Embed Size (px)
Citation preview

Chief Advisor: Dr. Jagdish Prasad, Director General of Health Services, Editorial Board: Dr. N.K. Agarwal, Deputy Director General (O) & Ms. Sujaya Krishnan, Joint Secretary (NPCB), Ministry of Health and Family Welfare, Dr. A.S. Rathore, Assistant Director General (O), Ms. Gayatri Mishra, Director (NCD), Dr. V. K. Tewari, Health Education Officer (NPCB), Dr. V. Rajshekhar, Eye Specialist, Safdarjung Hospital/MOHFW, Dr. Suman, Temporary Professional (NPCB) and Shri K.K. Jhell, Under Secretary (NCD).
NPCB-India is a quarterly newsletter of the National Programme for Control of Blindness. For further information contact or write: Dr. V. K. Tewari, Health Education Officer, 342-B, A Wing, Nirman Bhawan, New Delhi-110 108. Telefax: 011-23063875 Email: [email protected]
Designed & Printed by: ESSENCE ADVERTISING SERVICES, 45, 1st Floor, Corner Market, Malviya Nagar, New Delhi-110 017 (Quantity of Newsletter: 10,000 nos.)
QUARTERLY
INDIANPCBNPCBNPCBNPCB
QUARTERLY October - December 2011
Theme of the Issue: Quality Aspects of Cataract Operations
From Editor's Desk It has been more than thirty years since the inception of National Programme
for Control of Blindness (NPCB) in 1976, which has resulted in remarkable
gains and successes on every aspect in our country. Survey conducted by (1)
MoH&FW during the year 2006-07 revealed that prevalence of blindness has
come down from 1.4% to 1%. Along with other causes Blindness, cataract still
remains the major challenge, constituting 62.6% of total blindness, due to
raised awareness, increased longevity of life and increasing population. Since
surgical intervention is involved, quality issues are attached with the
programme. It is really unfortunate that cataract surgeries were also reported
as one of the reasons for blindness in National survey on, “Blindness & (2)visual outcomes after cataract surgery” conducted in 2001-02. Along
with achievement of target quantum wise, improvement in quality of cataract
surgery is also one of the prime objectives of the programme.
INBOX FEEDBACK / RESPONSE
Articles in Hindi Language should be included in this Quarterly issue. The postal address should be exact.
Dr. P.C. Dwivedi,Prof. of Ophthalmology,
D2-8, Doctors Colony, GMH Campus, Rewa, (M.P.)Email: [email protected]
Sir, it is an asset for medical colleges. It is heartening to see such commitment of NPCB organization, interesting. It keeps us update of various programs being done in far flung areas. Thanks a lot of all basic information.
Dr. Mrs. P. SadhotraProf. & Head. Deptt. of Ophthalmology ASCMS,
Sidhra. Jammu (JK), Tawi 180017Email: [email protected]
Respected Sir, NPCB Newsletter is an informative quarterly magazine for Indian, through which national data of community ophth. is available. If you give details about superspeciality training institutes, it will be very much helpful to RIO.
Dr. Kamini Mukesh Kumar PrajapatiAssistant Professor, M& J Inst. of ophth & RIO Civil
Hospital, Ahmedabad-16Email: [email protected]
It was also observed that there was a direct entry to the eye OT from corridor, and labour room was also situated near by to the eye OT. All surgeries were performed by a fresh MS eye surgeon while senior surgeon was out of the town.
2. Eye mishap at Indore Eye Hospital: Indore eye Hospital Society, Madhya Pradesh conducted two eye camps (Sarwas and Sonkatch) at Dewas and one eye camp at Mhow in Indore District. Cataract surgery was performed on 197 patients on 16th, 22nd and 30th December, 2010. Out of all operated cases 18 patients developed post operative endophthalmitis. It was found that water used for scrubbing was infected with Klebsella organisms.
3. Community Health Centre, Balod, District Chhatisgarh:An eye camp was organized by Indian Medical Association from 20-31 September, 2011 at Community Health Centre, Balod district Chhatisgarh in which 334 patients were operated for Cataract, 46 patients developed infection out of which 2 had been advised operation,6 for cataract surgery in other eye after 4 week & 3 for immediate cataract operation. On investigation it was found that pseudomonas bacteria was responsible for infection and same was also found in OT trolley, OT table and OT almirah. Failure of autoclave was reported by the inspection team, as also laxity in observing other universal O.T. precaution while conducting surgery on a mass basis.
Eye Check-up Campaign during "World Sight Day"Awareness Speech to a Self Help Group during "World Sight Day"
Shri S. GandhiselvanHon’ble Minister of State
for Health & Family Welfare
Shri Ghulam Nabi AzadHon’ble Union Minister
of Health & Family Welfare
Shri Sudip BandyopadhyayHon’ble Minister of State
for Health & Family Welfare
thWORLD SIGHT DAY – 13 October '2011“Eye Care f r All”
Prime Activities of NPCBInfrastructure Development,
ØDevelopment of Regional Institutes of Ophthalmology (RIO),
ØDevelopment of Medical Colleges, District Hospitals, Sub-district Hospitals &
vision centers by providing Financial support and Guidance
Grant-in-Aid to States for implementing NPCB activities.
Provision of Eye Care Professionals for States on Contractual basis,
Training of Eye Surgeons in Various disciplines of Ophthalmology,
Training of Paramedical Ophthalmic Assistant, Accredited Social Health Activists
& Nurses all over the country.
Technical Research to improve services.
Celebration of key events like National Eye Donation Fortnight, World Sight Day,
World Glaucoma Day etc.
Services given to General Public all over India, free of cost:Cataract Surgery with Intra Ocular Lens (IOL),
Screening and Provision of spectacles to school children with Refractive
Error,
Collection of Donated Eyes (Cornea) and Keratoplasty for Corneal blind
persons,
Screening for Diabetic Retinopathy and Laser Treatment for affected
persons,
Screening for Glaucoma and Medical & Laser Treatment of those
suffering,
Detection and Treatment of Childhood Blindness, Trachoma etc, and
Providing primary Eye Care Services for all, including rural folk/poor.
NATIONAL PROGRAMME FOR CONTROL OF BLINDNESSMinistry of Health & Family Welfare,
Nirman Bhawan, New Delhi – 110 108. www.mohfw.in/npcb.nic.in
If you are over 40 years of age and have a family history of Diabetes or Glaucoma, you MUST get your Eyes check up done at
least once a year.
For more information, please contact Primary Health Center, District Hospital, Medical College

22 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIANATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA 7NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Quality issues in Cataract surgeries:
5000000
5404406
6000000
5810336
6000000
5942578
6000000
6031678
7000000
1954200
0
1000000
2000000
3000000
4000000
5000000
6000000
7000000
8000000
2007-08 2008-09 2009-10 2010-11 2011-12*
Target
Achievement
Year
Nu
mb
er
of
cata
ract
su
rgeri
es
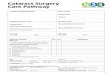
Fig 1: Cataract surgeries performed during last five year period:
Prevalence of cataract in India: Considering current population (121crore) of India as per census 2011, 1% blindness (vision 6/60 or <6/60) constitutes approximately 1crore 21 lakhs. Out of this approximately 62% i.e. 72 lakhs (7.2 million) are blind due to cataract. As per NPCB incidence of cataract is 0.4 to 0.5 % thus the no. of new cases of cataract to be operated upon each year comes to 61.5 lakhs (6.15 million).
Estimation of Cataract surgical load: Approximately 7 million people are / become blind due to cataract at any point of time (prevalence) and 6.15 million cataract cases are added each year (Incidence). India is performing 6 million cataract surgeries every year and to minimize the existing backlog NPCB has targeted 7 million cataract surgeries for the current financial year (2011-12). NPCB's first target is mature bilateral cataract cases that can cause blindness if left untreated. Most of the new immature cataract cases are those who can afford to wait for cataract surgery for at least six months or more.
NPCB has done a commendable job in the cataract surgical field. NPCB is achieving its target of cataract surgeries year after year by performing approximately 60 lakh surgeries each year. During year 2010-11 NPCB performed 60 lakh
thsurgeries, thus meeting the targets. Given below is the chart showing the cataract surgeries performed during 11 five year plan. IOL implantation has gone up above 95%.
However since surgical interventions are involved there are some prerequisites for this surgery based programme. These are as follows:
1. Availability of good Screening and diagnostic equipments
2. Dedicated Eye Wards/ Eye OT
3. Fully trained surgical team
4. Modern surgical machines and instruments and intra operative patient care
5. Full asepsis at all levels to prevent post operative infection
6. High quality pre-sterilized drugs and surgical consumables
7. High quality post operative eye and general eye care
Role of NPCB to cover each of the above aspects1. To equip our eye care hospitals, Medical colleges and Regional Institutes of Ophthalmology with modern technology
and equipments NPCB provides grant in aid of ` 20 lakh to District hospitals and ` 40 lakh to Medical Colleges and RIOs respectively.
2. Along with it NPCB provide grant in aid for strengthening of District Hospitals/ sub district hospitals / PHCs /CHC / Vision Centres, Eye Banks and Eye Donation Centres.
3. NPCB grants ` 5 lakh for maintenance of equipments.
4. Supports the state to build exclusive eye OTs @ ` 75 lakhs. Guidelines for construction of dedicated Eye Wards/Eye OTs are available on NPCB website i.e. www.npcb.nic.in
5. Training of manpower – Eye surgeons, PMOAS, and other paramedics.
Factors leading to poor sterility and post operative infection
Management of Post operative Endophthalmitis (POE):
Mass Eye infection reports and their analysis:
Post operative Endophthalmitis (POE) is defined as a severe inflammation involving both the anterior and posterior segments of the eye secondary to an infection.
The prognosis in postoperative endophthalmitis depends on the virulence of the microorganisms and early intervention. For early recognition of postoperative infection, frequent postoperative follow up at 24 hours, 72 hour and 7 days is necessary. Every follow up examination comprises of recording visual acuity, slit lamp biomicroscopic examination and looking for media clarity with an indirect Ophthalmoscope and B –Scan Ultrasonography to know the extent of vitreous cavity involvement. After the clinical diagnosis of endophthalmitis is made, the further management depends on the presenting visual acuity and the microbiological spectrum as well as ultrasonography report.
Data from the Endophthalmitis Vitrectomy Study (EVS) indicates that initial management for patients who meet EVS entry criteria should include 3 port pars plana vitrectomy if patients present with vision worse than hand motions, but that an initial vitreous tap/biopsy with intravitreal antibiotics should generally be sufficient if presenting vision is hand motions or better. Systemic antibiotics were not found be of much benefit in this study.
Though EVS did provide general guidelines for treatment of endophthalmitis, clinicians should individualise treatment for each patient based on the clinical course, signs and symptoms.
Once a clinical diagnosis of acute bacterial endophthalmitis made, it is to be considered as a medical emergency requiring:! Immediate vitreal tap for culture and sensitivity and instillation of intravitreal antibiotics. ! Intravitreal antibiotics which is commonly used include Vancomycin (1 mg/0.1ml) and Ceftazidime (2.25mg/0.1ml)
because 94% of the culture positive cases are caused by gram positive organisms which are 100% sensitive to Vancomycin and 6% of culture positive cases are by gram negative group of organisms which are 90% sensitive to Ceftazidime.
! Admit to hospital for observation and treatment.! Intensive fortified antibiotics e.g Vancomycin and tobramycin 1hrly.! Atropine 1% qid.
The indications for pars plana vitrectomy are ! Perception of light or worse at presentation.! Deterioration or no improvement despite intravitreal antibiotics.! Delayed onset endophthalmitis.! Fungal endophthalmitis.
For more advance treatment, a posterior segment specialist should be contacted immediately.
1. Mandala, MP: A total 113 cataract patients were operated upon in September, 2010 from 10-16 september. All surgeries were conducted in Yogiraj Hospital which is managed by strategic concept pvt. ltd. and is a registered hospital. On investigation it was found that hospital had not taken permission from Health Department. After getting reports a central team visited the place and carried out detail investigation. It was found that total 38 patients lost their eye and out of which 30 patients were eviscerated in Yogiraj hospital on 13.9.2010. Despite reporting of pain, redness, pus discharge and no improvement in sight by 20 patients who were operated upon starting 11.9.2011, surgeries were continued till 16.9.2010. All eviscerated patients were not informed about removal of the operated eye.
Instrumental and Consumables factorsSpecial attention should be paid to:• Not checking indicator tapes
(autoclave, ETO etc)• Not checking irrigating fluid for
particulate matter/ presence and concentration of antibiotic
• Tubular instruments• Devices with ant peristaltic pumps
and reflux mechanisms • Ensure suction bottle is empty• Linen is soaked with moisture, still
using it.• Sterility of any instrument or object
is doubtful still using it.
Surgeon factors• Exposed scalp hair and nostrils• Operating inspite of having an open wound or URI/
skin infection• Improperly scrubbed hands• Ungloved hands• Wearing fluid soaked/ wet gown• Inadvertently touching an unsterile area but not
changing gloves• Same irrigation line used for several surgeries• Reusing instruments from trolley of another patient
directly• Reusing dropped instrument or IOL without
adequate resterlization• Predisposing eye to infection by leaving wound gape,
exposed suture knots,& vitreous wick
Patient preparation• Operating on Patient having
adnexal & ocular surface infection, presence of active systemic septic foci at the time of surgery
• Unclean patient attire and exposed scalp
• Improper surgical preparation• Not washing conjunctival sac
thoroughly before surgery

36 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Dictums to be followed to ensure quality cataract surgeryDictums-Pre-operativeEvaluate Your infrastructureKnow well Your MachinesProcure What is lackingCheck The quality of consumablesEngage An anaesthetist for monitored anaesthesia surgery whenever requiredInstruct Your associates well about the kind of service you expect from themEnsure Proper sterilization of OT/OT materialObserve All universal precautionsKeep All relevant recordsDictums-Intra-operativeLearn Fully well the technique before trying on a patient Have the Presence of a senior, conversant with the techniqueSeek help If complication has occurred, don't try to hide itEnsure Presence of minimum support staffMaintain Adequate supply of consumables/non consumables in OT premises Dictums-Post-operativeProvide Adequate space for post-OP recoveryRemain Vigilant in the post -operative periodCheck Vision on regular basisDeliver Best corrected visionKeep Records of technique/materialsContemplate If complication has occurredAdmit Your deficiencies/mistakesRectify Defects/Improve technique
Waste Disposal: All doctors and staff should get training in handling of biomedical waste material.Segregation:! Sharps to be disposed separately after disinfection with
sodium hypochloride.! Gowning and gloving after scrubbing by no touch
technique after each case.! Infected material to be handled only by gloved staff.
Post operative instructions to the patient and the (5)attendant
! Do not lift the heavy weight.! Do not stoop or bend.! Do not touch the operated eye with bare hands.! Avoid head bath for 1-4 weeks, depending upon
technique used for cataract surgery.! Face can be cleaned with wet cloth. Shaving allowed.
Avoid vigorous shaking of head and exercises like yogasans, jogging etc.
! Avoid dirty and crowded places.! Avoid smoking, alcoholic drinks and usages of snuff.
There are no special diet restrictions.! In case of cough or constipation, consult a physician for
treatment.! Use dark glasses outdoors. The dark glasses should
have side shields.! The eye should be cleaned by an attendant in the
manner as shown by the surgeon, twice daily.! Use medications as prescribed by the treating surgeon.Deciding factors for minimum complications! How well the operating surgeon knows the technique
being used by him/her.
! If fresh in technique, any guide available.! Ability to recognize a complication at an early stage.! Any help available in case of mishap.! Infrastructure in terms of OT/surrounding area layout.! Working of machine, proper understanding by support
team.! Sterilization of all components of machines,
instruments.! Quality and sterility of all consumables used during
surgery.! Post operative care by surgical team.! Observance of precautions by patient.
Barriers in attainment of best visual acuity (Post cataract / cataract IOL surgery)! Corneal diseases! IOL defect/Displacement/deposits! Vitreous opaciies! Chorio-Retinal diseases! Optic disc defects! Visual pathway defects
References: 1. MoH & FW(NPCB). Rapid assessment of Avoidable Blindness- India.
Report-2006-07
2. MoH & FW (NPCB). National Survey on Blindness and Visual
Outcomes after Cataract Surgery . A report -2001-02
3. NPCB – Guidelines for pre-operative, operative and post-operative
precautions for Eye surgery. .
4. NPCB – General Precautions to safeguard against post-operative
Infections following Ophthalmic Surgery.
5. Dr. Jacob Mathew, Dr. Minu M. Mathen. Quality Assurance in Cataract
Surgery. Page : 21
www.npcb.nic.in
Major activities of NPCB done during the quarter:! World sight day (WSD) was celebrated in the entire country on 2nd Thursday of October i.e.
on 13th Oct, 2011. The theme for this year was “Eye care for all”. The celebration of WSD was held at Udaipur, wherein a seminar on Eye Care Delivery was conducted by Vision 2020 in collaboration with Alakh Nayan Mandir. Ms. Sujaya Krishnan, Joint Secretary, NPCB and Dr. N.K. Agarwal, DDG(O), NPCB attended and made presentation.
! WSD was also observed in UT Puduchhery. Community was made aware about general eye care by displaying educational material having message about general eye care (at schools, PHCs / CHCs, District Hospital & Medical College), distributing pamphlets, delivering health talks and telecasting educational messages at local cable TV. State Programme Officer also delivered health talks on general eye care at PHCs in rural areas. NPCB team visited special school for the visually impaired students and examined all the students. NPCB team also conducted screening camps for Diabetic Retinopathy and Glaucoma at 10 PHCs in rural areas.
! A workshop on Kalyani Video Magzine Programme (KVMP) was organized at Goa on 31st October & 1st November, 2011. Ms. Sujaya Krishnan, Joint Secretary NPCB and Dr. V. K. Tewari, Health Education Officer attended the workshop along with eight producers of KVMP and provided valuable inputs for further improvement in the production of KVMP.
NPCB participated in the International Trade Fair (IITF) from November 14-27, 2011 at Pragati Maidan, New Delhi. Along with display of educational material, screening of eye was done with undilated pupils in a specialized way to detect cataract, Glaucoma and Diabetic Retinopathy. It was highly appreciated by the visiting team from Ministry of Health & Family Welfare and the general public.
To cover requisite number NPCB has empanelled 30 training Institutes which provide trainings to the Govt. ophthalmic surgeons. In order to enable eye surgeons to keep abreast with the advancements in the field of ophthalmology, NPCB trains 400 eye surgeons annually. Under this scheme the Eye Surgeons from Sub-District Hospitals, District Hospitals, Medical Colleges / RIOs, whose names have been recommended by the State Programme Officer (NPCB), are being trained in the various fields of ophthalmology. ` 55,000 to 70,000 per trainee is being paid to the training institutes to meet training material, T/A, D/A and other expanses. (Refer to page 72-73 of NPCB guidelines for State and district Health society on NPCB website www.npcb.nic.in ) for more detailed information.
6. To ensure quality, full asepsis NPCB has laid down guidelines which are available on NPCB website i.e. www.npcb.nic.in. refer to page 5 for detail instructions.
NPCB has instructed State Programme officers and District Programme managers that they are not to overlook any of the universal precautions, those specially pertaining to intraocular surgery in their zeal to achieve the given targets. Their attempt should be focused on organizing all the existing workforce in the state together like the NGOs, private eye hospitals, private practitioners in addition to the existing Medical Colleges, District Hospitals and Sub District Hospitals to create more avenues for performing the cataract surgery. As regards the Eye surgeons present in the District Hospitals, Sub District Hospital and Medical Colleges there should be some guidelines for performing a minimum number of cataract surgeries in addition to super specialty work.
NPCB has laid down guidelines for surgical work as well as for construction of dedicated eye wards and operation theatres, which are available on NPCB website (www.npcb.nic.in). Refer to page number 6 for eye OT layout.
How to ensure quality cataract Surgery:
Role of State Programme Managers and HODs in Medical Colleges in assuring quality cataract surgeries:! Ensuring the experience of District eye surgeon/NGO in providing eye care services.
! Checking whether all necessary equipments and drugs and consumables for the cataract surgery are available or not.
! Whether operation theatre mentioned is well maintained and thoroughly sterilized as per the guidelines before each surgical procedure
! Whether District Hospital/NGO has adequate trained manpower to handle the workload.
! Previous history of the operating surgeon and the NGO.
! Random checks to assess the validity of reported data, status of follow up and patient satisfaction.

54 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA
(3)Guidelines regarding Operation Theatre Layout Level-I • Restricted entry for patients and medical and para-medical Staff
Level-II • Changing room for medical * Para-medical staff & Preparation of patients• Caps / mask to be worn• Air conditioning must be there (with HEPA filters)• Scrub room/gloving and gowning
Level-III • Sterile area (Separate Slippers)• Entry restricted to patients, Medical & para-medical staff, trolleys etc.• Fumigated areas with air lock / AC• Ultra Violet light at night if possible• Floor, walls, surface, to be scrubbed and carbolized• Air conditioning with HEPA filters (filter optional)
Level-IV • Fully sterilized OTs• Scrub rooms• Instrument maintenance (under supervision of the staff Sisters/OT Technicians) • Clean & washed with Savlon/soap.• Ultrasonic cleaning.• Examined under magnification for defect /repair/packing for sterilization.
! Hands always above waist and elevated so that water drains away from hand.
(3):Intra-operative Precautions ! A drop of betadine before starting the surgery.! Minimal handling of tissues.! Instruments meant for extraocular manipulations not
to be used inside the eyes.! No wick left in to the anterior chamber / uvea/ capsule/
vitreous and complete removal and formation of anterior chamber with irrigating fluid/ air.
! No foreign material should be left in the surgical area.(3)Post operative
! S u b - c o n j u n c t i v a l antibiotics to be given in the conjunctival sac after completion of surgery.
! In case of adnexal infection, use systemic antibiotics
! Topical antibiotics in association with anti inflammatory steroidal or NSAIDS.
! Dilating drops once daily to keep pupil mobile.! Thorough eye check up must be done post operatively
on every patient before discharging them from the hospital.
! Personal hygiene to be looked after, avoidance of dust, smoke and sunlight must be kept in mind.
! Wear protective dark glasses outdoors.! Frequent visits to the eye care facility to detect any
complication.! Frequent instillation of eye drops and adherence to the
treatment advised.
Operating surgeon has to be extremely vigilant against all sorts of ocular infections occurring within 24-48 hrs after surgery particularly so when surgery is being performed in eye camp settings even though the camp is being held within the permitted premises like District Hospital Eye operation theatre. As soon as there is even a hint of some sort of infection having taken place even in 1-2 patients out of a lot of five or more cases, further surgery must be immediately suspended and the OT shut to prevent a mass catastrophy.
All efforts must be made to find out the causative organism, source of infection, culture and sensitivity pattern of the organism and treatment of infected persons must be started immediately to salvage their vision. Also visual acuity improvement from the next day onwards from the day of operation is an all time parameter to be followed to ensure the quality of the cataract surgery having been performed.
Importance must be given to other symptoms associated with ocular infection such as pain in eye, headache, redness, lacrimation, photophobia, fever etc. in addition to no recovery of vision.
NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Standard outlay of Operation Theatre
Level-I Level-II Level-III Level-IV
Preparation of the Patient for operation theatre:! S y s t e m i c p r o p hy l a c t i c
antibiotics 1-2 days preceding surgery should be given.
! Ciprofloxacin or Tobramycin eye drops four times a day should be instilled in the eyes.
! Adequate facial wash with antiseptic soap on the preceding night and painting of periocular skin with betadiene solution should be done on the preceding night and morning of surgery.
Instructions for the Personnel and other operation (4)room aspects
! General health & hygiene of the personnel working in the operation theatre should be ensured. Person having Upper Respiratory tract Infection (URI), infection of eyes, skin, ears or mouth should not be allowed to work in the OT.
! Dress code should be strictly followed as per the instructions.
! Everyone should wear clean OT dress.(3)Sterlization of Operation Theatre :
! OT to be washed / scrubbed before use and surface carbolized.
! Fumigation at frequent time intervals or after an infected case has been done/ large volume cases operated.
! Bi-weekly cultures of the OT to be sent from specified points of the OT.
! Ultraviolet light is recommended for overnight use.! Infected cases to be done in a separate OT. Extra
ocular surgery cases to be taken preferably after intra-ocular surgery cases are over.
Cleaning and draping: ! Spirit and betadine from inwards to outwards (at least
twice).! Special note of eyebrow/ medial canthus and nasal area.! Draping to isolate the eye; no drape should used again
on next patient.! Eye to be washed with betadine 5% and BSS.Surgical Scrubbing:! Water used for scrubbing
should be bacteria free. Off & on culture of water being used must be done.
! Cleaning agent used for scrubbing should be of proven efficacy like antiseptic scrub gel, soap, Iodine enriched sponge etc.
! To proceed in a methodical manner from distal to proximal.
! Hands/ Palms/Fingers/Medial, lateral, dorsal, ventral aspects.
! Nail bed to be scrubbed with nail brush.! Fore-arm- medial, lateral, anterior, posterior up to
beyond elbow.! Scrubbing from distal to proximal.
Patient should be instructed to consult his doctor immediately in case of! Excessive watering, discharge, pain and
sudden marked redness! Lid swelling! Sudden blurring/ decreased or loss of
vision! Floaters and flashes! Excessive photophobia
Pre operative, intra operative and post operative guidelines:There are certain preoperative, intra-operative and postoperative precautions which need to be ensured prior to performing, during and after any surgery.
(3)Pre-operative precautions :! Along with complete physical examination by physician, check up for systemic illness like diabetes Mellitus,
hypertension & pre-existing, known cardiovascular complications, chronic obstructive pulmonary diseases (COPD), and renal diseases, must be done.
! All necessary investigations like BP, ECG, Complete haemogram, and urine examination (R/M, albumin) should be done.! Mandatory ocular examination to be done as per guidelines.! Keratometry and biometry to be done as per NPCB guidelines to calculate accurate IOL power.! Consumable items lots like gloves, eye wash fluid, methylcellulose, intra ocular lens should be subjected to culture and
sensitivity before use, particularly in a mass surgery setting
FromWard
Common areaRelatives/Patients
waiting patients
Restricted entry
Patient
Trolley etc.
Pre-anaesthesiaroom
Open to Sky
ScrubArea OT-I
Inner Corridor
ScrubArea
OT NurseChanging room (CR)
ParaMedical staff
CRCR
Doctor
Doctors
Open to Sky Store
Store
Store
OT-II

54 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA
(3)Guidelines regarding Operation Theatre Layout Level-I • Restricted entry for patients and medical and para-medical Staff
Level-II • Changing room for medical * Para-medical staff & Preparation of patients• Caps / mask to be worn• Air conditioning must be there (with HEPA filters)• Scrub room/gloving and gowning
Level-III • Sterile area (Separate Slippers)• Entry restricted to patients, Medical & para-medical staff, trolleys etc.• Fumigated areas with air lock / AC• Ultra Violet light at night if possible• Floor, walls, surface, to be scrubbed and carbolized• Air conditioning with HEPA filters (filter optional)
Level-IV • Fully sterilized OTs• Scrub rooms• Instrument maintenance (under supervision of the staff Sisters/OT Technicians) • Clean & washed with Savlon/soap.• Ultrasonic cleaning.• Examined under magnification for defect /repair/packing for sterilization.
! Hands always above waist and elevated so that water drains away from hand.
(3):Intra-operative Precautions ! A drop of betadine before starting the surgery.! Minimal handling of tissues.! Instruments meant for extraocular manipulations not
to be used inside the eyes.! No wick left in to the anterior chamber / uvea/ capsule/
vitreous and complete removal and formation of anterior chamber with irrigating fluid/ air.
! No foreign material should be left in the surgical area.(3)Post operative
! S u b - c o n j u n c t i v a l antibiotics to be given in the conjunctival sac after completion of surgery.
! In case of adnexal infection, use systemic antibiotics
! Topical antibiotics in association with anti inflammatory steroidal or NSAIDS.
! Dilating drops once daily to keep pupil mobile.! Thorough eye check up must be done post operatively
on every patient before discharging them from the hospital.
! Personal hygiene to be looked after, avoidance of dust, smoke and sunlight must be kept in mind.
! Wear protective dark glasses outdoors.! Frequent visits to the eye care facility to detect any
complication.! Frequent instillation of eye drops and adherence to the
treatment advised.
Operating surgeon has to be extremely vigilant against all sorts of ocular infections occurring within 24-48 hrs after surgery particularly so when surgery is being performed in eye camp settings even though the camp is being held within the permitted premises like District Hospital Eye operation theatre. As soon as there is even a hint of some sort of infection having taken place even in 1-2 patients out of a lot of five or more cases, further surgery must be immediately suspended and the OT shut to prevent a mass catastrophy.
All efforts must be made to find out the causative organism, source of infection, culture and sensitivity pattern of the organism and treatment of infected persons must be started immediately to salvage their vision. Also visual acuity improvement from the next day onwards from the day of operation is an all time parameter to be followed to ensure the quality of the cataract surgery having been performed.
Importance must be given to other symptoms associated with ocular infection such as pain in eye, headache, redness, lacrimation, photophobia, fever etc. in addition to no recovery of vision.
NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Standard outlay of Operation Theatre
Level-I Level-II Level-III Level-IV
Preparation of the Patient for operation theatre:! S y s t e m i c p r o p hy l a c t i c
antibiotics 1-2 days preceding surgery should be given.
! Ciprofloxacin or Tobramycin eye drops four times a day should be instilled in the eyes.
! Adequate facial wash with antiseptic soap on the preceding night and painting of periocular skin with betadiene solution should be done on the preceding night and morning of surgery.
Instructions for the Personnel and other operation (4)room aspects
! General health & hygiene of the personnel working in the operation theatre should be ensured. Person having Upper Respiratory tract Infection (URI), infection of eyes, skin, ears or mouth should not be allowed to work in the OT.
! Dress code should be strictly followed as per the instructions.
! Everyone should wear clean OT dress.(3)Sterlization of Operation Theatre :
! OT to be washed / scrubbed before use and surface carbolized.
! Fumigation at frequent time intervals or after an infected case has been done/ large volume cases operated.
! Bi-weekly cultures of the OT to be sent from specified points of the OT.
! Ultraviolet light is recommended for overnight use.! Infected cases to be done in a separate OT. Extra
ocular surgery cases to be taken preferably after intra-ocular surgery cases are over.
Cleaning and draping: ! Spirit and betadine from inwards to outwards (at least
twice).! Special note of eyebrow/ medial canthus and nasal area.! Draping to isolate the eye; no drape should used again
on next patient.! Eye to be washed with betadine 5% and BSS.Surgical Scrubbing:! Water used for scrubbing
should be bacteria free. Off & on culture of water being used must be done.
! Cleaning agent used for scrubbing should be of proven efficacy like antiseptic scrub gel, soap, Iodine enriched sponge etc.
! To proceed in a methodical manner from distal to proximal.
! Hands/ Palms/Fingers/Medial, lateral, dorsal, ventral aspects.
! Nail bed to be scrubbed with nail brush.! Fore-arm- medial, lateral, anterior, posterior up to
beyond elbow.! Scrubbing from distal to proximal.
Patient should be instructed to consult his doctor immediately in case of! Excessive watering, discharge, pain and
sudden marked redness! Lid swelling! Sudden blurring/ decreased or loss of
vision! Floaters and flashes! Excessive photophobia
Pre operative, intra operative and post operative guidelines:There are certain preoperative, intra-operative and postoperative precautions which need to be ensured prior to performing, during and after any surgery.
(3)Pre-operative precautions :! Along with complete physical examination by physician, check up for systemic illness like diabetes Mellitus,
hypertension & pre-existing, known cardiovascular complications, chronic obstructive pulmonary diseases (COPD), and renal diseases, must be done.
! All necessary investigations like BP, ECG, Complete haemogram, and urine examination (R/M, albumin) should be done.! Mandatory ocular examination to be done as per guidelines.! Keratometry and biometry to be done as per NPCB guidelines to calculate accurate IOL power.! Consumable items lots like gloves, eye wash fluid, methylcellulose, intra ocular lens should be subjected to culture and
sensitivity before use, particularly in a mass surgery setting
FromWard
Common areaRelatives/Patients
waiting patients
Restricted entry
Patient
Trolley etc.
Pre-anaesthesiaroom
Open to Sky
ScrubArea OT-I
Inner Corridor
ScrubArea
OT NurseChanging room (CR)
ParaMedical staff
CRCR
Doctor
Doctors
Open to Sky Store
Store
Store
OT-II

36 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Dictums to be followed to ensure quality cataract surgeryDictums-Pre-operativeEvaluate Your infrastructureKnow well Your MachinesProcure What is lackingCheck The quality of consumablesEngage An anaesthetist for monitored anaesthesia surgery whenever requiredInstruct Your associates well about the kind of service you expect from themEnsure Proper sterilization of OT/OT materialObserve All universal precautionsKeep All relevant recordsDictums-Intra-operativeLearn Fully well the technique before trying on a patient Have the Presence of a senior, conversant with the techniqueSeek help If complication has occurred, don't try to hide itEnsure Presence of minimum support staffMaintain Adequate supply of consumables/non consumables in OT premises Dictums-Post-operativeProvide Adequate space for post-OP recoveryRemain Vigilant in the post -operative periodCheck Vision on regular basisDeliver Best corrected visionKeep Records of technique/materialsContemplate If complication has occurredAdmit Your deficiencies/mistakesRectify Defects/Improve technique
Waste Disposal: All doctors and staff should get training in handling of biomedical waste material.Segregation:! Sharps to be disposed separately after disinfection with
sodium hypochloride.! Gowning and gloving after scrubbing by no touch
technique after each case.! Infected material to be handled only by gloved staff.
Post operative instructions to the patient and the (5)attendant
! Do not lift the heavy weight.! Do not stoop or bend.! Do not touch the operated eye with bare hands.! Avoid head bath for 1-4 weeks, depending upon
technique used for cataract surgery.! Face can be cleaned with wet cloth. Shaving allowed.
Avoid vigorous shaking of head and exercises like yogasans, jogging etc.
! Avoid dirty and crowded places.! Avoid smoking, alcoholic drinks and usages of snuff.
There are no special diet restrictions.! In case of cough or constipation, consult a physician for
treatment.! Use dark glasses outdoors. The dark glasses should
have side shields.! The eye should be cleaned by an attendant in the
manner as shown by the surgeon, twice daily.! Use medications as prescribed by the treating surgeon.Deciding factors for minimum complications! How well the operating surgeon knows the technique
being used by him/her.
! If fresh in technique, any guide available.! Ability to recognize a complication at an early stage.! Any help available in case of mishap.! Infrastructure in terms of OT/surrounding area layout.! Working of machine, proper understanding by support
team.! Sterilization of all components of machines,
instruments.! Quality and sterility of all consumables used during
surgery.! Post operative care by surgical team.! Observance of precautions by patient.
Barriers in attainment of best visual acuity (Post cataract / cataract IOL surgery)! Corneal diseases! IOL defect/Displacement/deposits! Vitreous opaciies! Chorio-Retinal diseases! Optic disc defects! Visual pathway defects
References: 1. MoH & FW(NPCB). Rapid assessment of Avoidable Blindness- India.
Report-2006-07
2. MoH & FW (NPCB). National Survey on Blindness and Visual
Outcomes after Cataract Surgery . A report -2001-02
3. NPCB – Guidelines for pre-operative, operative and post-operative
precautions for Eye surgery. .
4. NPCB – General Precautions to safeguard against post-operative
Infections following Ophthalmic Surgery.
5. Dr. Jacob Mathew, Dr. Minu M. Mathen. Quality Assurance in Cataract
Surgery. Page : 21
www.npcb.nic.in
Major activities of NPCB done during the quarter:! World sight day (WSD) was celebrated in the entire country on 2nd Thursday of October i.e.
on 13th Oct, 2011. The theme for this year was “Eye care for all”. The celebration of WSD was held at Udaipur, wherein a seminar on Eye Care Delivery was conducted by Vision 2020 in collaboration with Alakh Nayan Mandir. Ms. Sujaya Krishnan, Joint Secretary, NPCB and Dr. N.K. Agarwal, DDG(O), NPCB attended and made presentation.
! WSD was also observed in UT Puduchhery. Community was made aware about general eye care by displaying educational material having message about general eye care (at schools, PHCs / CHCs, District Hospital & Medical College), distributing pamphlets, delivering health talks and telecasting educational messages at local cable TV. State Programme Officer also delivered health talks on general eye care at PHCs in rural areas. NPCB team visited special school for the visually impaired students and examined all the students. NPCB team also conducted screening camps for Diabetic Retinopathy and Glaucoma at 10 PHCs in rural areas.
! A workshop on Kalyani Video Magzine Programme (KVMP) was organized at Goa on 31st October & 1st November, 2011. Ms. Sujaya Krishnan, Joint Secretary NPCB and Dr. V. K. Tewari, Health Education Officer attended the workshop along with eight producers of KVMP and provided valuable inputs for further improvement in the production of KVMP.
NPCB participated in the International Trade Fair (IITF) from November 14-27, 2011 at Pragati Maidan, New Delhi. Along with display of educational material, screening of eye was done with undilated pupils in a specialized way to detect cataract, Glaucoma and Diabetic Retinopathy. It was highly appreciated by the visiting team from Ministry of Health & Family Welfare and the general public.
To cover requisite number NPCB has empanelled 30 training Institutes which provide trainings to the Govt. ophthalmic surgeons. In order to enable eye surgeons to keep abreast with the advancements in the field of ophthalmology, NPCB trains 400 eye surgeons annually. Under this scheme the Eye Surgeons from Sub-District Hospitals, District Hospitals, Medical Colleges / RIOs, whose names have been recommended by the State Programme Officer (NPCB), are being trained in the various fields of ophthalmology. ` 55,000 to 70,000 per trainee is being paid to the training institutes to meet training material, T/A, D/A and other expanses. (Refer to page 72-73 of NPCB guidelines for State and district Health society on NPCB website www.npcb.nic.in ) for more detailed information.
6. To ensure quality, full asepsis NPCB has laid down guidelines which are available on NPCB website i.e. www.npcb.nic.in. refer to page 5 for detail instructions.
NPCB has instructed State Programme officers and District Programme managers that they are not to overlook any of the universal precautions, those specially pertaining to intraocular surgery in their zeal to achieve the given targets. Their attempt should be focused on organizing all the existing workforce in the state together like the NGOs, private eye hospitals, private practitioners in addition to the existing Medical Colleges, District Hospitals and Sub District Hospitals to create more avenues for performing the cataract surgery. As regards the Eye surgeons present in the District Hospitals, Sub District Hospital and Medical Colleges there should be some guidelines for performing a minimum number of cataract surgeries in addition to super specialty work.
NPCB has laid down guidelines for surgical work as well as for construction of dedicated eye wards and operation theatres, which are available on NPCB website (www.npcb.nic.in). Refer to page number 6 for eye OT layout.
How to ensure quality cataract Surgery:
Role of State Programme Managers and HODs in Medical Colleges in assuring quality cataract surgeries:! Ensuring the experience of District eye surgeon/NGO in providing eye care services.
! Checking whether all necessary equipments and drugs and consumables for the cataract surgery are available or not.
! Whether operation theatre mentioned is well maintained and thoroughly sterilized as per the guidelines before each surgical procedure
! Whether District Hospital/NGO has adequate trained manpower to handle the workload.
! Previous history of the operating surgeon and the NGO.
! Random checks to assess the validity of reported data, status of follow up and patient satisfaction.

22 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIANATIONAL PROGRAMME FOR CONTROL OF BLINDNESS IN INDIA 7NPCB INDIA NEWSLETTER, OCTOBER - DECEMBER 2011
Quality issues in Cataract surgeries:
5000000
5404406
6000000
5810336
6000000
5942578
6000000
6031678
7000000
1954200
0
1000000
2000000
3000000
4000000
5000000
6000000
7000000
8000000
2007-08 2008-09 2009-10 2010-11 2011-12*
Target
Achievement
Year
Nu
mb
er
of
cata
ract
su
rgeri
es
Fig 1: Cataract surgeries performed during last five year period:
Prevalence of cataract in India: Considering current population (121crore) of India as per census 2011, 1% blindness (vision 6/60 or <6/60) constitutes approximately 1crore 21 lakhs. Out of this approximately 62% i.e. 72 lakhs (7.2 million) are blind due to cataract. As per NPCB incidence of cataract is 0.4 to 0.5 % thus the no. of new cases of cataract to be operated upon each year comes to 61.5 lakhs (6.15 million).
Estimation of Cataract surgical load: Approximately 7 million people are / become blind due to cataract at any point of time (prevalence) and 6.15 million cataract cases are added each year (Incidence). India is performing 6 million cataract surgeries every year and to minimize the existing backlog NPCB has targeted 7 million cataract surgeries for the current financial year (2011-12). NPCB's first target is mature bilateral cataract cases that can cause blindness if left untreated. Most of the new immature cataract cases are those who can afford to wait for cataract surgery for at least six months or more.
NPCB has done a commendable job in the cataract surgical field. NPCB is achieving its target of cataract surgeries year after year by performing approximately 60 lakh surgeries each year. During year 2010-11 NPCB performed 60 lakh
thsurgeries, thus meeting the targets. Given below is the chart showing the cataract surgeries performed during 11 five year plan. IOL implantation has gone up above 95%.
However since surgical interventions are involved there are some prerequisites for this surgery based programme. These are as follows:
1. Availability of good Screening and diagnostic equipments
2. Dedicated Eye Wards/ Eye OT
3. Fully trained surgical team
4. Modern surgical machines and instruments and intra operative patient care
5. Full asepsis at all levels to prevent post operative infection
6. High quality pre-sterilized drugs and surgical consumables
7. High quality post operative eye and general eye care
Role of NPCB to cover each of the above aspects1. To equip our eye care hospitals, Medical colleges and Regional Institutes of Ophthalmology with modern technology
and equipments NPCB provides grant in aid of ` 20 lakh to District hospitals and ` 40 lakh to Medical Colleges and RIOs respectively.
2. Along with it NPCB provide grant in aid for strengthening of District Hospitals/ sub district hospitals / PHCs /CHC / Vision Centres, Eye Banks and Eye Donation Centres.
3. NPCB grants ` 5 lakh for maintenance of equipments.
4. Supports the state to build exclusive eye OTs @ ` 75 lakhs. Guidelines for construction of dedicated Eye Wards/Eye OTs are available on NPCB website i.e. www.npcb.nic.in
5. Training of manpower – Eye surgeons, PMOAS, and other paramedics.
Factors leading to poor sterility and post operative infection
Management of Post operative Endophthalmitis (POE):
Mass Eye infection reports and their analysis:
Post operative Endophthalmitis (POE) is defined as a severe inflammation involving both the anterior and posterior segments of the eye secondary to an infection.
The prognosis in postoperative endophthalmitis depends on the virulence of the microorganisms and early intervention. For early recognition of postoperative infection, frequent postoperative follow up at 24 hours, 72 hour and 7 days is necessary. Every follow up examination comprises of recording visual acuity, slit lamp biomicroscopic examination and looking for media clarity with an indirect Ophthalmoscope and B –Scan Ultrasonography to know the extent of vitreous cavity involvement. After the clinical diagnosis of endophthalmitis is made, the further management depends on the presenting visual acuity and the microbiological spectrum as well as ultrasonography report.
Data from the Endophthalmitis Vitrectomy Study (EVS) indicates that initial management for patients who meet EVS entry criteria should include 3 port pars plana vitrectomy if patients present with vision worse than hand motions, but that an initial vitreous tap/biopsy with intravitreal antibiotics should generally be sufficient if presenting vision is hand motions or better. Systemic antibiotics were not found be of much benefit in this study.
Though EVS did provide general guidelines for treatment of endophthalmitis, clinicians should individualise treatment for each patient based on the clinical course, signs and symptoms.
Once a clinical diagnosis of acute bacterial endophthalmitis made, it is to be considered as a medical emergency requiring:! Immediate vitreal tap for culture and sensitivity and instillation of intravitreal antibiotics. ! Intravitreal antibiotics which is commonly used include Vancomycin (1 mg/0.1ml) and Ceftazidime (2.25mg/0.1ml)
because 94% of the culture positive cases are caused by gram positive organisms which are 100% sensitive to Vancomycin and 6% of culture positive cases are by gram negative group of organisms which are 90% sensitive to Ceftazidime.
! Admit to hospital for observation and treatment.! Intensive fortified antibiotics e.g Vancomycin and tobramycin 1hrly.! Atropine 1% qid.
The indications for pars plana vitrectomy are ! Perception of light or worse at presentation.! Deterioration or no improvement despite intravitreal antibiotics.! Delayed onset endophthalmitis.! Fungal endophthalmitis.
For more advance treatment, a posterior segment specialist should be contacted immediately.
1. Mandala, MP: A total 113 cataract patients were operated upon in September, 2010 from 10-16 september. All surgeries were conducted in Yogiraj Hospital which is managed by strategic concept pvt. ltd. and is a registered hospital. On investigation it was found that hospital had not taken permission from Health Department. After getting reports a central team visited the place and carried out detail investigation. It was found that total 38 patients lost their eye and out of which 30 patients were eviscerated in Yogiraj hospital on 13.9.2010. Despite reporting of pain, redness, pus discharge and no improvement in sight by 20 patients who were operated upon starting 11.9.2011, surgeries were continued till 16.9.2010. All eviscerated patients were not informed about removal of the operated eye.
Instrumental and Consumables factorsSpecial attention should be paid to:• Not checking indicator tapes
(autoclave, ETO etc)• Not checking irrigating fluid for
particulate matter/ presence and concentration of antibiotic
• Tubular instruments• Devices with ant peristaltic pumps
and reflux mechanisms • Ensure suction bottle is empty• Linen is soaked with moisture, still
using it.• Sterility of any instrument or object
is doubtful still using it.
Surgeon factors• Exposed scalp hair and nostrils• Operating inspite of having an open wound or URI/
skin infection• Improperly scrubbed hands• Ungloved hands• Wearing fluid soaked/ wet gown• Inadvertently touching an unsterile area but not
changing gloves• Same irrigation line used for several surgeries• Reusing instruments from trolley of another patient
directly• Reusing dropped instrument or IOL without
adequate resterlization• Predisposing eye to infection by leaving wound gape,
exposed suture knots,& vitreous wick
Patient preparation• Operating on Patient having
adnexal & ocular surface infection, presence of active systemic septic foci at the time of surgery
• Unclean patient attire and exposed scalp
• Improper surgical preparation• Not washing conjunctival sac
thoroughly before surgery

Chief Advisor: Dr. Jagdish Prasad, Director General of Health Services, Editorial Board: Dr. N.K. Agarwal, Deputy Director General (O) & Ms. Sujaya Krishnan, Joint Secretary (NPCB), Ministry of Health and Family Welfare, Dr. A.S. Rathore, Assistant Director General (O), Ms. Gayatri Mishra, Director (NCD), Dr. V. K. Tewari, Health Education Officer (NPCB), Dr. V. Rajshekhar, Eye Specialist, Safdarjung Hospital/MOHFW, Dr. Suman, Temporary Professional (NPCB) and Shri K.K. Jhell, Under Secretary (NCD).
NPCB-India is a quarterly newsletter of the National Programme for Control of Blindness. For further information contact or write: Dr. V. K. Tewari, Health Education Officer, 342-B, A Wing, Nirman Bhawan, New Delhi-110 108. Telefax: 011-23063875 Email: [email protected]
Designed & Printed by: ESSENCE ADVERTISING SERVICES, 45, 1st Floor, Corner Market, Malviya Nagar, New Delhi-110 017 (Quantity of Newsletter: 10,000 nos.)
QUARTERLY
INDIANPCBNPCBNPCBNPCB
QUARTERLY October - December 2011
Theme of the Issue: Quality Aspects of Cataract Operations
From Editor's Desk It has been more than thirty years since the inception of National Programme
for Control of Blindness (NPCB) in 1976, which has resulted in remarkable
gains and successes on every aspect in our country. Survey conducted by (1)
MoH&FW during the year 2006-07 revealed that prevalence of blindness has
come down from 1.4% to 1%. Along with other causes Blindness, cataract still
remains the major challenge, constituting 62.6% of total blindness, due to
raised awareness, increased longevity of life and increasing population. Since
surgical intervention is involved, quality issues are attached with the
programme. It is really unfortunate that cataract surgeries were also reported
as one of the reasons for blindness in National survey on, “Blindness & (2)visual outcomes after cataract surgery” conducted in 2001-02. Along
with achievement of target quantum wise, improvement in quality of cataract
surgery is also one of the prime objectives of the programme.
INBOX FEEDBACK / RESPONSE
Articles in Hindi Language should be included in this Quarterly issue. The postal address should be exact.
Dr. P.C. Dwivedi,Prof. of Ophthalmology,
D2-8, Doctors Colony, GMH Campus, Rewa, (M.P.)Email: [email protected]
Sir, it is an asset for medical colleges. It is heartening to see such commitment of NPCB organization, interesting. It keeps us update of various programs being done in far flung areas. Thanks a lot of all basic information.
Dr. Mrs. P. SadhotraProf. & Head. Deptt. of Ophthalmology ASCMS,
Sidhra. Jammu (JK), Tawi 180017Email: [email protected]
Respected Sir, NPCB Newsletter is an informative quarterly magazine for Indian, through which national data of community ophth. is available. If you give details about superspeciality training institutes, it will be very much helpful to RIO.
Dr. Kamini Mukesh Kumar PrajapatiAssistant Professor, M& J Inst. of ophth & RIO Civil
Hospital, Ahmedabad-16Email: [email protected]
It was also observed that there was a direct entry to the eye OT from corridor, and labour room was also situated near by to the eye OT. All surgeries were performed by a fresh MS eye surgeon while senior surgeon was out of the town.
2. Eye mishap at Indore Eye Hospital: Indore eye Hospital Society, Madhya Pradesh conducted two eye camps (Sarwas and Sonkatch) at Dewas and one eye camp at Mhow in Indore District. Cataract surgery was performed on 197 patients on 16th, 22nd and 30th December, 2010. Out of all operated cases 18 patients developed post operative endophthalmitis. It was found that water used for scrubbing was infected with Klebsella organisms.
3. Community Health Centre, Balod, District Chhatisgarh:An eye camp was organized by Indian Medical Association from 20-31 September, 2011 at Community Health Centre, Balod district Chhatisgarh in which 334 patients were operated for Cataract, 46 patients developed infection out of which 2 had been advised operation,6 for cataract surgery in other eye after 4 week & 3 for immediate cataract operation. On investigation it was found that pseudomonas bacteria was responsible for infection and same was also found in OT trolley, OT table and OT almirah. Failure of autoclave was reported by the inspection team, as also laxity in observing other universal O.T. precaution while conducting surgery on a mass basis.
Eye Check-up Campaign during "World Sight Day"Awareness Speech to a Self Help Group during "World Sight Day"
Shri S. GandhiselvanHon’ble Minister of State
for Health & Family Welfare
Shri Ghulam Nabi AzadHon’ble Union Minister
of Health & Family Welfare
Shri Sudip BandyopadhyayHon’ble Minister of State
for Health & Family Welfare
thWORLD SIGHT DAY – 13 October '2011“Eye Care f r All”
Prime Activities of NPCBInfrastructure Development,
ØDevelopment of Regional Institutes of Ophthalmology (RIO),
ØDevelopment of Medical Colleges, District Hospitals, Sub-district Hospitals &
vision centers by providing Financial support and Guidance
Grant-in-Aid to States for implementing NPCB activities.
Provision of Eye Care Professionals for States on Contractual basis,
Training of Eye Surgeons in Various disciplines of Ophthalmology,
Training of Paramedical Ophthalmic Assistant, Accredited Social Health Activists
& Nurses all over the country.
Technical Research to improve services.
Celebration of key events like National Eye Donation Fortnight, World Sight Day,
World Glaucoma Day etc.
Services given to General Public all over India, free of cost:Cataract Surgery with Intra Ocular Lens (IOL),
Screening and Provision of spectacles to school children with Refractive
Error,
Collection of Donated Eyes (Cornea) and Keratoplasty for Corneal blind
persons,
Screening for Diabetic Retinopathy and Laser Treatment for affected
persons,
Screening for Glaucoma and Medical & Laser Treatment of those
suffering,
Detection and Treatment of Childhood Blindness, Trachoma etc, and
Providing primary Eye Care Services for all, including rural folk/poor.
NATIONAL PROGRAMME FOR CONTROL OF BLINDNESSMinistry of Health & Family Welfare,
Nirman Bhawan, New Delhi – 110 108. www.mohfw.in/npcb.nic.in
If you are over 40 years of age and have a family history of Diabetes or Glaucoma, you MUST get your Eyes check up done at
least once a year.
For more information, please contact Primary Health Center, District Hospital, Medical College
![Overview of Congenital, Senile and Metabolic Cataractrelated cataract [7] and metabolic cataract [8]. Congenital & Senile Cataract Cataract is a clouding of the eye’s natural lens](https://img.pdfslide.us/doc/110x75/5f361b7a353bcc123d74d127/overview-of-congenital-senile-and-metabolic-cataract-related-cataract-7-and-metabolic.jpg)