Embed Size (px)
Citation preview

QUALITY OF LIFE BEFORE RECONSTRUCTIVE BREAST SURGERY:A PREOPERATIVE COMPARISON OF PATIENTS WITH IMMEDIATE,DELAYED, AND MAJOR REVISION RECONSTRUCTION
GEDGE D. ROSSON, M.D.,1* SACHIN M. SHRIDHARANI, M.D.,1 MICHAEL MAGARAKIS, M.D.,1 MICHELE A. MANAHAN, M.D.,1
BASAK BASDAG, M.H.S.,1,2 MARTA M. GILSON, Ph.D.,2 and ANDREA L. PUSIC, M.D.3
Background: Women undergo breast reconstruction at different time-points in their cancer care; knowing patients’ preoperative quality oflife (QoL) is critical in the overall care of the patient with breast cancer. Our objective was to describe presurgical QoL among womenundergoing immediate, delayed, or major revision breast reconstructive surgery at our institution. Methods: From March 2008 to February2009, we administered preoperative BREAST-Q questionnaires to women who presented to our institution for breast reconstruction. Univar-iate and multivariate analyses were performed to compare patient cohorts across multiple QoL domains including body image, physicalwell-being, psychosocial well-being, and sexual well-being. Results: Of the 231 patients who presented for preoperative consultation, 176returned the questionnaire (response rate 76%; 117 from the immediate, 21 from the delayed, and 32 from the major revision reconstruc-tion groups, plus 6 mixed or unknown). The three groups differed significantly (P < 0.05) across four of the six domains: body image (sat-isfaction with breasts), psychosocial well-being, sexual well-being, and physical well-being of the chest and upper body. The immediatereconstruction group had higher (better) scores than the delayed reconstruction group, which had higher (better) scores than the major re-vision group. Conclusion: These data suggest that women presenting for breast reconstruction at different stages of reconstruction havedifferent baseline QoL. Such data may help us better understand patient selection, education, and expectations, and may lead to improvedpatient–surgeon communication. VVC 2013 Wiley Periodicals, Inc. Microsurgery 33:253–258, 2013.
Breast cancer is the second leading cause of cancer
deaths among women in the United States. The American
Cancer Society estimated that in 2011, there would be an
estimated 230,480 new cases of invasive breast cancer as
well as 39,520 deaths.1 In addition to breast conserving
treatments, mastectomy can be another important and de-
finitive treatment option for certain patients. However,
mastectomy is often associated with substantial psycho-
logical, social, and sexual sequelae, as well as significant
body image distortion.2–5 Modern breast reconstruction
surgery offers a wide range of options with the potential
to significantly improve quality of life (QoL) for breast
cancer survivors.3,6–9
Although studies in the surgical literature have exten-
sively evaluated many options for breast reconstruction, a
limited number of studies have addressed the timing of
reconstruction with respect to QoL. The timing of breast
reconstruction after mastectomy is determined through a
combination of patient-related factors, including patient
preference and the likelihood that the patient will require
post-mastectomy radiation therapy.10,11 Typically, breast
reconstruction can occur at the time of mastectomy
(termed ‘‘immediate’’ breast reconstruction) or at a laterdate to accommodate radiation, chemotherapy, or patientpreference (‘‘delayed’’ reconstruction). In certain cases,revision reconstruction can be performed on an alreadyreconstructed breast to try to correct problems with theprevious surgery, such as implant capsular contracture,abnormal scarring, and dissatisfaction with the recon-structed breast’s appearance. These cases are designatedas breast reconstruction ‘‘major revision’’ operations.
In general, breast reconstruction may reduce the dis-
tress of mastectomy,3,12–15 and several studies have
shown that patients with delayed reconstruction are more
likely to be distraught and less satisfied than patients
with immediate reconstruction.3,14,16 The higher level of
distress in patients in the delayed reconstruction group is
a likely consequence of these women dealing with the
complete absence of their breast(s) and feeling self-con-
scious about having a ‘‘deformity.’’ Patient perceptions ofthe impact of disease and surgical intervention on physi-cal, psychosocial, and sexual well-being have become anintegral part of the surgical algorithm. Clinical researchendeavors have increasingly focused on determining thelevel of satisfaction and the QoL of different patientgroups.
1Department of Plastic Surgery, The Johns Hopkins University School ofMedicine, Baltimore, MD2The Center for Surgical Trials & Outcomes Research, the Department ofSurgery, The Johns Hopkins University School of Medicine, Baltimore, MD3The Plastic and Reconstructive Surgical Service, the Department of Sur-gery, Memorial Sloan Kettering Cancer Center, New York, NY
The BREAST-Q is jointly owned by Memorial Sloan-Kettering Cancer Centerand the University of British Columbia. Dr. Pusic is a co-developer of theBREAST-Q and, as such, receives a share of any license revenues based onthe inventor sharing policies of these two institutions.
Presented at the 26th Annual Meeting of the American Society of Recon-structive Microsurgery, Boca Raton, Florida, January 10, 2010. Poster pre-sentation at the 96th Annual Clinical Congress of the American College ofSurgeons, Washington, DC, October 6, 2010.
Grant sponsor: Safeway Foundation; Grant sponsor: Sidney Kimmel Compre-hensive Cancer Center; Johns Hopkins Medical Institutions; Baltimore, Maryland
*Correspondence to: Gedge D. Rosson, MD, Director of Breast Reconstruc-tion, Department of Plastic Surgery, The Johns Hopkins Hospital OutpatientCenter, 601 N. Caroline St., McElderry 8161, Baltimore, Maryland 21287.E-mail: [email protected].
Received 3 June 2012; Revision accepted 16 November 2012; Accepted26 November 2012
Published online 17 February 2013 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/micr.22081
VVC 2013 Wiley Periodicals, Inc.
The BREAST-Q is a new patient-reported outcome
measure that evaluates patients’ experiences with recon-
structive breast surgery.8,17 The BREAST-Q was carefully
developed and validated in accordance with internationally
recognized guidelines.17 Specifically, the BREAST-Q asks
patients to report their views and feelings across multiple
domains including satisfaction with breasts and abdomen,
psychosocial well-being, physical well-being (chest and ab-
domen), and sexual well-being. Although numerous studies
have investigated patient satisfaction and QoL after breast
reconstruction, to the authors’ knowledge, only one has
examined QoL parameters before reconstructive surgery
and compared them among patients in various presentation
cohorts.18 The goal of this study was to use the six domains
of the BREAST-Q to assess the presurgical QoL and patient
satisfaction of women seeking immediate, delayed, or
major revision breast reconstruction.
METHODS
During a 1-year period from March 2008 to February
2009, the preoperative BREAST-Q, a self-administered,
validated, breast reconstruction-specific questionnaire,
was routinely given to all patients during the initial con-
sultation for breast reconstruction surgery at our institu-
tion. The conceptual framework and scale structure of the
BREAST-Q address both QoL (psychosocial well-being;
sexual well-being; physical well-being: chest and upper
body; and physical well-being: abdomen) and patient sat-
isfaction (body image: satisfaction with breasts; and body
image: satisfaction with abdomen).15 The BREAST-Q
was developed with strict adherence to internationally
accepted guidelines and all scales fulfill traditional psy-
chometric criteria (including: Person Separation Indices:
0.76–0.96; Cronbach’s alphas: 0.81–0.97; and test–retest
reproducibility: 0.73–0.96).17
We investigated three groups of patients. The first
group included patients diagnosed with breast cancer and
interested in immediate reconstruction at the time of their
mastectomy (immediate group). The second group
included patients that had already undergone a mastec-
tomy for breast cancer and were now interested in breast
reconstruction (delayed group). The third group included
patients that had already undergone a breast reconstruction
at various time-points in the past but were not satisfied with
the results. These patients were interested in revision recon-
struction to improve their breast contour and/or symmetry
(major revision group). All women who presented to our
breast center for potential mastectomy and reconstruction,
prior mastectomy desiring delayed reconstruction, or prior
mastectomy with prior reconstruction were included, as the
BREAST-Q was given to all new patients as part of routine
clinical work-flow. Patients were only excluded if they pre-
sented with desire for lumpectomy with oncoplasty recon-
struction or prior lumpectomy and desire for revision sur-
gery (i.e., non-mastectomy).
Data analyses focused on detecting differences
between the three patient groups with respect to the
BREAST-Q in four QoL domains: psychosocial well-being;
sexual well-being; body image: satisfaction with breasts;
and physical well-being: chest and upper body. Raw scores
were recorded for each question. BREAST-Q question val-
ues were transformed and scored using QScore, a statistical
program developed specifically for the BREAST-Q by
RUMM laboratories (Perth, Australia). The BREAST-Q
transformed and scored values were used for analysis.
Patients who did not answer at least half of the ques-
tions for a specific subscale were removed from analysis
of that subscale. Univariate nonparametric statistical anal-
yses (Kruskal–Wallis test) were performed to compare
the immediate, delayed, and major revision patient
groups’ age, body mass index (BMI), and QoL scores.
Statistical significance was set a priori at P < 0.05. Mul-
tiple regression analyses were used to determine if the
three groups’; (immediate, delayed, and major revision)
QoL scores differed while adjusting for age and BMI.
The Johns Hopkins Medicine Institutional Review
Board approved this study.
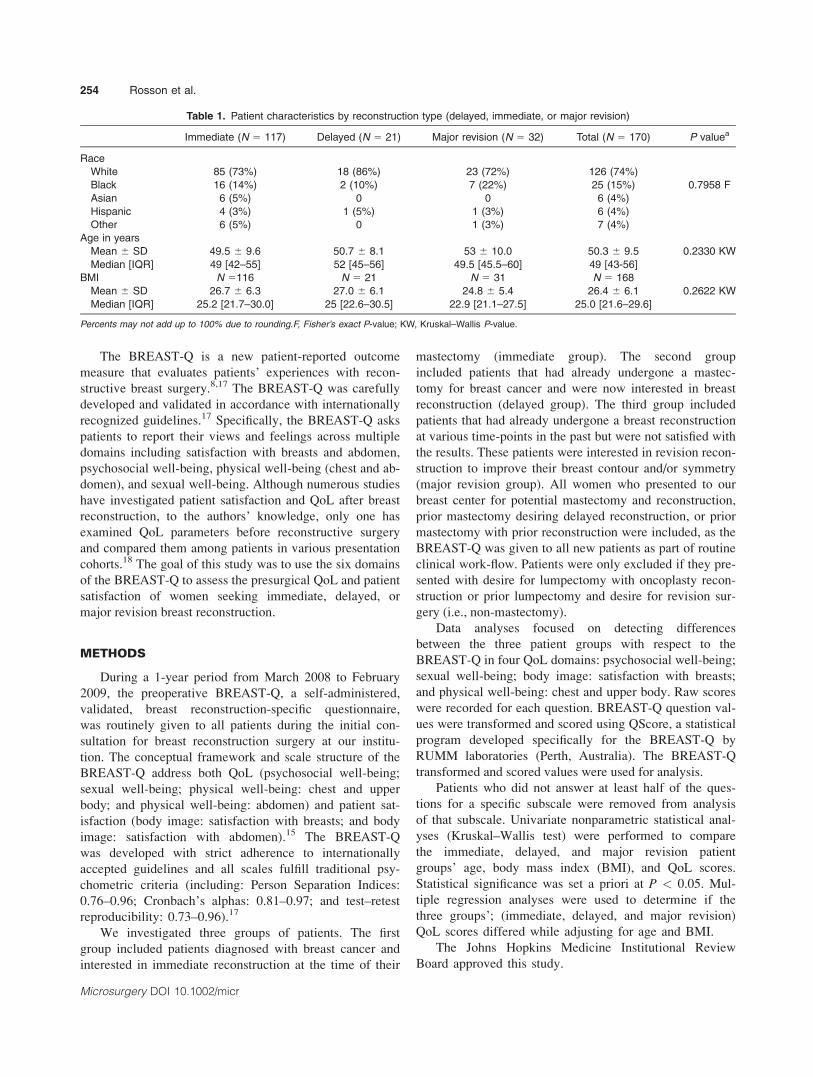
Table 1. Patient characteristics by reconstruction type (delayed, immediate, or major revision)
Immediate (N 5 117) Delayed (N 5 21) Major revision (N 5 32) Total (N 5 170) P valuea
Race
White 85 (73%) 18 (86%) 23 (72%) 126 (74%)
Black 16 (14%) 2 (10%) 7 (22%) 25 (15%) 0.7958 F
Asian 6 (5%) 0 0 6 (4%)
Hispanic 4 (3%) 1 (5%) 1 (3%) 6 (4%)
Other 6 (5%) 0 1 (3%) 7 (4%)
Age in years
Mean 6 SD 49.5 6 9.6 50.7 6 8.1 53 6 10.0 50.3 6 9.5 0.2330 KW
Median [IQR] 49 [42–55] 52 [45–56] 49.5 [45.5–60] 49 [43-56]
BMI N 5116 N 5 21 N 5 31 N 5 168
Mean 6 SD 26.7 6 6.3 27.0 6 6.1 24.8 6 5.4 26.4 6 6.1 0.2622 KW
Median [IQR] 25.2 [21.7–30.0] 25 [22.6–30.5] 22.9 [21.1–27.5] 25.0 [21.6–29.6]
Percents may not add up to 100% due to rounding.F, Fisher’s exact P-value; KW, Kruskal–Wallis P-value.
254 Rosson et al.
Microsurgery DOI 10.1002/micr
RESULTS
Of the 231 patients who presented for consultation
during this time period, 176 returned the questionnaire
(response rate 76%). Five questionnaires were excluded
because the patients did not fit exclusively into any one
of our three groups. In addition, one questionnaire was
excluded because the patient answered less than half the
questions for every ‘‘subscale’’ in the BREAST-Q. There
were a total of 170 completed questionnaires: 117 were in
the immediate group, 21 in the delayed group, and 32 in
the major revision group. Table 1 presents the patient
characteristics. Mean patient age was 50 years (range: 29–
84 years). All patients had pathology-proven stage 0–III
breast carcinoma. There were no patients with stage IV
breast carcinoma. BMI was available for 168 patients: 2
(1%) were underweight (BMI < 18.5), 82 (49%) normal
weight (BMI: 18.5–24.9), 44 (26%) overweight (BMI:
25–29.9), and 40 (24%) obese (BMI � 30). Of the 40
obese patients, 21 were class I (BMI: 30–34.9), 11 were
class II (BMI: 35–39.9), and 8 were class III (BMI � 40).
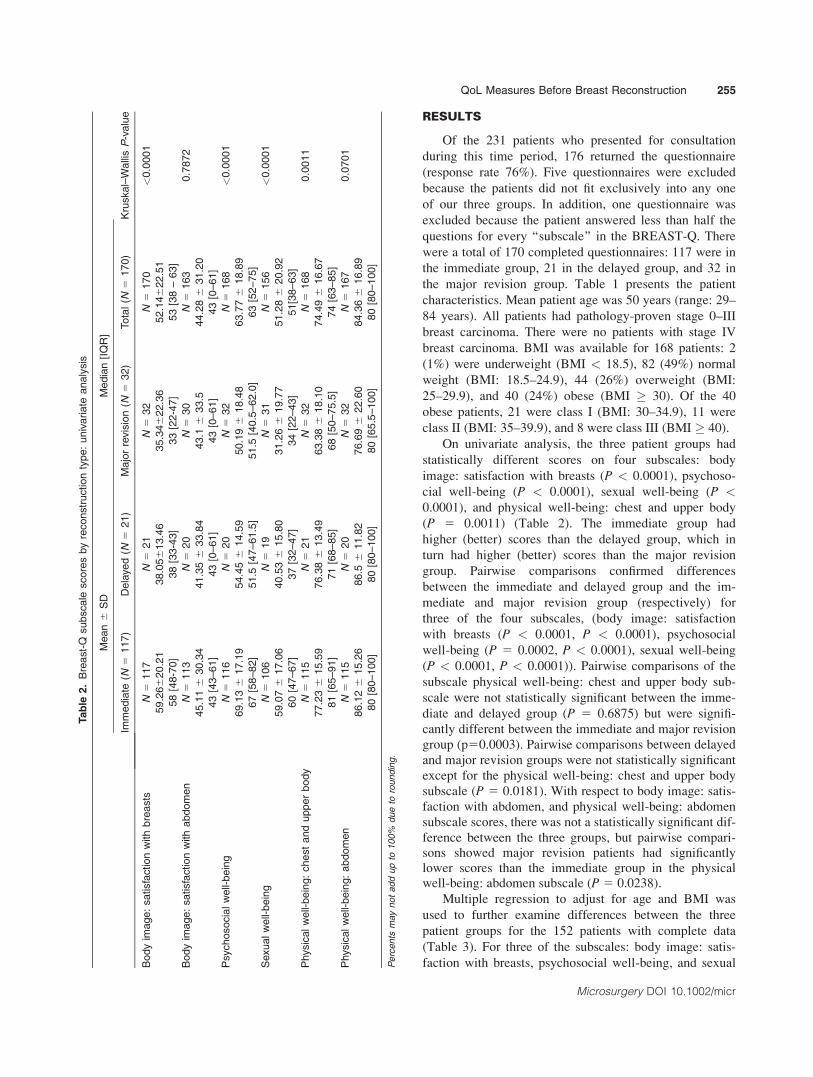
On univariate analysis, the three patient groups had
statistically different scores on four subscales: body
image: satisfaction with breasts (P < 0.0001), psychoso-
cial well-being (P < 0.0001), sexual well-being (P <0.0001), and physical well-being: chest and upper body
(P 5 0.0011) (Table 2). The immediate group had
higher (better) scores than the delayed group, which in
turn had higher (better) scores than the major revision
group. Pairwise comparisons confirmed differences
between the immediate and delayed group and the im-
mediate and major revision group (respectively) for
three of the four subscales, (body image: satisfaction
with breasts (P < 0.0001, P < 0.0001), psychosocial
well-being (P 5 0.0002, P < 0.0001), sexual well-being
(P < 0.0001, P < 0.0001)). Pairwise comparisons of the
subscale physical well-being: chest and upper body sub-
scale were not statistically significant between the imme-
diate and delayed group (P 5 0.6875) but were signifi-
cantly different between the immediate and major revision
group (p50.0003). Pairwise comparisons between delayedand major revision groups were not statistically significant
except for the physical well-being: chest and upper body
subscale (P 5 0.0181). With respect to body image: satis-faction with abdomen, and physical well-being: abdomen
subscale scores, there was not a statistically significant dif-
ference between the three groups, but pairwise compari-sons showed major revision patients had significantlylower scores than the immediate group in the physicalwell-being: abdomen subscale (P 5 0.0238).
Multiple regression to adjust for age and BMI was
used to further examine differences between the three
patient groups for the 152 patients with complete data
(Table 3). For three of the subscales: body image: satis-
faction with breasts, psychosocial well-being, and sexual
Table
2.
Bre
ast-
Qsubsca
lescore
sby
reconst
ruction
type:
univ
ariate
analy
sis
Mean6
SD
Media
n[I
QR
]
Kru
skal–
Walli
sP
-valu
eIm
media
te(N
5117)
Dela
yed
(N5
21)
Majo
rre
vis
ion
(N5
32)
Tota
l(N
5170)
Body
image:
satisfa
ction
with
bre
asts
N5
117
N5
21
N5
32
N5
170
<0.0
001
59.2
66
20.2
138.0
56
13.4
635.3
46
22.3
652.1
46
22.5
1
58
[48-7
0]
38
[33-4
3]
33
[22-4
7]
53
[38
–63]
Body
image:
satisfa
ction
with
abdom
en
N5
113
N5
20
N5
30
N5
163
0.7
872
45.1
16
30.3
441.3
56
33.8
443.1
633.5
44.2
86
31.2
0
43
[43–61]
43
[0–61]
43
[0–61]
43
[0–61]
Psy
chosoci
alw
ell-
bein
gN
5116
N5
20
N5
32
N5
168
<0.0
001
69.1
36
17.1
954.4
56
14.5
950.1
96
18.4
863.7
76
18.8
9
67
[58–82]
51.5
[47–61.5
]51.5
[40.5
–62.0
]63
[52–75]
Sexualw
ell-
bein
gN
5106
N5
19
N5
31
N5
156
<0.0
001
59.0
76
17.0
640.5
36
15.8
031.2
66
19.7
751.2
86
20.9
2
60
[47–67]
37
[32–47]
34
[22–43]
51[3
8–63]
Physic
alw
ell-
bein
g:
chest
and
upper
body
N5
115
N5
21
N5
32
N5
168
0.0
011
77.2
36
15.5
976.3
86
13.4
963.3
86
18.1
074.4
96
16.6
7
81
[65–91]
71
[68–85]
68
[50–75.5
]74
[63–85]
Physic
alw
ell-
bein
g:
abdom
en
N5
115
N5
20
N5
32
N5
167
0.0
701
86.1
26
15.2
686.5
611.8
276.6
96
22.6
084.3
66
16.8
9
80
[80–100]
80
[80–100]
80
[65.5
–100]
80
[80–100]
Percents
maynotaddupto
100%
dueto
rounding.
QoL Measures Before Breast Reconstruction 255
Microsurgery DOI 10.1002/micr

well-being, both the delayed group (P < 0.0001, P 5
0.0004, and P < 0.0001, respectively) and the major revi-
sion group (P < 0.0001, P < 0.0001, and P < 0.0001,
respectively) were statistically significantly different from
the immediate group (reference group) while adjusting for
age and BMI. While adjusting for age and BMI, the physi-
cal well-being: chest and upper body subscale as well as the
physical well-being: abdomen subscale showed a signifi-
cant difference between the immediate and major revision
groups (P < 0.0001 and P 5 0.0112, respectively), but the
delayed group was not significantly different from the im-
mediate group (P 5 0.9863 and P 5 0.6755, respectively).
There were no statistically significant differences between
any of the groups with respect to body image: satisfaction
with abdomen subscale scores (P 5 0.6874 (delayed), P 5
0.4559 (major revision)).
DISCUSSION
Breast cancer is the second most common cancer in
women in the United States, and many women diagnosed
with this cancer may require (or choose) therapeutic mas-
tectomy.1 Currently in the United States, mastectomy
rates are increasing among patients with early-stage can-
cer. Contralateral prophylactic mastectomy rates are also
increasing. Although several factors have contributed to
these trends, perhaps the most important is the increased
use of skin-sparing mastectomy along with immediate or
delayed breast reconstruction surgery.19 Accordingly,
breast reconstruction is becoming an integral part of the
breast cancer care algorithm.
Women who undergo breast reconstruction may expe-
rience less psychological morbidity and may be more sat-
isfied with their surgical results compared to women who
receive mastectomy alone.14 Studies have tried to show a
correlation between the timing of reconstruction and
patient satisfaction. Multiple studies have reported imme-
diate breast reconstruction to be superior to delayed
reconstruction in overall aesthetics, psychological well-
being, and cost effectiveness.3,14,16,20–23 Only one such
study was a truly prospective randomized controlled
trial,21 and that study is thoroughly reviewed in a
Cochrane Review article.24
To the authors’ knowledge, however, only one study
has examined patients’ psychological state of mind and
QoL specifically prior to breast reconstruction using vali-
dated questionnaires,18 but unfortunately that study did
not use a breast reconstruction-specific validated ques-
tionnaire. Thus, the objective of this study was to quan-
tify potential baseline differences in QoL among women
presenting for reconstruction at different time points in
their cancer care using the BREAST-Q. Looking at the
timing of breast reconstruction with respect to QoL, we
note that women in the major revision group, when com-
pared to women in the delayed and immediate groups,
reported the lowest QoL. This clearly indicates the mag-
nitude of the effect that unsatisfactory breast reconstruc-
tion may have on patients’ psychological well-being. Spe-
cifically, ‘‘failed’’ breast reconstruction may place the
patients’ psychological ‘‘plateau’’ at a level lower than
that of patients who have had mastectomies without
reconstruction (delayed group). For surgeons who per-
form breast reconstruction, this presents an important
insight and highlights the importance of successful recon-
struction. In some cases, delayed reconstruction may be
advisable if the patient presents with potential risk factors
(e.g. smoking, obesity). In addition, patients should be
provided counsel regarding complications and their poten-
tial impact on QoL. It is hypothesized that adequate pre-
operative counseling could potentially prevent some of
the negative psychological sequelae of an unsatisfactory
outcome.
It is quite interesting that the one previous study that
investigated preoperative quality of life; Roth et al.,18
found patients presenting for immediate reconstruction
had lower QoL scores than those presenting for delayed
reconstruction, whereas our study found the opposite.
Although our study was focusing on the QoL scores
at presentation to our institution, prior to selecting any
surgical plan with us, it should be noted that these
patients were presenting to our institution for all types of
reconstructions, whether autologous or implant-based. We
primarily offer DIEP, SGAP, TUG autologous options,
and one-stage direct implant or two-stage expander-
implant alloplastic options.25,26 We did not use any
Becker-type implants during this time period (2008–
Table 3. Multiple regression coefficients (and P-values) of Breast-Q 2 subscale scores as a function of reconstruction type (delayed or
major revision; immediate is reference group): adjusting for age and BMI for 152 patients with complete data
Intercept (immediate) Delayed Major Revision Age BMI
Body image: satisfaction with breasts 107.86 (<0.0001) 220.30 (<0.0001) 225.67 (<0.0001) 20.30 (0.1029) 21.26 (<0.0001)
Body image: satisfaction with abdomen 118.87 (<0.0001) 22.93 (0.6874) 24.62 (0.4559) 20.55 (0.0528) 21.77 (<0.0001)
Psychosocial well-being 95.13 (<0.0001) 214.62 (0.0004) 221.26 (<0.0001) 20.08 (0.6032) 20.81 (0.0003)
Sexual well-being 85.70 (<0.0001) 218.26 (<0.0001) 228.34 (<0.0001) 20.10 (0.5327) 20.82 (0.0006)
Physical well-being: chest and upper body 79.87 (<0.0001) 0.07 (0.9863) 214.61 (<0.0001) 0.02 (0.9090) 20.14 (0.5251)
Physical well-being: abdomen 120.81 (<0.0001) 1.71 (0.6755) 28.93 (0.0112) 20.37 (0.0203) 20.64 (0.0045)
Each row of the table is a separate model.
256 Rosson et al.
Microsurgery DOI 10.1002/micr

2009). Typically, those patients with dissatisfaction with
or failure of prior implant-based reconstruction were often
presenting to us with a request for autologous reconstruc-
tion. Those patients with prior failed autologous reconstruc-
tion often had radiation, so they might need a second auto-
logous flap. Those patients presenting for delayed recon-
struction could choose either autologous or implant,
depending on their body habitus and radiation status. Those
patients presenting for immediate reconstruction often
chose a babysitter technique with placement of a tissue ex-
pander; however, immediate autologous reconstruction is
common for patients with early stage disease, small tumors
and no chance for post-mastectomy radiation therapy.
Limitations of our study include the manner in which
the patients were selected, incomplete response rate,
incomplete knowledge of which ‘‘major revision’’ patients
had a prior TRAM flap, and potential lack of statistical
power for certain subgroups. First, this study was not
designed prospectively; rather, the BREAST-Q is routinely
given as part of the clinical care of the patients at our insti-
tution. Furthermore, while our response rate was high, it is
clear that we were not able to capture all patients seen at
our institution. In addition, comments about abdominal sat-
isfaction with appearance and abdominal physical well-
being in the ‘‘major revision’’ patients may not be meaning-
ful without clearly linking this to whether or not a woman
has had a TRAM. The post-op breast-Q does not ask about
abdominal satisfaction if the patient undergoes TUG/
SGAP/Implant reconstructions (those questions are
skipped), so those pre-op data are then not used. For this
study, we simply included all data, as we did not know
which surgery the patients would undertake. These ques-
tionnaires were all filled out prior to the patient deciding on
their surgical plan at our institution. Finally, our study may
not have been adequately powered to detect difference, par-
ticularly given the limited number of patients in the delayed
reconstruction group (n 5 21). Since the time of this study,
we have implemented prospective collection of QoL data
throughout the breast reconstruction process to better
understand how these patient-reported outcomes may
change following surgery and over time.
In conclusion, these data suggest that women present-
ing for breast reconstruction at different stages in their
cancer care have different baseline QoL. The immediate
reconstruction group had higher (better) scores than the
delayed reconstruction group, which had higher (better)
scores than the major revision group. Understanding these
differences may improve communication between the sur-
geon and the patient.
ACKNOWLEDGMENTS
We thank Terri Carter, Department of Surgery, The
Johns Hopkins University, for her assistance with editing
this manuscript, and Raghunandan Venkat, MD, MPH,
Department of Surgery, The Johns Hopkins University,
for his assistance with some statistical analysis.
REFERENCES
1. American Cancer Society. Cancer Facts & Figures 2009. Atlanta:American Cancer Society; 2009.
2. Eric M, Mihic N, Krivokuca D. Breast reconstruction followingmastectomy; patient’s satisfaction. Acta Chir Belg 2009;109:159–166.
3. Al-Ghazal SK, Sully L, Fallowfield L, Blamey RW. The psychologi-cal impact of immediate rather than delayed breast reconstruction.Eur J Surg Oncol 2000;26:17–19.
4. Weitzner MA, Meyers CA, Stuebing KK, Saleeba AK. Relationshipbetween quality of life and mood in long-term survivors of breastcancer treated with mastectomy. Support Care Cancer 1997;5:241–248.
5. Ray C. Psychological implications of mastectomy. Br J Soc ClinPsychol 1977;16:373–377.
6. Edsander-Nord A, Brandberg Y, Wickman M. Quality of life,patients’ satisfaction, and aesthetic outcome after pedicled or freeTRAM flap breast surgery. Plast Reconstr Surg 2001;107:1142–1153; discussion 1154–1145.
7. Girotto JA, Schreiber J, Nahabedian MY. Breast reconstruction inthe elderly: Preserving excellent quality of life. Ann Plast Surg2003;50:572–578.
8. Klassen AF, Pusic AL, Scott A, Klok J, Cano SJ. Satisfaction andquality of life in women who undergo breast surgery: A qualitativestudy. BMC Womens Health 2009;9:11.
9. Damen TH, Timman R, Kunst EH, Gopie JP, Bresser PJ, SeynaeveC, Menke-Pluijmers MB, Mureau MA, Hofer SO, Tibben A. Highsatisfaction rates in women after DIEP flap breast reconstruction. JPlast Reconstr Aesthet Surg 2010;63:93–100.
10. Cordeiro PG, Pusic AL, Disa JJ, McCormick B, VanZee K. Irradia-tion after immediate tissue expander/implant breast reconstruction:Outcomes, complications, aesthetic results, and satisfaction among156 patients. Plast Reconstr Surg 2004;113:877–881.
11. Ananthakrishnan P, Lucas A. Options and considerations in the tim-ing of breast reconstruction after mastectomy. Cleve Clin J Med2008;75 (Suppl 1):S30–S33.
12. Schain WS. Psychosocial factors in mastectomy and reconstruction.In:Noone RB, editor. Plastic and Reconstructive Surgery of theBreast. Pennsylvania: B.C. Decker; 1991. pp327–343.
13. Teimourian B, Adham MN. Survey of patients’ responses to breastreconstruction. Ann Plast Surg 1982;9:321–325.
14. Wellisch DK, Schain WS, Noone RB, Little JW III. Psychosocialcorrelates of immediate versus delayed reconstruction of the breast.Plast Reconstr Surg 1985;76:713–718.
15. Ueda S, Tamaki Y, Yano K, Okishiro N, Yanagisawa T, Imasato M,Shimazu K, Kim SJ, Miyoshi Y, Tanji Y, Taguchi T, Noguchi S.Cosmetic outcome and patient satisfaction after skin-sparing mastec-tomy for breast cancer with immediate reconstruction of the breast.Surgery 2008;143:414–425.
16. Stevens LA, McGrath MH, Druss RG, Kister SJ, Gump FE, FordeKA. The psychological impact of immediate breast reconstructionfor women with early breast cancer. Plast Reconstr Surg1984;73:619–628.
17. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, CanoSJ. Development of a new patient-reported outcome measure forbreast surgery: the BREAST-Q. Plast Reconstr Surg 2009;124:345–353.
18. Roth RS, Lowery JC, Davis J, Wilkins EG. Quality of life and affec-tive distress in women seeking immediate versus delayed breastreconstruction after mastectomy for breast cancer. Plast ReconstrSurg 2005;116:993–1002; discussion 1003–1005.
19. Balch CM, Jacobs LK. Mastectomies on the rise for breast can-cer: ‘‘The tide is changing’’. Ann Surg Oncol 2009;16:2669–2672.
QoL Measures Before Breast Reconstruction 257
Microsurgery DOI 10.1002/micr

20. Kroll SS, Coffey JA Jr, Winn RJ, Schusterman MA. Acomparison of factors affecting aesthetic outcomes of TRAMflap breast reconstructions. Plast Reconstr Surg 1995;96:860–864.
21. Dean C, Chetty U, Forrest AP. Effects of immediate breast recon-struction on psychosocial morbidity after mastectomy. Lancet1983;1:459–462.
22. Elkowitz A, Colen S, Slavin S, Seibert J, Weinstein M,Shaw W. Various methods of breast reconstruction after mas-tectomy: An economic comparison. Plast Reconstr Surg1993;92:77–83.
23. Khoo A, Kroll SS, Reece GP, Miller MJ, Evans GR, RobbGL, Baldwin BJ, Wang BG, Schusterman MA. A comparison
of resource costs of immediate and delayed breast reconstruc-tion. Plast Reconstr Surg 1998;101:964–968; discussion 969–970.
24. D’Souza N, Darmanin G, Fedorowicz Z. Immediate versus delayedreconstruction following surgery for breast cancer. Cochrane data-base Syst Rev 2011;7:CD008674.
25. Flores JI, Magarakis M, Venkat R, Shridharani SM, Rosson GD.Bilateral simultaneous breast reconstruction with SGAP flaps. Micro-surgery 2012;32:344–350.
26. Venkat R, Lee JC, Rad AN, Manahan MA, Rosson GD. Bilateral au-tologous breast reconstruction with deep inferior epigastric arteryperforator flaps: Review of a single surgeon’s early experience.Microsurgery 2012;32:275–280.
258 Rosson et al.
Microsurgery DOI 10.1002/micr