with them.
8. Board supports a. The Board has an Annual Cycle of business for the Board and its Committees b. The Board has an Annual Board Review in November, and the Chair will at this time
also ensure the Board is aware of its responsibilities, and has the appropriate mix of skills and a culture of constructive challenge.
c. There are clear Serious Incident procedures which escalate certain incidents to the Clinical Governance Committee, and, through the chair of this committee, to the Board.
d. The Whistleblowing procedure is promoted to staff each year e. The Complaints procedure is promoted to service users and stakeholders, and Stage
3 of the procedure is in confidence to the Chief Executive.
9. Knowing the organisation and the market a. We conduct market analysis for the purpose of understanding our position and
potential partnerships.
Page 41 of 41
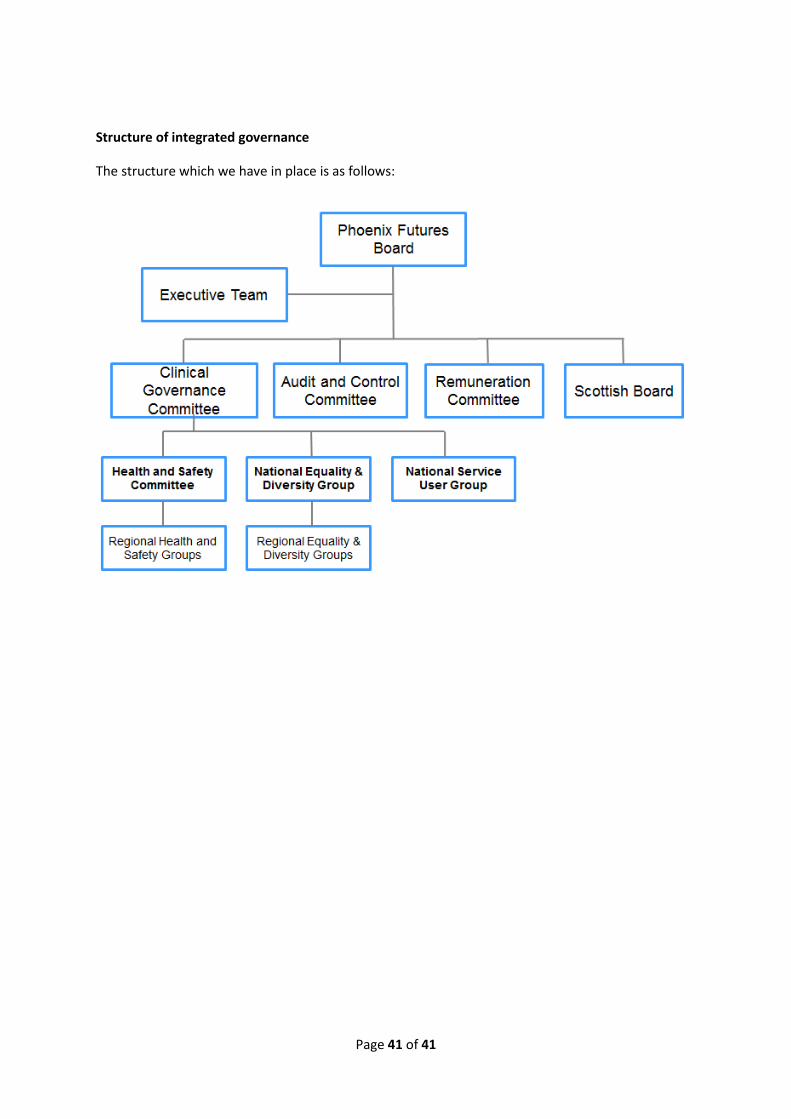
Structure of integrated governance
The structure which we have in place is as follows: