Embed Size (px)
Citation preview
PULMONARY
REHABILITATION
Anna Sárközi MD.
Dept. of Pulmonology
University of Debrecen 05.04.2013
•1

DEFINITION
evidence-based, multidisciplinary, and comprehensive intervention for patients with chronic respiratory diseases
who are symptomatic and often have decreased daily life activities
integrated into the individualized treatment of the patient
it is designed to reduce symptoms, optimize functional status, increase participation, and reduce health care costs by stabilizing or reversing systemic manifestations of the disease
Nici, L et.al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med 2006; 173: 1390.
•2
WHY IS IT IMPORTANT ??
The total number of case of COPD in
the world approxi. 280 million persons
6th cause of death worldwide in 1990
by 2002 the ranking had risen to 5th
by 2030 COPD would become the 3-4th
cause of death worldwide (WHO)
Prevalence and morbidity data greatly underestimate the total burden of COPD because the disease is usually not diagnosed until it is clinically apparent and moderately advanced
•3

Age-adjusted death rates for COPD by country and by sex, ages 35 to 74 years adapted from World Health Statistics Annual, WHO
Hurd S Chest 2000;117:1S-4S ©2000 by American College of Chest Physicians •4
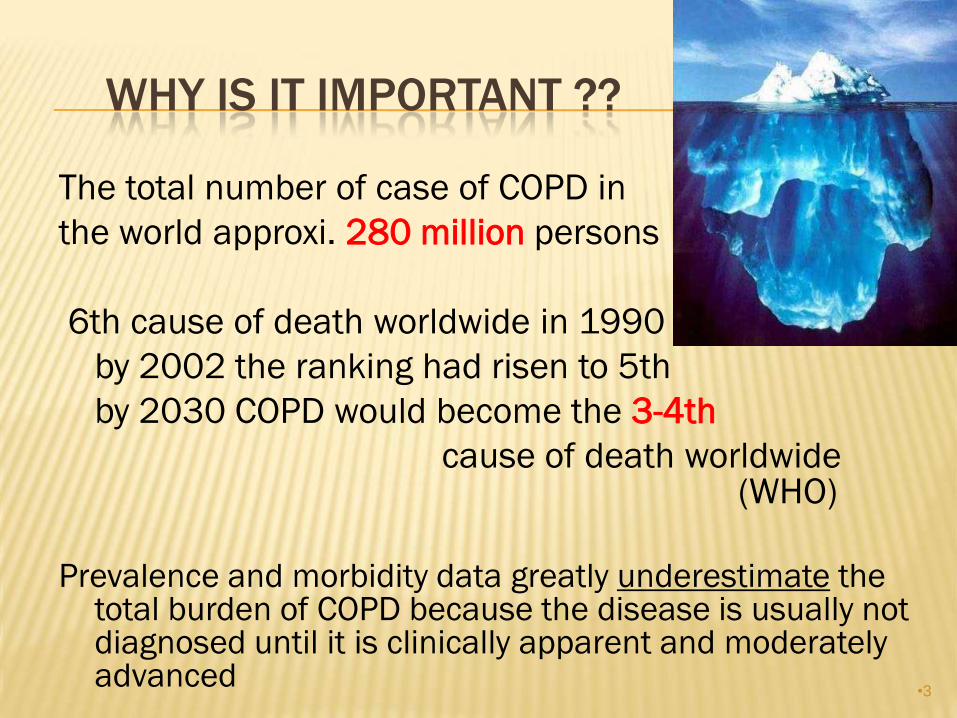
MORTALITY TRENDS
NHLBI/WHO 2002
Percent change in age-adjusted death rates; proportion of 1965 rate in the USA
•0
•0.5
•1.0
•1.5
•2.0
•2.5
•3.0
Coronary
heart
disease
Stroke Other CVD COPD All other
causes
1965–1998 1965–1998 1965–1998 1965–1998 1965–1998
– 59% – 64% – 35% + 163% – 7%
•5

WHEN TO START ??
•6
AIMS
•7
PRINCIPAL GOALS OF PULMONARY
REHABILITATION
to reduce the patient symptoms
increase participation in physical and social activities
to decrease disability
to improve the overall quality of life (QOL)
retain the achieved results by the optimal medication in
the treatment
to reduce the numbers of exacerbations, the numbers of
emergency health cares, health care costs and
numbers of hospitalization
stabilizing or reversing systemic manifestations of
disease •8
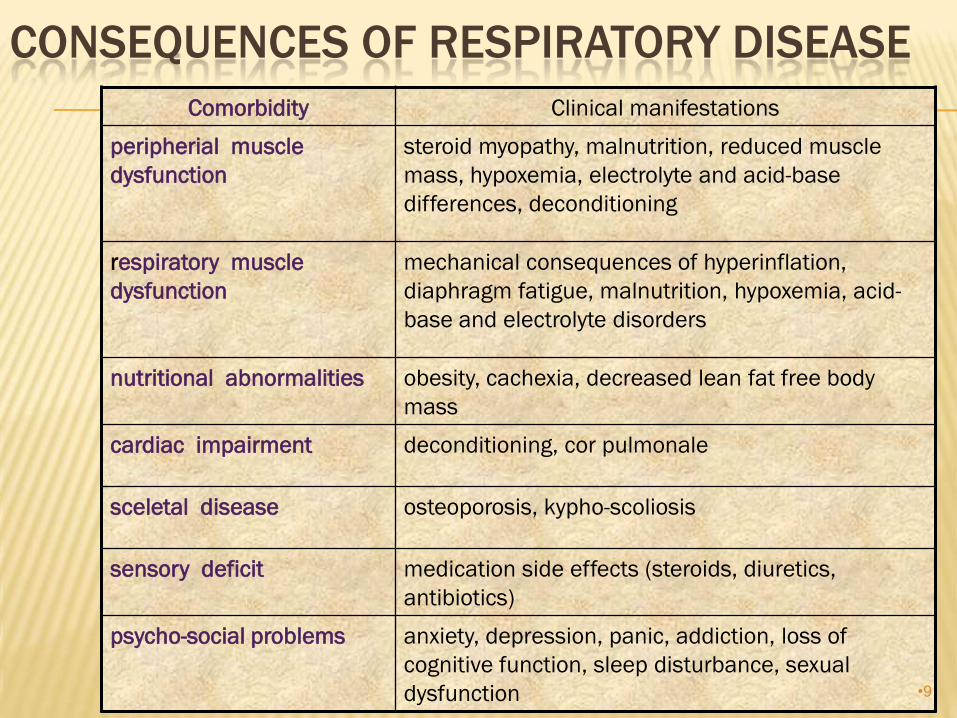
CONSEQUENCES OF RESPIRATORY DISEASE
Comorbidity Clinical manifestations
peripherial muscle
dysfunction
steroid myopathy, malnutrition, reduced muscle
mass, hypoxemia, electrolyte and acid-base
differences, deconditioning
respiratory muscle
dysfunction
mechanical consequences of hyperinflation,
diaphragm fatigue, malnutrition, hypoxemia, acid-
base and electrolyte disorders
nutritional abnormalities obesity, cachexia, decreased lean fat free body
mass
cardiac impairment deconditioning, cor pulmonale
sceletal disease osteoporosis, kypho-scoliosis
sensory deficit medication side effects (steroids, diuretics,
antibiotics)
psycho-social problems anxiety, depression, panic, addiction, loss of
cognitive function, sleep disturbance, sexual
dysfunction •9

SETTING FOR PULMONARY REHABILITATION
choice varies depending on
distance to program
patient preference
physical, functional, psychosocial status of patient
Outpatient
Inpatient intensive ward
pulmonary ward
rehabilitation ward
Home
Community Based
•10
HOSPITAL WARD
HOSPITAL BASED PROGRAM
monitor the patient over 24h
comorbid conditions
before-after a chest surgery
psychosocial problems
travelling difficulties
after intensive ward attendance, after
permanent automatic respiration
•11

INTERMITTENT POSITIVE
PRESSURE BREATHING
Active training
Mucus management
Recruitment of atelectasis
Special techniques
Photo from Prof. Dr. Pénzes István
•12

OUTPATIENTS
living active life
are employed
mild or middling serious disease
•13
CHOOSE THE RIGHT PATIENT
complain of dyspnea
non-smoking or smoking cessation program
involved
exercise intolerance
adequately motivated
accept the guideline
•14

PATIENTS SELECTION
obstructive diseases : COPD, bronchiectasis, persistent
asthma, bronchiolitis obliterans, cystic fibrosis
restrictive
interstitial diseases
chest wall neuromuscular (for example paralysis of n.phrenicus)
other diseases : lung cancer, pre-post surgery on thorax or abdomen, obesity-related respiratory disease, before – after lung transplantation
Pulmonary Rehabilitation; Guidelines To Success
John E. Hodgkin,MD; Bartolome Celli, MD; GerilynConners, RRT2009
•15

EMPHYSEMA
•16
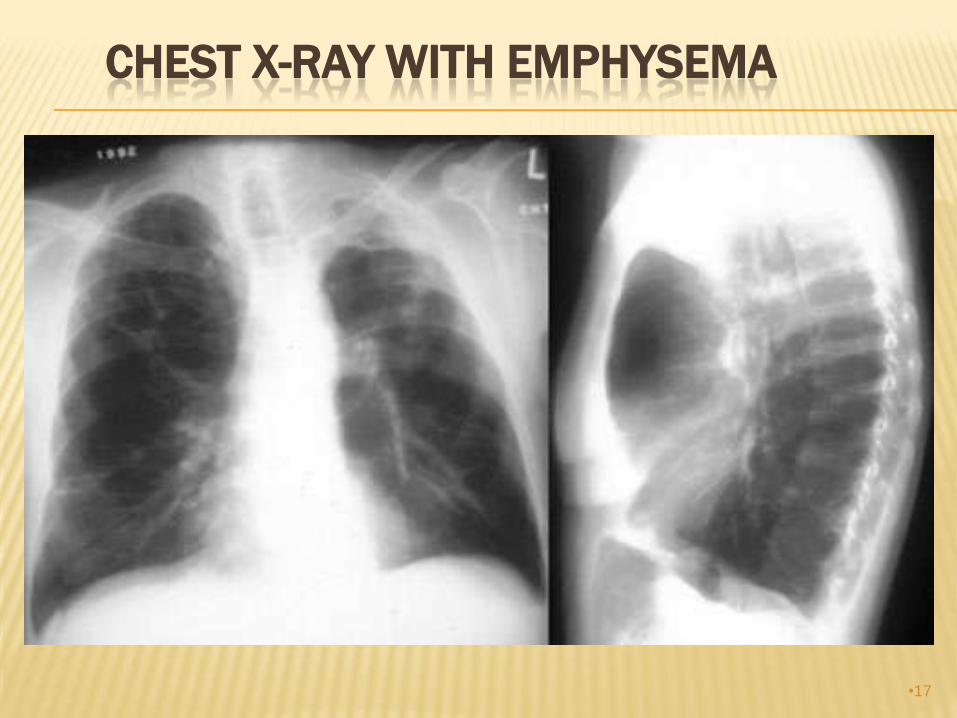
CHEST X-RAY WITH EMPHYSEMA
•17

CONTRAINDICATION OF PR
Absolute:
inflammation
acidosis
have bloody sputum
acut pulmonary embolia
acut pneumothorax
intolerantia of dyspnea
don´t compensated cor pulmonale
severe heart failure
severe musculo-sceletal disease •18

CONTRAINDICATION OF PR
Relative:
dementia
do not feel like it
drugs are not normally treated with
COPD and asthma bronchiale
•19
ASSESS THE PATIENT'S CONDITION
measurement of lost functions (mild, moderate, serious) :
physical examination
spirometry
x-ray
bloodgas
daily activity record
complications in the patient's medical history, which may occur in the stress test (ischemic heart disease, low oxygen levels, cardiac arrhythmia)
•20

INTERDISCIPLINARY TEAM
pulmonary rehabilitation physicians
specialist nurse and assistant
respiratory, physical and occupational therapists
dieticians
psychologists
social worker
exercise specialist
•21
ESSENTIAL COMPONENTS OF PR
exercise training and chest physiotherapy:
upper and lower endurance training
respiratory muscle training
strength training
psychosocial and behavioral intervention
nutritional advice and intervention
education
smoking cessation program
long-term oxygen therapy
End-life training!! •22
BREATH EXERCISE AND CHEST
PHYSIOTHERAPY
Controlled breathing out exercise
pursed lip respiration
lean forward
diaphragmatic breath
Chest physiotherapy posturnal drainage
to hit and vibrate the chest
flutter and PEEP mask
controlled cough
at forced breathing out
technic
„Breathing is the basic rhythm of life” Hippocrates
•23

PURSED LIP BREATHE
1. breathe in through nose
2. purse the lips as if you are going to whistle
3. breathe out through your pursed lip
4. don’t force the air out
5. breathe out should take
3-4x longer then breathing in
•24

DIAPHRAGMATIC BREATHING
1. place one hand (left) on the upper chest and the other
on your abdomen
2. breathe in slowly but deeply through your
nose keeping the upper chest quiet
3. slowly breathe out through your
pursed lip
4. let your abdomen relax to its original
position
Repeat 10 times, 1-2 times daily
•25

LEAN FORWARD
Lean forward at the waist and keep your back straight
Bending forward can help breathing more easily
Photo from Dr.Somfay A. •26

EXERCISE TRAINING
does not alter underlying respiratory impairment
improve dyspnea
targets endurance training of 60% max for 20-30 minutes,
repeated 2-5 times a week
interval training of 2-3 minutes high intensity with equal periods of
rest or low level exercise is tolerated well
unsupported arm exercise aids ADLs and respiratory accessory
muscle use
respiratory muscle training benefits have not been well
established
•27
LOAD TRAINING FORMS
two kind of load training forms:
endurance load training:
move bigger set of muscle with average intensity:
bicycle ergometer, runner
strengh generate training:
less muscle for a short period
of time with very intensive:
limb motions done with dumbbells
•28
ENDURANCE LOAD TRAINING
The training of the lower limbs:
runner, bicycle ergometer, stairs, in the
hallway, outdoors
over 60% of the max. capacity
30-45 min.
3-5 times a week
Training of upper limbs
•29
STRENGH GENERATIVE TRAINING
With 80% of the once liftable max. weight
8 repetitions
3 rounds
3 times a week
For 6-8 weeks
•30

EDUCATION
medication therapies
types of medication, action, adverse effects,
dose and proper us of inhaled medications
instructions in inhaler technique
appropriate use of oxygen
smoking cessation
therapeutic recreation
nutrition
psychosocial
•31
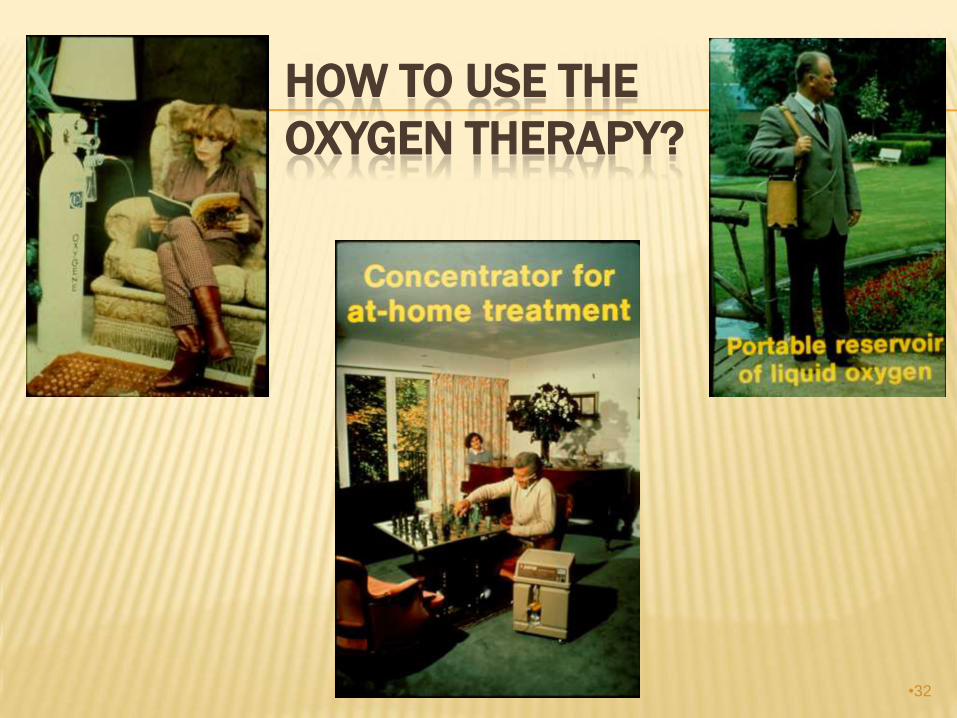
HOW TO USE THE
OXYGEN THERAPY?
•32
NUTRITIONAL COUNSELLING
both overweight and underweight can be a problem
25% of patients with moderate to severe COPD show a reduction in BMI which is an independent risk factor for mortality in COPD
reasons for difficulty eating should be explored: poor dentition, dyspnoea whilst eating
advise frequent small meals
•33

DIET
Loss of weight, cachexia causes weakness of muscle
Causes:
during meal the respiration changes, reduces arterial oxygensaturation
a full stomach reduces respiratory capacity, increases the dyspnoe
anxiety, depression reduces appetite
increased basic energy consuption
•34
PSYCHOSOCIAL INTERVENTION
Anxiety, depression, difficulties coping with chronic
disease
Aided by regular patient education session or
support groups
Instruction in progressive muscle relaxation, stress
reduction, panic control
•35
BENEFITS
improved exercise capacity
improved muscle strength
reduced dyspnoea
improved health-related QOL
duration of benefit
exercise benefit 12-18 mths
QoL benefit 24 mths
•36

WHAT THE PATIENTS SAY ABOUT PR
„I’m able to walk for 300-400 maters without stopping. I hadn’t been able to do for several years.”
Male age 69
„Being able to see and talk to other patients” Male age 72
„Before I didn’t do anything I just sat down, now I feel I really want to do the exercises. It has given me a new lease of life. Now I have more confidence going out, I go out more often to the market and shops.”
Female age 70
•37

REFERENCES
ATS/ERS statement on pulmonary rehabilitation (2006). American Journal of Respiratory and Critical Care Medicine, 173,1390-1413.
Bernard et al. (1998). Peripheral muscle weakness in patients with chronic obstructive pulmonary disease. American Journal of Respiratory and Critical Care Medicine, 158(2), 629-634.
BTS statement (2001). British Thoracic Society standards of care subcommittee on pulmonary rehabilitation. Thorax, 56, 827-834.
Foglio et al. (1999). Long term effectiveness of pulmonary rehabilitation in patients with chronic airway obstruction. European Respiratory Journal, 13(1), 125-32.
Griffiths et al. (2001). Cost-effectiveness of an outpatient mulit-disciplinary pulmonary rehabilitation programme. Thorax, 56(10), 779-784.
Guell et al. (2000). Long term effects of outpatient rehabilitation of COPD: A randomised trial. Chest, 117(4), 976-983.
•38

THANKS FOR YOUR ATTENTION
AND PARTICIPATION
•39