Embed Size (px)
Citation preview

Accepted Manuscript
Quality of life in treatment of mandibular fractures using closed reduction andmaxillomandibular fixation in comparison with open reduction and internal fixation - Arandomized prospective study -
Kevin U. Omeje, DDS Majeed Rana, MD, DDS Adetokunbo R. Adebola, DDSAkinwale A. Efunkoya, DDS Hector O. Olasoji, DDS Nicolai Purcz, MD, DDS Nils-Claudius Gellrich, MD, DDS Madiha Rana, MSc, PhD, Prof
PII: S1010-5182(14)00205-4
DOI: 10.1016/j.jcms.2014.06.021
Reference: YJCMS 1842
To appear in: Journal of Cranio-Maxillo-Facial Surgery
Received Date: 24 January 2014
Revised Date: 17 June 2014
Accepted Date: 18 June 2014
Please cite this article as: Omeje KU, Rana M, Adebola AR, Efunkoya AA, Olasoji HO, Purcz N,Gellrich N-C, Rana M, Quality of life in treatment of mandibular fractures using closed reduction andmaxillomandibular fixation in comparison with open reduction and internal fixation - A randomizedprospective study -, Journal of Cranio-Maxillofacial Surgery (2014), doi: 10.1016/j.jcms.2014.06.021.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Quality of life in treatment of mandibular fractures using closed
reduction and maxillomandibular fixation in comparison with open
reduction and internal fixation
- A randomized prospective study -
Kevin U. Omeje1,#, DDS, Majeed Rana3,#,*, MD, DDS, Adetokunbo R. Adebola1,
DDS, Akinwale A. Efunkoya1, DDS, Hector O. Olasoji2, DDS, Nicolai Purcz3, MD,
DDS, Nils-Claudius Gellrich3, MD, DDS, Prof., Madiha Rana4, MSc, PhD
1Oral and Maxillofacial Surgery Department, Aminu Kano Teaching Hospital, Kano, Nigeria 2Oral and Maxillofacial Surgery Department, Faculty of Dentistry, University of Maiduguri
Teaching Hospital, Maiduguri, Nigeria
3Department of Personality Psychology and Psychological Assessment, Helmut-Schmidt-
University/University of the German Federal Armed Forces Hamburg, Holstenhofweg 85,
22043 Hamburg, Germany
4Department of Craniomaxillofacial Surgery, Hannover Medical School, Carl-Neuberg-Str. 1,
30625 Hannover, Germany
# contributed equally
*Correspondence to:
Majeed Rana, MD, DDS
Department of Craniomaxillofacial Surgery
Hannover Medical School
Carl-Neuberg-Street 1
D-30625 Hannover, Germany
E-mail: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Quality of life in treatment of mandibular fractures using closed
reduction and maxillomandibular fixation in comparison with
open reduction and internal fixation
- A randomized prospective study -
Abstract
Treatment of mandibular fractures by open reduction and internal fixation (ORIF) is
often assumed to be superior to treatment by close reduction and
maxillomandibular fixation (MMF) because patients managed by ORIF seem to be
rehabilitated earlier according to functional and social aspects. This assumption is
often from surgeon’s perspective, not taking into account patient’s viewpoint. This
study highlights a comparative assessment between ORIF and MMF from the
patients’ perspective.
Fifty six patients with mandibular fractures within the tooth bearing areas of the
mandible were prospectively studied in a randomized controlled pattern for post-
operative Quality of Life (QoL) after ORIF versus MMF. Both groups were analyzed
preoperatively, at 1 day, 6 and 8 weeks regarding their QoL using the General Oral
Health Assessment Index questionnaire (GOHAI). No significant statistical
difference was found between the groups regarding overall QoL. Patients managed
by MMF were more affected by psychosocial and physical domains whereas
patients managed by ORIF were more affected by the pain domain.
The results demonstrate that the treatment affects the psychosocial, physical and
pain domain differentially. When both treatments are possible the patient’s should
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
be enlightened on the advantages and disadvantages of both treatment modalities
to guide their choice of treatment.
Keywords: Quality of life, mandibular fracture, open reduction, closed reduction.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
INTRODUCTION
Quality of life can be defined as peoples’ perception of their position in life in the
context of their culture and value systems, also in relation to their goals,
expectations, standards and concerns (WHO, 1996). QoL as it applies to medicine
is specifically known as Health Related QoL (HR-QoL) or subjective health status
(O’Boyle, 1992; Olschewki et. al, 1994; Infante-Cassio et. al, 2009). QoL studies
measure the effect of illness, disease and its treatment on patients’ welfare by
going beyond the physician dominated indicators of patient’s progress. These
studies also allow patients to define those aspects of the disease condition or
treatment they consider most distressing and to take part in therapeutic decisions.
A QoL study to compare different treatment modalities of mandibular fractures was
carried out in Kano, Nigeria.
HR-QoL and its assessment have become increasingly important in health care,
especially in the field of maxillofacial surgery. There are several studies about the
quality of life of head and neck cancer patients but only few studies on HR-QoL of
patients treated for mandibular fractures (Atchison et. al, 2006). There are however
studies on QoL in patients treated for condylar fractures (Worsaae and Thorn,
1994; Kommers et. al, 2013), as well as studies that assess the psychological
response of patients’ to mandibular fracture treatment (Shepherd, 1992; Gironda et
al., 2009). QoL studies confirm that the quality of life of patients following facial
surgeries is often affected since there may be resultant facial disfigurement
(Dropkin, 1999; Katz et al., 2003). Similarly vital functions such as speaking,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
swallowing or chewing might be affected (Mignogna et al., 2001; Van Cann et. al,
2005; Guntinas-Lichius et al., 2007). A low quality of life can also lead to a low
survival rate (Osthus et al., 2011; Tarsitano et al., 2012) and due to this reason it is
important to support patients with a low quality of life.
A search of the literature found only one study on QoL of various types of
mandibular fracture (Atchison et al., 2006), which showed that the patients whose
mandibular fractures were managed by MMF reported fewer problems and had a
better immediate post-operative QoL compared to the ORIF group. To the best of
the authors’ knowledge, there is no prospective study comparing QoL of patients
treated by ORIF or MMF in the tooth-bearing region of the mandible.
Mandibular fracture may be defined as a breach in the continuity of any part of the
mandible as a result of injury (Mosby, 2005). Mandibular fractures are worldwide in
distribution and account for about 36-59% of all maxillofacial fractures (Van Hoof et
al., 1977; Brook and Wood, 1983; Ellis et al., 1985). These fractures are often the
result of road traffic accidents, assaults, falls, missiles, sports injuries and
occasionally from pre-existing pathologies (Sojot et al., 2001).
Mandibular fracture treatment aims to restore form and function, and it involves
reduction, immobilization and fixation of the fractured mandible. Reduction is the
re-apposition of the fracture segments to their normal anatomic forms;
immobilization is the restriction of movement at the temporomandibular joints while
healing occurs while fixation is the maintenance of the fracture segments in the

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
reduced position to prevent displacement during healing. Reduction techniques in
mandibular fracture treatment may be classified as open or closed based on the
presence or absence of direct visual access to the fracture site (Iizuka and
Lindqvist, 1992). Closed reduction allows manipulation of the fracture segments
taking advantage of dental occlusion without direct visual access whereas open
reduction involves direct visual access to the fracture site through a surgical
incision. Closed reduction and maxillomandibular fixation may be performed using
splints in the form of bonded orthodontic brackets, arch bars, direct wires or eyelet
wires (Iizuka and Lindqvist, 1992). Open reduction and internal fixation involves the
use of wires, plates and other hard-wares placed directly across the fractured site
via a surgical access.
Treatment of mandibular fractures by ORIF is often assumed to be superior to
treatment by MMF in a simple fracture that can be indicated for either modality.
Patients managed by ORIF have the advantage of immediate or early
postoperative joint mobilization, ability to clean all aspects of their mouth
postoperatively and an absence of limitation in choice of food to eat. They are also
noted to return earlier to work and normal life. This assumption of superiority is
often from surgeon’s perspective not taking into account the patients view point
which is equally a critical element in determining success of surgical treatment.
The aim of the study was to assess patients’ perspective, identifying patients’
expectations and determining aspects of mandibular fracture treatment that affect
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
patient’s QoL. It will enhance evidence-based practice in management of
mandibular fractures.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
MATERIAL AND METHODS
This study was a randomized prospective cross sectional comparative analysis of
health related quality of life following treatment for mandibular fractures that
occurred within the tooth bearing portions of the mandible. A comparison of ORIF
versus MMF at Aminu Kano Teaching Hospital (AKTH) Kano from January to
December 2012 was undertaken. Ethical approval for the study was obtained from
the Research and Ethics Committee of Aminu Kano Teaching Hospital Kano
(AKTH/MAC/SUB/12A/P-3/VI/957). Also written informed consent was obtained
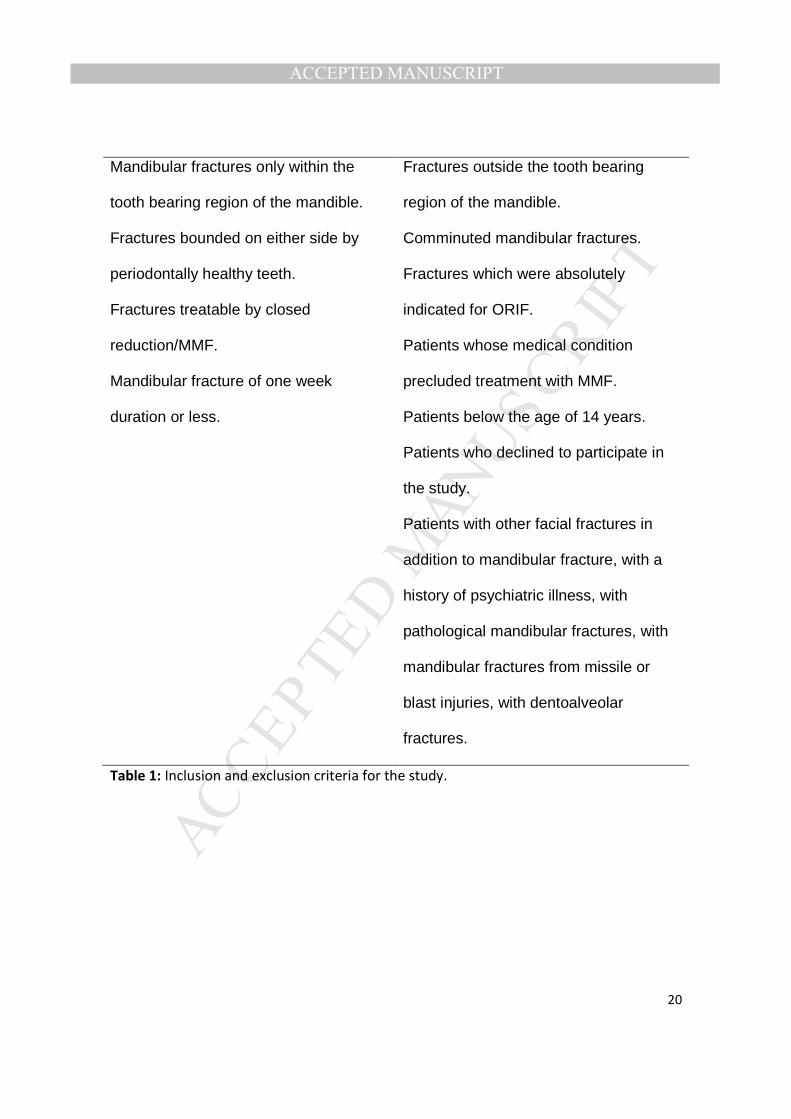
from each patient before their enrollment into the study. Inclusion and exclusion
criteria for the study are shown in Table 1.
Study protocol
Patients who met the inclusion criteria were recruited into the study from the
accident and emergency unit and the maxillofacial surgery unit of the hospital. All
patients had prophylactic scaling and polishing by dental therapists retrained for
the purpose of the study to ensure standardization prior to treatment. Mandibular
fracture treatment was paid for by the patients and commenced after routine
preoperative investigations were carried out to ensure fitness for surgery.
The patients were randomly allotted into 2 groups (Group A and B) representing
those to be treated by MMF or ORIF techniques respectively. A research assistant
balloted for the first patient into one of the two groups and allotted subsequent
consecutive patients to the opposite group in alternation until exhaustion of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
patients who met the inclusion criteria for the comparative study. Patients who
were randomized into open reduction were only required to pay the cost for closed
reduction. Healthy patients’ relatives or friends matched for age and sex were
recruited as controls for the study at the last inquiry period 8 weeks
postoperatively.
Maxillary and mandibular Erich type arch bars were employed in patients treated
by MMF and was maintained for 6 weeks while Indian type 2mm stainless steel
mini plates using screws of length 10mm at the lower border and 8mm at the sub-
apical region for the patients treated by ORIF. The patients treated by ORIF had
intraoperative trial occlusion using tie-wires anchored on maxillary and mandibular
eyelet wires. These were removed following insertion of osteosynthetic plates.
General Oral Health Assessment Index questionnaire (GOHAI; original English
version) adopted from Atchison et al. (Atchison et. al, 2006) was completed
preoperatively to obtain a pre-treatment score and post-surgery scores on day 1, 6
weeks and 8 weeks respectively. The respondents independently filled the
questionnaires in the maxillofacial clinic during their admission and postoperative
reviews. Also 28 healthy people were assessed once at the inquiry period 8 weeks
postoperatively for comparison using the same GOHAI questionnaire.
GOHAI questionnaire assesses the oral health function of the patient in three
domains namely physical, psychosocial and pain domains. Physical domain
assesses functions related to eating, speech and swallowing, psychosocial domain
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
assesses functions related to worry and concern about oral health, dissatisfaction
with appearance, self-consciousness about oral health and avoidance of social
contacts because of oral problems while pain domain evaluates discomfort and the
use of medications to relive pain from the mouth.
The 12-item GOHAI index score ranges from 12 to 60, reflecting 1 for the least
score (never) and 5 for the maximum score (always) for each individual item
(Atchison and Dolan, 1990). GOHAI is analyzed by summing up all the individual
scores of the 12-items. A higher GOHAI score represents a more positive oral
health status. GOHAI questionnaire also has been shown to demonstrate a high
validity and reliability (Brook et al., 1979)
Statistical analysis
The statistical analysis was conducted using SPSS for Windows version 20.0
(SPSS Inc., Chicago, IL, USA). The socio-demographic data and results of the
questionnaires were analyzed by means of descriptive statistics. The comparison
of the interval-scaled data of the different groups was performed by t-tests and
univariate variance analysis. For categorical variables the χ²-test was used for
comparison. To analyze the groups over the four review periods, the ANOVA for
repeated measures was conducted. For all tests, p values less than 0.05 were
considered statistically significant.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
RESULTS
During the period of study, 152 patients (M/F=135/17) with mandibular fractures
were seen. Only 96 patients had fractures exclusively within the tooth bearing
portion of the mandible. A further 40 patients were excluded based on the outlined
exclusion criteria thus 56 patients (M/F=53/3) with fractures exclusively within the
tooth bearing portion of the mandible participated in the study with 28 patients each
in ORIF and MMF groups (Figure 1).
The average age of patients with mandibular fracture managed by MMF was 30.4
± 10.7 years; the average age of patients managed with ORIF was 30.5 ± 6.7
years, while the average age of the subjects used for control was 29.3 ± 10.3. A
comparison of the mean values of the three groups with univariate variance
analysis showed that they do not significantly vary from themselves with respect to
age (df = 2 , F = 0.125, p = 0.882) and a χ²-test showed that they do not
significantly vary with respect to sex (df = 2 , p = 0.808) (Table 2).
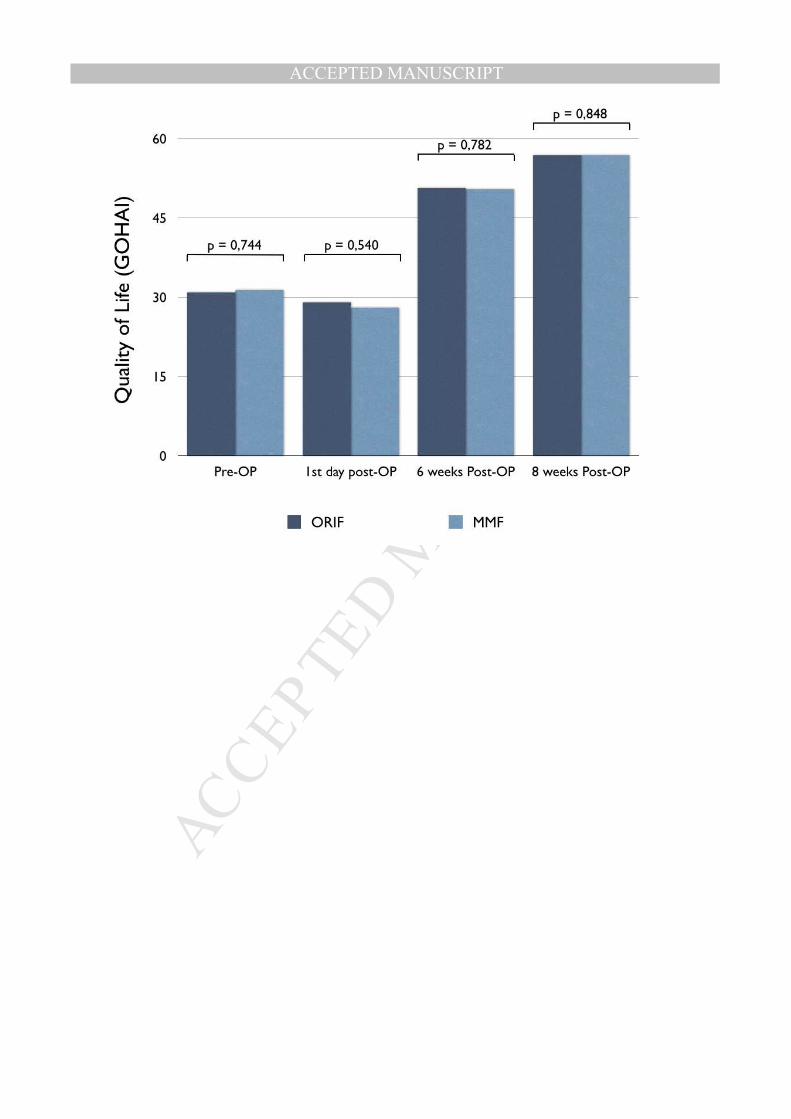
Findings from this study showed that there was no statistical significant difference
in the mean QoL score of subjects treated by MMF when compared with those
treated by ORIF throughout the review periods (GOHAI Baseline, df = 54, T =
0.329, p = 0.744; GOHAI 1st day post-op, df = 54, T = -0.616, p = 0.540; GOHAI 6
weeks post-op, df = 54, T = -0.278, p = 0.782; GOHAI 8 weeks post-op, df = 54, T
= 0.192, p = 0.848) (Figure 2).
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
When analyzing the groups over the four review periods, the ANOVA for repeated
measures showed, that the GOHAI scores of the two groups differ significantly
over the review points (df = 3, F = 828.880, p = 0.000).
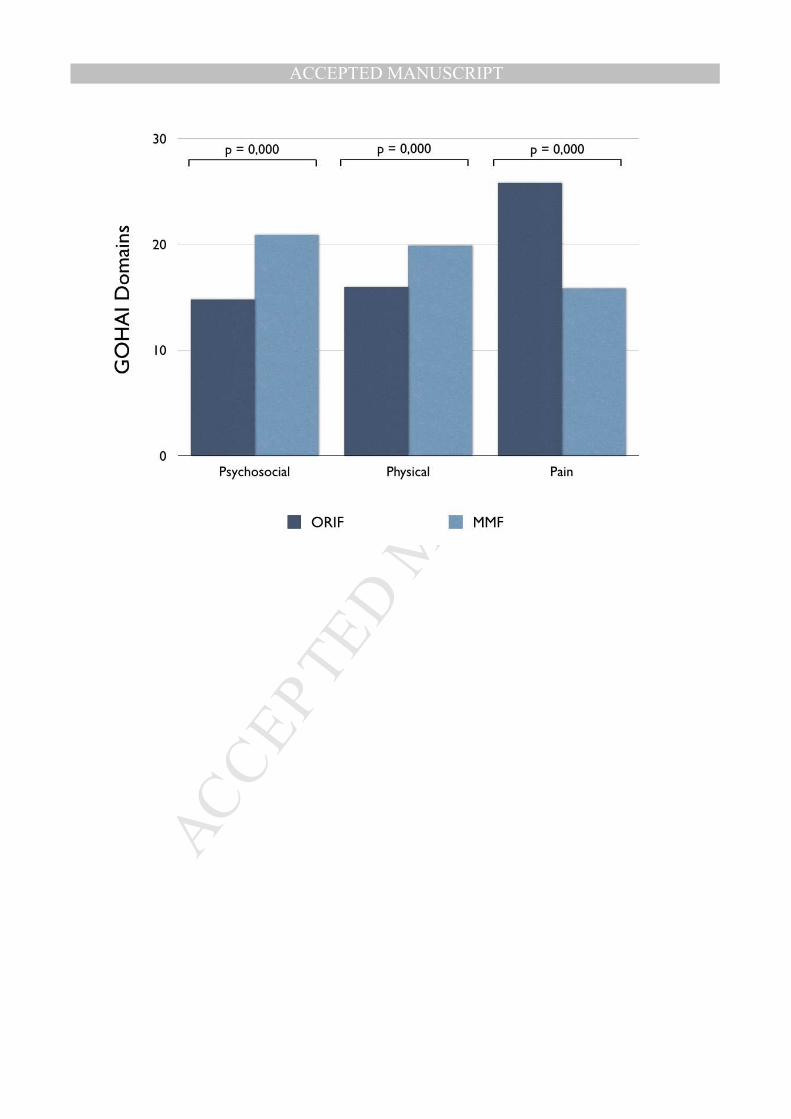
Regarding the Psychosocial, Physical and Pain domains of the GOHAI 8 weeks
postoperatively, the patients treated with ORIF reported significant higher
impairment in the pain domain (ORIF: 25.82 ± 3.24; MMF: 15.86 ± 1.1; p = 0.000)
compared to the Psychosocial (ORIF: 14.78 ± 1.56; MMF: 20.89 ± 2.53; p = 0.000)
and Physical domain (ORIF: 15.93 ± 1.42; MMF: 19.89 ± 2.44; p = 0.000) (Figure
3).
This study also revealed that there was a significant statistical difference between
subjects that were treated by either ORIF or MMF techniques when compared with
healthy people 8 weeks postoperatively (control group and ORIF, df = 54, T = -
0.708, p = 0.000; control group and MMF, df = 54, T = -5.519, p = 0.000, ORIF and
MMF, df = 54, T = 0.192, p = 0.848) (Figure 4).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
DISCUSSION
Peoples’ perception of life is known to be affected by many factors including their
culture, belief and value systems. Their perception, psychological predisposition or
personality types are intimately related (WHO, 1996). The interplay between these
factors is dynamic and unpredictable thus making their independent assessment
difficult. QoL studies are an attempt to peek into a patients’ mind and assign a
value to his mood, thoughts and thinking at that time.
Patients treated for mandibular fractures in this study were seen to experience a
gradual improvement in their quality of life scores within the postoperative review
periods after an initial decline at the first post-operative day. This decline in the
QoL score within the first postoperative day may be attributed to pain, oedema,
irritation by hard-ware and the stress of surgery.
The findings from the QoL of subjects studied showed that patients managed by
MMF were more affected by the psychosocial and physical domains whereas the
patients managed by ORIF were more affected by the pain domain. Patients
treated with MMF may have been affected psychologically by the presence of MMF
which limits both the types of food eaten as well as social interactions. This is
usually not the case for patients managed by ORIF; the extensive tissue dissection
for placement of osteosynthetic plates in ORIF when compared with the tissue
manipulation in MMF may have been responsible for pain response scores in ORIF
as seen in the present study.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
Since the patients did not differ in overall QoL despite the differences in the scales,
it can not be clearly stated which treatment is superior. The lack of difference
between the two treatment modalities regarding overall QoL may also be related to
the absence of interfragmentary mobility in both groups. Fixation with plates (ORIF)
limits interfragmentary mobility even during function while placement of MMF limits
the masticatory function of the mandible and ultimately also reduces
interfragmentary mobility. Interfragmentary mobility can be a cause of non-union,
mal-union and possibly infection.
Compared to healthy people, there was a significant difference between them and
the patient´s managed by ORIF or MMF techniques at 8 weeks postoperatively.
Posttraumatic stress that is often accompanied by emotional and psychological
depression in the subjects treated for mandibular fractures (Dorval et. al, 1998)
may have contributed to the difference in the QoL outcome between the subjects
that had surgical treatment and the healthy people. It is expected that subjects that
had traumatic injury should have a greater degree of post-traumatic stress. This
assumption should be taken with caution since no analysis of the severity of the
trauma was done in this study. Glynn et al. (2003) argued in a prospective study in
a large urban hospital that the degree of impact is a factor that must be considered
in the development of acute posttraumatic stress disorder after orofacial injury.
It should also be borne in mind that this study was performed on Nigerians who
have been noted to have a positive disposition towards life despite adversity. The
psyche of the Nigerian is also a factor which must be considered as expressed
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
above. The study was also limited by the largely male sex distribution thereby not
giving an indication of female perspective to treatment outcome. However, the
largely male preponderance is typical for Maxillofacial trauma. Reasons theorized
for these include male involvement in fights and disputes and greater male
community involvement in this part of the world (Allan and Daly, 2006; Mwaniki and
Guthua, 1990). Studies in Nigeria frequently report more males involved in
mandibular fractures (Adekeye, 1980; Olasoji et al., 2006). Thus the results
presented in this study though representing typical sex distribution of mandibular
fractures in Nigerian environment, does not represent QoL responses from both
sexes. Further study on females response to these issues may be warranted.
Also the age group represented in the study corroborates regional and world data
on ages of subjects affected by facial trauma (Ansari, 2004; Erol et al., 2004).
The level of education of patients surveyed does not represent the population in
Nigeria. Therefore, the results are not representative, which is why illiterated
patients should be asked via interviews in further studies.
Different surgeons managed the cases presented here. No attempt was made to
assess the effect of individual surgeons or their years of experience on patients
postoperative QoL. However, the QoL scores recorded during the study period
(significant postoperative improvement ) suggests that such differences could be
overlooked.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
CONCLUSION
The study found a significant statistical difference in treatment of mandibular
fractures of the tooth-bearing regions using ORIF and MMF based on patients’
perception assessed using GOHAI questionnaire. It was found that the patients
treated with ORIF reported higher values in the pain domain, while the patients
treated with MMF reported higher values in the psychosocial and physical
domains. Although the patients reported different values regarding the domains,
there was no significant difference in the the overall QoL. The choice between
ORIF and MMF in subjects with similar fractures may be aided by considering
other parameters such as patients’ choice, availability of surgical hardware and
competence of the surgeon.
Financial interests: None
Sources of support: None
Conflict of Interest Statement:
The authors declare that they have no conflict of interest.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
REFERENCES
Adekeye EO. The pattern of fractures of the facial skeleton in Kaduna, Nigeria. A
survey of 1,447 cases. Oral Surg Oral Med Oral Pathol 49:491-495, 1980.
Allan BP, Daly CG. Fractures of the mandible. A 35-year retrospective study. Int J
Oral Maxillofac Surg 19:268-271, 1990.
Ansari MH. Maxillofacial fractures in Hamedan province, Iran: a retrospective study
(1987-2001). J Craniomaxillofac Surg 32:28-34, 2004.
Atchison KA, Dolan TA. Development of the Geriatric Oral Health Assessment
Index. J Dent Educ 54:680-687, 1990.
Atchison KA, Shetty V, Belin TR, Der-Martirosian C, Leathers R, Black E, et al.
Using patient self-report data to evaluate orofacial surgical outcomes.
Community Dent Oral Epidemiol 34:93-102, 2006.
Brook IM, Wood N. Aetiology and incidence of facial fractures in adults. Int J Oral
Surg 12:293-298, 1983.
Brook RH, Ware JE, Jr., Davies-Avery A, Stewart AL, Donald CA, Rogers WH, et
al. Overview of adult health measures fielded in Rand's health insurance
study. Med Care 17:iii-x, 1-131, 1979.
Dorval M, Maunsell E, Deschenes L, Brisson J. Type of mastectomy and quality of
life for long term breast carcinoma survivors. Cancer 83:2130-2138, 1998.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
Dropkin MJ. Body image and quality of life after head and neck cancer surgery.
Cancer Pract 7:309-313, 1999.
Ellis E, 3rd, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of
2,137 cases. Oral Surg Oral Med Oral Pathol 59:120-129, 1985.
Erol B, Tanrikulu R, Gorgun B. Maxillofacial fractures. Analysis of demographic
distribution and treatment in 2901 patients (25-year experience). J
Craniomaxillofac Surg 32:308-313, 2004.
Gironda MW, Der-Martirosian C, Belin TR, Black EE, Atchison KA. Predictors of
depressive symptoms following mandibular fracture repair. J Oral Maxillofac
Surg 67:328-334, 2009.
Glynn SM, Asarnow JR, Asarnow R, Shetty V, Elliot-Brown K, Black E, et al. The
development of acute post-traumatic stress disorder after orofacial injury: a
prospective study in a large urban hospital. J Oral Maxillofac Surg 61:785-
792, 2003.
Guntinas-Lichius O, Straesser A, Streppel M. Quality of life after facial nerve repair.
Laryngoscope 117:421-426, 2007.
Iizuka T, Lindqvist C. Rigid internal fixation of mandibular fractures. An analysis of
270 fractures treated using the AO/ASIF method. Int J Oral Maxillofac Surg
21:65-69, 1992.
Infante-Cossio P, Torres-Carranza E, Cayuela A, Gutierrez-Perez JL, Gili-Miner M.
Quality of life in patients with oral and oropharyngeal cancer. Int J Oral
Maxillofac Surg 38:250-255, 2009.
Katz MR, Irish JC, Devins GM, Rodin GM, Gullane PJ. Psychosocial adjustment in
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
head and neck cancer: the impact of disfigurement, gender and social
support. Head Neck 25:103-112, 2003.
Kommers SC, van den Bergh B, Forouzanfar T. Quality of life after open versus
closed treatment for mandibular condyle fractures: a review of literature. J
Craniomaxillofac Surg 41:e221-225, 2013.
Mignogna MD, Fedele S, Lo Russo L, Ruoppo E, Lo Muzio L. Oral and pharyngeal
cancer: lack of prevention and early detection by health care providers. Eur
J Cancer Prev 10:381-383, 2001.
Mosby’s Medical Dictionary, 7th edition. St. Louis MO: Elsevier Mosby, 2005.
Mwaniki DL, Guthua SW. Occurrence and characteristics of mandibular fractures in
Nairobi, Kenya. Br J Oral Maxillofac Surg 28:200-202, 1990.
O'Boyle CA. Assessment of quality of life in surgery. Br J Surg 79:395-398, 1992.
Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern
Nigeria. Br J Oral Maxillofac Surg 40:140-143, 2002.
Olschewski M, Schulgen G, Schumacher M, Altman DG. Quality of life assessment
in clinical cancer research. Br J Cancer 70:1-5, 1994.
Osthus AA, Aarstad AK, Olofsson J, Aarstad HJ. Head and neck specific Health
Related Quality of Life scores predict subsequent survival in successfully
treated head and neck cancer patients: a prospective cohort study. Oral
Oncol 47:974-979, 2011.
Shepherd JP. Strategies for the study of long-term sequelae of oral and facial
injuries. J Oral Maxillofac Surg 50:390-399, 1992.
Sojot AJ, Meisami T, Sandor GK, Clokie CM. The epidemiology of mandibular

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
fractures treated at the Toronto general hospital: A review of 246 cases. J
Can Dent Assoc 67:640-644, 2001.
Tarsitano A, Pizzigallo A, Ballone E, Marchetti C. Health-related quality of life as a
survival predictor for patients with oral cancer: is quality of life associated
with long-term overall survival? Oral Surg Oral Med Oral Pathol Oral Radiol
114:756-763, 2012.
Van Cann EM, Dom M, Koole R, Merkx MA, Stoelinga PJ. Health related quality of
life after mandibular resection for oral and oropharyngeal squamous cell
carcinoma. Oral Oncol 41:687-693, 2005.
van Hoof RF, Merkx CA, Stekelenburg EC. The different patterns of fractures of the
facial skeleton in four European countries. Int J Oral Surg 6:3-11, 1977.
WHO. What quality of life? The WHOQOL Group. World Health Organization
Quality of Life Assessment. World Health Forum 17:354 356, 1996.
Worsaae N, Thorn JJ. Surgical versus nonsurgical treatment of unilateral
dislocated low subcondylar fractures: a clinical study of 52 cases. J Oral
Maxillofac Surg 52:353-360; discussion 360-351, 1994.
INCLUSION CRITERIA EXCLUSION CRITERIA
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
Mandibular fractures only within the
tooth bearing region of the mandible.
Fractures bounded on either side by
periodontally healthy teeth.
Fractures treatable by closed
reduction/MMF.
Mandibular fracture of one week
duration or less.
Fractures outside the tooth bearing
region of the mandible.
Comminuted mandibular fractures.
Fractures which were absolutely
indicated for ORIF.
Patients whose medical condition
precluded treatment with MMF.
Patients below the age of 14 years.
Patients who declined to participate in
the study.
Patients with other facial fractures in
addition to mandibular fracture, with a
history of psychiatric illness, with
pathological mandibular fractures, with
mandibular fractures from missile or
blast injuries, with dentoalveolar
fractures.
Table 1: Inclusion and exclusion criteria for the study.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
Closed reduction
(n = 28)
ORIF
(n = 28)
Control group
(n = 28) p
Age (years) ± SD 30.4 ± 10.7 30.5 ± 6.7 29.3 ± 10.3 0.882
Sex m/f 27/1 26/2 26/2 0.808
Table 2. Comparison of the groups with respect to age and sex (N = 84)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
Pre-OP
1st day
post-OP
6 weeks
post-OP
8 weeks
post-OP
p
ORIF
M ± SD 30.86 ± 5.20 29.00 ± 6.99 50.64 ± 4.47 56.79 ± 2.56 0.000
Closed reduction
M ± SD 31.29 ± 4.52 28.00 ± 4.99 50.36 ± 3.11 56.89 ± 1.47 0.000
Table 3. Comparison of the treatment groups with respect to the four times of
review (N = 56)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
Figure 1. Flow diagram of the progress through the phases of a parallel
randomised trial of two groups
Figure 2. Comparison of QoL of the ORIF group with the MMF group throughout
the review periods. Both groups do not differ significantly regarding their QoL over
the four review periods
Figure 3. Comparison of the ORIF and MMF groups regarding the Psychosocial,
Physical and Pain domains of the GOHAI. The differences between the groups
were significant across all scales.
Figure 4. Comparison of the QoL of the ORIF and MMF groups with healthy
people. The healthy people have a higher QoL as the ORIF and MMF group after 8
weeks postoperatively, while the ORIF and the MMF group do not differ
significantly.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT





























