Embed Size (px)
Citation preview

Int. J. Radiation Oncology Biol. Phys., Vol. 78, No. 2, pp. 454–460, 2010Copyright � 2010 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$–see front matter
robp.2009.07.1702
doi:10.1016/j.ijCLINICAL INVESTIGATION Head and Neck
QUALITY-OF-LIFE-ADJUSTED SURVIVAL ANALYSIS OF CONCURRENT CHEMORADIOTHERAPY FOR LOCALLY ADVANCED (NONMETASTATIC)
NASOPHARYNGEAL CANCER
FEI GAO, PH.D.,*y JOSEPH WEE, FRCR.,*z HWEE BEE WONG, M.SC.,x AND DAVID MACHIN, D.SC.{
*Division of Clinical Trials and Epidemiological Sciences, National Cancer Centre, Singapore; yHealth Services & Systems Research,Duke-NUS Graduate Medical School, Singapore; zDepartment of Radiation Oncology, National Cancer Centre, Singapore; xClinicalTrials and Epidemiology Research Unit, Singapore; and {Medical Statistics Unit, School of Health and Related Research, University of
Sheffield, Sheffield, United Kingdom
Correspand Epide11 HospE-mail: ct
Purpose: To assess whether the benefits of adding cisplatin (CDDP) concurrent with radiotherapy, followed byadjuvant CDDP and fluorouracil, justifies the toxicity cost for nasopharyngeal cancer (NPC) using the quality-adjusted time without symptoms or toxicity (Q-TWiST) approach.Methods and Materials: One hundred seven patients treated with radiotherapy (RT) and 111 with concurrentchemotherapy and radiotherapy (CRT) were analyzed. The overall survival was divided into three health states:time on active treatment only, during which any subjective nonhematologic toxic event of grade > = 3 was reported;time without symptoms of disease relapse; or treatment and time following first disease RELapse. The relativeadvantage of CRT and RT was examined by conducting the analysis cumulatively at restriction times 3, 6, 24,36, 48 months.Results: At 48 months, the improvement in disease-free survival was 14.4% for CRT, whereas that for overallsurvival was 18.9%. The differences in Q-TWiST were �0.4, �0.7, 0.1, 1.6, and 3.6 months at 3, 6, 24, 36, and48 months, respectively, with positive differences favoring CRT. At 24 months, the difference in Q-TWiST beganto favor CRT. At 36 months, CRT may be the preferred option from the patient’s viewpoint if the time spent in theREL state is valued to be <0.83, with the value of perfect health being 1. Finally, Q-TWiST accumulated within 48months indicated a significant advantage in quality-adjusted survival time for CRT (p = 0.020).Conclusion: Irrespective of how patients valued periods of toxicity and delayed disease progression, concurrentchemotherapy and radiotherapy offered NPC patients significantly more quality-adjusted survival than radiother-apy alone in the long term. � 2010 Elsevier Inc.
Q-TWiST, Survival analysis, Nasopharyngeal cancer, Concurrent chemoradiotherapy, Cisplatin.
INTRODUCTION
It is important that the consequences of favorable results of
randomized therapeutic trials conducted in cancer are fully
placed in an appropriate context. Thus, at the end of a trial,
if one of the treatment options has a therapeutic advantage
and brings a clear survival advantage, then this treatment
should be brought quickly into use for future patients. How-
ever if, for example, this ‘‘advantage’’ is accompanied by
significant additional serious toxicity, it may not be easy to
recommend its use for all patients. Such considerations led
Gelber and Goldhirsch (1), among others, to weigh the
(survival) benefits against the (symptoms and toxicity) costs
by means of the quality-adjusted time without symptoms or
toxicity (Q-TWiST). Basically, the Q-TWiST method
involves the partitioning of survival duration into clinically
relevant health states (e.g., treatment toxicity, progression-
ondence to: Gao Fei, Ph.D., Division of Clinical Trialsmiological Sciences, National Cancer Centre Singapore,
ital Drive, Singapore 169610. Fax: (+65) 62250047;[email protected]
454
free time, disease progression), assigning preference weights
(or utilities) to these health states, and then calculating
quality-of-life-adjusted weighted sums of the mean duration
of each health state to create the overall Q-TWiST survival
time (2, 3). This approach to analysis and interpretation of
some trials in breast cancer led to support for the use of
adjuvant chemoendocrine therapy in postmenopausal node-
positive patients for a wide range of relative values assigned
to periods with symptoms and toxicity (1, 4, 5). In addition to
breast cancer, Q-TWiST analyses have been used to compare
treatments for other types of cancers, such as resectable rectal
cancer (6) and high-risk resected cutaneous melanoma (7).
A fuller list of relevant publications can be found in Revicki
et al. (8). However, to our knowledge, the Q-TWiST method-
ology has not been applied in nasopharyngeal cancer (NPC).
The situation for patients treated with surgery and chemo-
radiation therapy for NPC is similar to those with breast
Conflict of interest: none.Received May 27, 2009, and in revised form July 28, 2009.
Accepted for publication July 28, 2009.

Q-TWiST analysis of concurrent chemoradiotherapy for NPC d F. GAO et al. 455
cancer in that the survival ‘‘gain’’ and treatment ‘‘cost’’ have
to be balanced in some way. Thus, although the clinical trial
conducted by Wee et al. (9) demonstrated a clear survival
advantage to concurrent chemotherapy and radiotherapy
(CRT) vs. radiotherapy alone (RT), this was offset by a higher
toxicity rate. The trial reported ‘‘oropharyngeal mucositis
remained a significant problem, especially for the CRT
arm.. The incidence of grade 3 or 4 mucositis was 48%
for the CRT arm and 32% for the RT alone arm; these figures
were much higher than those reported in the 0099 Trial (37%
and 28%, respectively) probably because of the difference in
RT techniques and possibly because of the split-dose sched-
uling of CDDP’’ (9). Thus, questions were raised concerning
whether the benefits of chemotherapy justified the costs for
the individual NPC patients. As a consequence, we have
reexamined the clinical trial data to assess whether the impact
of time duration with and without progression and duration
of toxicities resulted in differences in quality-adjusted sur-
vival. The purpose of this article is integrate these aspects
into a composite recommendation using the Q-TWiST
approach.
METHODS AND MATERIALS
Study designBetween September 1997 and May 2003, the survival benefit of
adding cisplatin (CDDP) concurrent with radiotherapy, followed by
adjuvant CDDP and fluorouracil (FU), in patients with endemic
NPC was studied in a Phase III clinical trial (9). The details of
patient selection and random assignment to treatment, as well as
evaluation have been described previously. In brief, all patients,
with Stage II–IV NPC received standard-course radiotherapy to
a dose of 70 Gy in 35 fractions (2 Gy per fraction). Those who
were randomized to CRT received CDDP on Weeks 1, 4, and 7 con-
current with their radiotherapy followed by a further three cycles of
adjuvant chemotherapy comprising CDDP and FU administered
between Weeks 11 and 19.
Because the Radiation Therapy Oncology Group Acute Radiation
Morbidity Scoring Criteria does not have a classification for renal,
infection, metabolic, and GI toxicities, toxicity during treatment
was classified based on the National Cancer Institute Common Tox-
icity Criteria. Treatment toxicity was evaluated at the completion of
each cycle for CRT and at the completion of treatment for RT alone.
Util
ity
0.0
0.5
1.0
TOX
TWiST
Months from s
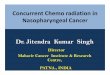
Fig. 1. Calculation of quality-adjusted time without symptomsspent on active treatment, during which any subjective toxic eventoms of disease relapse or treatment (TWiST), and time followinfor TOX and mrel = 0.5 for REL.
Statistical analysisOverall survival (OS) is defined as the time from the start of treat-
ment to death from any cause or to the date when the patient was last
known to be alive. Survival curves were calculated using the
Kaplan-Meier technique, and between treatments comparisons
were made using the log-rank test (10). The hazard ratios (HR) sum-
marizing the differences between treatment groups were estimated
by Cox regression, and 95% confidence intervals (CI) were
obtained. Although data on relapse and death are available up to
9 years from the date of the start of treatment, our analysis is con-
fined to the first 4 years because the ascertainment of recurrence
are more complete for this time period.
Health statesComponents of the OS time are the disease-free survival (DFS)
and the time spent on treatment, during which any subjective toxic
events of grade >= 3 was reported (TOX). DFS is the time from
the start of the treatment to whichever occurred first, relapse or death,
and is censored if the patient is alive without progression (6). TOX is
the period of time on active treatment and has no censored observa-
tions. Any nonhematologic toxicities (mucositis, pharyngitis/oro-
pharyngitis, anorexia, emesis, skin desquamation, renal toxicity, or
hospital admission) of grade >= 3 were noted by the investigators
during the active treatment. TOX was defined as encompassing the
entire period of active treatment because there are multiple toxicities
of concern; zero TOX time was assigned to the remainder of patients.
The trial schedule permitted 1 or 2 weeks’ delay in CRT cycles to al-
low recovery from toxicity, and thus an additional 2 weeks (14 days)
of time were added to TOX following CRT. Following Gelber et al.(6), hematologic toxic effects, such as neutrophils and platelets, were
not included in TOX because these side effects did not have a direct
subjective influence on the patients’ quality of life.
The OS for the individual patients was divided into three clinical
health states associated with differing quality of life:
1. time spent with radiotherapy only or CDDP concurrent with
radiotherapy followed by adjuvant CDDP and FU, during which
any subjective nonhematologic toxic events of grade >= 3 were
reported, TOX;
2. time without symptoms of disease relapse or treatment
(TWiST) = DFS – TOX; and
3. time following first disease RELapse ending with death or cen-
soring, REL = OS – DFS.
The mean time spent in each of TOX, DFS, and OS was estimated
for each treatment group as the area under the corresponding sur-
vival curves.
REL DEATH
tart of treatment
or toxicity (Q-TWiST): weighted summation of the timets of grade >= 3 were reported (TOX), time without symp-g first disease relapse (REL). Utility weights of mtox = 0.5

Months from start of treatment
Perc
ent
0 1 2 3 4 5
1.0
0.8
0.6
0.4
0.2
0.0
RTCRT
a
Months from start of treatment
Perc
ent
0 12 24 36 48 60 72 84 96 108
0.0
0.4
0.8
0.2
0.6
1.0
RTCRT
b
Months from start of treatment
Perc
ent
0 12 24 36 48 60 72 84 96 108
0.0
0.4
0.8
0.2
0.6
1.0
R TC RT
c
Fig. 2. Kaplan-Meier estimates for (a) toxicity state (TOX), (b) dis-ease-free survival (DFS), and (c) overall survival (OS) by treatmentgroup. CRT = concurrent chemotherapy and radiotherapy; RT = ra-diotherapy alone.
Table 1. Median (months) and 95% CI for TOX, DFS, andOS by treatment group
Healthstate
RT(95% CI)
CRT(95% CI) Difference
Log-rank,p
TOX 0 (0 to 0) 2.1 (0 to 2.4) 2.1 <0.001DFS 51.6
(28.0 to 109.2)95.7
(65.8 to 114.4)44.1 0.037
OS 55.0(43.8 to 93.8)
—(79.8 to 114.4)
— 0.005
Abbreviations: CI = confidence interval; CRT = concurrent che-motherapy and radiotherapy; DFS = disease-free survival; OS =overall survival; RT = radiotherapy alone; TOX = toxicity state.
456 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 2, 2010
Q-TWiSTQ-TWiST analysis defines utility weights mtox and mrel, taking
values between 0 and 1 to represent the quality of life value during
TOX and REL, relative to life experiencing TWiST (3). The weight
for the health state of DEATH is 0, and the weight for TWiST is 1.
Each weighting represents the valuation a newly diagnosed patient
would place on a health state after being given a description of the
associated symptoms and their frequency of occurrence. For exam-
ple, mrel = 0.5 for REL indicates that each 2 months of survival fol-
lowing relapse is equivalent to 1 month were the patients in the
TWiST state. This scenario is illustrated in Fig. 1. Finally:
Q-TWiST ¼ mtoxTOXþ TWiSTþ mrelREL;
the value of which will depend critically on the choice of weights
assigned.
Threshold utility analysisA threshold utility analysis was used to determine for which
values of the utility parameters the two treatment arms, RT and
CRT, have the same expected Q-TWiST (3, 11). This approach is
also called inverse inference (12). Treatments were compared using
a spectrum of utility parameter, mtox and mrel, values, over the full
range of utility weight values between 0 and 1. However, because
the relative advantage of CRT and RT in terms of Q-TWiST is likely
to change over time, this pattern was examined by conducting the
analysis cumulatively at restriction times 3, 6, 24, 36, and finally
48 months (Fig. 4). The first two of these were chosen to correspond
to the completion of RT and of CRT, respectively.
The treatment comparison is obtained by subtracting
the RT from the CRT group estimate to obtain:
Q-TWiST6 ¼ Q-TWiSTCRT � Q-TWiSTRT: The bootstrap
technique (13) was used to obtain standard error estimates for
mean time spent in TOX, DFS, and OS using 2,000 bootstrap sam-
ples of the same size as the number of patients under consideration.
Standard error estimates, seRT and seCRT, were obtained for RT and
CRT separately at each restriction. The 95% CIs of difference be-
tween treatments were calculated from the standard error estimates
on the basis of the standard normal distribution. The 95% CI for the
treatment effect is given by Q-TWiST6 � 196se6, where
se6 ¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffise2
RT þ se2CRT
p: The null hypothesis of no difference in
mean Q-TWiST between RT and CRT was tested using a Z test.
RESULTS
Patient characteristics and toxicityTwo hundred eighteen patients were included in the
randomized trial, 107 patients treated with RT and 111
with CRT. Three RT patients defaulted treatment soon after
random assignment and were excluded from this analysis.
The two groups were well balanced in terms of age, sex, eth-
nicity, tumor size, nodal status, and tumor staging (9).
Altogether, 96 patients experienced Grade 3, 4, or 5 nonhe-
matologic toxicity: RT 35 (Grade 3 only), and CRT 61. Over-
all, 49 CRT patients were assigned zero TOX because there

Months from start of treatment
Perc
ent
Perc
ent
0 3 6 12 24 38 48
1.0
0.8
0.6
0.4
0.2
0.0
a
TWiST
REL
TOX
Months from start of treatment0 3 6 12 24 36 48
1.0
0.8
0.6
0.4
0.2
0.0
b
TWiST
REL
TOX
Fig. 3. Partitioned survival plots showing the mean times in activetreatment during which any subjective toxic events of grade >= 3were reported (TOX), time without symptoms of disease relapseor treatment (TWiST), and time following first disease relapse(REL) by treatment group (a) radiotherapy alone (RT) and (b) con-current chemotherapy and radiotherapy (CRT).
Q-TWiST analysis of concurrent chemoradiotherapy for NPC d F. GAO et al. 457
was no indication of any Grade 3–5 nonhematologic toxicity
in this group.
Kaplan-MeierThe Kaplan-Meier curves for TOX, DFS, and OS by treat-
ment group are shown in Fig. 2, and the corresponding
median survival times are given in Table 1. It is clear that
less time is spent in the toxicity state with RT than CRT
(median 0 vs. 2.1 months, p < 0.001), but DFS (51.6 vs.
95.7 months, p = 0.037) and OS (p = 0.005) are extended
with CRT. At 4 years, the improvement in DFS is 14.4%,
whereas that for OS is 18.9%. The hazard ratios in favor of
CRT, using all the updated data including that beyond 4 years,
are HRDFS = 0.67 (95% CI, 0.46 to 0.98) and HROS = 0.58
(95% CI, 0.39 to 0.85).
Q-TWiSTFigure 3 displays the partitioned survival plots for RT and
CRT groups accumulated 48 months after start of treatment.
For each selected restriction time, and for mtox = mrel = 0.5,
Table 2 gives the mean duration in the three health states
by treatment group and the difference between treatments
in Q-TWiST. The differences in Q-TWiST were �0.4,
�0.7, 0.1, 1.6, and 3.6 months at the restriction times 3, 6,
24, 36, and 48 months, respectively, with positive differences
favoring CRT.
During the radiotherapy phase (about 3 months), TWiST
was longer with RT alone than with CRT (2.4 vs. 1.5 months,
respectively; 95% CI, �1.2 to �0.6 months; p < 0.001),
whereas REL was zero with both treatments. After the initi-
ation of adjuvant CDDP and FU, restriction time 6 months,
of CRT, this patient group spent an average of 1.5 more
months under treatment compared with RT alone arm (95%
CI, 1.1 to 1.9 months; p < 0.001). As would be expected,
TWiST was even longer with RT alone (5.2 vs. 3.8 months,
respectively; 95% CI, �1.9 to �0.9 months; p < 0.001), but
REL was still similar for both arms. Thus, with the utility
weights set at 0.5, for TOX and REL health states, there
was a 0.7-month significant difference in Q-TWiST favoring
RT alone (5.6 vs. 4.9 months, respectively; 95% CI, �0.9 to
�0.5 months; p < 0.001).
At 24 months, TWiST was slightly shorter in RT alone
(18.1 vs. 18.2 months, respectively; 95% CI, �1.8 to 2.0
months; p = 0.919). The difference in Q-TWiST between
RT and CRT albeit close to zero, was beginning to favor
CRT over RT alone (+0.1 months, 95% CI, �1.1 to 1.3
months, p = 0.866). Thereafter, an increasing treatment effect
in favor of CRT was seen over time. The effect increases in
both the amount of TWiST and Q-TWiST. Eventually at
48 months from start of treatment Q-TWiST was signifi-
cantly different between the treatments in favor of CRT
over RT (p = 0.020).
Threshold utility analysisIn the utility threshold plot (Fig. 4), the vertical axis is the
utility for time spent in TOX (mtox) and the horizontal axis is
the utility associated with time after first disease relapse
(mrel). The sloping lines within the graph correspond to the
threshold at each of restriction times. The utility plane con-
tains all possible pairs of values for mtox and mrel between
0 and 1 (shaded area). The vertical axis has been extended
downward into negative utilities (although in practice nega-
tive utilities are not theoretically possible) for toxicity to
emphasize that when the restriction time is 48 months all
value pairs of mtox and mrel, within the range from 0 to 1,
give greater Q-TWiST to CRT. In contrast, both the 3- and
6-month lines lie completely in the utility plane, so that dur-
ing the active treatment stage, patients’ preference for CRT or
RT is determined by their utility, mtox, for time spent in TOX.
The 24-month restriction line lies within the utility plane for
mrel >0.07, whereas that at 36-month line is within the utility
plane when mrel >0.83.
DISCUSSION
The majority of clinical trials concerned with several
modalities for cancer therapy often have multiple endpoints

Table 2. Restricted mean duration of health states (months) and differences between treatments accumulated with 3, 6, 24, 36, and 48months and all follow-up to 9 years from start of treatment (mtox = mrel = 0.5)
3 months 6 months
Healthstate
RT alone(n = 107)
CRT(n = 111)
Difference(95% CI) p
RT alone(n = 107)
CRT(n = 111)
Difference(95% CI) p
TOX 0.6 1.5 0.9 (0.6 to 1.2) <0.001 0.6 2.1 1.5 (1.1 to 1.9) <0.001DFS 3.0 3.0 0.0 (�0.1 to 0.1) 1 5.8 5.9 0.1 (�0.1 to 0.3) 0.317OS 3.0 3.0 0.0 (�0.1 to 0.1) 1 5.9 5.9 0.0 (�0.2 to 0.2) 1.000TWiST = DFS – TOX 2.4 1.5 �0.9 (�1.2 to –0.6) <0.001 5.2 3.8 �1.4 (�1.9 to �0.9) <0.001REL = OS – DFS 0.0 0.0 0.0 (�0.1 to 0.1) 1 0.1 0.0 �0.1 (�0.3 to 0.1) 0.432Q-TWiST 2.7 2.3 �0.4 (�0.6 to –0.2) <0.001 5.6 4.9 �0.7 (�0.9 to �0.5) <0.001
24 months 36 monthsTOX 0.6 2.1 1.5 (1.1 to 1.9) <0.001 0.6 2.1 1.5 (1.1 to 1.9) <0.001DFS 18.7 20.3 1.6 (�0.3 to 3.5) 0.097 25.6 29.1 3.5 (0.2 to 6.8) 0.036OS 22.0 22.1 0.1 (�1.2 to 1.4) 0.879 30.8 31.9 1.1 (�1.3 to 3.5) 0.371TWiST = DFS – TOX 18.1 18.2 0.1 (�1.8 to 2.0) 0.919 25.0 27.0 2.0 (�1.3 to 5.3) 0.235REL = OS – DFS 3.3 1.8 �1.5 (�3.8 to 0.8) 0.196 5.2 2.8 �2.4 (�6.4 to 1.6) 0.224Q-TWiST 20.1 20.2 0.1 (�1.1 to 1.3) 0.866 27.9 29.5 1.6 (�0.5 to 3.7) 0.129
48 months All information to 9 years of follow-upTOX 0.6 2.1 1.5 (1.1 to 1.9) <0.001 0.6 2.1 1.5 (1.1 to 1.9) <0.001DFS 31.9 37.5 5.6 (0.9 to 10.3) 0.019 57.1 73.3 16.2 (3.6 to 28.8) 0.012OS 38.1 41.2 3.1 (�0.6 to 6.8) 0.099 63.6 80.9 17.3 (6.2 to 28.4) 0.002TWiST = DFS – TOX 31.3 35.4 4.1 (�0.6 to 8.8) 0.087 56.5 71.2 14.7 (2.1 to 27.3) 0.022REL = OS – DFS 6.2 3.7 �2.5 (�8.4 to 3.4) 0.405 6.5 7.6 1.1 (�15.7 to 17.9) 0.898Q-TWiST 34.7 38.3 3.6 (0.6 to 6.6) 0.020 60.1 76.1 16.0 (7.6 to 24.4) <0.001
Abbreviations: CI = confidence interval; CRT = concurrent chemotherapy and radiotherapy; DFS = disease-free survival; OS = overall sur-vival; Q-TWiST = quality-adjusted time without symptoms or toxicity; RT = radiotherapy alone; TOX = toxicity state; TWiST = time withoutsymptoms of disease relapse or treatment.
0.0 0.2 0.4 0.6 0.8 1.0µrel
µ tox
-3-2
-10
1
48m
0.0 0.4 0.80.2 0.6 1.0
3 & 6m
24m
36m
Fig. 4. Utility threshold plot (artificially extended down on thetoxicity scale for illustrative purposes). Each upward sloping linecorresponds to the threshold at each of the corresponding restrictiontime. The shaded utility plane contains all possible pairs of valuesfor mtox and mrel between 0 and 1. This figure shows that concurrentchemotherapy and radiotherapy (CRT) provides more quality-adjusted time without symptoms or toxicity (Q-TWiST) thanradiotherapy alone (RT) for all utilities value pairs ranging from0 (death) to 1 (time without symptoms of disease relapse or treat-ment, TWiST) at 48 months.
458 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 2, 2010
of concern, such as overall survival, disease-free survival,
toxicity profile, and quality of life, and these are often
reported separately. However, if the major purpose of the trial
is to help decide which treatment strategy is more likely to
benefit the patient, then clinical decision making on the value
of a therapy must balance the trade-offs between treatment
toxicities and expected survival. The trial we analyzed used
the 0099 trial regimen (14) and demonstrated a survival
benefit in favor of concurrent chemotherapy and radiother-
apy, but it was not specifically designed to provide an insight
into the quality of survival. Nevertheless, this article provides
a comprehensive view of when and how a concurrent chemo-
therapy and radiotherapy regimen may be preferred from the
patient’s viewpoint by examining treatment comparisons
across a range of possible utilities and restriction times
from 3 to 48 months. We also provide additional information
about the trade-off between toxicities and delayed disease
progression using Q-TWiST. This approach quantitatively
adjusts periods in which treatment toxicities or symptoms
of disease progression are present to reflect the potentially
reduced value for the patient.
Although patients allocated to CRT arm had a greater
mean time spent in the treatment (2.1 vs. 0.6 months, respec-
tively; p < 0.001), we have shown a survival advantage after
55.3 months (4.6 years) median follow-up. The Q-TWiST
accumulated within 48 months from the start of treatment
also indicated a significant advantage in quality-adjusted sur-
vival time for the CRT arm (p = 0.020). At 24 months, the
difference in quality-adjusted time begins to favor concurrent
chemotherapy and radiotherapy. At 36 months, the concur-
rent chemotherapy and radiotherapy could be the preferred
option from the patient’s point of view when the time spent
in REL state is valued to be <0.83, with the value of perfect
health being 1. Finally at 48 months, the inferences from

Q-TWiST analysis of concurrent chemoradiotherapy for NPC d F. GAO et al. 459
Q-TWiST results are not dependent on their actual values,
because the 48-month threshold utility line lies completely
below the utility plane containing all possible pairs of utility
values relative to the two treatments. Thus, whatever values
are chosen for mtox and mrel, the quality-adjusted survival
time is always greater for the CRT arm than the RT alone
at 48 months.
The main Q-TWiST analysis depends on the values
assigned to utility weights for the selected health states. It
is the most desirable if prospective measurement of utilities
from subjects participating in the clinical trial are assessed
using the time trade-off method or standard gamble (8). In
the absence of study-based utility measures, investigators
have tried to estimate utilities from the health-related quality
of life (HRQL) and other patient reported outcomes prospec-
tively collected in a clinical trial (15, 16). For example,
Fairclough et al. (15) compared intensity of adjuvant chemo-
therapy regimens for breast cancer using Q-TWiST methods.
They used Breast Chemotherapy Questionnaire scores to es-
timate utilities for treatment-related toxicity. A few sets of
values used include mtox = 0.68 to 0.9, mrel = 0.5 or 0.6.
Thus, a drawback of our study is the use of utility assessment
by means of threshold utility analysis, because Revicki et al.(8) ranked it less valid than various possible sources of utility
data, such as prospective utility measurement (most valid).
As with survival analyses, the Q-TWiST analysis does not
take into account the relative importance of early costs of
treatment toxicity y delayed benefits of adjuvant chemother-
apy. For example, in the present trial, patients are aged from
14 to 76 years. Thus, for elderly patients, early times may be
more important, and the delayed benefits of adjuvant chemo-
therapy will be less important relative to immediate toxicity.
In such cases, it may make more sense to use age-specific
utility weights. In this analysis, we were arbitrarily assigning
1.0 to the best possible health state TWiST, which may bias
the comparison in favor of the treatment with the longest du-
ration in the ‘‘best’’ health state.
In general, in applying Q-TWiST methodology, TOX is
meant to represent the period of treatment-related toxicity,
which can extend significantly beyond the final day of radia-
tion or the final infusion of adjuvant chemotherapy. For
example, in a Q-TWiST study of rectal cancer, Gelber
et al. (6) defined TOX using the actual duration of patient-
reported symptoms, and additional amounts of time (up to
3 weeks) were added to TOX to allow for recovery from toxic
effects. Further, in a breast cancer study, Gelber et al. (17)
defined TOX to include an entire month when any subjective
toxic effect of any grade occurred and an additional 3 months
after the last report of alopecia or weight gain to allow for
recovery. In our trial, the data have shown that CRT patients
could receive reduced doses or experience delay in cycles
because of toxicity (9). They could even decline all cycles
of chemotherapy without toxicities of grade >= 3 having
been noted. Therefore, we chose to define TOX as the ‘‘entire
time on active treatment’’ when any subjective nonhemato-
logic toxicities of grade >= 3 were noted during the active
treatment and without the precise knowledge of details con-
cerning intensity of symptoms or subjective burden of toxic-
ity. Our definition of TOX provided the possibility of
applying the method to other adjuvant NPC trials for which
only the type of treatment is known, but the patient records
lack information about the precise nature and grade of toxic-
ity. This is important because combined chemoradiotherapy
is increasingly being used to treat advanced head and neck
cancers.
Radiation therapy for head and neck cancers, however,
often results in some unpleasant side effects, such as perma-
nent xerostomia and hearing loss. Unfortunately, the late
radiation-induced toxicities after the completion of the last
cycle of treatment were not evaluated in our trial (9). Hence,
we are unable to consider the influence of late occurring toxic
effects on the patients’ quality of life. This may affect our
findings regarding the time point at which quality-adjusted
survival is improved. In the present trial (9), all patients
were treated using conventional techniques. The dose was
restricted to 70 Gy. However, a greater hearing loss up to
2 years after treatment in CDDP was shown in a subset of
patients from this trial (18). However, in the Al-Sarraf trial
(14) (using the same regimen as in this trial), no Grade 3 or
4 xerostomia was observed in the concurrent phase.
The Q-TWiST analysis used here shows that irrespective
of how patients value periods of toxicity and delayed disease
progression, adding CDDP concurrent with radiotherapy fol-
lowed by adjuvant CDDP and FU offers patients significantly
more quality-adjusted survival than radiotherapy alone in the
long term, although, should the comorbidity have reduced
the expected life span of the patient to <2 years, radiation
alone might have been regarded as the best treatment.
REFERENCES
1. Gelber RD, Goldhirsch A, for the Ludwig Breast Cancer StudyGroup. A new endpoint for the assessment of adjuvant therapyin postmenopausal women with operable breast cancer. J ClinOncol 1986;4:1772–1779.
2. Gelber RD, Gelman RS, Goldhirsch A. A quality-of-life-oriented endpoint for comparing therapies. Biometrics 1989;45:781–795.
3. Glasziou PP, Simes RJ, Gelber RD. Quality adjusted survivalanalysis. Stat Med 1990;9:1259–1276.
4. Gelber RD, Goldhirsch A, Castiglione M, et al. Time withoutsymptoms and toxicity (TWiST): A quality-of-life-oriented
endpoint to evaluate adjuvant therapy. In: Salmon SE, editor.Adjuvant therapy of cancer, Vol.5. Philadelphia: Grune & Strat-ton; 1987. p. 455–465.
5. Goldhirsch A, Gelber RD, Simes RJ, et al., for the LudwigBreast Cancer Study Group. Costs and benefits of adjuvanttherapy in breast cancer: A quality-adjusted survival analysis.J Clin Oncol 1989;7:36–44.
6. Gelber RD, Goldhirsch A, Cole BF, et al. A quality-adjustedtime without symptoms or toxicity (Q-TWiST) analysis ofadjuvant radiation therapy and chemotherapy for resectablerectal cancer. J Natl Cancer Inst 1996;88:1039–1045.

460 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 2, 2010
7. Cole BF, Gelber RD, Kirkwood JM, et al. Quality-of-life-adjusted survival analysis of interferon alfa-2b adjuvant treat-ment of high-risk resected cutaneous melanoma: An EasternCooperative Oncology Group study. J Clin Oncol 1996;14:2666–2673.
8. Revicki DA, Feeny D, Hunt TL, Cole BF. Analyzing oncologyclinical trial data using the Q-TWiST method: Clinical impor-tance and sources for health state preference data. Qual LifeRes 2006;15:411–423.
9. Wee J, Tan EH, Tai BC, et al. Randomized trial of radiotherapyversus concurrent chemoradiotherapy followed by adjuvantchemotherapy in patients with American Joint Committee onCancer/International Union against cancer Stage III and IVnasopharyngeal cancer of the endemic variety. J Clin Oncol2005;23:6730–6738.
10. Peto R, Pike MC, Armitage P, et al. Design and analysis ofrandomized clinical trials requiring prolonged observation ofeach patient. II. Analysis and examples. Br J Cancer 1977;35:1–39.
11. Simes RJ. Application of statistical decision theory to treatmentchoices: Implications for the design and analysis of clinicaltrials. Stat Med 1986;5:411–420.
12. Hilden J. Reporting clinical trials from the viewpoint ofa patient’s choice of treatment. Stat Med 1987;6:745–752.
13. Davison AC, Hinkley DV. Bootstrap methods and their applica-tion. Cambridge, UK: Cambridge University Press; 1997.
14. Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapyversus radiotherapy in patients with advanced nasopharyngealcancer: Phase III randomized Intergroup study 0099. J ClinOncol 1998;16:1310–1317.
15. Fairclough DL, Fetting JH, Cella D, et al. Quality of life andquality adjusted survival for breast cancer patients receivingadjuvant therapy. Eastern Cooperative Oncology Group(ECOG). Qual Life Res 1999;8:723–731.
16. Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ 2002;21:271–292.
17. Gelber RD, Goldhirsch A, Cavalli F. Quality-of-life-adjustedevaluation of adjuvant therapies for operable breast cancer.The International Breast Cancer Study Group. Ann InternMed 1991;114:621–628.
18. Low WK, Toh ST, Wee J, et al. Sensorineural hearing loss after ra-diotherapy and chemoradiotherapy: A single, blinded, randomizedstudy. Clin Oncol 2006;24:1904–1909.