Embed Size (px)
Citation preview

1
Q
UMBILICAL CORD CARE AND MANAGEMENT OUTCOME
AMONG MOTHERS IN CALABAR SOUTH LOCAL
GOVERNMENT AREA, CROSS RIVER STATE,
NIGERIA.
BY
OSUCHUKWU, EASTER CHUKWUDI
PG/M.Sc/08/47723
DEPARTMENT OF NURSING SCIENCES
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
UNIVERSITY OF NIGERIA
ENUGU CAMPUS.
JANUARY,2014

2
TITLE PAGE
UMBILICAL CORD CARE AND MANAGEMENT OUTCOME
AMONG MOTHERS IN CALABAR SOUTH LOCAL
GOVERNMENT AREA, CROSS RIVER STATE,
NIGERIA.
BY
OSUCHUKWU, EASTER CHUKWUDI
PG/M.Sc/08/47723
M.Sc. DISSERTATION
SUBMITTED TO DEPARTMENT OF NURSING SCIENCES
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
UNIVERSITY OF NIGERIA
ENUGU CAMPUS.
IN PARTIAL FULFILMENT OF THE REQUIREMENT FOR THE
AWARD OF A MASTER OF SCIENCE DEGREE IN NURSING
(MEDICAL – SURGICAL NURSING).
DR (Mrs.), I. L. OKORONKWO
(SUPERVISOR)
JANUARY, 2014

3

4
CERTIFICATION
This is to certify that this research work ‘‘Umbilical Cord Care and Management Outcome
among Mothers in Calabar South Local Government Area of Cross River State, Nigeria” is the
original research work of Easter C. Osuchukwu with Registration Number PG/M.Sc./08/47723, a
post graduate student in the Department of Nursing Sciences. The work embodied in this
dissertation is original and has not been submitted in parts or full for any other degree in this or
any other University.
……………………………………. ………………………...
Osuchukwu, Easter C Date
(Student)
………………………………. …………………
Dr (Mrs.), I. L. Okoronkwo Date
(Supervisor)

5
DEDICATION
This work is dedicated to the Lord Almighty.

6
ACKNOWLEDGEMENT
With a heart full of joy, I thank the God Almighty who has been my source of strength
throughout the period of the program.
In a special way I express my immeasurable gratitude to my supervisor, Dr (Mrs.), I.L
Okoronkwo for painstakingly reading through this work, making very useful suggestions and
seeing that the work takes its desired form. You were always there for me. Thank you very
much Ma!
I must thank my dynamic Head of Department of Nursing Sciences, Dr (Mrs.), U. Okolie for the
motherly guide given to me. My gratitude also goes to my distinguished and acclaimed scholars
– Prof. C. Okafor, Dr. (Mrs.), I. O. Ehiemere, Dr. (Mrs.), A. Anarado, Dr. A. Nwaneri, Dr. E.
Nwonu and Dr. (Mrs.), P. Ihenacho for their unique concern and ever ready to listen. To all of
you my intellectual models, I say a big thank you. A lot of appreciation goes to all my reputable
lecturers for their encouragement and advice.
To my very dear friend, my confidant and above all a loving and caring husband Dr. N. C.
Osuchukwu. I express my affectionate gratitude. I am also appreciative of my lovely children,
My Joy, Chika and Desire Chijioke for their endurance who have been prayerfully expecting the
completion of this program. My beloved mother, siblings and in-laws, deserve a special mention
for their moral support and prayers. I salute you all.
I must not forget my friends and colleagues; they have been wonderful with their constructive
criticisms and eagerness to render assistance. Thanks ever so much.
Finally, I am grateful to all the respondents for their cooperation and the various authors whose
publications were very useful. I thank you all.

7
TABLE 0F CONTENTS Page
TITLE PAGE i
APPROVAL ii
CERTIFICATION iii
DEDICATION iv
ACKNOWLEDGEMENT v
TABLE OF CONTENTS vi
LIST OF TABLES vii
ABSTRACT viii
CHAPTER ONE: INTRODUCTION
Background to the Study 1
Statement of Problem 3
Purpose of Study 4
Objectives of the Study 4
Research Questions 5
Significance of the Study 5
Scope of the Study 6
Operational Definition of Terms 6

8
CHAPTER TWO: LITERATURE REVIEW
Conceptual Review of Umbilical Cord 8
Management of Umbilical Cord 9
Knowledge of Standard Cord care and Sources 10
Material for Cord Management 11
Reasons for Choice of Substance for Cord Management 12
Techniques of Cord Care 14
Factors Influencing Umbilical Stump Management 15
Cord Infections 16
Cord Separation Time 20
Theoretical Review 20
Conceptual Model of the Study 23
Empirical Review 24
Summary of Literature Review 34
CHAPTER THREE: RESEARCH METHOD
Research Design 36
Area of Study 36
Population of Study 37
Sample 37
Sampling Procedure 38
Instrument for Data Collection 40
Validity of the Instrument 40

9
Reliability of the Instrument 41
Ethical Consideration 41
Procedure for Data Collection 41
Method of Data Analysis 42
CHAPTER FOUR: DATA PRESENTATION
Demographic Data of Respondents 43
Research Questions 45
Summary of major Findings 60
CHAPTER FIVE: DISCUSSION OF FINDINGS
Discussion of Major Findings 61
Implication to Nursing 67
Limitations of the Study 68
Suggest for further studies 68
Summary 69
Conclusion 70
Recommendations 72
REFERENCES 72
APPENDICES 77

10
LIST OF TABLES Page
Table 1: The Number of Sample for Each Clan 39
Table 2: Demographic Characteristics of Respondents 43
Tables 3-8 Knowledge of Standard Cord Care and Source 45
Table 9: Materials Used by Mothers for Core Care 51
Table 10: Reasons for Choice of Material for Cord Care 53
Table 11: Techniques Used by Mothers in Umbilical Care 54
Tables 12 Management outcome of umbilical care 56
Table 16: Correlation Test of Association between Age and cord management 57
Table 17: Correlation Test of Association between educational Attainments 58
Cord Management
Table 18: Correlation Test of Association between income and Cord Management 59

11
LIST OF FIGURE
Figure 1: Conceptual Model of the study 23

12
LIST OF APPENDICES
Appendix 1: Questionnaire 77
Appendix 2: Calculation of Sample Size 85
Appendix 3: Reliability Test Result 86
Appendix 4 Identification Letter 88
Appendix 5 Ethical Clearance Certificate 89
Appendix 6: Letter of Approval 90
Appendix 7 Information Letter 91
Appendix 8 Informed Consent 93

13
ABSTRACT
Umbilical cord remains the major means for the transmission of infection after birth and
constitutes 33% of neonatal mortality in Nigeria. Most of the cord care in Nigeria is home based
as two third of the delivery takes place at home. The purpose of this study was to determine the
umbilical cord care and management outcome among mothers in Calabar South Local
Government Area of Cross River State, Nigeria. The research method was a cross – sectional
descriptive survey design. Four hundred and fifty (450) respondents were selected using a snow
ball (networking) method. Data were collected using a researcher developed questionnaire. The
instrument was validated by the supervisor, two lecturers in the Department of Nursing Sciences
who are experts in child health and three neonatologists. The reliability was established using a
test re-test method at interval of two weeks. The scores obtained were correlated using Pearson
product correlation coefficient to obtain coefficient reliability of 0.993 – 0.99 at 0.05 level of
significance. Data collected were analyzed using mean, simple percentage and standard deviation
to answer the research questions. Findings revealed that 201 (44.7%) of the respondents had
good knowledge of standard cord care and their major sources of information was from mothers /
mothers-in-laws. Three hundred and fourteen (69.8%) used unhygienic and harmful materials for
cord care. The major reason for choice of materials was mainly to wade away evil spirit which
the respondents belief causes neonatal deaths. The technique for cord care was poor as only 92
(20.4%) cleaned the base of the cord before cleaning the surrounding skins. The management
outcome was poor as 338 (75.1%) of respondents reported signs of umbilical infections in their
neonates and only 5 (4.1%) reported the problem to the health facilities within 24hours of onset
of problem. There was a significant association between age, educational level, income and cord
management (p=<0.05). In conclusion, there was poor knowledge of standard cord care among
the respondents in this study. Unhygienic materials were used in the care of umbilical cord by
most of the respondents. Based on the findings, the study recommends that there should be
increased home visits and education of the mothers by the health personnel to reduce the
consequences of poor cord management after delivery.

14
CHAPTER ONE
INTRODUCTION
Background to the Study
In developing countries umbilical cord infections constitute a major cause of neonatal morbidity
and pose significant risk for mortality (WHO, 2009). Cord management introduced to mothers in
both developed and developing countries to reduce exposure of the cord to infectious pathogens
include clean cord cutting, hygienic cleaning and washing of hands before and after cord care
(Garner, 2008; Basil, Kayode, Mark & Mbe, 2009).
The umbilical cord is a unique tissue consisting of two arteries and one vein which at term is
about 56cm in length and extends normally from the centre of the placenta to the umbilicus of
the unborn baby (Abba, 2008). During pregnancy, the umbilical cord connects the fetus to the
mother through the placenta. The blood flowing through the cord brings nutrients and oxygen
from the mother to the fetus and carries away carbon dioxide and other metabolites from the
fetus (World Health Organisation, 2009; Bello & Omotara, 2010; Ezenduka & Eze, 2002).
After the delivery of the baby, the cord should be clamped firmly and cut with sterile instrument
to separate the baby from the placenta attached to the mother’s uterus leaving about 6cm with the
baby. The instrument used in cutting the cord cuts across the living tissues and the blood vessels
which are still connected to the baby. In view of the fact that this time the umbilical cord is wet
with an open surface wound and blood vessels still patent, they provide a nutritive culture
medium for bacterial growth. These require that some degree of hygiene practices must be
adopted to prevent infection, which may present as yellow discharge from the cord, foul
smelling, red skin around the base of the cord, pain when touched the skin around the stump and

15
excessive crying. These strengthen the need for standard cord management among mothers
(Bemor & Uta, 2011).
Methods of caring for the umbilical cord vary greatly between communities depending on their
cultural and religious beliefs, level of education and resources. In the developing countries most
deliveries occur at home where health care services may not be available. Sometimes materials
used to tie the cord include strings, thread and strips of cloth, scissors and sharp stone (Obuekwe
& Obuekwe, 2008). The risk of cord infection is increased by unhygienic cutting of the cord and
application of unclean substances such substances sand from door post mixed with saliva, herbal
preparations and lantern wax. Even babies delivered in hospitals may be affected by traditional
practices after discharge which most times lead to umbilical cord infection and dead among the
neonates (Sreeramaraddy, Josh, Sreekumaran & Giri, 2006).
The use of alcohol daily and as often as each diaper is changed has been recommended by the
World Health Organisation (WHO) as standard care. With standard care the cord usually falls off
between five to fifteen days after birth (WHO, 2007). Where clean cord care is not practiced, the
cord is readily colonized and infected by pathogenic organisms (Bennet & Adetunde, 2010;
WHO, 2007). Therefore, mothers who adopt clean cord management will by implication
contribute to the survival of the neonates and prevent neonatal death from infections such as
omphalitis, neonatal tetanus and septicaemia (Bemor &Uta, 2011; Bennet &Adetunde, 2010;
WHO,2007).
Globally, neonatal tetanus accounts for 7% of neonatal deaths, but accounts for more than 48%
in Africa (Peter & Johnson 2010). Nigeria has one of the highest infant mortality rates of 94
deaths/1,000 live births (WHO, 2009). According to the report, 26% was due to umbilical
infection (Peter & Johnson 2010; WHO, 2009). In Calabar South Local Government Area of

16
Cross River State, umbilical infection is responsible for 49% of neonatal deaths (Antai &
Effiong, 2009). This study therefore addressed umbilical cord care and management outcome
among mothers in Calabar South Local Government Area of Cross River State, Nigeria.
Statement of Problem
Globally, about 130million babies are delivered annually, 4million (3.1%) die within the first 4
weeks of life (Peter & Johnson, 2010). Twenty- five percent (25%) of these deaths are as a result
of umbilical infection (Peter & Johnson, 2010). In developing countries, most of the cord care is
home based since two third of births take place at home (WHO, 2009). Peter and Johnson (2010)
reported that, globally, about 150,000 neonates die annually from omphalitis. Each year some
600,000 infants die of neonatal tetanus in Africa; in untreated cases, case fatality rate approach
100% and a further 460,000 die as a consequence of other severe bacterial infections (Peter &
Johnson, 2010).
In Nigeria, several hospital-based studies have reported cases of umbilical cord infections. For
instance, in Port Harcourt, umbilical cord infection accounted for 10% of neonatal admissions
and 30% of neonatal deaths (Antai & Effiong, 2009). A review of umbilical infection in Ibadan
showed that it accounts for 18% of neonatal deaths (Bennet & Adetunde, 2010). In Calabar
South Local Government of Cross River State, 49% of neonatal deaths were due to umbilical
cord infection while the condition was responsible for 19% of all newborn admissions (Antai &
Effiong, 2009). Many of the neonatal deaths occur at home and therefore unseen and
unaccounted for in official statistics (Ambe, Bello, Yahaya & Omotara, 2010; Green, Udoh &
Peters, 2006; Garner, 2008). According to the reports, many of these neonates are brought in for
admission in very bad state, consequently resulting in neonatal deaths. Unfortunately, these

17
statistics reflect the hospital facility situation, little or no information is available for cases of
home neonatal deaths from umbilical cord infection.
From the researcher’s experience as a practicing pediatric nurse, several cases of umbilical
infections have been rushed to neonatal units often too late to be helped. It is not unusual at
primary health facilities to witness several cases of umbilical cord infections. The question that
comes to mind which is the problem is - how do mothers manage the umbilical cord since two
third of births take place at home in developing countries and cord care is home based? It is
therefore desirable to determine the Umbilical cord care and management outcome among
mothers in Calabar South Local Government Area of Cross River State, Nigeria.
Purpose of the Study
The aim of this study was to examine umbilical cord care and management outcome among
mothers in Calabar South Local Government Area of Cross River State - Nigeria.
Objectives of the Study
Specifically, the objectives of the study include to:
1. determine the level of knowledge of standard cord management and sources of
information among mothers in Calabar South Local Government Area.
2. identify the various materials used by mothers for umbilical cord management.
3. identify the reasons for the choice of materials used in umbilical cord management.
4. determine the techniques for cord management among mothers in Calabar South Local
Government Area.
5. determine outcome of cord management in relation to materials used.

18
6. determine the association between the demographic characteristics of mothers and cord
management.
Research Questions
1. What level of knowledge do mothers have regarding standard cord management and from
which source of information?
2. What materials do mothers use in the management of umbilical cord?
3. What are the reasons for the choice of materials for umbilical cord management?
4. What are the techniques used by mothers in umbilical cord management?
5. What are the outcomes of cord management in relation to materials used?
6. What is the association between demographic characteristics of mothers and cord
management?
Significance of the Study
Findings from this study will provide information to the health personnel on the various
materials used by mothers for umbilical cord care, reasons for the choice of materials, the basis
on which health decision are made by mothers in relation to cord management. These will
provide specific intervention(s) in form of health education to mothers to reinforce evidence -
based strategies for effective cord management for better neonatal outcome.
It is also hoped that findings will serve as source of knowledge to mothers on standard cord
management, thereby resulting in reduction in umbilical cord infections and neonatal deaths. The
findings will also serve as source of knowledge to the community on standard cord management,
thereby reducing umbilical infection and neonatal mortality in the community and society at
large.

19
Academically, this work will serve as reference to other researchers in related fields.
Scope of the Study
The study focused on mothers in Calabar South Local Government Area of Cross River State,
Nigeria. It was delimited to umbilical cord care and management outcome among mothers in
Calabar South Local Government area of Cross River State. It was also delimited to the
knowledge of standard cord management and sources of information, materials used by mothers,
reasons for choice of materials, techniques of cord care, and the association between the
demographic characteristics of mothers and cord management.
Operational Definition of Terms:
Umbilical Cord Care: the various materials used in cord care, the reason for the choice
of materials by mothers and the techniques used for cord care.
Knowledge of Standard Cord Management: implies awareness of the recommended methods
of cord care which are: tying the cord with cord clamp, cutting with clean object, cleaning with
methylated spirit and keeping it clean; the range of cord separation time which is between
15days and knowledge of advantages of cord care which is to prevent cord infection.
Materials used: tools for cutting and solutions/substances used for cleaning or applying on the
umbilical cord such as sterile scissors, surgical blade, sharp stones, alcohol (methylated spirit),
salty water, breast milk, herbal preparations, “Ndodop” lantern wax, salt, saliva and sand, triple
dye, strips of cloths and tree bark fiber.
Techniques Used by Mothers: method of cleaning the umbilical cord, the frequency, wet or
dry care, closed or open wound care.

20
Wet Care: use of liquid materials in cleaning the cord at the time of delivery and care is repeated
daily until the umbilicus heals.
Dry care: no cleaning nor application of liquid / substances to the cord after birth till it heals
naturally.
Closed wound care: the use of umbilical binders or bandage after cleaning the cord.
Open wound care: the umbilical cord is left uncovered after cleaning to promote drying, cord
separation and healing.
Reason for choice of substances: why mothers choosed the various materials for cord care. The
reasons may include cultural and religious beliefs, influence of health workers and significant
others (mothers/mother in-law, Traditional Birth Attendants, church members).
Management outcome: entails cord separation time and healing in relation to material used for
cord care. If there was any infection (red skin around the base of the cord, yellow discharge from
the cord, foul smelling cord, pain when touched the skin around the cord, unable to open
mouth/suck or twitching) and how it was managed.
Demographic characteristics: used in this study were age, educational attainment and income of
the mothers.

21
CHAPTER TWO
LITERATURE REVIEW
This chapter reviewed relevant literature on the topic and has been presented under the following
subheadings:
• Conceptual review
- Umbilical cord
- Management of umbilical cord
- Materials used for cord management.
- Reasons for choice of material
- Techniques of cord management
- Factor influencing cord management (age, educational attainment and income of
mothers)
- Cord infections
- Outcome of cord care by mothers
• Theoretical review
- Orem’s Self – care theory
• Empirical studies
• Summary of literature review
Conceptual Review of Umbilical Cord
The umbilical cord or funis when fully developed is about 1.3-1.9cm in diameter and about 56cm
in length. It begins at the umbilicus of the embryo and is inserted into the central region of the
placenta. The cord contains three blood vessels - two umbilical arteries and one umbilical vein.
These are enclosed and protected by Wharton’s jelly, a gelatinous substance formed from
mesoderm. The whole cord is covered in a layer of amnion continuous with that covering the

22
placenta. The blood flowing through the cord brings nutrients and oxygen from the mother to the
fetus and carries away carbon dioxide and other metabolites from the fetus (Abba, 2008).
When the umbilical cord is cut after delivery, the cord stump which is the distal end of the cord
is suddenly deprived of its blood supply and soon starts to dry and turns black and stiff (dry
gangrene). The instrument used cuts through living tissue and vessels that are still connected to
the infant’s blood stream; it therefore needs to be sterile to avoid infection. Drying and
separation of the cord is facilitated by exposure to air. The devitalized tissue of the cord can be
an excellent medium for bacterial growth, especially if the cord is kept moist and unclean
substances are applied to it (Bemor & Uta, 2011). The umbilical vessels remain patent for a few
days following birth, thus providing direct access to the bloodstream. The umbilical cord is a
common route of entry for systemic infection in the newborn infant, keeping the cord clean is
therefore imperative if infection is to be prevented (Bemor & Uta ,2011).
Management of Umbilical Cord
Clean cord care involves washing hands with soap and water before delivery, tying and cutting
the umbilical cord with sterile instrument and finally laying the baby on a clean surface. The
objectives of hygienic cord care practices as outlined by WHO (2006) are to prevent
consequences of unclean cord care which may include umbilical cord infections and neonatal
deaths. Thus mothers are to adopt current standard of cord care which are based on the principles
of asepsis that help in the reduction of cord infections. The sterile materials that can be used in
tying the umbilical cord as recommended by WHO (2007) include sterile plastic cord clamp,
narrow tapes and threads of cloth. These materials if sterile and properly applied will effectively
prevent infection of the umbilical cord and death of the neonates. It is recommended that
instruments used in cutting the cord should be sharp and sterile to avoid trauma and infection of

23
the cord. Such instruments include sterile scissors or new razor blade. A knife can be used
provided it is washed and sterilized.
The frequency of cord cleaning and dressing varies between institutions and between cultures.
WHO (2007) recommends on the average, cleaning once daily and as often as each diaper is
changed. The normal practice is to clean the cord with cotton swab soaked in methylated spirit
and left uncovered to promote drying, healing and cord separation (WHO, 2007). During the
cleansing process, the napkin should be folded below the umbilicus; particular attention should
be paid to the base of the cord to prevent infection. At this time the base of the cord is wet and
dark and therefore can form a nutritive culture medium for bacterial growth. The cord normally
falls off between 5 to 15 days after birth. These practices should constitute the measures adopted
by mothers to promote healing, prevent infection, neonatal morbidity and mortality.
In some communities in Bangladesh, mothers often cleanse the cord stump with dry gauze,
cotton ball or topical application of antimicrobial agents. In Nepal, colostrum, saliva or herbal
preparations are applied to facilitate early cord separation and healing, but rather these constitute
serious sources of neonatal infections. Clean cord care at birth and in the days following birth is
effective in preventing cord infection, increase the rate of child survival and reduction in
neonatal deaths (Ahmed & Verber, 2011; Garner, 2008; WHO, 2006).
Knowledge of Standard Cord Care and Sources
Senarath (2010) reported that lack of knowledge of standard cord care is an important factor
underlying unhygienic umbilical cord management among mothers. He added that mothers who
are knowledgeable of standard cord care and the possible risk for non-adherence are more likely
to employ standard cord management. Lack of knowledge of standard cord care affects mothers’
ability to make independent decision on cord care especially among the primiparas and these

24
neonates are thus in a vulnerable situation. He noted that the neonatal health outcome could be
improved significantly by strengthening information, education and communication to mothers.
Materials for Cord Management
The past decades have seen a reconsideration of what, if anything should be applied to the
umbilical cord after birth (Thompson, Udom & Ugorji, 2011). Dore, Buch and Tom (2007)
reported that the America Academy of pediatrics supports non application of antiseptics .to the
cord after birth, although many recent investigations suggest that colonization rate with
pathogens are unacceptably high without application of topical antiseptic to the cord especially
in developing countries where majority of births take place at home (Thompson, Udom &
Ugorji, 2011).
[[ Today cord management varies greatly from institution to institution. In the United States of
America, substances currently used for cord management include triple dye, alcohol, antibiotics
ointment, providence-iodine and polymixin bacitracin. Salicylic powder and salicylic sugar have
also been used in the cord care in neonates. Potential drawback in the use of the latter in
developing countries includes its cost and availability. Also the association of salicylic sugar
with cord bleeding may be a fatal complication at home (Bassey, Thompson & Udia, 2009;
Garner, 2008; WHO, 2007).
There is not enough evidence to recommend the wide spread use of topical antibiotics in
developing countries. There is some evidence, however, that they are protective against neonatal
tetanus and other neonatal infections when applied to the cord for the first few days. In some
high risk areas, especially where the custom is to apply dangerous substances to the cord; it
might therefore be useful to advice using topical antimicrobial as a transitional measure to help
wean the community away from harmful substances (Mueller & Johnson, 2009).

25
As documented by Obuekwe and Obuekwe (2008) various materials have been used by mothers
and other care givers for umbilical cord care in developing countries. These range from varieties
of tools used to cut the cord to substances applied. These tools are usually items that are
available in the home, such as scissors, knives, broken glass, sharp stones or used razorblades
which are rarely clean or boiled before use (Obuekwe & Obuekwe, 2008).
Reasons for Choice of Substance for Cord Management
There are various reasons for choice of substances for umbilical care. Some of these substances
and methods are based on traditional beliefs which often are interwoven with witchcraft, magic
and taboo. These substances are provided by older relatives and at most times by the Traditional
Birth Attendants (TBAs), who attend to more than 70% of deliveries in Nigeria (Ahmed &
Verber, 2011; Bello & Omotara, 2010). These substances are available in the form of various
traditional concoctions such as saliva mixed with herbs and administered topically, bathing the
neonate with grounded local herbs and in some cases, the liquid content of the leaf ’’Ndodop’’ is
wrung out and applied directly on the cord stump. These are directed at driving away the
suspected evil spirit that is responsible for neonatal deaths (Bennett & Adetunde, 2010).
The reality is, however, that the TBAs continue to attract large clients because they live within
and are easily accepted as part of the culture and tradition of their local communities. They are
easily accessible to their clients, they do not insist on payment before care is rendered and care
does not disrupt family processes which are some of the reasons they are patronized. Adeleye,
Sadiq and Tam (2011) also reported that most families do not save money to incur delivery
related cost due to economic constraint and social access to health facilities. Consequently, home
deliveries are common and conducted by mothers-in-law or TBAs who cut and dress the cord
with herbal preparations.

26
Furthermore, Waise and Kaikoba (2008), Okedo, Nelson and Lawal (2011) reported that these
substances are believed to help the cord to dry and separate faster within 3days and save the
neonate from “evil eye” which they believe causes neonatal deaths. The early cord separation
also enables women get back to their routine chores early as they are not expected to engage in
such or seen outside until the baby’s cord stump detaches (Buckley & Thompson, 2010; Alam &
Murray, 2008). The quick healing of the cord is also believed to stop the pains “afterpain” that
women feel following birth of a newborn baby. Visits to the baby are restricted while the
umbilical cord is still intact; as a measure to ward off evil spirit that could be attracted to the
baby (Alam & Murray, (2008). As a result, babies are kept indoors while mixture of salt, saliva
and sand from the door post, cow dung and herbal preparation are applied to the cord to enhance
quick separation. They authors assert that one of the most dangerous practices is the application
of sand to the cord, because such materials often harbor tetanus spores from the soil and thus
increase the risk of neonatal tetanus.
Cow dung is another substance applied to the umbilical cord, a practice that has its origin in
religious and cultural tradition. Cow dung is applied to umbilical cord because of its high
moisture absorption rate. It dries the cord rapidly, which is an advantage in many traditional
cultures as the mother and baby cannot join the rest of the house hold until the cord falls off
(Basil, Kayode, Mark & Mbe, 2009).
Basil, Kayode, Mark & Mbe, (2009) however, commented that traditional beliefs should be
taken into account when introducing clean cord care programmes in a community since their
beliefs may conflict with programme recommendation. Practice will not change unless people
are convinced that the new care regimen is indeed better. Other methods include severing the
cord very close to the base and application of herbs and sacrificial marks. The herbal preparation

27
and traditional practice are preferred because the cord falls within 3-4 days of application; the
wound heals faster and quicker relief of pain. The delayed cord separation usually increase
parents’ anxiety, thus all measures are taken to hasten cord separation (Bemor & Uta, 2011;
Basil, Kayode, Mark & Mbe, 2009; Mueller & Johnson, 2009).
Techniques of Cord Care
Various techniques have been used for umbilical cord care, many authors have suggested leaving
the cord stump dry. Different approaches to cord care have been evaluated in terms of their
impact on timing of cord separation, bacterial colonization and infection (Thompson, Udom &
Ugoji, 2011). Other supportive care to enhance healing includes exclusive breastfeeding,
maintenance of warmth and cleanliness (Garner, 2008; WHO, 2007).
Frequency of treatment also varies. In some cases the cord is cleaned and/or treated at the time of
delivery; in others, care is repeated daily until the umbilicus heals (Garner, 2008; WHO, 2007).
The use of umbilical binders was discontinued decades ago when it was found that they
frequently harbored bacteria and hindered healing by not allowing the cord to dry (Pezzati &
Biagioli, 2008).
Other methods of cord care include application of various substances. These substances are
either applied directly on the umbilical cord; the water is slightly squeezed out before application
or mixed with other substances and heated on fire in local earthenware pots before application.
Other techniques include placing certain leaves on the entrance to the baby’s room, herbal
preparation under the baby’s bed or on the baby’s forehead or applied on the whole body
including the cord. At other times, the herbal medicine which are mostly made from leaves, roots
and/or bark of trees are given as oral medication to the neonate in unregulated dosage. These

28
usually produce toxic effects which are difficult to manage, as antidotes are unknown. Other
forms of management include sacrifices to the gods (Bennet & Adetunde, 2010).
Umar and Alliu (2011) also reported of “bundling.” This consists of wrapping an infant for
prolonged periods in a sheep skin after dried cow dung is applied. This demonstrates the
vulnerability of the umbilical cord to infections during the first days after birth. Bemor and Uta,
(2011), Basil, Kayode, Mark and Mbe, (2009) and Mueller and Johnson, (2009) also reported
severing the cord very close to the base, application of herbs and sacrificial marks on the face
and on the anterior abdominal trunk. These measures may or may not have medicinal properties
to heal the cord as they are typically passed by laypersons and majority of these substances are
merely used as a result of tradition. Some, however, have been demonstrated to effectively aid
cord healing. One of the more popular examples is the warm compress to reduce inflammatory
process and aid healing.
Factors Influencing Umbilical Cord Management
Factors which may influence cord care practices include age, educational attainment and socio-
economic status of mothers. Smith and Kelly (2011) reported that age at first pregnancy was
significantly related to who cares for the baby’s umbilical cord and material used. Clean cord
care was found among mothers aged 35 and above while cord infections were higher in babies
whose mothers were 20years and below. They therefore, concluded that increased maternal age
was associated with safe cord care practice with improved neonatal outcome.
Socio-economic status has also been associated with clean cord management. Okedo, Nelson and
Lawal (2011) reported that mothers with low-income prefer home delivery for fear of facing
higher financial expenditure in heath facilities. This decision they noted increases neonatal cord
infection and death. Thompson et al (2011) also report that socio-economic barriers could cause

29
delay in decision making thereby increasing the risk of complications resulting from cord
infection and deaths among the neonates.
Peter and Ube (2010) reported that unclean cord care was found among mothers in the lowest
educational group. The report also indicated that women who had less than a high school
education are less likely to employ clean cord care practice. Tuladhar (2010) also reported that a
higher level of educational attainment has a positive effect on decision to practice clean cord
care. He added that cord infections and complications were common in babies whose mothers
were with demographic risk factors such as low level of education. These assertions are based on
the fact that a higher educational attainment helps to modify behavior and as such is capable of
improving hygienic cord practices and neonatal outcome.
Cord Infections
A large epidemiologic study in neonate has shown that the incidence of infection has been
increasing steadily over the past few years. Up to 90% of neonates who are not treated with
antiseptic in developing countries are colonized with pathogenic bacteria and the risk of
developing infection is related to the degree of colonization (Harrison & Stanley, 2007). It is
important to note that the exposed necrotic tissue of the umbilical cord is readily colonized and
infected by pathogenic bacteria. Once colonized, the umbilicus acts as a reservoir of bacteria.
Ready access of the bacteria into the system circulation places neonate at high risk for infection.
The greatest period of risk for umbilical cord contamination with bacteria including clostridium
tetani, is the first three days of life. Risk decreases with time as the umbilical wound heals and
the cord separates. The risk of cord infection is increased by unhygienic cutting of the cord and
the application of unclean substances to the cord. Infection may remain localized or may spread

30
inwardly. Infection can delay or prevent obliteration of umbilical vessels, and organisms thus
having direct access to the newborn’s blood stream. Septic thrombi may form within the
umbilical vessels, sending septic emboli to various organs – including the lungs, pancreas, heart
and kidneys and causing infection of these organs as well as septicemia (Peter and Ube, 2010).
Infection may also spread by direct extension onto the peritoneal cavity, causing peritonitis.
Associated signs such as fever, lethargy and poor feeding suggest systematic complication. In era
of early postpartum discharge, the care and management of the umbilical cord rest in the hands
of the mothers or relatives with likely risk for application of contaminated substances (Peter &
Ube, 2010; Gaana, 2009). Statistics indicate that globally, under – five mortality rates have
declined over the past decades, but high neonatal mortality rate have remained relatively
unchanged in the developing world, where 90% of babies are born (Gaana, 2009).
Neonatal tetanus caused by Clostridium tetani is among the most severe anaerobic neonatal
infections in developing countries (WHO, 2009). It often arises from infection of the umbilical
cord. Globally, tetanus accounts for 7% of neonatal deaths, but accounts for more than 33% in
Nigeria, one of 27 countries that account for 90% of the global burden of the disease (Peter &
Johnson, 2010). It is a deadly disease for newborns, with a case fatality rate of 70 percent to 100
percent (Peter & Johnson, 2010). In the University of Calabar Teaching Hospital, (UCTH),
Calabar, 63% percent of neonatal deaths were due to neonatal tetanus while this condition was
responsible for 31% of all newborn admissions (Basil et. al, 2009).
Neonatal tetanus (NNT) is an acute disease characterized by generalized rigidity and convulsive
spasms of skeletal muscles. It occurs as a result of unhygienic birth practices, most commonly
when tetanus spores contaminate the umbilical cord at the time that it is cut or dressed after
delivery (Thapa & Keshi 2011). Symptoms of neonatal tetanus usually appear on the third day

31
after birth. An apparently healthy baby will stop sucking, become progressively more rigid, and
develop an arching of the whole body and experience painful convulsions with associated
hyperthermia. The disease occurs most commonly in the lowest income countries and those with
the least developed health infrastructure. Within these countries, it is frequently found among
populations with little or no access to health care services or education. It has been described as a
social scourge.
A detailed analysis of the epidemiology of the disease has shown that the mothers are usually
very young (aged <20 years), single, with either no formal education or primary level education,
and resident in rural communities. They are therefore likely to have a low tetanus toxoid
coverage rate, unlikely to attend antenatal care during pregnancy, likely to deliver outside a
medical establishment and therefore attended to by unskilled personnel. Care of the cord after
delivery may be unhygienic, with attendant complications and deaths. Most of these deaths occur
at home before the baby reaches two weeks of age and neither the birth nor the death is reported,
the number of cases reported by countries is low. For this reason, neonatal tetanus is often called
the invisible killer (WHO, 2009).
Reducing deaths from neonatal tetanus is one of the simplest and most cost-effective means to
reduce the neonatal mortality rate. Immunizing women of reproductive age or every pregnant
woman with the tetanus toxoid vaccine can pass immunity on to the fetus and also prevent
tetanus infection in mother during child birth. It is important to note that neonatal infection with
tetanus does not provide long – term immunity. These infants should therefore not be omitted
from active immunization programs (Mentu & Benson, 2009; Abba, 2008).
Omphalitis is one of the most common neonatal infections that cause death in neonates with an
estimated 2.4 million annual deaths globally. In sub-Saharan Africa, the estimated proportion of

32
death attributed to omphalitis is 35%. Both gram-negative and gram-positive organisms may be
involved (Dibson & John, 2010; Mueller & Jonhson, 2009). Infections may be localized or
spread inwardly causing septicaemia and infections of internal body organs including the lungs,
heart, kidneys and pancreas. Omphalitis is therefore a very serious infection that requires
aggressive treatment. Signs of inflammation (Erythema, oedema, tenderness) of the tissues
surrounding the cord support the diagnosis of omphalitis. There may be a purulent discharge
from the cord. Associated signs may be fever, lethargy; poor feeding and this may suggest
systematic complications. Sometimes, there is no obvious outward sign of infection, and the
diagnosis can be made only at autopsy (Garner, 2008; Green, Udoh & Peter, 2006).
Treatment of omphalitis requires a full sepsis workup and parenteral antibiotics (usually clo-
xacillin and aminoglycoside). For neonates with omphalitis, appropriate case management with
antibiotics can avert most deaths, but only if families recognize signs of illness and seek care
promptly. However, due to lack of recognition of symptoms of severe illness, socio-economic,
geographic and cultural factors, many moderate and severe omphalitis are treated in the home or
seek care too late; sometimes resulting in death. The seriousness of the condition is emphasized
by the complications seen with progressive disease. These are related to continuous spread to
adjacent soft tissues or umbilical blood vessels. These include abdominal wall cellulites,
necrotizing fasciitis or peritonitis and umbilical arteries or phlebitis with hepatic vein thrombosis
or hepatic abscess.
Prevention of omphalitis includes routine cord care – the use of a plastic cord clamp at birth and
alcohol for cleaning. Alcohol helps drying of the cord and prevents colonization and infection.
Topical antibiotics (bacitracin, Neomycin) may also be used as part of an attack on an epidemic
of neonatal staph aureus infections (WHO, 2009; Dore, Buch & Tom, 2007).
[

33
Cord Separation Time
Separation of the umbilical cord occurs by inflammation of the junction between the cord and the
skin of the abdomen. Separation may be associated closely with the care of the cord (Bello &
Omotara, 2010; WHO, 2006). Zupan (2007) stated that care of the umbilical cord has an effect
on the length of time taken for the cord to separate. Antimicrobial ointment slows down the
drying and necrotizing processes. Triple dye on the other hand, is nearly as effective as
astringent powder in causing earlier sloughing of the cord. Various views on cord separation
time indicate that there is shorter cord separation time with no topical care or no intervention
compared to antiseptic but it is associated with high incidence of umbilical infections and
neonatal deaths (Arad, 2009; Farahani, 2008).
Shafique and Jack (2006) stated that the average time for separation with the use of antiseptic is
between five and fifteen days. According to them the clinical impact of delayed cord separation
has not been recorded, but it has social and cost implication in developing countries. Delay
makes mothers anxious, and increases the risk of tampering with the healing process, thus
increasing risk of infection. Awareness of this limitation calls for more commitment on the part
of health providers to increase the awareness of mothers and other caregivers. If the mother is
made aware that care of the umbilical cord may delay cord separation, she may be spared
unnecessary concern.
Theoretical Review
Concept of Orem’s Self – care Theory,
The conceptual model of the study is derived from the Orem’s self-care deficit nursing theory.
The theory provides guidance for defining variables, specifying the relationship between them
and evaluating programme concerned with umbilical cord management.

34
Orem’s self- care theory was first published in 1971. The theory consists of three related
theoretical constructs (a) theory of self-care (b) theory of self-care deficit and (c) theory of
nursing systems (George 2011). Orem’s self-care theory is useful in determining the kind of
nursing assistance needed by the client and therefore has merit as a theory that guides research
and practice. The theory offers nurses the basis to work with client or dependent care giver in
developing their self-care agency (George 2011). This study is directed primarily at self care
within the concept of dependent care agency.
The condition that validates the existence of a requirement for nursing in adult is the health-
associated absence of the ability to maintain continuously that amount and quality of self-care
that is therapeutic in sustaining life and health, in recovering from disease or injury or coping
with their effects. With children, the condition is the inability of the parent ( or guardian)
associated with the child’s health status to maintain continuously for the child the amount and
quality of care that is therapeutic, example of such required in the management of the umbilical
cord.
Self-care agency is concerned with the human acquired power and capabilities to engage in self-
care. Under usual circumstances, adults care for themselves. However, those who are young,
aged, ill, or disabled need either help with self-care or complete assistance in those activities
necessary to meet self-care needs. That is, those who are young like the neonates require that
another person described as the dependent care-agency or dependent giver (mother) should care
for him in activity such as umbilical cord management to maintain life, health and well-being.
Thus, babies rely on dependent care givers. The ability of the dependent care giver (mother) to
engage in self-care, that is umbilical care management could be affected by basic conditioning
factors. These include: age, educational attainment, socio-cultural orientation, and environmental

35
factors (unhygienic place of delivery) and resource adequacy and availability. That is, the basic
conditioning factors can enhance or hinder the ability of the mother to render care that is
therapeutic. For instance, among the demographic characteristics such as age, older mothers may
be more aware of clean cord care and risk of infection based on experience over the years (Smith
& Kelly, 2011).
Furthermore, one of the traditional measures used to assess social structure is education. The
social structure also relates to the income (socio- economic status). Increased educational
attainment increases knowledge of standard umbilical cord management. Increased educational
attainment could also increase mothers’ power in decision making that can promote hygienic
cord care and reduction in umbilical cord infection (Obimbo & Oruambo, 2008). In addition, an
individual financial capacity is determined by the level of education as well as the type of
occupation she is engaged in. Availability of funds to access health service may influence the
choice of source from which care is sought by mothers. Without money, mothers cannot make
independent choice about their health nor the health of their babies (Sharan, 2011)
Moreover, socio-cultural orientation could play a key role in individual beliefs and practices. It is
logical that when people believe and attribute causes of disease or death to supernatural powers,
such as attributing neonatal deaths to “odon”, they will be more likely to do something to keep it
under control. This is what prompts mothers to use various forms of materials for umbilical cord
management to hasten cord separation and prevent neonatal deaths which unfortunately may
result in cord infection. These materials are recommended by the elders (mothers, mother in-laws
and traditional birth attendants).

36
CONCEPTUAL MODEL OF THE STUDY
Independent variables
variables Intervening variables Dependent
variable variable
Independent variabl
Dependant variable
Intervening variables
Fig 1: Conceptual model of the study adapted from
Orem’s Self-Care theory.
Nursing system
(Supportive –
educative)
Dependent Care
Agency:
- Knowledge of
recommended
standard cord
management
- Skills in care
for dependant
Basic Conditioning Factors:
• Socio-cultural factor :
- customs, beliefs
- Family influences
- Resources adequacy
and
availability
• Educational attainment
• Age
• Developmental stage
Environmental Factors:
• Physical environment
- poor sanitation
- unhygienic place of
delivery
• Biological environment
- micro organisms
• Psycho-social environment :
- family and church members
• Proper
management of
umbilical cord:
- Use of
recommended
substances in
cord care
- Use of
recommended
Techniques/skill
- Positive outcome
(dry and healing)

37
The independent variables are the knowledge of recommended standard cord management and
skills in the care of the dependant. The intervening variables are the basic conditioning factors,
these include: age, educational attainment, socio-cultural orientation, environmental factors and
resource adequacy and availability.
The dependent variables are described as the expected outcome of the intervention. They
include: proper management of umbilical cord, use of recommended skills/ techniques and
positive outcomes (dry and healing cord). The intervening variables are expected to influence the
degree to which the independent variables will determine the umbilical cord management.
The researcher conceptualizes that providing support, guide and teach skill to dependent
caregivers using supportive - educative system will assist the dependent care givers to gain
knowledge of standard cord management, make decisions and control behavior. These will
prevent infection; promote health, well being and neonatal outcome.
Empirical Review
The focus of the empirical review was on umbilical cord care and management outcome among
mothers and the arrangement was based on the variables under study. Senarath (2010) assessed
the patterns of mothers’ knowledge of newborn care practices as well as factors associated with
poor knowledge. The respondents who were 446 mothers with newborn from five hospitals in
Puttalam district of Sri Lanka were interviewed. The findings revealed that mothers had a
satisfactory level of knowledge about breastfeeding and recognition of danger signs, but
knowledge about hygienic umbilical cord care was poor. Multivariate analysis results showed
that primiparae 69% and unemployed women, 32% were more likely to have poor knowledge.
The result indicates that women who are pregnant for the first time lack experience regarding
health care compared with those women in their subsequent pregnancies. Therefore, they are

38
likely to have poor knowledge. Being unemployed restricts women from contacting persons
outside their home, thus they are likely to acquire less health information compared with those
who are employed. Women who book for antenatal service later in pregnancy receive inadequate
health information and thus might miss out some of the important health messages. All these
conditions make them less knowledgeable about newborn care issues.
Luka (2011) studied the mother’s knowledge of cord care practices in an urban slum area in
Nairobi, Kenya, where 307 mothers with infants less than three months of age attending clinics
were interviewed using interview guide. The results showed that 91% of mothers knew of the
need for hygiene while cutting and tying the cord. As for postnatal cord care, 40% had good
knowledge and 66% had good practice. Results of a multivariate analysis showed that increased
levels of education, living in middle class areas, increased maternal age, and acquisition of
knowledge from health workers rather than from other sources had significant independent
association with good maternal knowledge, attitude and practice.
A related study on knowledge of cord care among mothers in south west zone of Nigeria as
documented by Green, Udoh and Peter (2006) indicated that out of 328 mothers with newborns
that were interviewed using questionnaire as interview guide, 11.9% reported knowledge of cord
care during antenatal visits. Sources of information on cord care were mainly from mothers,
53.3% and Traditional Birth Attendants, 29.6%. About 20.6% of the newborn had umbilical
infection while 3.5% reported fever, skin rashes and other minor ailments. They therefore
suggested increased awareness on standard cord care practices.
A cross sectional descriptive study was carried out by Alam and Murray (2008) on specific
behaviors regarding newborn cord management in Sylhet District in Bangladesh. Data were
collected by means of questionnaire developed by the researchers. The finding revealed that out

39
of the 436 infants of consenting mothers, 90% of deliveries occurred at home and the umbilical
cord was severed by mothers in more than 57% of the cases. Powder was commonly applied to
the cord after cutting in 52% of cases; while in 83% of cases “turmeric” was the most common
application. Umbilical cord care revolved around bathing, skin massage with mustard oil and
heat massage on the umbilical cord occurred in most cases; while only 40% of newborn were
bathed on the day of birth. Cord care was provided by mothers and mother- in-laws during the
neonatal period and 19% of respondents reported umbilical infections in their infants. Based on
the prevalence of unhygienic cord practices in the area and neonatal infections, the researchers
suggest increased efforts to promote hand-washing, topical application of antiseptic, avoiding
unclean home application to the cord to reduce exposure to infection and improved neonatal
outcome. Such efforts, according to them, should broadly target a range of care-givers, including
mothers and others female household members.
In similar studies, Bang and Andem (2011) in Ika in Akwa Ibom State and Ambe, Bello, Yahaya
and Omotora (2010) Konduga in Bornu State reported the use of lantern wax, natives and
various forms of herbal preparations in cord care in an urban setting using 420 and 380 mothers
of babies who were three months and below respectively. This reflects the persisting risk for new
neonatal tetanus in city centers, as well, where there is availability of health services and higher
vaccination. They therefore suggested that studies need to look beyond demand variables such as
the knowledge of mothers and utilization of health services to cultural influences on health
behaviors and need for health education in all communities, both rural and urban centers.
Ambe et al (2010) carried out a study in Konduga local Government Area of Borno State,
Nigeria on practices of cord management in the area. Two hundred and eighty (280) mothers
with infants of three months and below were interviewed using structured questionnaire.

40
Findings revealed that substances used by mothers in cord care include, the application of hot
fermentation, use of rag and lantern wax, use of Vaseline, ash, charcoal, groundnut oil, palm oil,
mangrove oil, use of powder and red sand. They pointed out that these practices are often
harmful, because these substances are often contaminated with bacteria and spores thus
increasing the risk of infection particularly neonatal tetanus. Only 12% of mothers/caregivers use
alcohol, while in about 10%, the cord was left alone to dry on its own. The researchers concluded
that mothers need to know about these harmful practices, what they may cause and the problems
associated with their use. Health providers should be able to educate the mothers about the
harmful practices of cord care. This will go a long way in reducing the morbidity or mortality in
the newborns.
A number of reviews on clean cord care and level of mothers’ education have been published.
The majority of these reviews concluded that apart from the place of residence, perhaps no other
social variable has been associated more often with difference of attitude with regards to health
care than education (Eneji, Eyamba & Makinde, 2010). Thus a significant correlation has been
noted between mothers’ level of education and clean cord management. The authors reported
that clean cord care was found among mothers in the highest education group and neonatal
outcome was better. This was attributed to the fact that these mothers had been exposed to some
medical information from the media and other forms of enlightenment pertaining to child care.
Uneducated women lacked decision making power and unable to resist social pressure from
family and peers, as such they comply with existing tradition. They concluded that it is nearly
impossible to consider behavioral changes in health care practice without simultaneously
considering the level of education of the subjects, which deeply influences personal conduct
especially in the area of child bearing and neonatal care (Thompson, et, al. 2011; Sharan, 2010;

41
Tuladhar, 2010). Studies in Minna, North Central Nigeria also reported the use of mentol/rub
ointment and hot compress in cord management among 84% of 448 mothers in low educational
level (Peter & Ube, 2010; Okedo, Nelson & Lawal 2010).
Findings from a qualitative data collected by Jeol- Madewase, Oyedeji and Elem (2008) showed
an association between socio- economic status and clean cord care. They studied factors
influencing new born care among rural community in South West, Nigeria. From an in depth
interview with 60 mothers whose babies were one year and below using check list, they observed
that about 27% of those with clean cord care belonged to middle socio-economic background,
about 53.4% fell within low socio-economic background and 19.6% fell within high socio-
economic background. Most families did not save money to incur delivery related cost due to
economic constraints and social access to health facilities. Consequently, home deliveries were
common and conducted by the mother-in-laws or Traditional Birth Attendants (TBAs).
In instances when the TBA was called/arrived after the delivery or until the placenta was
delivered the newborn was laid wet uncovered on the floor, increasing the risk of neonatal
hypothermia, which is known to account for almost 13% of neonatal deaths in rural
communities. Blade was dipped in hot water before cutting the cord. The mothers claim “using a
new cotton thread and dipping the new blade in hot water before using removed the poison of
blade and prevented umbilical sepsis.” Though this practice was carried out with good intention,
mere dipping this substance in hot water could not kill the bacteria but possibly increase the
newborn’s susceptibility to sepsis, which is a known cause of about 52% of neonatal deaths in
rural communities (Jeol- Madewase, Oyedeji and Elem, 2008).
In a study carried out by Baqui and William (2009) on influence of socio-economic status on
clean cord care among mothers in Edo, South West Nigeria. The 438 respondents were drawn

42
from consenting mothers whose babies were three months and below. A descriptive design was
used and data were collected over a period of six months using researcher developed
questionnaire. Finding indicated that, unforeseen emergencies due to delay in identifying the
problem related to unclean cord care, and subsequent delay in making last minutes arrangements
for money and transportation, the risk of complications were increased in newborn. They
submitted that women who where socio-economically advantaged were more health conscious of
clean cord care compared to women who were socio-economically disadvantaged (Baqui &
William, 2009).
A cross sectional study carried out in North West Nigeria by Adamu, Harrison and Wale (2009)
on newborn care revealed that 84% of mothers prefer traditional care at delivery and cord care
for economic and social – cultural reasons. Data were collected from 408 mothers whose babies
were six months and bellow with the aid of structured questionnaire. The study also revealed that
67% of the mothers who belonged to low socio – economic delivered in unhygienic environment
with harmful traditional practices that promotes neonatal infection and neonatal death. About
14% belonged to the high socio economic status. The researches therefore suggested education
and economic empowerment of women with soft loan
In a study carried out by Obimbo and Oruambo (2008) on knowledge, attitude and practice of
mothers regarding cord care, in Ile-ife, Osun State, 414 mothers whose babies were below 3
months old were recruited into the study. The mothers’ age ranged between 15 and 45years. A
three-step multi-stage sampling was used and data collected using a structured questionnaire.
Findings revealed that 44.4% of mothers were in their teen (15-19years) and about 52% of them
were single and 33% were school dropout. Unsafe methods and unhygienic cord care were
employed in cord care. 30.6% fell within age 20-24 years while 25.4% fell within 25 years and

43
above. They reported that older maternal age was associated with decreased use of unsafe
methods and unhygienic cord care practices. Older mothers were aware of clean cord care and
risk of cord infections. The researcher therefore suggested that early marriage and unwanted
pregnancy can be reduced with increased enrollment of girl child in schools.
Benson and White (2006) in a qualitative study followed 45 mothers through their post natal
period to determine risk factor in neonatal infection. Data were collected using interview guide.
They observed that the use of safe and modern methods in cord care was about five times higher
among mothers who were twenty-five years and above, followed by mothers whose babies
previously had developed one of the threatening complications or died as a result of cord
infection. Review by various authors agrees with Smith and Kelly (2011) in their study on
influence of age on cord care. They used descriptive survey to study 388 mothers whose babies
where two months and below. Data were collected using structured questionnaire. They
documented that about 48% of reported cord infections among new born were babies of mothers
who were below 30 years of age. They observed that age at first pregnancy was significantly
related to who cares for the cord and substances used. The observed that mothers with their first
babies usually depend on others or older relatives who employ cord care which depends on
beliefs, customs and social status and the babies are thus in a vulnerable situation (Dibson &
John 2010; Amin & Khan, 2009; Agarwal & Seith, 2009; Abba, 2008).
In a Large urban University Hospital in Turkey, Meberg and Brown (2007) conducted a pilot
study on umbilical cord care, using 150 healthy, full-term newborns and their mothers. Umbilical
cord care consisted of each of three methods: topical application of povidone-iodine twice daily,
topical application of mother’s milk twice daily or dry care (keeping the cord dry and clean).
Outcome was measured in terms of the presence or absence of omphalitis and the number of

44
days elapsed before cord separation. An ongoing questionnaire was administered by telephone
every other day after the participants left the hospital. In addition to demographic information,
the cord separation day and any sign of Omphalitis (foul smelling, yellow discharge from the
cord, red skin around the base of the cord and pain when touched the skin around the stump)
were recorded in the questionnaire. Omphalitis was observed in 4.2% of babies in the Povidone-
iodine group, 38.4% in breast milk group and 57.4% in dry care group. They recommended
regular cleansing with antiseptics. Report of similar study by Garner, (2008) revealed a
significant percentage (68.4%) of cord infection among new born in the dry care group. They
also suggested daily cleaning of the cord stump with alcohol until it falls off to prevent umbilical
cord infection.
In a randomized study on umbilical cord management, Pezzati & Biagioli (2008) reported on
two different regiments for umbilical disinfection in newborn infants: (1) a bandage of
hydrophobic material (n=1213), and (2) daily cleansing with 0.5% chlorhexidine in 70% ethanol
(n=1223). Infections were registered in the nursery as well as after discharge until 6 weeks of
age, and bacterial cultures taken from infected areas. Infections were registered in 377 (15.4%)
of the 2441 infants. Total infection rates of 16.3% and 14.6% were found in the hydrophobic
material group and the chlorhexidine - ethanol group respectively. Separation of the umbilical
cord stump occurred significantly later in the hydrophobic materials group than in the
chlorhexidine – ethanol group (6.2 + 2.2 vs 5.8 + 2.1). They concluded that daily cleansing with
ethanol prevents umbilical stump infection.
Johnson and Wale (2006) in a local hospital studied the risk factor in bacterial neonatal
omphalitis in South West Nigeria. He reported the relationship between regular cleansing of the
cord stump and bacterial infections in the neonates. Using a survey design, 346 neonate aged

45
below three months and their mothers were included in the study. Structured questionnaire were
used for data collection. Cord care regiments consisted of one of the methods: (i) topical
application of saline daily (locally prepared salt water solution), (ii) topical application of herbal
preparation at birth, (iii) topical application of colostrum at birth, (iv)dry care, (v) topical
application of 70% alcohol twice daily. The incidence of infection recorded 24.4% in alcohol
group, herbal group 25.4%, colostrum group 23.4%, dry care 26.4% and alcohol
0.4%respectively.
The mean age of infant when cord infection appeared was 3.2 days. The report further indicated
that 72% of cord infections in babies born at home were due to gram- negative organisms,
mostly Klebsiella and E. coli, whereas gram-positive infections were slightly more common in
babies born in health facilities. Staph. Aureus was the single most commonly isolated bacterium
both at home and in the hospital. They identified irregular cleansing of cord stump, strong family
influence, and illiteracy and low socio- economic status as some of the risk factors for bacterial
infection.
In a randomized study of cord care regimens and outcome, Anderson and Philip (2004) reported
that treatment with powdered antiseptic rather than aqueous antiseptic resulted in shorter time to
cord separation in 48% out of the 288 babies who participated in the study. The cords separated
in 5.6 + 2.3days for neonates treated with salicylic sugar powder, 6.7 + 2.2 days for neonates
treated with green clay powder, 11.6 + 6.6 days for neonates treated with triple dye, and 16.9+
7.5 days for neonates treated with 70% alcohol. Gladstone (2009) observed that 3.7% cords of
344 babies treated with Hexachlorophene remained attached at 10days compared with 27.9%
cord treated with chlorhexidine and 7.1% of untreated cords. Data were collected using
structured questionnaire

46
Luka (2011) studied 900 newborn and reported statistical differences in cord separation between
cord treated with alcohol (9.8days) and untreated cord (8.2days). Hoque & Selwyn (2008)
compared single triple dye application versus multiple triple dye treatment in neonates and noted
that umbilical cord separation time prolonged with multiple treatments 16.7+ 0.65 days and 12.6
+ 0.45 days with single treatment. Several researchers have compared the effect of various
methods on cord separation and healing time and come up with significant results. The authors
are of the opinion that cord separation is related to solutions used and it is not uncommon for
cord separation to occur after 21 days. The researcher therefore concluded on a strong need to
give appropriate education to mothers and other care givers on cord separation time to prevent
anxiety.
Muella & Johnson (2009) carried out a study on cord care practices in a rural community in
Nigeria. The researchers used a cross sectional design and 2000 mothers who brought their sick
neonates to the clinic were interviewed using structured questionnaire. The findings revealed
that 60% of the neonates had umbilical infection while 28% suffered from asphyxia, birth trauma
and malformations. Only two mothers reported umbilical infection to the clinic within 24hours of
onset of illness. About 84% tried some home remedies before seeking medical assistant. About
68.3% managed the cord stump based on culturally recommended therapies such as herpes, salt
and saliva, breast milk and sand from door post. The researchers therefore, concluded that there
is a strong need to give appropriate education and counseling to caregiver on standard cord care.

47
Summary of Literature Review
The umbilical cord is a unique tissue which connects the unborn baby to the mother through the
placenta for oxygen, nutrients, excretion of carbon dioxide and other metabolites. This cord
should be cut and dressed with sterile materials. Literature review revealed that the devitalized
tissue of the cord can be an excellent medium for bacterial growth, especially if the cord is kept
moist and unclean substances such as sand from door posts, herb prparations, cow dungs,
roots/or bark of trees are applied to it ( Bemor & Uta, 2011)
The theory on which the study was built upon was Orem’s self – care. T he theory is useful in
determining the kind of nursing assistance needed by the clients. It offers nurses the basis to
work with clients in developing their self- care agency and this study was directed primarily at
self care within the concept of dependent care agency. Nurses can use the supportive educative
under nursing system to provide knowledge of recommended standard cord management and
skill to the dependent care givers (mothers) for positive neonatal outcome (dry and healing cord).
Empirical review reported influence of beliefs, level of education, age and income of mothers on
newborn health in studies carried out in some developing countries such as Bangladesh, India
and Uganda. In Nigeria and particularly Cross River State, there are few reported studies as
evidenced from literature reviewed in these fields and majority are on incidence of neonatal
deaths which is related to umbilical infections in the newborn which accounts for about one
million neonatal deaths in Nigeria (Bello & Omotara, 2010). In general therefore, very few
studies have been done focusing on these variables and umbilical cord management among
mothers. This is considered a serious gap as studies on umbilical cord management will help in
identifying the specific problematic area that may require neonatal emergency attention and
resolution in keeping with today’s emphasis on primary prevention in health care delivery. This

48
will also provide a foundation on which behavior change communication programme can be
designed and implemented.
Most studies on umbilical cord care have been confined to the hospital. This present study,
which is community based is an attempt to bridge the gap.

49
CHAPTER THREE
RESEARCH METHODS
This chapter described the research design, setting for the study, population of study, sample,
sampling procedures, research instrument, validity and reliability of instrument, ethical
consideration, procedure for data collection and method of data analysis.
Research Design
A cross - sectional descriptive survey design was used in this study to determine the umbilical
cord care and management outcome among mothers in Calabar South Local Government Area of
cross River State. According to Isangedihi, Joshua, Asim & Ekuri (2004), the descriptive survey
allows one to describe conditions as they exist in their natural setting. It also allows orderly
collation of data. This method was considered suitable for the phenomena being studied.
Area of Study
The area of study was Calabar South Local Government Area of Cross River State, Nigeria.
Calabar South is one of the two Local Government Areas that make up Calabar Metropolis. It
was created from Calabar Municipality in 1996. The Local Government consists of 11 political
wards ( wards 1,2,3,4,5,6,7,8,9,10 and 11) which are grouped to ease traditional administration
into 22 clans namely, Eyamba, Duke, Etim Effiom, Ekpo Edem, Ntiero Edem Effiom Ekpo,
Archibong, Lower Cobha, Upper Cobhan, Ekpo Abasi, Ewa Ekeng, Effanga Offiong, Ekeng
Iwatt, Efut Abua East, Efut Abua West, Efut Ekondo, Efut Akwa, Efut Uwanse, Efut Obufa
Esuk, Efut Akani Esuk, Efut Anantigha, Effiom Ewa Nsa and Edet Nsa ( Antai & Effiong, 2009;
Ebong, 2006).

50
Calabar South Local Government has an area of 264km, and a land mass of 80,000 square
kilometers. In the north, Calabar South is bounded by Calabar Municipality, the Cross River in
the South, the Quo River in the east, and the Calabar River in the west. It is a semi-urban
settlement, with a mixture of many Nigerian ethnic groups, but it is predominantly made up of
the Efiks, Efuts, Quas, Ibibios and Yakkurs (Antai & Effiong, 2009).
The common language of the people of Calabar South is Efik. Most occupants of the area are
civil servants, businessmen, traders, farmers and fishermen. It is predominantly a Christian city
with a small percentage of Muslims and there are also traditionalists. Both the traditional and
orthodox health care services co-exist in Calabar South. Modern health care is organized in two
categories. There are 29 Government owned health facilities spread through all the 11 wards (1
general hospital, 2 comprehensive health centres, 6 primary Health centres and 20 health Posts) 8
private health facilities as well as 6 traditional birth homes. Most of these health institutions
provide both maternal and child health services. The setting for the study was the 22 clans in
Calabar South Local Government Area (Antia & Effiong, 2007)
Population of study
The National Programme on immunization (NPI) of the Federal Ministry of Health (2006)
quoting WHO (2000) states that population of women of child bearing age in every community
is 22% of the entire population. The entire population of calabar South Local Government Area
is 191,630. Thus, 22% of the entire population was estimated to be 42,159. Therefore, this
number represented the target population.
Sample
The study sample size determination used the probability (P) of .12% found in a cord
management survey among mothers in Nigeria (Ambe, et al, 2010). The minimum sample size of

51
451 was calculated using formula for estimating a single finite proportion. (Isangedihi et al,
2004),
n = Z 2
P (1 – P)
d2
Where n = Minimum sample size
Z = Confidence interval at 95% = 1.96
P = Proportion of people 0.12
d2
= Margin of error 0.03
(Appendix 2)
The inclusion criteria were:
• Willingness to participate in the study.
• Mothers aged between 15 and 49.
• Mothers whose babies were three months and below.
• Mothers residing within Calabar South Local Government Area at the time of the study
• Stable physically and mentally alert at the time of study.
Sampling Procedure
The 22 clans that made up Calabar South Local Government Area were used for the study. The
population of these 22 Clans could not be traced individually in the records of the National
population Commission (2007), thus a purposive allocation of equal percentage to each of the
clans was done in selecting the number of respondents for each clan. This was done to build in
representativeness in the study. These, in proportion to the total sample size for the study gave a
sample of 20.5 to each clan (Table 1). To reach each of the respondents, a snow ball
(networking) method was used putting into consideration the inclusion criteria such that when

52
the first respondent is correctly identified she helped to identify other respondents. The first
contacts were made at Health Centers and also in churches when it was observed by the
researcher that some of the mothers delivered their babies in churches. The names, addresses and
telephone numbers of the mothers who consented to participate in the study were obtained to
enable the researcher link up with other respondents in their homes.
Table 1: Number of Sample for Each Clan n = 451
Clan Number Percent
Eyamba
Duke
Etim Effiom
Ekpo Edem
Ntiero Edem Effiom Ekpo
Archibong
Lower Cobham
Upper Cobham
Ekpo Abasi
Ewa Ekeng
Effanga offiong
Ekeng iwatt
Efut abua East
Efut abua West
Efut Ekondo
Efut Akwa
Efut Uwanse
Efut Obufa Esuk
Efut akani Esuk
Efut Anantigha
Effion Ewa Nsa
Edet Nsa
Total
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
20.5
451
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
100

53
Instrument for Data Collection
Data were collected by means of questionnaire developed by the researcher which was used as
interview guide. The questionnaire was developed strictly based on extensive literature search on
umbilical cord management and stated objectives. The questionnaire was divided into six
sections. Section A was strictly on demographic information and was made up of ten questions.
Section B was made up of six questions on knowledge of standard cord care and source of
information, while section C consisted of six questions on substances used for umbilical cord
management. Section D consisted of one question with various options on reason for choice of
materials for cord management. While section E elicited information on techniques for umbilical
cord management with six questions, Section F consisted of five questions on outcome of care
with various options. The questionnaire was made up of both close and open-ended questions.
The close ended questions enabled the respondents to choose from available options while the
open-ended questions allowed them to express their own ideas in their own words. The
respondents were expected to choose and tick the options that best describes their disposition on
the issue. A total of 38 items were generated.
Validity of instrument
The face and content validity of the instrument (questionnaire) were determined through the
judgment of the project supervisor, two lecturers in the Department of Nursing who are experts
in child health and clinical experts (a consultant pediatrician and two pediatric nurses in the area
of neonatology). They were given the draft copy of the questionnaire, purpose of the study and
the research questions to critically determine the relevance of content, clarity of statements and
logical accuracy of the instrument. Their suggestions were effected; thus increasing the items
from 27 to 38. (Appendix 1)

54
Reliability
A test re-test approach was used to conduct a pilot study on 50 mothers selected from Quo
Calabar Municipality not included in the study, but have similar characteristics with the study
group. The data obtained from the copies of the questionnaire were collated; analyzed using
Pearson Product Correlation Coefficient and the result showed that the instrument
(questionnaire) had a reliability estimate of .99. This showed that the instrument was reliable and
was appropriate for the study (see Appendix 3).
Ethical Consideration
Ethical approval to carry out the study was obtained from Cross River State Ministry of Health
Research Ethics Committee (See Appendix 5). The purpose of the study was explained to the
respondents and a signed consent was obtained from each of them. Those who could not write
thumb printed (see Appendices 7 & 8). The respondents wishes and rights were respected at all
times, including right to discontinue with the study at any time.
Procedure for Data Collection
With the letter from the Department of Nursing Sciences and ethical approval from the Ministry
of Health, permission to carry out the study was obtained from His Royal Highness (Muri
Munene) and the ward chiefs of the 22 clans (See Appendices 4 & 6). The questionnaires were
used as interview guide to obtain information from the mothers who met the inclusion criteria.
This was done with aid of five research assistants who were trained on the purpose of the study
and selection of respondents. The snow ball method was used to reach respondents in each of the
clans. The first contacts were made at Health Centres and churches; copies of questionnaire were
administered to those who met the inclusion criteria. From here these first contacts helped in
identifying the other respondents, until the sample size was completed. Literate respondents were

55
given the questionnaire which they filled and the copies were collected thereafter. Respondents
who could neither read nor write were helped to complete the questionnaire. The distribution and
retrieval of the questionnaire from the respondents in the 22 clans lasted five months.
Method of data analysis
Item by item descriptive Analysis of the data was carried out to show response frequency and
percentages using the computer software programme statistical package for the social sciences
(SPSS version 18). A cross tabulation was done to determine the association between
demographic characteristics (age, educational attainment and income) of mothers and cord
management using Spearman’s Correlation test of association with 95% confidence interval.
Decision Rule
A P – value of less than 0.05 indicated that there was a significant association between the
demographic characteristics of mothers and umbilical cord management.

56
CHAPTER FOUR
DATA PRESENTATION
This chapter presents the results and summary of the findings. The results have been presented
in Tabular form according to research questions. Out of 451 questionnaire distributed, 450 was
correctly filled and returned giving a response rate of 99.7%
Table 2: Demographic Characteristics of Respondents n = 450
Variables Category Frequency Percent
Age Category 15-25 196 43.6
26-36 x = 26, SD =12 238 52.9
37-47
Total
16
450
3.6
100.0
Marital status Married 390 86.7
Single
Divorced
Separated
Widowed
60
0
0
0
13.3
0
0
0
Total
450 100.0
Religion Christianity 444 98.7
Moslem
Traditionalist
6
0
1.3
0
Total
450 100.0
Educational attainment None formal education 14 3.1
Primary 70 15.6
Secondary 188 41.8
Tertiary 178 39.6
Total
450 100.0
Occupation Petty Trading
Civil servant
Student
Applicant
Housewife
Farming
Hair dressing
Total
Income per month N18,000
N19,000-30,000
N31,000 and above
Total
156
92
80
76
30
12
4
450
316
87
4
450
34.7
20.4
17.8
16.9
6.7
2.7
0.9
100
70.2
19.3
10.4
100

57
Table 2 shows that out of the 450 respondents. 52.9% were young adults with mean age of 26
and standard deviation of 12. It also revealed that 81.4% had secondary education and above
while only 3.1% had non formal education. With regards to income, 70.2% were within the low
income group.

58
Research Questionnaire I
What level of knowledge do mothers have regarding standard cord management and from which
source of information?
Table 3: Knowledge of Standard Cord Care among Respondents n = 450
Questions Options Frequency Percent
What do you understand
by standard cord care?
Total
Tying, cutting and cleaning with
methylated spirit only.
Use of herbs and isolation of baby
Use of herbs
Nothing on the cord till separation
201
141
76
32
450
44.7
31.3
16
7.1
100.0
Table 3 indicates that out of the 450 respondents, 201(44.7 %) had good knowledge of standard
umbilical cord management. They had the knowledge of tying the cord stump, cutting it with a
clean object and cleaning with methylated spirit only with no application of any other material.
While others accounted for poor knowledge – 141 (31.3%) used herbs and isolated the baby, 76
(16.9%) used herbs only and 32 (7.1%) applied nothing on the cord till it detached.

59
Source of knowledge of Umbilical Cord Management among Respondents
Table 4: Source of knowledge of Umbilical Cord Management
Questions Options Frequency Percent
What was your source
of knowledge
Mother/mother-in-law
Church members
Health worker
Traditional Birth Attendants
187
162
149
52
34
29.4
27.1
9.5
On the source of knowledge, Table 4 revealed that out of the 450 respondents, 187 (34%) got
their information from their mother/mother-in-law,164 (29.4%) from church members and 52
(9.5%) from traditional birth attendants. These were regarded as poor sources of information.
Those whose sources were from the health workers which were regarded as good sources were
149 (27.1%)
`

60
Knowledge of Material Used for Tying the Umbilical Cord among Respondents
Table 5: Knowledge of Material Used for Tying the Cord n =450
Questions Options Frequency Percent
What material should
be used in tying the
cord
Total
Cord clamp
Hair thread
Rubber band
Hair thread String of cloth
255
176
17
2
450
56.7
39.1
3.8
.4
100.0
Table 5 indicates that out of the 450 respondents, 255 (56.7%) had good knowledge of cord
clamp as material used for tying the umbilical cord while others accounted poor knowledge –
hair thread 176 (39.1%), rubber band 17 (3.8%) and string of cloth 2 (.4%)

61
Knowledge of Solution Used in Cleaning Umbilical Cord among Respondents
Table 6: Knowledge of Solution for Cord Cleaning n=450
Questions Options Frequency Percent
What cleaning
solution should be
used for cord care.
Total
Methylated spirit
Herbal solution
Salt and saliva
Hot water
254
88
66
42
450
56.4
19.6
14.7
9.3
100.0
[
Table 6 shows that out of a total of 450 respondents 254 (56.4%) had good knowledge of
Methylated spirit as cleansing solution. While others accounted for poor knowledge – herbal
solution 88 (19.6%), salt mixed with saliva 66 (14.7%) and hot water (9.3%).

62
Knowledge of Cord Separation Time among Respondents
Table 7: Knowledge of Cord Separation Time n =450
Questions Options Frequency Percent
How long does it take
cord to detach
Total
3-4 days
5-15 days
4 weeks and above
372
78
0
450
82.7
17.3
0
100
Table 7 shows that out of 450 respondents, 372 (82.7%) had poor knowledge of the stipulated
range of time for cord separation which is between 5 – 15days. While 78 (17.3%) of the
respondents had good knowledge.

63
Table 8: Knowledge of Advantage of Umbilical Cord Care n = 450
Questions Options Frequency Percent
What is the advantage
of cord care
Total
Wades off evil spirit
Prevent infection
Prevent neonatal tetanus (Odon)
Prevent abdominal Pain
220
113
87
30
450
48.9
25.1
19.3
6.7
100
With regards to knowledge of the advantage of cord care, Table 8 shows that out of the 450
respondents those with poor knowledge which include to wade off evil spirit were 220 (48.9%),
to prevent neonatal tetanus were 87 (19.3) and to prevent abdominal pain were 30 (6.7%) While
only 113 (25.1%) accounted for good knowledge of advantage of cord management, which is to
prevent infection.

64
Research Question 2
What materials do mothers use in the management of umbilical cord in Calabar South Local
Government Area?
Table 9: Materials Used for umbilical Cord management n = 450 Questions Options Frequency Percent
Which of the following was
used in tying the umbilical
cord
Cord clamp
Hair thread
twine
String of cloth
Bandage
279
13
12
8
8
62.0
31.8
2.7
1.8
1.8
Total 450 100.0 What was used to separate
baby from mother
Knife
Razor blade
Sterile Scissors/Surgical blade
Farm instrument
No idea
187
165
94
4
4
41.6
36.7
20.9
0.8
0.8
Total 450 100.0 Which of the following did
you use in cleaning the
umbilical cord stump?
Alcohol (methylated spirit)
Dettol solution
Saliva and salt
Herbal preparation
Hot water
Saliva only
Salt solution
224
88
44
44
42
4
4
49.8
19.6
9.8
9.8
9.3
0.9
0.9
Total 450 100.0
After cleaning did you
apply anything else to the
stump?
Yes
No
Total
314
136
450
69.8
30.2
100.0
If yes, which of the
following
Where did you delivery
your last child
nothing else was applied
“Ndodop’’
Saliva mixed with salt and sand
Herbal preparation
Breast milk
Palm Kernel oil
Tooth paste ‘ Close up’
nothing else was applied
Rub/menthol
Gentian violet
Dusting powder
Native chalk
Penicillin ointment
Tincture of Iodine
Cow dung
Lantern wax
Total
Church
Prayer house
Hospital
Health centre
At home
Traditional birth attendant home
Total
136
105
79
40
36
21
16
6
3
6
2
0
0
0
0
0
0
450
180
138
80
30
14
0.8
450
30.2
23.3
17.6
8.9
8.0
4.5
3.6
1.3
0.6
1.3
0.4
0
0
0
0
0
0
100.0
40.0
30.7
17.8
6.7
3.1
2.0
100

65
Table 9 reveals that out of the 450 respondents, 279 (62 %) used cord clamp to tie the umbilical
cord, 187 (41.6%) used sterile scissors/surgical blades to sever the cord and 224 (49.8%) of the
respondents used Methylated spirit to clean the cord. However, a large percentage of 69.8%
added other substances other than methylated spirit to the umbilical cord. With regards to various
materials added, “Ndodop’’ was commonly used by the respondents accounting for 33.3%.
Tooth paste “Close Up” was used by 16 (3.6%) of the respondents.

66
Research Question 3
What are the reasons for the choice of materials for umbilical cord management?
Table 10: Reason for Choice of Material for Umbilical Cord Management
Question Option Frequent Percent
What are the reasons
for the choice of
materials for
umbilical care?
To wade off evil spirit and hasten cord separation
prevent “Ibio okop”
Prevents neonatal tetanus “Odon”
Prevents infection
Pressure from family members
Prevents failure to thrive “Akpa”
Stop “ after birth pains’’
Very effective and hasten cord separation
270
185
80
61
56
6
6
4
55.9
38.3
16.6
12.6
11.6
1.2
1.2
0.8
Table 10 shows that to wade off evil spirit and hasten cord separation were the main reasons
given by 270 (55.9%) of the respondents.185 (38.3%) specified that the materials prevent “Ibio
okop” About 80 (16.6% )of the respondents used the materials to prevent neonatal tetatenus
“odon”, 61 (12.6%) used to prevent infection while 56 (11.6%) used the various substances due
to pressure from family members.

67
Research Questions 4
What are the techniques used by mothers in umbilical cord management?
Table 11: Techniques for Cord Management n = 450
Questions Option Frequency Percent
Which of the cleaning
technique was
practiced?
Did you practice dry
or wet method?
How did you take care
of your hands during
cord care?
Clean cord base before surrounding skin Clean cord base and surrounding skin at same
time Clean cord stump only Clean surrounding skin only Clean only material used in tying stump Total
Dry method Wet method Total
Washed hands with water before attending to the
cord Washed hands with soap and water before and
after attending to cord Washed hands with soap and water after attending
to cord Cleaned hands on wrapper after cord care Cleaned hands with clean serviette/handkerchief
after cord care Total
180 108 92 52 18
450
0 450 450
186 116 108 40 0 450
40 24
20.4 11.6 4
100.0
0 100 1000.0
41.3 25.8 24.0 8.9 0
100.0
Which of the
following methods did
you practice
Open method Closed method Total
413 37
450
91.8 8.2 100.0
How often was the
cord stump cleaned Morning, afternoon and evening (3 times) Once a day After each nappy changed Delivery time only No cleaning Total
219 86 73 62 2
450
49.5 19.5 16.1 14.0 0.5 100.0
If closed which of the
following was used to
cover the stump?
Bandage Piece of mother’s cloth Gauze bandage Abdominal binder Total
28 7 2 0
37
75 19.0 5.4 0 100.0

68
Table 11 revealed that out of the 450 respondents only 40% cleaned cord base and surrounding
skin at the same time, all the respondents practiced wet care, 41.3% observed clean hand care
only after umbilical cord care while 91.8% practiced open method and gauze bandage wasused
by 75% of the respondent who used the closed method.

69
Table: 12 Management outcome of Umbilical Cord care n =450 Questions Options
Frequency Percent
Did you observe any
abnormal changes
while treating the cord
stump?
Yes No Total
338 112 450
75.1 24.9 100.0
How was the problem
resolved? Child taken to patent medicine dealer Child taken to health facility Child taken to TBA/traditional healer Child taken to church Cared for at home
16 122 62 5 133
5 36 18.3 1.4 39.3
Total 338 100.0
What was the duration
of problem before
reporting to health
facility?
Within 24hours 2 – 3 days 4 – 6 days 7 days and above
5 37 65 15
4.1 30.3 63.3 12.2
Total 122 100.0
What other thing did
you observe on the
baby?
Persistent fever Twitching of whole body, unable to open mouth/suck Difficulty in breathing Nothing else Total
146 40 20 132 338
43.2 11.8 6.0 39.0 100.0
Have any of your
children died within
first 6 weeks of life?
Yes No Total
115 335 450
25.6 74.4 100.0
If yes, what was the
causes Did not cry immediately after birth Cried excessively, unable to open mouth/suck. Purulent discharge from cord stump Congenital malformation
29 52 32 2 115
25.2 45.2 27.8 1.7 100
Table 12 revealed that out of 450 respondents 75.1% observed abnormal changes which were
regarded as signs of infection in their babies while 24.9% did not. On how the problems were
resolved 64% gave home based care while only 36% reported to health facilities. With reference
to the duration before medical attention, only 4% reported within 24hours of onset of the
problem. With regards to home neonatal deaths, 115 (25%) out of the 450 respondent claimed to
have lost babies at some point during their neonatal period (first 6 weeks of live). On the causes
of death, 84 (73%) was related to umbilical infections.

70
Table 13: Correlation Test of Association between Age and Cord Management among
respondents. n =450
AGE
CORD
CLEANING
SOLUTION
OTHER
MATERIALS
APPLIED
HAND
CARE
PRACTICE
CLEANING
TECHNIQUE
FREQUENCY
OF STUMP
CLEANING
Spearma
n's rho
Correlation
Coefficient 1.000 .047 .150(*) .298(*) .080(*) .351(*)
Sig. (1-tailed) . .160 .001 .000 .046 .000
N 450 450 450 450 450 450
Correlation
Coefficient .047 1.000 .291(*) .142(*) -.101(*) .212(*)
Sig. (1-tailed) .160 . .000 .001 .016 .000
N 450 450 450 450 450 450
Correlation
Coefficient .150(*) .291(*) 1.000 -.282(*) -.398(*) -.026
Sig. (1-tailed) .001 .000 . .000 .000 .290
N 450 450 450 450 450 450
Correlation
Coefficient .298(*) .142(*) -.282(*) 1.000 .261(*) .179(*)
Sig. (1-tailed) .000 .001 .000 . .000 .000
N 450 450 450 450 450 450
Correlation
Coefficient .080(*) -.101(*) -.398(*) .261(*) 1.000 -.102(*)
Sig. (1-tailed) .046 .016 .000 .000 . .015
N 450 450 450 450 450 450
Correlation
Coefficient .351(*) .212(*) -.026 .179(*) -.102(*) 1.000
Sig. (1-tailed) .000 .000 .290 .000 .015 .
N 450 450 450 450 450 450
* Correlation is significant at the 0.05 level (1-tailed).
Table 12 shows significant association at p<0.05 between age of mothers and four cord care
management variables. The most significant associations were frequency of stump cleaning and
hand care practices with correlation coefficients of .351 and .298 respectively. Application of
other materials to cord after cleaning and cord cleaning techniques were also significantly
associated with the age of the mothers at .001 and .046 level of significance. Solution used for
cord cleaning was however not associated with the age of the respondents.

71
Table 14: Correlation Test of Association between Educational Level and Cord
Management among Respondents. n = 450
EDUCATIONAL
LEVEL
CORD
CLEANING
SOLUTION
CORD
CLEANING
EXCESSES
HAND
CARE
CLEANING
TECHNIQUE
FREQUENCY
OF STUMP
CLEANING
Spearman
's rho
Correlation
Coefficient
.064 1.000 .291(*) .142(*) -.101(*) .212(*)
Sig. (1-tailed) .087 . .000 .001 .016 .000
N 450 621 450 450 450 450
Correlation
Coefficient
.440(*) .291(*) 1.000 -.398(*) -.026
Sig. (1-tailed) .000 .000 . -.282(*) .000 .290
N 450 450 450 450 450 450
Correlation
Coefficient
.300(*) .142(*) -.282(*) 1.000 .261(*) .179(*)
Sig. (1-tailed) .000 .001 .000 . .000 .000
N 450 450 450 450 450 450
Correlation
Coefficient
.351(*) -.101(*) -.398(*) .261(*) 1.000 -.102(*)
Sig. (1-tailed) .000 .016 .000 .000 . .015
N 450 450 450 450 450 450
Correlation
Coefficient
.103(*) .212(*) -.026 .179(*) -.102(*) 1.000
Sig. (1-tailed) .014 .000 .290 .000 .015 .
N 450 450 450 450 450 450
Correlation
Coefficient
1.000 .064 .440(*) .300(*) .341(*) .103(*)
Sig. (1-tailed) . .087 .000 .000 .000 .014
N 450 450 450 450 450 450
* Correlation is significant at the 0.05 level (1-tailed).
Findings from Table 13 revealed that all the examined cord care practice variables had
significant association with the educational level of the respondents except the Solution used
(p=.087) at p<0.05. The application of other materials (rho=.440) had a strong association with
the educational level of the respondents, while hand care practices (rho=-.300), cleaning
technique (rho=.341) and frequency of stump cleaning (rho=.103) were also associated

72
Table 1: Correlation Test of Association between Income and Cord Management among
Respondents n = 450
INCOME
PER
MONTH
CORD
CLEANING
MATERIAL
CORD
CLEANING
EXCESSES
HAND
CARE
PRACTICE
CLEANING
TECHNIQUE
FREQUENCY
OF STUMP
CLEANING
Spearman
's rho
Correlation
Coefficient
.192(*) 1.000 .291(*) .142(*) -.101(*) .212(*)
Sig. (1-tailed) .000 . .000 .001 .016 .000
N 450 621 450 450 450 450
Correlation
Coefficient
.661(*) .291(*) 1.000 -.282(*) -.398(*) -.026
Sig. (1-tailed) .000 .000 . .000 .000 .290
N 450 450 450 450 450 450
Correlation
Coefficient
.229(*) .142(*) -.282(*) 1.000 .261(*) .179(*)
Sig. (1-tailed) .000 .001 .000 . .000 .000
N 450 450 450 450 450 450
Correlation
Coefficient
.276(*) -.101(*) .398(*) .261(*) 1.000 .102(*)
Sig. (1-tailed) .000 .016 .000 .000 . .015
N 450 450 450 450 450 450
Correlation
Coefficient
.313(*) .212(*) -.026 .179(*) .102(*) 1.000
Sig. (1-tailed) .003 .000 .290 .000 .015 .
N 450 450 450 450 450 450
Correlation
Coefficient
1.000 .192(*) .661(*) .229(*) .276(*) -.131(*)
Sig. (1-tailed) . .000 .000 .000 .000 .003 N 450 450 450 450 450 450
* Correlation is significant at the 0.05 level (1-tailed).
Table 19 shows that all the examined cord care practices of the respondents were significantly
associated with their income level. Application of other materials after cord cleaning (rho=.661),
cord cleaning solution used (rho=.192), hand care practice (rho=-.229), cleaning technique
(rho=-.276) and frequency of stump cleaning (rho=-.131) were association with the income of
respondents

73
Summary of Major Findings
• Knowledge of standard cord management was poor among the respondents and the major
sources of information were from mothers and mother -in-laws
• Majority (69.8%) of the respondents applied harmful and contaminated material/
substances to the umbilical cord.
• The Major reason for choice of material was mainly to wade away evil spirit which the
respondents believe causes neonatal deaths.
• Technique for cord management was poor as majority of the respondents did not clean
the base of the cord before the surrounding skin nor cleaned after each nappy is changed
nor washed hand before and after cord care.
• The outcome of cord management was poor as majority of the respondents reported signs
of umbilical infection in their neonates.
• Very low percentage (4.1%) of the respondents whose babies were infected following
unhygienic cord care reported the umbilical infection to the health facilities within 24
hours of onset; while the majority managed the cord infection at home based on culturally
recommended therapies such as herbal preparations.
• Umbilical cord management was associated with age, the older the respondents, the more
likelihood of practicing clean cord care.
• Umbilical cord management was associated with educational attainment: the more
educated the respondents, the more clean cord care practice.
• Umbilical care management was associated with income of respondents; the higher the
income of respondents, the more clean cord care practice.

74
CHAPTER FIVE
Discussion of Findings
This chapter presents discussion of major findings, limitations, implication for nursing,
suggestions for further studies, summary, conclusion and recommendations.
Research Question 1
Do mothers in Calabar South Local Government have knowledge of standard cord
management and from which source of information?
Findings of this study indicated that the respondents had poor knowledge of standard cord care.
The knowledge of cord separation time was also poor. The explanation for this poor knowledge
could be from the poor sources of information as majority of the respondents had information
from their mothers, mother -in – laws, church members and Traditional birth Attendants. This
agrees with the report of Senarath (2010) that knowledge of standard care was poor among
mothers. It is also in accordance with Green, et. al, (2006), who reported very poor knowledge
among mothers. It however, disagrees with the findings of Luka (2009) in which majority of the
mothers knew hygienic cord care.
As documented by George (2011) mothers (dependent care givers) require help when they are
unable to maintain continuously for the child the amount and quality of care that is therapeutic;
in this instance, umbilical cord management. The health outcome of neonates could be improved
significantly by strengthening information, education and communication of standard cord
management to mothers. These could be done by grouping the mothers in each of the clans for
intensive and focused health education on standard cord management.

75
Research Question 2
What materials do mothers use in the management of umbilical cord?
Findings from the study showed that there was common use of cord clamp and surgical
blades/scissors in cord management which indicated good practice. Methylated spirit was also
widely used in cord care by mothers. These findings may not be unconnected with the fact that
the majority of the mothers delivered their babies in hospitals, where clean cord care is practiced.
This percentage of hospital delivery as reported from this study may have been influenced by the
free maternal and child health services declared by the Cross River State Government in 2009.
The result however, indicated that the majority of the respondents also applied other substances
to the umbilical cord after being discharged from the hospital. These practices are more often
very harmful as they are contaminated with bacteria and spores thus increasing the risk of
umbilical infection particularly neonatal tetanus which accounts for more than 52% of neonatal
deaths in developing countries (Jeol-Madewase et, al 2008).
These findings are in agreement with Sneeramaraddy et, al. (2006) who documented that babies
delivered in hospitals may be affected by traditional practices after discharge as care of the cord
during neonatal period is provided by mother and mother in-law. The findings from this study is
also in line with the report of Bang and Andem (2011) and Ambe et, al (2010) which revealed
the use of native and various forms of herbal preparation in cord care in a semi urban setting as
the one studied.
It is worthy of note that some percentage of the respondents specified ‘close up” tooth paste as
one of the substances used in cord management. Although the percentage is low, there is no
literature related to this, thus making it very significant in neonatal health. It is pertinent

76
therefore, to assess the active ingredients in close up tooth paste in relation to neonatal umbilical
care and neonatal health in general to prevent an adverse effect and poor neonatal outcome.
Research Question 3
What are the reasons for the choice of materials for umbilical cord management?
Finding revealed that to wade off evil spirit and hasten cord separation were the reasons given by
the majority of the respondents for choice of materials for cord management. This could be as a
result of their cultural beliefs. Traditional beliefs about child birth, misconception and fear of
neonatal death could have led to the mothers’ decision to use various materials in cord
management to hasten cord separation. This is in consonant with Waise and Kaikoba (2008)
who reported that the use of various materials are believed to help the cord dry and separate
faster within 3 days and save the neonate from evil spirit which they believe causes neonatal
death. This is similar to the report of Okedo, Nelson and Lawal (2010) in which the influence of
cultural beliefs and traditional practices were implicated in cord management and separation
time. Whatever the reasons may be unhygienic cord care is a risk behavior which can lead to
neonatal infection and death as the umbilical vessels are still patent for a few days after birth,
thus making umbilical cord a common route of entry for systemic infection in the newborn
Research Question 4
What are the techniques used by mothers in umbilical cord management?
The low percentage recorded by the respondents on clean hand during cord management showed
evidence of unhygienic cord management. This finding is contrary to WHO (2007)
recommendation on hand care which is washing before and after cord care to prevent cord
infection particularly neonatal tetanus and omphalitis.

77
The study also revealed that the technique for cord management was poor. Majority of the
mothers cleaned the cord base and surrounding skin at the same time which encourages transfer
of pathogenic organisms and spread of infection. These findings may not be unconnected with
their sources of knowledge of cord care where a good percentage of the respondents had
knowledge of cord management from their mothers, mother-in-laws, church member and
Traditional Birth Attendants (TBA). On frequency of cleaning, majority of the mothers cleaned
the cord stump only once a day. This is a risk factor because at this time the base of the cord is
wet and can provide a nutritive culture medium for bacterial growth if it is cleaned only once a
day (Garner, 2006). WHO (2007) recommends on the average, cleaning as often as each diaper
is changed. This should constitute the health measures adopted by mothers to promote healing,
prevent infection, neonatal morbidity and mortality.
Research Question 5
What were the outcomes of umbilical care in relation to material used for cord
management?
Finding from the study showed that cord infections (fever, red skin around base of cord,
yellowish discharge from cord, foul smell from cord, pain when skin around the cord is touched)
were reported by the majority of the respondents. The findings were consistent with the findings
of Bello and Omotara (2006) who reported that a high proportion of cord infection was recorded
among neonates who had topical application of native and herbal preparation on umbilical cord.
It is also similar to the findings of Meberg and Brown (2007) that majority of omphalitis was
observed in babies with unhygienic cord care. Alam and Murray (2008) also reported of
umbilical infection among neonates whose umbilical cords were dressed with unhygienic
materials.

78
Majority of the umbilical cord fell off within 3-4 days contrary to WHO (2006) report of
between 5 and 15 days. The study also revealed that only few of the navels healed within the
recommended interval of one month and six weeks. It could be that the infection interferes with
the healing process, providing direct access to systemic infection (Benor & Uta, 2011).
There was also late report for medical attention. A very low percentage reported umbilical
infection to the health facilities within 24 hours of onset of illness. Majority of the respondents
managed the cord infection at home based on culturally recommended therapies. This may not
be unconnected with their traditional beliefs and misconception about child birth and causes of
neonatal death. The findings were consistent with the findings of Muella and Johnson (2009)
that only very few mothers 2% reported umbilical cord infection to the clinic within 24 hours and
more than 68% managed the cord infection at home. These possibly explained the high neonatal
morbidity and mortality rates in the study area. Thus the proportion of neonates with severe
umbilical infections and deaths could be reduced if appropriate education is given to mothers on
cord management and separation time to prevent anxiety.
Research Question 6
What is the association between demographic characteristics of mothers and cord
management?
The demographic profiles of the respondents revealed that majority of the respondents were
young adults with mean age of 25.8 years. This means that they were at the pick of their
reproductive health and require information on neonatal health and child survival. Majority of
the respondents had secondary education and above. The implication is that most of them are
literate. Consequently, they can easily imbibe recommended health practices, influence those
with less education as well as those holding unto unhealthy traditional practices and invariably

79
putting an end to unhygienic cord management. This agrees with Eneji, Eyamba and Markinde
(2010) who noted a significant correlation between mothers’ level of education and clean cord
management. They concluded that it is nearly impossible to consider behavioral changes in
health care practice without simultaneously considering the level of education of the subjects,
which deeply influences personal conduct especially in the area of child bearing and neonatal
care.
The result also revealed that there was a significant association between age of the respondents
and cord management. The older the maternal age the better the cord care practices. The result
agrees with Obimbo et al (2008) in which unsafe methods and unhygienic cord cares were seen
to be more among younger mothers. They reported that older maternal age was associated with
decreased use of unsafe methods because older mothers are aware of the importance of clean
cord care and the risk of cord infections. The result was also in line with the study of Benson et
al (2006) and review of Smith and Kelly (2011) which revealed that about 48% of reported
unclean cord care and cord infections among new born were babies of mothers who were below
age 30 years; age at first pregnancy was significantly related to who cares for the cord and
substance used thus placing the babies in vulnerable situation. The younger mothers are
inexperience in neonatal care, unaware of risk of cord infection, majority of them in their teen,
school dropout, single and in low socio- economic status. Thus cord care decisions are deferred
to older relatives who employ care which depends on beliefs, customs and social status which
promote neonatal infection and death ( Dibson John, 2010 ).
Furthermore, finding revealed that there was significant association between educational
attainment of mothers and cord management. The higher the mothers’ educational attainment,
the better the use of standard cord management. This was in line with the assertions of Eneji,

80
Eyamba and Makinde (2010) that a significant correlation has been noted between mothers’ level
of education and clean cord management and better neonatal outcome. Uneducated mothers
lacked decision making power and unable to resist social pressure from family and peers; as such
they comply with existing tradition. Peter, et. al, (2010); Okedo, et. al,(2010); Sharan, (2010).
also reported unclean cord management among mothers with low educational level.
With regards to the association between cord management and income of respondents, the result
showed that there was significant association between income of the respondent and cord
management. This finding is in consonant with Adamu, Harrison and Wale (2009) in which
income had direct association with cord management.
Implication to Nursing
Since respondents in Calabar South Local Government Area used herbal preparation and
contaminated material in cord management, the implication of this is that neonates are at risk of
developing umbilical infections such as neonatal tetanus, omphalitis and necrotizing fasciitis
from the use of these substances. More so, neonates are at risk of developing adverse reactions
from these preparations which are administered in unregulated dosage as antidotes are unknown.
Furthermore, majority of the respondents did not report umbilical infection nor seek medical
attention, the few respondents who reported the cord infection to health facilities did that very
late. The implication of this is that delay in presentation at health facilities could lead to poor
neonatal outcome, thus increasing the neonatal morbidity and mortality rates which are already
unacceptably high.
All these have implications for nurses. The nurse should re-direct and re-package the contents of
their health education, directing it more towards discouraging poor traditional practices in cord
management. Nurses should increase mothers’ knowledge on cord separation time with the use

81
of methylated spirit. If the mothers are made aware of the recommended range of cord
separation time with standard cord management they may be spared the unnecessary concern
which most times prompt mothers to seek ways to enhance cord separation to prevent
supernatural power which they believed causes neonatal deaths. This could be achieved through
well planned effective and consistent health education of mothers. Nurses could also repeat
health talk after antenatal session for the benefit of those who arrived late and after delivery for
those who were not regular during antenatal period.
This study has shown why there is increased burden of umbilical infections and high neonatal
deaths. The problem lies on the choice of materials applied to the umbilical cord for various
reasons. Therefore, nurses could help to save the situation through direct and focused health
education, home visit where mothers and other care givers/significant others could be accessed;
and home delivery to reduce neonatal mortality as a good number of mothers still engage the
services of churches and traditional birth attendants in the study area.
Limitations of the Study
The major constraint in this study was the sensitive nature of the study which posed constraint in
accessing respondents because of traditional practices and beliefs. Nursing mothers are not
allowed to interact with other women whose “odon” status is unknown till after the umbilical
cord has detached.
Several visits were made to the same respondents to either administer the questionnaire or
retrieve it.
Suggestions for further Studies
Similar study should be carried out in other semi urban communities in the state and in other
geopolitical zones in Nigeria so as to achieve generalized application.

82
Study should be conducted to analyze the active properties in “close-up” tooth paste in relation
to umbilical cord care and separation time as well as effect on the neonate to prevent poor
neonatal outcome.
Summary
This study assessed the umbilical cord care and management outcome among mothers in Calabar
South Local Government Area of Cross River State.
This study was designed to determine the:
• knowledge of standard cord management and sources of information among mothers.
• various materials used by mothers for umbilical cord management.
• identify the reasons for the choice of materials used in umbilical cord management.
• techniques used by mothers in umbilical cord management
• outcome of umbilical cord management in relation to material used
• association between demographic characteristics of mothers and their practices (age,
educational attainment and income).
The conceptual and empirical reviews were based on the objectives of the study. The research
design was descriptive survey and a snowball sampling technique was used to reach four
hundred and fifty (450) respondents from 22 clans that made up Calabar South Local
government Area. Validated questionnaire constructed by the researcher were used for the
collection of data; data derived from the study were subjected to descriptive statistics and
Spearman’s Correlation test of association. Findings of the study showed that the respondents
had poor knowledge of standard cord management and their major sources of information were
from their mothers/mother-in-laws. This may not be unconnected with the poor knowledge of

83
cord separation time shown by the respondents. Majority of respondents applied various harmful
and contaminated materials/ substances to the umbilical cord and the reasons for choice of
materials for cord care were based on traditional and cultural beliefs, which was to wade off evil
spirit. More so, the technique for cord care was poor thus, resulting in umbilical infection.
Majority of respondents did not seek for medical assistance and the few that opted for did that
fairly late. Finding further revealed that umbilical cord management was associated with age,
educational attainment and income of respondents.
Conclusion
Based on the findings of this study the following conclusions were made;
• The respondents had poor knowledge of standard cord care and the major sources of
information were the mother/mother in - laws.
• Majority of the respondents applied harmful and contaminated materials/ substances to
the umbilical cord.
• The major reason for choice of materials was mainly to wade away evil spirit which the
respondents belief causes neonatal deaths
• Majority of respondents did not use recommended technique for cord management
• Outcome of cord management was poor as majority of the respondents reported signs of
infections in their neonates indicating the use of unclean and contaminated materials for
cord care.
• A very low percentage of the respondents reported the problem to health facility within
24 hours of onset of illness.
• Umbilical cord management was associated with age, the older the respondents the more
likelihood of practicing clean cord care.

84
• Umbilical cord management was also associated with educational attainment; the more
educated the respondents, the more clean cord care practice.
• Umbilical cord management was also associated with income of respondents; the higher
the income the more clean cord care practice.
[
Recommendations:
1. Nurses should embark on direct and focused health education, home visits and home
delivery to improve on umbilical care management to prevent hazardous consequences.
Nurses should specifically disabuse mothers’ mind on superstitious beliefs and old
midwife tales. Nurses should emphasize the use of recommended antiseptic solution,
technique of cleaning and non-application of any other substance to the umbilical cord
after cleaning and mother should have knowledge of acceptable range of cord separation
time.
2. Traditional Birth Attendants (TBAs) should be trained and re-trained including those in
various churches since a good number of deliveries were taken by them in the area of
study.
3. Enlightenment on girl child education should be intensified by all tiers of government to
improve future mothers.
4. The government and related health agencies should do more in the provision of health
facilities, logistics, equipments and skilled manpower to facilitate access to mothers.

85
REFERENCES
Abba, K. T. (2008). Management of Puberty and Child Birth. Philadelphia: Saunders.
P 25-38.
Adamu, T. K., Harrison W. & Wale, T. (2009). Contextual Factors Influencing Newborn Care
among Rural Communities in North West Nigeria.
Journal of Tropical Pediatrics 4 (4): 273-275.
Adeleye, G., Sadiq, P. Tam, N. (2011). Factors Associated with Neonatal Tetanus Mortality in
North East Nigeria. Global Journal of Medical science. 74(6): 507-509.
Agarwal, S. & Seith, V. (2009). Newborn Care Practices among Urban Poor in Indore, India:
Gaps Reasons and Possible Programme Options. Available @ Http:// www.uhrc.in
retrieved Nov.20, 2009.
Ahmed, O. & Verber (2011). Home Delivery and Newborn Care among Women in Nigeria.
Global Journal of Medical Sciences 9 (7): 204-209.
Alam, M. A. & Murray, C. O. (2008). Newborn Umbilical Cord and Skin Care in Sylhet District,
Bangladesh: Implication for Promotion of Umbilical Cleansing with Topical
Chlorhexidine. Biomedical Journal 17(8): 13 -16.
Ambe, J., Bello, M., Yahaya, S. & Omotora, B. (2010). Umbilical Cord Practices in Konduga
Local Government Area of Bornu State, North East Nigeria. Journal of Tropical Medicine
9 (6): 87 - 92
Amin, R. & Khan, A. H. (2009). Traditional Beliefs and Cord Care in Rural Bangladesh.
Journal of Tropical Pediatrics. 60(4): 293-295.
Anderson, S. & Philip, A. (2004). Management of the Umbilical Cord: Cord Regimen,
Colonization, Infection and Separation. Available @ http: neoreviews.aappublications.org
Antai, T. E. & Effiong, F. O. (2009). Septicaemia among Neonates with Tetanus. Journal of
Tropical Pediatrics 3 (10) 210-213.
Arad, P. (2009). Umbilical Care and Cord Separation. Available at http://www.fetaneonatal.com
Retrieved February 12, 2010.

86
Bang, H. & Andem G. (2011). Neonatal Tetanus: Mortality Rate and Risk Factors. Int. Journal
of Epidemiology 86(9):392-401.
Baqui, A. & William, T. (2009). Newborn Care in Rural Uttah Predesh. Indian Journal of
Paediatrics 74(3): 241-247.
Basil T., Kayode, S., Mark, S. & Mbe, T. (2009). Neonatal Tetanus: A Continuing Challenge:
Risk Factors, Clinical Features and Prognostic Factors. Global Journal of Medical
Sciences 6(4):20-28.
Bassey. U., Thompson, W. & Udia, T. (2009). Role of Antimicrobial Application to the
Umbilical Cord in Neonates: A Review of the Evidence. American Academy of
Pediatrics 12(2):50-56
Bello, K. & Omotara, B. (2010). Neonatal Tetanus: Mode of Infection, Prevalence and
Prevention. International Journal of Epidemiology 67(9): 56 - 59
Bemor, F & Uta, D. (2011). Saving Newborn Lives in Nigeria: Integrated Health Strategy.
Global Journal 74(6): 21-26
Bennett. J. & Adetunde, T. (2010). Influence of Native Customs on Newborn Care in Nigeria.
Internaltional Journal of Epidemiology 25(4): 879-884.
Benson, T. & White R, (2006). Risk Factors in Neonatal Infection. Journal Pediatric
98(16):224-228
Buckley, Y. & Thompson, K. (2010). Umbilical Cord: Trans-Cultural Care and Customs.
Journal of Advanced Nursing 17, 21-25.
Danulo, B., Dickson, A & Kule, S. (2010). 4 Million Neonatal Deaths: When? Where? How?
Global Journal 36(7):81-85.
Dibson, T. W. & John, F. (2010). A Comparative Study of Neonates’ Umbilical Cord
Management. Journal of Pediatric 97:817-822.
Dore, H. N., Buch, S. C. & Tom, K. (2007). Increased of Staphylococci in Neonatal Septicaemia.
American Academy of Pediatrics 24 (6) 313-316.
Ebong, T. O. (2006) Old Calabar Through the Century. Lagos: ACE Press.
P. 53-61.

87
Eneji, R., Eyemba, S. & Markinde (2010). Bacterial Colonization and Neonatal Infection.
Global Journal 78:1227-1233.
Ezenduka, P.O. & Eze, P. (2002). Umbilical Cord Care among Nursing Mothers in Enugu East
Local Government Area, Enugu. West Africa Journal of nursing 13(2) 110-111.
Farahani, L. A. (2008) Effect of Tropical Application of Breast Milk and Dry Cord Care on
Bacterial Colonization and Umbilical Cord Separation Time in Neonate. Clinical
Medicine 3(6) 18-24.
Federal Ministry of Health Nigeria. (2006). Fact on Safe Motherhood Abuja. Federal Ministry of
Health. P.23:7-11
Gaana, P. E. (2009). Neonatal and Perinatal Mortality. International. Journal of Tropical
Medicine 4(4):16-24.
Garner, F. V. (2008). Care In Normal Birth: A Practical Guide. New York: Jack ken. P.18-31
George, J. B. (2011). Nursing Theories: The Base for Professional Nursing Practice. New York:
Pearson. P. 113-135.
Green, P. T., Udoh, E. & Peters, J. (2006). Clinical Study of Septicemia. Journal of Pediatrics
43: 328-332.
Gladstone, T. (2009). Randomized Study of Two Regiments. American Academy of Pediatrics
27: 124-127
Harrison, T. S. & Stanley, H. (2007). Umbilical Cord as a Reservoir of Infection Clinical
Pediatric 20:925-28.
Hoque, B. & Selwyn, C. (2008) A Comparative Study of Neonatal Umbilical Cord Management.
J. Pediatr 8:210-214
Isangedihi, A., Joshua, M., Asim, A. & Ekuri, E. (2004). Fundamentals of Research and
Statistics, Calabar: University Press.
Jeol-Madewase, V.I., Oyedeji, Y. & Elemi, T. (2008). Cord Care Practices of South West
Nigerian Mothers. Journal of Tropical Pediatrics 15(8):115-118.

88
Johnson, T. & Wale, T. (2006). Risk factors in Bacterial Neonatal Omphalitis. Global Journal 42
(8) : 92-98.
Luka, J. W. (20011). Effect of Cord Regimen on Bacteria Colonization in Newborn Infants.
American Academy of Pediatrics 79(9): 395-398.
Meberg, B. & Brown, P. T. (2007). Bacterial Colonization and Cord Infection. Clininal Pediatr
73(7):47-51.
Mentu, K. Benson, R. (2009). Risk Factors for Neonatal Infections. Journal of Advance
Nursing. 42(1) 24-30.
Mueller, H. & Johnson, M. (2009) Avoiding Neonatal Deaths: An Intervention Study of
Umbilical Cord management. Journal of Tropical Pediatrics 23 (4): 50 - 54
Obimbo, O. & Oruambo, T. (2008): Knowledge, Attitude and Practice of Mothers and Health
Workers Regarding Care of Newborn Umbilical Cord in South West, Nigeria . Journal of
Tropical Pediatrics 8 (15): 45 - 48
Obuekwe, T. R. & Obuekwe, E. (2008). Identifying Indigenous Health Technology Used By
women in a Rural Community in Nigeria on the Stumps of Newborns: An Increase in
Cord Infection and Neonatal Tetanus. Clininal Pediatr 36:648-652.
Okedo, K. & Nelson. P. & Lawal, W (2010). An Analysis of Custom Related to Child Birth.
Tropical Medicine 25:172-176.
Park, K. (2009). Park’s Textbook of Preventive and Social Medicine. Jabalpur: Nagar. P. 34-39.
Peter, O. & Johnson, J. (2010). Risk Factors for Neonatal Infections. Global Journal 12:40-46.
Peters, U. & Ube, L. (2010). Factors nfluencing Neonatal Cord Management. Journal of Tropical
Pediatrics 53(3):302-306.
Pezzati, M. U. & Biagioli, D. (2008). Management of the Newborn. Chicago: WB. P. 23-36
Senarath, T. R. (2010). Who Teaches Mothers How to Care for Babies Cords? West African
Journal of Nursing 16 (1):54
Shafique, F. & Jack, G. (2006). Trends in Umbilical Cord Care: Scientific Evidence for Practice:
Relationship between Bacterial Colonization and Infection. Available at
http://www.comminit.Com/c Accessed Feb. 23, 2010

89
Sharan, H. (2010). Determinate of Safe Newborn Care Behavior in Rural Karnataka. Journal of.
Pediatr. 4:45 - 48
Smith, C & Kelly O. (2011). Newborn Care among Indigenous People of Zimbabwe. Journal of
advance Nursing 99(14): 322-226.
Sreeramaraddy, C. T., Josh, I. Sreekumaran & Giri (2006). Newborn Care among Urban Women
in Western Nepal. Clinical Pediatr. 19 (71): 34 - 38
Thapa, N. & Keshi, P. (2011). Infant Death Rates and Animal-Shed Delivery in Remote Rural
Community of Turkey. Journal of Tropical Pediatrics (21):26-9.
Thompson, F., Udom, P. & Ugorji, H. (2011). A Comparative Study of Neonates’ Umbilical
Cord Management. Clinical Pediatr 9 (3): 76 - 79.
Tuladhar, S. (2010). The Determinants of Good Newborn Care in the Rural Area of Nepal.
Available At http://Ir.centerbury.ac.nz/bitstream/pdf Accessed March 23, 2010.
Ulum, R. & Dorek, E. (2007). Attitude, Change and Social Influence. Lagos: WIMCO.
P. 43-55
Umar, J. & Alliu, M. (2011). Bundling a New Identified Risk Factor for Neonatal Infections :
Implication for Global control. International Journal of Epidemiology. 25 (9): 16-18
Waise, P. & Kaikoba, S. (2008). Acceptability of Evidence Based Neonatal Care Practice in
Rural Uganda: Implications for Programming. International nursing journal 2(2): 52 -
54.
World Health Organization (2006). Neonatal and Perinatal Mortality: Country, Regional and
Global Estimate. Available At Http://Www..Who.Int.Accessed January 18, 2010.
World Health Organization (2007). Review of Evidence on Cord Care Practices. Available At
http://www.who.int Accessed Jan 18. 2010
World Health Organization (2009). Essential Newborn Care. Report of a Technical Working
Group. Geneva P. 22-28.
Zupan, Q. T. (2007). Tropical Antimicrobials Applied to the Umbilical Cord Stump, a New
Intervention Against Tetanus. Journal of Tropical Pediatrics. 6 (5): 35 - 37

90
Appendix 1
DEPARTMENT OF NURSING SCIENCE
UNIVERSITY OF NIGERIA, ENUGU CAMPUS
ENUGU.
Dear Respondents,
This questionnaire is designed to study and determine the umbilical cord care and management
outcome among mothers in Calabar South, Cross River State. Nigeria. The questionnaire is
purely designed for academic purpose and all the information collected will be kept strictly
confidential. The researcher will appreciate genuine, direct, specific and clear answers.
Section A: Bio data
Instruction: Please tick the appropriate response to the following questions:
1. Age: Last birthday of mother ………………………………..
2. Tribe (Ethnicity)………………………………………………………..
3. Marital status:
a. Married [ ]
b. Single [ ]
c. Separated [ ]
d. Divorced [ ]
e. Widowed [ ]
4. Number of children
a. 1 [ ]
b. 2 [ ]
c. 3 [ ]
d. 4 [ ]
e. 5 and above [ ]
5. Position of present infant…………………………………….
6. Age of infant………………………………………………………….

91
7. Religion:
a. Christianity [ ]
b. Moslem [ ]
c. Traditionalist [ ]
d. Others specify..............................
8. Highest Educational attainment
a. No schooling [ ]
b. primary [ ]
c. Secondary [ ]
d. Tertiary [ ]
9. Occupation:
a. Farming [ ]
b. Hair dressing [ ]
c. Petty trading [ ]
d. House wife [ ]
e. Student [ ]
f. Civil servant [ ]
g. Applicant [ ]
10. Income per Month:
a. Less than N18, 000.00 [ ]
b. N19, 000.00 - N30, 000.00 [ ]
c. More than N31, 000.00 [ ]
Section B: Knowledge of Standard Cord Management
11. What do you understand by umbilical care? [ ]
a. It involves the use of herbs on the cord [ ]
b. Use of herbs and keeping the baby away from visitors [ ]
c. Tying,cutting and cleaning with methylated spirit only [ ]
d. Non application of substances on the cord till it detaches [ ]
e. others specify…………………………………………..

92
12. What material should be used in tying the umbilical cord ?
a. String of cloth [ ]
b. cord clamp [ ]
c. rubber band [ ]
d. hair thread [ ]
e. Others (specify)………………………………………..
13. What solution do you think should be used in cleaning the umbilical cord?
a. salt and saliva [ ]
b. herbal solution [ ]
c. methylated spirit [ ]
d. hot water [ ]
e. Others (specify)……………..
14. How long does it take an umbilical cord to detach?
a. 3- 4days [ ]
b. 5-15days [ ]
c. 4weeks and above [ ]
d. others specify…… ………………………. [[
15. What is the advantage of clean cord care?
a. To wade off evil spirit/fast cord separation [ ]
b. To prevent infection [ ]
c. To prevent abdominal pain [ ]
d. To prevent ‘Odon’ [ ]
e. Others specify…………... {
16. What is your source of knowledge?
a. Mother/mother–in-law [ ]
b. Church members [ ]
c. Traditional Birth Attendants [ ]
d. Health worker [ ]
e. Mass media [ ]

93
Section C: Materials for Cord Care
17. Where did you deliver your last baby?
a. Church [ ]
b. prayer house [ ]
c. Hospital [ ]
d. health centre [ ]
e. Home [ ]
f. Traditional Birth Attendant [ ]
18. Which of the following was used in tying the umbilical cord after delivery?
a. Twine [ ]
b. Hair Thread [ ]
c. String of cloth [ ]
d. Cord clamp [ ]
e. Bandage [ ]
f. Others (specify)………………………………….
19. What was used to separate baby from mother after delivery?
a. knife [ ]
b. Razor blade [ ]
c. Sterile scissors/surgical blade [ ]
d. Farm instrument [ ]
e. No idea [ ]
f. Others (specify)…………………………….............
20. Which of the following solutions was used in cleaning the umbilical cord? (Tick as many as
applicable)
a. Dettol solution [ ]
b. Hot water [ ]
c. Saliva only [ ]
d. Saliva and salt [ ]
e. Salt solution [ ]

94
f. Alcohol (methylated spirit) [ ]
g. Herbal preparation [ ]
21. After cleaning, did you apply anything else to the cord?
a. No [ ]
b. yes [ ]
22. If yes to question 15, which of the following did you apply to umbilical cord? (Tick as
many as applicable)
a. Breast milk (colostrum) [ ]
b. Herbal preparation [ ]
c. Native chalk [ ]
d. Dusting powder [ ]
e. Saliva mixed with salt and sand
from door post [ ]
f. “ Ndodop” [ ]
g. Gentian violet [ ]
h. Penicillin ointment [ ]
i. Palm kernel oil [ ]
j. Rub/mentol [ ]
k. Hot sand [ ]
l. Lantern wax [ ]
m. Tincture of Iodine [ ]
n. Cow dung [ ]
O. others specify………………………………………
Section D: Reason for Choice of Materials for Cord Care
23. What was your reason for choice of materials for umbilical care (tick as many as applicable)?
a. To wade off evil spirit and hasten cord separation [ ]
b. Very cheap [ ]
c. Stops after birth pains [ ]
d. Prevents infection [ ]
e. Very effective and for fast cord separation [ ]

95
f. Pressure from family members [ ]
g. Protects baby from ‘‘evil eye’’ [ ]
h. Prevents ‘‘Akpa’’ [ ]
i. Prevents ‘‘Odon’’ [ ]
j. lack the power to take any Other [ ]
k. Others specify …………………………………………………
Section E: Techniques for cord Care
24. How did you take care of your hands during cord care?
a. Washed hands with water before attending to the cord [ ]
b. Washed hands with soap and water before and after
attending to the cord [ ]
c. Washed with soap and water after attending to the cord [ ]
d. Clean hand on wrapper after cord care [ ]
e. Clean hand with clean serviette/handkerchief after cord care [ ] {
25. Did you practice?
a. Dry method? [ ]
b. wet method ? [ ]
26. If wet method, which of the cleaning methods was practiced?
a. Cleaning cord base before surrounding skin [ ]
b. Cleaning cord and surrounding skin at the same time [ ]
c. cleaned cord stump only [ ]
d. cleaned the surrounding skin only [ ]
e. cleaned only the material used in tying the cord stump [ ] [ {
27. How often was the cord stump cleaned?
a. morning, afternoon and evening (3times) [ ]
b. Once a day [ ]
c. After each nappy is changed [ ]
d. Delivery time only [ ]
e. no cleaning [ ]

96
28. Which of the following methods did you practice?
a. Open method [ ]
b. Closed method [ ]
29. If closed method, which of the following was used to cover the umbilical cord?
a. Bandages [ ]
b. piece of mother’s cloth [ ]
c. Gauge bandage [ ]
d. Abdominal binder [ ]
Section F: Outcome of Care
30. Did you observe any abnormal changes while treating the umbilical cord?
a. Yes [ ]
b. No [ ]
31. If yes to question 31, which of the following did you observe? (Tick as many as applicable).
a. Red skin around the base of the umbilical stump [ ]
b. Yellowish discharge from the cord [ ]
c. Foul smelling cord [ ]
d. Pain when touched the skin around the stump [ ]
e. Child unable to open mouth/suck [ ]
f. Others specify……………………………………
32. How was the problem resolved?
a. child taken to patent medicine dealer [ ]
b. Child taken to health facility [ ]
c. child taken to TBA/traditional healer [ ]
d. Child taken to church [ ]
e. Cared for at home [ ]
f. others specify………………………………………………….

97
33. What was the duration of the problem before reporting to the health
Facility.
a. within 24 hours [ ]
b. 2-3days [ ]
c. 4-6days [ ]
d. 7days and above [ ]
34. What other thing did you observe on the baby? (Tick as many as applicable)
a. Persistent fever [ ]
b. Twitching of the body [ ]
c. difficulty in breathing [ ]
d. nothing else [ ]
e. others specify……………………………………………….
35. How many days did it take the cord stump to detach?
a. 3 - 4days [ ]
b. 5 – 15days [ ]
c. 16days and above [ ]
d. Others specify…………............................... [ ]
36. How long did it take the navel to heal?
a. Between one month and six weeks [ ]
b. Two months [ ]
c. no idea [ ]
d. No idea [ ]
37. has any of your children died within the first six weeks of life?
A. Yes [ ]
B. N0 [ ]
38. If yes to question 38, what was the cause?
a. Did not cry immediately after birth [ ]
b. Cried excessively, unable to open mouth and refusal to suck. [ ]
c. Redness, purulent discharge from cord stump, oedema and pains [ ]
d. Congenital malformations [ ]
e. others specify………………………………………………………..

98
Appendix 2
CALCULATION OF SAMPLE SIZE
n = Z 2
P (1 – P)
d2
Where n = the sample size
Z = Confidence Coefficient (1.96)
P = Proportion of women who used standard procedure for cord care
from previous study (0.12) (Ambe et al, 2010)
d2
= Tolerable error = 0.03
n = (1.96)2 (.12) (.88)
0.032
n = (3.84) (.12) (.88)
0.03× 0.03
n = 451

99
Appendix 3
SPSS-18 results: Test-retest Reliability Estimate for Umbilical Cord Management
Questionnaire.
A test- retests reliability estimate was carried out to ensure the reliability of the test instrument.
The questionnaire has a re-test reliability estimate (two weeks interval)
of r = .99 showing that the questionnaire is reliable and can be used for the study
Test-retest reliability estimate
Retest
Test_1 Pearson Correlation .993
Sig. (2-tailed) .000
N 50



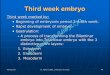
![hernia of the umbilical cord [وضع التوافق] of the umbilical cord.pdf · Umbilical cord hernia…cont Conclusion: ¾Hernia of the umbilical cord is a rare entityy, of the](https://img.pdfslide.us/doc/110x75/5ea7ce695a148409cd011fd0/hernia-of-the-umbilical-cord-of-the-umbilical-cordpdf.jpg)























