Embed Size (px)
Citation preview

Quality Improvement: Overview of basic principles and our curriculum
Melanie Donnelly

Goals of this presentation
• Introduce some Quality Improvement and Patient Safety Terminology
• Introduce the process we are going to use this year for teaching some Quality Improvement and Patient Safety principles

What is Quality Improvement?• “the combined and unceasing efforts of everyone-healthcare
professionals, patients, and their families, researchers, payers, planners and educators-to make the changes that will lead to better patient outcomes (health), better system performance (care), and better professional development (learning).” *
Batelden PB, Davidoff F. What is “quality improvement” and how can it transformHealthcare? Qual Saf Health Care. 2007:16;2-3.

What put the issue of “quality” at the top of our agenda?
• Institute of Medicine Report– 1999: To Err is Human
• 98,000 deaths in US hospitals each year due to preventable medical errors
– “faulty systems, processes, and conditions that lead people to make mistakes”
– 2001 Crossing the Quality Chasm• Defines 6 dimensions of healthcare quality• Makes suggestions for improvement to healthcare

Institute of Medicine
• Safe: mortality rates• Effective: how well are evidence based practices
followed? Match care to science• Efficient: Analysis of the costs of care by patient,
provider, organization, and community• Timely: waits and delays with services and results• Patient centered: patient and family satisfaction• Equitable: differences in quality measures by race,
gender, income and other SES and demographic variables

“Just Culture”
• Describes an environment that recognizes that competent individuals make mistakes and that individual providers should not be held accountable for systems failures over which they have no control
• Many errors represent predictable interactions between professionals and the systems they work in
• Creates a culture where professionals are more comfortable disclosing errors
Continuing data on errors
– 2013, John T. James “A New, Evidence-based Estimate of Patient Harms Associated with Hospital Care”
• The number of premature deaths associated with preventable harm to patients is 210,000-400,000/year
• Serious harm is 10-20 times more common then lethal harm
• Now what?– Systematically seek patient voice in identifying harm– Accountability for harm of the organization– Intentional correction of root causes of harm

Why is QI important?
• Mechanism for providers to engage in improving patient care and possibly reducing patient deaths and harm
• Incentives based on “quality measures”• Board Certification, for some specialties, tied to
completion of quality improvement activities• Academic medical center and we have been
mandated to teach it– MILESTONES– CLER

CLER
• Clinical Learning Environment Review Program• ACGME program• “to generate national data on program and institutional
attributes that have a salutary effect on quality and safety in setting where residents learn and on the quality of care rendered after graduation”
• Provides on site sampling of learning environment that they hope will increase the educational emphasis on patient safety and provide an opportunity for institutions to demonstrate leadership in patient safety and quality improvement

Some select recommendations from our CLER visit
• Increase safety report submission rate• Develop clear definition of near misses• Increase resources for research in patient
safety• Provide support for institutional patient safety
curriculum• Early participation in QI teams• Engaging early in selection of QI initiatives
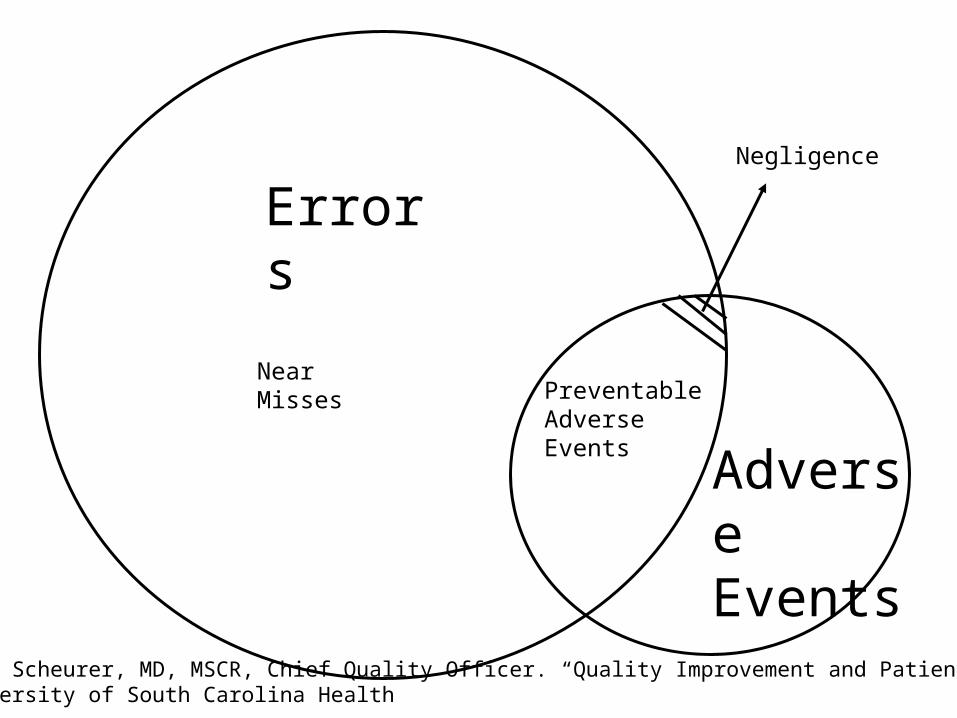
Errors
Adverse Events
Preventable Adverse Events
Near Misses
Negligence
PPT Danielle Scheurer, MD, MSCR, Chief Quality Officer. “Quality Improvement and Patient Safety”Medical University of South Carolina Health

Resident Curriculum• Global aim
– Empower residents to create changes they think are important to their work environment and to improve patient and provider experiences, using quality improvement/patient safety methods.
• SMART aim– Over the course of the academic year, residents will
• perform a root cause analysis of an adverse event/near miss OR obstacles to care
• develop a flowchart/process map outlining the process which allowed the event to occur
• identify an area for improvement• develop a quality improvement project (using PDSA methodology) that is
ready for implementation with a CA3 leading the project and a faculty advisor

Steps in process: abbreviated timeline
• CA3 sets up first group meeting for September
• Sept: choose/understand problem, process map, begin thinking about root cause analysis, assign specific tasks
• Oct/Nov: continue work on process map and RCA based on findings of group, possibly select area of improvement you will focus on, consider writing smart aim or at least determine data you need to create aim for your project, assign tasks
• Jan/Feb: completed RCA, flowchart, have target for intervention, finish SMART aim, begin designing QI project, assign specific tasks
• March/April: continue working on QI project, start organizing presentation
• May: finalize presentation• June 6 afternoon:
presentation to dept, with judge from ACGME and an award
What problem will you work on?• Step 1:Identify adverse event/near miss/obstacle to
care– Your group will choose this
• Pick something YOU care about and figure out WHY it matters
– Why would it be considered a problem?– When and where is this happening?– Who else cares about the problem?
• Stakeholder: patients, nurses, patient family members, administrators
• Is there data to support your contention that this is a problem?– Local data is great- ask around- informal surveys– Literature is a good source as well– PSN’s, QA’s

Process map from institution XPatient called day before with time for surgery, NPO guidelines
Patient arrives at 6am to facility
Patient seated at 6-610am for first start block
Patient ready by 650 to be seen by anesthesia AND surgery for consent and preop
Patient consented for anesthesia and surgery by 710
Resident: place monitors, get drugs and draw them up, open kit, get patient positioned, call nurse and attending
Time out done: allergies verified, coag status verified, consent verified and patient affirms
Block started

Root Cause Analysis Basics
Why• Joint Commission defines situations where we
MUST do an RCA• Department of Health has defined reportable
events• Value from a process or systems base

Root Cause Analysis Basics
Who• Involved providers• Risk• Quality• Key stakeholders for implanting changes• Ad hoc members on case by case basis

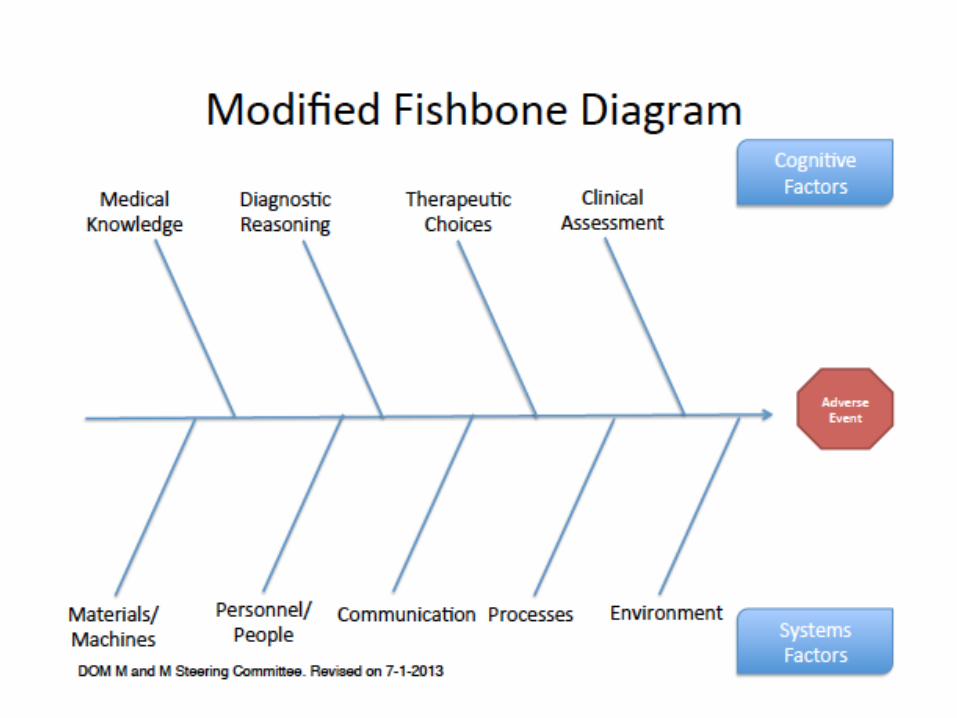
Root Cause Analysis Basics
How• Multi-disciplinary meeting• Usually facilitated by Risk• Fishbone diagram utilization• Needs to have action items and identifiable
individuals or teams to address


Areas for improvement, step 2
Create idealized process map incorporating changes you think would improve the system/process now that you know what factors contributed to your negative outcome (from your RCA)
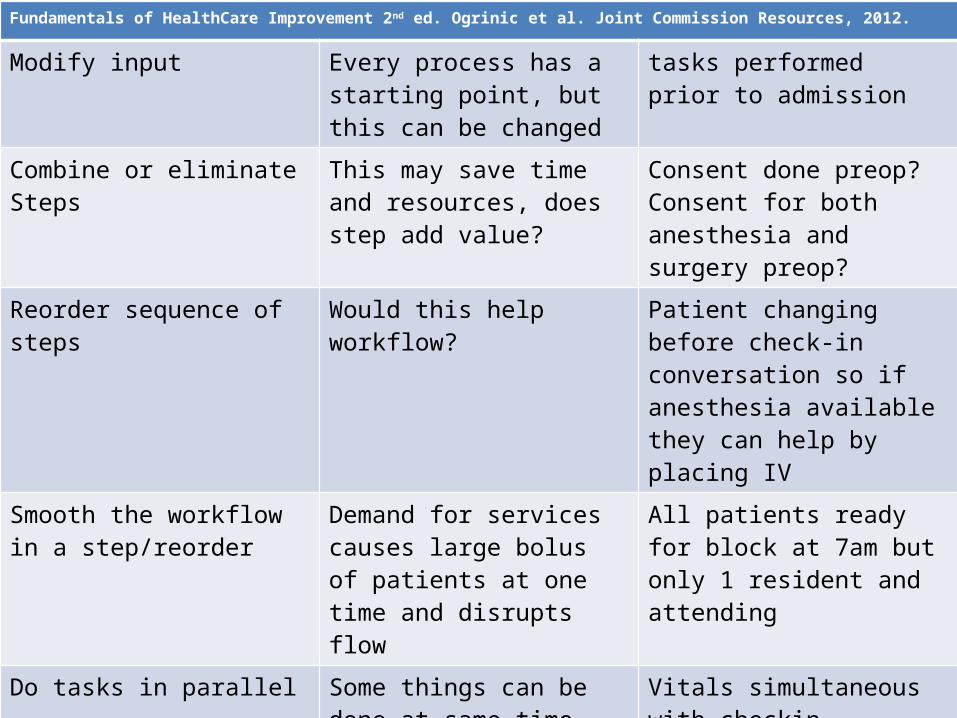
Fundamentals of HealthCare Improvement 2nd ed. Ogrinic et al. Joint Commission Resources, 2012.
Modify input Every process has a starting point, but this can be changed
tasks performed prior to admission
Combine or eliminate Steps This may save time and resources, does step add value?
Consent done preop? Consent for both anesthesia and surgery preop?
Reorder sequence of steps Would this help workflow? Patient changing before check-in conversation so if anesthesia available they can help by placing IV
Smooth the workflow in a step/reorder
Demand for services causes large bolus of patients at one time and disrupts flow
All patients ready for block at 7am but only 1 resident and attending
Do tasks in parallel Some things can be done at same time
Vitals simultaneous with checkin conversation, IV simultaneous
From knowledge of outcome redesign process
Outcome and process measures can direct team towards changes
Based on fall data we know that those with strokes have higher rate
Listen to patients and families Feel conversation with anesthesia is rushed and get too much information too fast

Thoughts on areas to target….
• Surgical consent in clinic• Educational information/dvd provided to
patient about their anesthesia• Patients arrive earlier to preop holding area• Anesthesia access to all block patients by
630am to set clear expectation• Streamlined check-in process with some
components completed with phone-call

What area of the system or process can you target to improve? Step 3
http://asq.org/healthcare-use/why-quality/impact-effort.html

Now start thinking about how you will measure your improvement, step 4a
• Outcome measures: number of patients who receive preoperative blocks?
• Process: time that patients are ready for anesthesia in the morning?
• Balancing measures: unintended consequences– Nurses feel overwhelmed and rushed– All preop nurses quit because you are asking them to
come in at 530am– Patients are educated about blocks and expect them
but then don’t get them due to time constraints

Now you know what you want to do…
• Need a SMART aim• Specific• Measureable• Aggressive but Achievable• Relevant• Time Bound

SMART aim step 4b
• Patients identified as a first start block to preop (the day before surgery) for urology will be ready for anesthesia and surgery consent by 630am beginning on June 1, and will arrive to preop 15 minutes before all other patients.
• Over the course of the academic year, residents will perform a root cause analysis of an adverse event/near miss OR obstacles to care, develop a flowchart outlining the process which allowed the event to occur, identify an area for improvement, and develop a quality improvement project (using PDSA methodology) that is ready for implementation with a CA3 leading the project and a faculty advisor.

Remember….
• ACHIEVABLE!!!!!!!• SPECIFIC!!!!• INTERESTING TO YOU!!!!!• RESIDENT DRIVEN!!!!

PDSA Video
• Learn PDSA (plan-do-study-act) QI methods by viewing its application to a household process we can maybe all relate to…..
• http://www.youtube.com/watch?v=jsp-19o_5vU

Step 5

Resources• Money• People: Kezia Windham (risk manager), Kaci Meddings (Quality
Improvement Specialist, Nicole Babu (Perioperative Patient Safety RN)



Next steps
• Pretest to residents– Via email and return to Colleen Dingman– She will create an anonymous product for grading– Post test at the end of year
• CA3’s will get emails with groups listed• CA3 contact group members to set up first
meeting in September- Email Melanie Donnelly with date for meeting– One faculty member at each meeting
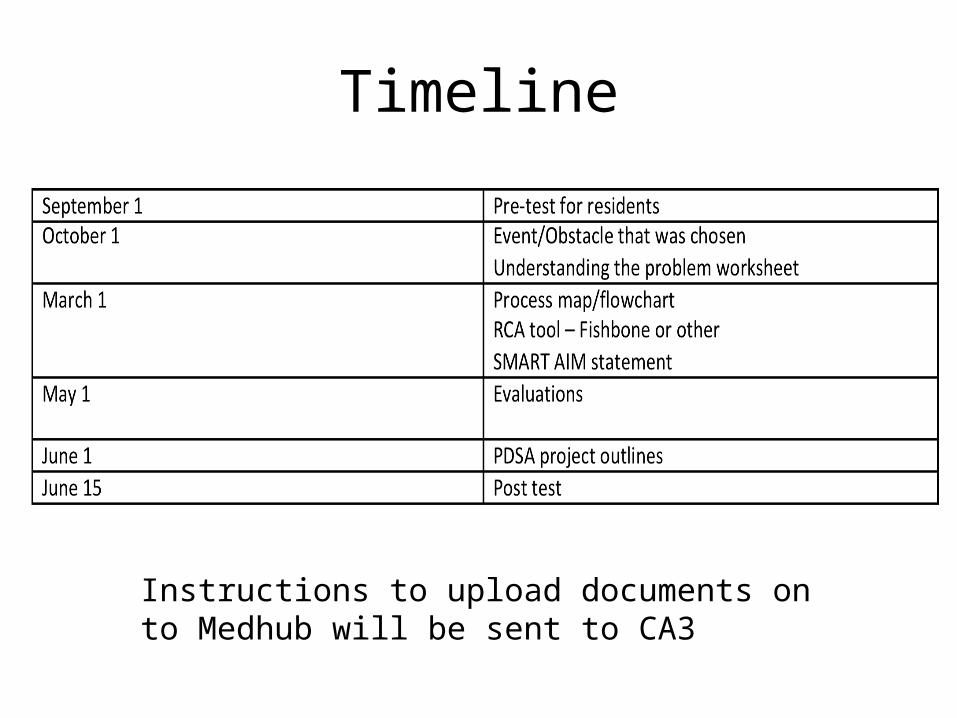
Timeline
Instructions to upload documents on to Medhub will be sent to CA3

A plea from me….• Be patient with us….new curriculum and we know there
will be issues• Feedback!!! Please let us know issues that arise throughout
the year and at the end of the year when you get a SURVEY• Ask for help!
– Handbook lists people resources who can get you in touch with more resources
– Faculty fill in…..– Teamwork issues
• Evaluations at end of year– Teammates– Process– Mentors and Mentees