Embed Size (px)
Citation preview
w w w . s c o t l a n d . g o v . u k
QualityStandards for PaediatricAudiologyServices
© Crown copyright 2009
This document is also available on the Scottish Government website:www.scotland.gov.uk
RR Donnelley B60164 04/09
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
Telephone orders and enquiries0131 622 8283 or 0131 622 8258
Fax orders0131 557 8149
Email [email protected]
Quality Standards for Paediatric Audiology Services
Audiology Services Advisory GroupApril 2009

© Crown copyright 2009
ISBN 978-0-7559-1987-1
Scottish GovernmentSt Andrew’s HouseEdinburghEH1 3DG
Produced for the Scottish Government by RR Donnelley B60164
Published by the Scottish Government, April 2009
Executive Summary
In January 2003, the Public Health Institute of Scotland (PHIS) published a Needs Assessment Report on NHS Audiology Services in Scotland. This report identified a number of areas in which both Adult and Paediatric Audiology services were failing to meet the standards expected by service users and other stakeholders. The modernisation of hearing aid services tried to address these areas as well as modernise the patient journey. Scotland began the modernisation of its audiology services in 2003 by investing in new Digital Signal Processing (DSP) hearing aid technology, new infrastructure, information systems and training based around the patient care pathway. However, whilst there was clarity around the patient pathway there was no clarity around appropriate quality standards by which the services could be audited or on which services could base a service improvement plan. One of the recommendations of the PHIS Report was that “NHS Quality Improvement Scotland (QIS) would produce an agreed set of standards for audiology services and conduct an assessment of the service’s ability to meet these standards, taking into account established documents from voluntary bodies and professional organisations.” In its response to this recommendation, NHS QIS indicated that it would not be possible to fulfill this within a timescale that all interested parties could agree to. It was then suggested that the work be undertaken by a sub-group of the Scottish Government’s Audiology Services Advisory Group following the NHS QIS standards development methodology and that NHS QIS would consequently quality assure the development process. This work covered Adult Hearing Rehabilitation Services. Around the same time, a multidisciplinary group of professionals working in Paediatric Audiology from England, Scotland and Wales, under the guidance of MRC Hearing and Communication Group, began developing draft quality standards and an accompanying quality rating tool for Paediatric Audiology, also using the NHS QIS methodology. This final document evolved from that original work. A 6 Paediatric site audit of the modernisation process was carried out by Davis et al 2007, with support from the late Professor Stuart Gatehouse, which used the draft standards to assess services against. In taking that task forward the audit group developed a Quality Rating Tool (QRT) which attempted to directly assess services against those draft standards to establish whether the services
• are responsive to their needs • empower patients to be good partners in meeting those needs • make the best use of staff skills and resources.
The draft standards and QRT have been updated in the light of their use, together with comments from stakeholders.
Contents
1. Quality Standards for Paediatric Audiology
2. Development of the Quality Standards for Paediatric Audiology Services
3. The Quality Standards
4. A Quality Rating Tool for Paediatric Audiology Services
5. Appendices
Acknowledgements We are indebted to the original multidisciplinary working group, with members from England, Wales and Scotland, who initially developed draft Quality Standards for Paediatric Audiology and acknowledge the considerable work that had been undertaken prior to the further development work in Scotland. We would like to thank the original group for giving us their permission to take this piece of work forward in Scotland and are grateful to them for their ongoing support and advice. The membership of the original group was:
Lesley Batchelor Christine Cameron Adrian Davis Martin Evans Jackie Grigor Ann MacKinnon Sally Minchom Liz Orton Tony Sirimanna
Quality Standards for Paediatric Audiology Context
In 2005, a multidisciplinary group of professionals working in Paediatric Audiology
from England, Scotland and Wales, under the guidance of MRC Hearing and
Communication Group, began developing quality standards and an accompanying
quality rating tool (QRT) for Paediatric Audiology using the NHS Quality Improvement
Scotland (QIS) methodology. This, for a number of reasons, was not completed,
although a draft document was produced.
In 2008 the multidisciplinary Paediatric sub-group of the Scottish Audiology Services
Advisory Group (ASAG), using the draft document as a starting point, undertook to
complete this work resulting in the production of this document.
At the same time, discussions were undertaken within the Welsh Assembly
Government to undertake a similar development process for the production of
standards and the audit of paediatric services.
Comments and feedback are welcome on the document.
1.1 Introduction
In January 2003 the Public Health Institute of Scotland published a Needs
Assessment Report on Audiology Services in Scotland. This report identified a
number of areas in which Audiology services were failing to meet the standards
expected by service users and stakeholders. Many of the concerns raised were
applicable to both adult and paediatric services; some were specific to either adults
or paediatrics. Concerns raised included:
• Inadequate facilities at base hospital, peripheral clinics and community sites
• Shortages in qualified staff and appropriately skilled staff leading to compromised
service access and quality
1
• Financial pressures compromising service quality, with an undue emphasis on
activity at the expense of outcome
• Poor inter-agency links
• Large variations in services across NHS Boards
• Inferior service quality and outcomes in comparison to elsewhere in the United
Kingdom and overseas
• Good working practices often not in place. Developments in Audiology services
elsewhere in the United Kingdom largely absent in Scotland
• A lack of well functioning Children’s Hearing Services Working Groups
• A need for audiologists with additional paediatric training and experience to
deliver the audiology care for children
As a result of these findings a number of recommendations were made by the
Audiology Needs Assessment Group. Among these were the recommendations that
“NHS Quality Improvement Scotland (QIS) should produce an agreed set of
standards for audiology services, and conduct an assessment of the services’ ability
to meet these standards, taking into account established documents from voluntary
bodies and professional organisations” and “The Scottish Executive should establish
a formal Audiology Services Advisory Group”.
In response, an Audiology Services Advisory Group was established “to monitor the
development of NHS audiology services in Scotland and to provide appropriate
advice to NHS Boards, the health department and other relevant bodies that will
facilitate effective and efficient development.”
When approached, NHS QIS indicated that it would not be possible to undertake the
work within a timescale that would be acceptable to the Group. It was then suggested
that work be undertaken by a sub-group of the Scottish Government’s Audiology
Services Advisory Group (ASAG), following the NHS QIS standards development
methodology, to write standards for adult hearing rehabilitation services.
2
1.2 NHS QIS Methodology
1.2.1 Basic Principles
Standards developed using the NHS QIS quality assurance process are required to
be clear and measurable, based on appropriate evidence, and written to take into
account other recognised standards and clinical guidelines. The standards are:
• Written in simple language and available in a variety of formats
• Focussed on clinical issues and include non-clinical factors that impact on the
quality of care
• Developed by healthcare professionals and members of the public, and consulted
on widely
• Regularly reviewed and revised to make sure they remain relevant and up to date
• Achievable but stretching
1.2.2 Process The way in which standards are developed is a key element of the quality assurance
process. Project groups working on standards development are expected to
• Adopt an open and inclusive process involving members of the public, voluntary
organisations and health care professionals
• Work within NHS QIS policies and procedures
• Test the measurability of draft standards by undertaking pilot reviews
1.2.3 Format of Standards and Definition of Terminology All standards quality assured using the NHS QIS process follow a similar format:
• Each standard has a title, which summarises the area on which that standard
focuses
• This is followed by the standard statement, which explains what level of
performance needs to be achieved
3
• The rationale section provides the reasons why the standard is considered
important
• The standard statement is expanded in the section headed criteria, which states
exactly what must be achieved for the standard to be reached and how the
service will achieve this. Each criterion is expected to be met wherever a service
is provided. The criteria are numbered for the sole reason of making the
document easier to work with, particularly for the assessment process. The
number of the criteria is not a reflection of priority.
1.2.4 Assessment of Performance Against the Standards Assessment of the performance of Audiology services against the standards will take
place using the attached Quality rating tool. This will include both self assessment by
individual services and external assessment by peers. The Audiology Quality
Improvement sub-group of the Audiology Services Advisory Group will be
responsible for overseeing this assessment procedure.
4
2. Development of the Quality Standards for Paediatric Audiology Services
2.1 Introduction to Paediatric Audiology Services
The prevalence of permanent childhood hearing impairment, greater than 40dBHL in
the better ear, is estimated to be 1.33/1000 live births in children age 5 years and
older, possibly rising to 2.05/1000 live births for children aged 9 years and older. The
yield from newborn hearing screening programmes is approximately 1/1000 live
births.
Childhood conductive hearing impairment is a far commoner condition. It is reported
that approximately 80% of children will have had at least one episode of otitis media
by the age of 3.
It is well documented that permanent childhood hearing impairment can have a
significant negative impact on a child’s communication skills, social integration and
educational progress.
The impact of fluctuating conductive hearing losses on a child’s communication skills
and educational progress are less clear. There is evidence that persistent otitis
media with effusion associated with a mild to moderate hearing loss can have an
adverse effect on early language development and longer term effects on both
behaviour and quality of life.
It is important that children with permanent childhood hearing impairment and
children with persisting or recurring conductive hearing losses are identified early in
order to provide the children and their families with appropriate intervention, support
and advice.
The increasing prevalence of permanent hearing impairment throughout childhood,
and the fluctuating nature of many conductive hearing losses, means that paediatric
audiology services must have the capacity and appropriate skills, not only to identify
and manage children referred from the newborn hearing screen, but also to be able
to offer timely assessments and appropriate management of confirmed permanent or
5
temporary hearing deficits whenever there are concerns raised about a child’s
hearing status.
Paediatric audiology services are generally multidisciplinary and may include:
• audiologists
• scientists
• audiovestibular physicians
• audiological paediatricians
• speech and language therapists
• education staff
• social services and
• voluntary organisations
Across the United Kingdom paediatric audiology services are delivered by many
differing combinations of skill mix. This is historically due to different local service
models, rapid technological progress and emphasis on consumer led, family friendly
services. There are also well recognised difficulties with recruitment and training in
some professional groups, and in some geographical areas. Some audiological skills
are common to all members of the team, but each discipline brings unique skills and
expertise, all of which are necessary if services are to comply with accepted best
practice.
It is important that individual paediatric audiology teams, irrespective of their service
model, aspire to deliver the best possible audiology care for children and their
families. They must also know the minimum acceptable standards of care that
children and their families can expect to receive on their journey through paediatric
audiology services.
2.2 Development and Scope of the Standards
This document covers all aspects of the paediatric audiology services delivered by
health service staff and acknowledges the important role of education, social services
and the voluntary sector within the multidisciplinary team; it aims to establish quality
assurance throughout all aspects of the paediatric audiology process for children and
their families, regardless of where the service is delivered.
6
Development of these Standards in Paediatric Audiology began in 2005 when a
multidisciplinary group of health professionals working in paediatric Audiology, in
partnership with the voluntary sector, met to identify key critical areas for clinical
standards.
The standards are applicable to children of all ages, from birth to school leaving, and
incorporate the audiology services provided at primary, secondary and tertiary level.
They are based on the child and family’s journey as they move through the paediatric
audiology service. For the purposes of this document “parent” is defined as any
person who has parental responsibility.
Paediatric audiology services will regularly self-assess their performance against the
standards using the Quality Rating Tool to help identify any possible areas of
weakness and highlight strengths and areas of good practice within the local
audiology service. In Scotland, overseeing the assessment of performance against
the Standards will be the responsibility of the Audiology Services Advisory Group
with a clearly defined assessment process and cycle.
The standards will be reviewed by ASAG 2 years post-implementation and thereafter
a regular review cycle established. This will take into account ongoing developments
in paediatric audiology and the emergence of new evidence to ensure that they
remain relevant and up to date.
2.3 Context
These standards are designed to improve service quality issues in clinical areas
unique to Audiology within the NHS: elements of service quality such as cleanliness
of facilities or workforce development are outside of the scope of this work as they
are expected to be addressed by local healthcare governance mechanisms and/or
more generic NHS standards.
7
The standards are evidence based and make reference to other recognised
standards, clinical guidelines and best practice documents, which must be
considered alongside these standards. (see appendix 3)
Although the standards apply to NHS Audiology, the hope is that their
implementation will encourage and further develop collaborative working, both with
fellow NHS professionals and external agencies.
In addition, awareness of and compliance with statutory requirements, such as the
Disability Discrimination Act 2005, is assumed, as is awareness and understanding
of consent requirements.
It would be impossible to exhaustively list the many and varied service user groups
who access paediatric Audiology services. It is intended that these standards apply
to all children and families using the service.
8
Standard 1. Accessing the service
Standard Statement
Rationale Criteria
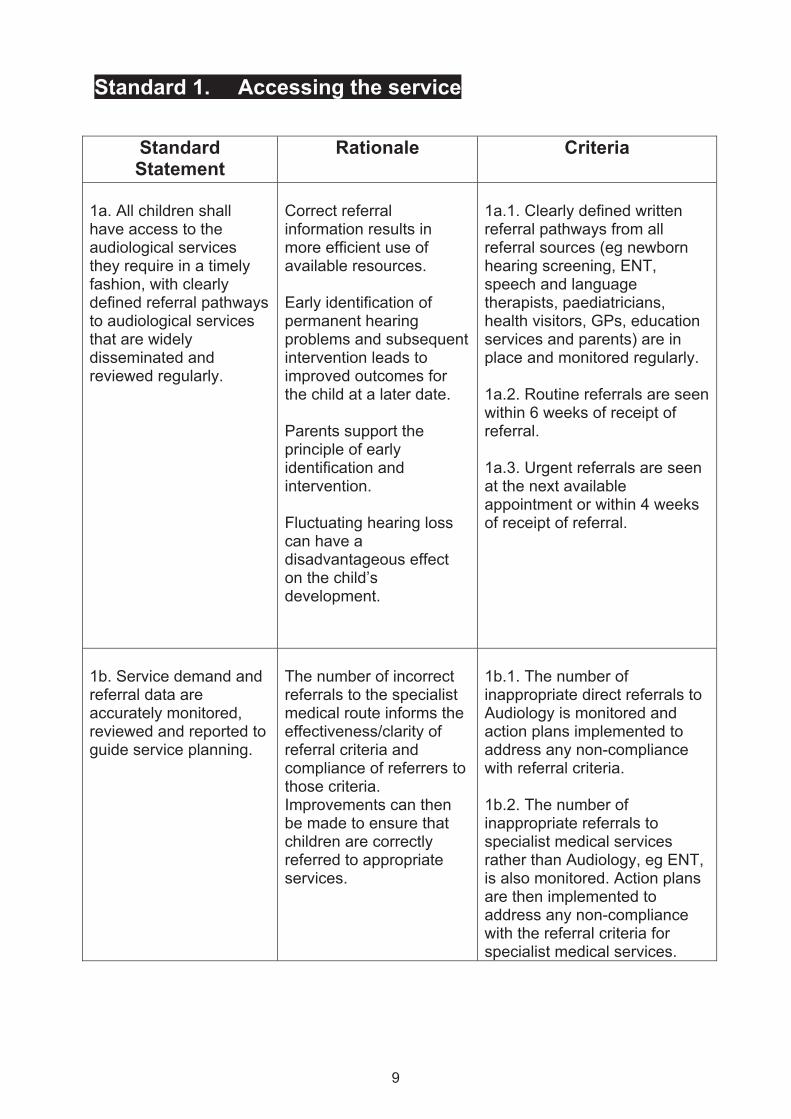
1a. All children shall have access to the audiological services they require in a timely fashion, with clearly defined referral pathways to audiological services that are widely disseminated and reviewed regularly.
Correct referral information results in more efficient use of available resources. Early identification of permanent hearing problems and subsequent intervention leads to improved outcomes for the child at a later date. Parents support the principle of early identification and intervention. Fluctuating hearing loss can have a disadvantageous effect on the child’s development.
1a.1. Clearly defined written referral pathways from all referral sources (eg newborn hearing screening, ENT, speech and language therapists, paediatricians, health visitors, GPs, education services and parents) are in place and monitored regularly. 1a.2. Routine referrals are seen within 6 weeks of receipt of referral. 1a.3. Urgent referrals are seen at the next available appointment or within 4 weeks of receipt of referral.
1b. Service demand and referral data are accurately monitored, reviewed and reported to guide service planning.
The number of incorrect referrals to the specialist medical route informs the effectiveness/clarity of referral criteria and compliance of referrers to those criteria. Improvements can then be made to ensure that children are correctly referred to appropriate services.
1b.1. The number of inappropriate direct referrals to Audiology is monitored and action plans implemented to address any non-compliance with referral criteria. 1b.2. The number of inappropriate referrals to specialist medical services rather than Audiology, eg ENT, is also monitored. Action plans are then implemented to address any non-compliance with the referral criteria for specialist medical services.
9
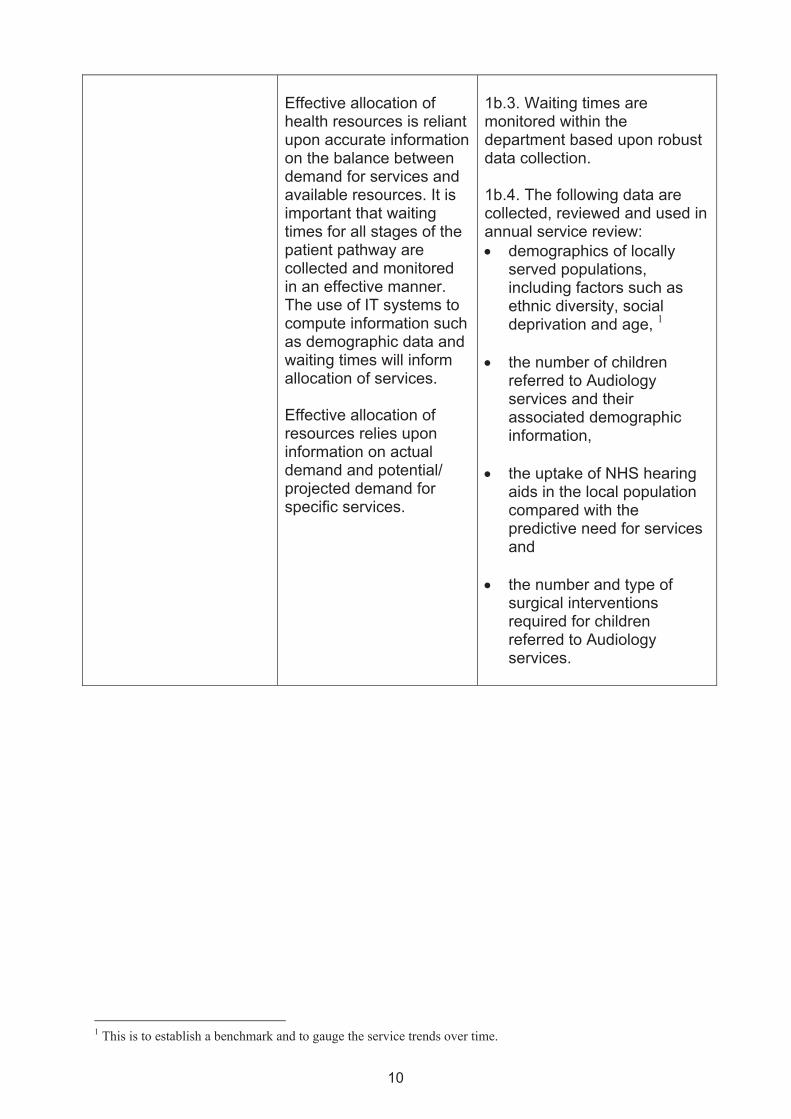
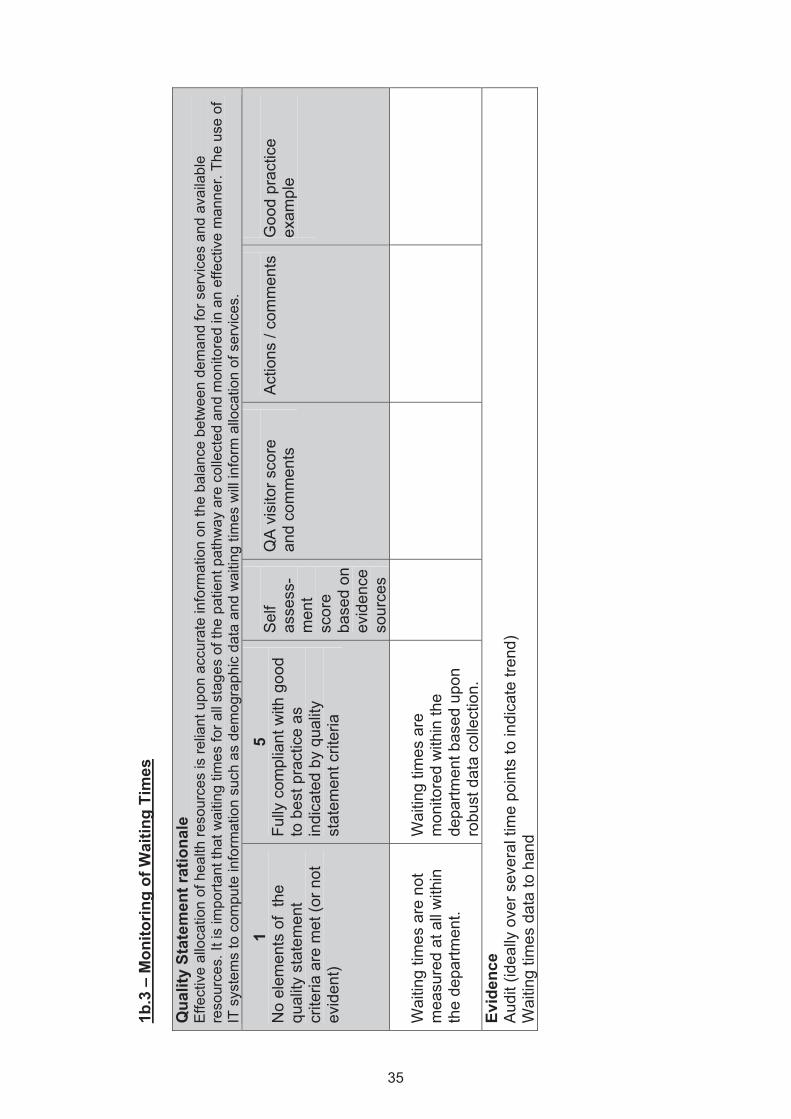
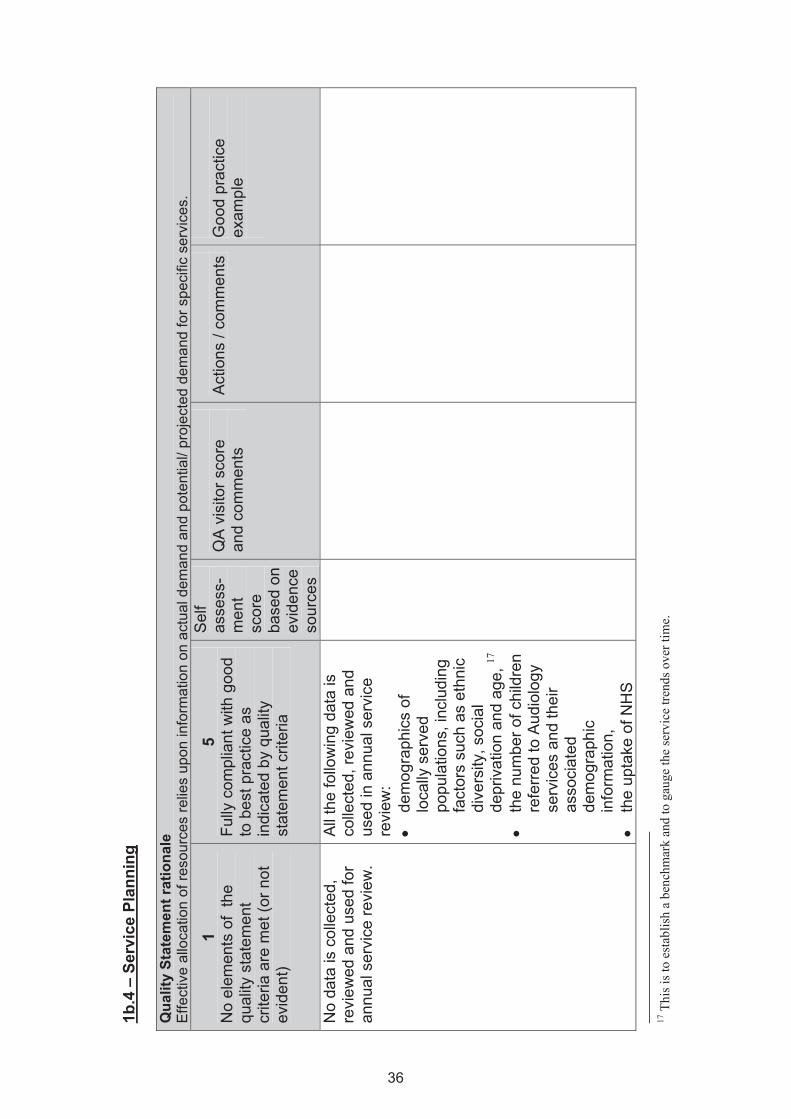
Effective allocation of health resources is reliant upon accurate information on the balance between demand for services and available resources. It is important that waiting times for all stages of the patient pathway are collected and monitored in an effective manner. The use of IT systems to compute information such as demographic data and waiting times will inform allocation of services. Effective allocation of resources relies upon information on actual demand and potential/ projected demand for specific services.
1b.3. Waiting times are monitored within the department based upon robust data collection. 1b.4. The following data are collected, reviewed and used in annual service review: • demographics of locally
served populations, including factors such as ethnic diversity, social deprivation and age, 1
• the number of children
referred to Audiology services and their associated demographic information,
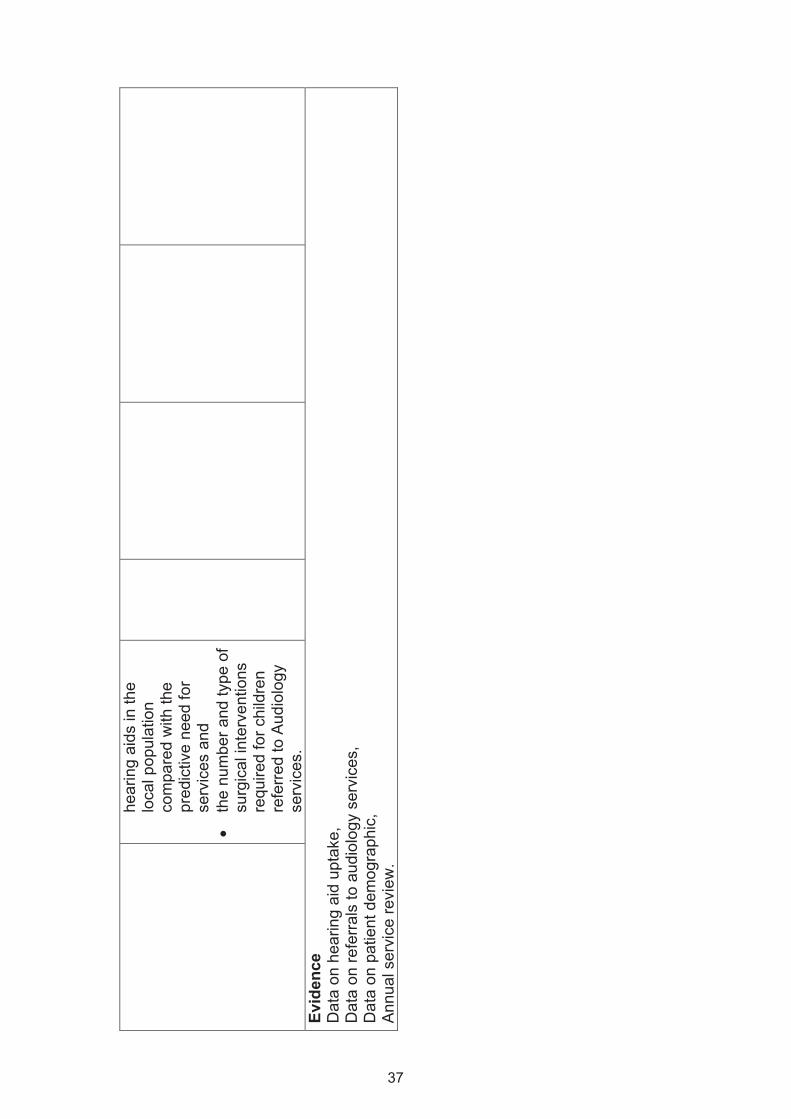
• the uptake of NHS hearing
aids in the local population compared with the predictive need for services and
• the number and type of
surgical interventions required for children referred to Audiology services.
1 This is to establish a benchmark and to gauge the service trends over time.
10
Standard 2 Assessment
Standard Statement
Rationale Criteria
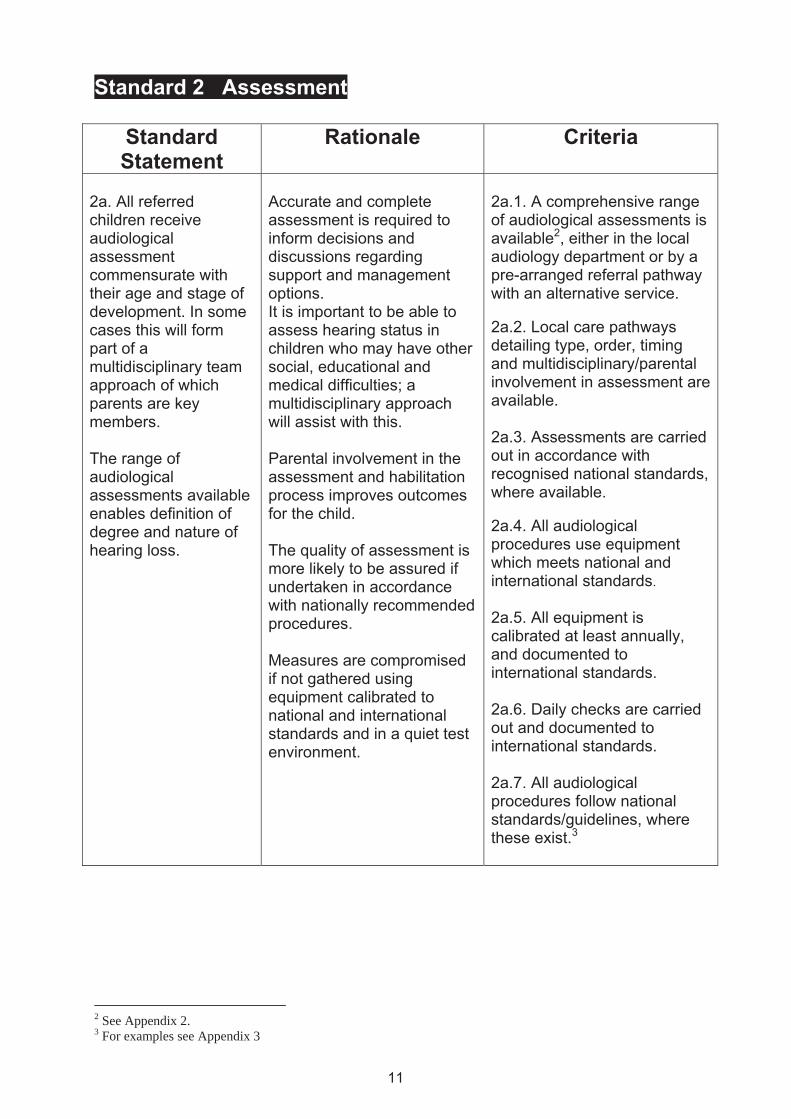
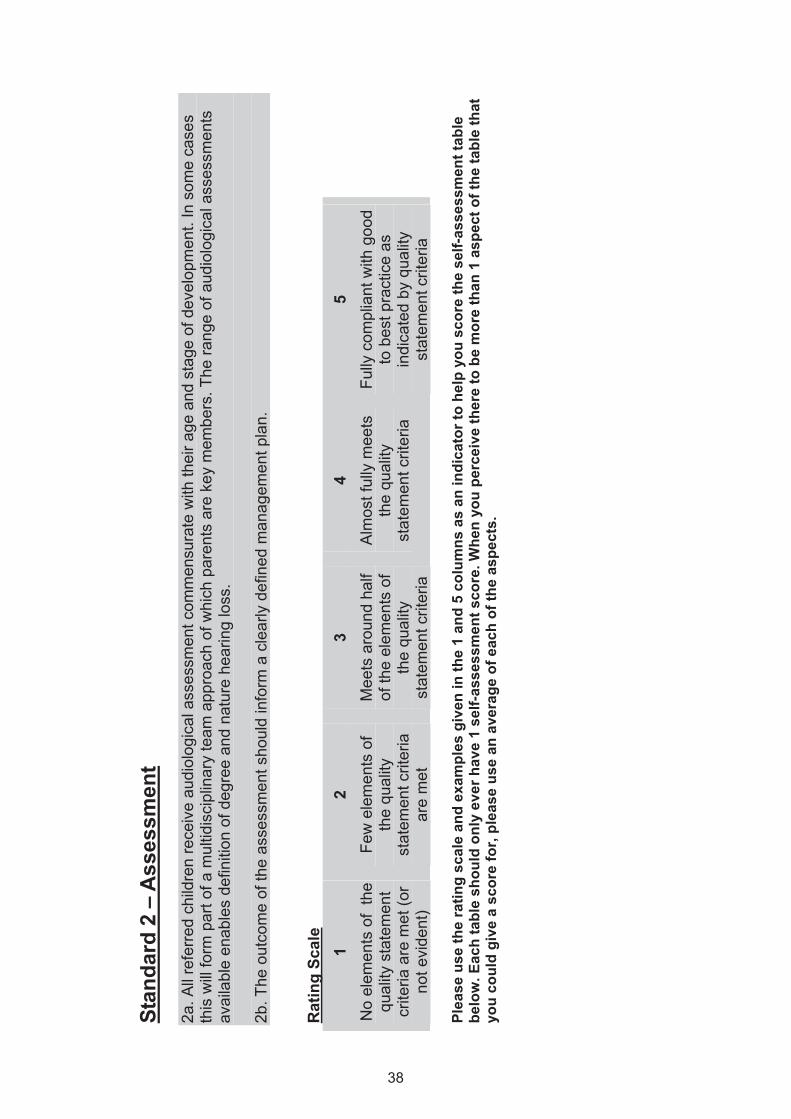
2a. All referred children receive audiological assessment commensurate with their age and stage of development. In some cases this will form part of a multidisciplinary team approach of which parents are key members. The range of audiological assessments available enables definition of degree and nature of hearing loss.
Accurate and complete assessment is required to inform decisions and discussions regarding support and management options. It is important to be able to assess hearing status in children who may have other social, educational and medical difficulties; a multidisciplinary approach will assist with this. Parental involvement in the assessment and habilitation process improves outcomes for the child. The quality of assessment is more likely to be assured if undertaken in accordance with nationally recommended procedures. Measures are compromised if not gathered using equipment calibrated to national and international standards and in a quiet test environment.
2a.1. A comprehensive range of audiological assessments is available2, either in the local audiology department or by a pre-arranged referral pathway with an alternative service. 2a.2. Local care pathways detailing type, order, timing and multidisciplinary/parental involvement in assessment are available. 2a.3. Assessments are carried out in accordance with recognised national standards, where available. 2a.4. All audiological procedures use equipment which meets national and international standards. 2a.5. All equipment is calibrated at least annually, and documented to international standards. 2a.6. Daily checks are carried out and documented to international standards. 2a.7. All audiological procedures follow national standards/guidelines, where these exist.3
11
2 See Appendix 2. 3 For examples see Appendix 3
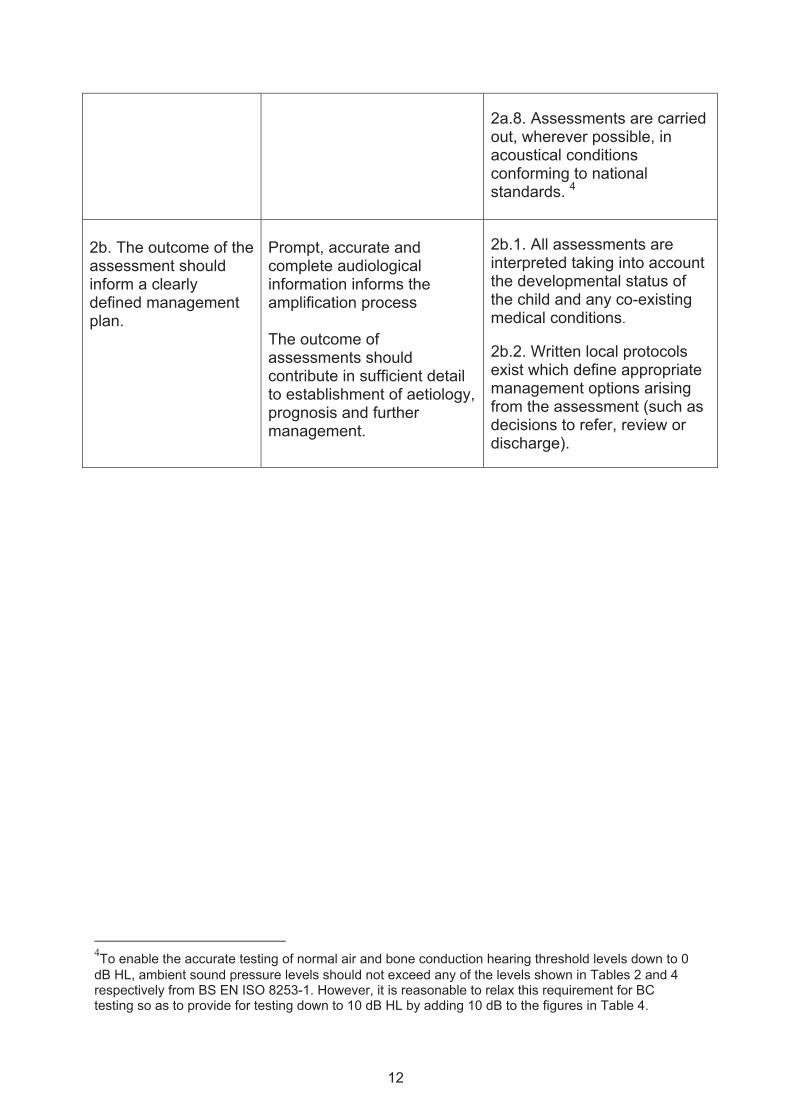
2a.8. Assessments are carried out, wherever possible, in acoustical conditions conforming to national standards. 4
2b. The outcome of the assessment should inform a clearly defined management plan.
Prompt, accurate and complete audiological information informs the amplification process The outcome of assessments should contribute in sufficient detail to establishment of aetiology, prognosis and further management.
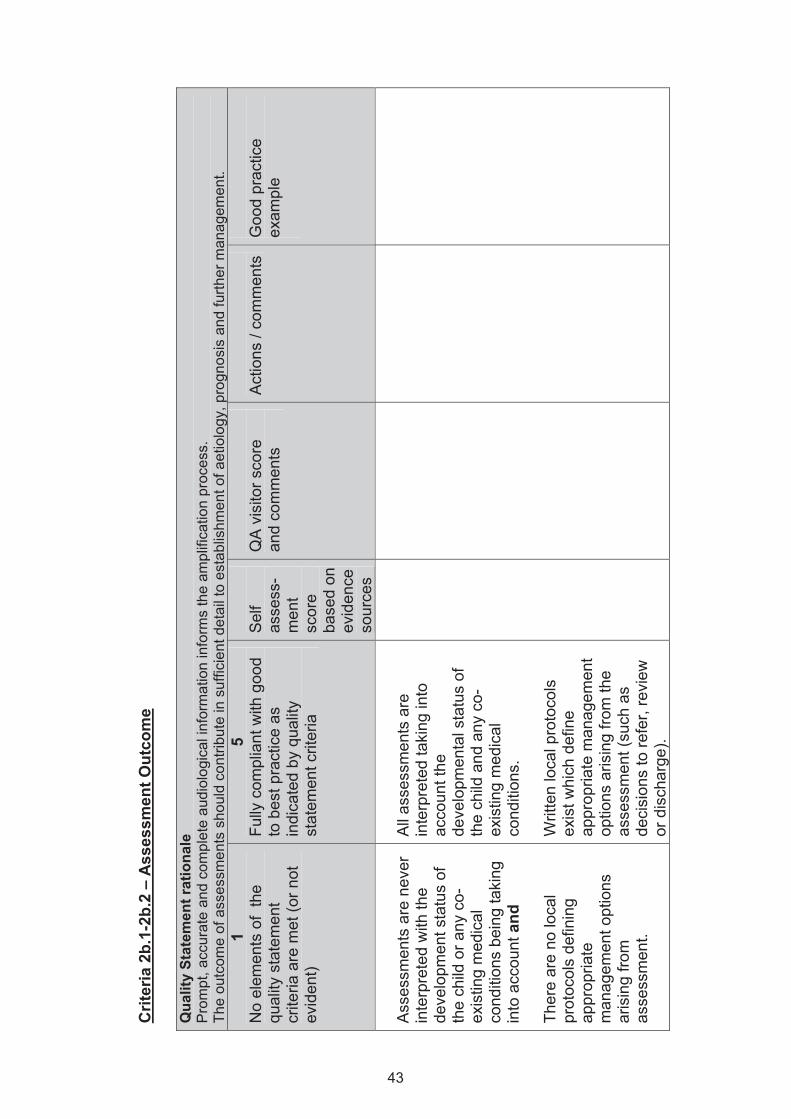
2b.1. All assessments are interpreted taking into account the developmental status of the child and any co-existing medical conditions.
2b.2. Written local protocols exist which define appropriate management options arising from the assessment (such as decisions to refer, review or discharge).
4To enable the accurate testing of normal air and bone conduction hearing threshold levels down to 0 dB HL, ambient sound pressure levels should not exceed any of the levels shown in Tables 2 and 4 respectively from BS EN ISO 8253-1. However, it is reasonable to relax this requirement for BC testing so as to provide for testing down to 10 dB HL by adding 10 dB to the figures in Table 4.
12
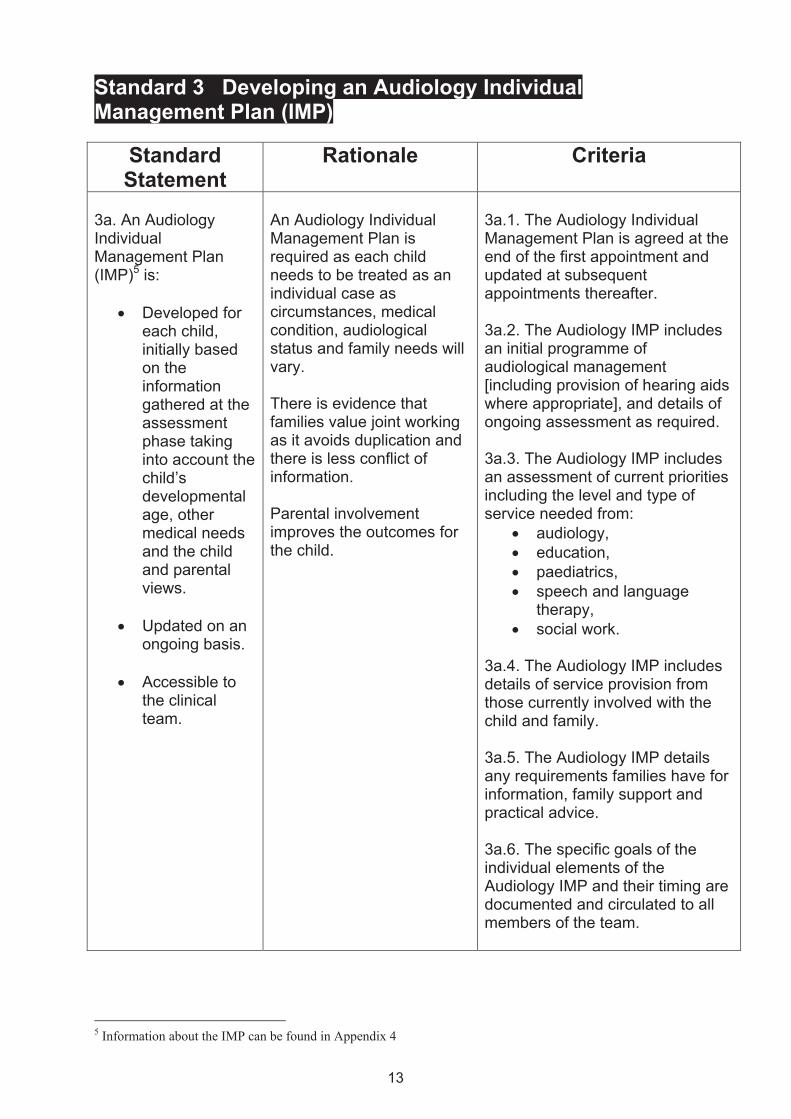
Standard 3 Developing an Audiology Individual Management Plan (IMP)
Standard Statement
Rationale Criteria
3a. An Audiology Individual Management Plan (IMP)5 is:
• Developed for each child, initially based on the information gathered at the assessment phase taking into account the child’s developmental age, other medical needs and the child and parental views.
• Updated on an
ongoing basis.
• Accessible to the clinical team.
An Audiology Individual Management Plan is required as each child needs to be treated as an individual case as circumstances, medical condition, audiological status and family needs will vary. There is evidence that families value joint working as it avoids duplication and there is less conflict of information. Parental involvement improves the outcomes for the child.
3a.1. The Audiology Individual Management Plan is agreed at the end of the first appointment and updated at subsequent appointments thereafter. 3a.2. The Audiology IMP includes an initial programme of audiological management [including provision of hearing aids where appropriate], and details of ongoing assessment as required. 3a.3. The Audiology IMP includes an assessment of current priorities including the level and type of service needed from:
• audiology, • education, • paediatrics, • speech and language
therapy, • social work.
3a.4. The Audiology IMP includes details of service provision from those currently involved with the child and family. 3a.5. The Audiology IMP details any requirements families have for information, family support and practical advice. 3a.6. The specific goals of the individual elements of the Audiology IMP and their timing are documented and circulated to all members of the team.
5 Information about the IMP can be found in Appendix 4
13
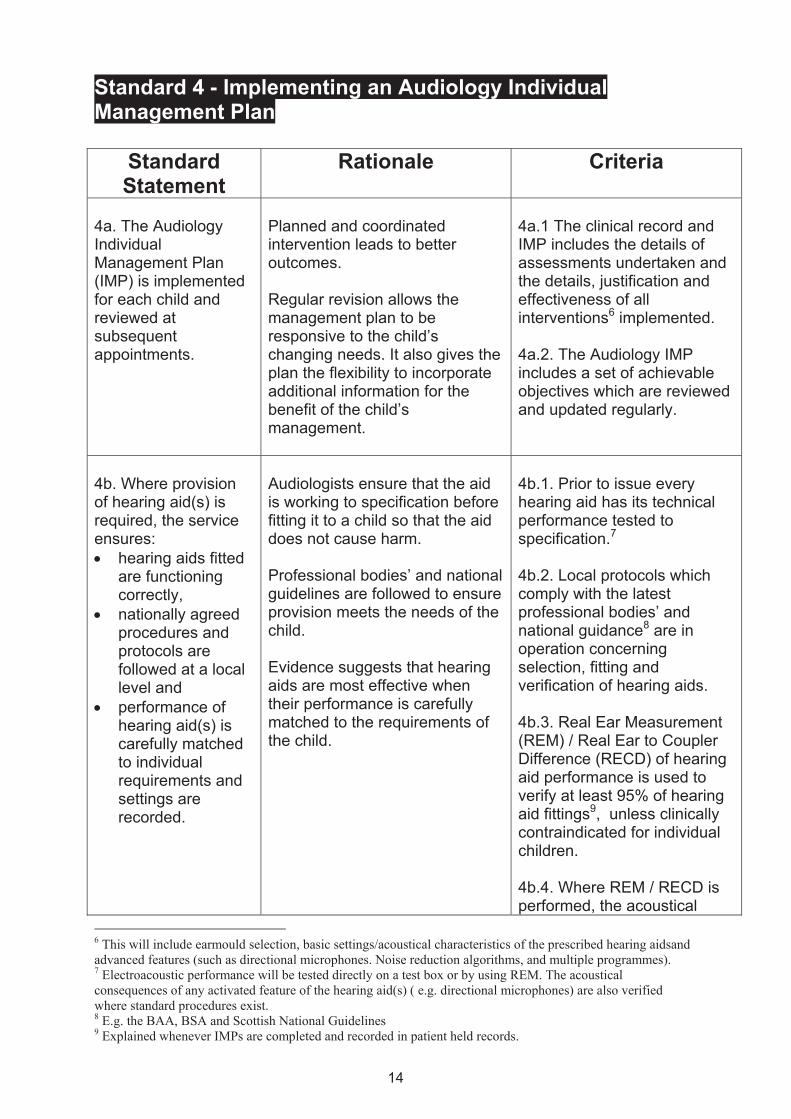
Standard 4 - Implementing an Audiology Individual Management Plan
Standard Statement
Rationale Criteria
4a. The Audiology Individual Management Plan (IMP) is implemented for each child and reviewed at subsequent appointments.
Planned and coordinated intervention leads to better outcomes. Regular revision allows the management plan to be responsive to the child’s changing needs. It also gives the plan the flexibility to incorporate additional information for the benefit of the child’s management.
4a.1 The clinical record and IMP includes the details of assessments undertaken and the details, justification and effectiveness of all interventions6 implemented. 4a.2. The Audiology IMP includes a set of achievable objectives which are reviewed and updated regularly.
4b. Where provision of hearing aid(s) is required, the service ensures: • hearing aids fitted
are functioning correctly,
• nationally agreed procedures and protocols are followed at a local level and
• performance of hearing aid(s) is carefully matched to individual requirements and settings are recorded.
Audiologists ensure that the aid is working to specification before fitting it to a child so that the aid does not cause harm. Professional bodies’ and national guidelines are followed to ensure provision meets the needs of the child. Evidence suggests that hearing aids are most effective when their performance is carefully matched to the requirements of the child.
4b.1. Prior to issue every hearing aid has its technical performance tested to specification.7 4b.2. Local protocols which comply with the latest professional bodies’ and national guidance8 are in operation concerning selection, fitting and verification of hearing aids. 4b.3. Real Ear Measurement (REM) / Real Ear to Coupler Difference (RECD) of hearing aid performance is used to verify at least 95% of hearing aid fittings9, unless clinically contraindicated for individual children. 4b.4. Where REM / RECD is performed, the acoustical
6 This will include earmould selection, basic settings/acoustical characteristics of the prescribed hearing aidsand advanced features (such as directional microphones. Noise reduction algorithms, and multiple programmes). 7 Electroacoustic performance will be tested directly on a test box or by using REM. The acoustical consequences of any activated feature of the hearing aid(s) ( e.g. directional microphones) are also verified where standard procedures exist. 8 E.g. the BAA, BSA and Scottish National Guidelines 9 Explained whenever IMPs are completed and recorded in patient held records.
14
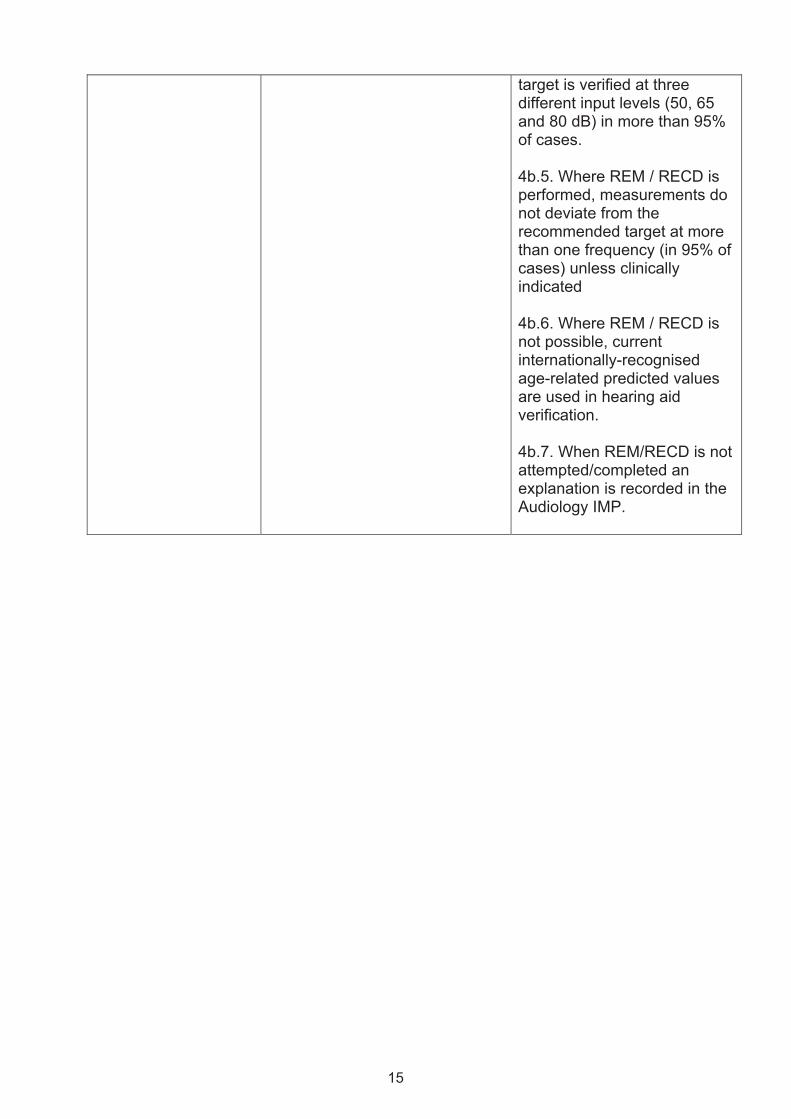
target is verified at three different input levels (50, 65 and 80 dB) in more than 95% of cases. 4b.5. Where REM / RECD is performed, measurements do not deviate from the recommended target at more than one frequency (in 95% of cases) unless clinically indicated 4b.6. Where REM / RECD is not possible, current internationally-recognised age-related predicted values are used in hearing aid verification. 4b.7. When REM/RECD is not attempted/completed an explanation is recorded in the Audiology IMP.
15
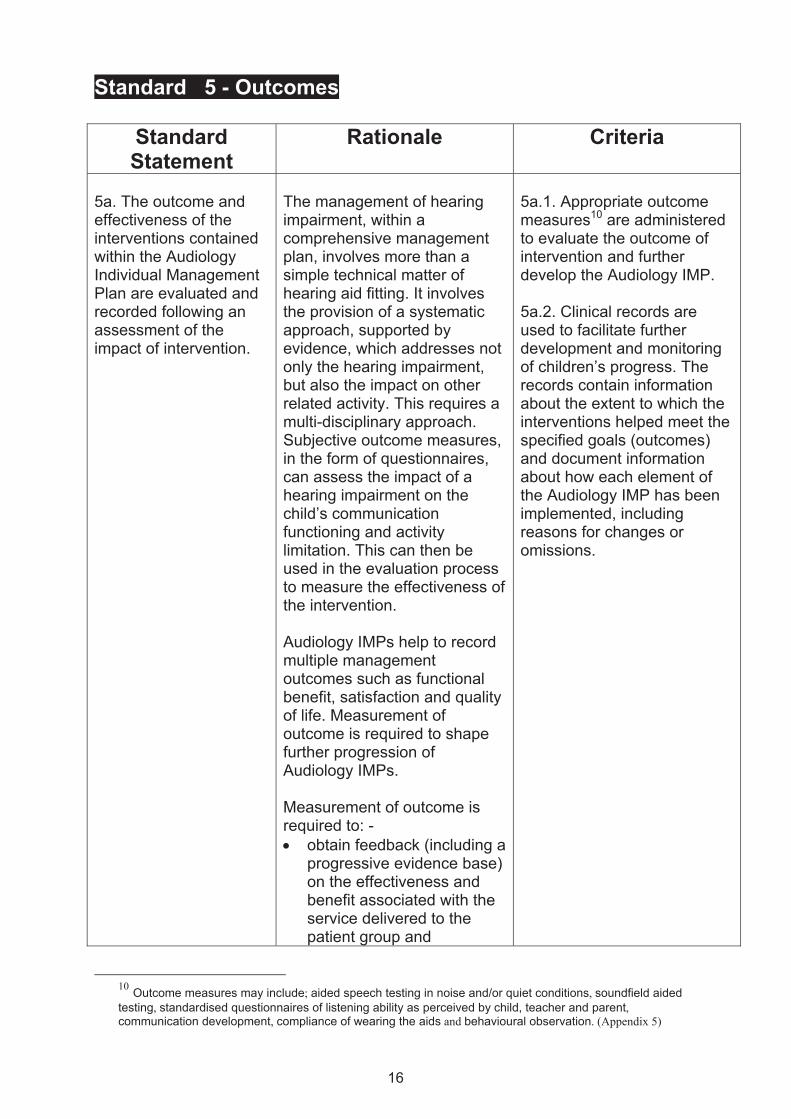
Standard 5 - Outcomes
Standard Statement
Rationale Criteria
5a. The outcome and effectiveness of the interventions contained within the Audiology Individual Management Plan are evaluated and recorded following an assessment of the impact of intervention.
The management of hearing impairment, within a comprehensive management plan, involves more than a simple technical matter of hearing aid fitting. It involves the provision of a systematic approach, supported by evidence, which addresses not only the hearing impairment, but also the impact on other related activity. This requires a multi-disciplinary approach. Subjective outcome measures, in the form of questionnaires, can assess the impact of a hearing impairment on the child’s communication functioning and activity limitation. This can then be used in the evaluation process to measure the effectiveness of the intervention. Audiology IMPs help to record multiple management outcomes such as functional benefit, satisfaction and quality of life. Measurement of outcome is required to shape further progression of Audiology IMPs. Measurement of outcome is required to: - • obtain feedback (including a
progressive evidence base) on the effectiveness and benefit associated with the service delivered to the patient group and
5a.1. Appropriate outcome measures10 are administered to evaluate the outcome of intervention and further develop the Audiology IMP. 5a.2. Clinical records are used to facilitate further development and monitoring of children’s progress. The records contain information about the extent to which the interventions helped meet the specified goals (outcomes) and document information about how each element of the Audiology IMP has been implemented, including reasons for changes or omissions.
10 Outcome measures may include; aided speech testing in noise and/or quiet conditions, soundfield aided testing, standardised questionnaires of listening ability as perceived by child, teacher and parent, communication development, compliance of wearing the aids and behavioural observation. (Appendix 5)
16
• facilitate further
development of the Audiology IMP and judge progress on the child’s outcomes.
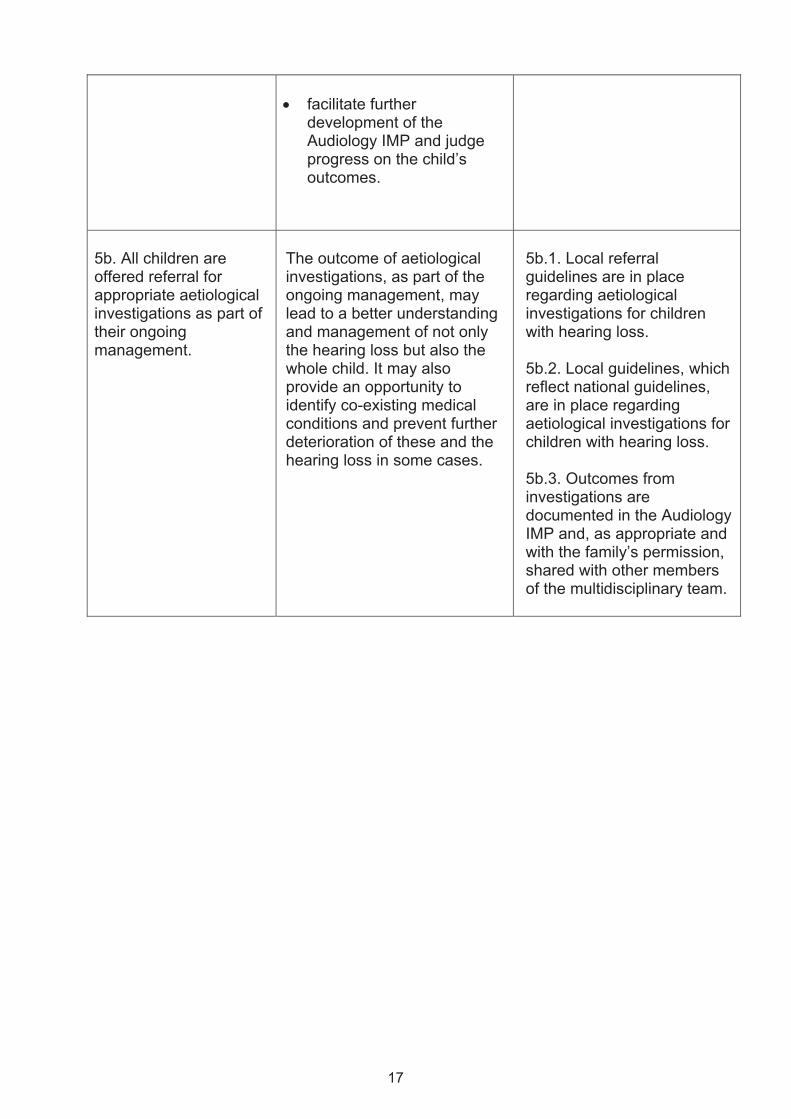
5b. All children are offered referral for appropriate aetiological investigations as part of their ongoing management.
The outcome of aetiological investigations, as part of the ongoing management, may lead to a better understanding and management of not only the hearing loss but also the whole child. It may also provide an opportunity to identify co-existing medical conditions and prevent further deterioration of these and the hearing loss in some cases.
5b.1. Local referral guidelines are in place regarding aetiological investigations for children with hearing loss. 5b.2. Local guidelines, which reflect national guidelines, are in place regarding aetiological investigations for children with hearing loss. 5b.3. Outcomes from investigations are documented in the Audiology IMP and, as appropriate and with the family’s permission, shared with other members of the multidisciplinary team.
17
Standard 6 Professional Competence
Standard Statement
Rationale
Criteria
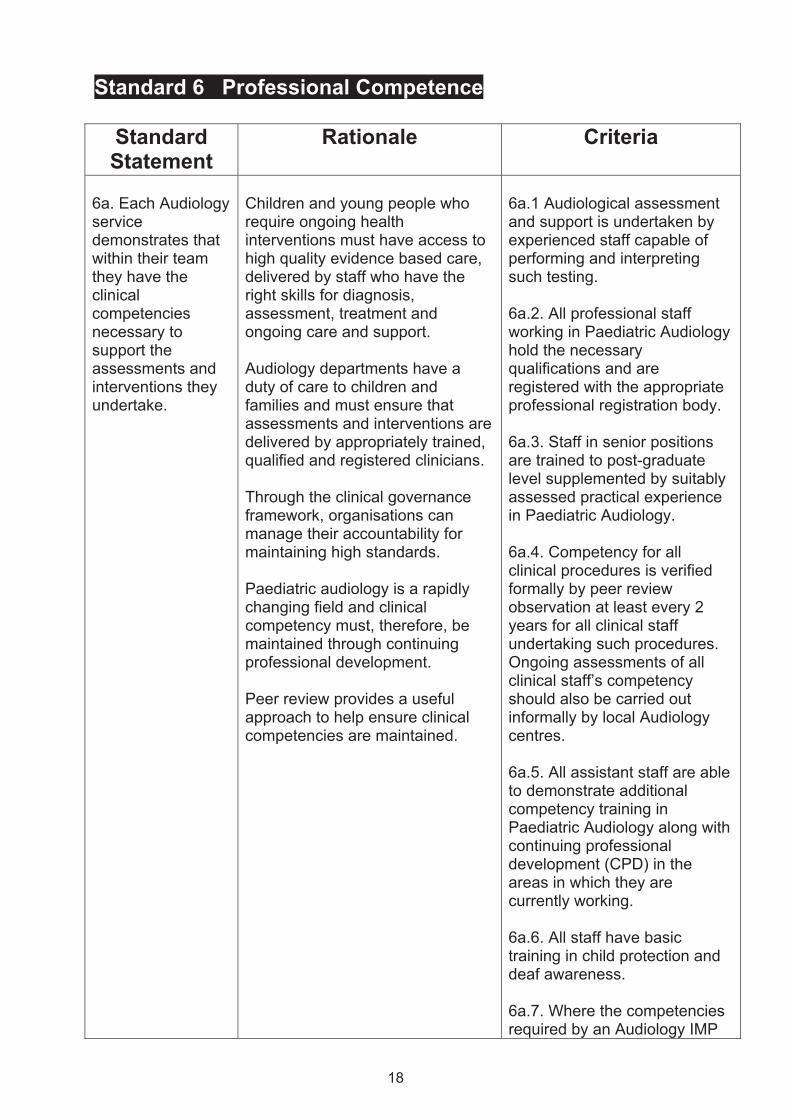
6a. Each Audiology service demonstrates that within their team they have the clinical competencies necessary to support the assessments and interventions they undertake.
Children and young people who require ongoing health interventions must have access to high quality evidence based care, delivered by staff who have the right skills for diagnosis, assessment, treatment and ongoing care and support. Audiology departments have a duty of care to children and families and must ensure that assessments and interventions are delivered by appropriately trained, qualified and registered clinicians. Through the clinical governance framework, organisations can manage their accountability for maintaining high standards. Paediatric audiology is a rapidly changing field and clinical competency must, therefore, be maintained through continuing professional development. Peer review provides a useful approach to help ensure clinical competencies are maintained.
6a.1 Audiological assessment and support is undertaken by experienced staff capable of performing and interpreting such testing. 6a.2. All professional staff working in Paediatric Audiology hold the necessary qualifications and are registered with the appropriate professional registration body. 6a.3. Staff in senior positions are trained to post-graduate level supplemented by suitably assessed practical experience in Paediatric Audiology. 6a.4. Competency for all clinical procedures is verified formally by peer review observation at least every 2 years for all clinical staff undertaking such procedures. Ongoing assessments of all clinical staff’s competency should also be carried out informally by local Audiology centres. 6a.5. All assistant staff are able to demonstrate additional competency training in Paediatric Audiology along with continuing professional development (CPD) in the areas in which they are currently working. 6a.6. All staff have basic training in child protection and deaf awareness. 6a.7. Where the competencies required by an Audiology IMP
18

are not held within a service, clear referral routes to external providers exist.
19
Standard 7 Information Provision and Communication with Children and Families
Standard Statement
Rationale Criteria
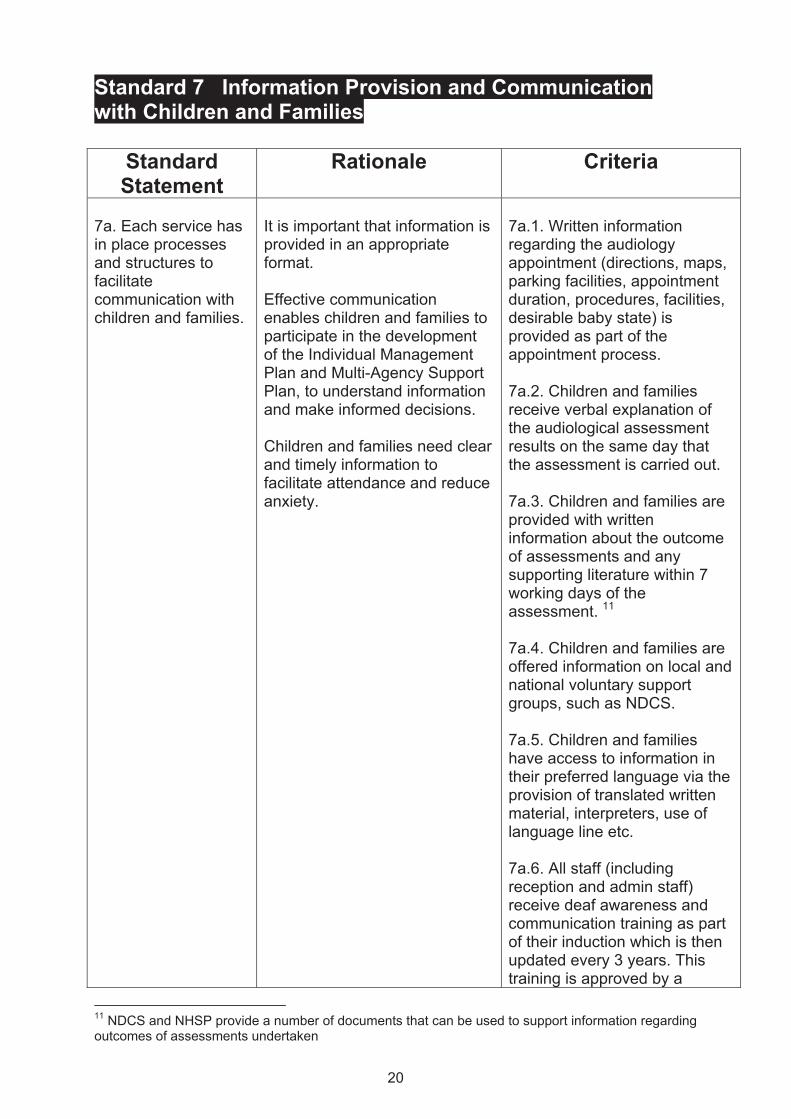
7a. Each service has in place processes and structures to facilitate communication with children and families.
It is important that information is provided in an appropriate format. Effective communication enables children and families to participate in the development of the Individual Management Plan and Multi-Agency Support Plan, to understand information and make informed decisions. Children and families need clear and timely information to facilitate attendance and reduce anxiety.
7a.1. Written information regarding the audiology appointment (directions, maps, parking facilities, appointment duration, procedures, facilities, desirable baby state) is provided as part of the appointment process. 7a.2. Children and families receive verbal explanation of the audiological assessment results on the same day that the assessment is carried out. 7a.3. Children and families are provided with written information about the outcome of assessments and any supporting literature within 7 working days of the assessment. 11 7a.4. Children and families are offered information on local and national voluntary support groups, such as NDCS. 7a.5. Children and families have access to information in their preferred language via the provision of translated written material, interpreters, use of language line etc. 7a.6. All staff (including reception and admin staff) receive deaf awareness and communication training as part of their induction which is then updated every 3 years. This training is approved by a
11 NDCS and NHSP provide a number of documents that can be used to support information regarding outcomes of assessments undertaken
20

relevant third party such as a voluntary sector organisation.
21
Standard 8 Multi-Agency Working
Standard Statement
Rationale Criteria
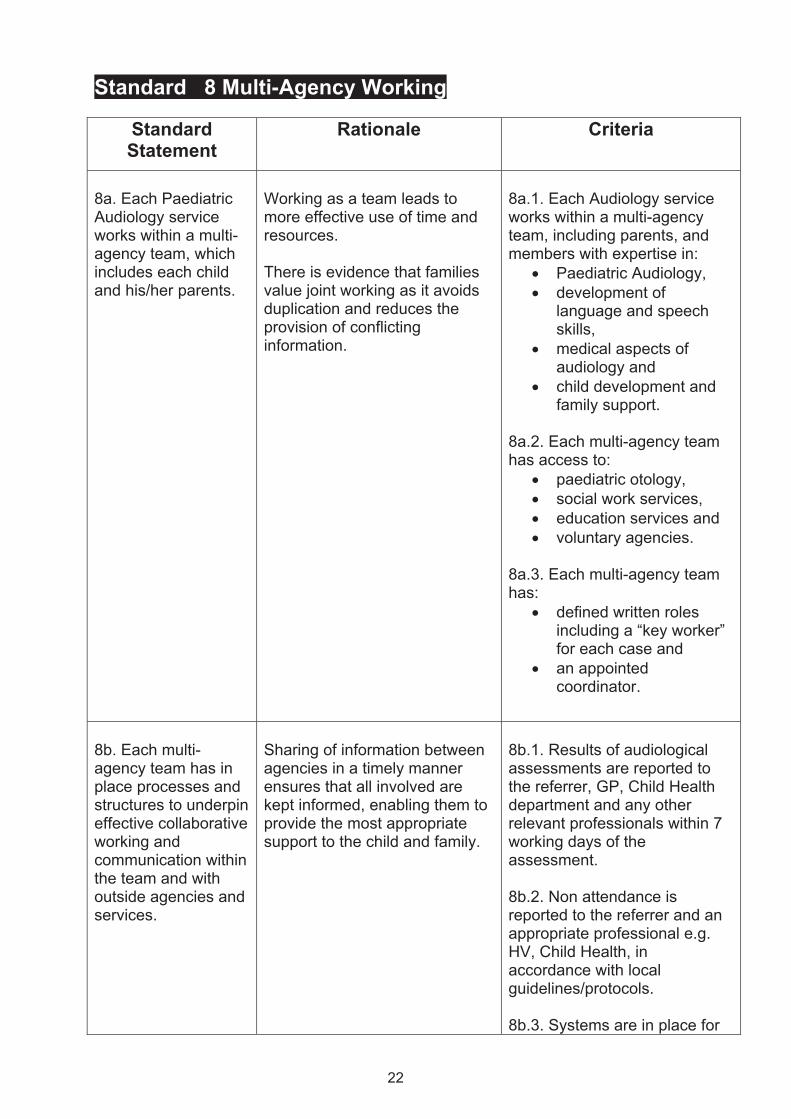
8a. Each Paediatric Audiology service works within a multi-agency team, which includes each child and his/her parents.
Working as a team leads to more effective use of time and resources. There is evidence that families value joint working as it avoids duplication and reduces the provision of conflicting information.
8a.1. Each Audiology service works within a multi-agency team, including parents, and members with expertise in:
• Paediatric Audiology, • development of
language and speech skills,
• medical aspects of audiology and
• child development and family support.
8a.2. Each multi-agency team has access to:
• paediatric otology, • social work services, • education services and • voluntary agencies.
8a.3. Each multi-agency team has:
• defined written roles including a “key worker” for each case and
• an appointed coordinator.
8b. Each multi-agency team has in place processes and structures to underpin effective collaborative working and communication within the team and with outside agencies and services.
Sharing of information between agencies in a timely manner ensures that all involved are kept informed, enabling them to provide the most appropriate support to the child and family.
8b.1. Results of audiological assessments are reported to the referrer, GP, Child Health department and any other relevant professionals within 7 working days of the assessment. 8b.2. Non attendance is reported to the referrer and an appropriate professional e.g. HV, Child Health, in accordance with local guidelines/protocols. 8b.3. Systems are in place for
22
the referral of families to other agencies and services involved in the management of children with hearing impairment. 8b.4. When Audiology refers families to other agencies and services, there is ongoing sharing and exchange of information between Audiology and these services and agencies. 8b.5. The Audiology service encourages and facilitates referral of families to appropriate voluntary organisations and parent support groups. 8b.6. Systems are in place to manage the transition from Paediatric to Adult Audiology services.12 8b.7. A Children’s Hearing Services Working Group13, including parent representatives, meets regularly to consider the development and delivery of services for hearing impaired children and their families. The remit will include the extent to which services meet the Standards described in this document.
8c. Each service has a major role in facilitating the development and ongoing review of a Multi-Agency Support Plan (MASP)14 for each child who has
When a number of different services work with a family, the Multi-Agency Support Plan ensures that individual components of the plan are understood in relation to one another and, more importantly, in relation to the overall aims
8c.1. The Multi-Agency Support Plan is tailored by the information gathered throughout the multi-agency assessment phase. 8c.2. The MASP is in place within 3 months of confirmation
12 The details of standards around transition from paediatric to adult services is outside the scope of this document. Consideration is being given to developing separate standards around this in the future. 13 For information describing Children’s Hearing Services Working Groups see Appendix 6 14 An example of a Multi-Agency support Plan can be found in Appendix 7
23
and wishes of the family. Multi-Agency Support Plans encourage:
• joint holistic discussions of an individual child’s needs,
• agreement of priorities, • engagement with and
involvement of the family and
• regular reviews of any support that is being provided, resulting in improved quality of ongoing care.
Regular revision allows the Multi-Agency Support Plan to be responsive to the child’s changing needs. It also gives the plan the flexibility to incorporate additional information for the benefit of the child’s management.
of a significant hearing loss. 8c.3. The MASP includes an assessment of current priorities including the level and type of service needed from:
• Audiology • Education • Paediatrics • Speech and language
therapy • Social work and • Specialist services, e.g.
cochlear implant team. 8c.4. The MASP includes details of service provision from those currently involved with the child and family. 8c.5. The MASP includes a set of achievable objectives which are reviewed and updated regularly (at least 6 monthly for pre-school children and annually for school age children) and circulated to all members of the team. 8c.6. The team has a close working relationship and meets on a regular basis (at least every 6 months for pre-school children and annually for school age children) to ensure that the support plan is being implemented in a coordinated way and in line with the wishes and needs of the family. 8c.7. Each agency carries out its own role in the further, more detailed assessments and information gathering necessary to complete the clinical, educational and social picture of the MASP. During this process, information is fed
15 “significant” hearing loss is not defined solely by the hearing level, but this must be considered alongside any other medical, developmental or social problems.
24
an ongoing significant15 hearing loss. The MASP takes into account the individual needs of the child and family, reflects the child and parental views and is clear, coordinated and flexible.
back and shared with all other members of the multi-agency team.
25
Standard 9 Service Effectiveness and Improvement
Standard Statement
Rationale Criteria
9a Each service has processes in place to measure service quality and improvement.
Measurement of qualitative and quantitative data helps to inform ongoing service improvement.
9a.1. Children and/or families are encouraged to complete surveys on, at least, an annual basis to determine satisfaction with different elements of the service received. These include: -
• accessibility, • proximity, • information provision, • professionalism of staff, • care and treatment and • overall service received.
9a.2. Participation rates in the survey are checked, annually, to ensure an acceptable proportion of patients have participated and a representative sample of the local population is covered (including gender and ethnicity). 9a.3. Sufficient analysis and interpretation of findings from satisfaction surveys are carried out annually by Audiology services. 9a.4. Action plans are implemented, when needed, to address areas of concern arising from surveys16and QRT data and performance.
16 An example of a survey satisfaction questionnaire used by audiology services is listed in appendix 8
26
9b. Each Audiology service actively participates in the local Children’s Hearing Services Working Group (CHSWG). Where a CHSWG does not exist, the service is active in the setting up of such a group.
Close working with parents as well as across organisations will lead to improved services for deaf children and their families. Effective recruitment to CHSWGs will ensure appropriate representation for the child and family, and demonstrates a truly inclusive approach. CHWSGs can ensure that children’s hearing services remain high on the agenda of those responsible for planning and delivering services at a strategic level. They can offer advice and guidance to ensure high quality services are available.
9b.1. The CHSWG meets regularly to review the multi-agency services for children and their families known to have, or considered to be at risk of having, a hearing impairment. 9b.2. The CHSWG helps to develop and improve the services delivered to deaf children and their families through the processes of ongoing support to all agencies involved. 9b.3. CHSWGs monitor the extent to which services meet the Standards detailed in this document.
9c Each service has processes in place to regularly consult with children, families and stakeholders.
Paediatric Audiology services that seek, consider and respond to the views of users will be more likely to meet their needs.
9c.1. The Audiology service has a framework in place to ensure regular consultation with children, families and stakeholders. 9c.2. Results of satisfaction surveys and service QRT scores are made available and discussed with children and families on an annual basis.
27
Improving quality and outcomes in Paediatric Audiology Services through critical evaluation
A quality rating tool for service providers
Foreword This quality rating tool (QRT) for Paediatric Audiology service providers and their partners has been developed to highlight best practice in Paediatric Audiology service provision in order to ensure local Audiology services meet population requirements and address health inequalities.
The QRT has been developed to assist providers of Paediatric Audiology services in assessing their ability to deliver services to meet the needs of their local population against the Quality Standards in Paediatric Audiology. It is envisaged that service providers will find the format of the tool helpful in measuring their progress towards meeting and indeed exceeding the quality standards. Beyond use by providers for self assessment, the tool could also be employed within an external (independent) assessment process. The publication of externally verified service quality ratings could also help potential service users make more informed decisions on the services that they choose to access. The Quality Rating Tool can be implemented in different ways, depending on the medium used, but on-line self assessment can be readily achieved. Using the Quality Rating Tool This quality rating tool covers 9 Quality Standards in Paediatric Audiology. Standards are only part of the cycle within which services are delivered and reviewed/monitored. Assessment against the standards will inform participating stakeholders of areas of good practice and areas in need of development, performance management and consolidation. Assessment should be an ongoing service management function. External quality assurance programmes will reinforce local ratings and contribute additional objectivity and transparency. Each section contains several quality statements relating to different criteria within the quality standards. Providers can rate their current activity against the scale 1-5 where 1 means that no elements of the quality statement are met/implemented and 5 represents full compliance with good to best practice, with graduations in between. Examples of what a score of 1 and 5 might look like have been given so that users of the tool can make better judgements about where on the scale the service corresponds. The 5 positions are: 1. No elements of the quality statement are met (or not evident*) 2. Few elements of the quality statement are met 3. Meets around half of the elements of the quality statement
28
4. Almost fully meets the quality statement 5. Fully compliant with good to best practice as indicated by quality statement criteria In judging evidence of performance (assigning an overall score for each standard) those completing assessment should consider the following elements of compliance: • All examples of best practice (where there is more than one) • The population served, (eg, all geographical areas, and all facilities) • Reflecting practice over the preceding 12 week period as a minimum (prior to the date of the assessment) NB Evidence must always be provided to support scores. In addition, a separate field provides suggestions of evidence to assist users of the tool in their rating assessment and direct discussion for any external quality assurance visit. On completion of the Quality Rating Tool, an overall position will indicate those areas that require further development and review. Understanding the score The underlying assumption used here is that, when scoring each standard, all quality statements (criteria) are equally important and therefore carry the same score weighting. Some criteria may have more aspects than others but each criteria should only be scored once. For instance when a criteria achieves 2 out of 4 different standards that the service should meet then appropriate approximate score would be 3 out of 5. A reminder of how to score the standards can be found in the rating scale at the top of each standard. For each standard, a percentage quality score can be calculated and an interpretation given of the meaning of these scores (eg needs urgent attention, needs attention, does not need attention). For instance; if a service scores a total of 32 out of 40 then the service is deemed to have 80% compliance with standard 1.
29
Stan
dard
1 –
Acc
ess
1a. A
ll ch
ildre
n sh
all h
ave
acce
ss to
the
audi
olog
ical
ser
vice
s th
ey re
quire
in a
tim
ely
fash
ion,
with
cle
arly
def
ined
refe
rral p
athw
ays
to a
udio
logi
cal s
ervi
ces
that
are
wid
ely
diss
emin
ated
and
revi
ewed
regu
larly
. 1b
. Ser
vice
dem
and
and
refe
rral d
ata
are
accu
rate
ly m
onito
red,
revi
ewed
and
repo
rted
to g
uide
ser
vice
pla
nnin
g.
Rat
ing
Scal
e
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts.
30
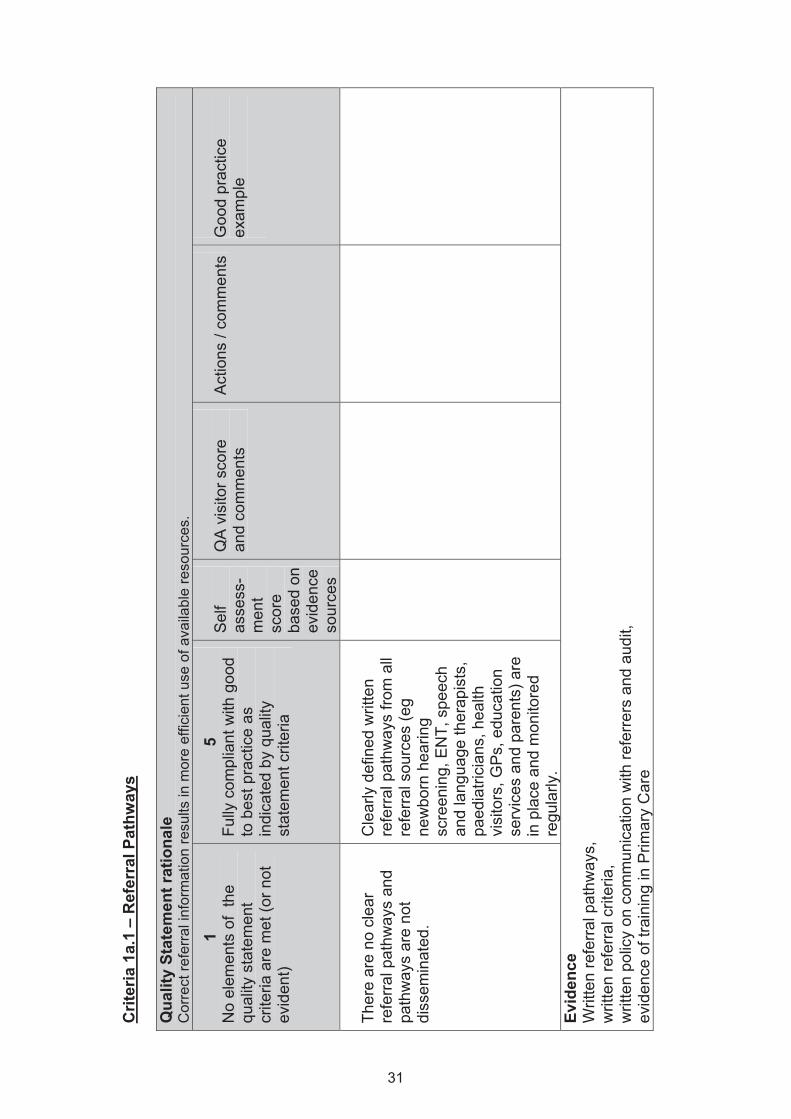
Crit
eria
1a.
1 –
Ref
erra
l Pat
hway
s Q
ualit
y St
atem
ent r
atio
nale
C
orre
ct re
ferr
al in
form
atio
n re
sults
in m
ore
effic
ient
use
of a
vaila
ble
reso
urce
s.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ther
e ar
e no
cle
ar
refe
rral p
athw
ays
and
path
way
s ar
e no
t di
ssem
inat
ed.
Cle
arly
def
ined
writ
ten
refe
rral p
athw
ays
from
all
refe
rral
sou
rces
(eg
new
born
hea
ring
scre
enin
g, E
NT,
spe
ech
and
lang
uage
ther
apis
ts,
paed
iatri
cian
s, h
ealth
vi
sito
rs, G
Ps, e
duca
tion
serv
ices
and
par
ents
) are
in
pla
ce a
nd m
onito
red
regu
larly
.
Evid
ence
W
ritte
n re
ferra
l pat
hway
s,
writ
ten
refe
rral c
riter
ia,
writ
ten
polic
y on
com
mun
icat
ion
with
refe
rrer
s an
d au
dit,
ev
iden
ce o
f tra
inin
g in
Prim
ary
Car
e
31
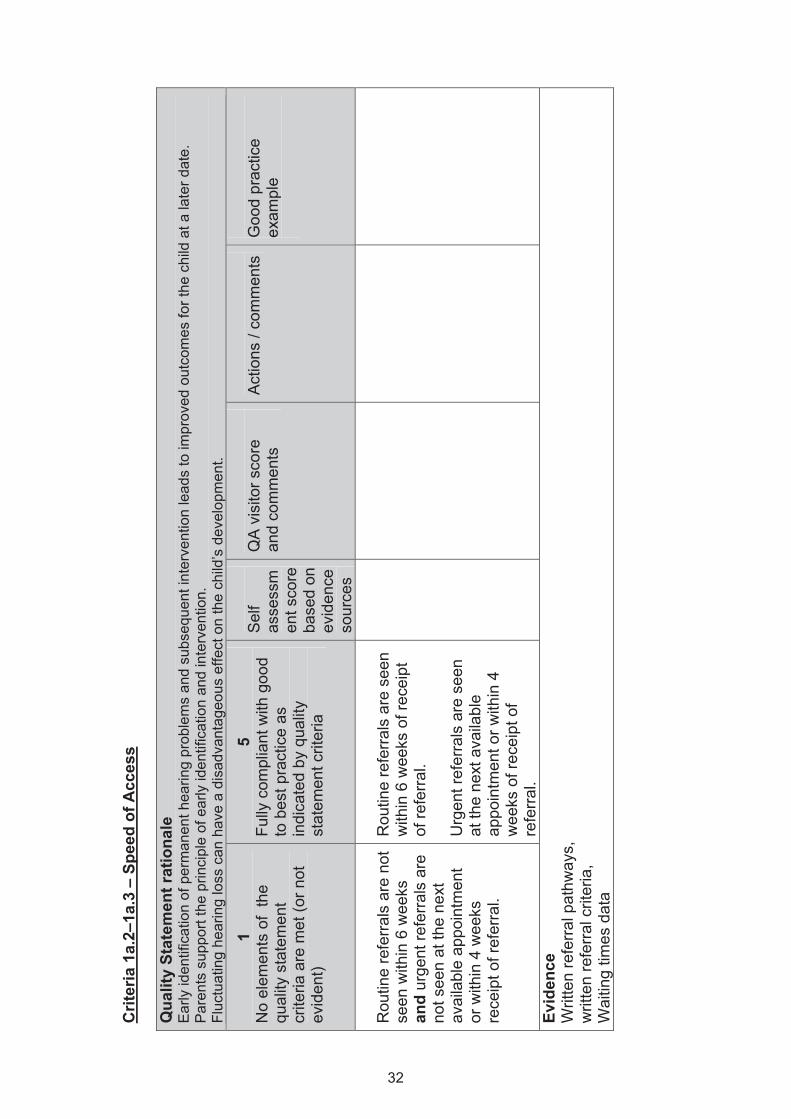
Crit
eria
1a.
2–1a
.3 –
Spe
ed o
f Acc
ess
Qua
lity
Stat
emen
t rat
iona
le
Ear
ly id
entif
icat
ion
of p
erm
anen
t hea
ring
prob
lem
s an
d su
bseq
uent
inte
rven
tion
lead
s to
impr
oved
out
com
es fo
r the
chi
ld a
t a la
ter d
ate.
P
aren
ts s
uppo
rt th
e pr
inci
ple
of e
arly
iden
tific
atio
n an
d in
terv
entio
n.
Fluc
tuat
ing
hear
ing
loss
can
hav
e a
disa
dvan
tage
ous
effe
ct o
n th
e ch
ild’s
dev
elop
men
t.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
men
t sco
re
base
d on
ev
iden
ce
sour
ces
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Rou
tine
refe
rrals
are
not
se
en w
ithin
6 w
eeks
an
d ur
gent
refe
rral
s ar
e no
t see
n at
the
next
av
aila
ble
appo
intm
ent
or w
ithin
4 w
eeks
re
ceip
t of r
efer
ral.
Rou
tine
refe
rrals
are
see
n w
ithin
6 w
eeks
of r
ecei
pt
of re
ferr
al.
Urg
ent r
efer
rals
are
see
n at
the
next
ava
ilabl
e ap
poin
tmen
t or w
ithin
4
wee
ks o
f rec
eipt
of
refe
rral
.
Evid
ence
W
ritte
n re
ferra
l pat
hway
s,
writ
ten
refe
rral c
riter
ia,
Wai
ting
times
dat
a
32
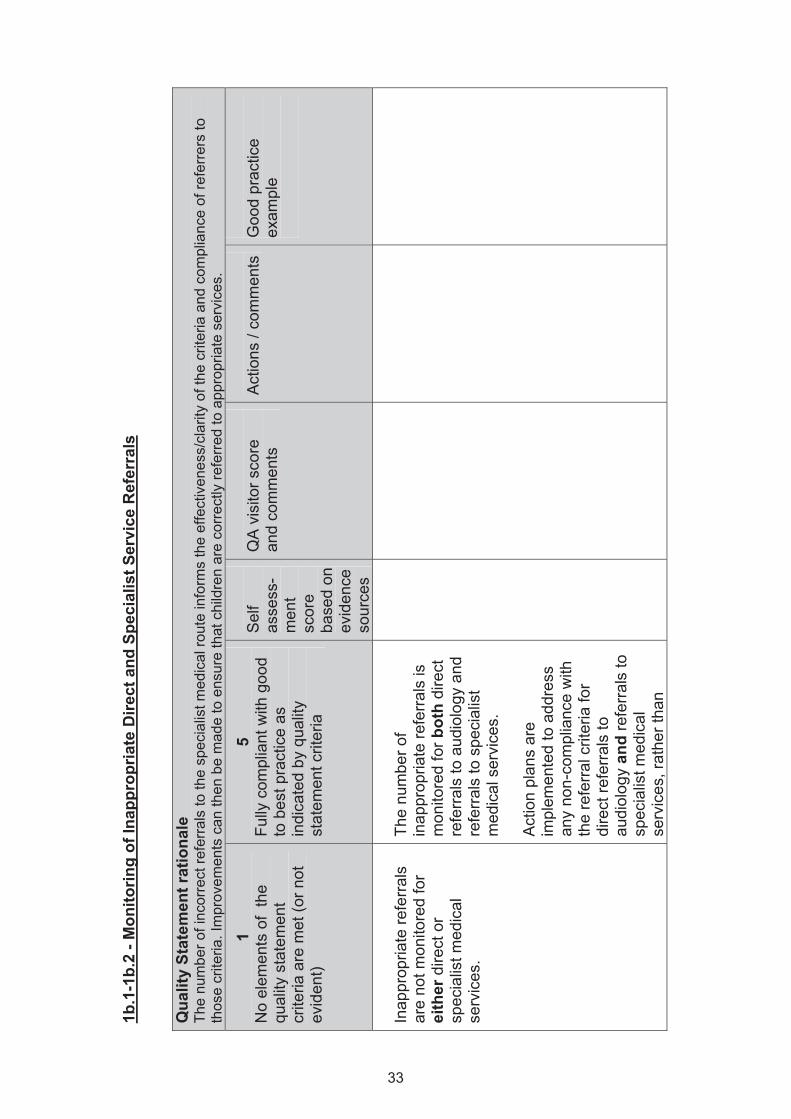
1b.1
-1b.
2 - M
onito
ring
of In
appr
opria
te D
irect
and
Spe
cial
ist S
ervi
ce R
efer
rals
Qua
lity
Stat
emen
t rat
iona
le
The
num
ber o
f inc
orre
ct re
ferr
als
to th
e sp
ecia
list m
edic
al ro
ute
info
rms
the
effe
ctiv
enes
s/cl
arity
of t
he c
riter
ia a
nd c
ompl
ianc
e of
refe
rrers
to
thos
e cr
iteria
. Im
prov
emen
ts c
an th
en b
e m
ade
to e
nsur
e th
at c
hild
ren
are
corr
ectly
refe
rred
to a
ppro
pria
te s
ervi
ces.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Inap
prop
riate
refe
rral
s ar
e no
t mon
itore
d fo
r ei
ther
dire
ct o
r sp
ecia
list m
edic
al
serv
ices
.
The
num
ber o
f in
appr
opria
te re
ferr
als
is
mon
itore
d fo
r bot
h di
rect
re
ferra
ls to
aud
iolo
gy a
nd
refe
rrals
to s
peci
alis
t m
edic
al s
ervi
ces.
A
ctio
n pl
ans
are
impl
emen
ted
to a
ddre
ss
any
non-
com
plia
nce
with
th
e re
ferr
al c
riter
ia fo
r di
rect
refe
rrals
to
audi
olog
y an
d re
ferr
als
to
spec
ialis
t med
ical
se
rvic
es, r
athe
r tha
n
33
audi
olog
y.
Evid
ence
A
udit
(idea
lly o
ver s
ever
al ti
me
poin
ts to
indi
cate
tren
d)
34
1b.3
– M
onito
ring
of W
aitin
g Ti
mes
Q
ualit
y St
atem
ent r
atio
nale
E
ffect
ive
allo
catio
n of
hea
lth re
sour
ces
is re
liant
upo
n ac
cura
te in
form
atio
n on
the
bala
nce
betw
een
dem
and
for s
ervi
ces
and
avai
labl
e re
sour
ces.
It is
impo
rtant
that
wai
ting
times
for a
ll st
ages
of t
he p
atie
nt p
athw
ay a
re c
olle
cted
and
mon
itore
d in
an
effe
ctiv
e m
anne
r. Th
e us
e of
IT
sys
tem
s to
com
pute
info
rmat
ion
such
as
dem
ogra
phic
dat
a an
d w
aitin
g tim
es w
ill in
form
allo
catio
n of
ser
vice
s.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Wai
ting
times
are
not
m
easu
red
at a
ll w
ithin
th
e de
partm
ent.
Wai
ting
times
are
m
onito
red
with
in th
e de
partm
ent b
ased
upo
n ro
bust
dat
a co
llect
ion.
Evid
ence
A
udit
(idea
lly o
ver s
ever
al ti
me
poin
ts to
indi
cate
tren
d)
Wai
ting
times
dat
a to
han
d
35
1b.4
– S
ervi
ce P
lann
ing
Qua
lity
Stat
emen
t rat
iona
le
Effe
ctiv
e al
loca
tion
of re
sour
ces
relie
s up
on in
form
atio
n on
act
ual d
eman
d an
d po
tent
ial/
proj
ecte
d de
man
d fo
r spe
cific
ser
vice
s.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
No
data
is c
olle
cted
, re
view
ed a
nd u
sed
for
annu
al s
ervi
ce re
view
.
All
the
follo
win
g da
ta is
co
llect
ed, r
evie
wed
and
us
ed in
ann
ual s
ervi
ce
revi
ew:
• de
mog
raph
ics
of
loca
lly s
erve
d po
pula
tions
, inc
ludi
ng
fact
ors
such
as
ethn
ic
dive
rsity
, soc
ial
depr
ivat
ion
and
age,
17
• th
e nu
mbe
r of c
hild
ren
refe
rred
to A
udio
logy
se
rvic
es a
nd th
eir
asso
ciat
ed
dem
ogra
phic
in
form
atio
n,
• th
e up
take
of N
HS
17
Thi
s is t
o es
tabl
ish
a be
nchm
ark
and
to g
auge
the
serv
ice
trend
s ove
r tim
e.
36
hear
ing
aids
in th
e lo
cal p
opul
atio
n co
mpa
red
with
the
pred
ictiv
e ne
ed fo
r se
rvic
es a
nd
• th
e nu
mbe
r and
type
of
surg
ical
inte
rven
tions
re
quire
d fo
r chi
ldre
n re
ferre
d to
Aud
iolo
gy
serv
ices
. Ev
iden
ce
Dat
a on
hea
ring
aid
upta
ke,
Dat
a on
refe
rral
s to
aud
iolo
gy s
ervi
ces,
D
ata
on p
atie
nt d
emog
raph
ic,
Ann
ual s
ervi
ce re
view
.
37
Stan
dard
2 –
Ass
essm
ent
2a. A
ll re
ferre
d ch
ildre
n re
ceiv
e au
diol
ogic
al a
sses
smen
t com
men
sura
te w
ith th
eir a
ge a
nd s
tage
of d
evel
opm
ent.
In s
ome
case
s th
is w
ill fo
rm p
art o
f a m
ultid
isci
plin
ary
team
app
roac
h of
whi
ch p
aren
ts a
re k
ey m
embe
rs. T
he ra
nge
of a
udio
logi
cal a
sses
smen
ts
avai
labl
e en
able
s de
finiti
on o
f deg
ree
and
natu
re h
earin
g lo
ss.
2b. T
he o
utco
me
of th
e as
sess
men
t sho
uld
info
rm a
cle
arly
def
ined
man
agem
ent p
lan.
R
atin
g Sc
ale
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r no
t evi
dent
)
2 Fe
w e
lem
ents
of
the
qual
ity
stat
emen
t crit
eria
ar
e m
et
3 M
eets
aro
und
half
of th
e el
emen
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
4 A
lmos
t ful
ly m
eets
th
e qu
ality
st
atem
ent c
riter
ia
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Plea
se u
se th
e ra
ting
scal
e an
d ex
ampl
es g
iven
in th
e 1
and
5 co
lum
ns a
s an
indi
cato
r to
help
you
sco
re th
e se
lf-as
sess
men
t tab
le
belo
w. E
ach
tabl
e sh
ould
onl
y ev
er h
ave
1 se
lf-as
sess
men
t sco
re. W
hen
you
perc
eive
ther
e to
be
mor
e th
an 1
asp
ect o
f the
tabl
e th
at
you
coul
d gi
ve a
sco
re fo
r, pl
ease
use
an
aver
age
of e
ach
of th
e as
pect
s.
38
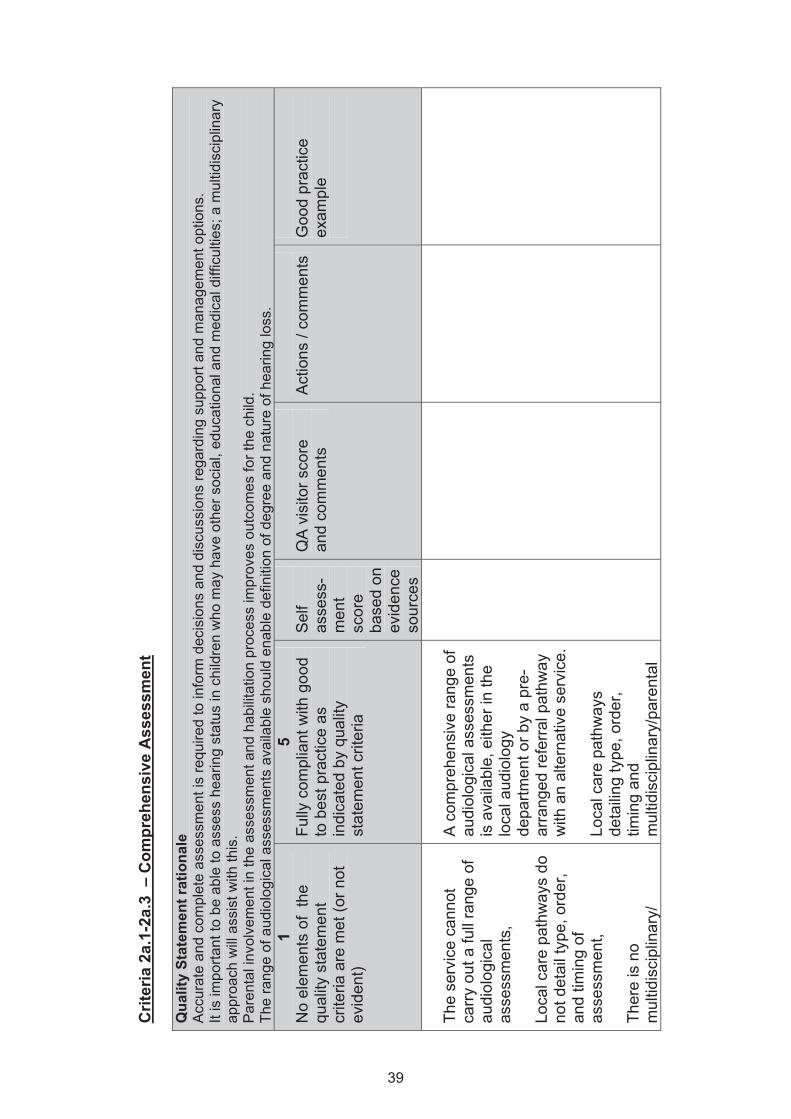
Crit
eria
2a.
1-2a
.3 –
Com
preh
ensi
ve A
sses
smen
t Q
ualit
y St
atem
ent r
atio
nale
A
ccur
ate
and
com
plet
e as
sess
men
t is
requ
ired
to in
form
dec
isio
ns a
nd d
iscu
ssio
ns re
gard
ing
supp
ort a
nd m
anag
emen
t opt
ions
. It
is im
porta
nt to
be
able
to a
sses
s he
arin
g st
atus
in c
hild
ren
who
may
hav
e ot
her s
ocia
l, ed
ucat
iona
l and
med
ical
diff
icul
ties;
a m
ultid
isci
plin
ary
appr
oach
will
ass
ist w
ith th
is.
Par
enta
l inv
olve
men
t in
the
asse
ssm
ent a
nd h
abili
tatio
n pr
oces
s im
prov
es o
utco
mes
for t
he c
hild
. Th
e ra
nge
of a
udio
logi
cal a
sses
smen
ts a
vaila
ble
shou
ld e
nabl
e de
finiti
on o
f deg
ree
and
natu
re o
f hea
ring
loss
. 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or n
ot
evid
ent)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
serv
ice
cann
ot
carry
out
a fu
ll ra
nge
of
audi
olog
ical
as
sess
men
ts,
Loca
l car
e pa
thw
ays
do
not d
etai
l typ
e, o
rder
, an
d tim
ing
of
asse
ssm
ent,
Ther
e is
no
mul
tidis
cipl
inar
y/
A c
ompr
ehen
sive
rang
e of
au
diol
ogic
al a
sses
smen
ts
is a
vaila
ble,
eith
er in
the
loca
l aud
iolo
gy
depa
rtmen
t or b
y a
pre-
arra
nged
refe
rral p
athw
ay
with
an
alte
rnat
ive
serv
ice.
Lo
cal c
are
path
way
s de
taili
ng ty
pe, o
rder
, tim
ing
and
mul
tidis
cipl
inar
y/pa
rent
al
39
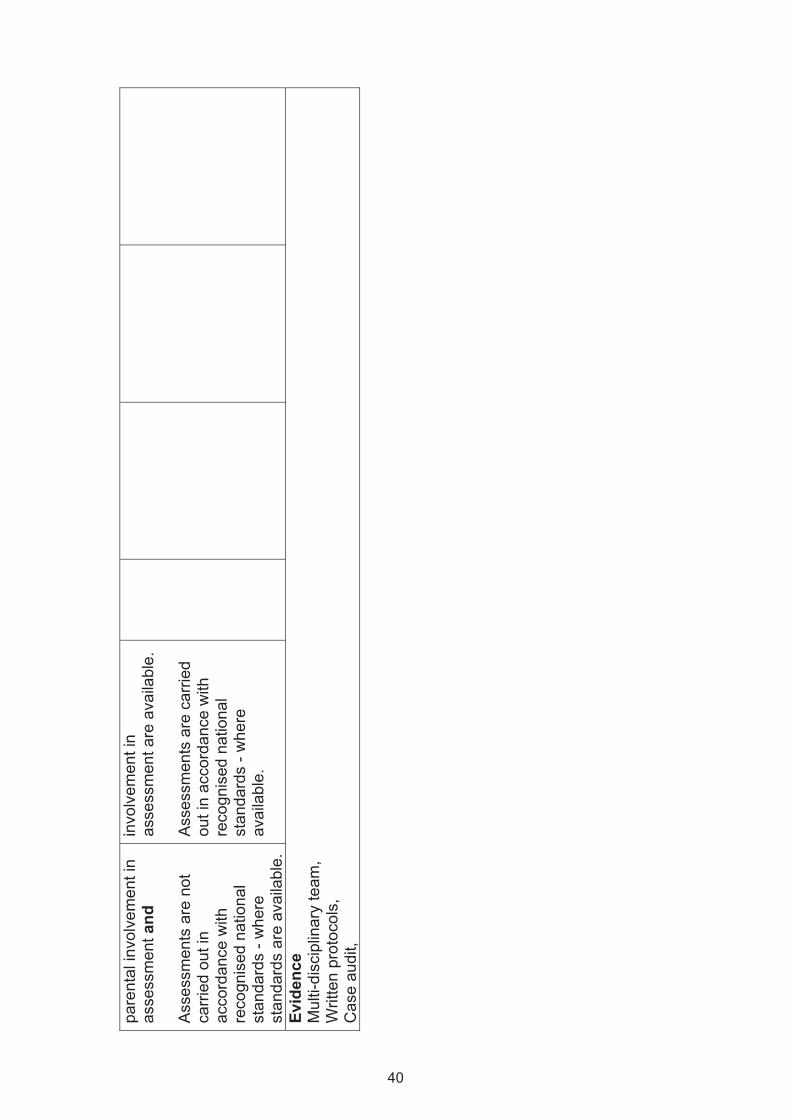
pare
ntal
invo
lvem
ent i
n as
sess
men
t and
A
sses
smen
ts a
re n
ot
carri
ed o
ut in
ac
cord
ance
with
re
cogn
ised
nat
iona
l st
anda
rds
- whe
re
stan
dard
s ar
e av
aila
ble.
invo
lvem
ent i
n as
sess
men
t are
ava
ilabl
e.
Ass
essm
ents
are
car
ried
out i
n ac
cord
ance
with
re
cogn
ised
nat
iona
l st
anda
rds
- whe
re
avai
labl
e.
Ev
iden
ce
Mul
ti-di
scip
linar
y te
am,
Writ
ten
prot
ocol
s,
Cas
e au
dit,
40
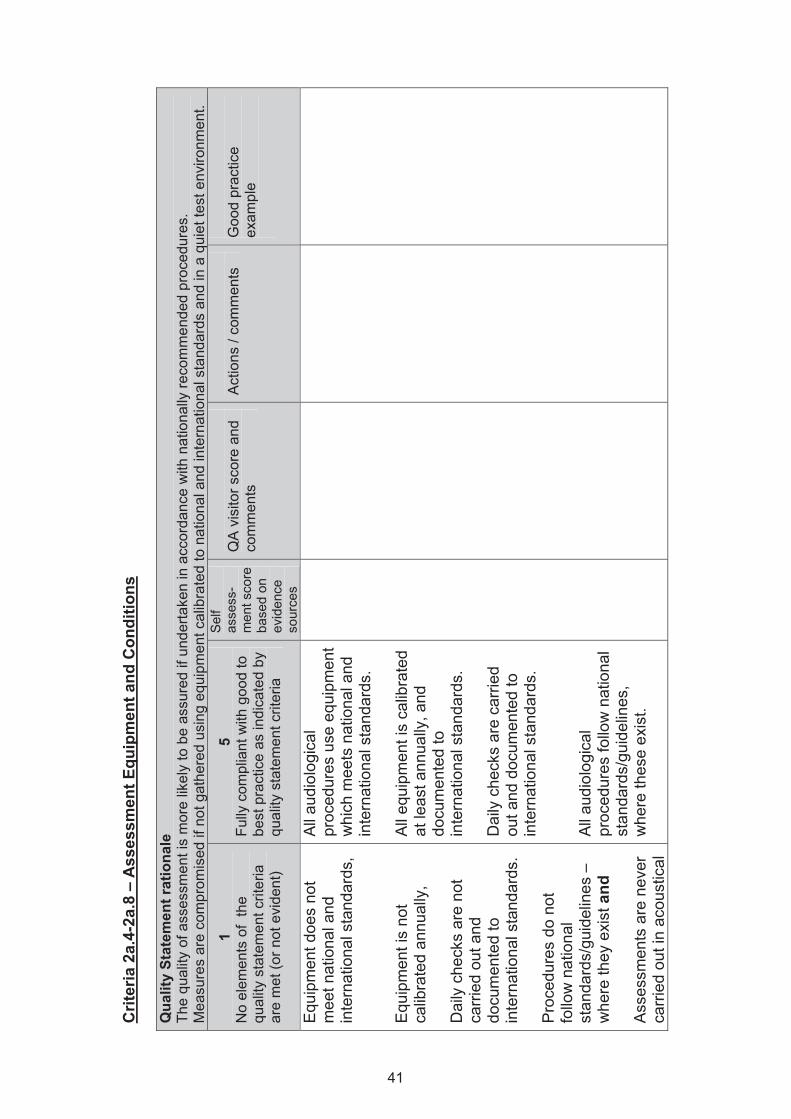
Crit
eria
2a.
4-2a
.8 –
Ass
essm
ent E
quip
men
t and
Con
ditio
ns
Qua
lity
Stat
emen
t rat
iona
le
The
qual
ity o
f ass
essm
ent i
s m
ore
likel
y to
be
assu
red
if un
derta
ken
in a
ccor
danc
e w
ith n
atio
nally
reco
mm
ende
d pr
oced
ures
. M
easu
res
are
com
prom
ised
if n
ot g
athe
red
usin
g eq
uipm
ent c
alib
rate
d to
nat
iona
l and
inte
rnat
iona
l sta
ndar
ds a
nd in
a q
uiet
test
env
ironm
ent.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent c
riter
ia
are
met
(or n
ot e
vide
nt)
5 Fu
lly c
ompl
iant
with
goo
d to
be
st p
ract
ice
as in
dica
ted
by
qual
ity s
tate
men
t crit
eria
Sel
f as
sess
-m
ent s
core
ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
and
co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Equ
ipm
ent d
oes
not
mee
t nat
iona
l and
in
tern
atio
nal s
tand
ards
, E
quip
men
t is
not
calib
rate
d an
nual
ly,
Dai
ly c
heck
s ar
e no
t ca
rried
out
and
do
cum
ente
d to
in
tern
atio
nal s
tand
ards
. P
roce
dure
s do
not
fo
llow
nat
iona
l st
anda
rds/
guid
elin
es –
w
here
they
exi
st a
nd
Ass
essm
ents
are
nev
er
carri
ed o
ut in
aco
ustic
al
All a
udio
logi
cal
proc
edur
es u
se e
quip
men
t w
hich
mee
ts n
atio
nal a
nd
inte
rnat
iona
l sta
ndar
ds.
All
equi
pmen
t is
calib
rate
d at
leas
t ann
ually
, and
do
cum
ente
d to
in
tern
atio
nal s
tand
ards
. D
aily
che
cks
are
carri
ed
out a
nd d
ocum
ente
d to
in
tern
atio
nal s
tand
ards
. Al
l aud
iolo
gica
l pr
oced
ures
follo
w n
atio
nal
stan
dard
s/gu
idel
ines
, w
here
thes
e ex
ist.
41
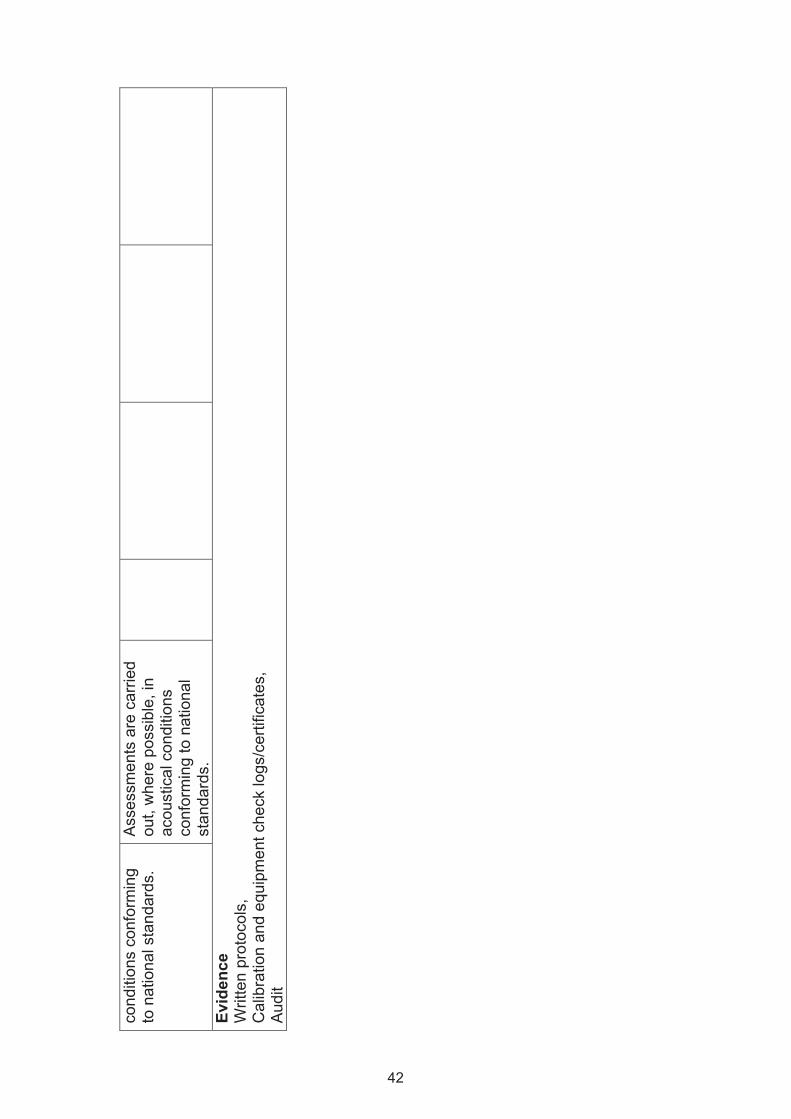
cond
ition
s co
nfor
min
g to
nat
iona
l sta
ndar
ds.
Ass
essm
ents
are
car
ried
out,
whe
re p
ossi
ble,
in
acou
stic
al c
ondi
tions
co
nfor
min
g to
nat
iona
l st
anda
rds.
Ev
iden
ce
Writ
ten
prot
ocol
s,
Cal
ibra
tion
and
equi
pmen
t che
ck lo
gs/c
ertif
icat
es,
Audi
t
42
Crit
eria
2b.
1-2b
.2 –
Ass
essm
ent O
utco
me
Qua
lity
Stat
emen
t rat
iona
le
Pro
mpt
, acc
urat
e an
d co
mpl
ete
audi
olog
ical
info
rmat
ion
info
rms
the
ampl
ifica
tion
proc
ess.
Th
e ou
tcom
e of
ass
essm
ents
sho
uld
cont
ribut
e in
suf
ficie
nt d
etai
l to
esta
blis
hmen
t of a
etio
logy
, pro
gnos
is a
nd fu
rther
man
agem
ent.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ass
essm
ents
are
nev
er
inte
rpre
ted
with
the
deve
lopm
ent s
tatu
s of
th
e ch
ild o
r any
co-
exis
ting
med
ical
co
nditi
ons
bein
g ta
king
in
to a
ccou
nt a
nd
Ther
e ar
e no
loca
l pr
otoc
ols
defin
ing
appr
opria
te
man
agem
ent o
ptio
ns
aris
ing
from
as
sess
men
t.
All
asse
ssm
ents
are
in
terp
rete
d ta
king
into
ac
coun
t the
de
velo
pmen
tal s
tatu
s of
th
e ch
ild a
nd a
ny c
o-ex
istin
g m
edic
al
cond
ition
s.
Writ
ten
loca
l pro
toco
ls
exis
t whi
ch d
efin
e ap
prop
riate
man
agem
ent
optio
ns a
risin
g fro
m th
e as
sess
men
t (su
ch a
s de
cisi
ons
to re
fer,
revi
ew
or d
isch
arge
).
43
Evid
ence
W
ritte
n pr
otoc
ols,
C
ase
audi
t, P
eer r
evie
w o
f cas
es
44
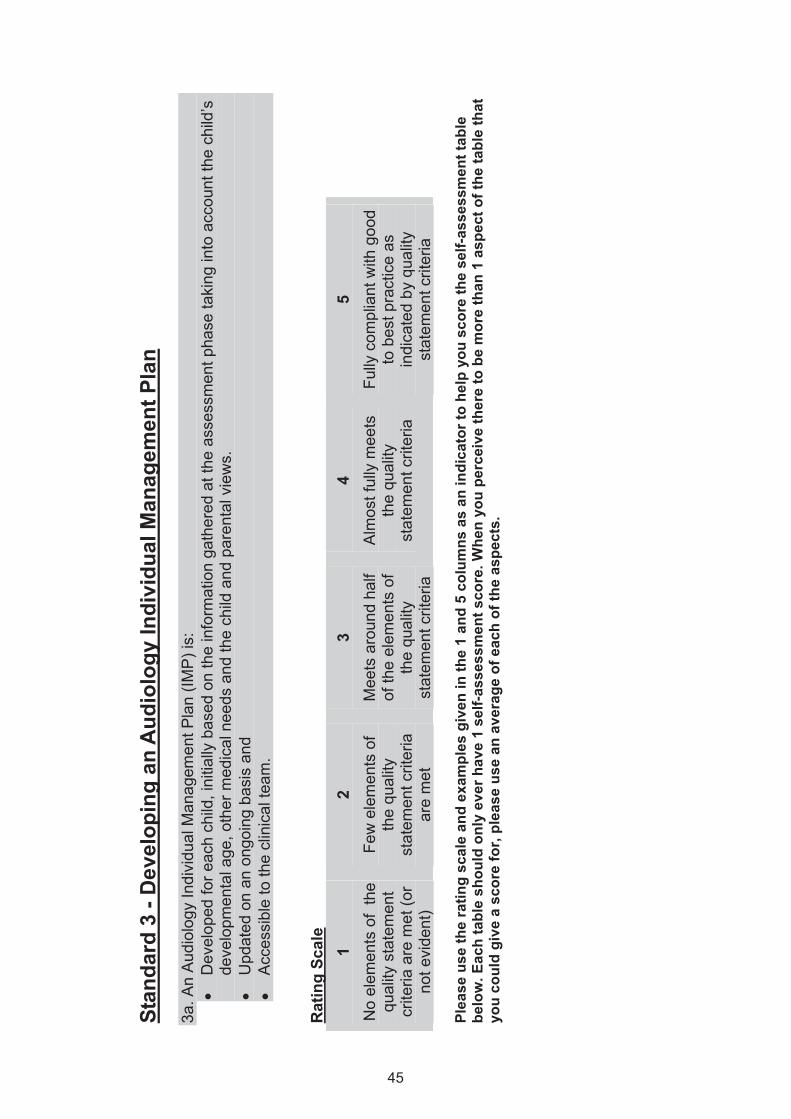
Stan
dard
3 -
Dev
elop
ing
an A
udio
logy
Indi
vidu
al M
anag
emen
t Pla
n 3a
. An
Aud
iolo
gy In
divi
dual
Man
agem
ent P
lan
(IMP
) is:
•
Dev
elop
ed fo
r eac
h ch
ild, i
nitia
lly b
ased
on
the
info
rmat
ion
gath
ered
at t
he a
sses
smen
t pha
se ta
king
into
acc
ount
the
child
’s
deve
lopm
enta
l age
, oth
er m
edic
al n
eeds
and
the
child
and
par
enta
l vie
ws.
•
Upd
ated
on
an o
ngoi
ng b
asis
and
•
Acc
essi
ble
to th
e cl
inic
al te
am.
Rat
ing
Scal
e 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2 Fe
w e
lem
ents
of
the
qual
ity
stat
emen
t crit
eria
ar
e m
et
3 M
eets
aro
und
half
of th
e el
emen
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
4 A
lmos
t ful
ly m
eets
th
e qu
ality
st
atem
ent c
riter
ia
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Plea
se u
se th
e ra
ting
scal
e an
d ex
ampl
es g
iven
in th
e 1
and
5 co
lum
ns a
s an
indi
cato
r to
help
you
sco
re th
e se
lf-as
sess
men
t tab
le
belo
w. E
ach
tabl
e sh
ould
onl
y ev
er h
ave
1 se
lf-as
sess
men
t sco
re. W
hen
you
perc
eive
ther
e to
be
mor
e th
an 1
asp
ect o
f the
tabl
e th
at
you
coul
d gi
ve a
sco
re fo
r, pl
ease
use
an
aver
age
of e
ach
of th
e as
pect
s.
45
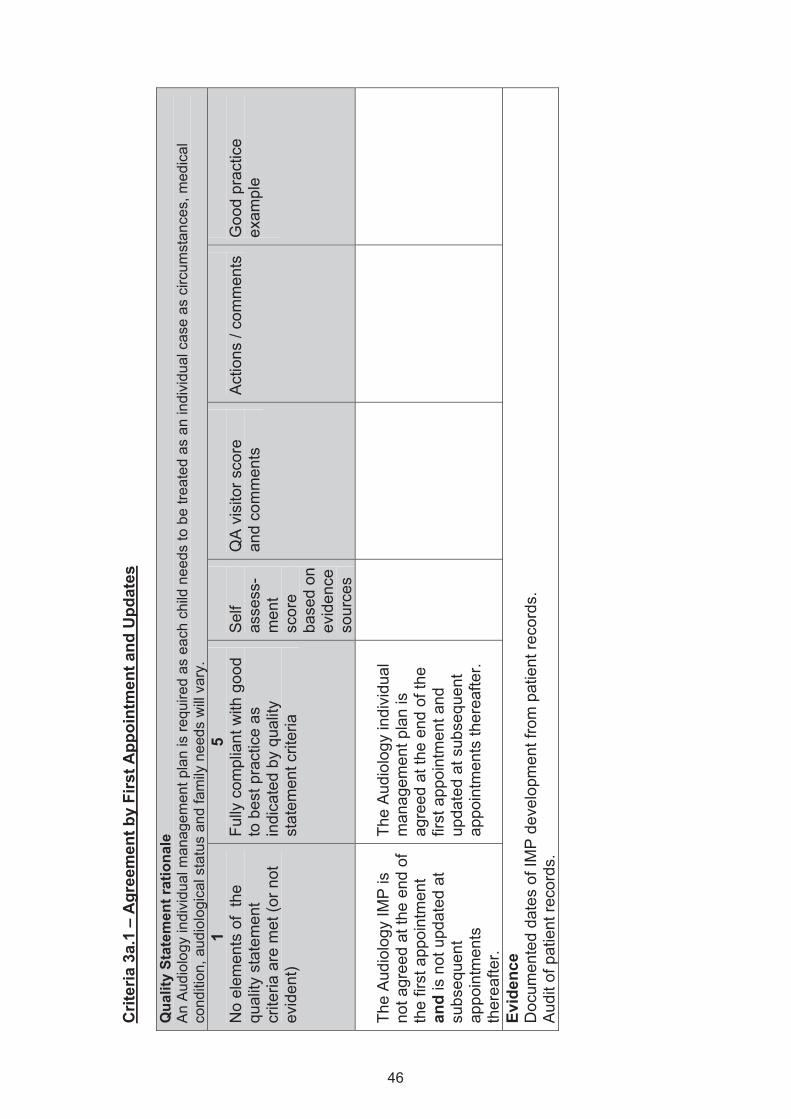
Crit
eria
3a.
1 –
Agr
eem
ent b
y Fi
rst A
ppoi
ntm
ent a
nd U
pdat
es
Qua
lity
Stat
emen
t rat
iona
le
An
Aud
iolo
gy in
divi
dual
man
agem
ent p
lan
is re
quire
d as
eac
h ch
ild n
eeds
to b
e tre
ated
as
an in
divi
dual
cas
e as
circ
umst
ance
s, m
edic
al
cond
ition
, aud
iolo
gica
l sta
tus
and
fam
ily n
eeds
will
var
y.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Th
e A
udio
logy
IMP
is
not a
gree
d at
the
end
of
the
first
app
oint
men
t an
d is
not
upd
ated
at
subs
eque
nt
appo
intm
ents
th
erea
fter.
The
Aud
iolo
gy in
divi
dual
m
anag
emen
t pla
n is
ag
reed
at t
he e
nd o
f the
fir
st a
ppoi
ntm
ent a
nd
upda
ted
at s
ubse
quen
t ap
poin
tmen
ts th
erea
fter.
Evid
ence
D
ocum
ente
d da
tes
of IM
P d
evel
opm
ent f
rom
pat
ient
reco
rds.
A
udit
of p
atie
nt re
cord
s.
46
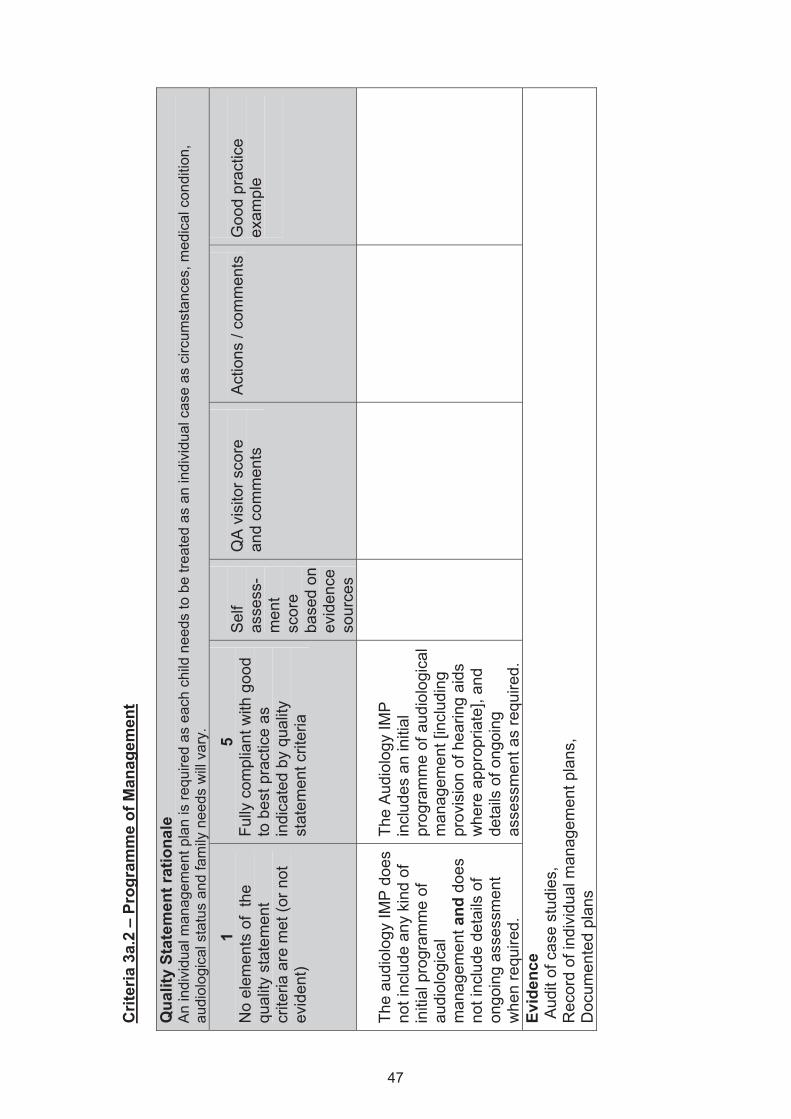
Crit
eria
3a.
2 –
Prog
ram
me
of M
anag
emen
t Q
ualit
y St
atem
ent r
atio
nale
A
n in
divi
dual
man
agem
ent p
lan
is re
quire
d as
eac
h ch
ild n
eeds
to b
e tre
ated
as
an in
divi
dual
cas
e as
circ
umst
ance
s, m
edic
al c
ondi
tion,
au
diol
ogic
al s
tatu
s an
d fa
mily
nee
ds w
ill v
ary.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
audi
olog
y IM
P d
oes
not i
nclu
de a
ny k
ind
of
initi
al p
rogr
amm
e of
au
diol
ogic
al
man
agem
ent a
nd d
oes
not i
nclu
de d
etai
ls o
f on
goin
g as
sess
men
t w
hen
requ
ired.
The
Aud
iolo
gy IM
P
incl
udes
an
initi
al
prog
ram
me
of a
udio
logi
cal
man
agem
ent [
incl
udin
g pr
ovis
ion
of h
earin
g ai
ds
whe
re a
ppro
pria
te],
and
deta
ils o
f ong
oing
as
sess
men
t as
requ
ired.
Evid
ence
A
udit
of c
ase
stud
ies,
R
ecor
d of
indi
vidu
al m
anag
emen
t pla
ns,
Doc
umen
ted
plan
s
47
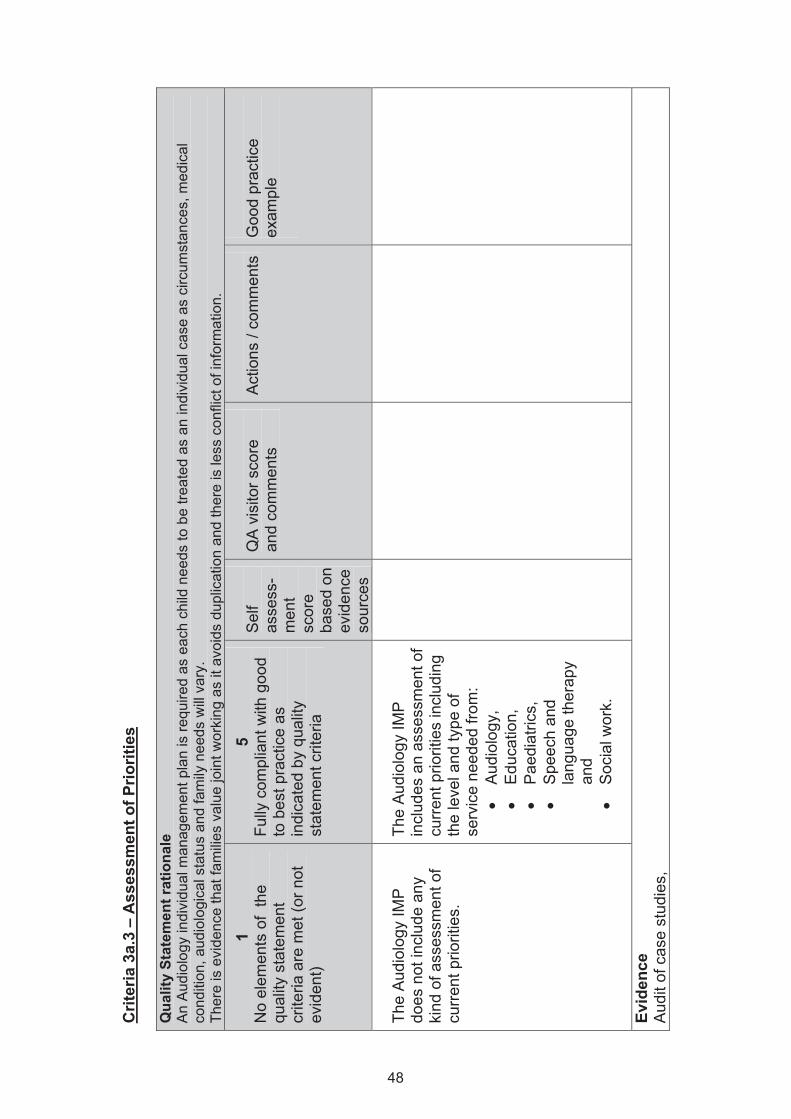
Crit
eria
3a.
3 –
Ass
essm
ent o
f Prio
ritie
s Q
ualit
y St
atem
ent r
atio
nale
A
n A
udio
logy
indi
vidu
al m
anag
emen
t pla
n is
requ
ired
as e
ach
child
nee
ds to
be
treat
ed a
s an
indi
vidu
al c
ase
as c
ircum
stan
ces,
med
ical
co
nditi
on, a
udio
logi
cal s
tatu
s an
d fa
mily
nee
ds w
ill v
ary.
Th
ere
is e
vide
nce
that
fam
ilies
val
ue jo
int w
orki
ng a
s it
avoi
ds d
uplic
atio
n an
d th
ere
is le
ss c
onfli
ct o
f inf
orm
atio
n.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
Aud
iolo
gy IM
P
does
not
incl
ude
any
kind
of a
sses
smen
t of
curr
ent p
riorit
ies.
The
Aud
iolo
gy IM
P
incl
udes
an
asse
ssm
ent o
f cu
rrent
prio
ritie
s in
clud
ing
the
leve
l and
type
of
serv
ice
need
ed fr
om:
• A
udio
logy
, •
Edu
catio
n,
• P
aedi
atric
s,
• S
peec
h an
d la
ngua
ge th
erap
y an
d •
Soc
ial w
ork.
Evid
ence
A
udit
of c
ase
stud
ies,
48
Rec
ords
of i
ndiv
idua
l man
agem
ent p
lans
, D
ocum
ente
d pl
ans
49
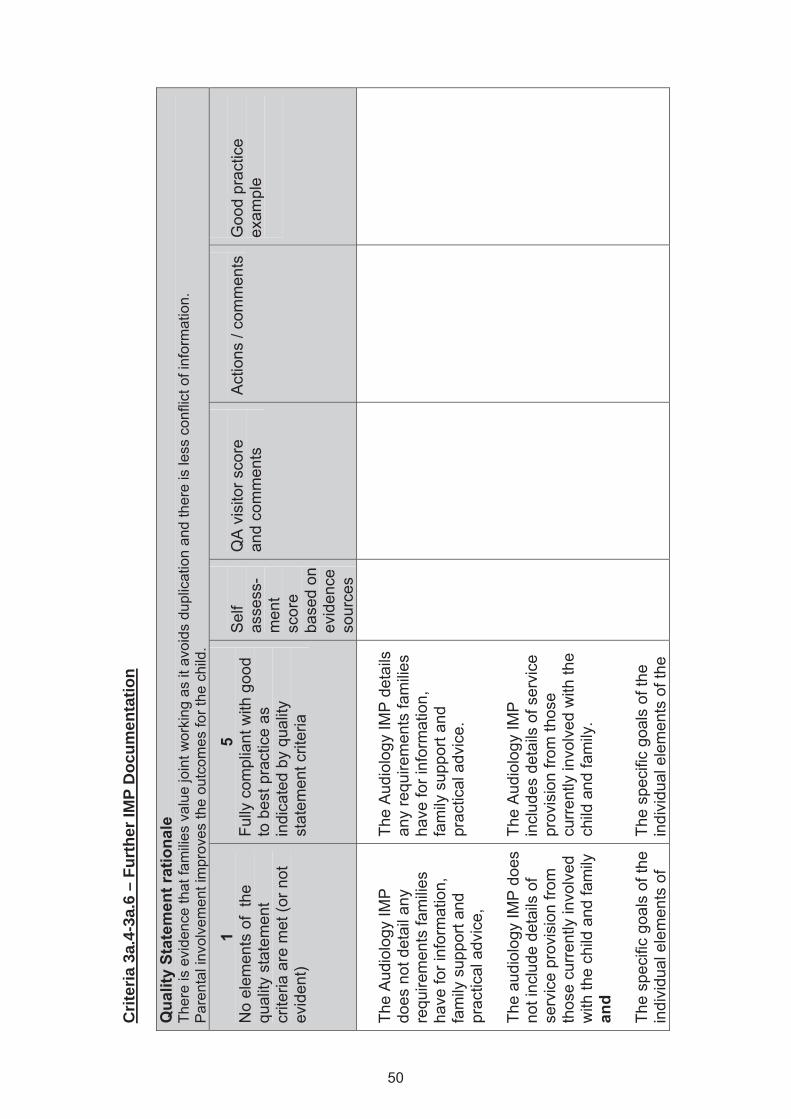
Qua
lity
Stat
emen
t rat
iona
le
Ther
e is
evi
denc
e th
at fa
mili
es v
alue
join
t wor
king
as
it av
oids
dup
licat
ion
and
ther
e is
less
con
flict
of i
nfor
mat
ion.
P
aren
tal i
nvol
vem
ent i
mpr
oves
the
outc
omes
for t
he c
hild
.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
Aud
iolo
gy IM
P
does
not
det
ail a
ny
requ
irem
ents
fam
ilies
have
for i
nfor
mat
ion,
fa
mily
sup
port
and
prac
tical
adv
ice,
Th
e au
diol
ogy
IMP
doe
s no
t inc
lude
det
ails
of
serv
ice
prov
isio
n fro
m
thos
e cu
rrent
ly in
volv
ed
with
the
child
and
fam
ily
and
The
spec
ific
goal
s of
the
indi
vidu
al e
lem
ents
of
The
Aud
iolo
gy IM
P d
etai
ls
any
requ
irem
ents
fam
ilies
have
for i
nfor
mat
ion,
fa
mily
sup
port
and
prac
tical
adv
ice.
Th
e A
udio
logy
IMP
in
clud
es d
etai
ls o
f ser
vice
pr
ovis
ion
from
thos
e cu
rren
tly in
volv
ed w
ith th
e ch
ild a
nd fa
mily
. Th
e sp
ecifi
c go
als
of th
e in
divi
dual
ele
men
ts o
f the
50
Crit
eria
3a.
4-3a
.6 –
Fur
ther
IMP
Doc
umen
tatio
n
the
IMP
and
thei
r tim
ing
are
not d
ocum
ente
d an
d ci
rcul
ated
to a
ny
othe
r mem
bers
of t
he
team
.
IMP
and
thei
r tim
ing
are
docu
men
ted
and
circ
ulat
ed to
all
mem
bers
of
the
team
.
Evid
ence
A
udit
of c
ase
stud
ies,
R
ecor
ds o
f ind
ivid
ual m
anag
emen
t pla
ns
51
Sta
ndar
d 4
– Im
plem
entin
g an
Aud
iolo
gy In
divi
dual
Man
agem
ent P
lan
4a. T
he A
udio
logy
Indi
vidu
al M
anag
emen
t Pla
n is
impl
emen
ted
for e
ach
child
and
revi
ewed
at s
ubse
quen
t app
oint
men
ts.
4b. W
here
pro
visi
on o
f hea
ring
aid(
s) is
requ
ired,
the
serv
ice
ensu
res:
•
hear
ing
aids
fitte
d ar
e fu
nctio
ning
cor
rect
ly,
• na
tiona
lly a
gree
d pr
oced
ures
and
pro
toco
ls a
re fo
llow
ed a
t a lo
cal l
evel
and
•
perfo
rman
ce o
r hea
ring
aid(
s) is
car
eful
ly m
atch
ed to
indi
vidu
al re
quire
men
ts a
nd s
ettin
gs a
re re
cord
ed.
Rat
ing
Scal
e 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2 Fe
w e
lem
ents
of
the
qual
ity
stat
emen
t crit
eria
ar
e m
et
3 M
eets
aro
und
half
of th
e el
emen
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
4 A
lmos
t ful
ly m
eets
th
e qu
ality
st
atem
ent c
riter
ia
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Plea
se u
se th
e ra
ting
scal
e an
d ex
ampl
es g
iven
in th
e 1
and
5 co
lum
ns a
s an
indi
cato
r to
help
you
sco
re th
e se
lf-as
sess
men
t tab
le
belo
w. E
ach
tabl
e sh
ould
onl
y ev
er h
ave
1 se
lf-as
sess
men
t sco
re. W
hen
you
perc
eive
ther
e to
be
mor
e th
an 1
asp
ect o
f the
tabl
e th
at
you
coul
d gi
ve a
sco
re fo
r, pl
ease
use
an
aver
age
of e
ach
of th
e as
pect
s.
52
Crit
eria
4a.
1 –
Reg
ular
ly U
pdat
ed O
bjec
tives
Q
ualit
y St
atem
ent r
atio
nale
R
egul
ar re
visi
on a
llow
s th
e m
anag
emen
t pla
n to
be
resp
onsi
ve to
the
child
’s c
hang
ing
need
s. It
als
o gi
ves
the
plan
the
flexi
bilit
y to
inco
rpor
ate
addi
tiona
l inf
orm
atio
n fo
r the
ben
efit
of th
e ch
ild’s
man
agem
ent.
Pla
nned
and
coo
rdin
ated
inte
rven
tion
lead
s to
bet
ter o
utco
mes
.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
Aud
iolo
gy IM
P
does
not
, at a
ny s
tage
, in
clud
e a
set o
f ac
hiev
able
obj
ectiv
es.
The
Aud
iolo
gy IM
P
incl
udes
a s
et o
f ac
hiev
able
obj
ectiv
es
whi
ch a
re re
view
ed a
nd
upda
ted
regu
larly
.
Evid
ence
R
ecor
ds fr
om m
anag
emen
t pla
n,
Cas
e A
udit
53
Crit
eria
4b.
1-4b
.7 -
Verif
icat
ion
of H
earin
g A
ids
Qua
lity
Stat
emen
t rat
iona
le
Aud
iolo
gist
s en
sure
that
the
aid
is w
orki
ng to
spe
cific
atio
n be
fore
fitti
ng it
to a
chi
ld s
o th
at th
e ai
d do
es n
ot c
ause
har
m.
Pro
fess
iona
l bod
ies
and
natio
nal g
uide
lines
are
follo
wed
to e
nsur
e pr
ovis
ion
mee
ts th
e ne
eds
of th
e in
divi
dual
. E
vide
nce
sugg
ests
that
hea
ring
aids
are
mos
t effe
ctiv
e w
hen
thei
r per
form
ance
is c
aref
ully
mat
ched
to th
e re
quire
men
ts o
f the
in
divi
dual
.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Hea
ring
aids
nev
er
have
thei
r tec
hnic
al
perfo
rman
ce te
sted
to
spec
ifica
tion.
Prio
r to
issu
e ev
ery
hear
ing
aid
has
its
tech
nica
l per
form
ance
te
sted
to s
peci
ficat
ion.
Lo
cal p
roto
cols
whi
ch
com
ply
with
the
late
st
prof
essi
onal
bod
ies’
and
na
tiona
l gui
danc
e ar
e in
op
erat
ion
conc
erni
ng
sele
ctio
n, fi
tting
and
ve
rific
atio
n of
hea
ring
aids
.
54
Rea
l Ear
Mea
sure
men
t (R
EM
) / R
eal E
ar to
C
oupl
er D
iffer
ence
(R
EC
D) o
f hea
ring
aid
perfo
rman
ce is
use
d to
ve
rify
at le
ast 9
5% o
f he
arin
g ai
d fit
tings
, un
less
cl
inic
ally
con
train
dica
ted
for i
ndiv
idua
l chi
ldre
n.
Whe
re R
EM
/ R
EC
D is
pe
rform
ed, t
he a
cous
tical
ta
rget
is v
erifi
ed a
t thr
ee
diffe
rent
inpu
t lev
els
(50,
65
and
80
dB) i
n m
ore
than
95%
of c
ases
. W
here
RE
M /
RE
CD
is
perfo
rmed
, mea
sure
men
ts
do n
ot d
evia
te fr
om th
e re
com
men
ded
targ
et a
t m
ore
than
one
freq
uenc
y (in
95%
of c
ases
) unl
ess
clin
ical
ly in
dica
ted
Whe
re R
EM
/ R
EC
D is
not
po
ssib
le, c
urre
nt
inte
rnat
iona
lly-r
ecog
nise
d ag
e-re
late
d pr
edic
ted
55
valu
es a
re u
sed
in h
earin
g ai
d ve
rific
atio
n.
Whe
n R
EM
/RE
CD
is n
ot
atte
mpt
ed/ c
ompl
eted
an
expl
anat
ion
is re
cord
ed in
th
e A
udio
logy
IMP
.
Evid
ence
R
ecor
ds fr
om m
anag
emen
t pla
n,
Cas
e A
udit;
In
terv
iew
s w
ith p
aren
ts
56
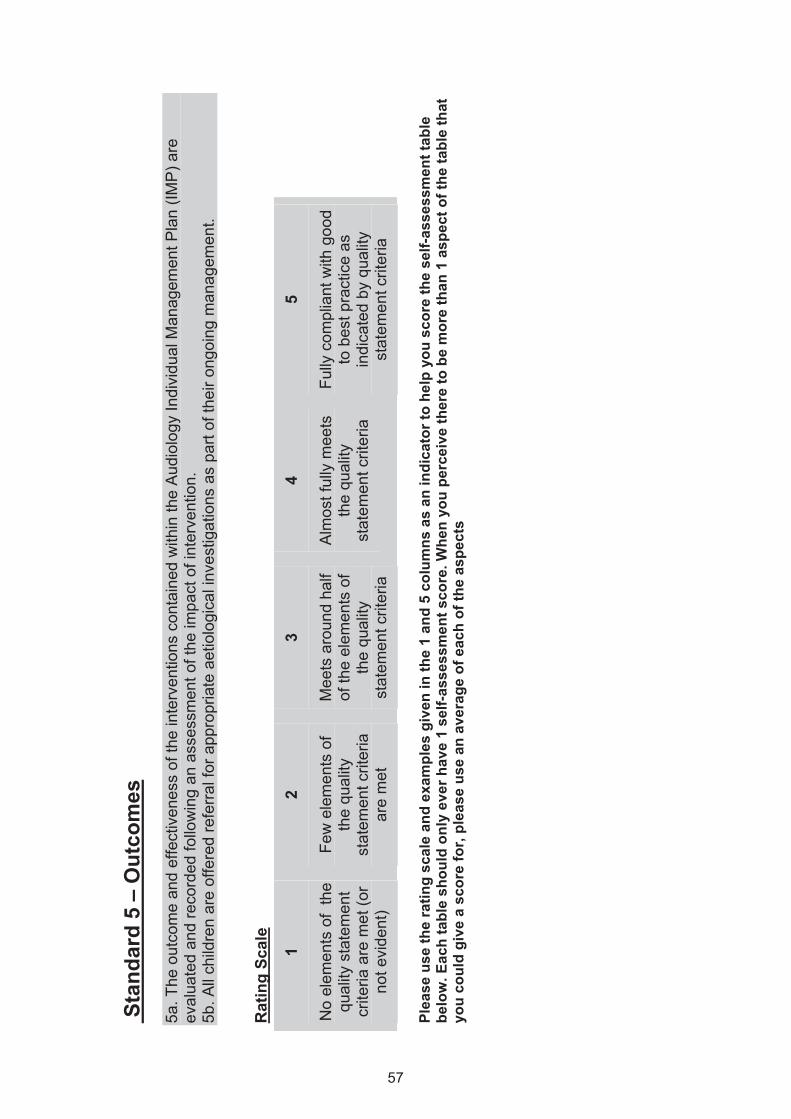
Sta
ndar
d 5
– O
utco
mes
5a
. The
out
com
e an
d ef
fect
iven
ess
of th
e in
terv
entio
ns c
onta
ined
with
in th
e A
udio
logy
Indi
vidu
al M
anag
emen
t Pla
n (IM
P) a
re
eval
uate
d an
d re
cord
ed fo
llow
ing
an a
sses
smen
t of t
he im
pact
of i
nter
vent
ion.
5b
. All
child
ren
are
offe
red
refe
rral
for a
ppro
pria
te a
etio
logi
cal i
nves
tigat
ions
as
part
of th
eir o
ngoi
ng m
anag
emen
t.
Rat
ing
Scal
e
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts
57
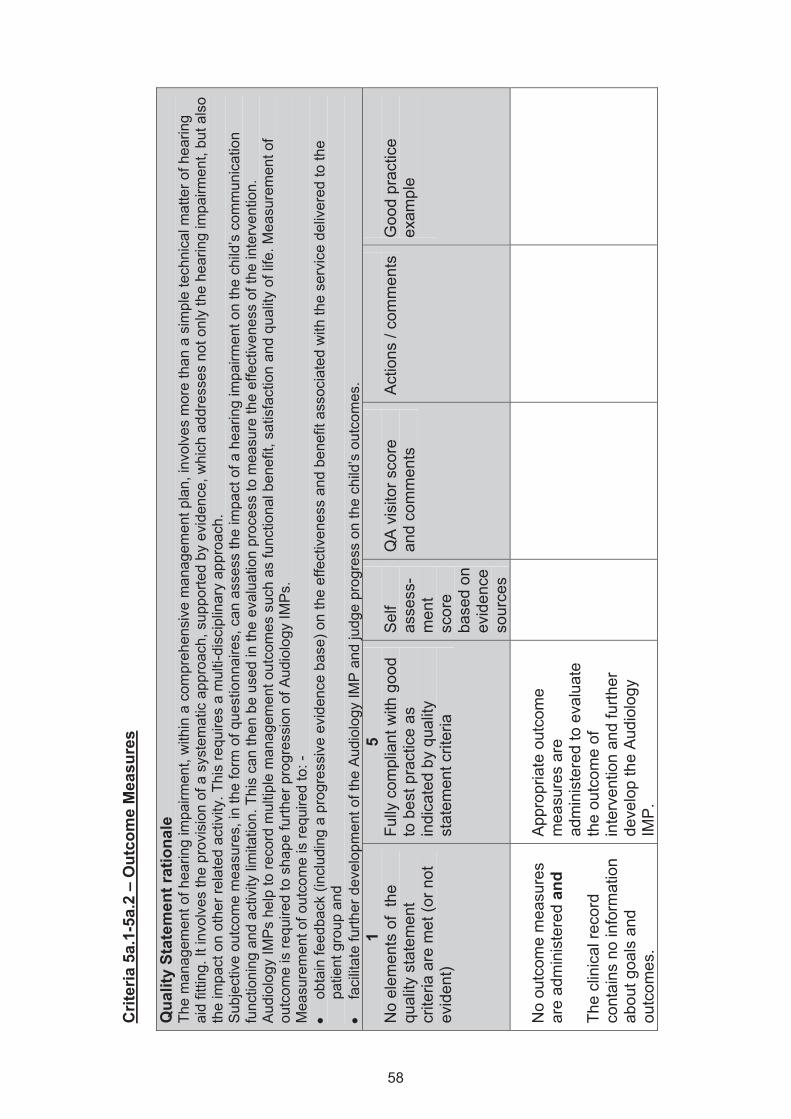
Crit
eria
5a.
1-5a
.2 –
Out
com
e M
easu
res
Qua
lity
Stat
emen
t rat
iona
le
The
man
agem
ent o
f hea
ring
impa
irmen
t, w
ithin
a c
ompr
ehen
sive
man
agem
ent p
lan,
invo
lves
mor
e th
an a
sim
ple
tech
nica
l mat
ter o
f hea
ring
aid
fittin
g. It
invo
lves
the
prov
isio
n of
a s
yste
mat
ic a
ppro
ach,
sup
porte
d by
evi
denc
e, w
hich
add
ress
es n
ot o
nly
the
hear
ing
impa
irmen
t, bu
t als
o th
e im
pact
on
othe
r rel
ated
act
ivity
. Thi
s re
quire
s a
mul
ti-di
scip
linar
y ap
proa
ch.
Sub
ject
ive
outc
ome
mea
sure
s, in
the
form
of q
uest
ionn
aire
s, c
an a
sses
s th
e im
pact
of a
hea
ring
impa
irmen
t on
the
child
’s c
omm
unic
atio
n fu
nctio
ning
and
act
ivity
lim
itatio
n. T
his
can
then
be
used
in th
e ev
alua
tion
proc
ess
to m
easu
re th
e ef
fect
iven
ess
of th
e in
terv
entio
n.
A
udio
logy
IMP
s he
lp to
reco
rd m
ultip
le m
anag
emen
t out
com
es s
uch
as fu
nctio
nal b
enef
it, s
atis
fact
ion
and
qual
ity o
f life
. Mea
sure
men
t of
outc
ome
is re
quire
d to
sha
pe fu
rther
pro
gres
sion
of A
udio
logy
IMP
s.
Mea
sure
men
t of o
utco
me
is re
quire
d to
: -
• ob
tain
feed
back
(inc
ludi
ng a
pro
gres
sive
evi
denc
e ba
se) o
n th
e ef
fect
iven
ess
and
bene
fit a
ssoc
iate
d w
ith th
e se
rvic
e de
liver
ed to
the
patie
nt g
roup
and
•
faci
litat
e fu
rther
dev
elop
men
t of t
he A
udio
logy
IMP
and
judg
e pr
ogre
ss o
n th
e ch
ild’s
out
com
es.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
No
outc
ome
mea
sure
s ar
e ad
min
iste
red
and
The
clin
ical
reco
rd
cont
ains
no
info
rmat
ion
abou
t goa
ls a
nd
outc
omes
.
App
ropr
iate
out
com
e m
easu
res
are
adm
inis
tere
d to
eva
luat
e th
e ou
tcom
e of
in
terv
entio
n an
d fu
rther
de
velo
p th
e A
udio
logy
IM
P.
58
Clin
ical
reco
rds
are
used
to
faci
litat
e fu
rther
de
velo
pmen
t and
m
onito
ring
of c
hild
ren’
s pr
ogre
ss. T
he re
cord
s co
ntai
n in
form
atio
n ab
out
the
exte
nt to
whi
ch th
e in
terv
entio
ns h
elpe
d m
eet
the
spec
ified
goa
ls
(out
com
es) a
nd d
ocum
ent
info
rmat
ion
abou
t how
ea
ch e
lem
ent o
f the
A
udio
logy
IMP
has
bee
n im
plem
ente
d, in
clud
ing
reas
ons
for c
hang
es o
r om
issi
ons.
Ev
iden
ce
Cas
e au
dit,
Rec
ords
from
man
agem
ent p
lan
59
Crit
eria
5b.
1-5b
.3 –
Aet
iolo
gica
l Inv
estig
atio
ns
Qua
lity
Stat
emen
t rat
iona
le
The
outc
ome
of a
etio
logi
cal i
nves
tigat
ions
, as
part
of th
e on
goin
g m
anag
emen
t, m
ay le
ad to
a b
ette
r und
erst
andi
ng a
nd m
anag
emen
t of n
ot
only
the
hear
ing
loss
but
als
o th
e w
hole
chi
ld. I
t may
als
o pr
ovid
e an
opp
ortu
nity
to id
entif
y co
-exi
stin
g m
edic
al c
ondi
tions
and
pre
vent
furth
er
dete
riora
tion
of th
ese
and
the
hear
ing
loss
in s
ome
case
s.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ther
e ar
e no
loca
l gu
idel
ines
in p
lace
re
gard
ing
aetio
logi
cal
inve
stig
atio
ns a
nd
Out
com
es fr
om
inve
stig
atio
ns a
re n
ot
reco
rded
in th
e ch
ild’s
m
edic
al re
cord
s or
ou
tcom
es a
re n
ot
shar
ed w
ith a
ny
mem
bers
of t
he
mul
tidis
cipl
inar
y te
am.
Loca
l ref
erra
l gui
delin
es
are
in p
lace
rega
rdin
g ae
tiolo
gica
l inv
estig
atio
ns
for c
hild
ren
with
hea
ring
loss
. Lo
cal g
uide
lines
, whi
ch
refle
ct n
atio
nal
guid
elin
es, a
re in
pla
ce
rega
rdin
g ae
tiolo
gica
l in
vest
igat
ions
for c
hild
ren
with
hea
ring
loss
.
Out
com
es fr
om
inve
stig
atio
ns a
re
60
docu
men
ted
in th
e A
udio
logy
IMP
and
, as
appr
opria
te a
nd w
ith th
e fa
mily
’s p
erm
issi
on,
shar
ed w
ith o
ther
m
embe
rs o
f the
m
ultid
isci
plin
ary
team
.
Evid
ence
Lo
cal g
uide
lines
M
edic
al re
cord
s
61
Stan
dard
6 –
Pro
fess
iona
l Com
pete
nce
6a. E
ach
audi
olog
y se
rvic
e de
mon
stra
tes
that
with
in th
eir t
eam
they
hav
e th
e cl
inic
al c
ompe
tenc
ies
nece
ssar
y to
sup
port
the
asse
ssm
ents
and
inte
rven
tions
they
und
erta
ke.
Rat
ing
Scal
e
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts.
62
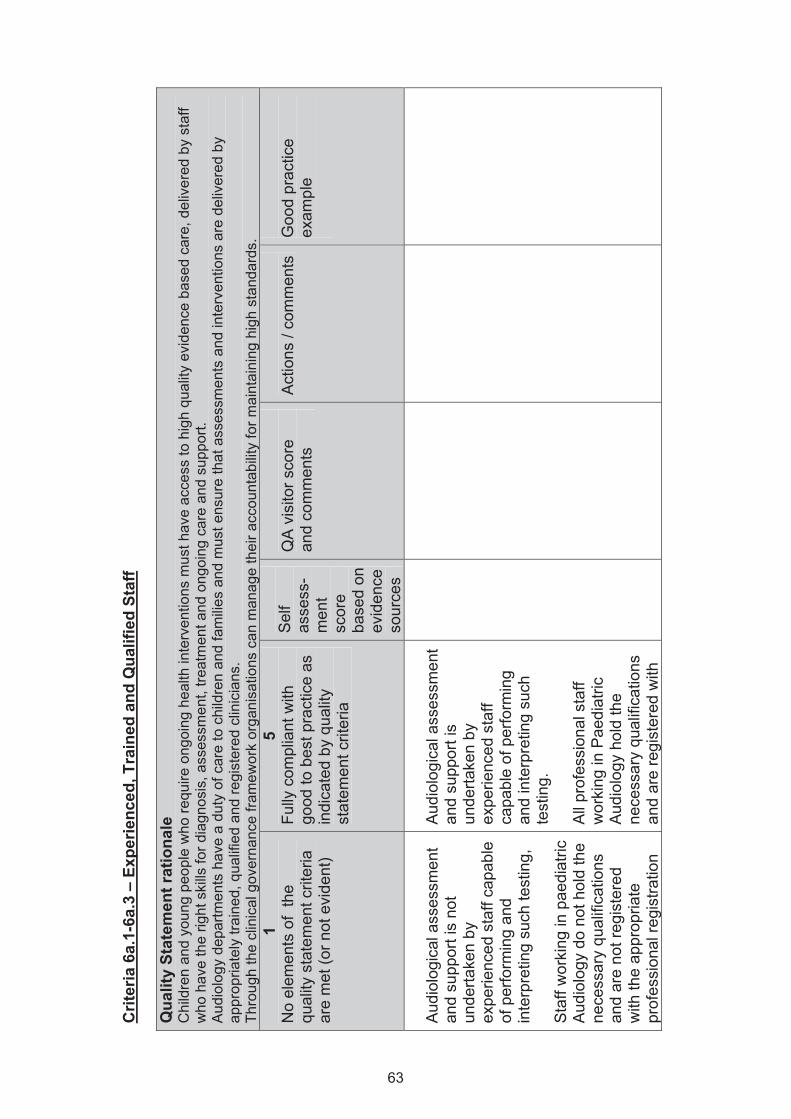
Crit
eria
6a.
1-6a
.3 –
Exp
erie
nced
, Tra
ined
and
Qua
lifie
d St
aff
Qua
lity
Stat
emen
t rat
iona
le
Chi
ldre
n an
d yo
ung
peop
le w
ho re
quire
ong
oing
hea
lth in
terv
entio
ns m
ust h
ave
acce
ss to
hig
h qu
ality
evi
denc
e ba
sed
care
, del
iver
ed b
y st
aff
who
hav
e th
e rig
ht s
kills
for d
iagn
osis
, ass
essm
ent,
treat
men
t and
ong
oing
car
e an
d su
ppor
t. A
udio
logy
dep
artm
ents
hav
e a
duty
of c
are
to c
hild
ren
and
fam
ilies
and
mus
t ens
ure
that
ass
essm
ents
and
inte
rven
tions
are
del
iver
ed b
y ap
prop
riate
ly tr
aine
d, q
ualif
ied
and
regi
ster
ed c
linic
ians
. Th
roug
h th
e cl
inic
al g
over
nanc
e fra
mew
ork
orga
nisa
tions
can
man
age
thei
r acc
ount
abili
ty fo
r mai
ntai
ning
hig
h st
anda
rds.
1
No
elem
ents
of
the
qual
ity s
tate
men
t crit
eria
ar
e m
et (o
r not
evi
dent
)
5 Fu
lly c
ompl
iant
with
go
od to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Aud
iolo
gica
l ass
essm
ent
and
supp
ort i
s no
t un
derta
ken
by
expe
rienc
ed s
taff
capa
ble
of p
erfo
rmin
g an
d in
terp
retin
g su
ch te
stin
g,
Sta
ff w
orki
ng in
pae
diat
ric
Aud
iolo
gy d
o no
t hol
d th
e ne
cess
ary
qual
ifica
tions
an
d ar
e no
t reg
iste
red
with
the
appr
opria
te
prof
essi
onal
regi
stra
tion
Aud
iolo
gica
l ass
essm
ent
and
supp
ort i
s un
derta
ken
by
expe
rienc
ed s
taff
capa
ble
of p
erfo
rmin
g an
d in
terp
retin
g su
ch
test
ing.
A
ll pr
ofes
sion
al s
taff
wor
king
in P
aedi
atric
A
udio
logy
hol
d th
e ne
cess
ary
qual
ifica
tions
an
d ar
e re
gist
ered
with
63
body
and
S
taff
in s
enio
r pos
ition
s ar
e no
t tra
ined
to p
ost-
grad
uate
leve
l and
do
not
have
pra
ctic
al e
xper
ienc
e in
pae
diat
ric a
udio
logy
.
the
appr
opria
te
prof
essi
onal
regi
stra
tion
body
. S
taff
in s
enio
r pos
ition
s ar
e tra
ined
to p
ost-
grad
uate
leve
l su
pple
men
ted
by
suita
bly
asse
ssed
pr
actic
al e
xper
ienc
e in
P
aedi
atric
Aud
iolo
gy.
Evid
ence
C
PD
evi
denc
e,
Cer
tific
ates
of a
ttend
ance
at t
rain
ing,
Q
ualif
icat
ion
Cer
tific
ates
64
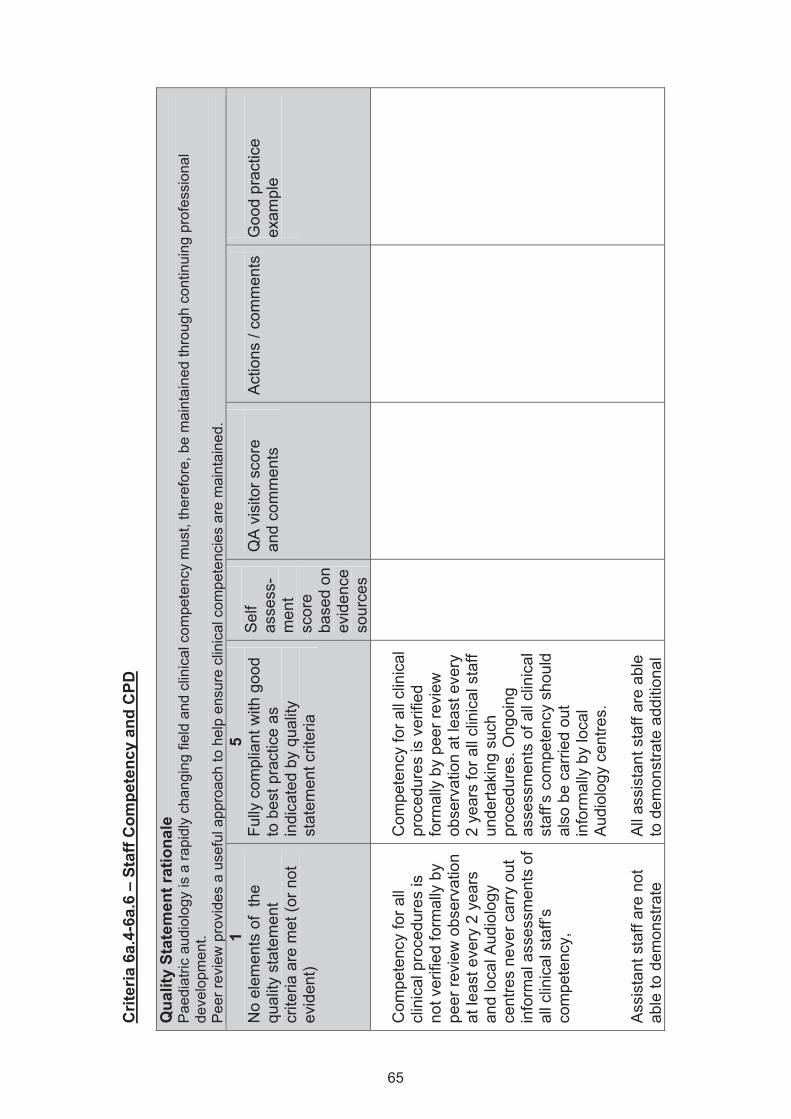
Crit
eria
6a.
4-6a
.6 –
Sta
ff C
ompe
tenc
y an
d C
PD
Qua
lity
Stat
emen
t rat
iona
le
Pae
diat
ric a
udio
logy
is a
rapi
dly
chan
ging
fiel
d an
d cl
inic
al c
ompe
tenc
y m
ust,
ther
efor
e, b
e m
aint
aine
d th
roug
h co
ntin
uing
pro
fess
iona
l de
velo
pmen
t. P
eer r
evie
w p
rovi
des
a us
eful
app
roac
h to
hel
p en
sure
clin
ical
com
pete
ncie
s ar
e m
aint
aine
d.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Com
pete
ncy
for a
ll cl
inic
al p
roce
dure
s is
no
t ver
ified
form
ally
by
peer
revi
ew o
bser
vatio
n at
leas
t eve
ry 2
yea
rs
and
loca
l Aud
iolo
gy
cent
res
neve
r car
ry o
ut
info
rmal
ass
essm
ents
of
all c
linic
al s
taff’
s co
mpe
tenc
y,
Ass
ista
nt s
taff
are
not
able
to d
emon
stra
te
Com
pete
ncy
for a
ll cl
inic
al
proc
edur
es is
ver
ified
fo
rmal
ly b
y pe
er re
view
ob
serv
atio
n at
leas
t eve
ry
2 ye
ars
for a
ll cl
inic
al s
taff
unde
rtaki
ng s
uch
proc
edur
es. O
ngoi
ng
asse
ssm
ents
of a
ll cl
inic
al
staf
f’s c
ompe
tenc
y sh
ould
al
so b
e ca
rried
out
in
form
ally
by
loca
l A
udio
logy
cen
tres.
All
assi
stan
t sta
ff ar
e ab
le
to d
emon
stra
te a
dditi
onal
65

addi
tiona
l com
pete
ncy
train
ing
in p
aedi
atric
au
diol
ogy
and
cann
ot
dem
onst
rate
con
tinui
ng
prof
essi
onal
de
velo
pmen
t (C
PD
) in
the
area
s th
ey a
re
curre
ntly
wor
king
and
. S
taff
do n
ot h
ave
basi
c tra
inin
g in
chi
ld
prot
ectio
n an
d de
af
awar
enes
s.
com
pete
ncy
train
ing
in
paed
iatri
c au
diol
ogy
alon
g w
ith c
ontin
uing
pr
ofes
sion
al d
evel
opm
ent
(CP
D) i
n th
e ar
eas
in
whi
ch th
ey a
re c
urre
ntly
w
orki
ng.
All
staf
f hav
e ba
sic
train
ing
in c
hild
pro
tect
ion
and
deaf
aw
aren
ess.
Evid
ence
W
ritte
n do
cum
enta
tion
of p
eer r
evie
w a
sses
smen
ts
CP
D e
vide
nce,
66
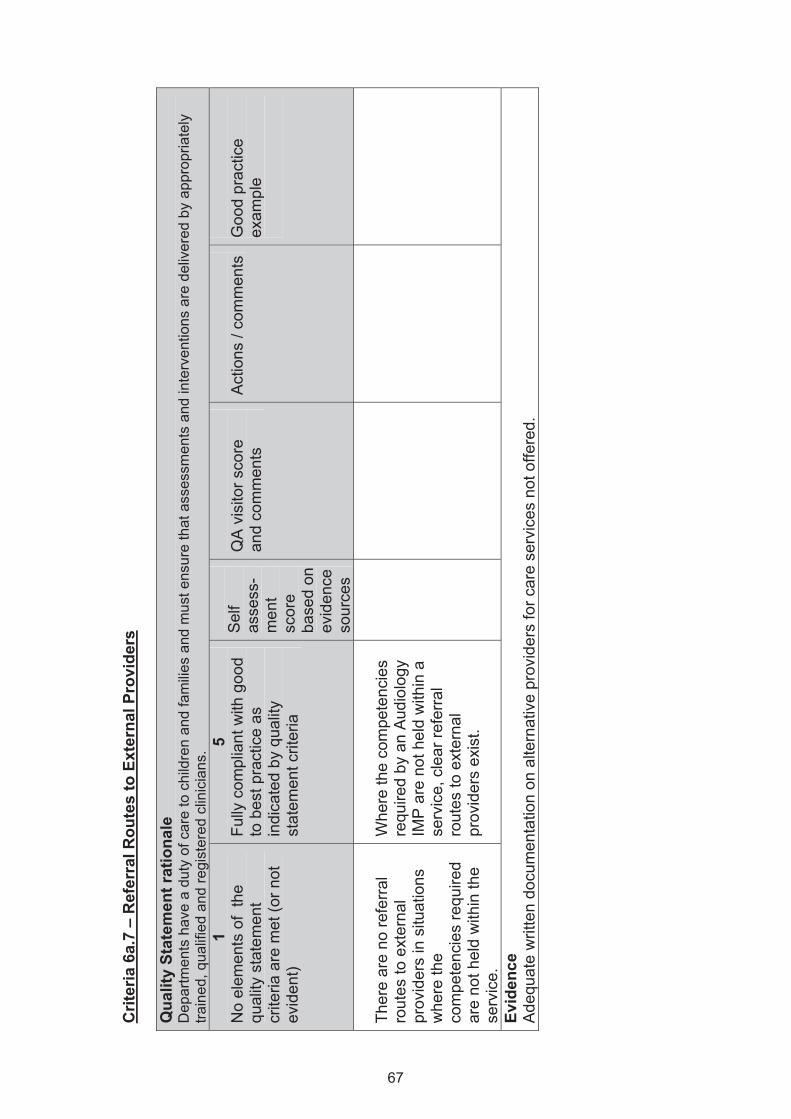
Crit
eria
6a.
7 –
Ref
erra
l Rou
tes
to E
xter
nal P
rovi
ders
Q
ualit
y St
atem
ent r
atio
nale
D
epar
tmen
ts h
ave
a du
ty o
f car
e to
chi
ldre
n an
d fa
mili
es a
nd m
ust e
nsur
e th
at a
sses
smen
ts a
nd in
terv
entio
ns a
re d
eliv
ered
by
appr
opria
tely
tra
ined
, qua
lifie
d an
d re
gist
ered
clin
icia
ns.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ther
e ar
e no
refe
rral
rout
es to
ext
erna
l pr
ovid
ers
in s
ituat
ions
w
here
the
com
pete
ncie
s re
quire
d ar
e no
t hel
d w
ithin
the
serv
ice.
Whe
re th
e co
mpe
tenc
ies
requ
ired
by a
n A
udio
logy
IM
P a
re n
ot h
eld
with
in a
se
rvic
e, c
lear
refe
rral
ro
utes
to e
xter
nal
prov
ider
s ex
ist.
Evid
ence
A
dequ
ate
writ
ten
docu
men
tatio
n on
alte
rnat
ive
prov
ider
s fo
r car
e se
rvic
es n
ot o
ffere
d.
67
Stan
dard
7 –
Info
rmat
ion
Prov
isio
n an
d C
omm
unic
atio
n w
ith C
hild
ren
and
Fam
ilies
7a
. Eac
h se
rvic
e ha
s in
pla
ce p
roce
sses
and
stru
ctur
es to
faci
litat
e co
mm
unic
atio
n w
ith c
hild
ren
and
fam
ilies.
R
atin
g Sc
ale
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts.
68
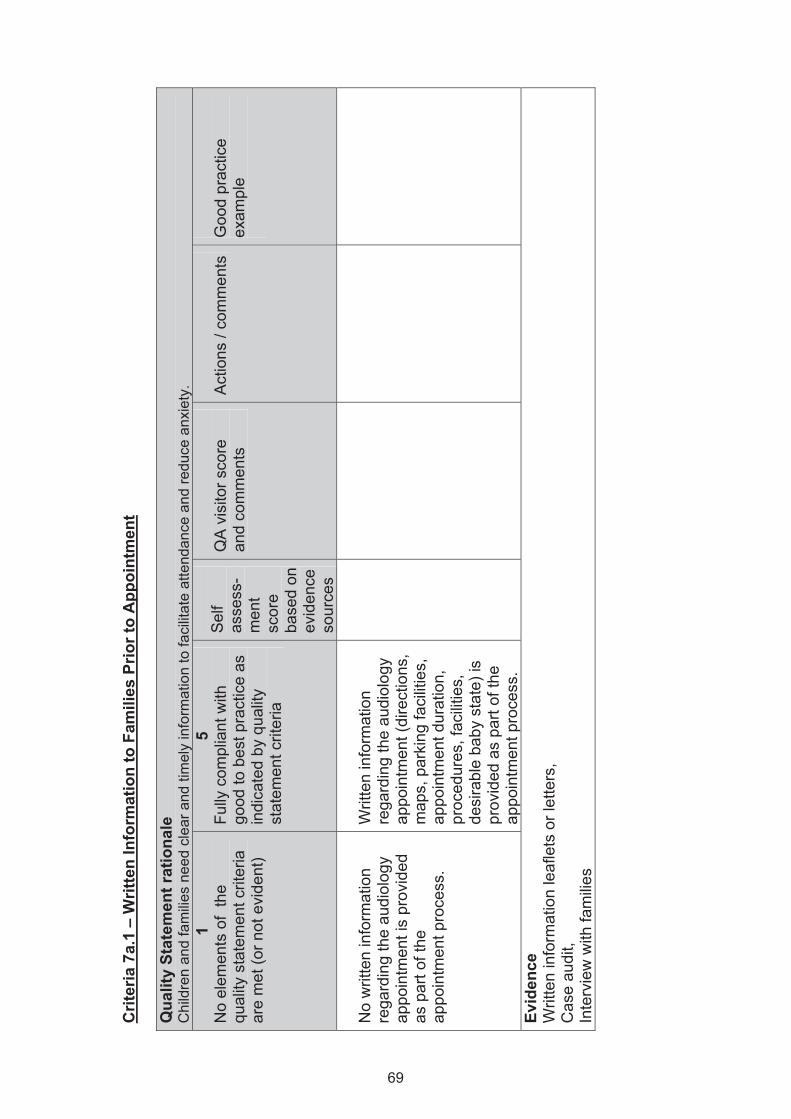
Crit
eria
7a.
1 –
Writ
ten
Info
rmat
ion
to F
amili
es P
rior t
o A
ppoi
ntm
ent
Qua
lity
Stat
emen
t rat
iona
le
Chi
ldre
n an
d fa
mili
es n
eed
clea
r and
tim
ely
info
rmat
ion
to fa
cilit
ate
atte
ndan
ce a
nd re
duce
anx
iety
. 1
No
elem
ents
of
the
qual
ity s
tate
men
t crit
eria
ar
e m
et (o
r not
evi
dent
)
5 Fu
lly c
ompl
iant
with
go
od to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
No
writ
ten
info
rmat
ion
rega
rdin
g th
e au
diol
ogy
appo
intm
ent i
s pr
ovid
ed
as p
art o
f the
ap
poin
tmen
t pro
cess
.
Writ
ten
info
rmat
ion
rega
rdin
g th
e au
diol
ogy
appo
intm
ent (
dire
ctio
ns,
map
s, p
arki
ng fa
cilit
ies,
ap
poin
tmen
t dur
atio
n,
proc
edur
es, f
acilit
ies,
de
sira
ble
baby
sta
te) i
s pr
ovid
ed a
s pa
rt of
the
appo
intm
ent p
roce
ss.
Evid
ence
W
ritte
n in
form
atio
n le
afle
ts o
r let
ters
, C
ase
audi
t, In
terv
iew
with
fam
ilies
69
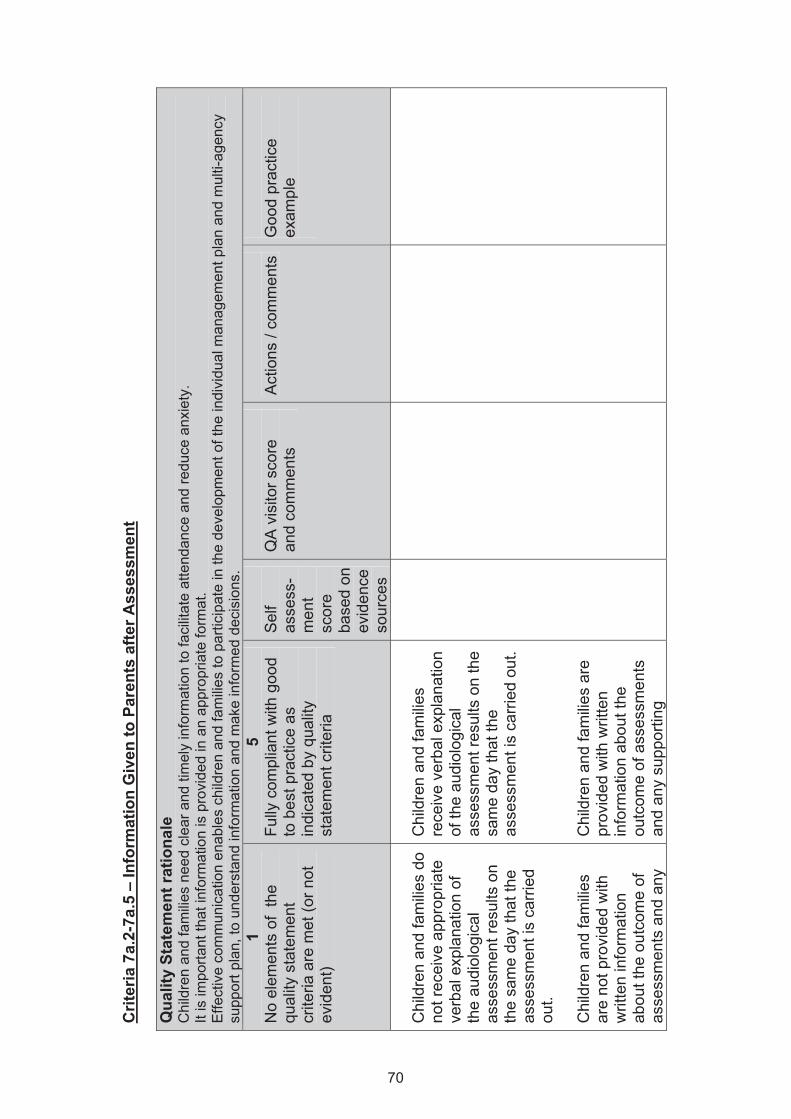
Crit
eria
7a.
2-7a
.5 –
Info
rmat
ion
Giv
en to
Par
ents
afte
r Ass
essm
ent
Qua
lity
Stat
emen
t rat
iona
le
Chi
ldre
n an
d fa
mili
es n
eed
clea
r and
tim
ely
info
rmat
ion
to fa
cilit
ate
atte
ndan
ce a
nd re
duce
anx
iety
. It
is im
porta
nt th
at in
form
atio
n is
pro
vide
d in
an
appr
opria
te fo
rmat
. E
ffect
ive
com
mun
icat
ion
enab
les
child
ren
and
fam
ilies
to p
artic
ipat
e in
the
deve
lopm
ent o
f the
indi
vidu
al m
anag
emen
t pla
n an
d m
ulti-
agen
cy
supp
ort p
lan,
to u
nder
stan
d in
form
atio
n an
d m
ake
info
rmed
dec
isio
ns.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Chi
ldre
n an
d fa
milie
s do
no
t rec
eive
app
ropr
iate
ve
rbal
exp
lana
tion
of
the
audi
olog
ical
as
sess
men
t res
ults
on
the
sam
e da
y th
at th
e as
sess
men
t is
carr
ied
out.
Chi
ldre
n an
d fa
milie
s ar
e no
t pro
vide
d w
ith
writ
ten
info
rmat
ion
abou
t the
out
com
e of
as
sess
men
ts a
nd a
ny
Chi
ldre
n an
d fa
milie
s re
ceiv
e ve
rbal
exp
lana
tion
of th
e au
diol
ogic
al
asse
ssm
ent r
esul
ts o
n th
e sa
me
day
that
the
asse
ssm
ent i
s ca
rrie
d ou
t. C
hild
ren
and
fam
ilies
are
prov
ided
with
writ
ten
info
rmat
ion
abou
t the
ou
tcom
e of
ass
essm
ents
an
d an
y su
ppor
ting
70
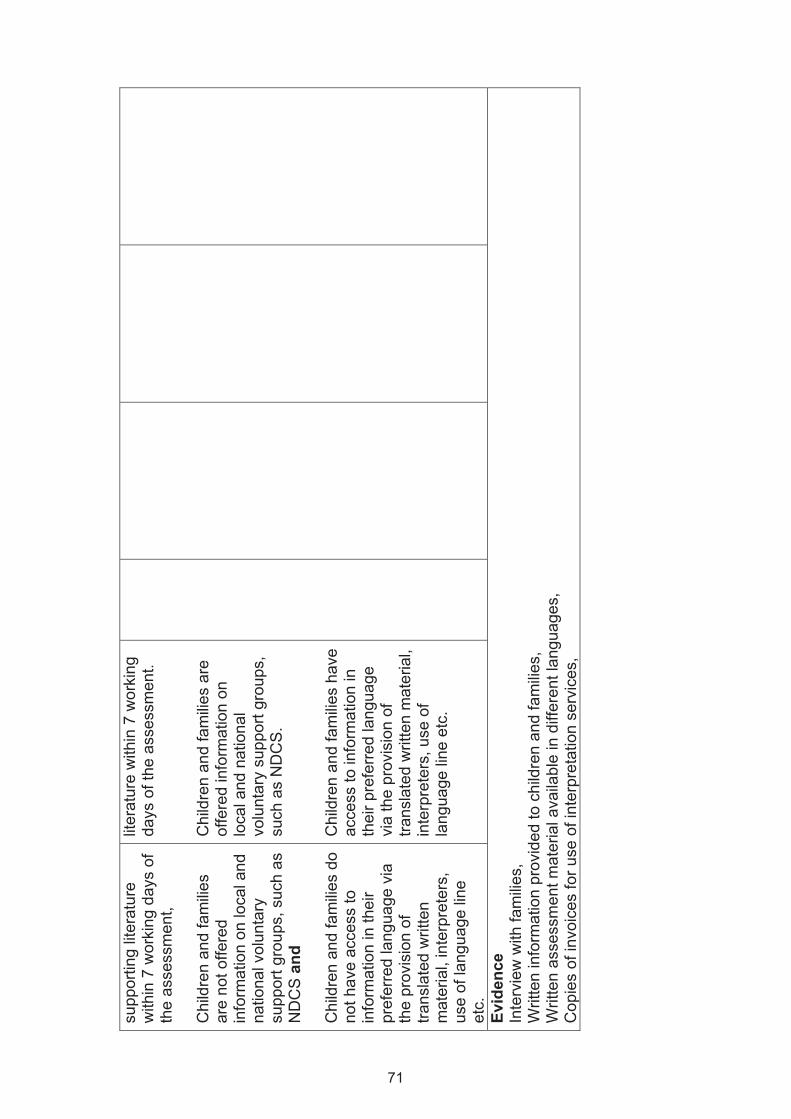
supp
ortin
g lit
erat
ure
with
in 7
wor
king
day
s of
th
e as
sess
men
t, C
hild
ren
and
fam
ilies
are
not o
ffere
d in
form
atio
n on
loca
l and
na
tiona
l vol
unta
ry
supp
ort g
roup
s, s
uch
as
ND
CS
and
C
hild
ren
and
fam
ilies
do
not h
ave
acce
ss to
in
form
atio
n in
thei
r pr
efer
red
lang
uage
via
th
e pr
ovis
ion
of
trans
late
d w
ritte
n m
ater
ial,
inte
rpre
ters
, us
e of
lang
uage
line
et
c.
liter
atur
e w
ithin
7 w
orki
ng
days
of t
he a
sses
smen
t.
Chi
ldre
n an
d fa
milie
s ar
e of
fere
d in
form
atio
n on
lo
cal a
nd n
atio
nal
volu
ntar
y su
ppor
t gro
ups,
su
ch a
s N
DC
S.
Chi
ldre
n an
d fa
milie
s ha
ve
acce
ss to
info
rmat
ion
in
thei
r pre
ferre
d la
ngua
ge
via
the
prov
isio
n of
tra
nsla
ted
writ
ten
mat
eria
l, in
terp
rete
rs, u
se o
f la
ngua
ge li
ne e
tc.
Evid
ence
In
terv
iew
with
fam
ilies,
W
ritte
n in
form
atio
n pr
ovid
ed to
chi
ldre
n an
d fa
milie
s,
Writ
ten
asse
ssm
ent m
ater
ial a
vaila
ble
in d
iffer
ent l
angu
ages
, C
opie
s of
invo
ices
for u
se o
f int
erpr
etat
ion
serv
ices
,
71
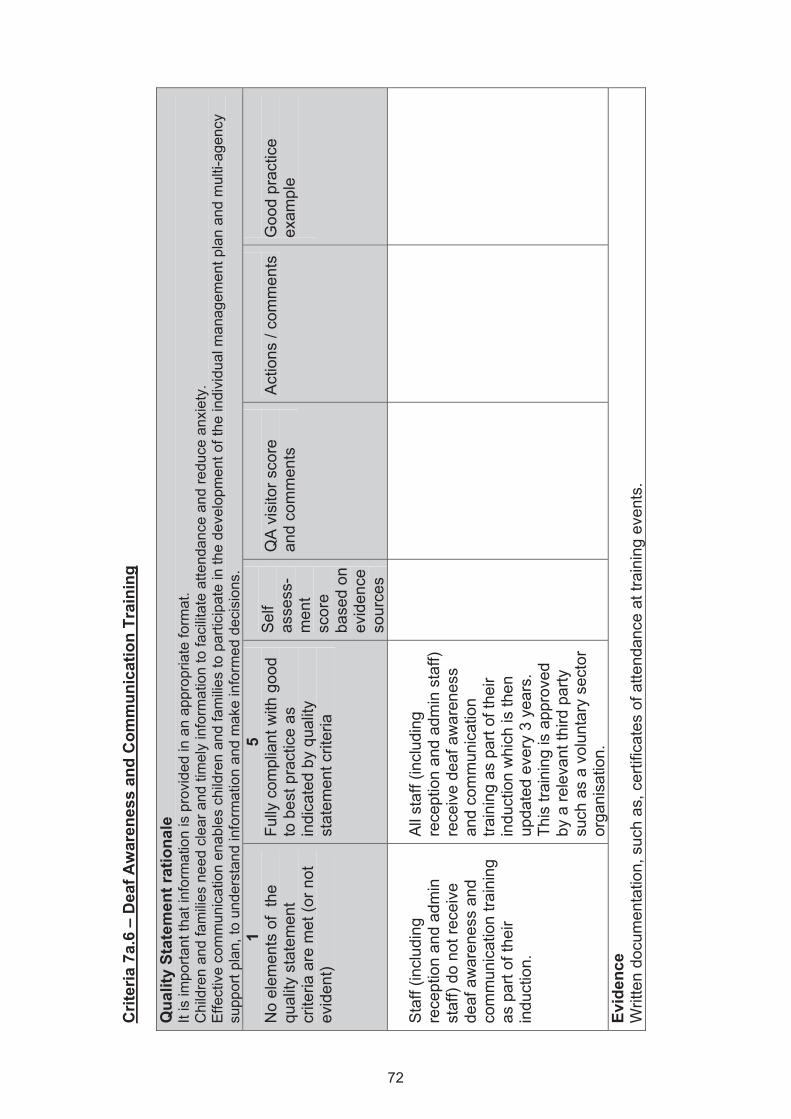
Crit
eria
7a.
6 –
Dea
f Aw
aren
ess
and
Com
mun
icat
ion
Trai
ning
Q
ualit
y St
atem
ent r
atio
nale
It
is im
porta
nt th
at in
form
atio
n is
pro
vide
d in
an
appr
opria
te fo
rmat
. C
hild
ren
and
fam
ilies
nee
d cl
ear a
nd ti
mel
y in
form
atio
n to
faci
litat
e at
tend
ance
and
redu
ce a
nxie
ty.
Effe
ctiv
e co
mm
unic
atio
n en
able
s ch
ildre
n an
d fa
mili
es to
par
ticip
ate
in th
e de
velo
pmen
t of t
he in
divi
dual
man
agem
ent p
lan
and
mul
ti-ag
ency
su
ppor
t pla
n, to
und
erst
and
info
rmat
ion
and
mak
e in
form
ed d
ecis
ions
. 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or n
ot
evid
ent)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Sta
ff (in
clud
ing
rece
ptio
n an
d ad
min
st
aff)
do n
ot re
ceiv
e de
af a
war
enes
s an
d co
mm
unic
atio
n tra
inin
g as
par
t of t
heir
indu
ctio
n.
All
staf
f (in
clud
ing
rece
ptio
n an
d ad
min
sta
ff)
rece
ive
deaf
aw
aren
ess
and
com
mun
icat
ion
train
ing
as p
art o
f the
ir in
duct
ion
whi
ch is
then
up
date
d ev
ery
3 ye
ars.
Th
is tr
aini
ng is
app
rove
d by
a re
leva
nt th
ird p
arty
su
ch a
s a
volu
ntar
y se
ctor
or
gani
satio
n.
Evid
ence
W
ritte
n do
cum
enta
tion,
suc
h as
, cer
tific
ates
of a
ttend
ance
at t
rain
ing
even
ts.
72
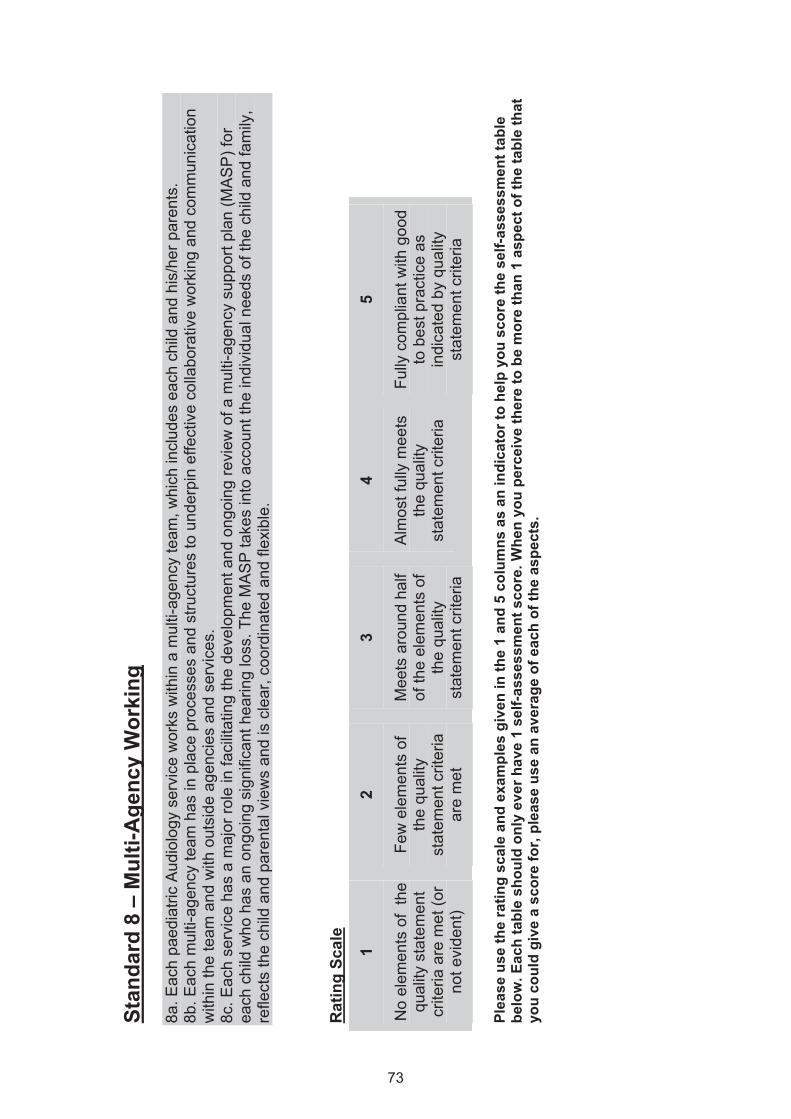
Stan
dard
8 –
Mul
ti-A
genc
y W
orki
ng
8a. E
ach
paed
iatri
c A
udio
logy
ser
vice
wor
ks w
ithin
a m
ulti-
agen
cy te
am, w
hich
incl
udes
eac
h ch
ild a
nd h
is/h
er p
aren
ts.
8b. E
ach
mul
ti-ag
ency
team
has
in p
lace
pro
cess
es a
nd s
truct
ures
to u
nder
pin
effe
ctiv
e co
llabo
rativ
e w
orki
ng a
nd c
omm
unic
atio
n w
ithin
the
team
and
with
out
side
age
ncie
s an
d se
rvic
es.
8c
. Eac
h se
rvic
e ha
s a
maj
or ro
le in
faci
litat
ing
the
deve
lopm
ent a
nd o
ngoi
ng re
view
of a
mul
ti-ag
ency
sup
port
plan
(MA
SP
) for
ea
ch c
hild
who
has
an
ongo
ing
sign
ifica
nt h
earin
g lo
ss. T
he M
AS
P ta
kes
into
acc
ount
the
indi
vidu
al n
eeds
of t
he c
hild
and
fam
ily,
refle
cts
the
child
and
par
enta
l vie
ws
and
is c
lear
, coo
rdin
ated
and
flex
ible
.
Rat
ing
Scal
e
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts.
73
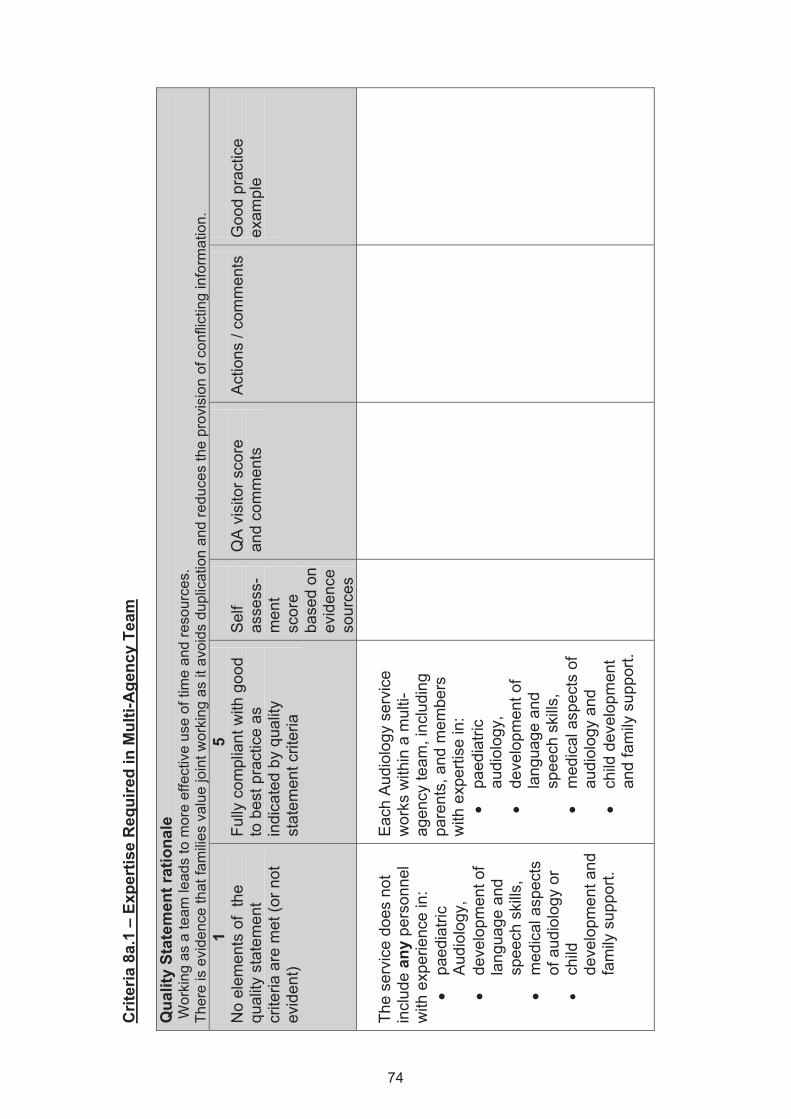
Crit
eria
8a.
1 –
Expe
rtis
e R
equi
red
in M
ulti-
Age
ncy
Team
Q
ualit
y St
atem
ent r
atio
nale
W
orki
ng a
s a
team
lead
s to
mor
e ef
fect
ive
use
of ti
me
and
reso
urce
s.
Ther
e is
evi
denc
e th
at fa
mili
es v
alue
join
t wor
king
as
it av
oids
dup
licat
ion
and
redu
ces
the
prov
isio
n of
con
flict
ing
info
rmat
ion.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
serv
ice
does
not
in
clud
e an
y pe
rson
nel
with
exp
erie
nce
in:
• pa
edia
tric
Aud
iolo
gy,
• de
velo
pmen
t of
lang
uage
and
sp
eech
ski
lls,
• m
edic
al a
spec
ts
of a
udio
logy
or
• ch
ild
deve
lopm
ent a
nd
fam
ily s
uppo
rt.
Eac
h A
udio
logy
ser
vice
w
orks
with
in a
mul
ti-ag
ency
team
, inc
ludi
ng
pare
nts,
and
mem
bers
w
ith e
xper
tise
in:
• pa
edia
tric
audi
olog
y,
• de
velo
pmen
t of
lang
uage
and
sp
eech
ski
lls,
• m
edic
al a
spec
ts o
f au
diol
ogy
and
•
child
dev
elop
men
t an
d fa
mily
sup
port.
74
Evid
ence
M
ultid
isci
plin
ary
team
evi
dent
in n
otes
from
man
agem
ent p
lan
mee
tings
, E
vide
nce
of e
xper
tise
in s
peci
alis
t are
a (c
ours
e ce
rtific
ates
, qua
lific
atio
ns, r
egis
tratio
n)
75
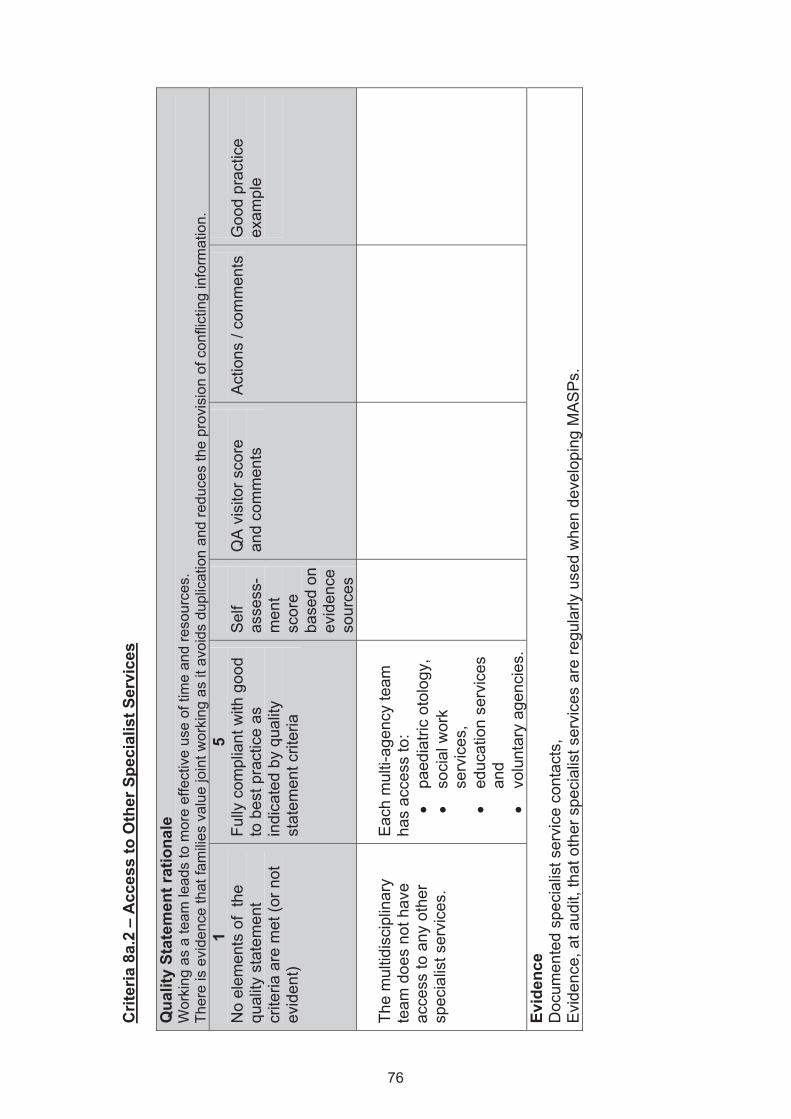
Crit
eria
8a.
2 –
Acc
ess
to O
ther
Spe
cial
ist S
ervi
ces
Qua
lity
Stat
emen
t rat
iona
le
Wor
king
as
a te
am le
ads
to m
ore
effe
ctiv
e us
e of
tim
e an
d re
sour
ces.
Ther
e is
evi
denc
e th
at fa
mili
es v
alue
join
t wor
king
as
it av
oids
dup
licat
ion
and
redu
ces
the
prov
isio
n of
con
flict
ing
info
rmat
ion.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
mul
tidis
cipl
inar
y te
am d
oes
not h
ave
acce
ss to
any
oth
er
spec
ialis
t ser
vice
s.
Eac
h m
ulti-
agen
cy te
am
has
acce
ss to
: •
paed
iatri
c ot
olog
y,
• so
cial
wor
k se
rvic
es,
• ed
ucat
ion
serv
ices
an
d •
volu
ntar
y ag
enci
es.
Evid
ence
D
ocum
ente
d sp
ecia
list s
ervi
ce c
onta
cts,
E
vide
nce,
at a
udit,
that
oth
er s
peci
alis
t ser
vice
s ar
e re
gula
rly u
sed
whe
n de
velo
ping
MA
SP
s.
76
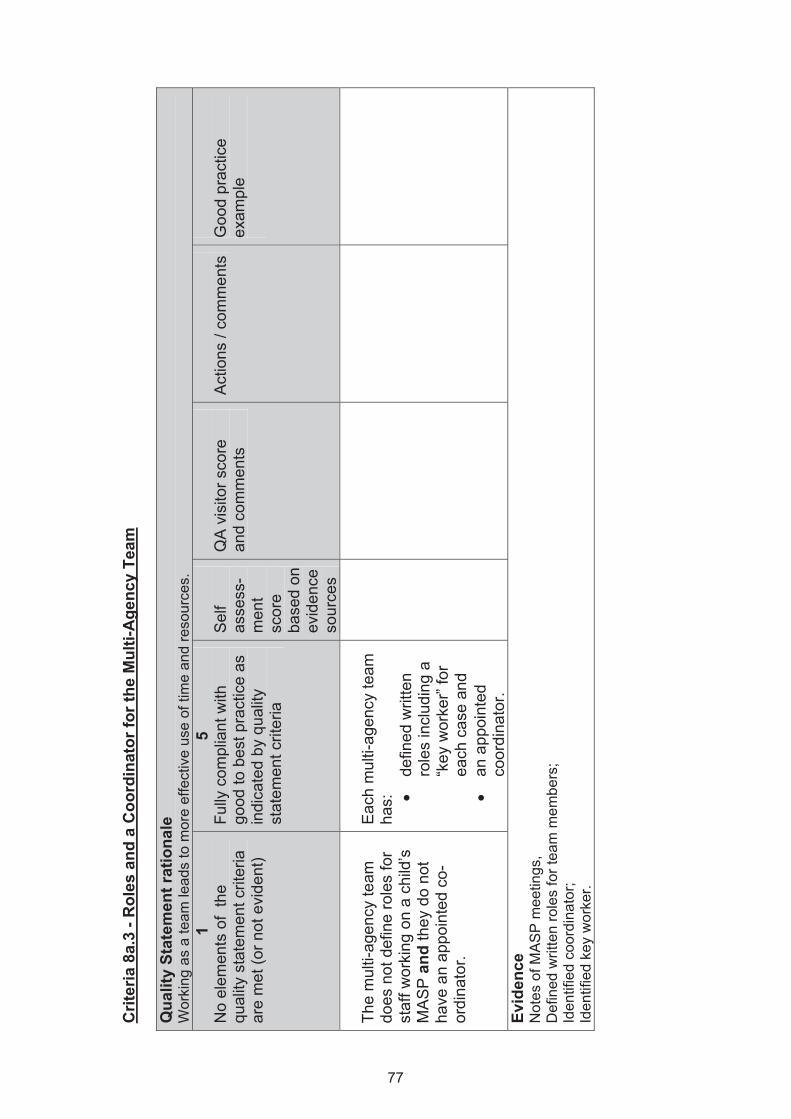
Crit
eria
8a.
3 - R
oles
and
a C
oord
inat
or fo
r the
Mul
ti-A
genc
y Te
am
Qua
lity
Stat
emen
t rat
iona
le
Wor
king
as
a te
am le
ads
to m
ore
effe
ctiv
e us
e of
tim
e an
d re
sour
ces.
1
No
elem
ents
of
the
qual
ity s
tate
men
t crit
eria
ar
e m
et (o
r not
evi
dent
)
5 Fu
lly c
ompl
iant
with
go
od to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
mul
ti-ag
ency
team
do
es n
ot d
efin
e ro
les
for
staf
f wor
king
on
a ch
ild’s
M
AS
P a
nd th
ey d
o no
t ha
ve a
n ap
poin
ted
co-
ordi
nato
r.
Eac
h m
ulti-
agen
cy te
am
has:
• de
fined
writ
ten
role
s in
clud
ing
a “k
ey w
orke
r” fo
r ea
ch c
ase
and
• an
app
oint
ed
coor
dina
tor.
Evid
ence
N
otes
of M
AS
P m
eetin
gs,
Def
ined
writ
ten
role
s fo
r tea
m m
embe
rs;
Iden
tifie
d co
ordi
nato
r;
Iden
tifie
d ke
y w
orke
r.
77
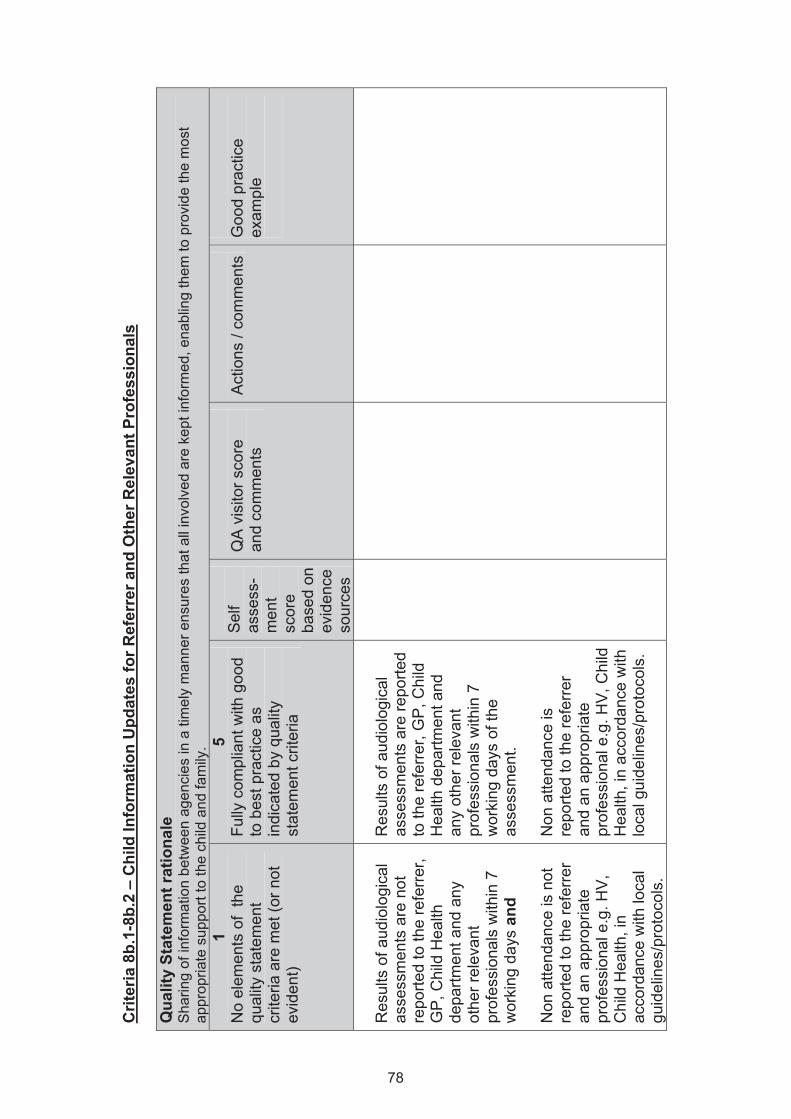
Crit
eria
8b.
1-8b
.2 –
Chi
ld In
form
atio
n U
pdat
es fo
r Ref
erre
r and
Oth
er R
elev
ant P
rofe
ssio
nals
Q
ualit
y St
atem
ent r
atio
nale
S
harin
g of
info
rmat
ion
betw
een
agen
cies
in a
tim
ely
man
ner e
nsur
es th
at a
ll in
volv
ed a
re k
ept i
nfor
med
, ena
blin
g th
em to
pro
vide
the
mos
t ap
prop
riate
sup
port
to th
e ch
ild a
nd fa
mily
. 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or n
ot
evid
ent)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Res
ults
of a
udio
logi
cal
asse
ssm
ents
are
not
re
porte
d to
the
refe
rrer
, G
P, C
hild
Hea
lth
depa
rtmen
t and
any
ot
her r
elev
ant
prof
essi
onal
s w
ithin
7
wor
king
day
s an
d N
on a
ttend
ance
is n
ot
repo
rted
to th
e re
ferre
r an
d an
app
ropr
iate
pr
ofes
sion
al e
.g. H
V,
Chi
ld H
ealth
, in
acco
rdan
ce w
ith lo
cal
guid
elin
es/p
roto
cols
.
Res
ults
of a
udio
logi
cal
asse
ssm
ents
are
repo
rted
to th
e re
ferr
er, G
P, C
hild
H
ealth
dep
artm
ent a
nd
any
othe
r rel
evan
t pr
ofes
sion
als
with
in 7
w
orki
ng d
ays
of th
e as
sess
men
t. N
on a
ttend
ance
is
repo
rted
to th
e re
ferre
r an
d an
app
ropr
iate
pr
ofes
sion
al e
.g. H
V, C
hild
H
ealth
, in
acco
rdan
ce w
ith
loca
l gui
delin
es/p
roto
cols
.
78
Evid
ence
C
ase
audi
t, In
terv
iew
s w
ith k
ey re
ferr
ers,
R
evie
w o
f writ
ten
patie
nt re
cord
s re
ceiv
ed a
nd k
ept b
y re
ferr
ers
and
othe
r pro
fess
iona
ls.
79
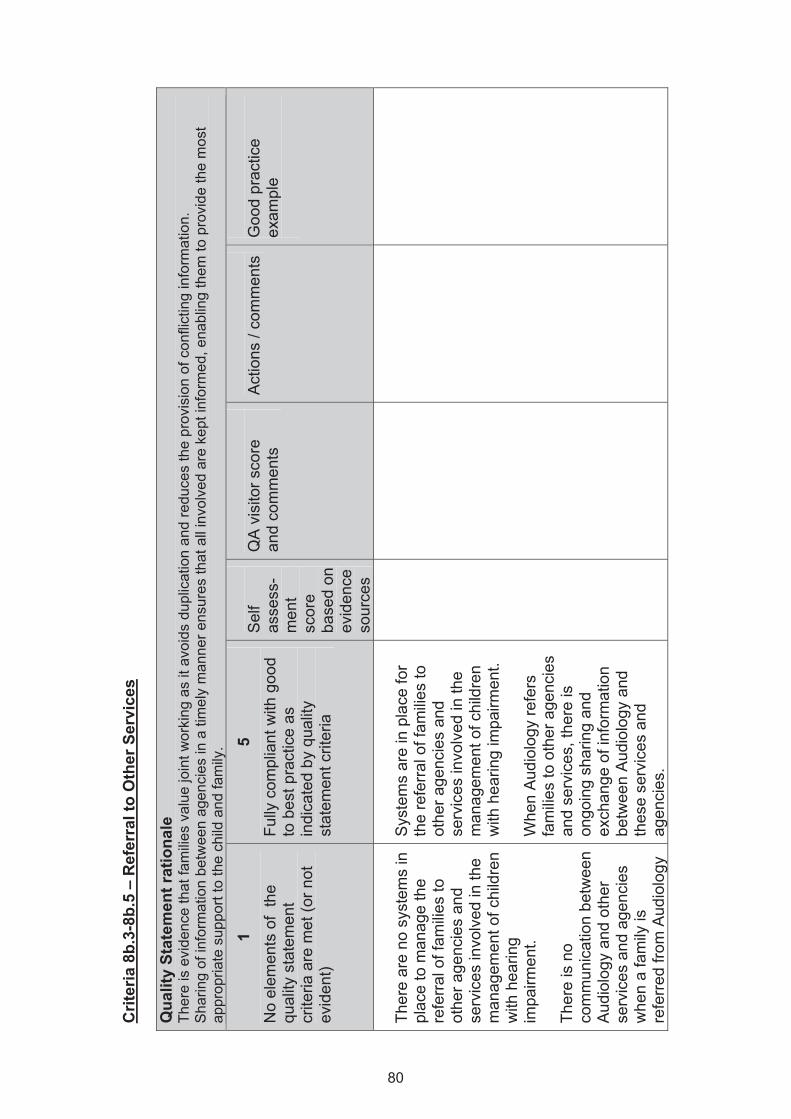
Crit
eria
8b.
3-8b
.5 –
Ref
erra
l to
Oth
er S
ervi
ces
Qua
lity
Stat
emen
t rat
iona
le
Ther
e is
evi
denc
e th
at fa
mili
es v
alue
join
t wor
king
as
it av
oids
dup
licat
ion
and
redu
ces
the
prov
isio
n of
con
flict
ing
info
rmat
ion.
S
harin
g of
info
rmat
ion
betw
een
agen
cies
in a
tim
ely
man
ner e
nsur
es th
at a
ll in
volv
ed a
re k
ept i
nfor
med
, ena
blin
g th
em to
pro
vide
the
mos
t ap
prop
riate
sup
port
to th
e ch
ild a
nd fa
mily
.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ther
e ar
e no
sys
tem
s in
pl
ace
to m
anag
e th
e re
ferra
l of f
amilie
s to
ot
her a
genc
ies
and
serv
ices
invo
lved
in th
e m
anag
emen
t of c
hild
ren
with
hea
ring
impa
irmen
t. Th
ere
is n
o co
mm
unic
atio
n be
twee
n A
udio
logy
and
oth
er
serv
ices
and
age
ncie
s w
hen
a fa
mily
is
refe
rred
from
Aud
iolo
gy
Sys
tem
s ar
e in
pla
ce fo
r th
e re
ferra
l of f
amilie
s to
ot
her a
genc
ies
and
serv
ices
invo
lved
in th
e m
anag
emen
t of c
hild
ren
with
hea
ring
impa
irmen
t. W
hen
Aud
iolo
gy re
fers
fa
milie
s to
oth
er a
genc
ies
and
serv
ices
, the
re is
on
goin
g sh
arin
g an
d ex
chan
ge o
f inf
orm
atio
n be
twee
n A
udio
logy
and
th
ese
serv
ices
and
ag
enci
es.
80
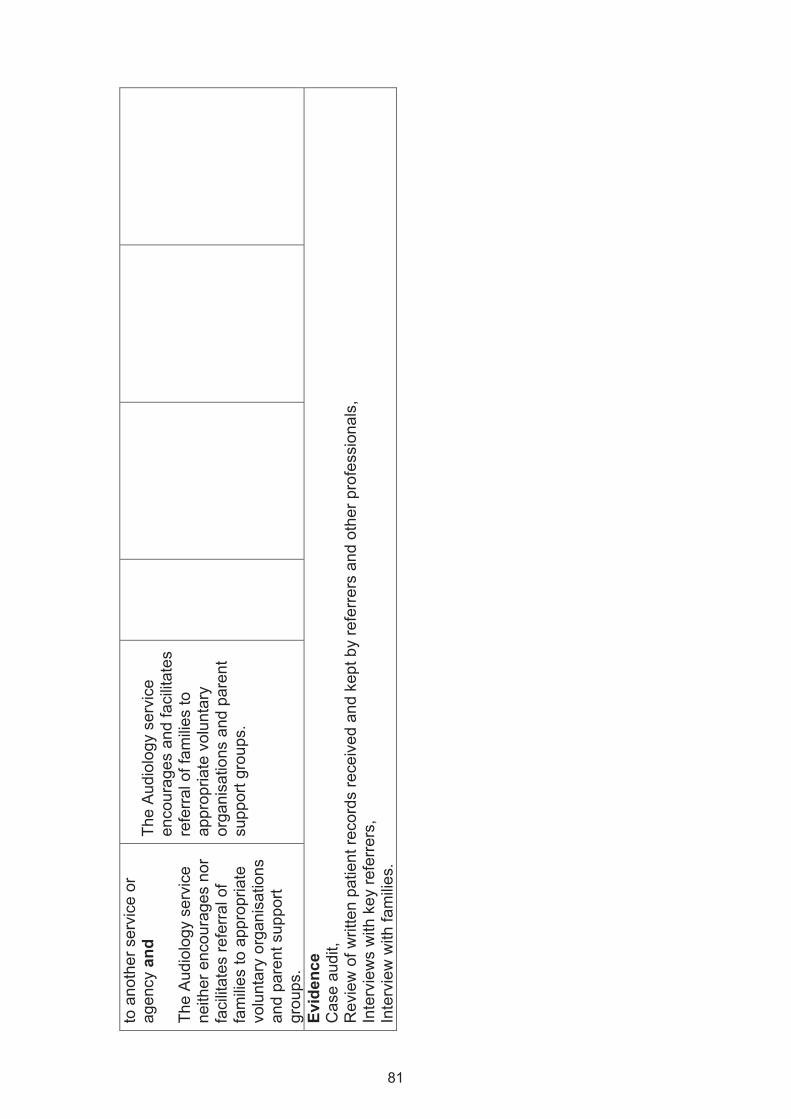
to a
noth
er s
ervi
ce o
r ag
ency
and
Th
e A
udio
logy
ser
vice
ne
ither
enc
oura
ges
nor
faci
litat
es re
ferr
al o
f fa
mili
es to
app
ropr
iate
vo
lunt
ary
orga
nisa
tions
an
d pa
rent
sup
port
grou
ps.
The
Aud
iolo
gy s
ervi
ce
enco
urag
es a
nd fa
cilit
ates
re
ferra
l of f
amilie
s to
ap
prop
riate
vol
unta
ry
orga
nisa
tions
and
par
ent
supp
ort g
roup
s.
Evid
ence
C
ase
audi
t, R
evie
w o
f writ
ten
patie
nt re
cord
s re
ceiv
ed a
nd k
ept b
y re
ferre
rs a
nd o
ther
pro
fess
iona
ls,
Inte
rvie
ws
with
key
refe
rrer
s,
Inte
rvie
w w
ith fa
milie
s.
81
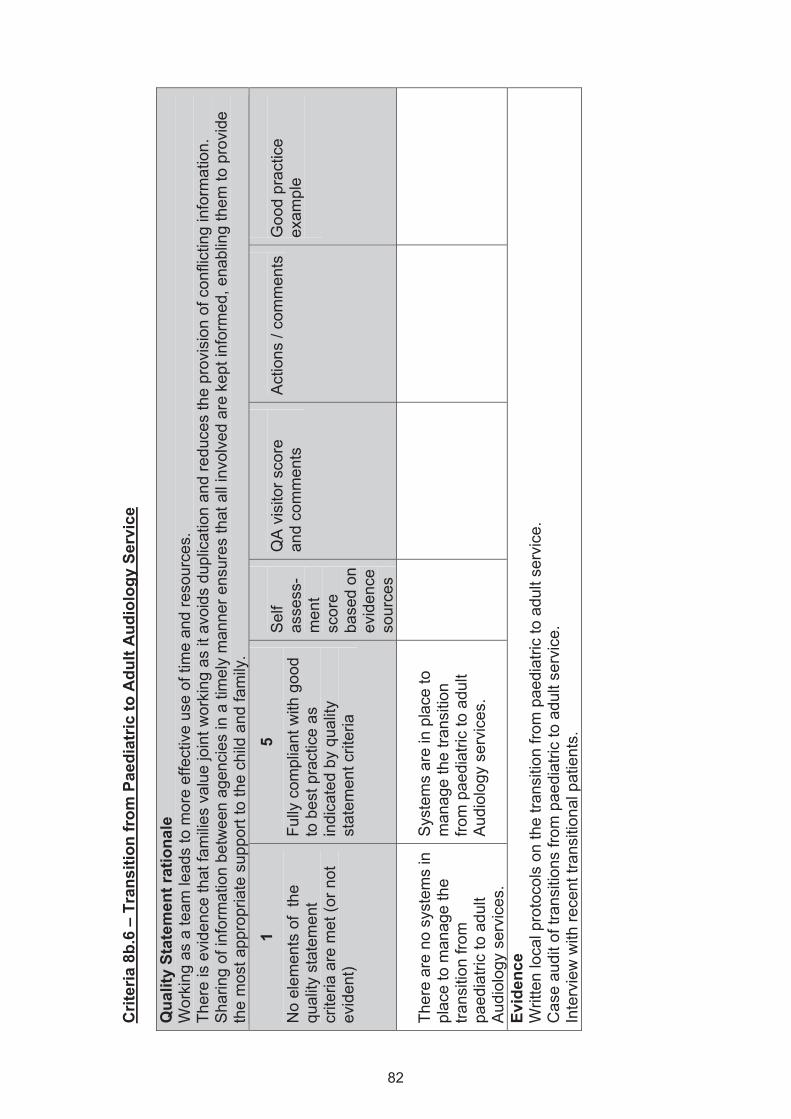
Crit
eria
8b.
6 –
Tran
sitio
n fr
om P
aedi
atric
to A
dult
Aud
iolo
gy S
ervi
ce
Qua
lity
Stat
emen
t rat
iona
le
Wor
king
as
a te
am le
ads
to m
ore
effe
ctiv
e us
e of
tim
e an
d re
sour
ces.
Ther
e is
evi
denc
e th
at fa
milie
s va
lue
join
t wor
king
as
it av
oids
dup
licat
ion
and
redu
ces
the
prov
isio
n of
con
flict
ing
info
rmat
ion.
Sha
ring
of in
form
atio
n be
twee
n ag
enci
es in
a ti
mel
y m
anne
r ens
ures
that
all
invo
lved
are
kep
t inf
orm
ed, e
nabl
ing
them
to p
rovi
de
the
mos
t app
ropr
iate
sup
port
to th
e ch
ild a
nd fa
mily
.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Ther
e ar
e no
sys
tem
s in
pl
ace
to m
anag
e th
e tra
nsiti
on fr
om
paed
iatri
c to
adu
lt A
udio
logy
ser
vice
s.
Sys
tem
s ar
e in
pla
ce to
m
anag
e th
e tra
nsiti
on
from
pae
diat
ric to
adu
lt A
udio
logy
ser
vice
s.
Evid
ence
W
ritte
n lo
cal p
roto
cols
on
the
trans
ition
from
pae
diat
ric to
adu
lt se
rvic
e.
Cas
e au
dit o
f tra
nsiti
ons
from
pae
diat
ric to
adu
lt se
rvic
e.
Inte
rvie
w w
ith re
cent
tran
sitio
nal p
atie
nts.
82
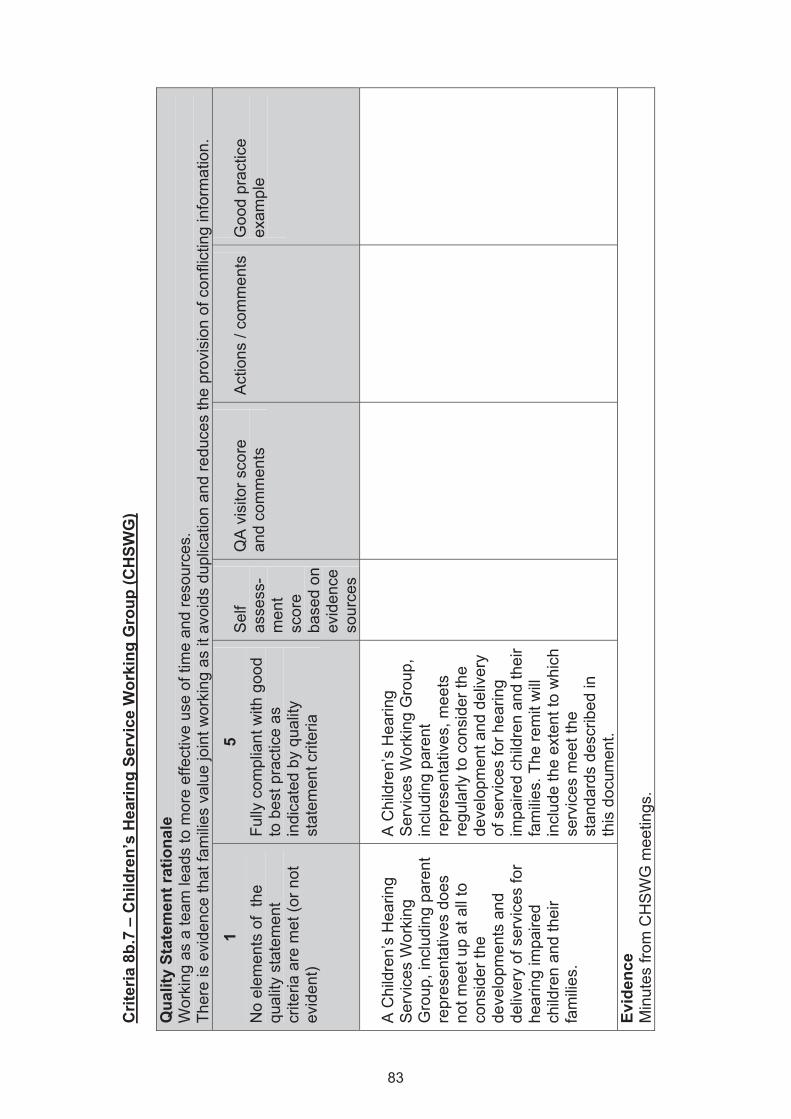
Crit
eria
8b.
7 –
Chi
ldre
n’s
Hea
ring
Serv
ice
Wor
king
Gro
up (C
HSW
G)
Qua
lity
Stat
emen
t rat
iona
le
Wor
king
as
a te
am le
ads
to m
ore
effe
ctiv
e us
e of
tim
e an
d re
sour
ces.
Th
ere
is e
vide
nce
that
fam
ilies
valu
e jo
int w
orki
ng a
s it
avoi
ds d
uplic
atio
n an
d re
duce
s th
e pr
ovis
ion
of c
onfli
ctin
g in
form
atio
n.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
A C
hild
ren’
s H
earin
g S
ervi
ces
Wor
king
G
roup
, inc
ludi
ng p
aren
t re
pres
enta
tives
doe
s no
t mee
t up
at a
ll to
co
nsid
er th
e de
velo
pmen
ts a
nd
deliv
ery
of s
ervi
ces
for
hear
ing
impa
ired
child
ren
and
thei
r fa
mili
es.
A C
hild
ren’
s H
earin
g S
ervi
ces
Wor
king
Gro
up,
incl
udin
g pa
rent
re
pres
enta
tives
, mee
ts
regu
larly
to c
onsi
der t
he
deve
lopm
ent a
nd d
eliv
ery
of s
ervi
ces
for h
earin
g im
paire
d ch
ildre
n an
d th
eir
fam
ilies.
The
rem
it w
ill in
clud
e th
e ex
tent
to w
hich
se
rvic
es m
eet t
he
stan
dard
s de
scrib
ed in
th
is d
ocum
ent.
Evid
ence
M
inut
es fr
om C
HS
WG
mee
tings
.
83
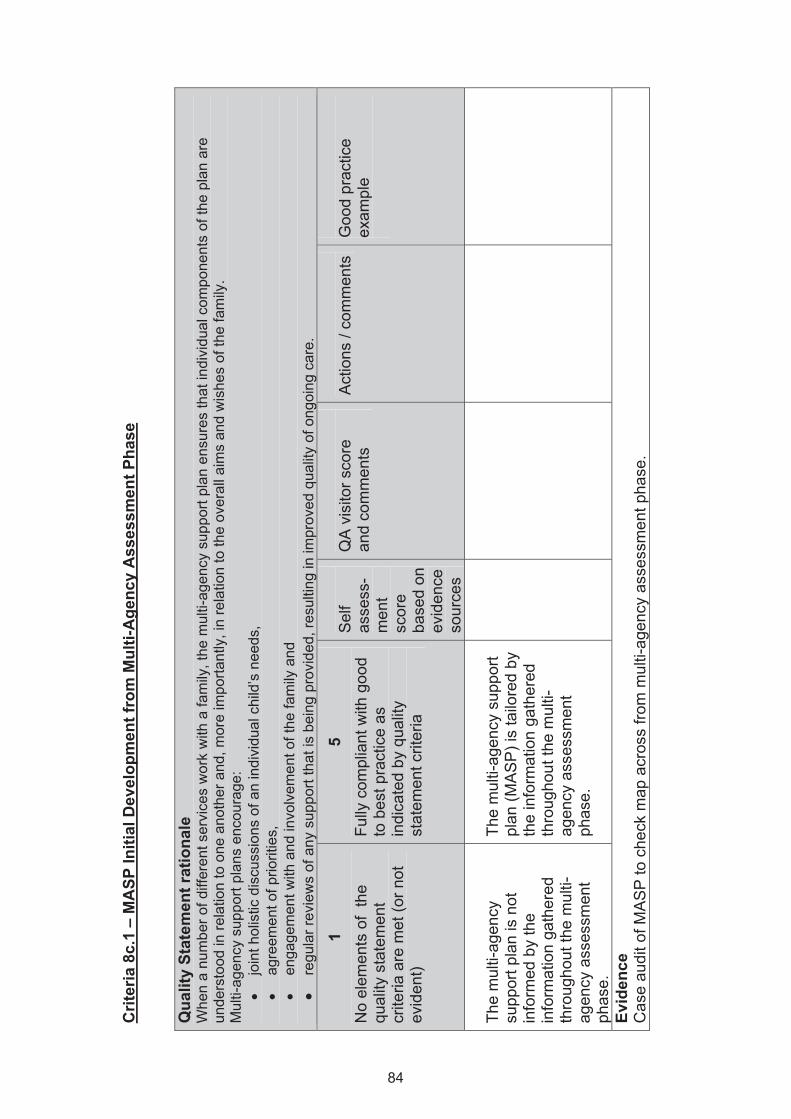
Crit
eria
8c.
1 –
MA
SP In
itial
Dev
elop
men
t fro
m M
ulti-
Age
ncy
Ass
essm
ent P
hase
Q
ualit
y St
atem
ent r
atio
nale
W
hen
a nu
mbe
r of d
iffer
ent s
ervi
ces
wor
k w
ith a
fam
ily, t
he m
ulti-
agen
cy s
uppo
rt pl
an e
nsur
es th
at in
divi
dual
com
pone
nts
of th
e pl
an a
re
unde
rsto
od in
rela
tion
to o
ne a
noth
er a
nd, m
ore
impo
rtant
ly, i
n re
latio
n to
the
over
all a
ims
and
wis
hes
of th
e fa
mily
. M
ulti-
agen
cy s
uppo
rt pl
ans
enco
urag
e:
• jo
int h
olis
tic d
iscu
ssio
ns o
f an
indi
vidu
al c
hild
’s n
eeds
, •
agre
emen
t of p
riorit
ies,
•
enga
gem
ent w
ith a
nd in
volv
emen
t of t
he fa
mily
and
•
regu
lar r
evie
ws
of a
ny s
uppo
rt th
at is
bei
ng p
rovi
ded,
resu
lting
in im
prov
ed q
ualit
y of
ong
oing
car
e.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
mul
ti-ag
ency
su
ppor
t pla
n is
not
in
form
ed b
y th
e in
form
atio
n ga
ther
ed
thro
ugho
ut th
e m
ulti-
agen
cy a
sses
smen
t ph
ase.
The
mul
ti-ag
ency
sup
port
plan
(MA
SP
) is
tailo
red
by
the
info
rmat
ion
gath
ered
th
roug
hout
the
mul
ti-ag
ency
ass
essm
ent
phas
e.
Evid
ence
C
ase
audi
t of M
AS
P to
che
ck m
ap a
cros
s fro
m m
ulti-
agen
cy a
sses
smen
t pha
se.
84
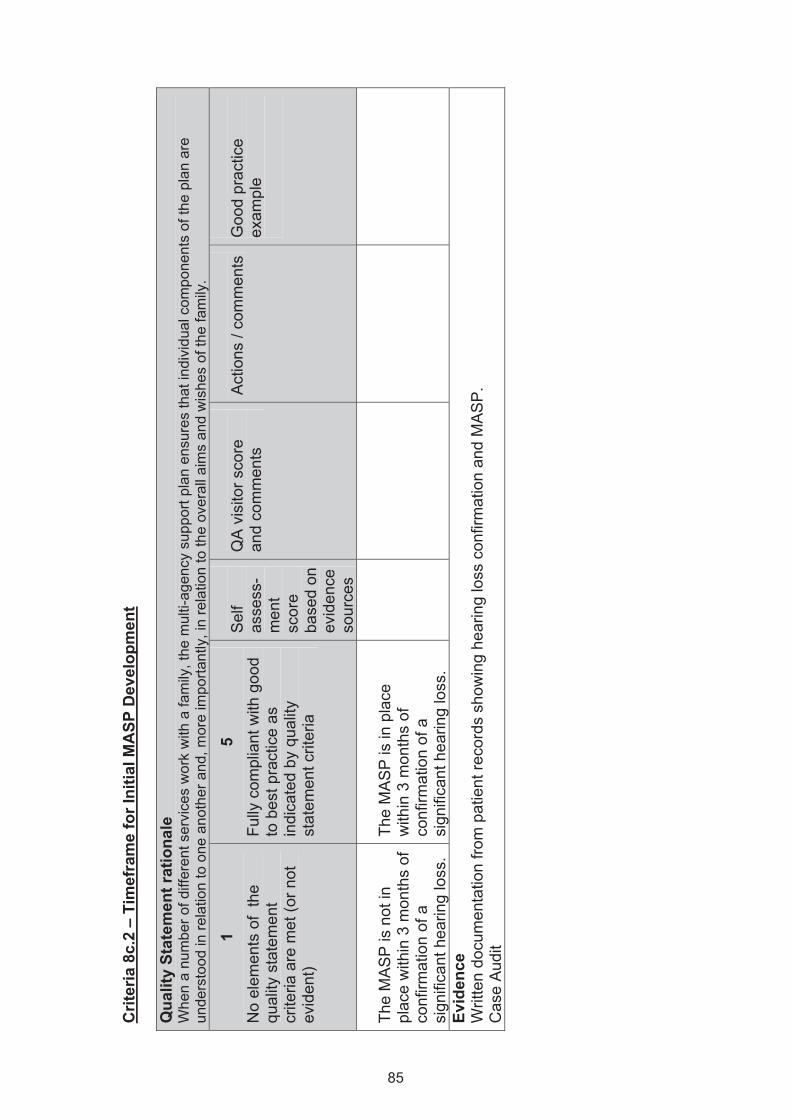
Crit
eria
8c.
2 –
Tim
efra
me
for I
nitia
l MA
SP D
evel
opm
ent
Qua
lity
Stat
emen
t rat
iona
le
Whe
n a
num
ber o
f diff
eren
t ser
vice
s w
ork
with
a fa
mily
, the
mul
ti-ag
ency
sup
port
plan
ens
ures
that
indi
vidu
al c
ompo
nent
s of
the
plan
are
un
ders
tood
in re
latio
n to
one
ano
ther
and
, mor
e im
porta
ntly
, in
rela
tion
to th
e ov
eral
l aim
s an
d w
ishe
s of
the
fam
ily.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
MA
SP
is n
ot in
pl
ace
with
in 3
mon
ths
of
conf
irmat
ion
of a
si
gnifi
cant
hea
ring
loss
.
The
MA
SP
is in
pla
ce
with
in 3
mon
ths
of
conf
irmat
ion
of a
si
gnifi
cant
hea
ring
loss
.
Evid
ence
W
ritte
n do
cum
enta
tion
from
pat
ient
reco
rds
show
ing
hear
ing
loss
con
firm
atio
n an
d M
AS
P.
Cas
e A
udit
85
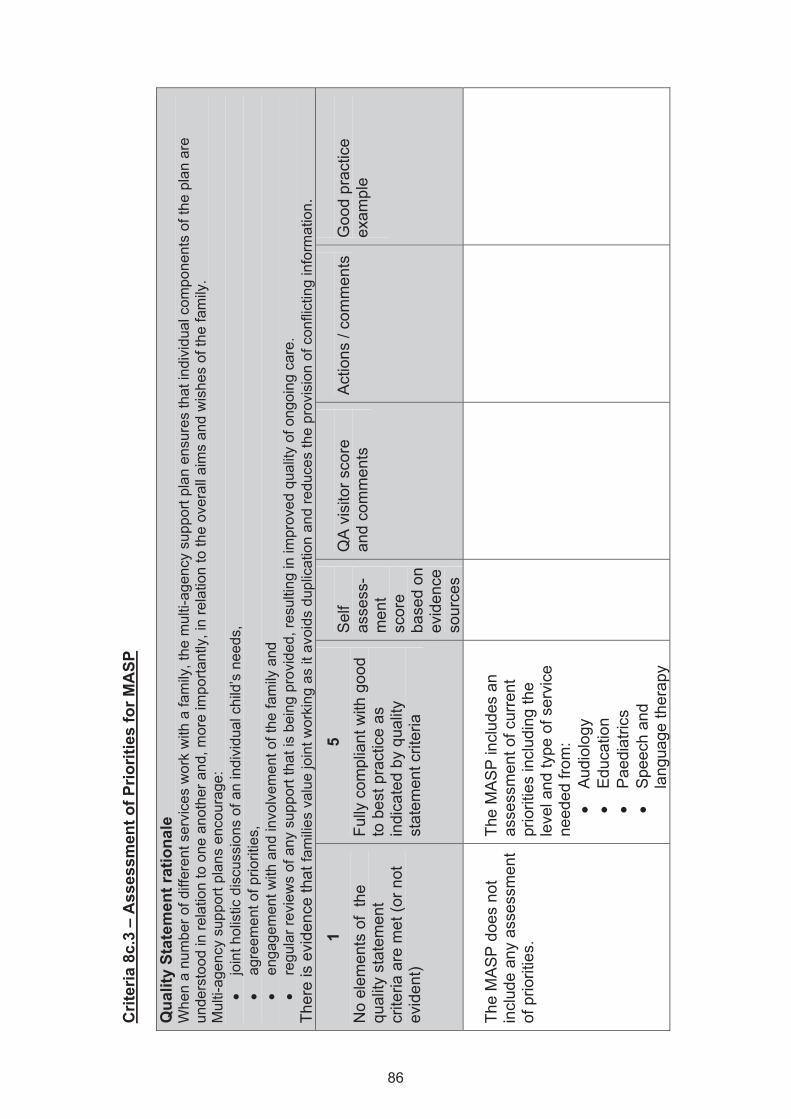
Crit
eria
8c.
3 –
Ass
essm
ent o
f Prio
ritie
s fo
r MA
SP
Qua
lity
Stat
emen
t rat
iona
le
Whe
n a
num
ber o
f diff
eren
t ser
vice
s w
ork
with
a fa
mily
, the
mul
ti-ag
ency
sup
port
plan
ens
ures
that
indi
vidu
al c
ompo
nent
s of
the
plan
are
un
ders
tood
in re
latio
n to
one
ano
ther
and
, mor
e im
porta
ntly
, in
rela
tion
to th
e ov
eral
l aim
s an
d w
ishe
s of
the
fam
ily.
Mul
ti-ag
ency
sup
port
plan
s en
cour
age:
•
join
t hol
istic
dis
cuss
ions
of a
n in
divi
dual
chi
ld’s
nee
ds,
• ag
reem
ent o
f prio
ritie
s,
• en
gage
men
t with
and
invo
lvem
ent o
f the
fam
ily a
nd
• re
gula
r rev
iew
s of
any
sup
port
that
is b
eing
pro
vide
d, re
sulti
ng in
impr
oved
qua
lity
of o
ngoi
ng c
are.
Th
ere
is e
vide
nce
that
fam
ilies
val
ue jo
int w
orki
ng a
s it
avoi
ds d
uplic
atio
n an
d re
duce
s th
e pr
ovis
ion
of c
onfli
ctin
g in
form
atio
n.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
MA
SP
doe
s no
t in
clud
e an
y as
sess
men
t of
prio
ritie
s.
The
MA
SP
incl
udes
an
asse
ssm
ent o
f cur
rent
pr
iorit
ies
incl
udin
g th
e le
vel a
nd ty
pe o
f ser
vice
ne
eded
from
: •
Aud
iolo
gy
• E
duca
tion
• P
aedi
atric
s •
Spe
ech
and
lang
uage
ther
apy
86
• S
ocia
l wor
k •
Spe
cial
ist s
ervi
ces,
e.
g. c
ochl
ear
impl
ant t
eam
Ev
iden
ce
Aud
it of
cas
e st
udie
s,
Rec
ords
of M
AS
P’s
, D
ocum
ente
d pl
ans.
87
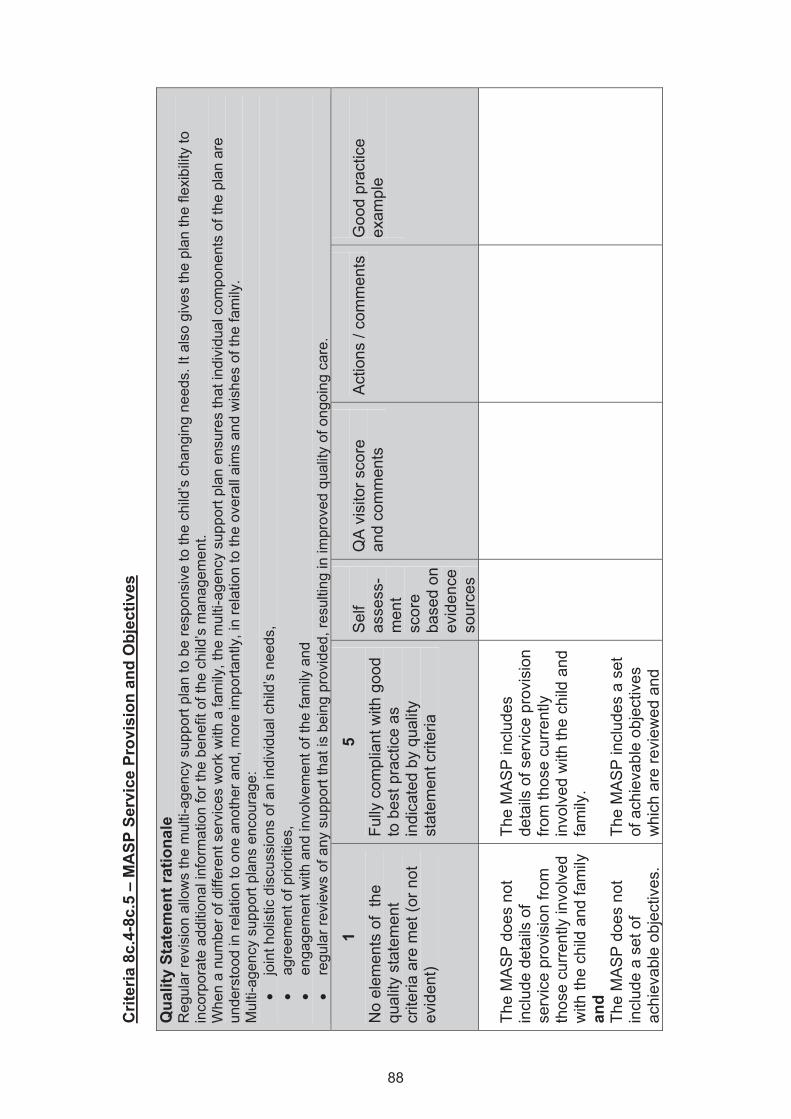
Crit
eria
8c.
4-8c
.5 –
MA
SP S
ervi
ce P
rovi
sion
and
Obj
ectiv
es
Qua
lity
Stat
emen
t rat
iona
le
Reg
ular
revi
sion
allo
ws
the
mul
ti-ag
ency
sup
port
plan
to b
e re
spon
sive
to th
e ch
ild’s
cha
ngin
g ne
eds.
It a
lso
give
s th
e pl
an th
e fle
xibi
lity
to
inco
rpor
ate
addi
tiona
l inf
orm
atio
n fo
r the
ben
efit
of th
e ch
ild’s
man
agem
ent.
Whe
n a
num
ber o
f diff
eren
t ser
vice
s w
ork
with
a fa
mily
, the
mul
ti-ag
ency
sup
port
plan
ens
ures
that
indi
vidu
al c
ompo
nent
s of
the
plan
are
un
ders
tood
in re
latio
n to
one
ano
ther
and
, mor
e im
porta
ntly
, in
rela
tion
to th
e ov
eral
l aim
s an
d w
ishe
s of
the
fam
ily.
Mul
ti-ag
ency
sup
port
plan
s en
cour
age:
•
join
t hol
istic
dis
cuss
ions
of a
n in
divi
dual
chi
ld’s
nee
ds,
• ag
reem
ent o
f prio
ritie
s,
• en
gage
men
t with
and
invo
lvem
ent o
f the
fam
ily a
nd
• re
gula
r rev
iew
s of
any
sup
port
that
is b
eing
pro
vide
d, re
sulti
ng in
impr
oved
qua
lity
of o
ngoi
ng c
are.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
MA
SP
doe
s no
t in
clud
e de
tails
of
serv
ice
prov
isio
n fro
m
thos
e cu
rrent
ly in
volv
ed
with
the
child
and
fam
ily
and
The
MA
SP
doe
s no
t in
clud
e a
set o
f ac
hiev
able
obj
ectiv
es.
The
MA
SP
incl
udes
de
tails
of s
ervi
ce p
rovi
sion
fro
m th
ose
curr
ently
in
volv
ed w
ith th
e ch
ild a
nd
fam
ily.
The
MA
SP
incl
udes
a s
et
of a
chie
vabl
e ob
ject
ives
w
hich
are
revi
ewed
and
88
upda
ted
regu
larly
(at l
east
6
mon
thly
for p
re-s
choo
l ch
ildre
n an
d an
nual
ly fo
r sc
hool
age
chi
ldre
n) a
nd
circ
ulat
ed to
all
mem
bers
of
the
team
.
Evid
ence
A
udit
of c
ase
stud
ies,
R
ecor
ds o
f MA
SP
s,
Doc
umen
ted
plan
s.
89
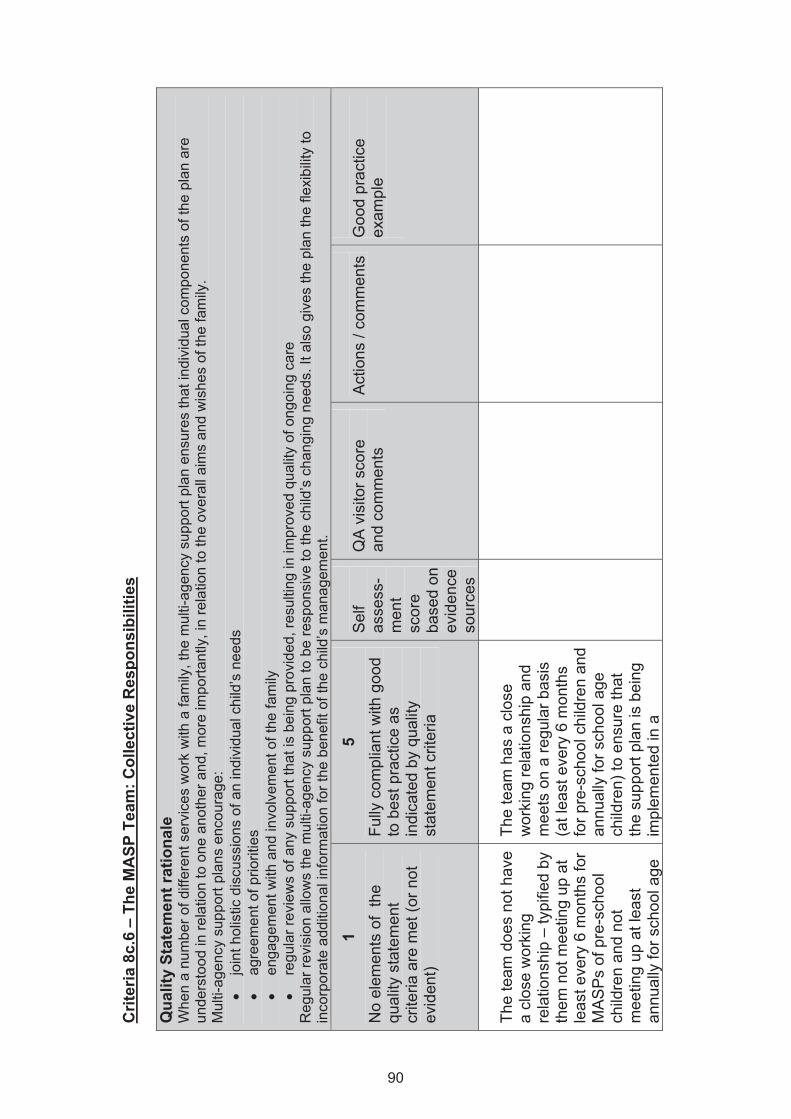
Crit
eria
8c.
6 –
The
MA
SP T
eam
: Col
lect
ive
Res
pons
ibili
ties
Qua
lity
Stat
emen
t rat
iona
le
Whe
n a
num
ber o
f diff
eren
t ser
vice
s w
ork
with
a fa
mily
, the
mul
ti-ag
ency
sup
port
plan
ens
ures
that
indi
vidu
al c
ompo
nent
s of
the
plan
are
un
ders
tood
in re
latio
n to
one
ano
ther
and
, mor
e im
porta
ntly
, in
rela
tion
to th
e ov
eral
l aim
s an
d w
ishe
s of
the
fam
ily.
Mul
ti-ag
ency
sup
port
plan
s en
cour
age:
•
join
t hol
istic
dis
cuss
ions
of a
n in
divi
dual
chi
ld’s
nee
ds
• ag
reem
ent o
f prio
ritie
s •
enga
gem
ent w
ith a
nd in
volv
emen
t of t
he fa
mily
•
regu
lar r
evie
ws
of a
ny s
uppo
rt th
at is
bei
ng p
rovi
ded,
resu
lting
in im
prov
ed q
ualit
y of
ong
oing
car
e R
egul
ar re
visi
on a
llow
s th
e m
ulti-
agen
cy s
uppo
rt pl
an to
be
resp
onsi
ve to
the
child
’s c
hang
ing
need
s. It
als
o gi
ves
the
plan
the
flexi
bilit
y to
in
corp
orat
e ad
ditio
nal i
nfor
mat
ion
for t
he b
enef
it of
the
child
’s m
anag
emen
t.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
team
doe
s no
t hav
e a
clos
e w
orki
ng
rela
tions
hip
– ty
pifie
d by
th
em n
ot m
eetin
g up
at
leas
t eve
ry 6
mon
ths
for
MA
SP
s of
pre
-sch
ool
child
ren
and
not
mee
ting
up a
t lea
st
annu
ally
for s
choo
l age
The
team
has
a c
lose
w
orki
ng re
latio
nshi
p an
d m
eets
on
a re
gula
r bas
is
(at l
east
eve
ry 6
mon
ths
for p
re-s
choo
l chi
ldre
n an
d an
nual
ly fo
r sch
ool a
ge
child
ren)
to e
nsur
e th
at
the
supp
ort p
lan
is b
eing
im
plem
ente
d in
a
90
child
ren.
co
ordi
nate
d w
ay a
nd in
lin
e w
ith th
e w
ishe
s an
d ne
eds
of th
e fa
mily
. Ev
iden
ce
Cas
e A
udit,
D
ocum
ente
d ev
iden
ce o
f MA
SP
mee
tings
– s
uch
as m
inut
es a
nd w
ritte
n do
cum
enta
tion
with
in p
atie
nt re
cord
.
91
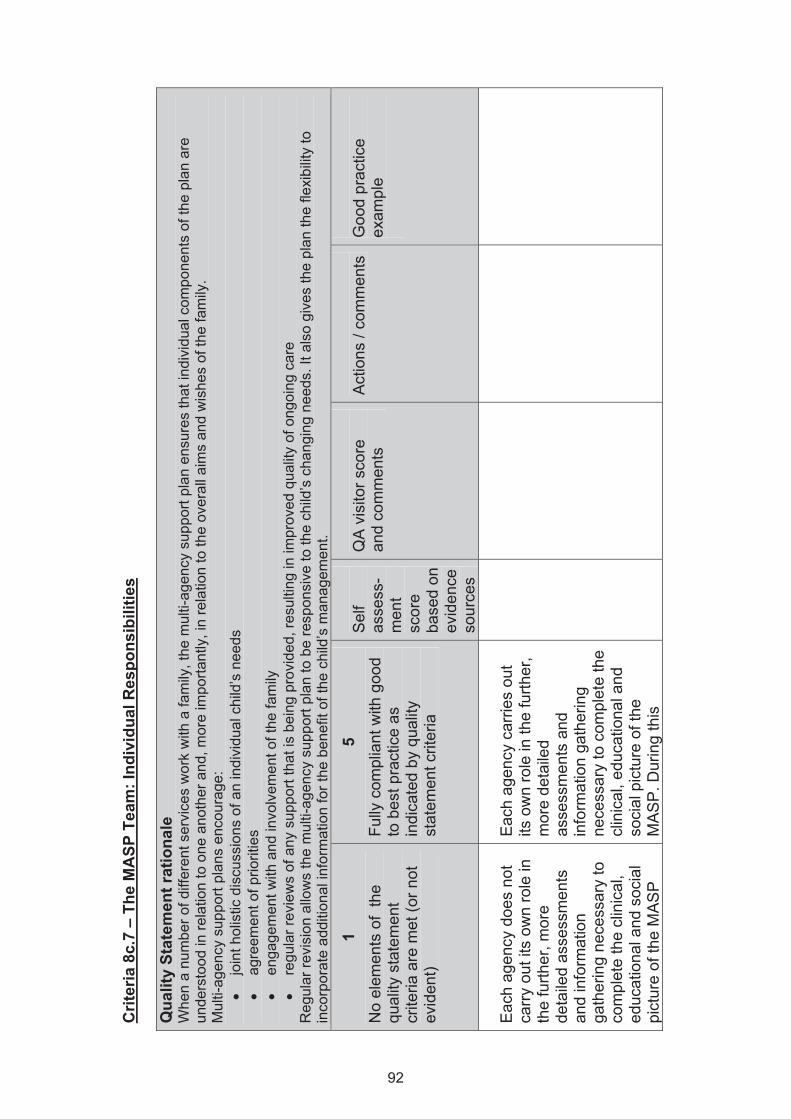
Crit
eria
8c.
7 –
The
MA
SP T
eam
: Ind
ivid
ual R
espo
nsib
ilitie
s Q
ualit
y St
atem
ent r
atio
nale
W
hen
a nu
mbe
r of d
iffer
ent s
ervi
ces
wor
k w
ith a
fam
ily, t
he m
ulti-
agen
cy s
uppo
rt pl
an e
nsur
es th
at in
divi
dual
com
pone
nts
of th
e pl
an a
re
unde
rsto
od in
rela
tion
to o
ne a
noth
er a
nd, m
ore
impo
rtant
ly, i
n re
latio
n to
the
over
all a
ims
and
wis
hes
of th
e fa
mily
. M
ulti-
agen
cy s
uppo
rt pl
ans
enco
urag
e:
• jo
int h
olis
tic d
iscu
ssio
ns o
f an
indi
vidu
al c
hild
’s n
eeds
•
agre
emen
t of p
riorit
ies
• en
gage
men
t with
and
invo
lvem
ent o
f the
fam
ily
• re
gula
r rev
iew
s of
any
sup
port
that
is b
eing
pro
vide
d, re
sulti
ng in
impr
oved
qua
lity
of o
ngoi
ng c
are
Reg
ular
revi
sion
allo
ws
the
mul
ti-ag
ency
sup
port
plan
to b
e re
spon
sive
to th
e ch
ild’s
cha
ngin
g ne
eds.
It a
lso
give
s th
e pl
an th
e fle
xibi
lity
to
inco
rpor
ate
addi
tiona
l inf
orm
atio
n fo
r the
ben
efit
of th
e ch
ild’s
man
agem
ent.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Eac
h ag
ency
doe
s no
t ca
rry o
ut it
s ow
n ro
le in
th
e fu
rther
, mor
e de
taile
d as
sess
men
ts
and
info
rmat
ion
gath
erin
g ne
cess
ary
to
com
plet
e th
e cl
inic
al,
educ
atio
nal a
nd s
ocia
l pi
ctur
e of
the
MA
SP
Eac
h ag
ency
car
ries
out
its o
wn
role
in th
e fu
rther
, m
ore
deta
iled
asse
ssm
ents
and
in
form
atio
n ga
ther
ing
nece
ssar
y to
com
plet
e th
e cl
inic
al, e
duca
tiona
l and
so
cial
pic
ture
of t
he
MA
SP
. Dur
ing
this
92
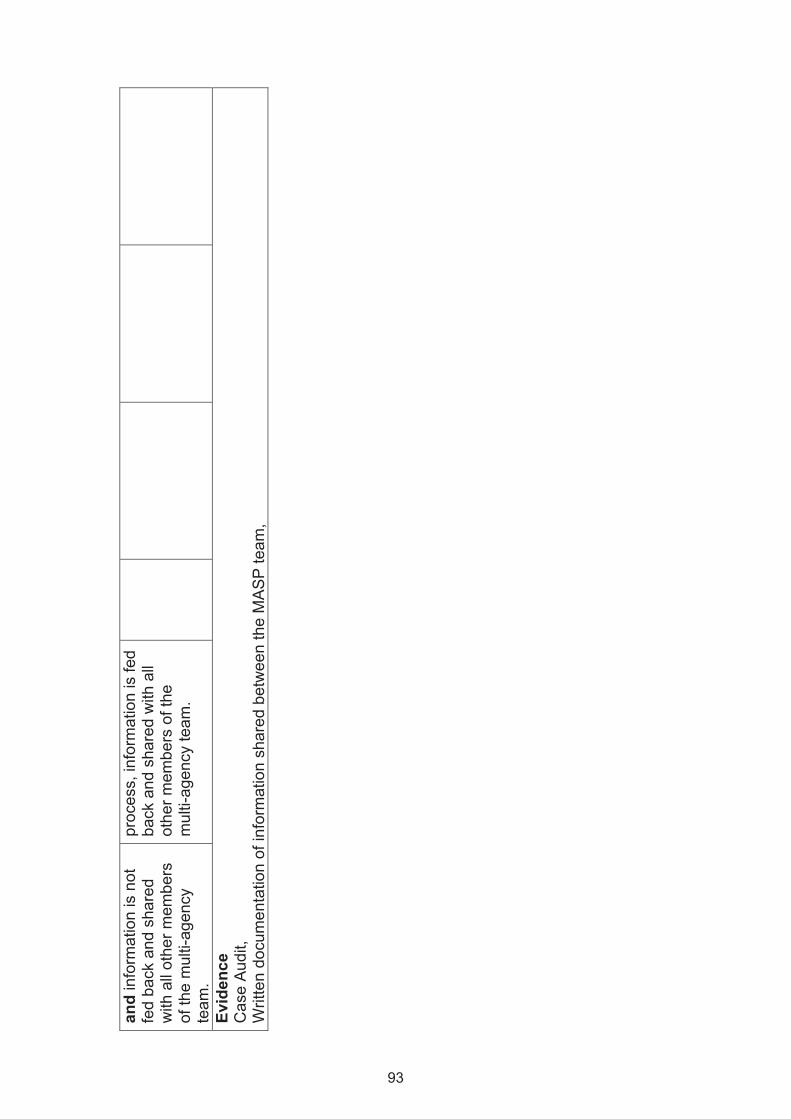
and
info
rmat
ion
is n
ot
fed
back
and
sha
red
with
all
othe
r mem
bers
of
the
mul
ti-ag
ency
te
am.
proc
ess,
info
rmat
ion
is fe
d ba
ck a
nd s
hare
d w
ith a
ll ot
her m
embe
rs o
f the
m
ulti-
agen
cy te
am.
Ev
iden
ce
Cas
e A
udit,
W
ritte
n do
cum
enta
tion
of in
form
atio
n sh
ared
bet
wee
n th
e M
AS
P te
am,
93
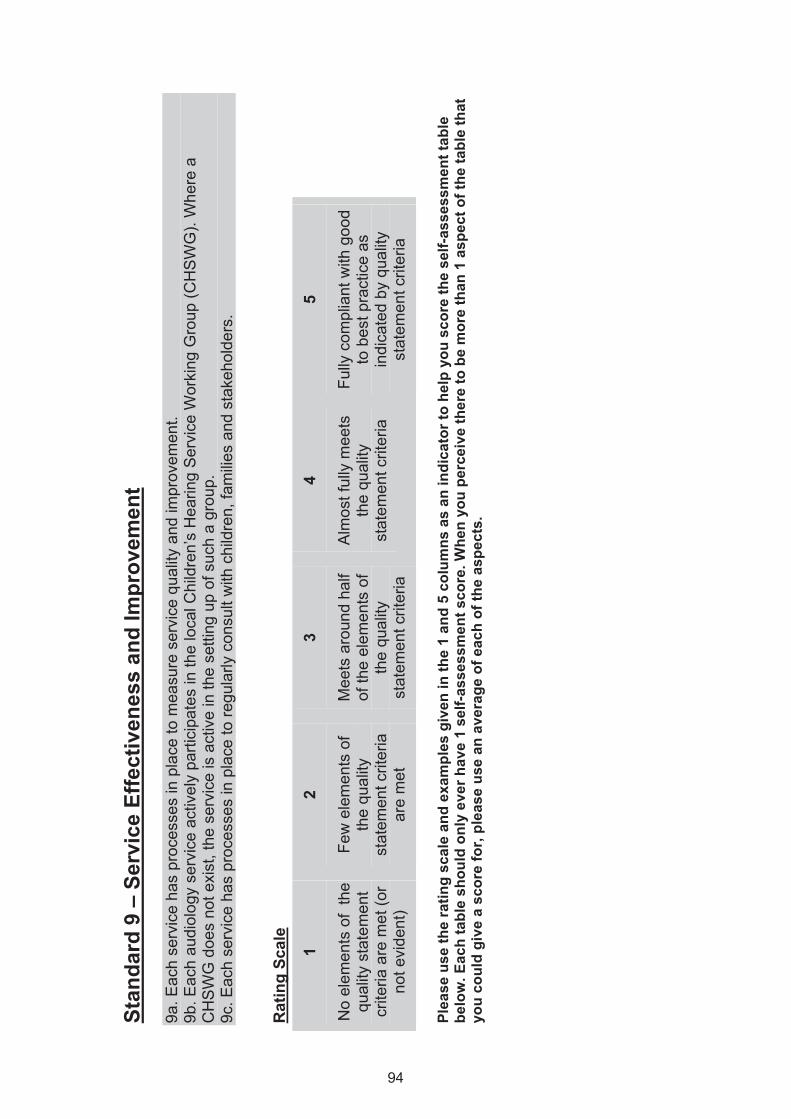
Stan
dard
9 –
Ser
vice
Effe
ctiv
enes
s an
d Im
prov
emen
t 9a
. Eac
h se
rvic
e ha
s pr
oces
ses
in p
lace
to m
easu
re s
ervi
ce q
ualit
y an
d im
prov
emen
t. 9b
. Eac
h au
diol
ogy
serv
ice
activ
ely
parti
cipa
tes
in th
e lo
cal C
hild
ren’
s H
earin
g S
ervi
ce W
orki
ng G
roup
(CH
SW
G).
Whe
re a
C
HS
WG
doe
s no
t exi
st, t
he s
ervi
ce is
act
ive
in th
e se
tting
up
of s
uch
a gr
oup.
9c
. Eac
h se
rvic
e ha
s pr
oces
ses
in p
lace
to re
gula
rly c
onsu
lt w
ith c
hild
ren,
fam
ilies
and
stak
ehol
ders
. R
atin
g Sc
ale
1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or
not e
vide
nt)
2
Few
ele
men
ts o
f th
e qu
ality
st
atem
ent c
riter
ia
are
met
3
Mee
ts a
roun
d ha
lf of
the
elem
ents
of
the
qual
ity
stat
emen
t crit
eria
4
Alm
ost f
ully
mee
ts
the
qual
ity
stat
emen
t crit
eria
5
Fully
com
plia
nt w
ith g
ood
to b
est p
ract
ice
as
indi
cate
d by
qua
lity
stat
emen
t crit
eria
Pl
ease
use
the
ratin
g sc
ale
and
exam
ples
giv
en in
the
1 an
d 5
colu
mns
as
an in
dica
tor t
o he
lp y
ou s
core
the
self-
asse
ssm
ent t
able
be
low
. Eac
h ta
ble
shou
ld o
nly
ever
hav
e 1
self-
asse
ssm
ent s
core
. Whe
n yo
u pe
rcei
ve th
ere
to b
e m
ore
than
1 a
spec
t of t
he ta
ble
that
yo
u co
uld
give
a s
core
for,
plea
se u
se a
n av
erag
e of
eac
h of
the
aspe
cts.
94
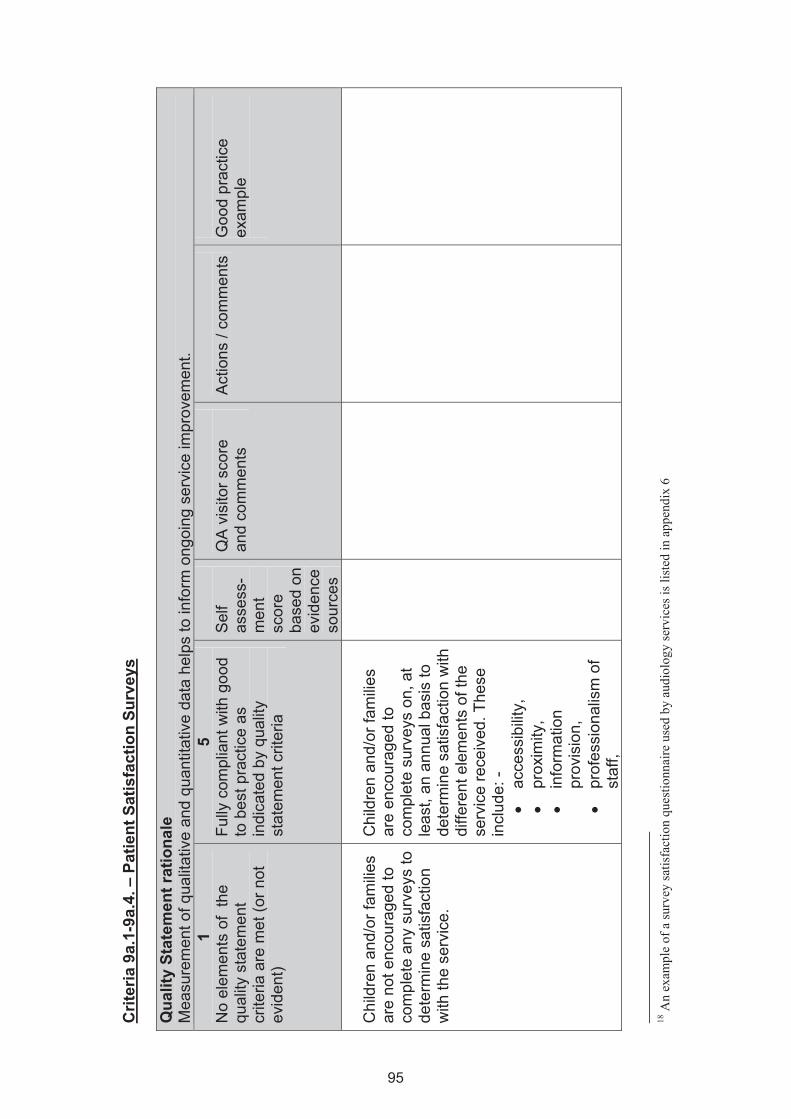
Crit
eria
9a.
1-9a
.4. –
Pat
ient
Sat
isfa
ctio
n Su
rvey
s Q
ualit
y St
atem
ent r
atio
nale
M
easu
rem
ent o
f qua
litat
ive
and
quan
titat
ive
data
hel
ps to
info
rm o
ngoi
ng s
ervi
ce im
prov
emen
t. 1
No
elem
ents
of
the
qual
ity s
tate
men
t cr
iteria
are
met
(or n
ot
evid
ent)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Chi
ldre
n an
d/or
fam
ilies
are
not e
ncou
rage
d to
co
mpl
ete
any
surv
eys
to
dete
rmin
e sa
tisfa
ctio
n w
ith th
e se
rvic
e.
Chi
ldre
n an
d/or
fam
ilies
are
enco
urag
ed to
co
mpl
ete
surv
eys
on, a
t le
ast,
an a
nnua
l bas
is to
de
term
ine
satis
fact
ion
with
di
ffere
nt e
lem
ents
of t
he
serv
ice
rece
ived
. The
se
incl
ude:
- •
acce
ssib
ility,
•
prox
imity
, •
info
rmat
ion
prov
isio
n,
• pr
ofes
sion
alis
m o
f st
aff,
18
An
exam
ple
of a
surv
ey sa
tisfa
ctio
n qu
estio
nnai
re u
sed
by a
udio
logy
serv
ices
is li
sted
in a
ppen
dix
6
95
• ca
re a
nd tr
eatm
ent
and
• ov
eral
l ser
vice
re
ceiv
ed.
P
artic
ipat
ion
rate
s in
the
surv
ey a
re c
heck
ed,
annu
ally
, to
ensu
re a
n ac
cept
able
pro
porti
on o
f pa
tient
s ha
ve p
artic
ipat
ed
and
a re
pres
enta
tive
sam
ple
of th
e lo
cal
popu
latio
n is
cov
ered
(in
clud
ing
gend
er a
nd
ethn
icity
). S
uffic
ient
ana
lysi
s an
d in
terp
reta
tion
of fi
ndin
gs
from
sat
isfa
ctio
n su
rvey
s ar
e ca
rrie
d ou
t ann
ually
by
audi
olog
y se
rvic
es.
Act
ion
plan
s ar
e im
plem
ente
d, w
hen
need
ed, t
o ad
dres
s ar
eas
of c
once
rn a
risin
g fro
m
surv
eys18
and
QR
T da
ta
and
perfo
rman
ce.
Evid
ence
C
opie
s of
sur
veys
and
resp
onse
s A
ctio
n pl
ans
96
Crit
eria
9b.
1 –
CH
SWG
Rev
iew
Mee
tings
Q
ualit
y St
atem
ent r
atio
nale
C
lose
wor
king
with
par
ents
as
wel
l as
acro
ss o
rgan
isat
ions
will
lead
to im
prov
ed s
ervi
ces
for d
eaf c
hild
ren
and
thei
r fam
ilies
. E
ffect
ive
recr
uitm
ent t
o C
HS
WG
s w
ill e
nsur
e ap
prop
riate
repr
esen
tatio
n fo
r the
chi
ld a
nd fa
mily
, and
dem
onst
rate
s a
truly
incl
usiv
e ap
proa
ch.
CH
WS
Gs
can
ensu
re th
at c
hild
ren’
s he
arin
g se
rvic
es re
mai
n hi
gh o
n th
e ag
enda
of t
hose
resp
onsi
ble
for p
lann
ing
and
deliv
erin
g se
rvic
es a
t a
stra
tegi
c le
vel.
They
can
offe
r adv
ice
and
guid
ance
to e
nsur
e hi
gh q
ualit
y se
rvic
es a
re a
vaila
ble.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
CH
SW
G d
oes
not
mee
t reg
ular
ly to
revi
ew
the
mul
ti-ag
ency
se
rvic
es fo
r chi
ldre
n an
d th
eir f
amilie
s kn
own
to h
ave,
or c
onsi
dere
d to
be
at ri
sk o
f hav
ing,
a
hear
ing
impa
irmen
t.
The
CH
SW
G m
eets
re
gula
rly to
revi
ew th
e m
ulti-
agen
cy s
ervi
ces
for
child
ren
and
thei
r fam
ilies
know
n to
hav
e, o
r co
nsid
ered
to b
e at
risk
of
havi
ng, a
hea
ring
impa
irmen
t.
Evid
ence
W
ritte
n, d
ocum
ente
d m
inut
es fr
om C
HS
WG
revi
ew m
eetin
gs.
97
Crit
eria
9b.
2 –
CH
SWG
Sup
port
Q
ualit
y St
atem
ent r
atio
nale
C
lose
wor
king
with
par
ents
as
wel
l as
acro
ss o
rgan
isat
ions
will
lead
to im
prov
ed s
ervi
ces
for d
eaf c
hild
ren
and
thei
r fam
ilies
. E
ffect
ive
recr
uitm
ent t
o C
HS
WG
s w
ill e
nsur
e ap
prop
riate
repr
esen
tatio
n fo
r the
chi
ld a
nd fa
mily
, and
dem
onst
rate
s a
truly
incl
usiv
e ap
proa
ch.
CH
WS
Gs
can
ensu
re th
at c
hild
ren’
s he
arin
g se
rvic
es re
mai
n hi
gh o
n th
e ag
enda
of t
hose
resp
onsi
ble
for p
lann
ing
and
deliv
erin
g se
rvic
es a
t a
stra
tegi
c le
vel.
They
can
offe
r adv
ice
and
guid
ance
to e
nsur
e hi
gh q
ualit
y se
rvic
es a
re a
vaila
ble.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
CH
SW
G d
oes
not
offe
r sup
port
to a
ny
agen
cies
invo
lved
with
he
arin
g lo
ss.
The
CH
SW
G h
elps
to
deve
lop
and
impr
ove
the
serv
ices
del
iver
ed to
dea
f ch
ildre
n an
d th
eir f
amilie
s th
roug
h th
e pr
oces
ses
of
ongo
ing
supp
ort t
o al
l ag
enci
es in
volv
ed.
Evid
ence
E
vide
nce
of c
onta
ct a
nd c
orre
spon
denc
e be
twee
n ag
enci
es a
s a
resu
lt of
CH
SW
G m
eetin
gs.
Min
utes
/act
ion
log
from
CH
SW
G m
eetin
gs..
98
Crit
eria
9b.
3 –
CH
SWG
Mon
itorin
g Q
ualit
y St
atem
ent r
atio
nale
C
lose
wor
king
with
par
ents
as
wel
l as
acro
ss o
rgan
isat
ions
will
lead
to im
prov
ed s
ervi
ces
for d
eaf c
hild
ren
and
thei
r fam
ilies
. E
ffect
ive
recr
uitm
ent t
o C
HS
WG
s w
ill e
nsur
e ap
prop
riate
repr
esen
tatio
n fo
r the
chi
ld a
nd fa
mily
, and
dem
onst
rate
s a
truly
incl
usiv
e ap
proa
ch.
CH
WS
Gs
can
ensu
re th
at c
hild
ren’
s he
arin
g se
rvic
es re
mai
n hi
gh o
n th
e ag
enda
of t
hose
resp
onsi
ble
for p
lann
ing
and
deliv
erin
g se
rvic
es a
t a
stra
tegi
c le
vel.
They
can
offe
r adv
ice
and
guid
ance
to e
nsur
e hi
gh q
ualit
y se
rvic
es a
re a
vaila
ble.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
CH
SW
G d
oes
not
mon
itor t
he e
xten
t to
whi
ch s
ervi
ces
mee
t the
st
anda
rds
deta
iled
in
this
doc
umen
t.
CH
SW
G m
onito
rs th
e ex
tent
to w
hich
ser
vice
s m
eet t
he s
tand
ards
de
taile
d in
this
doc
umen
t.
Evid
ence
W
ritte
n do
cum
enta
tion
of C
HS
WG
mon
itorin
g/re
porti
ng h
ow w
ell s
ervi
ces
mee
t the
se s
tand
ards
. R
evie
w o
f QR
T sc
orin
g on
CH
SW
G a
gend
as.
99
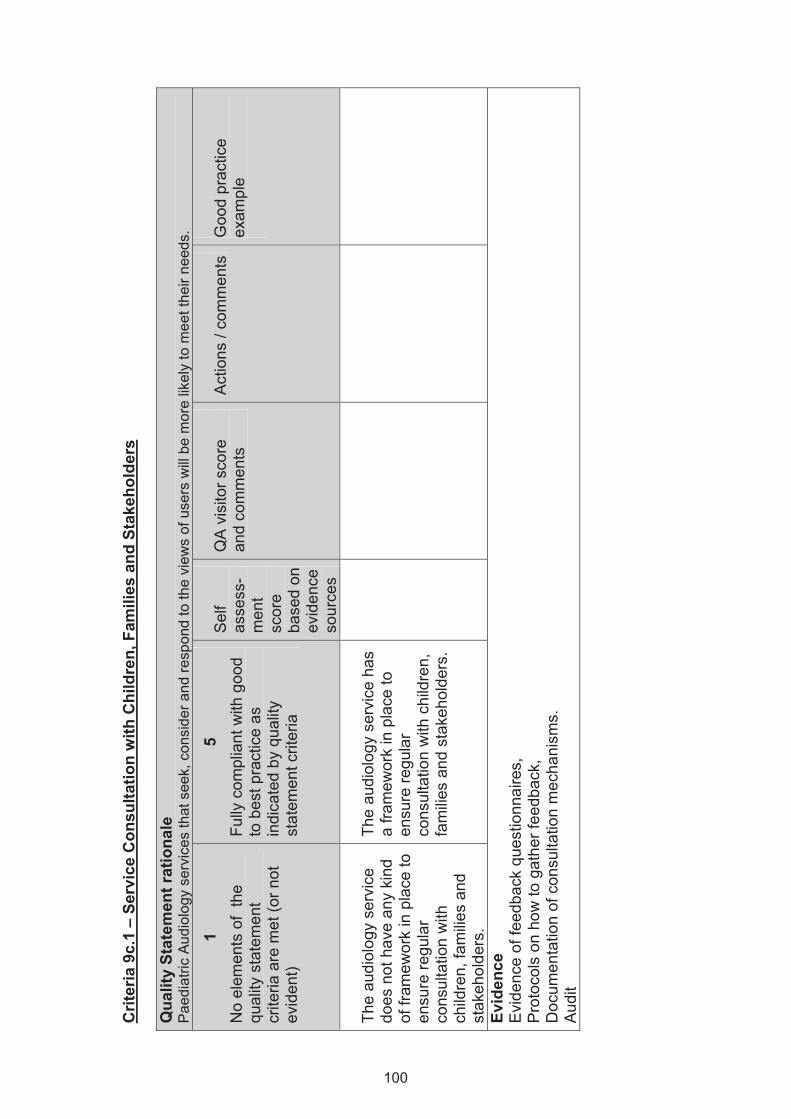
Crit
eria
9c.
1 –
Serv
ice
Con
sulta
tion
with
Chi
ldre
n, F
amili
es a
nd S
take
hold
ers
Qua
lity
Stat
emen
t rat
iona
le
Pae
diat
ric A
udio
logy
ser
vice
s th
at s
eek,
con
side
r and
resp
ond
to th
e vi
ews
of u
sers
will
be
mor
e lik
ely
to m
eet t
heir
need
s.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
The
audi
olog
y se
rvic
e do
es n
ot h
ave
any
kind
of
fram
ewor
k in
pla
ce to
en
sure
regu
lar
cons
ulta
tion
with
ch
ildre
n, fa
milie
s an
d st
akeh
olde
rs.
The
audi
olog
y se
rvic
e ha
s a
fram
ewor
k in
pla
ce to
en
sure
regu
lar
cons
ulta
tion
with
chi
ldre
n,
fam
ilies
and
stak
ehol
ders
.
Evid
ence
E
vide
nce
of fe
edba
ck q
uest
ionn
aire
s,
Pro
toco
ls o
n ho
w to
gat
her f
eedb
ack,
D
ocum
enta
tion
of c
onsu
ltatio
n m
echa
nism
s.
Aud
it
100
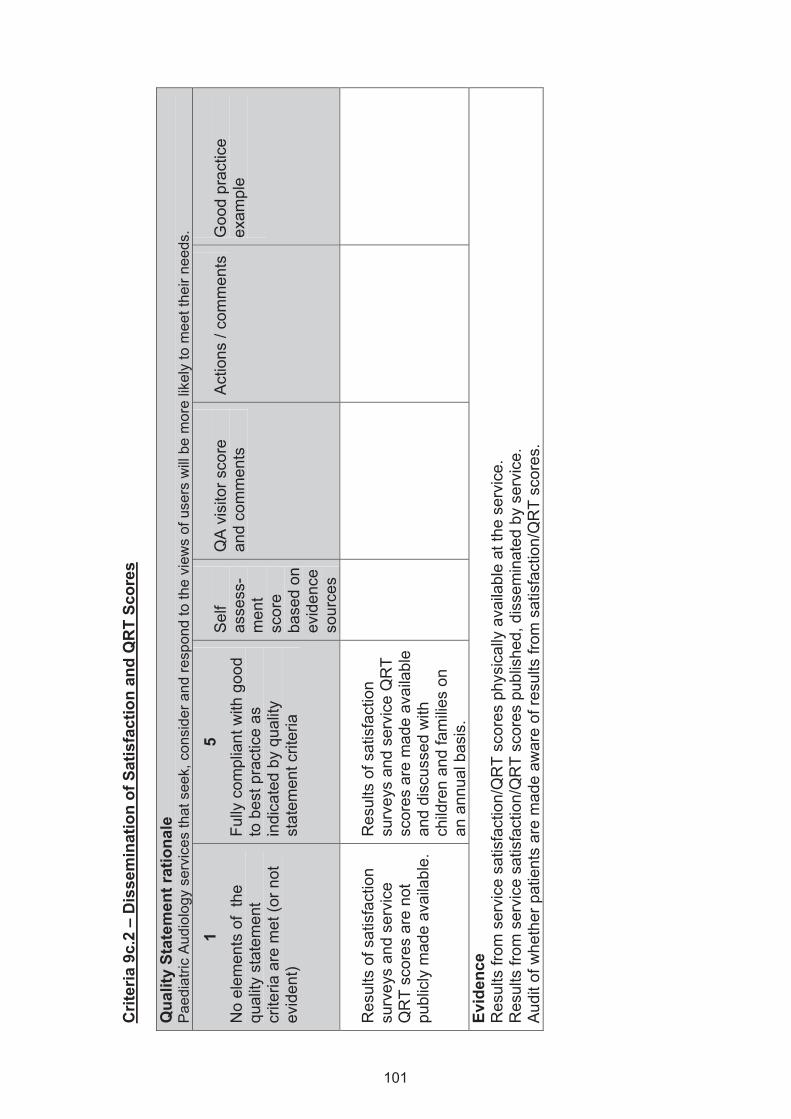
Crit
eria
9c.
2 –
Dis
sem
inat
ion
of S
atis
fact
ion
and
QR
T Sc
ores
Q
ualit
y St
atem
ent r
atio
nale
P
aedi
atric
Aud
iolo
gy s
ervi
ces
that
see
k, c
onsi
der a
nd re
spon
d to
the
view
s of
use
rs w
ill b
e m
ore
likel
y to
mee
t the
ir ne
eds.
1 N
o el
emen
ts o
f th
e qu
ality
sta
tem
ent
crite
ria a
re m
et (o
r not
ev
iden
t)
5 Fu
lly c
ompl
iant
with
goo
d to
bes
t pra
ctic
e as
in
dica
ted
by q
ualit
y st
atem
ent c
riter
ia
Sel
f as
sess
-m
ent
scor
e ba
sed
on
evid
ence
so
urce
s
QA
vis
itor s
core
an
d co
mm
ents
Act
ions
/ co
mm
ents
G
ood
prac
tice
exam
ple
Res
ults
of s
atis
fact
ion
surv
eys
and
serv
ice
QR
T sc
ores
are
not
pu
blic
ly m
ade
avai
labl
e.
Res
ults
of s
atis
fact
ion
surv
eys
and
serv
ice
QR
T sc
ores
are
mad
e av
aila
ble
and
disc
usse
d w
ith
child
ren
and
fam
ilies
on
an a
nnua
l bas
is.
Evid
ence
R
esul
ts fr
om s
ervi
ce s
atis
fact
ion/
QR
T sc
ores
phy
sica
lly a
vaila
ble
at th
e se
rvic
e.
Res
ults
from
ser
vice
sat
isfa
ctio
n/Q
RT
scor
es p
ublis
hed,
dis
sem
inat
ed b
y se
rvic
e.
Aud
it of
whe
ther
pat
ient
s ar
e m
ade
awar
e of
resu
lts fr
om s
atis
fact
ion/
QR
T sc
ores
.
101
APPENDIX 1: References and Evidence Base Introduction Public Health Institute of Scotland ( PHIS) Needs Assessment Report on NHS Audiology Services in Scotland 1993 Quality Improvement Scotland, www.nhshealthquality.org Development of the Quality standards for Paediatric Audiology Services Fortnum H, Summerfield Q, Marshall D, Davis A, Bamford J . Prevalence of permanent childhood hearing impairment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study. British Medical Journal 2001;323: 536 Casselbrant ML, Mandel EM. Epidemiology. In: Rosenfeld RM, Bluestone CD, eds. Evidence-based otitis media. Hamilton, British Columbia, Canada: Decker, Inc, 1999:117–37 Conrad R. The deaf schoolchild: language and cognitive function. London: Harper and Row, 1979 Wood D, Wood H, Griffiths A, Howarth I. Teaching and talking with deaf children. Chichester: Wiley 1996 Bennett KE, Haggard MP. Behaviour and cognitive outcomes from middle ear disease. Arch Dis Chil 1999;80:28-35 Paradise JL, Dollaghan CA, Campbell TF, Feldman HM, Bernard BS, Colborn DK, et al. Language, speech sound production, and cognition in 3-year-old children in relation to otitis media in their first 3 years of life. Pediatrics 2000;105:1119-30 Vernon-Feagans L. Impact of otitis media on speech, language, cognition, and behavior. In: Rosenfeld RM, Bluestone CD, eds. Evidence-based otitis media. Hamilton: British Columbia, Canada: Decker, Inc, 1999:353–73 Standard 1 Yoshinaga-Itano C. Sedey A. Coutter D. Mehl A. (1998) Language of early and later deafened children with hearing loss, Peadiatrics, 102, 1161-1171 Moeller MP.(2000) Early Intervention and language development in children who are deaf and hard of hearing. Pediatrics, 106(3) 1-9 Hind S. Davis A. Outcomes for children with permanent hearing impairment. In Seewald R, ed A sound foundation through early amplification. Procedings of the international conference sponsored by Phonak Oct 1998, Chicago, Illinois USA. Staefa Switzerland: Phonak AG 2000: 199-212 NDCS Quality Standards in Paediatric Audiology: vol IV ( 2000) Guidelines for the Early Identification and the Audiological Management of Children with Hearing Loss
102
Vernon-Feagans L. Impact of otitis media on speech, language, cognition, and behaviour. In: Rosenfeld RM, Bluestone CD, eds. Evidence-based otitis media. Hamilton: British Columbia, Canada: Decker, Inc, 1999:353–73 Jonathan Parsons. Redesigning Audiology/ENT Patient Pathway (RD&E/Devon PCT), www.swirl.nhs.uk/resource/115/ Standard 2 Transforming Services for Children with Hearing Difficulty and their Families (Department of Health, August 2008) Modernising Childrens’ Hearing Aid Services http://www.psych-sci.manchester.ac.uk/mchas/ NHS Newborn Hearing Screening Programme. Tympanometry in babies under 6 months : a recommended test protocol 2008 http://hearing.screening.nhs.uk/getdata.php?id=135 NHS Newborn Hearing Screening Programme. Visual reinforcement audiometry testing of infants : a recommended test protocol. Anonymous. Anonymous. 2008. http://hearing.screening.nhs.uk/getdata.php?id=10490 Do Once and Share: http://www.mrchear.info/cms/Resources.aspx?Action=Folder&ResourceID=177 British Society of Audiology (BSA) Procedure:Pure tone air and bone conductionthreshold audiometrywith and without maskinand determination of uncomfortable loudness levels (2004) Acoustics. Audiometric test methods – Part 1: Basic pure tone air and bone conduction threshold audiometry, BS EN ISO 8253-1:1998 Standard 3 Getting it right for every child, www.scotland.gov.uk/gettingitright/publications Moeller MP.(2000) Early Intervention and language development in children who are deaf and hard of hearing. Pediatrics, 106(3) 1-9 Calderon R Journal of deaf studies and deaf education 2000, vol. 5, no2, pp. 140-155 (1 p.1/4), Parental involvement in deaf children's education programs as a predictor of child's language, early reading, and social-emotional development Early years support programme http://www.earlysupport.org.uk/ Together from the start practical guidance for professionals working with disabled children (birth to third birthday) and their families, Department of Health publications National Deaf Children’s Society (NDCS) (2000) Quality Standards in Paediatric Audiology - Guidelines for the early identification and the audiological management of children with hearing loss, Volume IV. NDCS.
103
Standard 4 MCHAS Guidline; Guidelines for the Fitting, Verification and Evaluation of digital signal processing hearing aids within a Children’s Hearing Aid Service, www.psych-sci.manchester.ac.uk/mchas/guidelines/ Strauss S, Van DC. Hearing instrument fittings of pre-school children: Do we meet the prescription goals? International Journal of Audiology. 2008;47:S62-S71. National Services Framework for Children, Young People and Maternity Services in Wales (2006). Welsh Assembly Government National service framework for children, young people and maternity services 2004, Department of Health Getting it right for every child (2008), Scottish Government Standard 5 MCHAS Guidline; Guidelines for the Fitting, Verification and Evaluation of digital signal processing hearing aids within a Children’s Hearing Aid Service, www.psych-sci.manchester.ac.uk/mchas/guidelines/ Rotteveel LJ. Snik AF. Vermeulen AM. Cremers CW. Mylanus EA. Speech perception in congenitally, pre-lingually and post-lingually deaf children expressed in an equivalent hearing loss value. Clinical Otolaryngology. 33(6):560-9, 2008 Dec. Nikolopoulos TP. Archbold SM. Gregory S. Young deaf children with hearing aids or cochlear implants: early assessment package for monitoring progress. International Journal of Pediatric Otorhinolaryngology. 69(2):175-86, 2005 Feb Ching TY, Hill M, Dillon H. Effect of variations in hearing-aid frequency response on real-life functional performance of children with severe or profound hearing loss. International Journal of Audiology. 2008;47:461-475. Vohr B, Jodoin-Krauzyk J, Tucker R, Johnson MJ, Topol D, Ahlgren M. Early language outcomes of early-identified infants with permanent hearing loss at 12 to 16 months of age. Pediatrics. 2008;122:535-545. Aetiological Investigations into severe and profound hearing loss in children, British Association of Audiovestibular Physicians, British association of Paediatricians in Audiology, October 2008 Medical management of infants with significant congenital hearing loss identified through the national newborn hearing screening programme. Best Practice Guidelines, http://hearing.screening.nhs.uk/standards Standard 6 HPC –Standards of proficiency of registered practitioners - http://www.hpc-uk.org/publications/standards/index.asp?id=42 Department of Health (2004) The NHS Knowledge and Skills Framework and the Development review Process. Department of Health Publications
104
Role of the doctor in the NHSP team, British Association of Audiolgoical Physicians (BAAP) National Deaf Children’s Society (NDCS) (2000) Quality Standards in Paediatric Audiology - Guidelines for the early identification and the audiological management of children with hearing loss, Volume IV. NDCS. Transforming Services for Children with Hearing Difficulty and their Families (Department of Health, August 2008) Standard 7 Clinical Standards Board for Scotland. 2002. Clinical Standards: Generic. Edinburgh: Clinical Standards Board for Scotland. www.clinicalstandards.org/pdf/finalstand/generic.pdf [access to full document] Greenberg PB, Walker C, Buchbinder R. Optimisong communication between consumers and clinicians. Medical Journal of Australia. 2006 Vol 185(5) 246-247 National Deaf Children’s Society (NDCS) website; http://www.ndcs.org.uk Baguley D, Davis A & Bamford J (2000) Principles of family-friendly hearing services for children. BSA News 29, 35-39. Mitchell W & Sloper P (2000) User-friendly information for families with disabled children: a guide to good practice. Joseph Rowntree Foundation. Standard 8 Eleweke CJ, Gilbert S, Bays D, Austin E. Information about support services for families of young children with hearing loss: A review of some useful outcomes and challenges. Deafness & Education International. 2008;10:190-213. Fitzpatrick E, Angus D, Durieux-Smith A, Graham ID, Coyle D. Parents' needs following identification of childhood hearing loss. American Journal of Audiology. 2008;17:38-50. MCHAS Guidline: Guidelines for professional links between audiology and education services within a children’s hearing aid service, www.psych-sci.manchester.ac.uk/mchas/guidelines/ Quality standards and good practice guidelines: transition from paediatric to adult audiology services 2005, NDCS Department for Children, Schools and Families (DCSF) and Department of Health (DH). A Transition Guide for all Services. Key Information for Professionals about the Transition Process for Disabled Young People. 2007 Early Years and Early Intervention: A joint Scottish Government and COSLA policy statement (2008) Scottish Government
105
Appendix 2 – Range of Audiological Assessments Staff must have the appropriate knowledge, practical skills, competencies and experience to perform and interpret the results of all the assessments they undertake. It is expected that services should provide, or have arrangements in place to access the following assessments: Auditory Brainstem Response test (ABR)
• click, tone pip,
• air conduction / bone conduction
• cochlear microphonics
• conducted under sedation or anaesthetic if required Auditory Steady State Response Cortical evoked potentials Transient evoked oto-acoustic emissions Distortion products oto-acoustic emissions Tympanometry, including high frequency tympanometry Stapedial reflexes Visual reinforced audiometry
• soundfield
• inserts
• bone conduction Performance testing Play audiometry Toy tests, several modalities Speech testing, using several modalities Pure tone audiometry
• air conduction
• bone conduction
• with masking as required Tertiary centres will also provide Specific tests for further investigation of auditory neuropathy / dyssynchrony Specific tests for further investigation into auditory processing difficulties Assessments for the “difficult to test child” Paediatric vestibular assessments Paediatric tinnitus assessment
106
Appendix 3 – Examples of Good Practice Guidance, Standards and Protocols Modernising Children’s Hearing Aid Services (http://www.psych-sci.manchester.ac.uk/mchas/guidelines/) 1. Guidelines for the taking of impressions and provision of ear moulds within a children’s
hearing aid service 2. Guidelines for professional links between audiology and education services within a
children’s hearing aid service 3. Guidelines for testing digital signal processing hearing aids”in the field” within an integrated
children’s hearing aid service 4. Guidelines for fitting, verification and evaluation of digital signal processing hearing aids
within a children’s hearing aid service 5. Transition from paediatric to adult audiology services: Guidelines for professionals working
with deaf children and young people 6. Procedures for setting up of fm radio systems for use with hearing aids British Society of Audiology Recommended Procedures (http://www.thebsa.org.uk/) 1. Pure tone air and bone conductionthreshold audiometry with and without masking and
determination of uncomfortable loudness levels 2. Tympanometry 3. Taking an aural impression
British Society of Audiology and British Academy of Audiology (http://www.thebsa.org.uk/docs/RecPro/REM.pdf) 1. Guidance on the use of real ear measurements to verify the fitting of digital signal processing
hearing aids NHS Newborn Hearing Screening Programme (http://hearing.screening.nhs.uk/standards) 1. Medical management of infants with significant congenital hearing loss identified through the
national newborn hearing screening programme – Best practice guidelines
2. Audiology protocols for children referred for audiology assessment from the newborn hearing screen
a. Guidelines for the early audiological management and assessment of babies referred from the newborn hearing screen
b. ABR bone conduction testing in babies c. ABR tone pip testing in babies d. Air conduction ABR testing in babies using clicks e. TEOAE testing in babies f. Tympanometry in babies under 6 months g. Behavioural observation audiometry testing in babies h. Distraction diagnostic test protocol i. Visual reinforcement audiometry testing in infants
3. Audiological Calibration a. SLM target values for pure tones and ABR stimuli b. Routine (stage A) checks for ABR systems c. ABR calibration specification
4. Auditory Neuropathy/Auditory Dys-synchrony policy documents 5. Guidelines for surveillance following the newborn hearing screen
107
National Deaf Children’s Society (http://ndcs.org.uk/) 1. Quality Standards in Paediatric Audiology – Guidelines for the early identification and
audiological management of children with hearing loss 2. Quality Standards in the Early years: Guidelines on working with deaf children under two
and their families 3. Quality Standards and Good practice Guidelines: Transition from Child to Adult Services
108
Appendix 4 – Audiology Individual Management Plan (AIMP) AN EXPLANATION OF THE AUDIOLOGY INDIVIDUAL MANAGEMENT PLAN What is an Audiology Individual Management Plan? Individual Management Plans are a set of agreed needs and actions that are developed with the child and family.
The initial plan may simply note the date and time of appointment and any special requirements, and actions taken if appropriate, that have been identified from the referral information (e.g. arranging an interpreter).
At the first appointment a history, appropriate examination and audiological assessment will be undertaken. Information and results from these are documented in a format agreed locally, and will inform ongoing development of the management plan.
As for some children the assessment period may be lengthy, this is included within the Paediatric AIMP.
Who has an Audiology Individual Management Plan?
All children referred to the service will have an AIMP.
Who develops the Audiology Individual Management Plan?
The audiologist, child and family will develop the AIMP together using the information gathered during the assessment and following explanation and discussion about possible care options. When children are being seen within a combined clinic setting, for example with ENT or Paediatric colleagues, then information from the medical clinician must also be considered when developing the plan.
A list of agreed needs and actions will be recorded, a copy of which should be given to the child and family. The format of this information may vary depending on local arrangements. It may be in the form of a letter or completed template sent to the child and family, or a printout from the patient management system for example.
What do Audiology Individual Management Plans look like?
AIMPs will vary greatly depending on the individual child. They will record assessment information, needs and planned actions. When plans are updated the outcomes of actions undertaken will also be recorded.
The AIMP for a child referred to a Community Audiology clinic for a hearing assessment due to speech and language delay who is found to have normal hearing may be very simple. An AIMP for a pre-term baby referred from the hearing screen with additional needs and subsequently found to have a bilateral sensorineural deafness will be more complicated.
Initial AIMPs will be composed mainly of agreed needs and actions. These will be added to through time and the AIMP will also include completed actions and outcomes, detailing a summary of the effect of actions take.
109
What is meant by ‘actions’?
Actions are what the audiologist is going to do, or ask someone else to do, to actually attempt to meet the identified needs. Actions will be specific and directive, probably written in the future tense and attached or relevant to one or more of the needs.
What is meant by ‘completed actions’?
These are actions that the audiologist (or other audiologists / agencies) actually do at each stage (as opposed to plan to do). They will be directly linked to actions and probably written in the past tense.
What is meant by ‘outcomes’?
These will be a summary of the effects of actions and will enable the audiologist to evaluate whether or not the actions have met the needs. Ideally these will be supported by more formal outcome measures.
Outcomes will be linked to needs and may often reference specific actions, They will probably be written in the present tense.
When is a management plan completed?
The management plan is complete when there are no outstanding actions and when outcomes indicate that needs have been met.
Consideration needs to be given as to how you include outcomes or effects of referral to external agencies that may not have been delivered at final follow up appointment.
For children with permanent child hood hearing impairment Paediatric AIMPs will be required until transition to adult services. At that time the adult services will take over the plan.
Information in the Paediatric AIMP will be used to inform the Multi-Agency Support Plan, where one exists.
Audiology Individual Management Plans are not intended to create more work for audiology, but to encourage closer partnership working with children and their families and to provide a means of recording, reviewing, evaluating and updating the agreed needs and actions.
110
Agreed needs are whatever the audiologist and the family have agreed needs to be addressed or managed to ensure that the child has the best possible chance of fulfilling his or her potential. These initial needs will be based on the history, examination, assessment and full discussion with the parent.
What is meant by ‘agreed needs’?
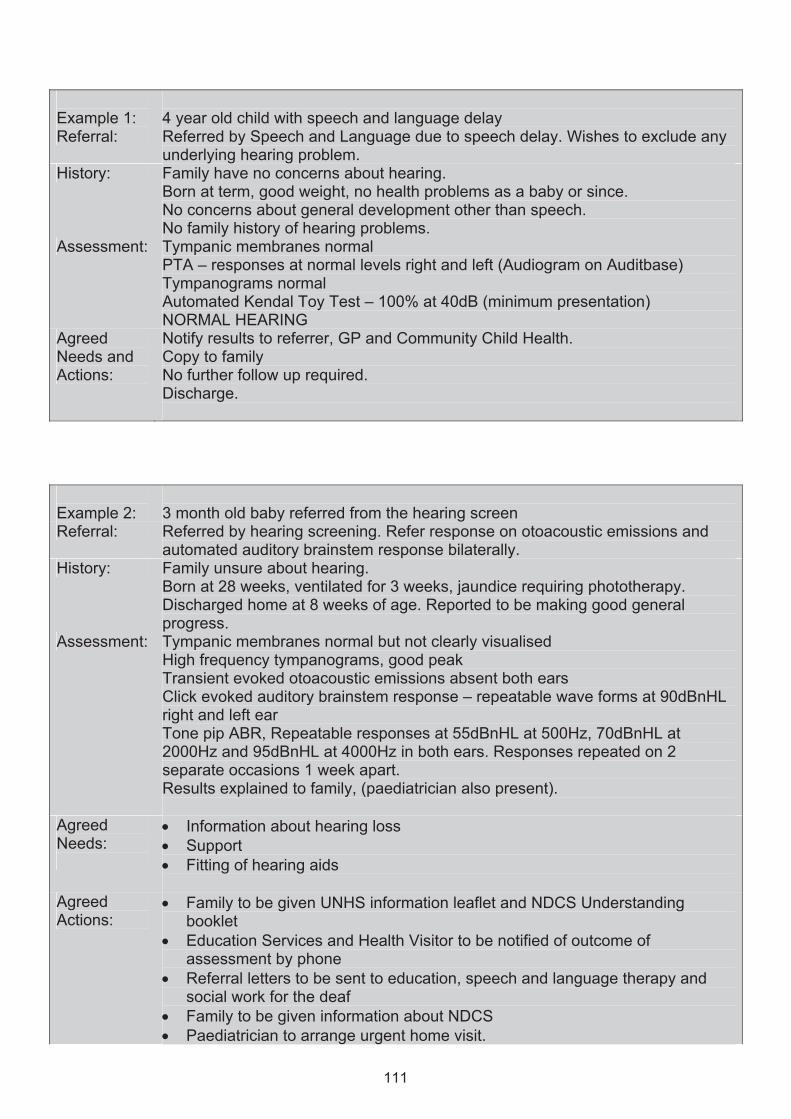
Example 1:
4 year old child with speech and language delay
Referral: Referred by Speech and Language due to speech delay. Wishes to exclude any underlying hearing problem.
History: Family have no concerns about hearing. Born at term, good weight, no health problems as a baby or since. No concerns about general development other than speech. No family history of hearing problems.
Assessment: Tympanic membranes normal PTA – responses at normal levels right and left (Audiogram on Auditbase) Tympanograms normal
NORMAL HEARING Agreed Needs and Actions:
Notify results to referrer, GP and Community Child Health. Copy to family No further follow up required. Discharge.
Example 2:
3 month old baby referred from the hearing screen
Referral: Referred by hearing screening. Refer response on otoacoustic emissions and automated auditory brainstem response bilaterally.
History: Family unsure about hearing. Born at 28 weeks, ventilated for 3 weeks, jaundice requiring phototherapy.
progress. Assessment: Tympanic membranes normal but not clearly visualised
High frequency tympanograms, good peak Transient evoked otoacoustic emissions absent both ears Click evoked auditory brainstem response – repeatable wave forms at 90dBnHL right and left ear Tone pip ABR, Repeatable responses at 55dBnHL at 500Hz, 70dBnHL at 2000Hz and 95dBnHL at 4000Hz in both ears. Responses repeated on 2 separate occasions 1 week apart. Results explained to family, (paediatrician also present).
Agreed Needs:
• Information about hearing loss • Support • Fitting of hearing aids
Agreed Actions:
• Family to be given UNHS information leaflet and NDCS Understanding booklet
• Education Services and Health Visitor to be notified of outcome of assessment by phone
• Referral letters to be sent to education, speech and language therapy and social work for the deaf
• Family to be given information about NDCS • Paediatrician to arrange urgent home visit.
111
Automated Kendal Toy Test – 100% at 40dB (minimum presentation)
Discharged home at 8 weeks of age. Reported to be making good general

• Impressions to be taken for ear moulds • Appontment to be given for hearing aid issue.
Completed Actions
• Family given NDCS information booklets and contact telephone numbers and emails for the paediatric audiology team
• Educational Audiologist and Health Visitor notified by phone • Referral letters sent to
o Education o S< o Social Work for the deaf o Local branch of NDCS
• Home visit arranged for .............. • Impressions for ear moulds taken • Appointment given for hearing aid issue on .........................
112
Local Children’s Hearing Service Specialist Centre Supra-Specialist Centre Appendix 5 – Examples of Outcome Measures and Resources for Evaluating Children’s Hearing Aids
1. Speech Test Resources
• Ling Speech Sounds (http://www.bionicear.com/UserFiles/File/Ling_Six_Sound_Check-6.pdf)
• McCormick Toy Test • Parrot (Recorded versions of the McCormick toy test, including English as an
additional language (EAL) toytest, Manchester picture test and AB word lists (http://www.soundbytesolutions.co.uk/products.htm)
• Phoenix - Automated McCormick toy test with algorithm for establishing thresholds for speech in quiet and speech in noise
• Consonant confusion task (http://www.chears.co.uk/downloads/sptestinfo.pdf) • Auditory Performance test (http://www.chears.co.uk/downloads/sptestinfo.pdf) • AB word lists (http://www.ihr.mrc.ac.uk/products/index.php?products=15) • BKB Sentence lists(http://www.ihr.mrc.ac.uk/products/index.php?products=15) • FAAF test (http://www.ihr.mrc.ac.uk/products/index.php?products=15)
2. Questionnaires
• LIFE - to help evaluate a child’s hearing aids in the classroom • Listening Situations Questionnaire - developed in the UK to provide a means to
evaluate a child’s benefit from hearing aids in the real world (http://www.psych-sci.manchester.ac.uk/mchas/eval/quest/LSQ.pdf)
• PEACH and TEACH – The NAL website has additional information on these tools (http://www.nal.gov.au/nal_products%20front%20page.htm) PEACH booklet, questionnaire and score sheet can be accessed via http://www.psych-sci.manchester.ac.uk/mchas/eval/quest/
113
Appendix 6 – Children’s Hearing Services Working Groups
What are Children’s Hearing Services Working Groups (CHSWGs)? (from http://hearing.screening.nhs.uk) • A CHSWG is a multi-disciplinary group, including service users, which takes the lead in
integrated service delivery for deaf children and their families. • The main focus of the group is both to monitor and to develop and improve the services
delivered to deaf children and their parents and other family members through the processes of ongoing support.
• A CHSWG should operate on both strategic and practical levels.
• The group should be represented by all organisations that are involved in the services
delivered to children and their families, and should include Children’s Services (with health, education and social service input), appropriate Voluntary Sector representation and parents and carers who are service-users.
• The group should be formally organised with a recognised chair. All members of the
group, their views and opinions, should be equally respected by all.
• The CHSWG is a formal group which:-
functions properly and in harmony with other groups to succeed in its goals and objectives
ensures that each member of the group conforms to shared values, attitudes and norms
expects it members to be fully committed to the aims of the group is allowed to make decisions on behalf of the services represented; and direct the
strategic developments of the services offered to deaf children
• The group should work as a team, all members should have mutual respect for individual roles and the contribution each can make whether that is from professional or user perspectives.
• CHSWGs need to continue to plan and be clear in their purpose in order to meet
the changing expectations from national initiatives and work closely with service providers to continue to deliver high quality children’s hearing services.
• The underlying principle of CHSWGs is that working closer with parents as well as across organisations will lead to improved services for deaf children and their families. Effective recruitment of parents to CHSWGs will ensure appropriate representation for the child and family, and demonstrates a truly inclusive approach.
• A key role of the group is to ensure that children’s hearing services remain high on the
agenda of those responsible for planning and delivering services at a strategic level. It should offer advice, guidance and, where necessary, pressure, to ensure high quality services are available.
114
What a CHSWG is not: • A part of other services (e.g. adult audiology, paediatrics, ENT, disability services). The
group should aim to maintain a separate identity to improve the profile of Children’s Hearing Services and to promote the requirements of the service as well as any successes to all of the relevant stakeholders.
• A ‘talking shop’. By being clear about the aims and objectives of the group and by ensuring
the best representation of local services the CHSWG should be a forum where services work closely together to continually monitor and improve services offered to deaf children and their families.
• A group that can operate in isolation from service providers, nor can it be managed as a
group with no real purpose and no accountability. Therefore a CHSWG needs to have the authority to act with the full knowledge and support from all service providers, at a practitioner, managerial and strategic level.
• A group where one person, irrespective of who they are representing, can use the group for
their own or their services’ purposes alone. Nor should the group be wholly dominated by any one (or a small number of members) to such an extent where other group members feel they are not included in the group’s direction or are unable to have an input to any decisions made. The aim of the group is to address all pertinent issues in a collaborative manner.
Further more detailed information about Children’s Hearing Services Working Groups is available at http://hearing.screening.nhs.uk/cms.php?folder=1955
115
Appendix 7 – Example of a Multi-Agency Support Plan
Date of Plan: …………………… Present:
INDIVIDUAL MULTI-AGENCY
SUPPORT PLAN
Name: D.O.B. Address: Telephone Number: Parent/Guardian:
Professionals Involved - Contact Details • Key Worker Teacher of the Deaf/Educational Audiologist
Speech and Language Therapist
Health Visitor
General Practitioner
Audiologist
Child Health Doctor
Social Worker
Consultant
Placement
Educational Psychologist
116
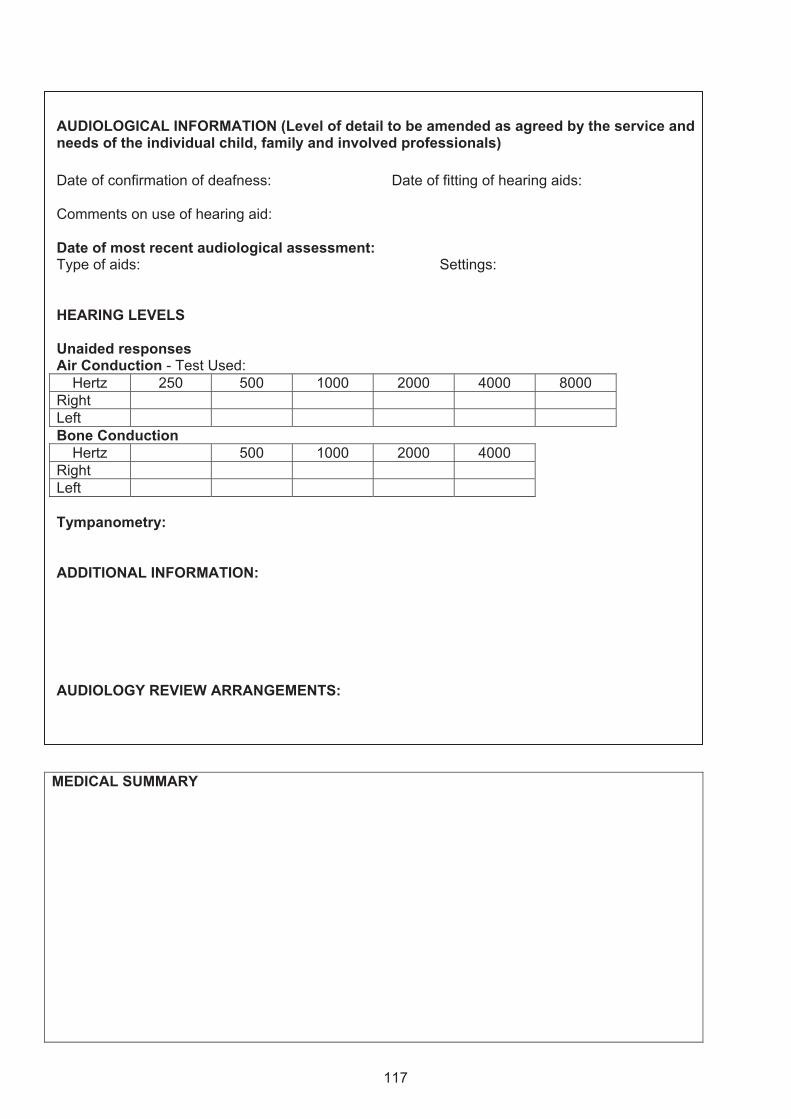
AUDIOLOGICAL INFORMATION (Level of detail to be amended as agreed by the service and needs of the individual child, family and involved professionals) Date of confirmation of deafness: Date of fitting of hearing aids: Comments on use of hearing aid: Date of most recent audiological assessment: Type of aids: Settings: HEARING LEVELS Unaided responses Air Conduction - Test Used:
Hertz 250 500 1000 2000 4000 8000 Right Left Bone Conduction
Hertz 500 1000 2000 4000 Right Left Tympanometry: ADDITIONAL INFORMATION: AUDIOLOGY REVIEW ARRANGEMENTS:
MEDICAL SUMMARY
117
EDUCATION INFORMATION
SPEECH AND LANGUAGE THERAPY INFORMATION
ADDITIONAL INFORMATION / POINTS FOR DISCUSSION
118

ASSESSMENTS and SUPPORTS REQUIRED
Agency Assessment / Input Required
Ongoing / Support / Review
Audiology
Hearing Impaired Education Services
Speech and Language Therapy
Medical
Social Services
Educational Psychology
Technology
Voluntary Agencies
119
ACTION PLAN
Action Item Person Responsible
Date to be completed by
1.
2.
3.
4.
5.
6.
7.
8.
9.
Review Date:
120
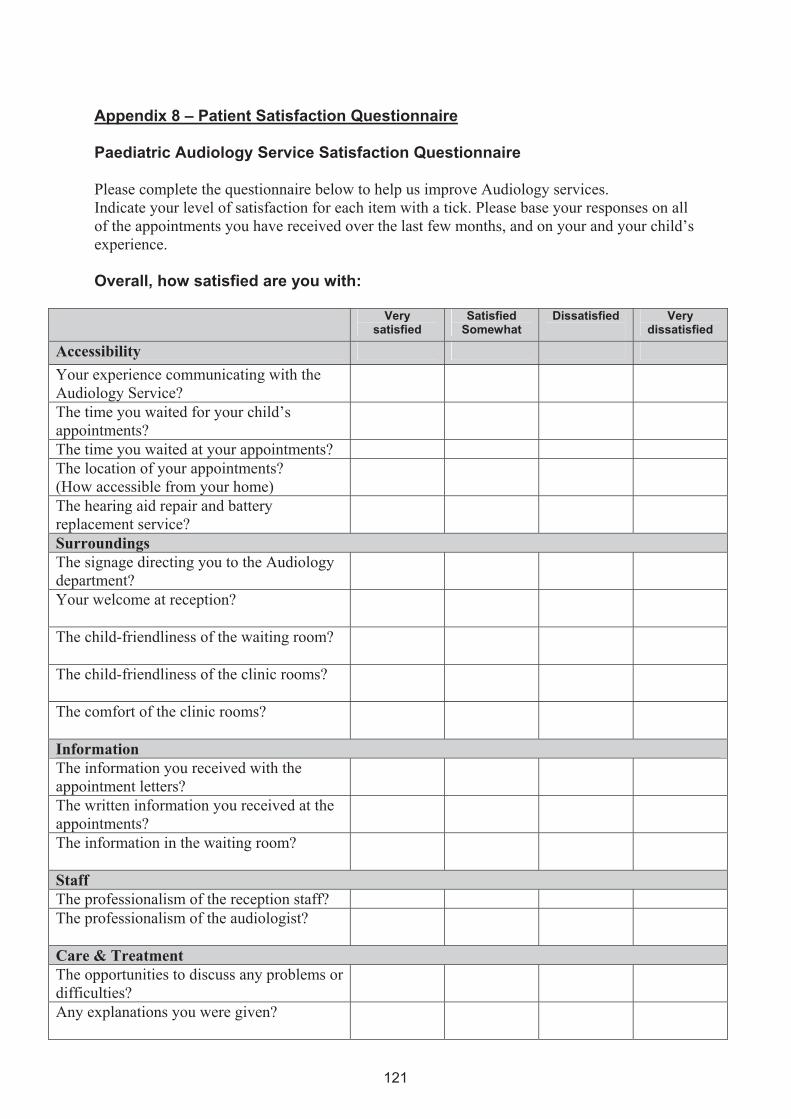
Appendix 8 – Patient Satisfaction Questionnaire Paediatric Audiology Service Satisfaction Questionnaire Please complete the questionnaire below to help us improve Audiology services. Indicate your level of satisfaction for each item with a tick. Please base your responses on all of the appointments you have received over the last few months, and on your and your child’s experience. Overall, how satisfied are you with:
Very satisfied
Satisfied Somewhat
Dissatisfied
Very dissatisfied
Accessibility Your experience communicating with the Audiology Service?
The time you waited for your child’s appointments?
The time you waited at your appointments? The location of your appointments? (How accessible from your home)
The hearing aid repair and battery replacement service?
Surroundings The signage directing you to the Audiology department?
Your welcome at reception?
The child-friendliness of the waiting room?
The child-friendliness of the clinic rooms?
The comfort of the clinic rooms?
Information The information you received with the appointment letters?
The written information you received at the appointments?
The information in the waiting room?
Staff The professionalism of the reception staff? The professionalism of the audiologist?
Care & Treatment The opportunities to discuss any problems or difficulties?
Any explanations you were given?
121
The assessment and management of your child’s hearing needs?
The appropriate involvement of other services?
Overall The audiology service you received?
Please state below one improvement you would make to the Audiology Service or please add any comments?
Section below for completion by Audiology staff: Clinic ________________________________________________ Date ______________ Type of Appointment _________________________________________________________ Comments
122
w w w . s c o t l a n d . g o v . u k
QualityStandards for PaediatricAudiologyServices
© Crown copyright 2009
This document is also available on the Scottish Government website:www.scotland.gov.uk
RR Donnelley B60164 04/09
Further copies are available fromBlackwell’s Bookshop53 South BridgeEdinburghEH1 1YS
Telephone orders and enquiries0131 622 8283 or 0131 622 8258
Fax orders0131 557 8149
Email [email protected]