Embed Size (px)
Citation preview

Qu XinkaiShanghai Chest Hospital
Shanghai Jiaotong University
Value of comprehensive cardiac evaluation using MSCT in
patients with CTO

3,277 STEMI pts treated with PCI;Three groups: SVD; MVD without CTO; MVD with a C TO in a non-IRA
The presence of a CTO is associated with reduced LVEF and further deterioration of LVEF.
Claessen . J ACC Intv 2009
Long-term mortality and LVEF of CTO

124 CTOs with DES;159 CTOs with BMS
Felice . JACC Intv 2009
After 3 yrs, DES were superior to BMS in reducing MACE in pts with CTO and should be considered the preferred treatment strategy
CTO 3yrs FU: DES vs BMS

Comprehensive cardiac assessment is necessary before revascularization is performed, so that the patients most suited for PCI can be selected.
CTO lesion; Myocardial viability

Inability to cross the lesion into the true lumen of the distal vessel with a guide wire (>60%);
Intimal dissection with creation of a false lumen;
Contrast extravasation; Failure to cross the lesion with a balloon; Failure to dilate adequately
Reasons for procedural failure of PCI for CTO

Most important predictors Severe calcification at the stump of CTO Tortuosity of the proximal vessel of CTO Very long occlusion length Other predictors for less-experienced operators Absence of antegrade flow and no or poor distal vessel
visibility Long occlusion duration Presence of antegrade bridging collaterals (reflection
of chronicity of the lesion) Blunt stump occlusion Presence of side branch at occlusion site
Predictors of procedural failure

Mowatt G, etal. Heart 2008;94:1386-1393
CTCA: meta-analysis (28 trials)

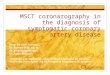
A : MPR
B : 3D-VR-Tree
C : 3D-VR-Outline
D : 3D-VR-Heart

The CTCA suggests PCI will be more difficult because of the absence of any clear stump, moderately long total occlusion, and poor distal vessel quality, PCI was not successful in the recanalization of the RCA
CTCA to CTO

the duration of the patient’s symptoms was for a few weeks, represents sub-acute occlusion and not a CTO
CTCA to CTO: MPR and 3D-MIP images

Assessment of tortuosity by MSCT
Garcia-Garcia. EuroInterv 2009

Garcia-Garcia. EuroInterv 2009

Garcia-Garcia. EuroInterv 2009


Hsu. IJC 2009


Route and course of CTO segment, as the distal vessel can be well visualized usually.
Length and diameter of the occluded segment without foreshortening. 3D-length measurement of occlusion is possible by CTCA even if retrograde or collateral contrast filling is poor or absent at catheterization
MP and 3D views allow planning of the best angiographic view of the occlusion trajectory during PCI, i.e., 3D-roadmapping fusion with catheterization laboratory data may be possible
What could we learn from CTCA for CTO

Presence of calcification at the stump of occlusion, especially severe or concentric calcification—this may assist in selection of targeted strategy, e.g., upfront use of ablative technique
Presence of proximal tortuosity at the occlusion site Presence of blunt occlusion stump or a side branch
at the occlusion site Collaterals or bridging vessels at the occlusion site
are not usually visualized by CTCA; septal collaterals cannot be demonstrated by CTCA due to their intramyocardial location
What could we learn from CTCA for CTO

Reconstruction of image from MSCT scanning

Henneman . Am J Cardiol 2008
69 pts with MI > 3 m
SPECT Normal (N)
Infarct (MI)
MSCT N 4 0
MSCT MI 3 62
Healed MI can be detected accurately using MSCT, with good correlation with SPECT
MSCT vs SPECT to healed MI

15 pigs with reperfusion after MI, 6months
A DE-MDCT provides a more detailed assessment of the PIZ in chronic MI and is less susceptible to partial volume effects than MRI.
Schuleri. JACC 2009

White arrows: enhanced scar tissueWhite circle: peri-infarct zone (PIZ)

1 min 5 min 10 min 15 min 20 min
MI volume (%) 11.87±3.54 9.78±2.88* 9.57±2.88* 8.99±2.69*†# 8.51±2.93*†#
CT value of
infarcted region
(HU)
26±15 68±11* 66±6* 64±7* 69±18*
CT value of cavity
(HU)
620±39 383±26* 302±27*† 245±25*†# 232±22*†#
CT value of normal
myocardium (HU)
253±32 179±23* 150±10* 129±5*†# 128±20*†#
Volume of infarction (percentage) and CT value of different cardiac tissues at various time-points

Comparison of MI size between TTC staining and MSCT using Bland-Altman plots at various time-points

Features of the CTO artery could be assessed using CTCA;
Infarct size and viable myocardium could be assessed using MSCT;
Comprehensive cardiac information for CTO could be afforded using only a single MSCT examination.
The data would be helpful for selection of patients with CTO for revascularization.
Conclusion

Due to exposure of patients to X-rays and potentially toxic contrast agents, MSCT perfusion imaging is unlikely to become a first-line test to assess myocardial viability in all patients. Until now, this modality has only been recommended for use in patients with definite CTO or previous MI.
It is still difficult and time-consuming to analyze the myocardial perfusion images. With the development of dedicated software, the problem of the heavy workload could be diminished in the future.
Clinical limitations