Upload
trinhdat
View
215
Download
1
Embed Size (px)
Citation preview
1 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
1
QualityinPrimaryCareFinalReportoftheQualityWorkingGrouptothePrimaryHealthcarePlanningGroup
August2011
i ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
i
TableofContents
WorkingGroupMembers ................................................................................................................... iii
Abbreviations ..................................................................................................................................... iv
ExecutiveSummary ............................................................................................................................. 1
Section1:Background.......................................................................................................................... 7
DevelopmentandEstablishmentofthePrimaryHealthcarePlanningGroup ......................................... 7
MandateoftheQualityWorkingGroup................................................................................................... 7
Section2:TrendsandCurrentStateofQualityImprovementinPrimaryHealthcareinOntarioandtheChangeImperative............................................................................................................................... 9
CurrentStateofPrimaryCareinOntario ................................................................................................. 9
CurrentStateofQualityinCanadaandOntario.....................................................................................10
CanadaRelativetoOtherCountriesandOntario ...............................................................................10PreventiveCareBonuses ....................................................................................................................12
CurrentStateofQualityImprovementInitiativesinOntario .................................................................13
Section3:TerminologyAssociatedWithQuality ................................................................................ 16
DefiningQuality,QualityImprovement,QualityAssurance,AccreditationandKnowledgeTransfer...16
Section4:StrategiesandEnablersofQuality:ALiteratureReview..................................................... 18
PerformanceMeasurement.................................................................................................................... 18
TripleAimFramework.........................................................................................................................19SuccessStories ....................................................................................................................................22
PerformanceTargets...............................................................................................................................23
ElectronicMedicalRecordandElectronicHealthRecord ......................................................................24
PrimaryHealthcareTeams......................................................................................................................26
PatientEnrolment...................................................................................................................................28
PatientEngagement................................................................................................................................28
ResearchandEvaluation.........................................................................................................................29
FinancialIncentives.................................................................................................................................30
TrainingandSupport ..............................................................................................................................31
PublicReporting......................................................................................................................................33
Accreditation...........................................................................................................................................35
PrimaryHealthcareOrganization/Governance ......................................................................................36
LeadershipDevelopment ........................................................................................................................38
ii ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
ii
Section5:GuidingPrinciplesforQualityImprovementinPrimaryHealthcareinOntario ................... 40
GuidingPrinciples ...................................................................................................................................40
Section6Recommendations............................................................................................................ 42
PerformanceMeasurement.................................................................................................................... 42
PerformanceTargets...............................................................................................................................43
ElectronicMedicalRecords/ElectronicHealthRecords..........................................................................44
PrimaryHealthcareTeams......................................................................................................................46
PatientEnrolment...................................................................................................................................47
PatientEngagement................................................................................................................................47
ResearchandEvaluation.........................................................................................................................48
FinancialIncentives.................................................................................................................................49
TrainingandSupport ..............................................................................................................................49
PublicReporting......................................................................................................................................50
Accreditation...........................................................................................................................................50
PrimaryHealthcareOrganization/Governance ......................................................................................51
LeadershipDevelopment ........................................................................................................................51
Section7:ImplementationPlan ......................................................................................................... 52
ActionPlan ..............................................................................................................................................52
EvaluationPlan........................................................................................................................................54
WorkCitedinReport ......................................................................................................................... 55
AppendixA:TermsofReferenceforImprovingQualityinPrimaryHealthcareinOntario................... 81
AppendixB:Trends............................................................................................................................ 83
AppendixCDefiningQuality,QualityImprovement,QualityAssurance,AccreditationandKnowledgeTransfer ............................................................................................................................................. 90
AppendixDTripleAimFramework................................................................................................... 95
AppendixEHQOQualityAttributes ................................................................................................. 97
iii ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
iii
WorkingGroupMembersBrianHutchisonHealthQualityOntarioSuzanneStrasbergOntarioMedicalAssociationMembersAngelaCarolCollegeofPhysiciansandSurgeonsofOntarioAlbaDiCensoSchoolofNursing,McMasterUniversityMichelleGreiverFamilyPhysician,NorthYorkFamilyHealthTeamJennieHumbertNursePractitioner,WestNipissingCommunityHealthCentreAnjaliMisraAssociationofOntarioHealthCentresMargieSillsMaerovMinistryofHealthandLongTermCareJohnStronksOntarioCollegeofFamilyPhysiciansLynnWilsonDepartmentofFamilyandCommunityMedicine,UniversityofTorontoWorkingGroupLeadandAuthorofReportMonicaAggarwal
iv ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
iv
AbbreviationsAOHC AssociationofOntarioHealthCentresAHRQ AgencyforHealthcareResearchandQualityBSM BlendedSalaryModelCAHPS ConsumerAssessmentofHealthcareProvidersandSystemsCCM ComprehensiveCareModelCHC CommunityHealthCentreCHQI CentreforHealthcareQualityImprovementCIHR CanadianInstituteforHealthResearchCQI ContinuousQualityImprovementCPOE ComputerizedPhysicianOrderEntryCPCSSN CanadianPrimaryCareSentinelSurveillanceNetworkDFLE DisabilityFreeLifeExpectancyDGP DivisionsofGeneralPracticeDHB DistrictHealthBoardsECFAA ExcellentCareforAllActEHR ElectronicHealthRecordEMR ElectronicMedicalRecordFHG FamilyHealthGroupFHN FamilyHealthNetworkFHO FamilyHealthOrganizationFHT FamilyHealthTeamFP FamilyPhysicianGDP GrossDomesticProductGP GeneralPractitionerHALE HealthAdjustedLifeExpectancyHCC HealthCouncilofCanadaHQO HealthQualityOntarioHLE HealthyLifeExpectancyHRA HealthRiskAppraisalICES InstituteforClinicalEvaluativeSciencesIHI InstituteforHealthcareImprovementIOM InstituteofMedicineKT KnowledgeTransferLDL LowDensityLipoproteinLHIN LocalHealthIntegrationNetworkMAS MedicalAdvisorySecretariatMOHLTC MinistryofHealthandLongTermCare
v ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
v
MSAA MasterServiceAccountabilityAgreementsNHS NationalHealthServiceNP NursePractitionerNPLC NursePractitionerLedClinicOECD OrganizationforEconomicCooperationandDevelopmentOHQC OntarioHealthQualityCouncilOHTAC OntarioHealthTechnologyAdvisoryCommitteeOMA OntarioMedicalAssociationP4P PayforPerformancePDSA PlanDoStudyActPEM PatientEnrolmentModelPHO PrimaryHealthOrganizationPHPG PrimaryHealthcarePlanningGroupQA QualityAssuranceQI QualityImprovementQIIP QualityImprovementandInnovationPartnershipQIP QualityImprovementPlanRNPGA RuralandNorthernPhysicianGroupAgreementTQ TotalQualityTQM TotalQualityManagement
1 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
1
ExecutiveSummaryPrimaryhealthcareisthefoundationofCanadashealthcaresystem.Theterm,"primaryhealthcare"referstothehealthprofessionalsandprogramsthatarethefirstpointofcontactforpatients.Effectiveprimaryhealthcareiscommunitybased,promoteshealthylifestylesasameansofpreventingdiseaseandinjury,andrecognizestheimportanceofsocialandeconomicfactorsthatcanaffecthealth(HealthCouncilofCanada,2007).Anexcellentprimaryhealthcaresystemensurestherightcareisprovidedattherighttimeintherightwaybytherightperson.Inthisway,primaryhealthcarecanhelptopreventacuteorchronichealthconditions,shortenthedurationofillnesses,andreducetheriskofcomplications(HealthCouncilofCanada,2007).ImprovingthequalityofprimaryhealthcarehasgainedgrowingattentioninCanada(andinOntario).ArecentCommonwealthFundsupported11countrysurvey(2009)rankedCanadainthebottomthreeamongparticipatingcountrieswithrespecttothepercentageofphysiciansreportingthat:theirpracticehadaprocessforidentifyingadverseeventsandtakingfollowupaction;theyusedelectronicmedicalrecords;theirclinicalperformancewasroutinelycomparedwithotherpractices;theirpracticeroutinelyreceivedandrevieweddataonclinicaloutcomesandpatientsatisfaction/experience;theyroutinelyusedwrittenguidelinestotreatpatientswithasthmaorchronicobstructivelungdiseaseanddiabetes;andtheirpracticehadafterhoursarrangementsforpatientstoseeadoctorornursewithoutgoingtoahospitalemergencyroom.Qualityinprimaryhealthcareisanebulousandmultidimensionalconceptandisdefineddifferentlybydifferentstakeholders.Definingqualitycanbedifficultbecauseprimaryhealthcareisacomplexenvironmentinwhichtherearedifferingneedsbasedonthedemographicsofthecommunityandthegeographicregion.Factorsimportantindefiningqualityinonepopulationmaybelessimportantinothersettings.AhighqualityhealthcaresystemisdefinedinTheExcellentCareforAllActasonethatisaccessible,appropriate,effective,efficient,equitable,integrated,patientcentred,populationhealthfocused,andsafe(HealthQualityOntario,2011).Qualityimprovementisastructuredprocessthatincludesassessment,refinement,evaluationandadoptionofprocessesbyanorganizationanditsproviderstoachievemeasurableimprovementsinoutcomestomeetorexceedexpectations.AlthoughthereareavarietyofqualityimprovementinitiativestakingplaceinOntario,thereisnosystemwideandsustainedapproachestosupportingqualityimprovementinprimary
2 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
2
healthcare.Toaddressthisgap,thePrimaryCareHealthcarePlanningGroup(PHPG)establishedtheQualityWorkingGroupwiththemandatetodeveloprecommendationsontheappropriateapplicationofevidenceinprimarycarepractice,andtoenhancequalityintheprimaryhealthcaresector.Recommendationsweretofocuson:qualityimprovementplanning;trainingandsupport;clinicalandorganizationalbestpracticesandevidenceinformeddeliveryofservices;qualitymeasurementframeworkforprimarycarepractices;and,barriersandenablersofqualityofcare.Toaddressquestionsabouthowtoimprovequalityinprimaryhealthcare,theQualityWorkingGroupreviewed13strategiesandenablersforimprovingquality.Aliteraturereviewwasconductedtodeterminetheimpactdifferentstrategies/enablersmighthaveonthequalityofhealthcare.Insomecases,evidenceregardingtheimpactofspecificinterventionswasfoundtobeconflictingorinsufficient.Recommendationshavebeenpreparedforeachofthe13potentialqualityenablers,informedbyasetofguidingprinciples.Whereevidenceofimpactwasweakorconflicting,theWorkingGrouprecommendationsidentifytheneedtocollectmoredataonwhichtobasequalityimprovementchanges,ortofundresearchandevaluationtogatherdefinitivedataonthesubject.TheWorkingGroupsrecommendationsare:PerformanceMeasurement
Primaryhealthcareperformancemeasurementatthepractice,local,regionalandprovinciallevelsshouldbebasedontheTripleAimFramework(improvedpopulationhealthoutcomes,enhancedpatientexperienceandreduction/controlofpercapitacosts)andtheHealthQualityOntarioattributesofahighperforminghealthsystem(safety,efficiency,effectiveness,personcentredness,timeliness,equity,integration,populationhealthfocus,appropriatelyresourced).
Capacitytomeasureprimaryhealthcareperformanceatalllevelsneedstobedeveloped,drawingonEMR/EHR,administrativeandpatientsurveydata.
Performancemeasurementdatashouldbedisseminatedwidelytodrivechangeandinformdecisionsatthelocalandsystemlevel.
PerformanceTargets
Performanceprioritiesandtargetsshouldbesetmainlyatthepracticeandcommunitylevelstakingintoconsiderationregional/provincial/nationaltargetsifavailable.
Provincialtargetsneedtobecarefullyselectedthroughaprocessofconsultationwithkeystakeholdersandshouldbebasedonshortandlongtermhealthsystemgoals,availablecapacity,evidenceofpotentialforimprovementandhighqualitydata.
3 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
3
ElectronicMedicalRecord/ElectronicHealthRecord
HighqualityprimaryhealthcarerequiresEMRfunctionalityrecommendedbytheAgencyforHealthcareResearchandQualityandtheInstituteforHealthcareImprovement.TheseorganizationsidentifiedthefollowingattributesascriticalelementsofahighlyfunctioningEMR:
ProactivePatientBasedo Allinvolvedinqualityimprovementshouldbeabletoquerythedatao Thesystemshouldsupportinstantaccesstoqueryresultso Thequeryingsystemshouldallowtheusertoaskanyquestiono Usersshouldbeabletoconstructandrunquerieswithouttechnicalassistanceo Usersshouldbeabletospecifytheinclusionofanydataelementsinquerieso Thesystemshouldsupportdrilldownintodatao Usersshouldbeabletosavequeriesforreuseand/orrefinemento Thesystemshouldsupportthesharingofquerieso Thetypesofactiontakenonthelistsofpatientsinaqueryshouldbeflexibleo Theactiontakenonthelistshouldincorporateandusepatientdatatofurther
segmenttheaction(e.g.,HbA1cfollowup)o Thesystemshouldautomatetheactionswheneverpossible
PlannedCareforIndividualPatientsThewholepatientshould:
o bedisplayedinoneplaceo bedynamico beusedforplanning,treatmentandfollowupo supportcareacrossallconditionsandhealthissues,notjustthecomplaint
associatedwithaparticularencountero bethecentrallocationforotherviewsofpatientdata,suchasrunchartsof
laboratoryresultsandvitalso incorporateevidencebasedpromptsandreminderso provideaportalforthepatientforbothinputandviewingdata,givingthepatient
somecontroloverhis/herrecordMeasurement
o Themeasurementmoduleshouldallowtheusertocustomizeanyreportbyaddingorchangingafilter
o Thequeryandfilterstructuresformeasurementandreportingshouldbeidenticaltothoseusedforthepopulationbasedcaretoolandforremindersandprompts
4 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
4
Othero Abilitytocustomizethedatapresentedo Easeofuseo Interoperabilityo Dataavailableacrossthecontinuumofcareo Appropriatedatastructuresprovideinformationthatsupportsimprovemento Automation
Commondatastandards,capacityfordatasharing,andappropriatetrainingand
supportforprovidersinmeaningfuluseofEMRsneedtobedevelopedandimplemented.
PrimaryHealthcareTeams
Continueexpandingthenumberofcollaborativeinterprofessionalprimaryhealthcareteams.Teamsshouldvaryinsize,compositionandorganizationalstructuretomeetlocalcommunityneeds.
Interprofessionalcollaborativepracticeopportunitiesthatareconsistentwiththeneedsofthepopulationbeingservedbemadeavailabletoallprimaryhealthcaremodelsregardlessoffundingorproviderpaymentmethods.
Supportcoordination,collaborationand/orintegrationofprimaryhealthcareteams/practiceswithothercommunityhealthandsocialservicestoallowforeffectiveandefficientpatientnavigationthroughthehealthcaresystem.
Toachieveefficienciesandimprovedoutcomes,teammembersshouldfunctionattheirlevelofcompetency,focusingonthepatientsneedsandrecognizingtheimportanceofcontinuityinbuildingtrustingproviderpatientrelationships.
PatientEnrolment
Formalpatientenrolmentreenforcespatientproviderrelationshipsandresponsibilitiesandisfoundationaltoproactive,populationbasedpreventivecareandchronicdiseasemanagementandtosystematicpracticelevelperformancemeasurementandqualityimprovement.OntarioshouldcontinuethespreadofPatientEnrolmentModels.
PatientEngagement
Patientengagementintheformofbothpatientselfmanagementandpatientinvolvementinservicesdesignandplanningiswidelybelievedtobeacriticaldriverofqualityimprovementinprimaryhealthcare.Moreinformationfromevaluativestudiesonthebestapproachestoengagingpatientsisrequired.
5 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
5
ResearchandEvaluation
Acontinuingflowofresearchandevaluationtoinformprimaryhealthcarepolicyandpracticeisanessentialunderpinningofahighperformingprimaryhealthcaresystemandneedstobesupportedbyadequatefundingofresearch,evaluationandresearchtraining.
Specificareasrequiringfocusedevaluationinclude:approachestopatientengagement,approachestoqualityimprovementtrainingandsupport,costsandbenefitsofprimarycareaccreditation,physicianversusteambasedincentives.
Promisingbutuntriedqualityrelatedinnovationsshouldbeimplementedandevaluatedonasmallscalepriortosystemwideimplementation.
FinancialIncentives
Giventheambiguityofcurrentevidenceandthepotentialforperverseeffectsofpayforperformance(P4P)inprimaryhealthcare,primarycareP4Pincentivesshouldbepursuedwithcautionandbecarefullyevaluated.
TrainingandSupport
Qualityimprovementtrainingandsupportshouldbemadeavailableovertimetoallprimarycareprovidersandorganizations.
Qualityimprovementtrainingshouldbeembeddedinallhealthcareprofessionaltrainingprograms.
PublicReporting
Publicreportingofprimaryhealthcareperformanceattheregionalandprovinciallevelsshouldtrackchangesovertimeandincludecomparisonacrossregions,takingdifferencesinpopulationcharacteristicsintoaccount.
Mandatorypublicreportingofperformanceisnotrecommendedforprimarycarepracticesand/ororganizations.
Accreditation
Primaryhealthcareaccreditationisapotentialdriverofquality.However,evidenceoflastingimpactisrequiredbeforeadefinitiverecommendationcanbemade.Asynthesisofinternationalexperiencewithprimaryhealthcareaccreditationandtheevidence
6 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
6
regardingitsimpactiscurrentlyunderwayundertheauspicesoftheCanadianHealthServicesResearchFoundationandshouldinformfuturedecisionmaking.
PrimaryHealthcareOrganization/Governance
Localprimaryhealthcareprovidernetworksthatengagepatientsandthepubliccouldplayakeyroleinpromoting,supportingandcoordinatingqualityimprovementinitiativesandinsharingqualityimprovementexpertiseandexperienceamonglocalproviders.
LeadershipDevelopment
Createprogramstosupportthedevelopmentofqualityimprovementleadershipcapacityamongprimaryhealthcarecliniciansandadministrativestaff.
7 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
7
Section1:Background
DevelopmentandEstablishmentofthePrimaryHealthcarePlanningGroupInJuneof2010,theMcMasterHealthForumheldadialoguewithavarietyofparticipants1onthetopicofSupportingQualityImprovementinPrimaryHealthcareinOntario.Atthisforum,dialogueparticipantsagreedthatOntariolacksasystemwideandsustainedapproachtosupportingqualityimprovementinprimaryhealthcare.ItwasdeterminedthatanoverarchingframeworkforstrengtheningprimaryhealthcareinOntariowasrequired.ForumparticipantsconcludedthatasmallplanninggroupshouldbeestablishedwithamandatetodraftandbuildconsensusonastrategyforstrengtheningprimaryhealthcareinOntario,andtoorganizeasummitatwhichthestrategywouldbedebated,finalizedandapprovedbyabroadbasedgroupofkeystakeholders.ThePrimaryCareHealthcarePlanningGroup(PHPG)wasestablishedandincludedrepresentativesfromtheMinistryofHealthandLongTermCare(MOHLTC),OntarioMedicalAssociation(OMA),RegisteredNursesAssociationofOntario(RNAO),OntarioCollegeofFamilyPhysicians(OCFP)andAssociationofOntarioHealthCentres(AOHC).ThePHPGrecommendedthatfiveworkinggroupsshouldbecreatedtoaddressquality,access,efficiency,accountabilityandgovernancetoinformtheapproachforstrengtheningprimaryhealthcareinOntario.
MandateoftheQualityWorkingGroupInAprilof2011,theQualityWorkingGroupwasestablishedtoproviderecommendationsontheappropriateapplicationofevidenceinprimarycarepracticeandonenhancingqualityintheprimaryhealthcaresector(RefertoAppendixAfortheTermsofReference).ThekeyareasoffocusforthisWorkingGroupincluded:
Qualityimprovementplanning,trainingandsupportintheprimaryhealthcaresector Clinicalandorganizationalbestpracticesandevidenceinformeddeliveryofservices Qualitymeasurementframeworkforprimarycarepractices Barriersandenablersofqualityofcare
1Participantsincludedrepresentativesfromthe:GovernmentofOntario,stakeholderorganizations(e.g.,OntarioMedicalAssociation(OMA),OntarioCollegeofFamilyPhysicians(OCFP),RegisteredNursePractitionersAssociationofOntario(RNAO),AssociationofOntarioHealthCentres(AOHC),AssociationofFamilyHealthTeamsofOntario,DietitiansofCanada),LocalHealthIntegrationNetworks(LHINs),QualityImprovementandInnovationPartnership(QIIP),CancerCareOntario(CCO),regulatorybodiesandacademics.
8 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
8
TheWorkingGroupwascomposedofrepresentativesfromacademicandresearchinstitutions,professionalassociations,regulatorycolleges,providersandothersystemleaders.TheCoChairsoftheQualityWorkingGroupwereDr.BrianHutchisonandDr.SuzanneStrasberg.
9 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
9
Section2:TrendsandCurrentStateofQualityImprovementinPrimaryHealthcareinOntarioandtheChangeImperative
CurrentStateofPrimaryCareinOntarioCanadaspends10.4%ofitsgrossdomesticproduct(GDP)onhealthcare(OrganizationforEconomicCooperationandDevelopment,2010).ThisishigherthantheOrganizationforEconomicCooperationandDevelopment(OECD)averageof9.0%.TheCanadianphysiciantopopulationratio(2.3per1,000population)isbelowtheOECDaverage(3.2per1,000).However,thegeneralpractitionertopopulationandnursetopopulationratiosareabovetheaverageformembercountriesoftheOECD(OECD,2010).Familyphysicians(FPs)makeup51%ofthephysicianworkforceinCanada(CIHI,2010).InApril2010,therewere25,886activephysiciansinOntario.Ofthesephysicians,approximately11,550weregeneralpractitioners(GPs)/familyphysicians.OftheGPs/FPs,approximately7,700(67%)wereaffiliatedwithapatientenrolmentmodel(PEM);15001600(1314%)werecomprehensivecareprimarycarephysiciansremuneratedthroughstraightfeeforservice(FFS);andtheremainder(approximately23002800;2024%)wereinfocusedorparttimepractice(ICESandOMA,personalcommunication,May2011).AccordingtotheHealthQualityOntario(HQO)report(2011),93.5%ofOntarianshadafamilydoctor.AsofJune2011,theMinistryofHealthandLongTermCare(2011)reportedthatover9.5millionOntarioresidentswereenrolledtoreceivecarefrom709PEMs.The709PEMsincluded:362FamilyHealthOrganizations(FHOs)(with3,631physicians);238FamilyHealthGroups(FHGs)(with3,003physicians);38RuralandNorthernPhysicianGroupAgreements(RNPGA)(with93physicians);36FamilyHealthNetworks(FHNs)(with346physicians);21BlendedSalaryModel(BSM)(with74physicians);14othergroups(with222physicians);and305physiciansintheComprehensiveCareModel(CCM).AsofAugust2011,therewillbe200FamilyHealthTeams(FHTs)with2,000physiciansandover1,500interprofessionalhealthcareprovidersserving2.5millionenrolledpatients(MOHLTC,personalcommunication,July2011).Inaddition,thereare300GPsandNPsin73CommunityHealthCentres(CHCs)serving367,216patients(AOHC,personalcommunications,July2011).ThereareeightNursePractitionerLedClinics(NPLCs)invariousstagesofimplementationandanadditional18clinicsthatwillbeimplemented.Over5,000OntarioresidentsareregisteredwithaNPLCtoreceiveprimaryhealthcare.Approximately6.5%ofOntariansdonothaveaccesstoafamilydoctor(HQO,2011).Ofthese,overhalfareactivelylookingforanFPbutcannotfindone(HQO,2011).TheseOntarianstendtohavelowerincomesandtobefromthenorthernregions(HQO,2011).ThereareregionaldisparitiesinthepercentageofOntarians
10 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
10
withafamilydoctor.ThisvariesbyLHINfrom85.8%intheNorthEastLHINto98.1%intheSouthEastLHIN(MOHLTC,2010).
CurrentStateofQualityinCanadaandOntario
CanadaRelativetoOtherCountriesandOntarioCanadahasparticipatedinaseriesofbenchmarkingsurveysthatareconductedbytheCommonwealthFundtotracktrendsinprimarycare.Surveysareconductedannually,providingameanstocomparepracticesandtrendsovertime,andtobenchmarkagainstothercountries.Keyindicatorshavebeendevelopedthatallowperformancetobecomparedbetweenparticipatingcountriesandtoleveragethedataforongoinghealthcareplanning.Surveysofprimarycarephysiciansin2009andadultsin2010showedthatCanadaisperformingwellonsomedimensionsofqualityanddoingpoorlyonothers.Inmostcases,Canadahasbeenmakingprogresswithimprovingscoresonkeyindicatorsofqualityexceptforsafety,efficiencyandaccessibility(RefertoAppendixBfordetailedinformationontrends).Canadaisachievinghighscoresonindicatorsrelatedtoqualitydimensionssuchaseffectiveness(chronicdiseasemanagement),focusonpopulationhealth(preventivecare),patientcentredness(communication)andsomeelementsofefficiency.ThesurveyofCanadianadultsindicatedthatCanadatrailedthetopperformingcountriesonlyslightlyinpreventivecare(exceptPapsmears)andchronicdiseasemanagement.CanadarankedinthetopthreecountrieswithrespecttothepercentageofCanadiansreportingthattheydiscussedattheirregularplaceofcareahealthydietandhealthyeating(52%),exerciseorphysicalactivity(56%)andthingsintheirlifethatworriedthemorcausedthemstress(44%).ComparedtoCanada,Ontarioscoredbetterinthepercentageofpatientswithhypertensionthatobtainedbloodpressureandcholesterolchecksandthepercentageofpatientswithasthma,diabetes,heartdisease,hypertension,highcholesterolthatreportedbeingveryconfidentintheirabilitytocontrolandmanagehealthproblems.AlthoughCanadaisdoingwellinrelationtoothercountriesonchronicdiseasemanagementandprevention,theHQOidentifiesroomforimprovement.The2011HQOannualreportnotedthatonlyhalfofOntarianswithdiabetespatientshavetheireyesandfeetexaminedwithintherecommendedtimeintervalsandslightlyfewerthanhalfaregettingthemedicationtheyneed.TheHQOalsosuggeststhatOntarioneedstodobetterinprevention.Therateofobesityhasincreasedfrom16%to18%overthepasteightyears;andoneinfiveCanadiansissmoking(HQO,2011).Furthermore,onethirdofwomenaged50to69didnothaveamammograminthepasttwoyears;oneinfouradultwomendidnothaveaPaptestinthelastthreeyears;andoneinfiveelderlywomendidnotgetscreenedforosteoporosis.
11 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
11
TheCommonwealthsurveyssuggestthatthesystemisperformingwellforsomeindicatorsofefficiencywith89%ofCanadianadultsreportingin2010thattheycouldnotrememberatimewhentheirtestresultsinformationwasnotavailableatthetimeoftheirappointmentand92%reportingthatduplicatetestswerenotdone(thishasslightlydeclinedfrom95%in2007).Withrespecttopatientcentredcare:themajorityofCanadianadultsgavehighscorestotheirregulardoctorsoncommunication:85%reportedthattheirregulardoctoralways/oftengivesthemanopportunitytoaskquestionsaboutrecommendedtreatment;89%reportedthattheirregulardoctorexplainsthingsinawaythatiseasytounderstand;83%reportedthattheirdoctorinvolvesthemasmuchastheywantincaredecisions;and80%reportedtheirdoctorspendsenoughtimewiththem.AlmostthreequarterofCanadians(74%)whoreceivedcareinthelastyearreportedthatthequalityofcaretheyreceivedfromtheirregulardoctorwasverygoodorexcellent.Canadaachievedlowerscoresonindicatorsrelatedtoqualitydimensionssuchas;appropriatelyresourced,accessibility,patientcentredcare,safety,equity,andeffectiveness.Physiciansreportedlowratesfor:theadoptionofinformationsystems;adoptionofinterprofessionalhealthcareprovidersinthehealthcaredeliveryteam;providingchronicallyillpatientswithwritteninstructions;providingpatientswithawrittenlistofmedicationsformanagingcare;and,accesstoafterhourarrangementsforpatients.OntarioperformedbetterthantheCanadianaverageintheuseofhealthinformationtechnology/officesystemsandintegrationofinterprofessionalhealthcareproviders.Canadianadultsreportedlowratesforconfidenceintheirabilitytomanagetheircareandrelativelyhighratesof:adversehealthcareincidentssuchasmedicationerrors;mistakesintreatment;incorrectdiagnosticorlaboratorytestresults;and,difficultyobtainingaccesstoprimarycarewhentheyweresick.TheHQO(2011)reportedthatthesystemisnotcompletelyequitablesinceCanadianswithlowincomesorpooreducationareathigherriskofunhealthybehavioursandnotgettinghealthpreventionservices.Forexample,lowerincomeOntariansare36%morelikelytoexperienceanacutemyocardialinfarctionandhavea32%higherrateofinjuryrelatedhospitalizationcomparedtothehighestincomeOntarians.InthemostrecentCommonwealthFundsurveys(2009;2010),Canadarankedinthebottomthreeamongallparticipatingcountrieswithrespecttothefollowingindicators:
percentageofphysiciansreportingthattheirpracticehasaprocessforidentifyingadverseeventsandtakingfollowupaction(10%);thisdeclinedfrom20%in2006
percentageofphysiciansusingelectronicmedicalrecords,whichenablesperformancemeasurementandfeedback(37%)
12 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
12
percentageofphysiciansreportingthattheirclinicalperformancewasroutinelycomparedwithotherpractices(11%)
percentageofphysiciansreportingthattheirpracticeroutinelyreceivesandreviewsdataonclinicaloutcomesofpatientcare(17%)andpatientsatisfaction/experience(15%)
percentageofphysiciansthatreportedtheroutineuseofwrittenguidelinestotreatasthmaorchronicobstructivelungdisease(76%)anddiabetes(82%)
percentageofphysiciansreportingthattheirpatientsoftenhavedifficultygettingspecializeddiagnostictests(47%)
percentageofphysiciansreportingthattheirpatientsoftenfacelongwaitingtimestoseeaspecialist(75%)
percentageofphysiciansreportingthattheirpracticehasanafterhoursarrangementtoseeadoctorornursewithoutgoingtoahospitalemergencyroom(43%);thishasdeclinedfrom47%in2006(Netherlandswith97%)
percentageofCanadiansthatreportedthatitwasveryeasytocontacttheirdoctor'spracticebyphoneduringregularpracticehours(26%)
percentageofCanadiansthatreportedobtaininganappointmentthesamedaywhensick(28%)
PreventiveCareBonuses
FPs/GPsinPEMsareentitledtoreceivingfinancialincentivesformeetingestablishedthresholdlevelsforperformingpreventivecareactivities.Theamountofthepreventivecarebonusvariesbasedonthelevelofthresholdachieved.Ananalysisoftheuptakeofthefinancialincentivesforinfluenzavaccine,Papsmear,mammogramandchildhoodimmunizationconsistentlyindicatesthatthedistributionisbimodal,withmostphysiciansclaimingattheextremeendsofthethresholdscaleratherthaninthemiddle(MOHLTC,2011).Thisrangedfrom:
37%ofphysiciansbillingnothing(0%)and36%ofphysiciansbillingforthemaximumthreshold(80%)fortheinfluenzavaccine
32.5%ofphysiciansbillingnothing(0%)and45%ofphysiciansbillingforthemaximumthreshold(80%)forPapsmears
29%ofphysiciansbillingnothing(0%)and53%ofphysiciansbillingforthemaximumthreshold(75%)formammograms
31%ofphysiciansbillingnothing(0%)and62%ofphysiciansbillingforthemaximumthreshold(95%)forchildhoodimmunization
13 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
13
ThesetrendsindicatethatmorephysiciansarereachingthemaximumthresholdforthemammogramandchildhoodimmunizationincentivecomparedtothePapsmearandinfluenzaincentive.ThecolorectalscreeningbonuswasmostwidelyadoptedbyPEMphysicians.Thedistributionforthisincentivewasskewedtowardstheright(thatis,towardsthehighestendoftherange)withmoreconcentrationaroundthemean.Theuptakeoftheincentiverangedfrom:26%ofphysiciansbillingnothing(0%);2%meetingthe15%threshold;8.3%meetingthe20%threshold;8.2%meetingthe40%threshold;21%meetingthe50%threshold;13%meetingthe60%threshold;and21%ofphysiciansbillingforthemaximumthreshold(70%).ThereisgreatvariationamongPEMswithrespecttotheuptakeofeachpreventivecareincentive.However,aconsistenttrendamongalltheincentivesisthatphysiciansintheRNPGAmodelwerethemostlikelytobillnothingforeachincentive;FHOsweresecond;CCMswerethird;FHGswerefourthandFHNswerefifth.PhysiciansinFHNswerethemostlikelytobillforthemaximumthresholdforeachincentive;FHGsweresecond;FHOswerethird;CCMswerefourth;andRNPGAswerefifth.
CurrentStateofQualityImprovementInitiativesinOntarioFederalandprovincialgovernmentsinCanadahaveinvestedinimprovingthequalityoftheprimaryhealthcaresectorthroughavarietyofinitiatives(McMasterForum,2010).Federalinitiativesinclude:
InvestinginaPrimaryHealthCareTransitionFundtosupporttargetedqualityimprovementpilotprojectsbetween2000and2006
EstablishingCanadaHealthInfowaytosupportthedevelopmentofelectronichealthrecords(EHRs)
Provincialinitiativesinclude:
EstablishingtheOntarioHealthQualityCouncil(OHQC)in2005tomonitoraccessandoutcomesandsupportcontinuousqualityimprovementinOntarioshealthcaresystem
Introducingfinancialincentivesforpreventionandchronicdiseasemanagementincomprehensivecaremodels
Fundingandsupportingtheadoptionandimplementationofelectronicmedicalrecords(EMRs)throughOntarioMDandeHealthOntario
Fundingaprimaryhealthcare'atlas'bytheInstituteforClinicalEvaluativeSciences(ICES)anddecisionsupporttoolsbytheCentreforEffectivePractice
EstablishingtheQualityImprovementandInnovationPartnership(QIIP)in2007toleadtheadvancementofqualityimprovementinprimaryhealthcare
14 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
14
Fundinginitiativestargetedtospecificgroups(e.g.,PrimaryCareAsthmaProgram,ProvincialPrimaryCareCancerNetwork)
EstablishingaccountabilityframeworksbetweenLocalHealthIntegrationNetworks(LHINs)andCHCs
CommissioningoftheMcMasterForumbyQIIPwithfundingfromtheMOHLTCtoconductanenvironmentalscanandestablishacapacitymapbyexaminingthenatureandextentofqualityimprovementactivitiesinprimaryhealthcareinOntario,andtocompleteasynthesisofsystematicreviewsonevidenceabouttheeffectivenessofqualityimprovementinterventionsinprimarycare.Thisworkinformedthedevelopmentofanissuebriefwhichwasusedtofacilitateastakeholderdialogueonqualityimprovementinprimaryhealthcare.
InJune2010,themandateoftheOHQC(nowHealthQualityOntario(HQO))wasexpandedbythegovernmentsExcellentCareforAllAct(ECFAA).Asaresult,HQOhasintegratedtheCentreforHealthcareQualityImprovement(CHQI),QIIP,theMinistryofHealthandLongTermCaresMedicalAdvisorySecretariat(MAS),theOntarioHealthTechnologyAdvisoryCommittee(OHTAC)andtheTechnologyEvaluationFundtoformasingleorganizationwiththeresponsibilityto:coordinate,consolidateandstrengthentheuseofevidencebasedpracticeinitiativesandtechnologies;supportcontinuousqualityimprovement;andcontinuetomonitorandpubliclyreportonhealthsystemoutcomes(HQO,2011).Thelegislationrequiresthateveryhealthcareorganization(currentlydefinedasahospitalwithinthemeaningofthePublicHospitalsAct)(HQO,2011):
Establishaqualitycommitteetoreportonqualityrelatedissues Developanannualqualityimprovementplanandmakeitavailabletothepublic Linkexecutivecompensationtotheachievementoftargetssetoutinthequality
improvementplan Conductpatient/careprovidersatisfactionsurveys Conductstaffsurveys Developapatientdeclarationofvaluesfollowingpublicconsultation,ifsucha
documentisnotcurrentlyinplace,and Establishapatientrelationsprocesstoaddressandimprovethepatientexperience.
AnenvironmentalscancommissionedbyQIIPonqualityimprovementinitiativesinOntarioshowedthatqualityimprovementprogramsinOntariosphysicianledprimaryhealthcarepracticesarefragmentedandlimitedincoverage(McPhersonetal,2010).Thescanidentified24distinctprogramsinwhichthefocusvariedfromdiseaseorcondition,team,organization,region,sector,orapproach.Onlyafewprogramshadafocusonqualityimprovement.Manyoftheprogramswerepilotswithnoclearindicationoftheirpossiblefitintoasystemwideandsustainedapproachtosupportingqualityimprovementinhealthcare.Incommunitygoverned
15 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
15
healthcareorganizations,16distinctprogramswereidentified.Manyoftheseprogramsintersectedwithqualityimprovementbutwerenotspecificallyfocusedonit.Forthesereasons,Ontariorequiresasystemwideandsustainedapproachtosupportingqualityimprovementinprimaryhealthcare.
16 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
16
Section3:TerminologyAssociatedWithQuality
DefiningQuality,QualityImprovement,QualityAssurance,AccreditationandKnowledgeTransferTheExcellentCareforAllActdefinesahighqualityhealthcaresystemas:accessible,appropriate,effective,efficient,equitable,integrated,patientcentred,populationhealthfocused,andsafe(HQO,2011).TheMOHLTC,throughtheExcellentCareforAllStrategyhasindicateditscommitmenttoleveragingallnineoftheseattributestoadvancequalityinitiativesacrosstheprovince.Inthefallof2010,aworkinggroupwasformedtoprovideadvicetotheMOHLTCaroundthedesignofQualityImprovementPlans(QIPs).Theconsensuswasthatwhileallnineattributesarevaluable,theQIPsshouldspecificallyfocusonfourofthemforstreamlinedprovincialandpublicreporting:
Safe Effective Accessible PatientCentred
AnexaminationoftheliteratureindicatesthatthereisnouniversallyaccepteddefinitionofQualityImprovement(QI),asitrelatestoprimaryhealthcare.QualityImprovement,ContinuousQualityImprovement(CQI),TotalQuality(TQ),TotalQualityManagement(TQM),andContinuousImprovement(CI)aretermsthatareoftenusedinterchangeably.QIinvolvesastructuredprocessthatincludesassessment,refinement,evaluationandadoptionofprocessesbyanorganizationanditsproviderstoachievemeasurableimprovementsinoutcomestomeetorexceedexpectations(RefertoAppendixC).ThefundamentalconceptunderlyingQIisthatinordertoachieveanewlevelofperformance,thesystemneedstochange.QIemphasizeschangesinprocessesandsystemsofhealthcaredeliveryandmeasurestheimpactofthosechanges.RepeatingtheseprocessescontinuouslytoimprovequalityoutcomesisCQI.QIinitiativescantargetpatients,families,staff,healthprofessionalsandthecommunity.QualityAssurance(QA)activitiesareintendedtoprovideconfidencethatqualityrequirementsarebeingmet.QAinvolvesmeasurementofperformance,usuallyagainstpredefinedstandardsorbenchmarks,andoftenfocusesonidentifyingdeficienciesoroutliers.Qualityassuranceactivitiesmaybeinternaltoanorganizationorconductedbyanexternalagency.Qualityassurancemayormaynotincludeprocessestoaddressidentifiedshortcomings.Inpractice,someprogramslabelledqualityassuranceincorporatetheessentialfeaturesofqualityimprovement.
17 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
17
Accreditationisarigorousexternalevaluationprocessthatcomprisesselfassessmentagainstagivensetofstandards,anonsitesurveyfollowedbyareportwithorwithoutrecommendations,andtheawardorrefusalofaccreditationstatus(Pomeyetal.,2010).InCanada,accreditationisvoluntaryexceptforFirstNationsfacilities,universityaffiliatedhospitalsandinstitutionsinQuebec.AccreditationCanadaisanationalnonprofitorganizationthatwasestablishedtoguaranteethathealthcareorganizationsinCanadaprovideservicesofacceptablequality.Thisorganizationfollowsinternationalaccreditationprotocolsfortheselfassessmentofhealthcareorganizationsagainstagivensetofstandardsdeterminedbyprofessionalconsensus.Anonsitesurveyisconductedandfollowedbyareportwithorwithoutrecommendationsandtheawardorrefusalofaccreditationstatus.AccreditationCanadahasdevelopedandpilottestedprimaryhealthcareaccreditationstandards.AccreditationisoneofmanypotentialQAactivities.AkeydifferencebetweenQAandaccreditationisthataccreditationofanorganizationtakesplacethroughathirdpartywhereasQAcantakeplaceinternallybyahealthcareorganizationorexternallybyathirdparty.Knowledgetranslation(KT)isarelativelynewtermcoinedbytheCanadianInstitutesofHealthResearch(CIHR)in2000.CIHRdefinedKTas"theexchange,synthesisandethicallysoundapplicationofknowledgewithinacomplexsystemofinteractionsamongresearchersanduserstoacceleratethecaptureofthebenefitsofresearchforCanadiansthroughimprovedhealth,moreeffectiveservicesandproducts,andastrengthenedhealthcaresystem"(CIHR,2005).Inaclinicalsetting,KTcanbedefinedastheeffectiveandtimelyincorporationofevidencebasedinformationintothepracticesofhealthprofessionalsinsuchawayastoeffectoptimalhealthcareoutcomesandmaximizethepotentialofthehealthsystem.KTinterventionsinclude:educationalinterventions(large,smallgroupsessions;continuingmedicaleducation;selfdirectedlearning);linkageandexchangeinterventions(knowledgebrokers,opinionleaders,educationaloutreachvisits);auditandfeedback;informaticsinterventions(education,remindersystems,clinicaldecisionsupportsystems,presentingandsummarizingdata);andpatientmediatedinterventions(selfcareandchronicdiseasemanagement)(Straussetal.,2009).KTinformsthecontentofQIprograms.KTinterventionsandstrategiescanbeusedtofacilitateQI.
18 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
18
Section4:StrategiesandEnablersofQuality:ALiteratureReviewTheliteratureidentifiesavarietyofpotentialenablersandstrategiesforqualityimprovement.Toinformrecommendationsforimprovingqualityinprimaryhealthcare,aliteraturereviewandanalysisforeachstrategywascompletedandissummarizedinthissection.
PerformanceMeasurementPerformancemeasurementistheprocesswherebyanorganizationestablishestheparametersbywhichprogramsandservicesaremeasuredanddetermineswhetherdesiredoutcomesarebeingachieved.Performancemeasurementisimportanttoqualityimprovementsinceitallowsfor:theidentificationofopportunitiesforimprovement;trackingprogressagainstorganizationalgoals;andcomparingofperformanceagainstbothinternalandexternalstandards.InOntario,currentinitiativesincludetheQIIP/HQOICESprojectinwhichhealthadministrativedatawillbeprovidedtoprimaryhealthcarepracticesparticipatingintheQIIP/HQOLearningCommunity.Thisinformationincludes;demographicandhealthcharacteristicsofthepracticepopulation,provisionofpreventivecare,chronicdiseasemonitoring,ERvisits,specialistreferrals,admissionratesforambulatorycaresensitiveadmissionsandspecificchronicdiseases,andhospitalreadmissionrates.CIHIhasaVoluntaryReportingSystemthroughwhichFPssubmitandreceivefeedbackbasedontheirEMRdata(CIHI,2011).TheCIHIprovidesparticipatinghealthcarepractitionerswith:informationandtools(qualityimprovement,patientcentricproviderfeedbackreports)toimprovequalityofpatientcareandpracticemanagement;aforumbywhichparticipatingPHCclinicianscancollaborateonqualityimprovementandPHCresearch;theabilitytogeneratenewinformationinpriorityareas,suchasaccesstocare,quality,utilizationandoutcomestosupporteffectivepolicydevelopmentandhealthsystemmanagement;and,insightonhowtomakeEMRsmoreusefulforpractitioners.TheCanadianPrimaryCareSentinelSurveillanceNetwork(CPCSSN)providesongoingfeedbackbasedondataextractedfromtheEMRstoparticipatingprimarycarepracticesontheirperformanceandtheirEMRdataquality.CPCSSNisaCanadawideEMRbasedresearchsystemwhichisfocusedonchronicdiseasepreventionandmanagement.ItmakesuseofepidemiologyandpracticebasedprimarycaredatafromFPsandnursepractitioners(NPs).Theprovidersindividualresultsarecomparedtolocalandnationalbenchmarkdata(CPCSSN,2011).
19 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
19
Theaccountabilityagendahasstressedtheimportanceofusingmeasurableindicatorsofperformancemeasurement(EmanuelandEmanuel,1996;RiesandCaulfield,2004;Segsworth,2003;AucoinandJarvis,2005;Brown,Porcellato,Barnsley,2006).Performancemeasuresshouldbe:clinicallyrelevant;scientificallysoundandtestedbeforeimplementation;feasibletocollect;capableofshowingimprovementovertime;designedandagreedonbyallstakeholderstopreventgaming;andalignedwithnationalmeasures(whenfeasible).Inestablishingperformancemeasuresforqualityimprovementitisalsoimportanttoconsider:crowdouteffectsonotheractivitiesthatmaynotreceiveattentionifcertainmeasuresareemphasized;downstreameffectsoftheprogramonotherhealthcareuse(e.g.,increasedvolumeoftesting,resourcesrequiredtotreatadditionalidentifiedcases);thetemptationtoselectactivitiesthatarerelativelyeasytomeasureratherthanmoreimportantonesthataredifficulttomeasure(MOHLTC,2007).Tobemeaningful,performancemeasurementdatamustbe:timely;consistent;andthemeaningofthedatamustbeunderstood.Welldefined,validlymeasuredperformancedatacanbecomparedbetweenhealthcareorganizationsandprovidersanddisseminatedtoinformdecisionsatthelocalandsystemlevel.
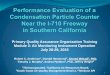
TripleAimFrameworkInCanada,thehealthcaresectorisincreasinglyembracinganewqualityimprovementframeworkreferredtoastheTripleAimFramework.ThisqualityimprovementmodelwasdevelopedbytheInstituteforHealthcareImprovement(IHI),anotforprofitorganizationlocatedinCambridge,Massachusetts.Theconceptdesignstartedin2005andhasbeenadoptedbyabroadrangeofhealthcareorganizationsinNorthAmericaandinternationallysince2007.TheOntarioLHINshaveadoptedtheTripleAimFrameworkasameansofimplementingandtrackingprogresswithhealthcareimprovementinitiatives(Loucks,2011).TheTripleAimFrameworkfocusesonthreeobjectives(the"TripleAim"):
Improvethehealthofthepopulation Enhancethepatientexperienceofcare(includingquality,accessandreliability) Reduce,oratleastcontrol,thepercapitacostofcare
20 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
20
Figure1TripleAimFramework(InstituteforHealthcareImprovement)AnexampleofasuccessfulTripleAiminitiativecitedbyBeasley(2011)involvedredefiningthewaycarewasprovidedbyalternativehealthcareworkers.Byinvolvingalternatehealthcareworkersandschedulinglonger,lessfrequentclinics,itwaspossibletoimprovepatientaccess,patientsatisfactionandreducethecostofprovidingcaretoafractionoftheoriginalcosts.Berwicketal.(2008)describedfivecomponentsoftheTripleAimframework:individualsandfamilies;definitionofprimarycare;preventionandhealthpromotion;percapitacostreduction;andintegration,socialcapitalandcapabilitybuilding(RefertoAppendixDformoredetails).TheIHITripleAimteamhasputtogetherasetofsuggestedmeasuresthatalsohelptooperationallydefinetheTripleAim.SomeexamplesofcriteriathatrelatetoPopulationHealthinclude:healthylifeexpectancy(HLE):lifeexpectancycombinedwithhealthstatus(e.g.,healthadjustedlifeexpectancy(HALE),disabilityfreelifeexpectancy(DFLE));mortality:lifeexpectancy,yearsofpotentiallifelost,standardizedmortalityrates;healthstatus:singlequestionormultidomainhealthstatus(e.g.,SF12,EuroQol);compositehealthriskappraisal(HRA)score;diseaseburden(e.g.,summaryoftheprevalenceofcertainconditions,summaryofpredictivemodelscores,hospitalandEDutilizationforambulatorycaresensitiveconditions).Examplesofcriteriathatrelatetopatientexperienceinclude:standardquestionsfrompatientsurveys(e.g.,U.S.ConsumerAssessmentofHealthcareProvidersandSystems(CAHPS)or
21 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
21
HowsYourHealthglobalquestions,NationalHealthService(NHS)WorldClassCommissioningorHealthcareCommissionexperiencequestions,likelihoodtorecommend);andsetofmeasuresbasedonkeydimensions(e.g.,U.S.InstituteofMedicine(IOM)dimensions).Examplesofindicatorsofpercapitacostmightinclude:costpermemberofthepopulationpermonth;or,costsinhighvolume/costcategories(e.g.,secondarycare).Berwicketal.(2008)believethatcertainpreconditionsmustbeinplacebeforehealthcareorganizationscanpursuetheTripleAimframework.Theorganizationorsystemmustrecognizetheneedtodealwiththehealthoftheentirepopulationnotjustindividualpatients.Theremustbeconstraintsonthefinancesavailableortheneedtoprovideanequitablehealthcaredeliverysystem,andtheremustbeanintegratorabletocoordinateservicesandfocusonpopulationhealth,patientexperience,andpercapitahealthcaresimultaneously.TheTripleAimFrameworkincludesrolesforMacroandMicroIntegrators.MacroIntegratorsareorganizationsorgroupsoforganizationsthatmanageresourcestosupportadefinedpopulation(e.g.,aLHIN).MacroIntegratorsworkwithfrontlineserviceprovidersandsystemsthatsupportindividuals.AMicroIntegratorisanindividualorteamthatdeliversthebestormostappropriatecaretoanindividual.AMicroIntegratorcouldbeahealthcareprofessional,orteamofhealthcareprofessionalsresponsiblefordeliveringhealthcare.AprimarycarepracticeororganizationwithanenrolledpatientpopulationcanserveasbothaMacroandMicroIntegrator.KeyindicatorstomeasureandtrackperformanceandongoingqualityimprovementfocusononeormoreoftheTripleAimfoci.Theseindicatorsareusedtomeasurebaselineperformancepriortochangesbeingintroduced,andatvariousperiodsduringandafterachangeismadetodeterminetheextentoftheimprovement,andwhethertheimprovementissustained.KeyindicatorsforaTripleAimprojectshouldalignwiththeIOM*andHQO**qualityindicators(RefertoAppendixEfordefinitions).KeyIndicator Population
HealthPatientExperience
PerCapitalHealthCost
Safety*,** X Effectiveness*,** X Personcenteredness*,** X Timeliness*,** X Equity*,** X X Efficiency*,** XIntegration** X XFocusonpopulationhealth** X Appropriateresources** X
22 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
22
SuccessStories
AnumberofsuccessstorieshavebeenidentifiedbyhealthcareorganizationsusingtheTripleAimFramework.Theseinclude:QueensHealthNetwork;HealthPartners;QuadMed;BellinHealth;andCareOregon(refertotheIHIwebsitehttp://preview.ihi.org/offerings/Initiatives/TripleAim/Pages/Materials.aspx).GenesysHealthSystemGenesysHealthSystem'ssuccessstoryisapplicabletotheprimarycaresector.GenesysHealthSystemisanonprofit,integratedhealthcaredeliverysystemthatprovidesacontinuumofmedicalcareservicestopatientsinGeneseeCountyandtheareasurroundingFlintMichigan.Itpartnerswithanetworkof150communitybasedprimarycarephysiciansaffiliatedwiththeGenesysPhysicianHospitalOrganization(PHO)(KleinandMcCarthy,2010).GenesysispursuingqualityimprovementusingtheTripleAimframeworkbyengagingcommunitybasedprimarycarephysicianstoenhancecarecoordination,preventivehealth,andefficientuseofspecialtycare.Itisalsopromotinghealththroughthedeploymentofhealthnavigators,whohelppatientsadopthealthybehaviours,andbypartneringwithacountyhealthplantoextendaccesstoprimarycareandotherservicestolowincome,uninsuredcountyresidents(KleinandMcCarthy,2010).Whilethehealthnavigatorprogramfocusesonbehavioursthatwillhavethegreatestimpactonhealthoutcomes,theyalsohelppatientsadaptbehaviourchangeplanstotheirpreferences,interests,andreadinessforchange.Forexample,apatientmaywishtoreducestressbeforetacklingweightloss(KleinandMcCarthy,2010).Genesysalsoengagesinothercommunityeffortstohelpimprovepopulationhealth.ThehealthsystemisamemberoftheGreaterFlintHealthCoalition,whichjoinslocalproviders,purchasers,consumers,insurers,schools,andfaithbasedorganizationsineffortstoimprovethehealthstatusofGeneseeCountyresidents,whiledecreasingcostsandinefficienciesincare.Themodelhashelpedlowertheuseandcostofcarewhileimprovingphysicianperformanceonqualityindicators.AstudybyGeneralMotorsfoundtheautomakerspent26%lessonhealthcareforenrolleeswhoreceivedservicesatGenesysversuslocalcompetitors.Theuseofhealthnavigatorshasimprovedhealthbehavioursandsatisfactionofpatients.Extendingthehealthnavigatormodeltolowincome,uninsuredpatientsenrolledinataxsupportedcountyhealthplanhasledtoimprovedhealthstatusandreduceduseofthehospitalandemergencydepartments(KleinandMcCarthy,2010).Apatientsurveyaskingpatientstoevaluatetheirphysiciansandtheirstateofagreementonafivepointscaleproducedaverageratingsof3.27outof5onwhetherpatientscouldachievelifechanges;3.95outof5onwhethertheproviderteamknewthem;andanoverallsatisfactionof4.4outof5(KleinandMcCarthy,2010).
http://www.commonwealthfund.org/Content/Publications/Case-Studies/2010/Jul/QuadMed.aspxhttp://preview.ihi.org/offerings/Initiatives/TripleAim/Pages/Materials.aspxhttp://www.commonwealthfund.org/Content/Publications/Case-Studies/2010/Jul/Genesys-HealthWorks.aspx
23 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
23
PerformanceTargetsAPerformancetargetisaquantitativeexpressionofanobjectivetobemetinthefuturebyanorganization,programoremployee.Performancetargetscanbeusedtofacilitatecontinuousqualityimprovementandareoftenusedinpayforperformance(P4P)programs.InOntario,theMOHLTChassignedMasterServiceAccountabilityAgreements(MSAA)withtheLHINswhichincludesectorspecificindicatorsforeachhealthcaresector(MSAA,2011).Intheprimaryhealthcaresector,CHCsarerequiredtoparticipateinaClientAccessforPrimaryCareClinicalServiceProgram.Thisinvolvesdevelopingandcollectingkeyexplanatoryandaccountabilityindicatorsrelatedtohealthequity,valueandaffordability,andquality.Theaccountabilityindicatorsincludebenchmarksofpreexistingdata;maybetiedtodedicatedfundingfromtheMOHTLC;mustbevalid,feasiblemeasuresofsystemperformance;andallowforcomparabilityacrosslikeorganizationsand/orregions.Theexplanatoryindicatorswill:becomplementarytotheaccountabilityindicators;supportplanning,negotiationandproblemsolvingattheprovincial,LHINleveloragencylevel;supporttransparencyandenableplanningdiscussions;andsupportandsustainqualityimprovement,effectivenessandefficiency.CHCshavealsocommittedtoparticipatingintheDataQualityAssessmentToolImplementationproject.ThistoolutilizedtheCIHIDataQualityFrameworkandprovidesaseriesofqualitativeandquantitativequalityindicators.Thereissomeevidencesuggestingthatperformancetargetscanbesuccessfuldriversofqualityifdesignedappropriatelyandareimplementedalongsideotherimprovementinitiatives(generalinspection,regulation,andfinancialincentives).Ifwelldesigned,targetscanhelporganizationsandpractitionersfocusonamanageablenumberofachievablegoals,whichtherebyleadtosystemimprovements.VanHertenandGunningSchepers(2000)concludedthatinorderforperformancetargetstobeeffective,theymustbespecific,measurable,accurate,realisticandtimebound.Performancetargetscanhaveperverseeffectsincluding:neglectofuntargetedaspectsofthehealthsystem;focusonshorttermtargetswithintheproviderscontrolratherthanlongtermorlesscontrollableobjectives;influencebyprofessionalinterests;underminingthereliabilityofthedataduetoaggressivetargets;inducingundesirablebehaviouralresponsesduetoaggressivetargets(Smith,inpress).IntheUK,PublicServiceAgreementsincludedstrategictargetsforallgovernmentdepartments,includingtheHealthMinistry(Smith,2007).TheseAgreementsfocusedprimarilyonoutcomes,suchastheimprovementofmortalityrates,reductionsinsmokingandobesity,andreductionsinwaitingtimes.Incontrasttomostnationaltargetsystems,thisprovedeffectiveinsecuringsomeofthetargetedobjectivesinhealthcare(BevanandHood,2006).
24 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
24
Thesuccessofthisinitiativehasbeenattributedto:precisetargets;generaltargetsbasedatthelocallevel,ratherthanthenationallevel;professionalsbeingengagedinthedesignandimplementationofsometargets;increasedfinancing,informationandmanagerialcapacitytoorganizations;andattachingincentivestotargets.Basedonthisexperience,performanceprioritiesandtargetsshouldbedevelopedinconsultationwithkeystakeholdersandsetmainlyatthepracticeandcommunitylevel.
ElectronicMedicalRecordandElectronicHealthRecordThetermElectronicMedicalRecord(EMR)generallyreferstoinformationsystemswithinonelocation(e.g.,adoctorsofficeorhospital)whileEHRreferstoasystemwhereinformationfrommultiplesourcescanbepooledand/orshared(OHQC,2010).TheOntariogovernmenthasinvestedsignificantlyinprovidingsubsidiestoprimarycarephysiciansforadoptionofEMRs.Thesesubsidieswerepreviouslyavailabletophysiciansinspecificprimarycaremodelsbutmorerecentlyhavebeenextendedtoallprimarycarephysicians(Hutchison,2011).AsofMay31,2011,therewereapproximately6,500Ontariophysiciansusing,orintheprocessofimplementinganEMR.Thisincludedapproximately4,700communityFPs.Inaddition,300CHCphysiciansreceivedfundingdirectlyfromeHealthOntariotoimplementanEMR(OntarioMD,personalcommunication,June26,2011).Thereissignificantconsensusintheliteratureandfieldthatsophisticatedhealthinformationtechnologyatthepracticelevelisfundamentaltotheprovisionofhighquality,efficientprimaryhealthcare.Informationmanagementsystemsneedto:supportclinicaldecisionmaking;identifycareneeds;supportperformancemeasurementandqualityimprovement;belinkedacrosshealthcaresettings;andsupportpatientsaspartners.ArecenthighqualityreviewfoundthatEHRsthatincludeclinicalinformationmanagementanddecisionsupporttools(particularlythosethattranslatedataintocontextspecificinformation)improvedproviderperformance.ThisreviewfoundsubstantialsavingscouldbeachievedbyimplementingEHRs.However,noneoftheincludedstudiesfocusedonprimaryhealthcare(McMasterHealthForum,2010).Theuseofinformationtechnologyforgeneratingremindersandforclinicaldecisionsupportsystemshasbeenshowntoimprovebothoperationalefficiencyandqualityofcare.Theseimprovementsincluded:increasedfrequencyofscreening;improvedpreventativecareanddiseasemanagement;reducedprescribingerrors;improvementsassociatedwithcomputerizedphysicianorderentry(CPOE)(e.g.,reducedrepeattestsandmoretimelytestsandprocedures);lessmissinginformation;andcostsavings(AHRQ,2007;Mitchell2001;Hunt,1998ascitedinCHSRF,2009).TheuseofEMRshasalsobeenshowntoimprove:overallpatientsatisfactionwiththeirvisits;patientsatisfactionwithphysiciansfamiliaritywiththem;patientprovider
25 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
25
communication;theuseoftimeduringthevisit,andcomprehensionofdecisionsmadeduringthevisit(Hsuetal.,2005ascitedinCHSRF,2009).Informationtechnologycanalsoleadtoimprovementsinthesystemofcarethroughproactiveplanningforpopulations,queriesandfollowuponsubpopulations,andhavingallpertinentpatientinformationinoneplaceallowingforthedevelopmentofaholisticcareplan(AHRQ,2007ascitedinCHSRF,2009).TheAgencyforHealthcareResearchandQuality(AHRQ)andtheInstituteforHealthcareImprovement(IHI)examinedtherequirementsforanEMRthatsupportsqualityimprovement.TheseorganizationsidentifiedthefollowingattributesascriticalelementsofahighlyfunctioningEMR:ProactivePatientBased
Allinvolvedinqualityimprovementshouldbeabletoquerythedata Thesystemshouldsupportinstantaccesstoqueryresults Thequeryingsystemshouldallowtheusertoaskanyquestion Usersshouldbeabletoconstructandrunquerieswithouttechnicalassistance Usersshouldbeabletospecifytheinclusionofanydataelementsinqueries Thesystemshouldsupportdrilldownintodata Usersshouldbeabletosavequeriesforreuseand/orrefinement Thesystemshouldsupportthesharingofqueries Thetypesofactiontakenonthelistsofpatientsinaqueryshouldbeflexible Theactiontakenonthelistshouldincorporateandusepatientdatatofurthersegment
theaction(e.g.,HbA1cfollowup) Thesystemshouldautomatetheactionswheneverpossible
PlannedCareforIndividualPatientsThewholepatientshould:
bedisplayedinoneplace bedynamic beusedforplanning,treatmentandfollowup supportcareacrossallconditionsandhealthissues,notjustthecomplaintassociated
withaparticularencounter bethecentrallocationforotherviewsofpatientdata,suchasrunchartsoflaboratory
resultsandvitals incorporateevidencebasedpromptsandreminders provideaportalforthepatientforbothinputandviewingdata,givingthepatientsome
controloverhis/herrecord
26 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
26
Measurement Themeasurementmoduleshouldallowtheusertocustomizeanyreportbyaddingor
changingafilter Thequeryandfilterstructuresformeasurementandreportingshouldbeidenticalto
thoseusedforthepopulationbasedcaretoolandforremindersandpromptsOther
Abilitytocustomizethedatapresented Easeofuse Interoperability Dataavailableacrossthecontinuumofcare Appropriatedatastructuresprovideinformationthatsupportsimprovement Automation
ThereportalsoindicatesthattheEMRmustsupportsystemsfor:informationsharing(e.g.,onedatawarehouseversusinteroperablesystems);dataownership;and,ensuredataaccuracy.EMRfunctionalityisnotnecessarilysufficienttopromoteitsutilizationforqualityimprovement.ProvidingappropriatetrainingandsupporttoprovidersonthemeaningfuluseofEMRisessentialforrealizingthebenefitsoftheEMR.TheCaliforniaNetworksforEHRAdoption(CNEA)programwasinitiatedin2006tospeedtheadoptionandlowerthecostsassociatedwithimplementingEHRsinthestateofCalifornia.Participantsshareexperiencesandlessonslearnedbetweenteamsasameansofacceleratingadoptionrates.Theprogramfoundthatwithoutcontinuous,structuredfollowuptraining,thebenefitsofEHRcannotbefullyrealized(CaliforniaHealthCareFoundation,2010).
PrimaryHealthcareTeamsCollaborativeprimaryhealthcareteamsconsistofavarietyofhealthcareprovidersresponsiblefordeliveringarangeofhealthcareservicestopatients.InOntario,nonFFSmodelsofprimaryhealthcareincludearangeofnonphysicianhealthcareprofessionalswithintheirpractice.InOntario,approximately21%ofFPsworkininterprofessionalhealthcaremodels(CHCs,FHTs)(Hutchison,2011).Thereisapotentialtoextendaccesstononphysicianhealthcareprofessionalstoprimarycarepracticesbasedonpopulationneeds.Agrowingbodyofevidenceshowsthatcollaborativeprimaryhealthcareteamscanimprovepatienthealthandqualityoflife,particularlyforthosewithchronichealthconditions.Suchteamsarealsoaneffectivewaytoprovideprimaryhealthcareservicestorural,remote,andunderservicedareas.
27 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
27
Collaborativecareforpeoplewithdepressionresultedinimprovementsthatweresustainedoverfiveyears(Gilbodyetal.,2006ascitedinHCC,2009).Patientsreceivingteambasedcarereportedbetterhealthresultssuchaslowerbloodpressure(Tayloretal.,2005ascitedinHCC,2009).Childrenwithasthmahadfewerdaysperyearofsymptomsthanasthmaticchildreninstandardcare(Lozanoetal.,2004ascitedinHCC,2009).Alzheimerspatientshadsignificantlyfewerpsychologicalsymptomsofdementiawithoutincreasingtheirmedication(Callahanetal.,2006ascitedinHCC,2009).Terminallyillpatientsreceivingteammanaged,homebasedprimaryhealthcarereportedsignificantimprovementsinfactorssuchastheirlevelofpainandmentalhealth(Hughesetal.,2000ascitedinHCC,2009).Overweightpatientsbeingtreatedbyamultidisciplinarygroupweremorelikelytoachievetheirweightlossgoalsthanthoseinothertreatmentgroups(Feigenbaumetal.,2005ascitedinHCC,2009).Grumbachetal.(2004)cautionedthatthesuccessofteambasedcarerestsonhowwelldifferenthealthcareprofessionalsworktogethertoformaneffectivelyfunctioningteam.Teammembersshouldfunctionattheirlevelofcompetency,focusingonthepatientsneedsandrecognizingtheimportanceofcontinuityinbuildingtrustingproviderpatientrelationshipstoachieveefficienciesandimprovedoutcomes(CronenwettandDzau,2010).Akeysuccessfactorforteamworkisempoweringteammemberstoperformtasksaccordingtotheirscopeofpractice,experience,andeducation(Schoen,2007).Todate,littleisknownabouttheteamstructures,composition,rolesorrelationshipsthataremosteffectiveandefficientinmeetingtheneedsofspecificpopulations.Collaborationbetweenprimaryhealthcareteamsandothersectorsisimportantinthecoordinationofpatientcare.Integratedhealthsystemsincludeaccesstoacomprehensiverangeofclinicalandhealthrelatedservices.Responsibilityforplanning,providingorprocuring,andcoordinatingallcoreservicesforthecontinuumofhealthrequirementsandforthepopulationservedisassumedbytheintegratedhealthsystem(Leattetal.,2003;MarriottandMable1998,2000).Thisincludesservicesfromprimarycarethroughtertiarycare,andcooperationbetweenhealthandsocialcareorganizations(SimoensandScott,2005).CurrentlycollaborationbetweenprimarycarephysiciansandsomecommunityprovidersisunderdevelopedinOntario.AsurveyexaminingtheperceptionofOntarioFPsoncollaborationwithcommunitypharmacistsindicatedthatphysicianshavefewerthanfiveconversationsaweekwithapharmacistaboutapatientsdrugtherapymanagement,veryfewusedpharmacistsastheirprimarysourceofmedicationinformationandfewparticipatedinhigherlevelcollaborativebehaviour(referringpatientstopharmacistsformedicationreviews)(Pojskicetal.,2010).Physiciansinthestudyreportedsignificantadvantagestocollaborationwithcommunitypharmacists,includingmoreaccuratepatientmedicationlistsandfinancialsavings
28 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
28
tothehealthcaresystem(e.g.,detectingdoubledoctoring/excessprescriptionuse,reducingneedforspecialistreferral).
PatientEnrolmentPatientenrolmentisaprocessinwhichpatientsinadefinedpopulationorgeographicalareaareformallyregisteredwithaprimarycareorganization,teamorprovider.Patientenrolmentfacilitatesaccountabilitybydefiningthepopulationforwhichtheprimarycareorganizationorproviderisresponsible(Hutchison,2008).InOntario,9.5millionOntarioresidentsareenrolledtoreceivecarefrom709PEMs.Formalpatientenrolmentwithaprimarycareproviderlaysthefoundationforaproactive,populationbasedapproachtopreventivecareandchronicdiseasemanagementandforsystematicpracticelevelperformancemeasurementandqualityimprovement.Itclearlyestablishesprimaryhealthcareprovidersashealthstewardsforadefinedpopulationratherthanprovidersofservicestothosewhopresentthemselvesforcareandclarifiesmutualresponsibilities.OntarioshouldcontinuethegrowthanddevelopmentofPEMs.
PatientEngagementPatientengagementcantaketheformofengagementinonesownhealth,careandtreatmentorinvolvementinthedesign,planninganddeliveryofhealthservices(Parsons,2010).Involvingpatientsinevaluatinghealthneedsandhealthcareperformanceisanessentialcomponentofqualityimprovement.Tounderstandthepatientandfamilyexperiences,shadowingguidelineshavebeendevelopedforhealthcarepractitioners(Digioia,2010).Theguidelinesprovidestepbystepinformationonhowashadowercanfollowthepatientandfamilycareexperience.HQOiscurrentlydevelopingaprimaryhealthcarepatientengagementframework(SpencerCameron,2010).Patientengagementenablespatientstocollaboratewiththeirhealthcareprofessionalsintheselfmanagementoftheircare;toevaluateandshapethedesignanddeliveryofcarewithinthecareteam;toevaluateandshapethestrategicdirectionofhealthcarewithinahealthcareorganization(e.g.,patientfocusgroups/patientinvolvementingovernance/planningandpolicy);andtosupportandadvocateforstrongpartnershipswithpatientsandtheprimaryhealthcarecommunity(SpencerCameron,2010).CoulterandEllins(2006)indicatethereisanassociationbetweentheengagementofpatientsintheirhealth,careandtreatmentand:patientsrecallofinformation,knowledgeandconfidencetomanagetheirconditions;thelikelihoodofpatientsreportingthatthechosentreatmentpathwasappropriateforthem;patientreportingoftheirexperiencesandsatisfactionwithcare;
29 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
29
and,theuseofhealthcareresources,whereengagedpatientsaremorelikelytoadheretochosencoursesoftreatment,andtoparticipateinmonitoringandpreventionforexample,byattendingscreening.Ithasalsobeenshownthatsomeinterventionstoinvolvepatientsinsharingthedecisionabouttreatmentchoiceresultinpatientschoosinglessinterventionist(andlesscostly)treatmentsthantheircliniciansmightotherwisehaverecommended(Parsonsetal.,2010).Onestudyindicatedthatthereislimitedevidencetosupportinterventionsthatpromotepatientinvolvementinimprovingsafety(Halletal.,2010).OtherstudiesindicatedthattherewasnoclearevidencethatempoweringpatientsthroughaccesstotheirEHRsimprovedqualityofcare(Koetal.,2010;Laugharne,2004;Gyselsetal.,2007).Therearefewreliableandrobuststudiesontheeffectsofpatientinvolvementinthedesign,planninganddeliveryofprimaryhealthcareservices.Involvingthepatientinselfmanagementandinthedesignandplanningofhealthcareservicesiswidelybelievedtobeacriticalstrategyforachievingqualityimprovementinprimaryhealthcare.Moreinformationisrequiredonthebestapproachestopatientengagement.
ResearchandEvaluationAconstantflowofresearchevidencetoinformprimaryhealthcarepolicyandpracticeisanessentialunderpinningofahighperformingandcontinuallyevolvingprimaryhealthcaresystem.Inadditiontoongoingperformancemeasurementandmonitoring,effectivehealthsystemplanningandmanagementrequirefocusedevaluationsoftheimplementationandimpactofkeypolicyandsystemmanagementinnovations.Suchevaluationsallowshortcomingstobeidentifiedandaddressedandsuccessestobereinforcedandspread.Evaluationsofpilotordemonstrationprojectsprovidealowriskopportunitytotesttheeffectivenessofqualityimprovementstrategiesandenablers.Adequatefundingofbothresearchandresearchtrainingareneededtocreateandsustainavibrantandproductiveprimaryhealthcareresearchenterprise.Qualityimprovementresearchthatpertainstotheprimaryhealthcaresectorislimited.Toensureefficiencyandeffectiveness,theremustbeinvestmentinhealthservicesresearchandevaluationfocusingonqualityimprovementintheprimaryhealthcaresector.
30 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
30
FinancialIncentivesPayforPerformance(P4P)inprimarycarerepresentsasetofstrategiesthatusefinancialleverstoencouragehealthcareproviderstoachievemeasuredstandardsofpatientcaretoimprovequality.P4Pismeanttoincreasepaybackonresourcesinvestedinmedicalcarebyprovidingincentiveswhichincreasethequalityofcareand/ortoincreasetheuseofmedicaltreatmentswithevidenceofenhancedvalueandbetterpatientoutcomes(InstituteofMedicineoftheNationalAcademies,2007;Pinketal.,2006).InOntario,financialincentivesinprimarycarearepaidformeetingestablishedthresholdlevelsforperformingpreventivecareactivities.Theamountofthepreventivecarebonusvariesbasedonthelevelofthresholdachieved.Otherincentivesarefocusedonencouragingtheprovisionofpriorityservices.AstudyfromtheMcMasterUniversityCentreforHealthEconomicsandPolicyAnalysis(Hurleyetal.,2011)assessedOntariophysiciansresponsestofinancialincentives,includingpreventivecareP4Pbonusesandspecialpaymentsforpriorityservices(e.g.,obstetricaldeliveries,prenatalcare,hospitalcare,palliativecare,inofficetechnicalprocedures,homevisits,andcareofpatientswithseriousmentalillness).ThestudyfoundP4Pincentivesledtoanincreaseoverbaselinelevelsintheprovisionoffouroffivepreventiveservices:5.1%forseniorsinfluenzavaccination;7%forPapsmears,2.8%formammography,and56.7%forcolorectalcancerscreening(Hurleyetal.,2011).Therewasnodetectableimprovementfromspecialpaymentsforpriorityservicesabovethresholdlevels.ThereareonlyafewrigorousstudiesofP4P,andoveralltheevidenceofitseffectsisweak(McMasterForum,2010).Thereviewfoundthatfinancialincentivestargetingindividualhealthcareprofessionalsappeartobeeffectiveintheshortrunforsimple,distinct,welldefinedbehaviouralgoals(McMasterForum,2010).Thereislessevidencethatfinancialincentivescansustainlongtermchanges.Halfoftheincludedstudiesfocusedonqualityimprovementinprimaryhealthcare(McMasterForum,2010).P4Piswellsuitedtoaddressissuesofunderusebutlesssuitedtocurtailingoveruseorinappropriateutilization(MOHLTC,2007).Ifimplemented,carefulconsiderationmustbegiventothedesignofaP4Pprogramandpotentialperverseeffects.AreviewofP4PprogramsthatprovidepaymentstoprimarycarephysiciansintheUnitedKingdom,AustraliaandUS(MOHLTC,2007)foundthatitisimportantfortheincentivesandgoalstobealignedandthatpolicymakersandprovidersknowthelinkbetweenperformancemeasuresandtheoverallgoalsofprimarycare.Itisalsoimportantforfinancialrewardstobelinkedtothedesiredoutcomeoractivitytoprovidethedesiredincentive.Tobeeffective,itisnecessarytomeasurebaselineperformancebeforeintroducingtheincentivestodetermine:theextenttowhichperformanceisalreadybeingachieved;howmuchitcanbeimproved;andtoforecastprogramcosts.Thisrequiresensuringdataaccuracy,
31 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
31
validityandreliabilityofmeasurement(MOHLTC,2007).Whensettingtargetsandpaymentstructures,bothachievementofsetgoalsandimprovementfrombaselinemeasuresshouldberewarded.Unlessthisisdone,targetsmaybeseenasunfairtogoodproviders(ifonlyimprovementisrewarded)orinsufficienttoencouragechangesinpractice(ifonlyattainmentisrewarded)(MOHLTC,2007).SeveralperverseeffectsofP4Phavebeenidentified.Highperformerstendtodobetter,whilepoorperformersimprovemoreslowlyorevendoworse.Netrevenuemaydeclineforthosewhoneedtoinvestthemostinqualityimprovement,andresourcepoorserviceprovidersmaynotinvestsufficientlytoqualifyfortheincentives(CHSRF,2009).Improvementinsomeareasmaybetothedetrimentofothersandtheincentivestructuremaypromotethecherrypickingofwhichpatientsareseen,orwhatservicesareprovided.Extrinsicincentivesmayundermineprovidersintrinsicmotivation(Hutchison,2008).P4Pschemestendtorewardprocessesratherthanoutcomes,andtheprocessesrewardedareonlyasubsetofdeliveryprocesses(oftenthoseforwhichdataareavailable).Focusingontheseratherthantheentiredeliveryprocessmaydivertattentionfromotherareaswhicharealsoimportant(Hutchison,2008;Miller,2007;Rosenthal,2004ascitedinCHSRF)Thereisalsothepotentialtocreateadetrimentaleffectondependentprogramsorservicessuchas:increaseddemandforlaboratorytestsordiagnosticprocedures;potentialiatrogeniceffectsoffindingfalsepositivecases;andincreasedresourcesrequiredtotreatadditionalidentifiedcases(MOHLTC,2007).ManyP4Pschemesmakepaymentstophysiciansbasedonmeasurementsthataremadeatthepracticelevel,orwhichmeasureactivitiesthatareperformedbymembersofthehealthcareteam.AstudyofP4PprogramsinAustralia,U.K.andU.S.foundnursesweretypicallysalariedemployeesofapracticegroupwhichweretypicallyownedbyphysicians(MOHLTC,2007).IntheU.K.thiscausedconflictwhenteamswerenotwellintegratedorcollegial.However,inothersettings(suchasaCaliforniaplanoperatedinaunionizedenvironment),bothprimarycareprovidersandpracticenursesweredirectemployeesofthehealthplanandtheunionwasabletonegotiateperformancepaymentfornursesforactivitiesthatwereprimarilyperformedbythenursingstaff.Paymentsschemesthatrewardhealthcareprofessionalsperformingspecificactivities(ratherthanthepracticegroup)aremorelikelytoensureanequitabledistributionofperformancepayment.Thereislimitedresearchonthepositiveornegativeeffectsincentivesmighthaveonteams.Moreresearchisrequiredinthisarea.
TrainingandSupportQualityimprovementtrainingandsupportcantaketheformofqualityimprovementcollaborativesandcoaching.Acollaborativeisalearnbydoingapproachtoqualityimprovementwhichreliesonspreadingexistingknowledgetoachievethedesiredoutcome.Keyfeaturesinclude:learningqualityimprovementtechniques;sharing"ontheground"
32 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
32
experiencesandsuccess;and,conductingsmalltestsofchangeknownasPlanDoStudyAct(PDSA)cycles.Coachingisamethodthatcustomizessupportforthepracticeandallowsimprovementexpertstogaingreaterinsightintohowthepracticefunctions.Practicecoacheshelpphysiciansandteamsdeveloptheskillstheyneedtoadaptclinicalevidencetothespecificcircumstancesoftheirpracticeenvironment(AligningForcesforQuality,2010).Qualityimprovementtoolsandtechniquesforplanningandimplementingchangeinclude:Lean,SixSigmaandtheModelforImprovement(Dawdaetal.,2010).Eachframeworkhasadifferentemphasis.Eachseekstofacilitatetheapplicationofevidenceorinnovationreliablyandefficiently.Organizationscommonlyadoptaspectsofmorethanoneframeworkintheirqualityimprovementendeavours.InOntario,theMOHLTCcreatedQIIPtoprovidetrainingandsupporttoprimarycarepractices.Todate,QIIPhascompletedthreelearningcollaborativeswith122FHTandCHCteams(Hutchison,2011).In2010,QIIPlaunchedtheLearningCommunitywhichcombinesvirtualandfacetofacelearningontheapplicationofQImethodsandtoolsandsupportfromqualityimprovementcoaches.InWave1,approximately127interprofessionalhealthcareteamsparticipatedinoneormoreofsixactiongroupsfocusedonimprovingchronicdiseasemanagement(Asthma,ChronicObstructivePulmonaryDisease,Diabetes,Hypertension),preventivecare(IntegratedCancerScreening)andAccessandEfficiency(OfficePracticeRedesign)(QIIP,2011).NinetytwoteamsareparticipatinginWave2whichfocusesonAccessandEfficiency(OfficePracticeRedesign)andincludesparticipantsfrommostprimarycaremodels,includingtraditionalfeeforservicespractices.TheLearningCommunityisbasedontheModelforImprovementandPDSAcyclesofchange,awebbased,realtimeworkspacecalledtheGATEWAY,andsupportfromanexternalqualityimprovementcoach(Hutchison,2011).Thereisincreasingevidencethatqualityimprovementtrainingandsupportcaneffectivelyhelphealthcareprovidersapplyqualityimprovementmethodsintheirpractice.Collaborativestargetingdiabetesmanagementhavebeenshownto:improveHbA1c,lowdensitylipid(LDL)andbloodpressuretestingratesandresults;improvepatienteducation;increasepreventiveprocedures;reducehospitalization;andimprovequalityoflifeindicators(Piatt,2006;Asch,2005;Tsai,2005;SperlHillen,2000;Wagner,2001;Camp,2004,ascitedinCHSRF,2009).IntheUK,theuseofcollaborativesbytheNationalPrimaryCareDevelopmentTeamresultedinimprovedaccesstoprimarycare,reductioninheartdiseasemortality,reductionincoronaryheartdiseasemortality,savingof6,070lives,andimprovementofdiabetescare(CHSRF,2009).InSaskatchewanandBritishColumbia,chronicdiseasemanagementcollaborativesresultedinimprovedoutcomesforpatientswithchronicdisease(HealthQualityCouncilSaskatchewan,2008;Tregillis,2006,ascitedinCHSRF,2009).
33 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
33
TheIHIsBreakthroughSeriesmodelhas:increasedpatientandprovidersatisfactionandimprovedhealthoutcomesbyenablingparticipantstoshareexperiences;acceleratelearning;andspreadbestpractices.Theseinitiativeshaveresultedin:reducedwaittimesforappointments;reducedwaittimeswhileatthephysiciansoffice;improvedcontinuityofcare;andincreasedpatientandprovidersatisfaction(IHI2008ascitedinCHSRF,2009).Thereisgrowingevidencethatpracticefacilitationpositivelyaffectstheadoptionofevidencebasedpracticeguidelines(Baskervilleetal.,inpress)andhelpsstaffapplyqualityimprovementtechniques(LawrenceandPackwood,1996;Hearnshaw,1998).Evidenceregardingtheimpactofcoachingonfacilitatingqualityimprovementinchroniccaremanagementisgrowing(Wu,2009).AstudybySteiner(2010)foundthatqualityimprovementcoachesresultedinincreasedofficeefficiencyandimprovedcareforpatientswithdiabetesandasthma.AresearchsynthesiscommissionedbyCanadianHealthServiceResearchFoundation(CHSRF)iscurrentlyunderwaytoexaminetheeffectivenessofqualityimprovementinterventionsinprimaryhealthcare.Trainingintheuseofcontinuousqualityimprovementmethodsandmeasurementtechniquesisnotwidelyavailabletohealthcarepractitioners.Providinghandsontrainingandsupporttohealthcarepractitionerscanfacilitatetheadoptionanduseofqualityimprovementmethodsandtools.Qualityimprovementtrainingandsupportshouldbemadeavailableovertimetoallprimarycareprovidersandorganizationsandbeembeddedinallhealthcareprofessionaltrainingprograms.
PublicReportingPublicreportinginhealthcareisamechanismbywhichthepublicisinformedoftheperformanceoftheirhealthcaresystem.Performancereportingcantakeplaceatthesystem,organizationalorproviderlevel.Informationcanbemadeavailabletothepolicymakers,healthcaremanagers,healthcareprovidersandthegeneralpublic.InOntario,theHQOisresponsibleforreportingonthenineattributesofqualityattheprovinciallevel.Publishinginformationinthepublicdomain,toinformthepublicandotherstakeholdersaboutsystemandproviderperformance,isgrowing.Thisinformationoftentakestheformofreportcardsorproviderprofilesthatsummarizemeasures,suchaswaittimes,patientsatisfactionratingsandmortalityrates,acrossproviders.Publicreportingonhealthcarequalityismotivatedbytheprincipleoftransparencyinpubliclyfundedhealthcareandistoutedasanimportantdriverofqualityimprovementandasameansofpromotingconsumerchoice(MorrisandZelmer,2005;Shekelle,inpress;Marshalletal.,2000;Marshalletal.,2003).Publicreportingcanimprovequalitythroughtwopathways:aselectionpathway,wherebyconsumersbecomebetterinformedandselectprovidersofhigherquality;andachange
34 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
34
pathway,wherebyinformationhelpsproviderstoidentifytheareasofunderperformance,thusactingasastimulusforimprovement(Berwicketal.,2003).Therefore,makinginformationaboutquality(andcosts)widelyavailableisseenasanimportanttoolforqualityimprovement.Althoughpublicreportingattheinstitutionallevel(e.g.,hospitals,integratedhealthorganizationsandhealthplans)isrecognizedtoimprovepatientoutcomes,thereislessevidenceontheimpactthatpublicdisclosureoftheperformanceofindividualprovidersandpracticeshasonqualityimprovementinitiativesandoutcomes.Todate,thereisnoevidencetosuggestthatpatientschangetheirmedicalproviderifdifferencesinqualityaredemonstrated(GalvinandMcGlynn,2003ascitedinSmith,2004;Reinertsenetal.,2008).Thereisstrongerevidencetosuggestthatreportingpromotesqualityimprovementinitiatives(Fung,2008;Sorbero,2008;Doran,2008;Werner,2008;Lindenaueretal.,2007,ascitedinCHSRF,2009).Studiesthatevaluatedimprovementofactualqualitymeasuresidentifiedsomeimprovement,buttheimprovementsweresmall(Castleetal.,2007;Lindenaueretal.,2007,ascitedinCHSRF,2009).Arecentmediumqualityreviewfoundthatpubliclyreleasingperformancedatastimulatesqualityimprovementactivityatthehospitallevel;however,thereviewdidnotidentifyaclearmessageabouttheprimaryhealthcaresector(McMasterForum,2010).InEngland,allNationalHealthServicehealthcareorganizationsareissuedanannualperformanceratingareportcardratingthemfromzerotothreestars,basedonabout40performanceindicators.Poorperformancehasputexecutivesjobsatrisk,andtheinitiativehadastrongeffectonreportedaspectsofhealthcare,suchaswaittimes.However,italsoinducedunintendedbehaviouralconsequencessuchaslackofattentiontosomeaspectsofclinicalquality(AuditCommission,2003;Carvel,2003ascitedinGrol,2004).IntheUnitedStates,twostates(NewYorkandPennsylvania)haveexperimentedwithpublicreportingofpostoperativemortalityratesforcoronaryarterybypassgraftsurgery.Ratesareriskadjustedandpublishedforboththehospitalandtheindividualsurgeon.TheschemesresultedinmarkedimprovementinriskadjustedmortalityinbothNewYorkandPennsylvania(Shekelle,inpress).However,thereisdebateaboutwhethertheseschemeshavebeenbeneficialsinceanumberofadverseoutcomeshavealsobeenreported(SchneiderandEpstein,1996;Dranoveetal.,2003ascitedinGrol,2004).InOntario,provincialinitiativesinvolvingpublicreportingofemergencydepartmentwaittimesandsurgeriesandotherprocedureshaveresultedinimprovedoutcomes.PublicreportingontheOntarioWaitTimeswebsitehasreducedtheamountoftimespentinemergencyroomsbycomplexpatientsbytwohours(HQO,2011).The90thpercentilewaittimesforhipreplacements,kneereplacementsandcataractsurgeriesdecreasedbymorethanhalfsince2005.The90thpercentilewaittimeforCTscansdecreasedfrom2.5monthstoaboutonemonthoverthesametimeperiod.
35 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
35
Thereisscantevidenceregardingpublicdisclosureofperformancedata,particularlyaboutindividualprovidersandpractices.Majorpublicreportingsystemshavenotbeenrigorouslyevaluated(Hibbardetal.,2003).IntheUnitedKingdom,theQualityandOutcomesFrameworkhasstimulatedgeneralpractitioneractivitysincedetailedresultsforeverypracticeareavailableontheInternet.Barretal.,(2006)foundthathealthcareorganizationsweremorelikelytorespondtopublicreportsthanindividualproviders.Organizationsdevelopculturesandbehavioursthatareoftenattherootofqualityissues,makingitfavourabletoreportatthelevelofthehealthcareorganizationtoachieve:accountability;qualityimprovement;orconsumerchoice.Thereareseveralunintendedconsequencesthatcanresultfromreportingtothepublic.MannionandDavies(2002)arguethatapublicreportmaypromptprovidersandhealthcareorganizationsto:focusonmeasuredclinicalareastothedetrimentofothers;focusononenarrowclinicalareawithoutcoordinatingwithothers;concentrateonshorttermgainsattheexpenseoflongtermgoals;bedisinclinedtoexperimentwithnewapproachestocare;andalterbehaviourtocreateanadvantageattheexpenseofpatients(Marshalletal.,2000).Otherconsequences,suchas:publicdistrustofthesystem;misinterpretationofthereport;andreducedstaffmorale,aremorelikelytooccurwhenthereportmadepublicisdifficulttounderstand(Shekelle,inpress).Wallaceandcolleagues(2007)suggestthatpublicreportingmustclearlyaddressobjective(s),audience,content,products,distributionandimpacts(intendedandunintended)andcarefullyconsideranypotentialadverseoutcomes.Toenhancetheircredibilityandusefulness,publicperformancereportsshouldbecreatedincollaborationwithphysiciansandotherlegitimateinterestgroups(AgencyforHealthcareResearchandQuality,2007;Marshalletal.,2000).Whenreportingdata,carefulriskadjustmentshouldbeimplementedtoofferaccuratecomparisonsbetweenprovidersandtoensurethatthelegitimacyofthecomparisonsisacceptedbyprofessionals(Marshalletal.,2003).Publicdisclosureofinformationshouldalsobeintegratedwithotherqualityimprovementstrategies(Marshalletal.,2000).Giventhepaucityofevidenceontheimpactofpublicreportingatthepracticelevelandthepotentialforunintendednegativeconsequences,atthepresenttimepublicreportingonprimaryhealthcareshouldbeconductedattheprovincialandregionallevelsratherthanatthepracticeorproviderlevel.
AccreditationAccreditationisarigorousexternalevaluationprocessthatcomprisesselfassessmentagainstagivensetofstandards,anonsitesurveyfollowedbyareportwithorwithout
36 ImprovingQualityinPrimaryCareReportoftheWorkingGrouptothePrimaryHealthcarePlanningGroup
36
recommendations,andtheawardorrefusalofaccreditationstatus(Pomeyetal.,2010).Accreditationcanbeavoluntaryoramandatedprocess.InCanada,accreditationisvoluntaryexceptforFirstNationsfacilities,universityaffiliatedhospitalsandinstitutionsinQuebec.AccreditationCanadaisanationalnonprofitorganizationthatwasestablishedtoguaranteethathealthcareorganizationsinCanadaprovideservicesofacceptablequality.Thisorganizationfollowsinternationalaccreditationprotocolsfortheselfassessmentofhealthcareorganizationsagainstagivensetofstandardsdeterminedbyprofessionalconsensus.Anonsitesurveyisconductedandfollowedbyareportwithorwithoutrecommendationsandtheawardorrefusalofaccreditationstatus.Thereislimitedevidencetosuggestthatexternalaccreditationresultsinsustainedqualityimprovement.GreenfieldandBraithwaite(2008)reviewedandanalysedtheliteratureonaccreditationandaccreditationprocesses.Thepicturewascomplex,withimprovementshavingbeenreportedinsomefieldsbutnotinothers.Theirreviewdidnotreportonthedesignorthequalityoftheincludedstudies,anddidnotgivequantitativeestimatesoftheeffectsofaccreditation.TheWorldHealthOrganization(2003)foundtheintroductionofaccreditationprogramsisdirectlytiedtofinancialincentivesandsuggestedmoreinformationisrequiredbeforedeterminingifaccreditationisthemo