Embed Size (px)
Citation preview
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 1/33
JOURNAL READING
Pembimbing : dr. Bambang sugeng, sp. b
QORRY AMANDA 01.209.5986KOAS BEDAH FK UNISSULA SEMARANG
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 2/33
JOURNAL IDENTITY
• Title :Preoperative radiotherapy versus selective postoperative
chemoradiotherapy in patients with rectal cancer (MRC CR07 and
NCIC-CTG C016): a multicentre, randomised trial
• Writers : David Sebag-Montefi ore, Richard J Stephens, Robert Steele,John Monson, Robert Grieve, Subhash Khanna, Phil Quirke, Jean
Couture, Catherine de Metz, Arthur Sun Myint, Eric Bessell, Gareth
Griffi ths, Lindsay C Thompson, Mahesh Parmar, on behalf of all the
trial collaborators*
• Published date : March 2009
• Published by : The Lancet of Oncology
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 3/33
BACKGROUND
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 4/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 5/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 6/33
The consensus statement by the US National Institutes for Health in 1990
recommended postoperative chemoradiotherapy as standard treatment inthe USA for all patients with completely resected stage II or III rectal cancer.
Nevertheless, pelvic radiotherapy is associated with an increased risk of late
complications, including a substantial increase in bowel frequency andincontinence and delayed healing of the perineal wound when an
abdominoperineal excision is done
Therefore, targeting radiotherapy to patients considered at high
risk of local recurrence is an attractive option, especially if thenumber of such patients can be kept to a minimum
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 7/33
MAIN PURPOSE:to compare the use ofroutine short-course
preoperativeradiotherapy with
initial surgery andselective
postoperativechemoradiotherapyreserved for patients
who had involvement ofthe circumferentialresection margin.
PRIMARY OUTCOME:The primary outcome
measure was localrecurrence,
irrespective of anyoccurrence of distant
metastases.
SECONDARY OUTCOME:
Secondary outcomemeasures were overallsurvival, disease-free
survival, local-recurrence-free
survival, postoperativemorbidity
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 8/33
METHOD & MATERIAL
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 9/33
Study design
• Not-blinded prospective randomised trial
Time• 1998-2009 (1998-2005 patients recruiting
; 2005-2009 trial conducted)
Sample
• 1350 patients
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 10/33
Inclution
had histologicallyconfirmed
adenocarcinoma of therectum
The primary tumour had to bedeemed resectable
Patients had to be regardedas sufficiently fit to receiveall treatments (an upper age
limit was not defi ned)
Exclution
those with previous or present malignantdisease that was likely to interfere with
protocol comparisons were regarded as ineligible
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 11/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 12/33
Eligible consenting patients were randomly
assigned to treatment groups by the MRC ClinicalTrials Unit by a minimisation procedure, with
stratification for surgeon, distance of distal
tumour extent from the anal verge, and WHO
performance status
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 13/33
Patients were assigned to either
• a preoperative radiotherapy regimen of 25 Gy in fiveconsecutive daily fractions followed by surgery
(recommended to take place within 7 days of the lastfraction of radiotherapy), or to
• a selected postoperative chemoradiotherapy regimen
of initialsurgery with selective postoperative
concurrent chemoradiotherapy of 45 Gy in 25fractions with concurrent 5-fluorouracil (either
continuous infusion 200 mg/m² per day or weekly bolus
5-fl uorouracil 300 mg/m² and leucovorin 20 mg/m²) for
patients with involvement of the circumferential
resection margin (≤1 mm).
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 14/33
Surgeons were encouraged to use total mesorectal excision, although it
was not mandated in the trial protocol.
This approach was already in clinical use in the UK at the time that the
trial was launched.
No formal training or accreditation programme was used for surgeons
participating in the trial.
a validated audit method to assess whether total mesorectal excision was
done, or to assess the quality of the surgical specimen, did not exist.
After randomisation, follow-up forms were required at 3, 6, 9, and 12months, and then every 6 months to 3 years and yearly thereafter.
Patient-reported quality of life was collected with the validated
questionnaires SF36,and EORTC (European Organisation for Research andTreatment of Cancer) quality-of-life questionnaire CR-38
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 15/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 16/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 17/33
DISCUSSION
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 18/33
Results show that both local control and diseasefree survival are improved by
preoperativeradiotherapy compared with
selectivepostoperative chemoradiotherapy.
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 19/33
Three trials compared short-course preoperativeradiotherapy followed by surgery with surgery alone,although 316 of the 557 patients in the Stockholm II
trial were also included in the Swedish Rectal Trial.
The pooled data of the remaining two trials show ahighly consistent and significant reduction in the
rate of local recurrence with the use ofpreoperative radiotherapy (HR 0·46, 95% CI 0·38–
0·56; figure 3)
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 20/33
Both trials assessed short-coursepreoperativeradiotherapy with a highly selective
postoperative radiotherapy regimen.
The CR07 trial used postoperative concurrent chemoradiotherapy, whereas the Dutch trial used
radiotherapy alone in the selective postoperativegroup. The combined data from the CR07 trial and the
Dutch trial (the two largest adjuvant radiotherapy trials,totalling 3211 patients) show a highly significant
reduction in the rate of local recurrence with the useof preoperative radiotherapy (HR 0·38, 95% CI 0·29–0·49)
when combined with total mesorectal excision
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 21/33
The preoperative radiotherapy regimen is also avery cost-effective way to deliver treatment,since it uses only five fractions of radiation.
Furthermore, evidence from the 13-yearfollow-up from the Swedish rectal cancer trial,
and data from three meta-analyses, lendsupport to the view that preoperative
radiotherapy prevents a proportion ofpatients from developing local recurrence
rather than merely delaying the event
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 22/33
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 23/33
CRITICAL APPRAISAL
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 24/33
TITLE:
Preoperativeradiotherapy versus
selective
postoperativechemoradiotherapy inpatients with rectalcancer (MRC CR07
and NCIC-CTG C016): amulticentre,
randomised trial
The title hasdescribed thearticle content
clearly andsuitably
The title does notput the
dependent andindependent
variables clearlyon the context
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 25/33
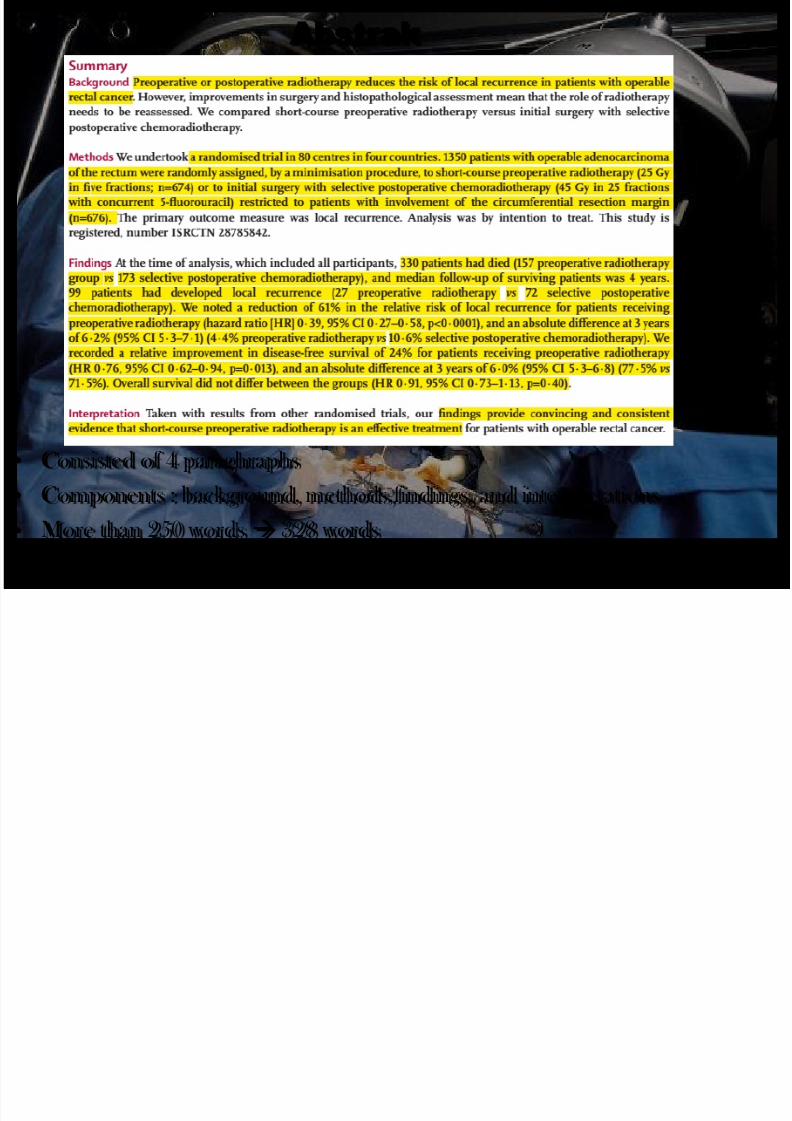
bstrak
• Consisted of 4 paraghraphs
• Components : background, methods,findings, and interpretations
• More than 250 words 328 words
• No keywords mentioned
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 26/33
PRIMARY OUTCOME
Local Recurence • 27 preoperative
radiotherapy vs 72
selectivepostoperative
Chemoradiotherapy• a reduction of 61% in the
relative risk of local
recurrence for patients
receiving preoperative
radiotherapy (hazard
ratio [HR] 0·39, 95% CI0·27–0·58, p<0·0001)
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 27/33
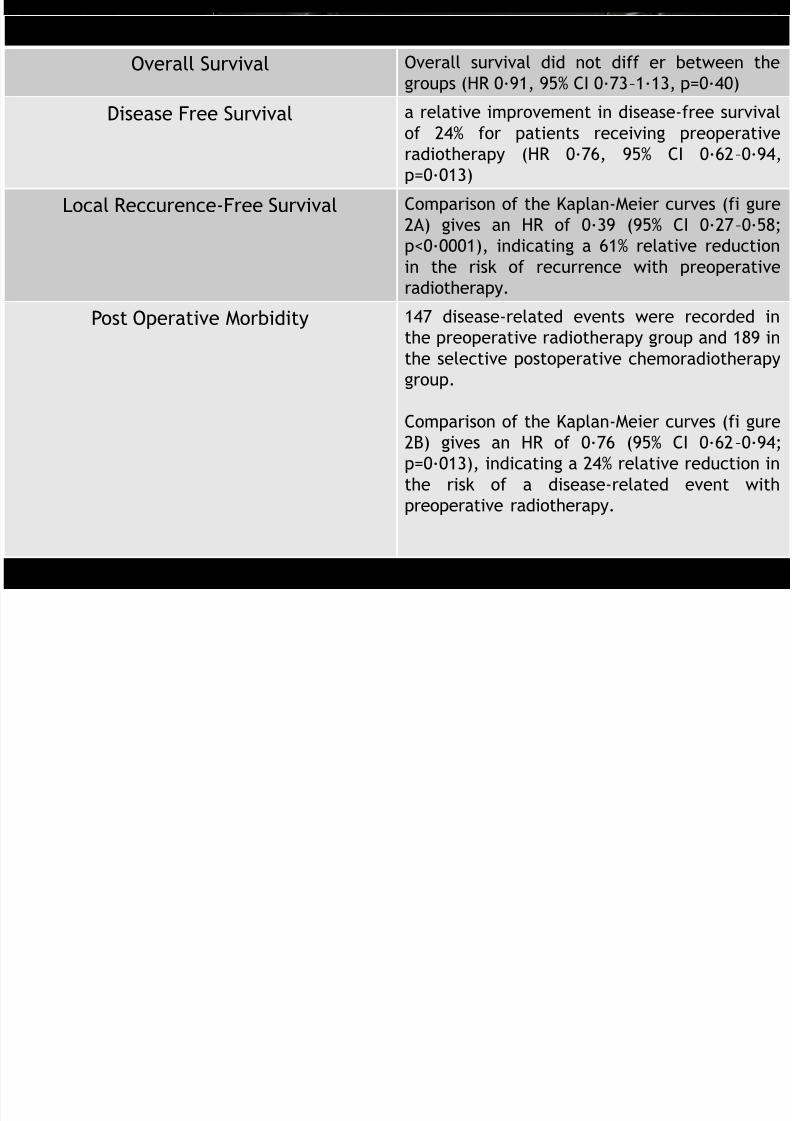
SECONDARY OUTCOME
Overall Survival Overall survival did not diff er between the
groups (HR 0·91, 95% CI 0·73–1·13, p=0·40)
Disease Free Survival a relative improvement in disease-free survival
of 24% for patients receiving preoperativeradiotherapy (HR 0·76, 95% CI 0·62–0·94,
p=0·013)
Local Reccurence-Free Survival Comparison of the Kaplan-Meier curves (fi gure
2A) gives an HR of 0·39 (95% CI 0·27–0·58;
p<0·0001), indicating a 61% relative reduction
in the risk of recurrence with preoperative
radiotherapy.
Post Operative Morbidity 147 disease-related events were recorded in
the preoperative radiotherapy group and 189 in
the selective postoperative chemoradiotherapy
group.
Comparison of the Kaplan-Meier curves (fi gure2B) gives an HR of 0·76 (95% CI 0·62–0·94;
p=0·013), indicating a 24% relative reduction in
the risk of a disease-related event with
preoperative radiotherapy.
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 28/33
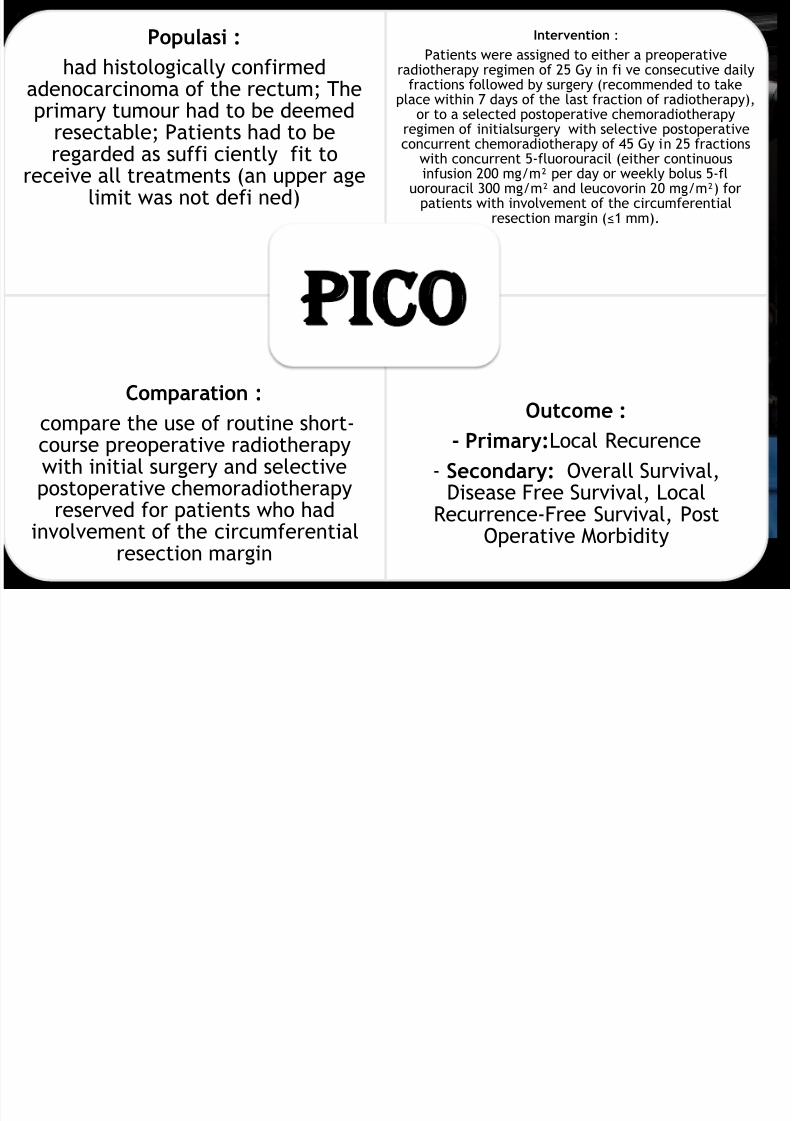
Populasi :
had histologically confirmedadenocarcinoma of the rectum; Theprimary tumour had to be deemed
resectable; Patients had to beregarded as suffi ciently fit toreceive all treatments (an upper age
limit was not defi ned)
Intervention :
Patients were assigned to either a preoperativeradiotherapy regimen of 25 Gy in fi ve consecutive daily
fractions followed by surgery (recommended to takeplace within 7 days of the last fraction of radiotherapy),
or to a selected postoperative chemoradiotherapyregimen of initialsurgery with selective postoperative
concurrent chemoradiotherapy of 45 Gy in 25 fractionswith concurrent 5-fluorouracil (either continuousinfusion 200 mg/m² per day or weekly bolus 5-fl
uorouracil 300 mg/m² and leucovorin 20 mg/m²) forpatients with involvement of the circumferential
resection margin (≤1 mm).
Comparation :
compare the use of routine short-course preoperative radiotherapywith initial surgery and selectivepostoperative chemoradiotherapy
reserved for patients who hadinvolvement of the circumferential
resection margin
Outcome :- Primary:Local Recurence
- Secondary: Overall Survival,Disease Free Survival, Local
Recurrence-Free Survival, PostOperative Morbidity
PI O
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 29/33
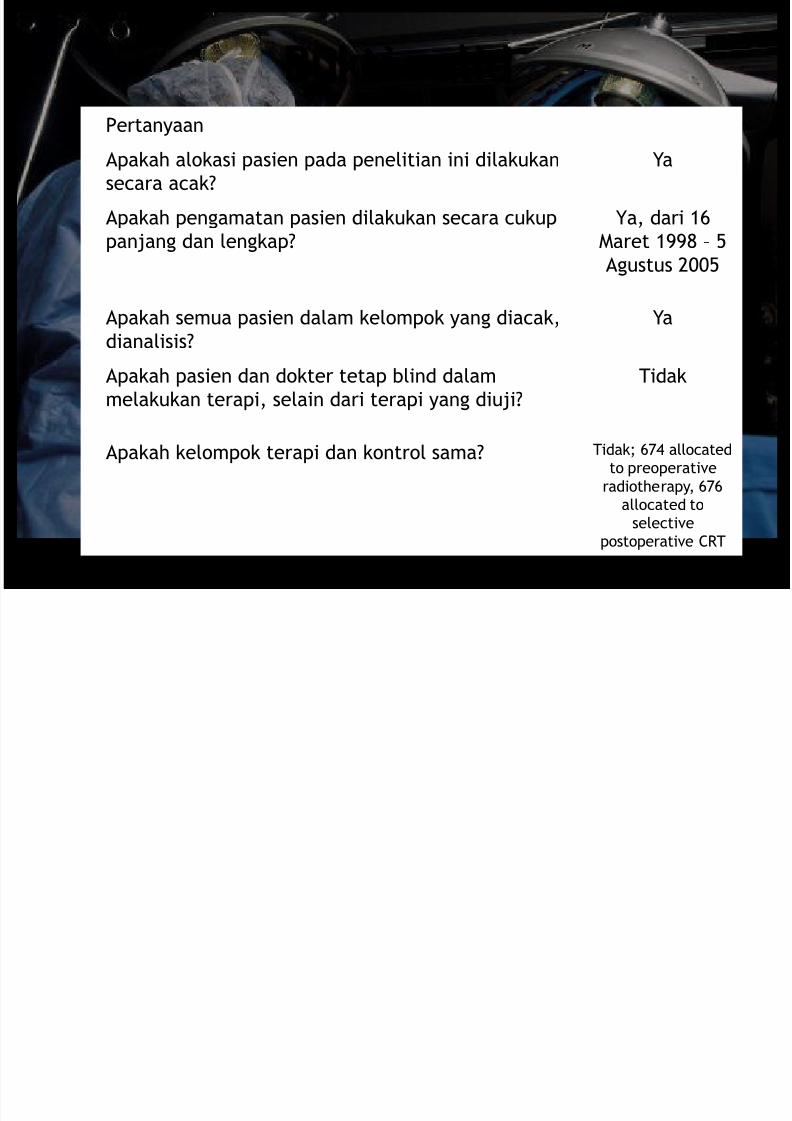
Pertanyaan
Apakah alokasi pasien pada penelitian ini dilakukan
secara acak?
Ya
Apakah pengamatan pasien dilakukan secara cukup
panjang dan lengkap?
Ya, dari 16
Maret 1998 – 5
Agustus 2005
Apakah semua pasien dalam kelompok yang diacak,
dianalisis?
Ya
Apakah pasien dan dokter tetap blind dalam
melakukan terapi, selain dari terapi yang diuji?
Tidak
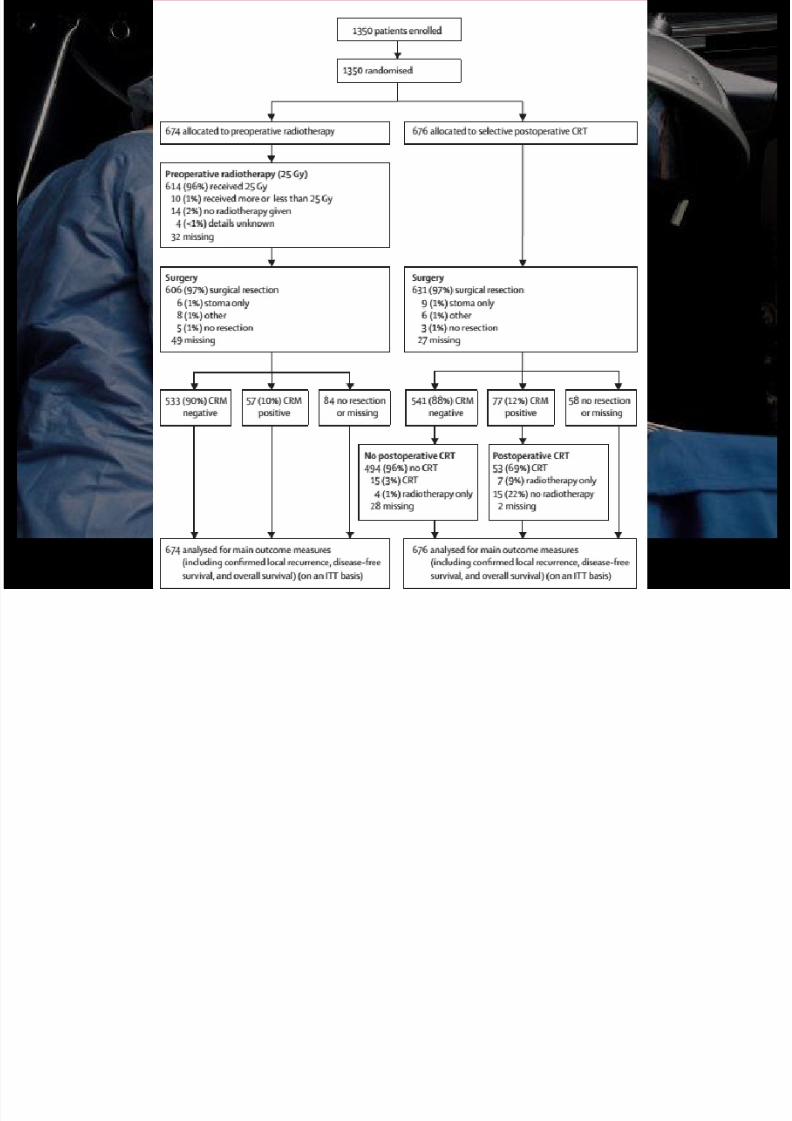
Apakah kelompok terapi dan kontrol sama? Tidak; 674 allocated
to preoperative
radiotherapy, 676
allocated to
selective
postoperative CRT
Bukti valid
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 30/33
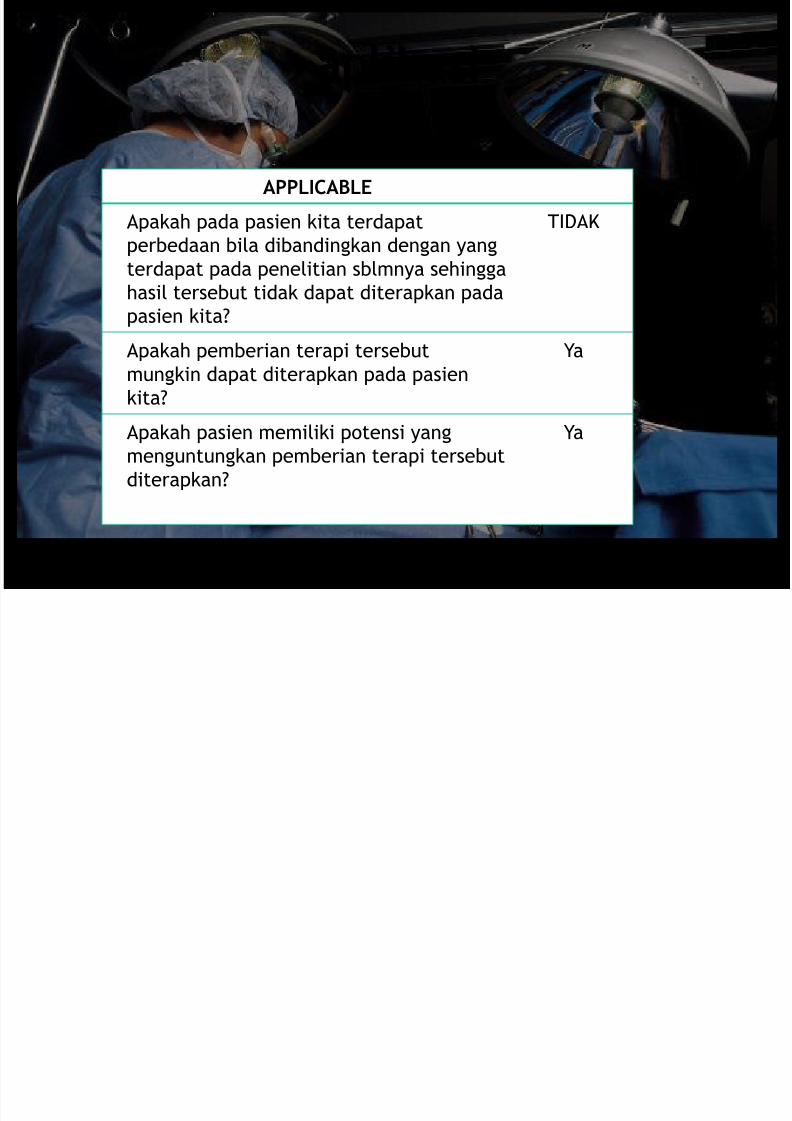
aplikasi
APPLICABLE
Apakah pada pasien kita terdapat
perbedaan bila dibandingkan dengan yang
terdapat pada penelitian sblmnya sehingga
hasil tersebut tidak dapat diterapkan pada
pasien kita?
TIDAK
Apakah pemberian terapi tersebut
mungkin dapat diterapkan pada pasien
kita?
Ya
Apakah pasien memiliki potensi yang
menguntungkan pemberian terapi tersebut
diterapkan?
Ya
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 31/33
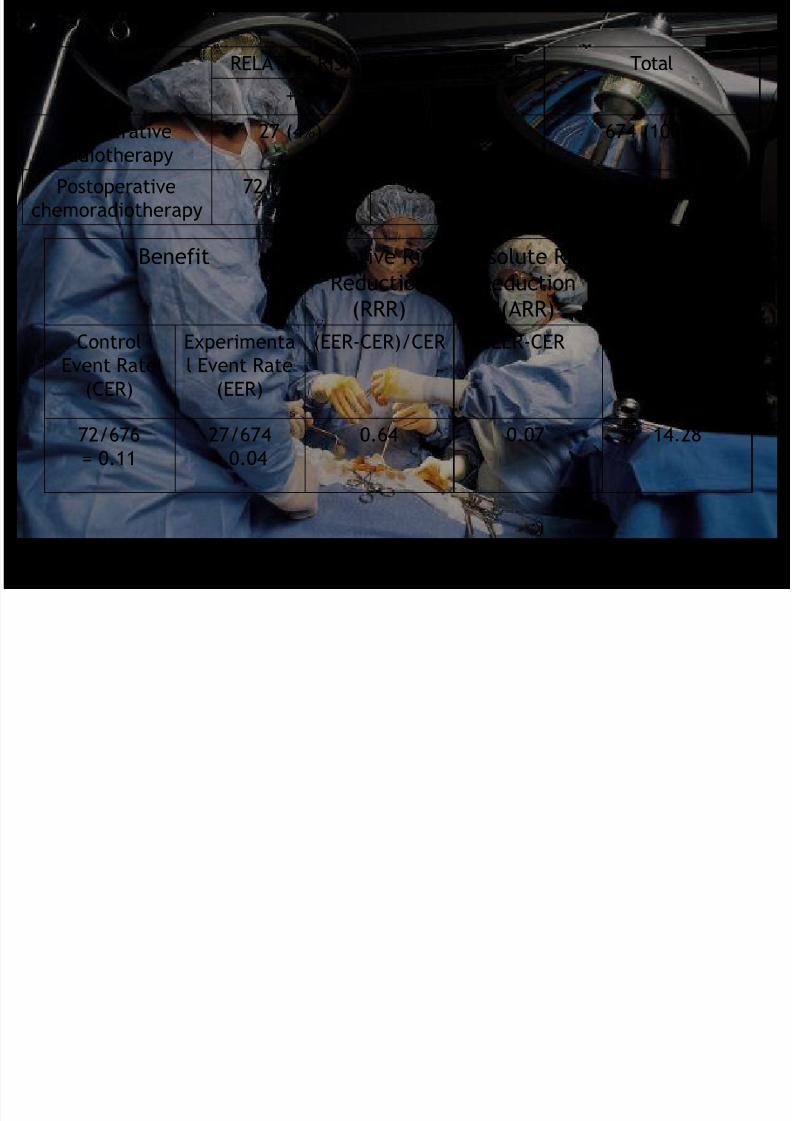
Benefit Relative Risk
Reduction(RRR)
Absolute Risk
Reduction(ARR)
Number
Needed toTreat (NNT)
Control
Event Rate
(CER)
Experimenta
l Event Rate
(EER)
(EER-CER)/CER EER-CER 1/ARR
72/676
= 0.11
27/674
= 0.04
0.64 0.07 14.28
RELATIVE RISK LOCAL RECURENCE Total
+ -
Preoperative
radiotherapy 27 (4%) 647 (96%) 674 (100%)
Postoperative
chemoradiotherapy 72 (10.65%) 604 (89.35%) 676 (100%)
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 32/33
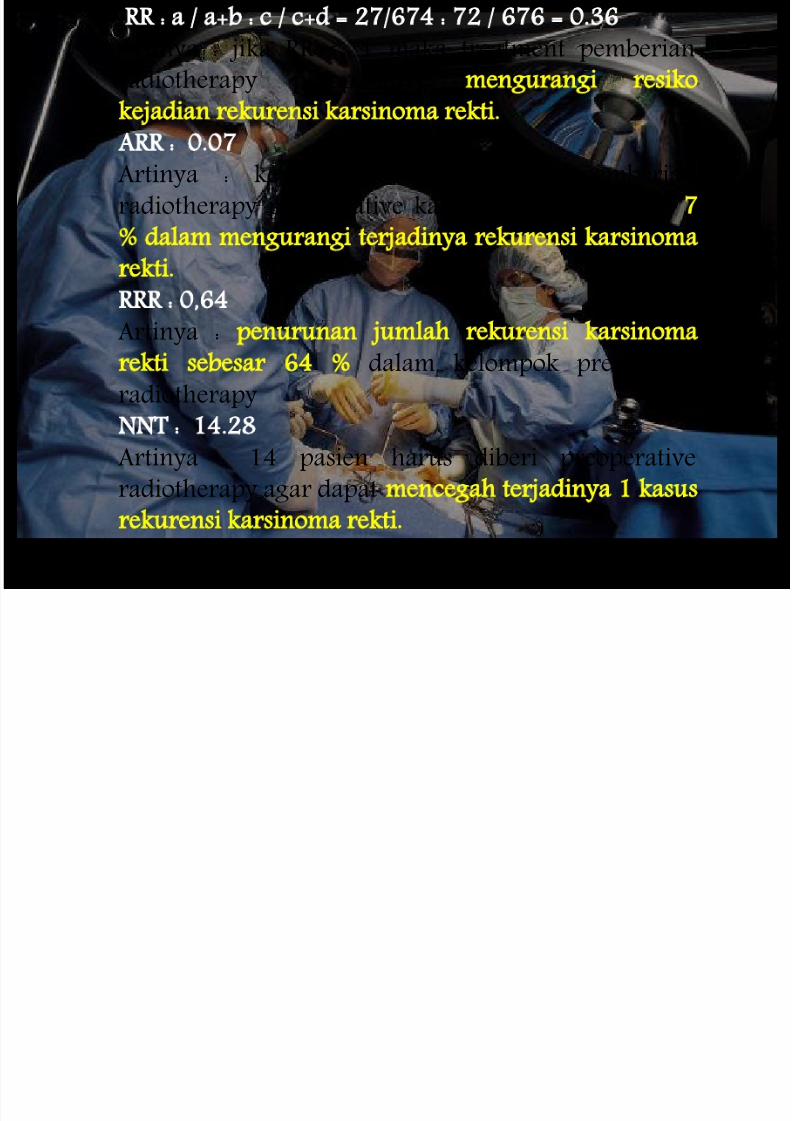
RR : a / a+b : c / c+d = 27/674 : 72 / 676 = 0.36
Artinya : jika RR < 1 maka treatment pemberian
radiotherapy preoperative mengurangi resiko
kejadian rekurensi karsinoma rekti.
ARR : 0.07
Artinya : keuntungan absolut dari pemberian
radiotherapy preoperative karsinoma rekti adalah 7
dalam mengurangi terjadinya rekurensi karsinoma
rekti.
RRR : 0,64
Artinya : penurunan jumlah rekurensi karsinoma
rekti sebesar 64 dalam kelompok preoperatif
radiotherapy
NNT : 14.28
Artinya : 14 pasien harus diberi preoperative
radiotherapy agar dapat mencegah terjadinya 1 kasus
rekurensi karsinoma rekti.
8/10/2019 qorryamanda.pptx
http://slidepdf.com/reader/full/qorryamandapptx 33/33