Embed Size (px)
Citation preview
Pulmonary embolism, pulmonary hypertension,cor pulmonale chronicum
KEY POINTS
• 1/1000/year• early treatment is highly effective, but is under- diagnosed, therefore, remains a major health problem• diagnostic strategy should be based on clinical evaluation (probability assessment)• value of PPV and NPV are high when concordant with clinical assessment• additional tetsting is neccessery when test result is inconsistent with clinical probability
Epidemiology
• USA: 117 %000VTE - 48 %000 DVT
- 69 %000 PE
(Arch Intern Med 1998; 158:585-593)
• NyE: 183 %000 VTE - 124 %000 DVT
- 60 %000 PE
(Thromb Haemost 2000; 83:657-660)
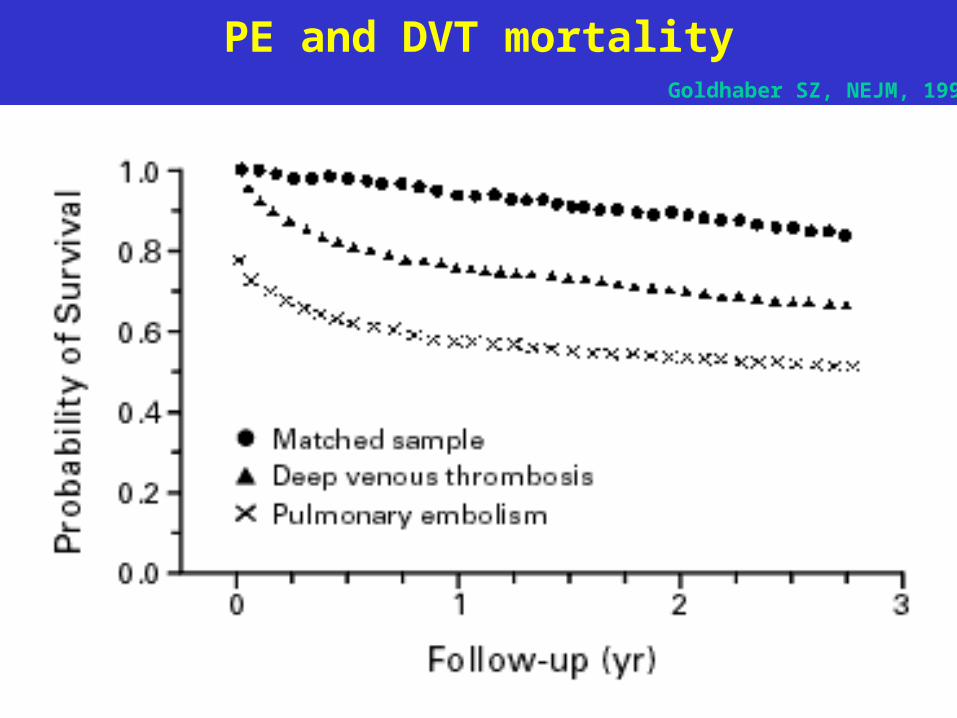
PE and DVT mortality Goldhaber SZ, NEJM, 1998
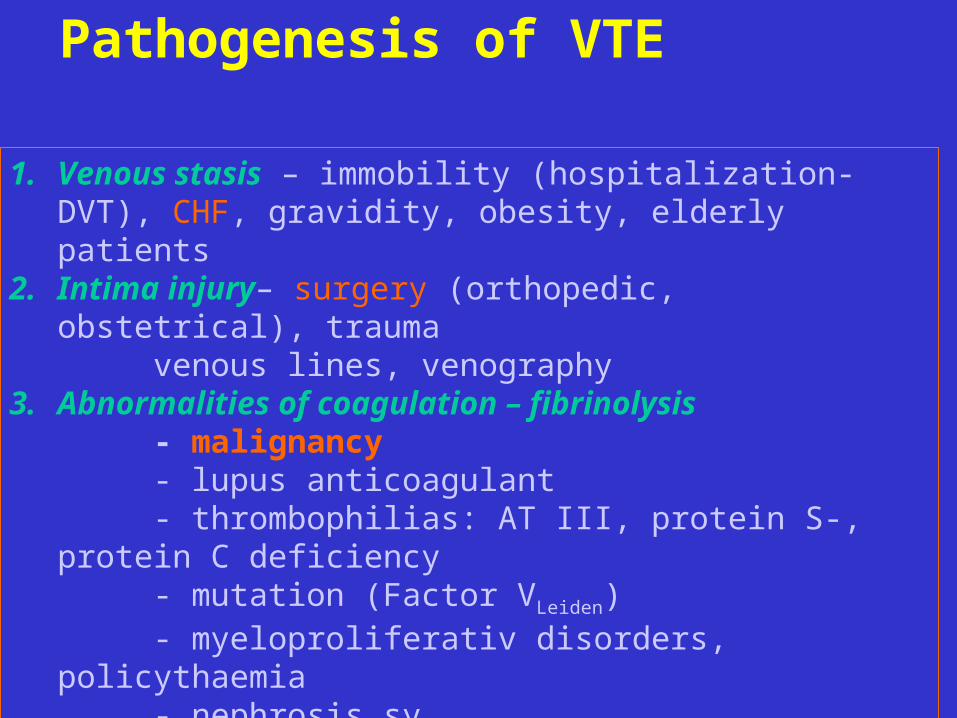
Pathogenesis of VTE
1. Venous stasis – immobility (hospitalization-DVT), CHF, gravidity, obesity, elderly patients
2. Intima injury– surgery (orthopedic, obstetrical), trauma venous lines, venography3. Abnormalities of coagulation – fibrinolysis
- malignancy- lupus anticoagulant - thrombophilias: AT III, protein S-, protein C deficiency- mutation (Factor VLeiden)- myeloproliferativ disorders, policythaemia- nephrosis sy- gravidity, contraceptive pills- colitis ulcerosa

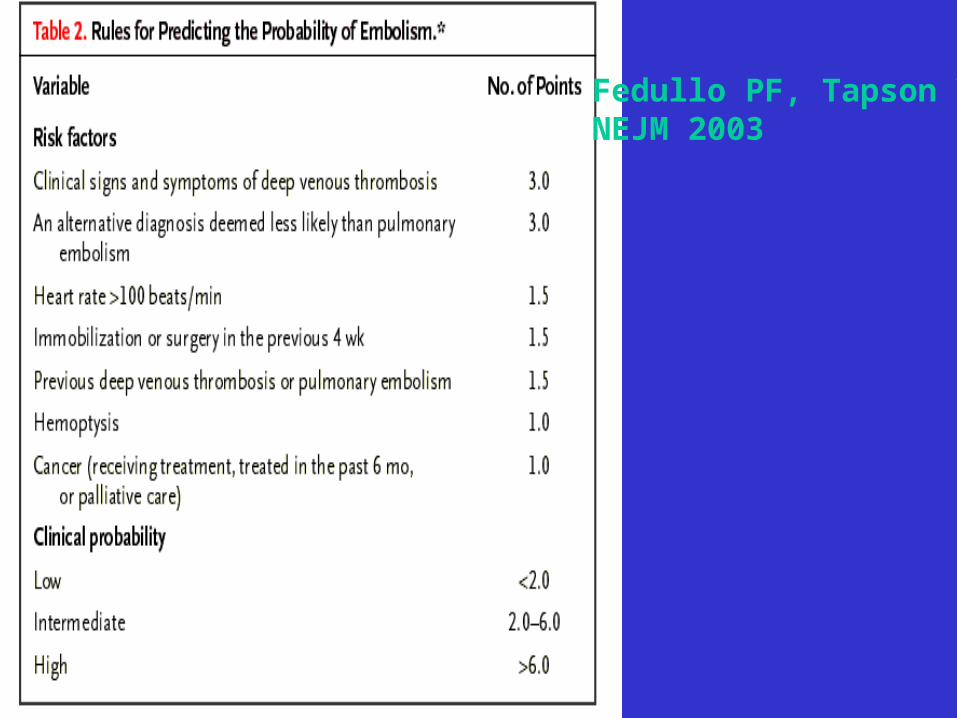
Fedullo PF, Tapson VFNEJM 2003
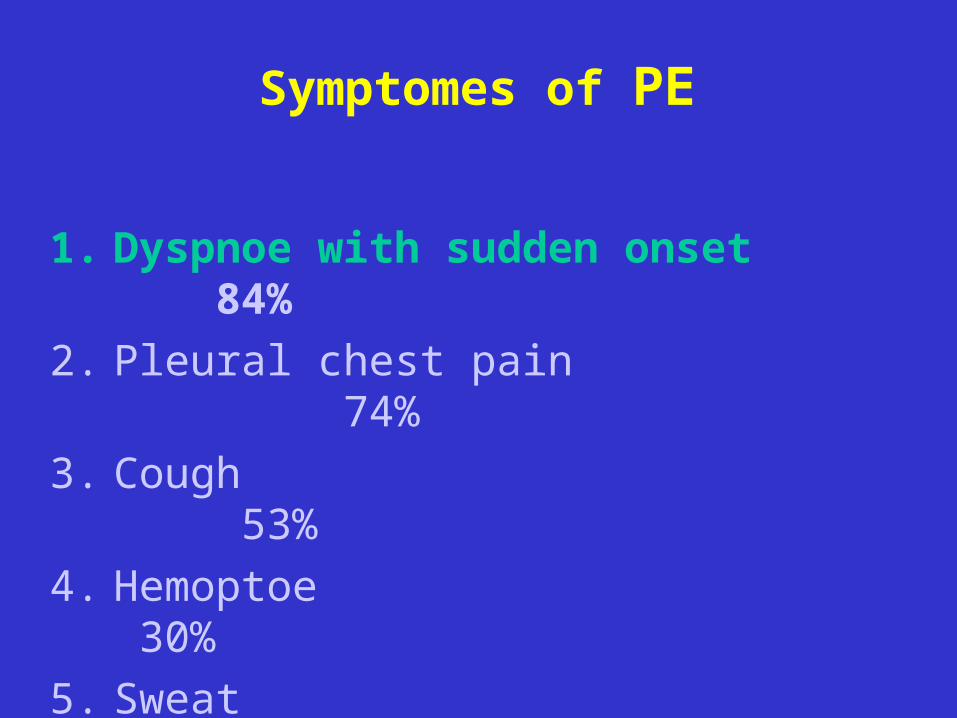
Symptomes of PE
1. Dyspnoe with sudden onset 84%
2. Pleural chest pain 74%
3. Cough 53%
4. Hemoptoe 30%
5. Sweat 27%
6. Non-pleural chest pain 14%
7. Syncope 13%
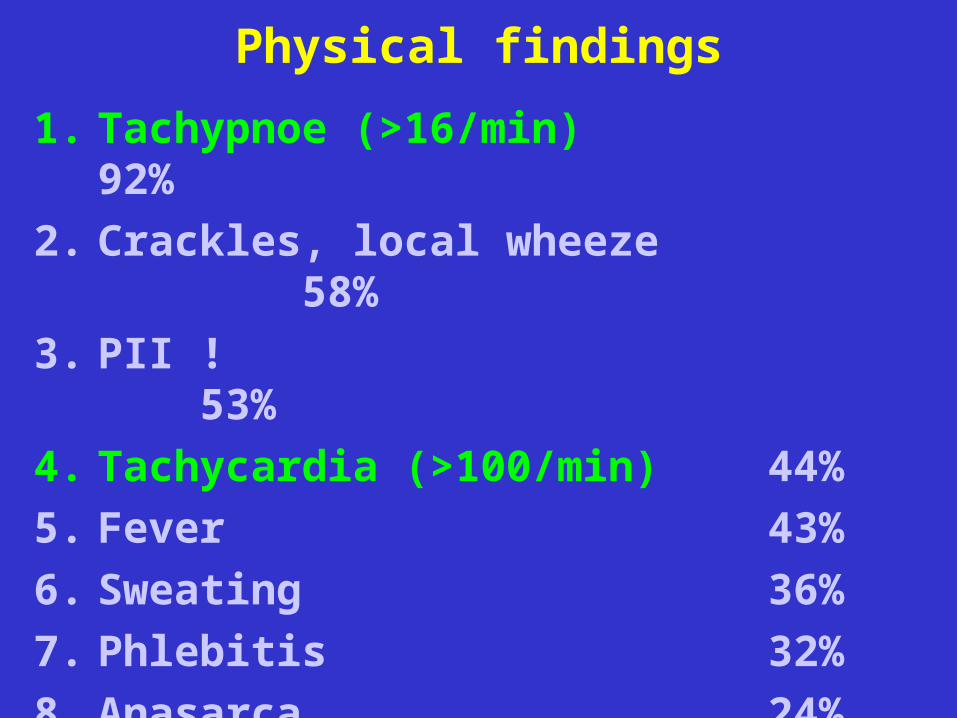
Physical findings
1. Tachypnoe (>16/min) 92%
2. Crackles, local wheeze 58%
3. PII ! 53%
4. Tachycardia (>100/min) 44%
5. Fever 43%
6. Sweating 36%
7. Phlebitis 32%
8. Anasarca 24%
9. Cyanosis 19%
10. Pleural friction rub, fluid 11%
Fedullo PF, Tapson VFNEJM 2003
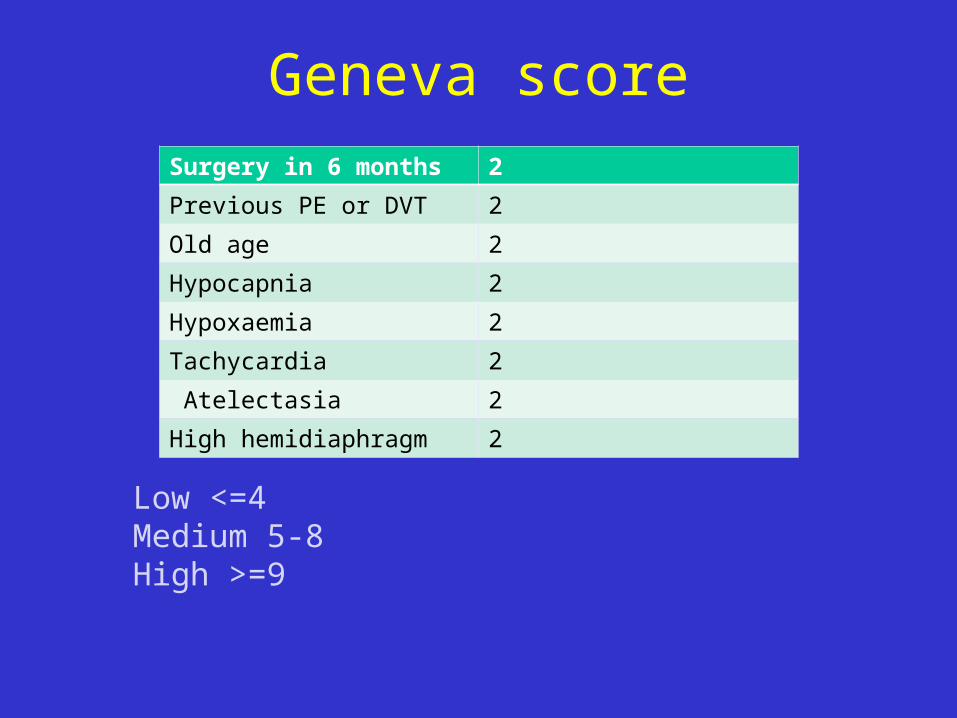
Geneva scoreSurgery in 6 months 2
Previous PE or DVT 2
Old age 2
Hypocapnia 2
Hypoxaemia 2
Tachycardia 2
Atelectasia 2
High hemidiaphragm 2
Low <=4Medium 5-8High >=9
Goldhaber SZ, NEJM, 1998
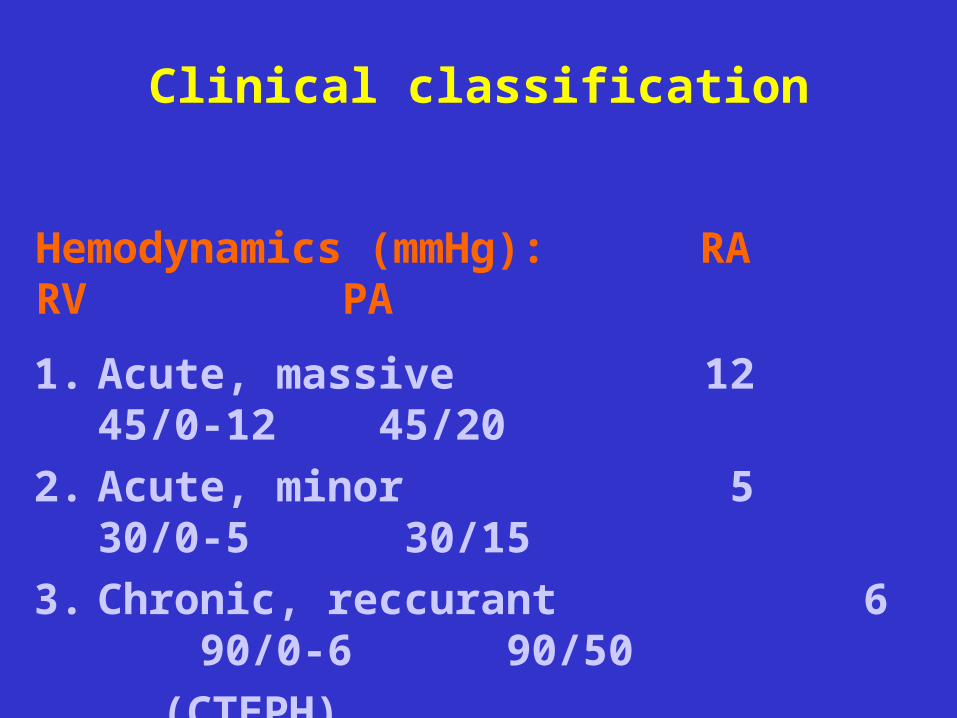
Clinical classification
1. Acute, massive 12 45/0-12 45/20
2. Acute, minor 5 30/0-5 30/15
3. Chronic, reccurant 6 90/0-6 90/50
(CTEPH)
Hemodynamics (mmHg): RA RV PA
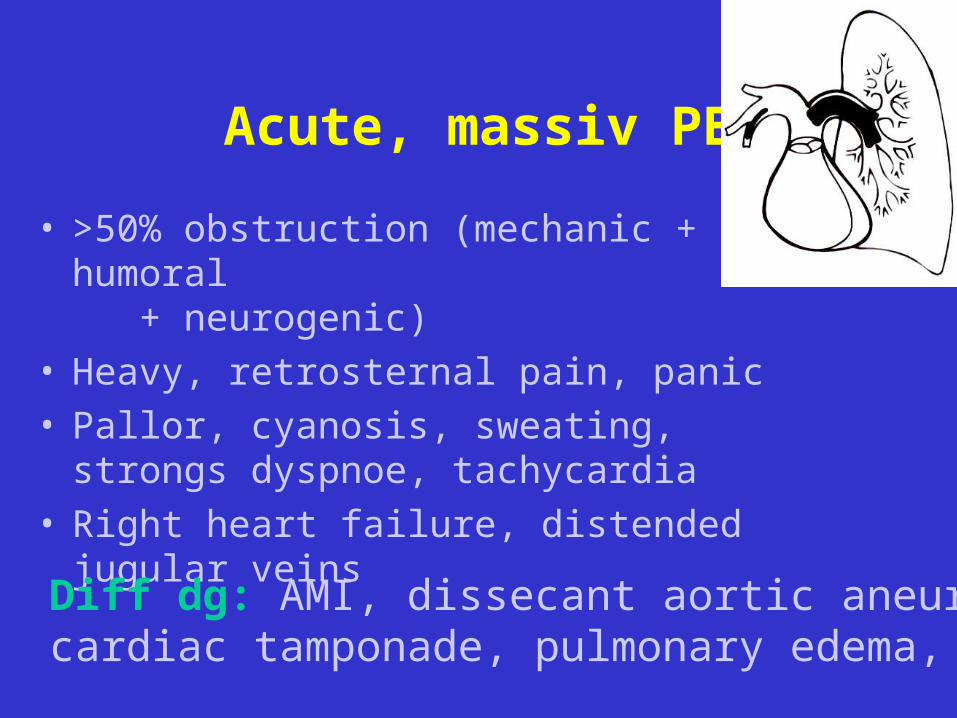
Acute, massiv PE
• >50% obstruction (mechanic + humoral + neurogenic)
• Heavy, retrosternal pain, panic• Pallor, cyanosis, sweating, strongs dyspnoe,
tachycardia• Right heart failure, distended jugular veins
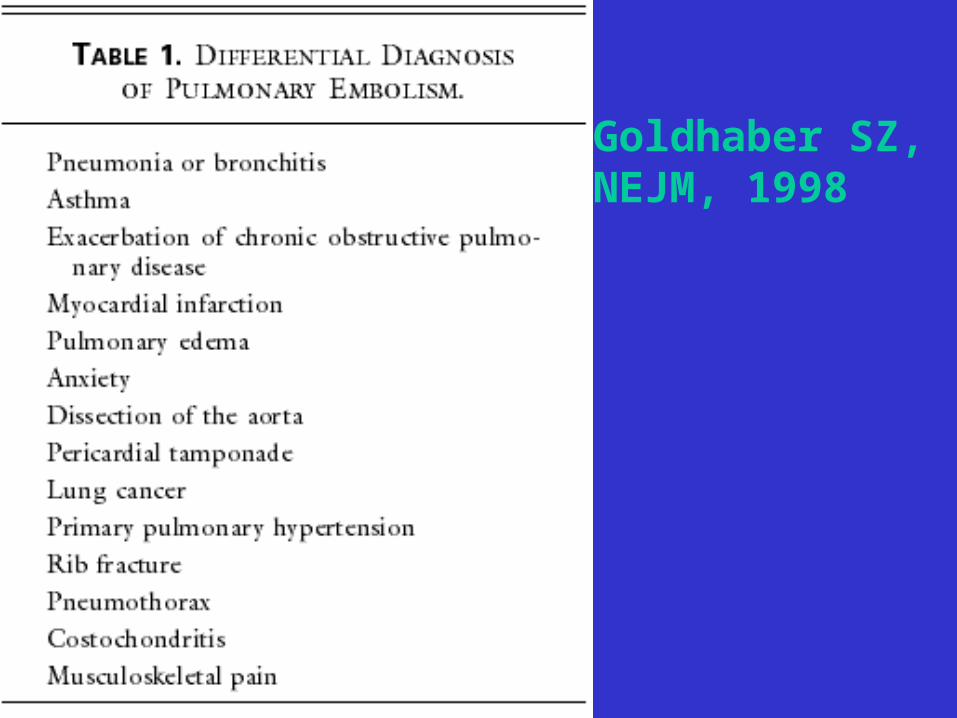
Diff dg: AMI, dissecant aortic aneurysm, cardiac tamponade, pulmonary edema, ptx, shock
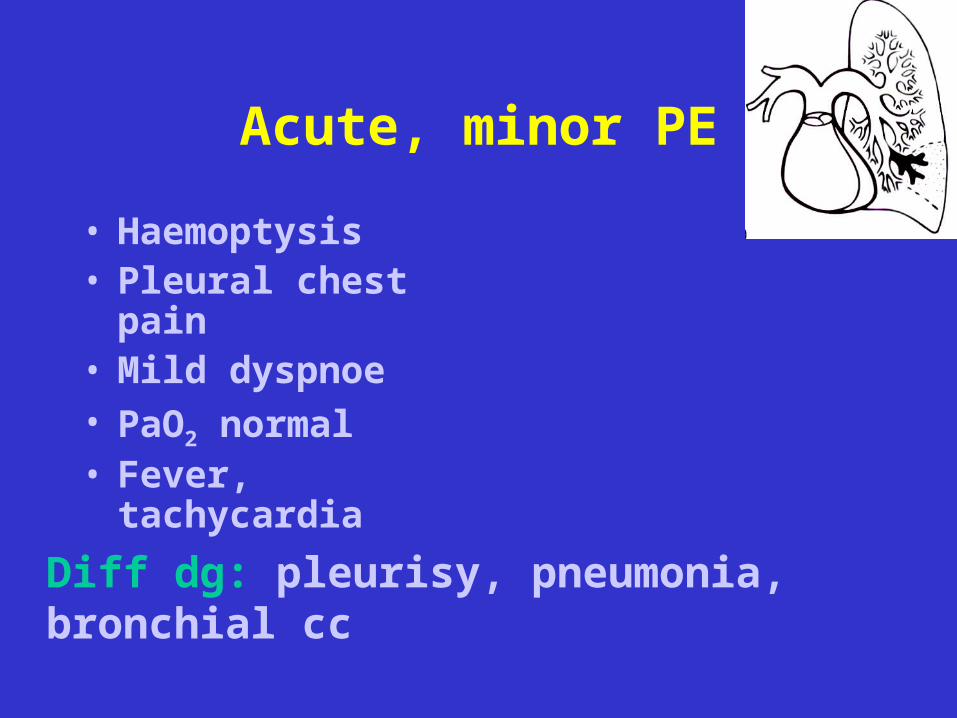
Acute, minor PE
• Haemoptysis• Pleural chest pain• Mild dyspnoe• PaO2 normal• Fever, tachycardia
Diff dg: pleurisy, pneumonia, bronchial cc
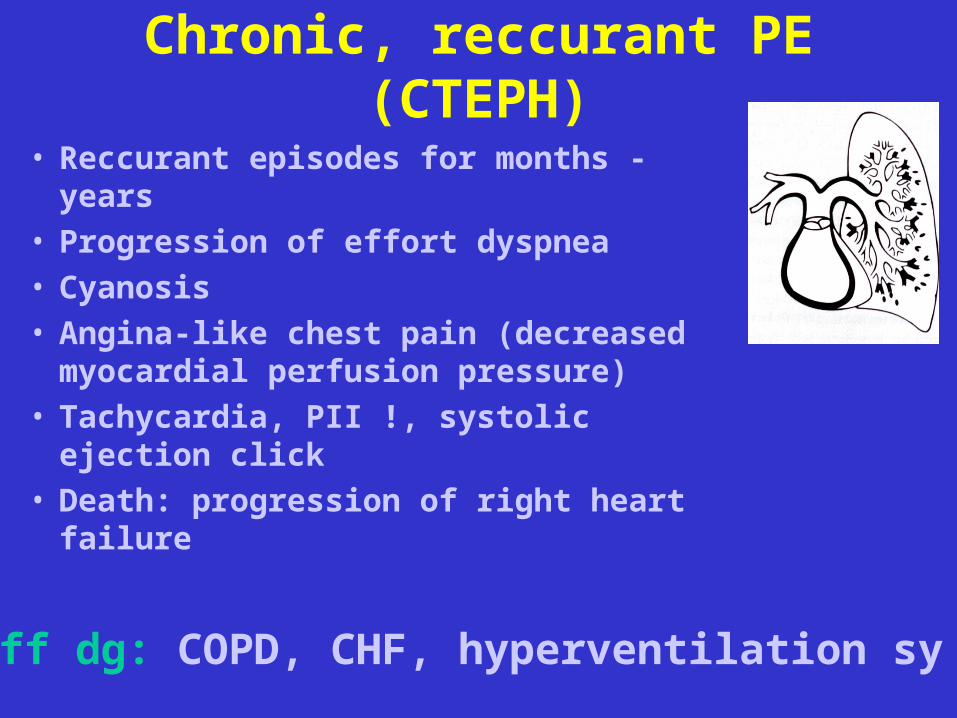
Chronic, reccurant PE (CTEPH)
• Reccurant episodes for months - years• Progression of effort dyspnea• Cyanosis• Angina-like chest pain (decreased
myocardial perfusion pressure)• Tachycardia, PII !, systolic ejection click• Death: progression of right heart failure
Diff dg: COPD, CHF, hyperventilation sy
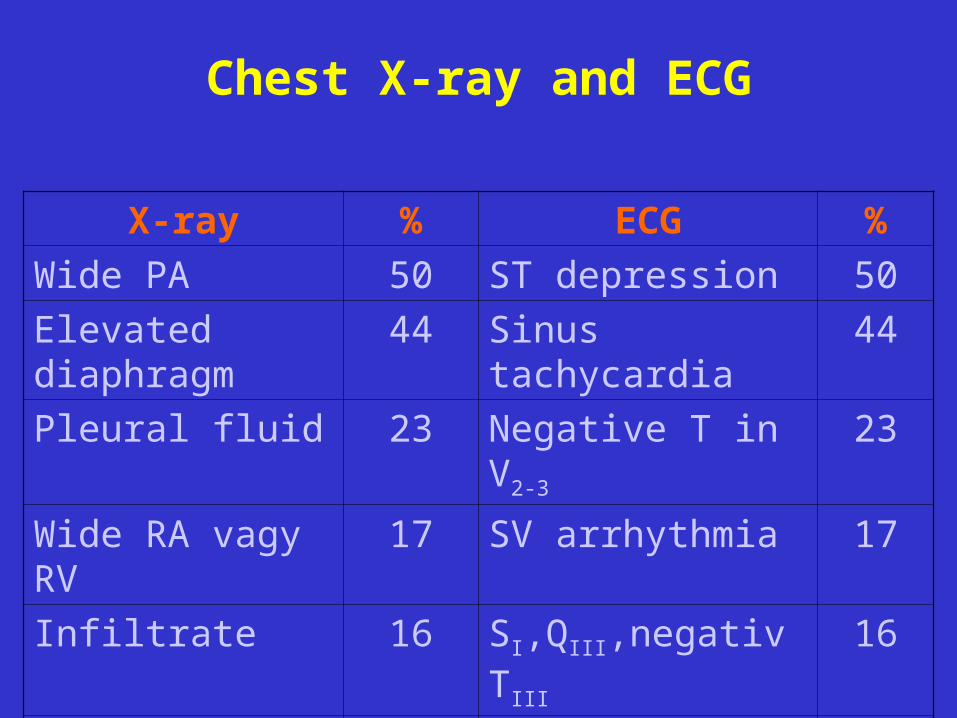
Chest X-ray and ECG
X-ray % ECG %
Wide PA 50 ST depression 50
Elevated diaphragm 44 Sinus tachycardia 44
Pleural fluid 23 Negative T in V2-3 23
Wide RA vagy RV 17 SV arrhythmia 17
Infiltrate 16 SI,QIII,negativ TIII 16
Atelectasia 13 RBBB 13
Local oligemia 6 P-pulmonale 6
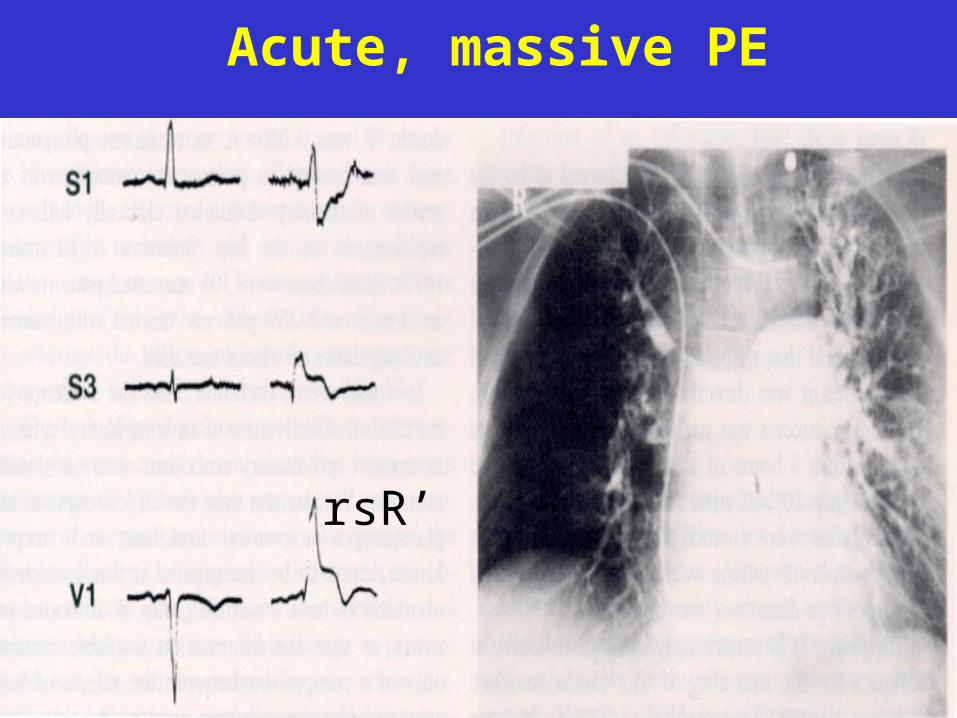
Acute, massive PE
rsR’
CTEPH
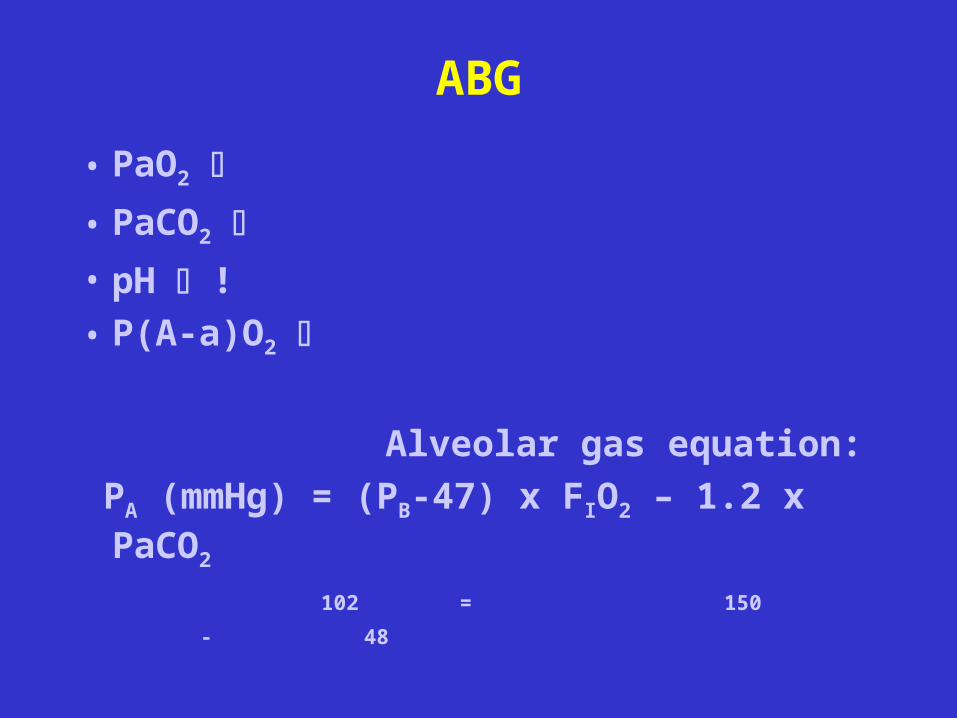
ABG
• PaO2
• PaCO2
• pH !• P(A-a)O2
Alveolar gas equation:
PA (mmHg) = (PB-47) x FIO2 – 1.2 x PaCO2
102 = 150 - 48
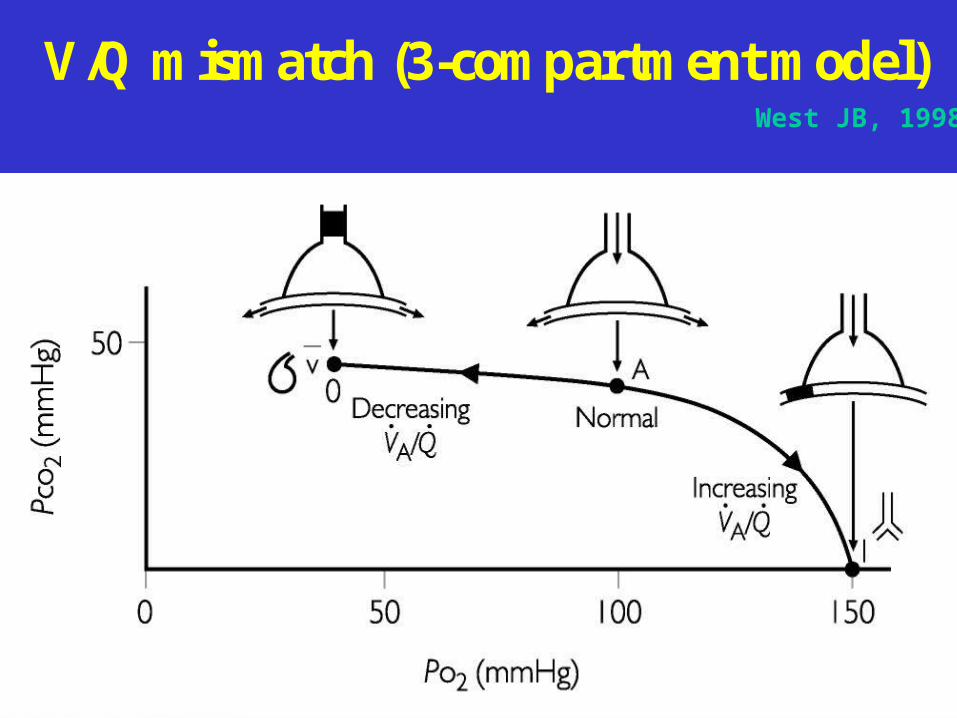
V/Q mismatch (3-compartment model)West JB, 1998
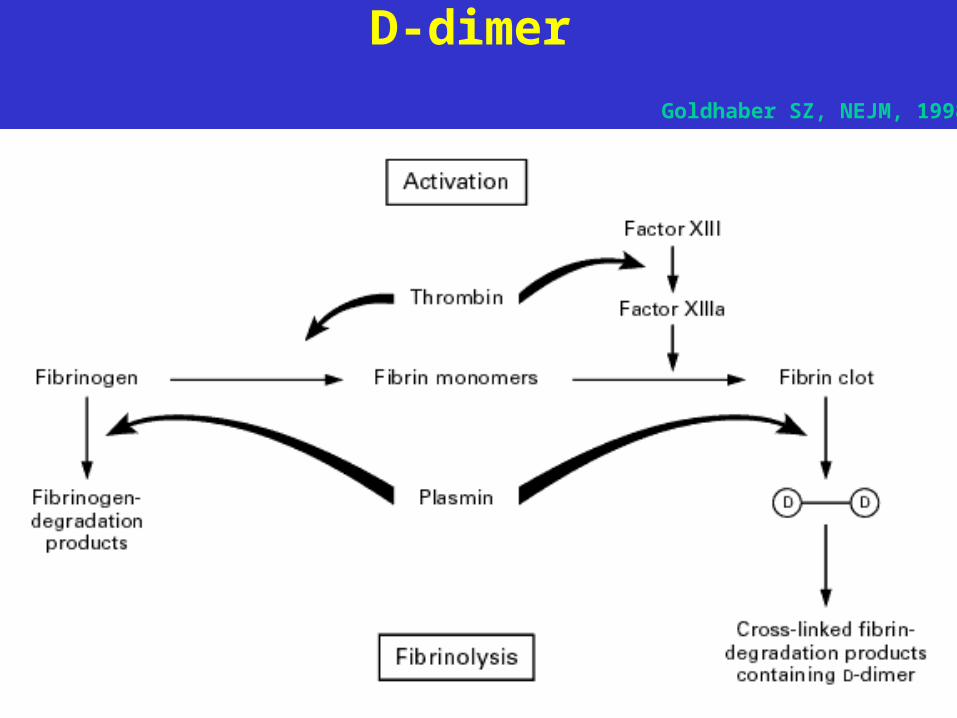
D-dimer
Goldhaber SZ, NEJM, 1998
Blood chemistry
- D-dimer (ELISA): sensitive, but not specific (AMI, pneumonia, CHF, cc, surgery)
> 500 ng/ml, in 90% of PE, (latex test 50%)
negative test: exclude PE - LDH-3 - Bi
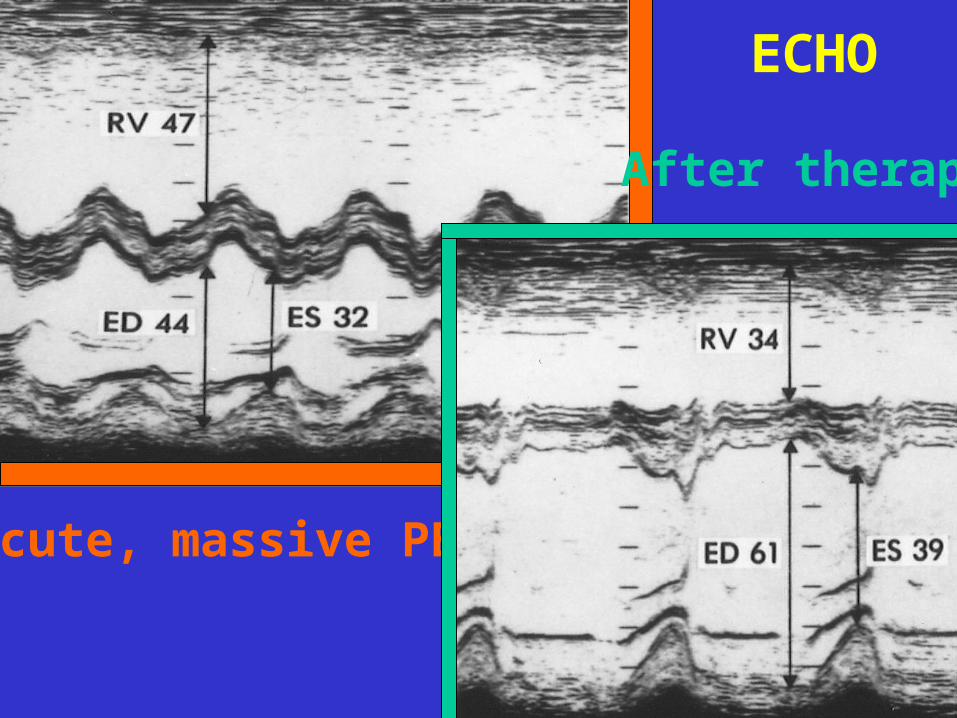
Acute, massive PE
After therapy
ECHO
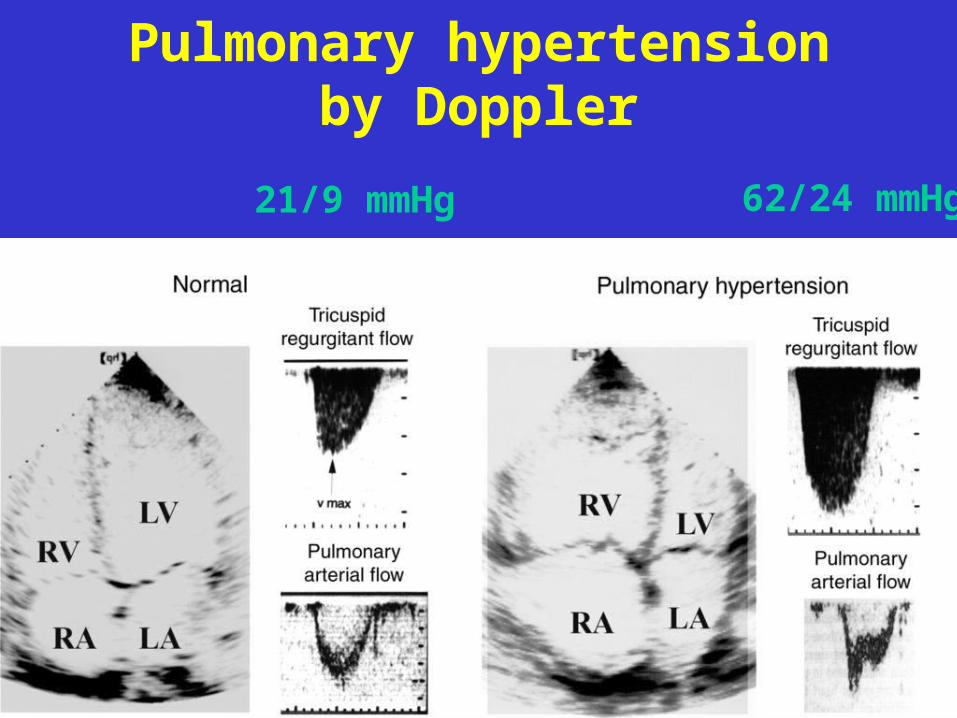
Pulmonary hypertension by Doppler
21/9 mmHg 62/24 mmHg
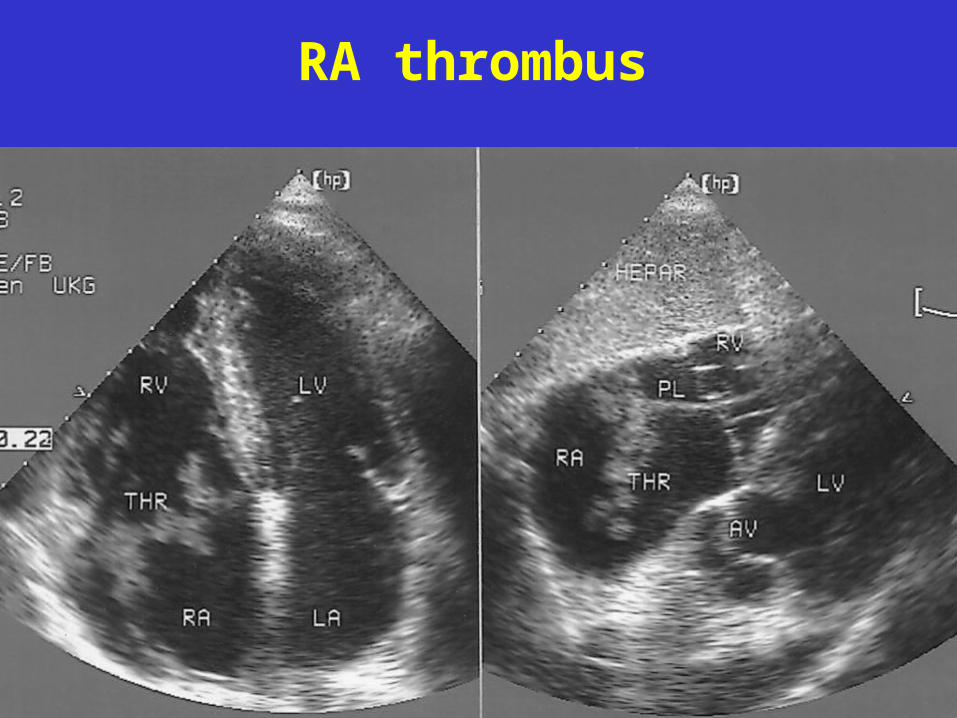
RA thrombus
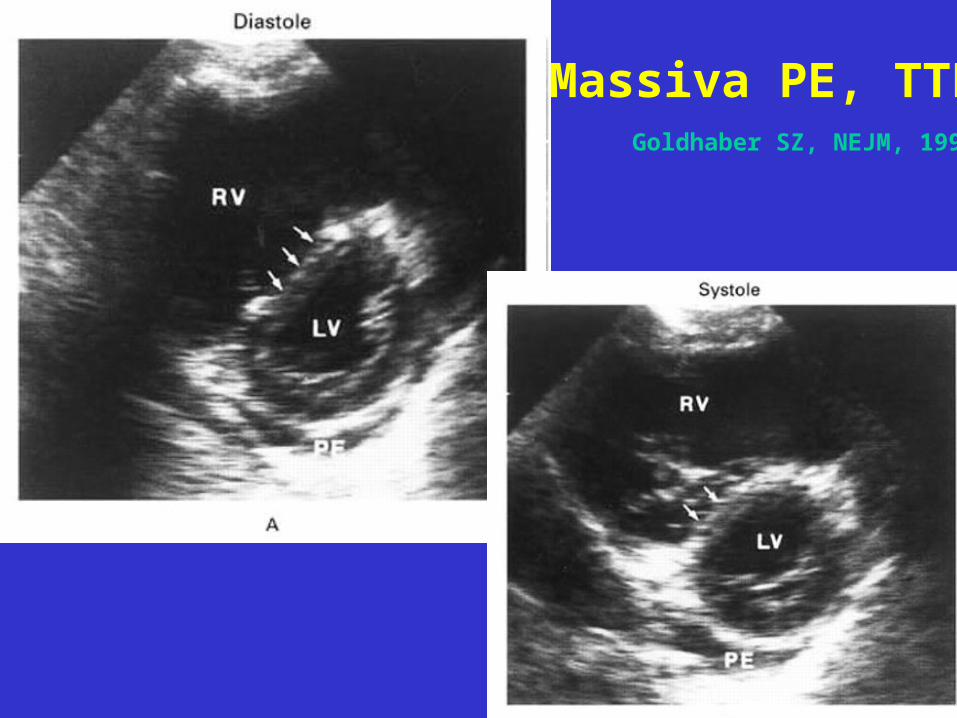
Massiva PE, TTEGoldhaber SZ, NEJM, 1998
Other diagnostic tests
• Vascular Doppler of the leg
• Inhalation-perfusion scintigraphy: V/Q mismatch
• Helical CT: central - segmental – subsegmental
• Angiography (gold standard)
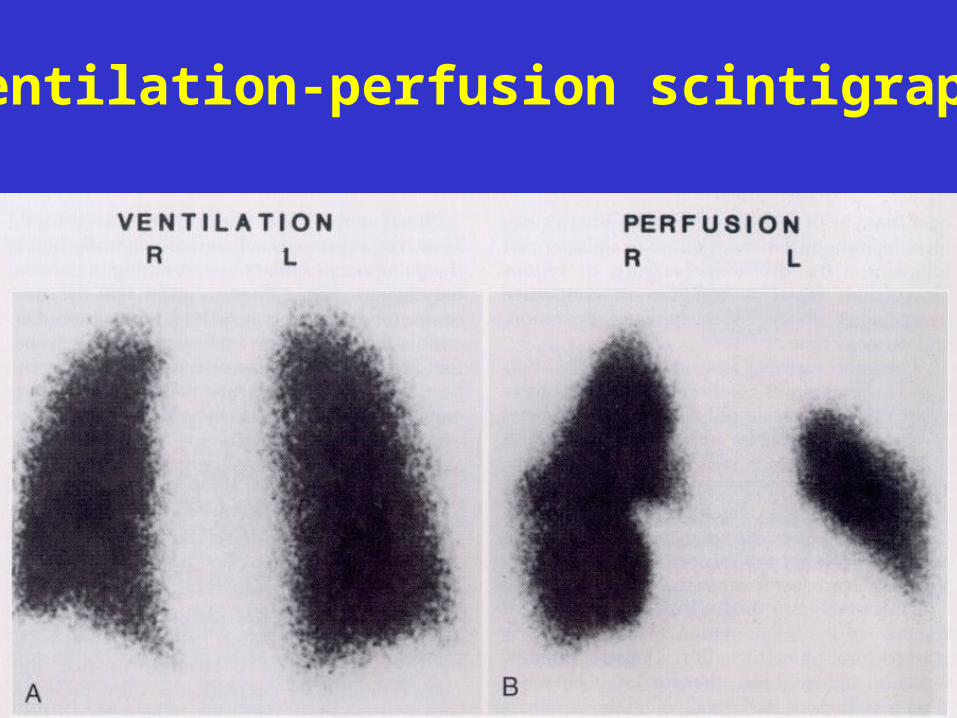
Ventilation-perfusion scintigraphy
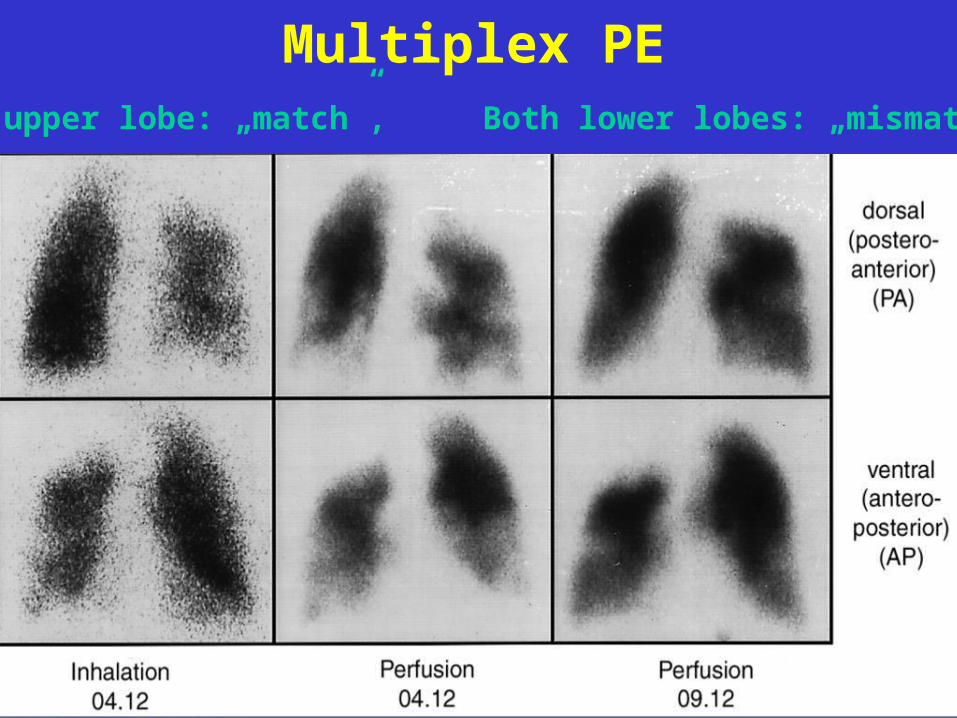
Multiplex PERight upper lobe: „match”, Both lower lobes: „mismatch”
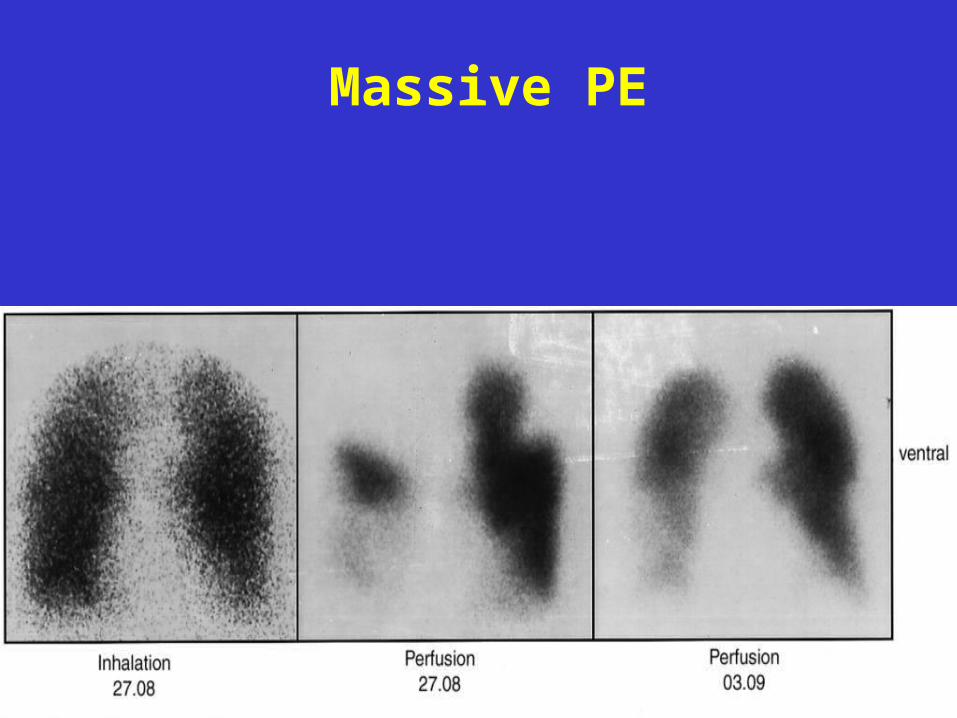
Massive PE
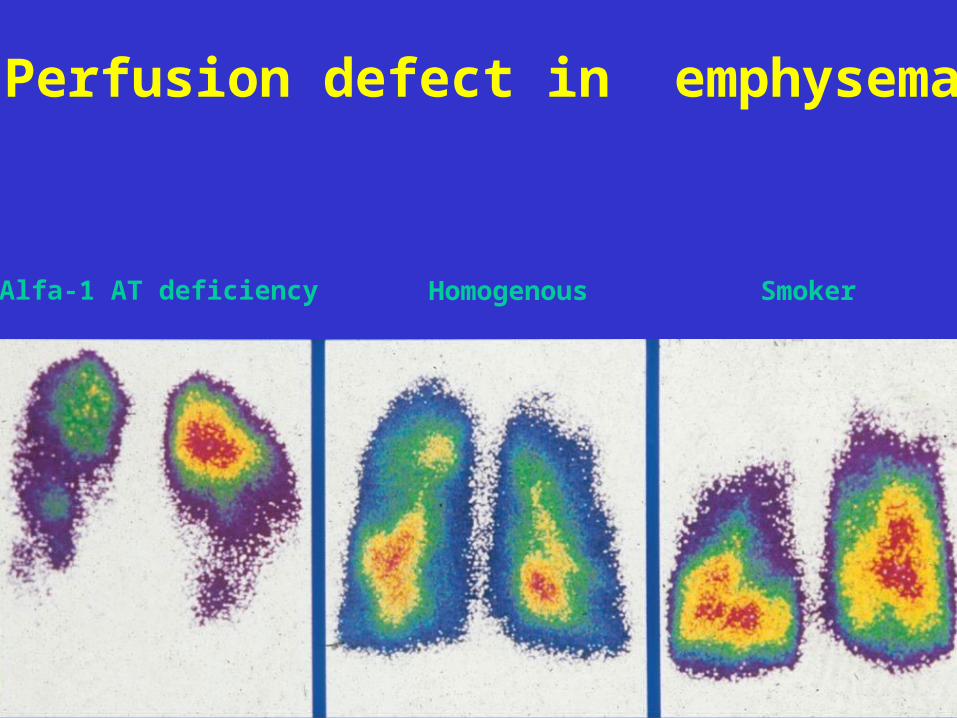
Perfusion defect in emphysema
Alfa-1 AT deficiency Homogenous Smoker
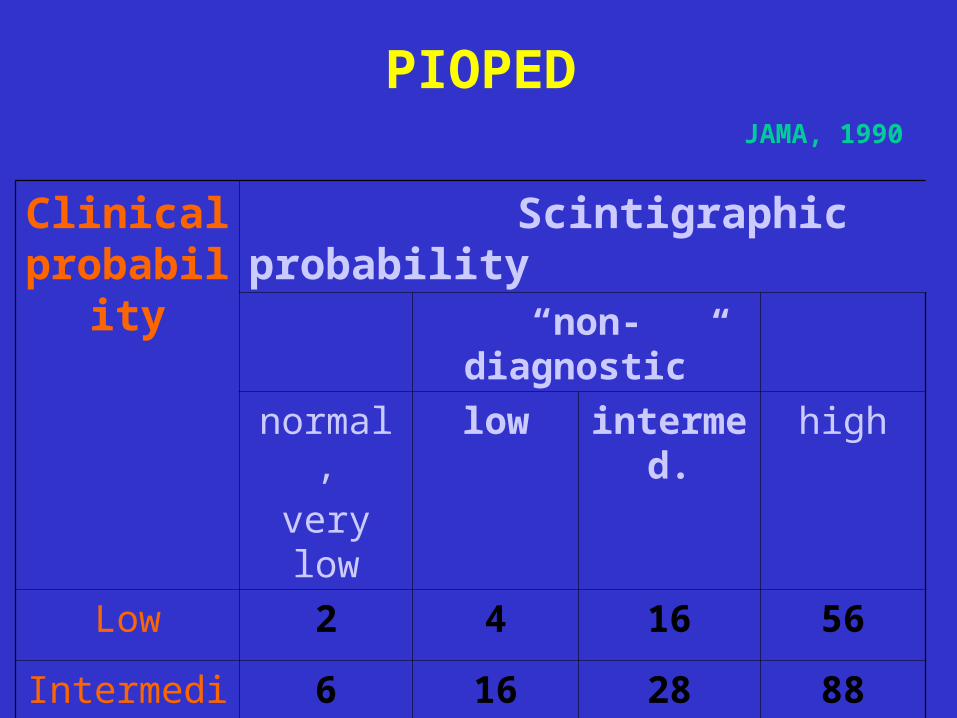
Clinical probability
Scintigraphic probability
“non-diagnostic”
normal,
very low
low intermed. high
Low 2 4 16 56
Intermedier 6 16 28 88
High 0 40 66 96
PIOPEDJAMA, 1990
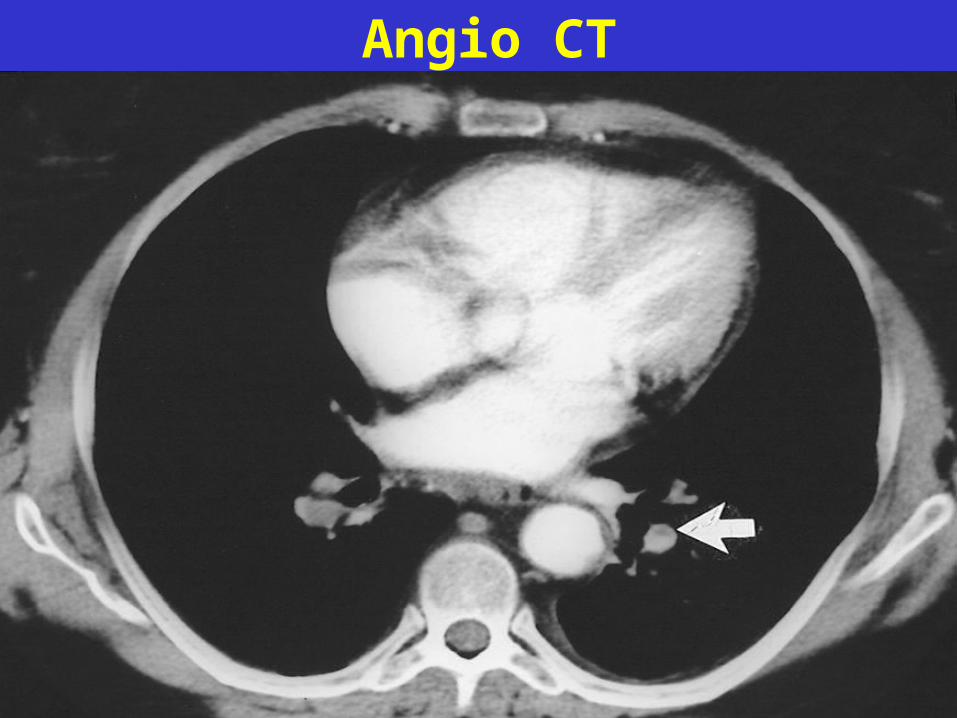
Angio CT
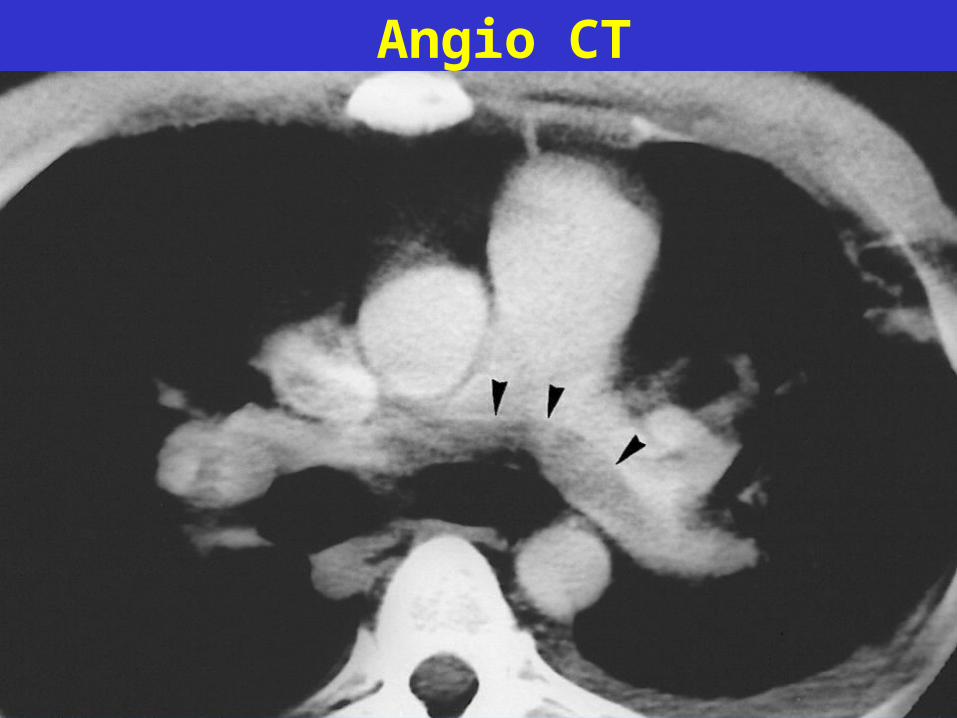
Angio CT
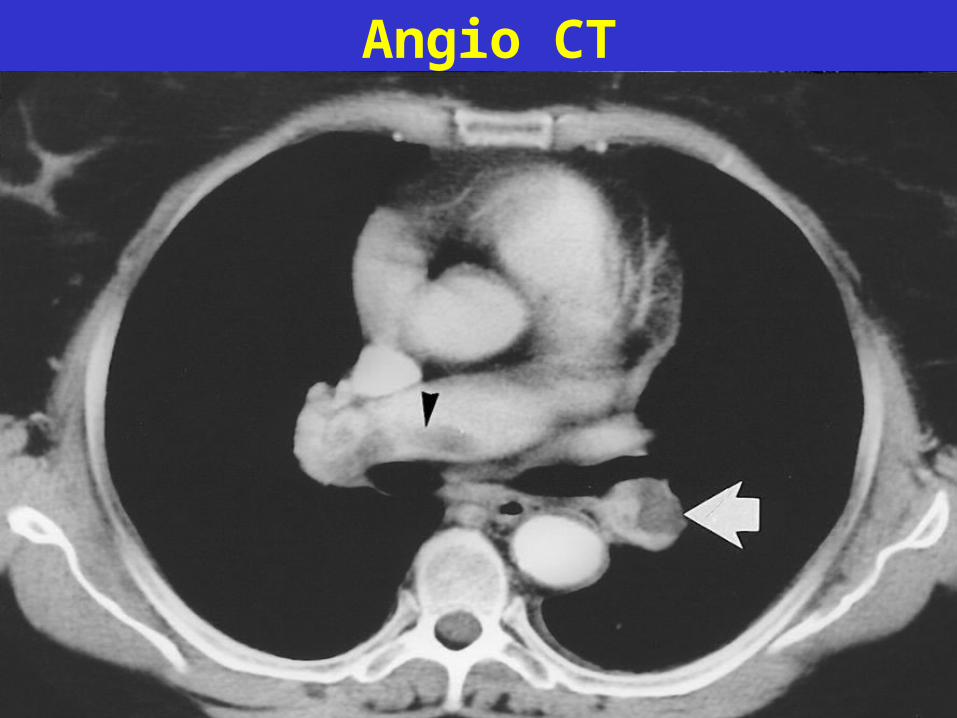
Angio CT
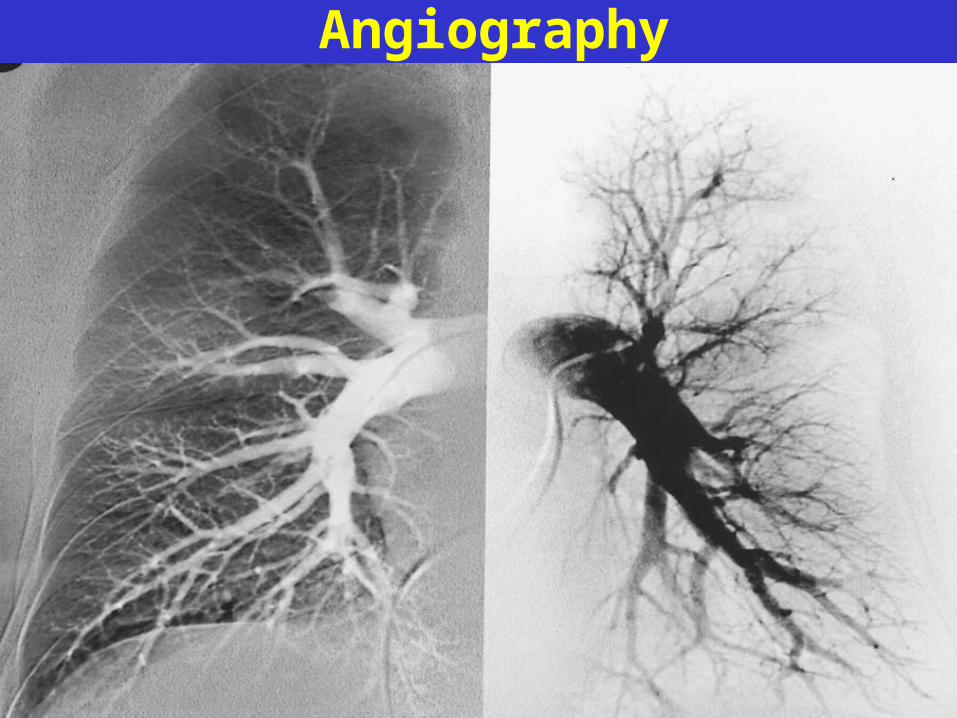
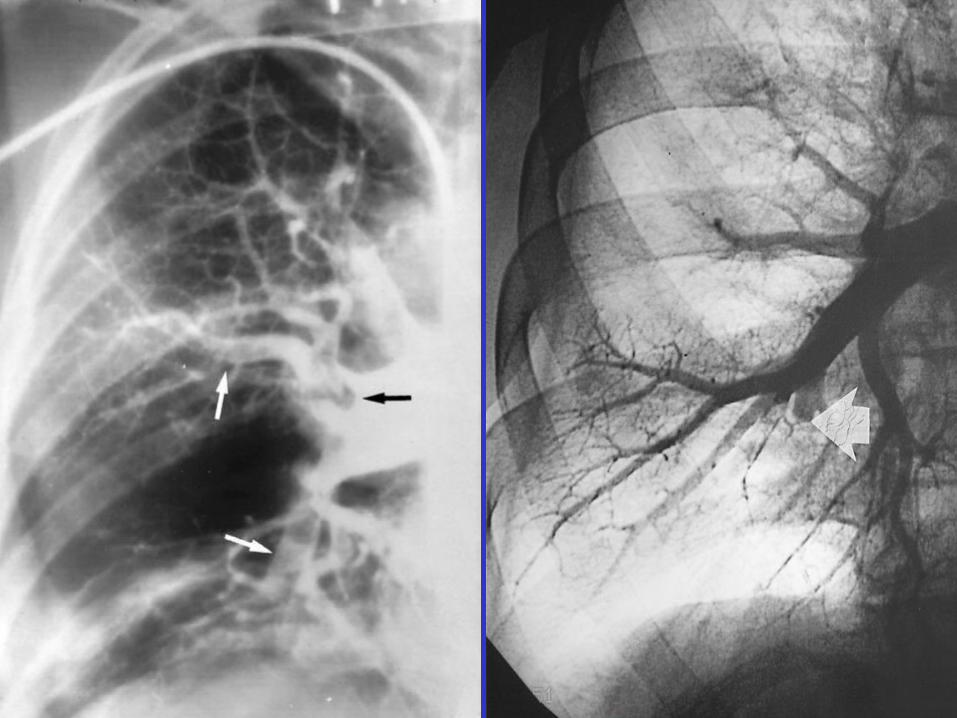
Angiography
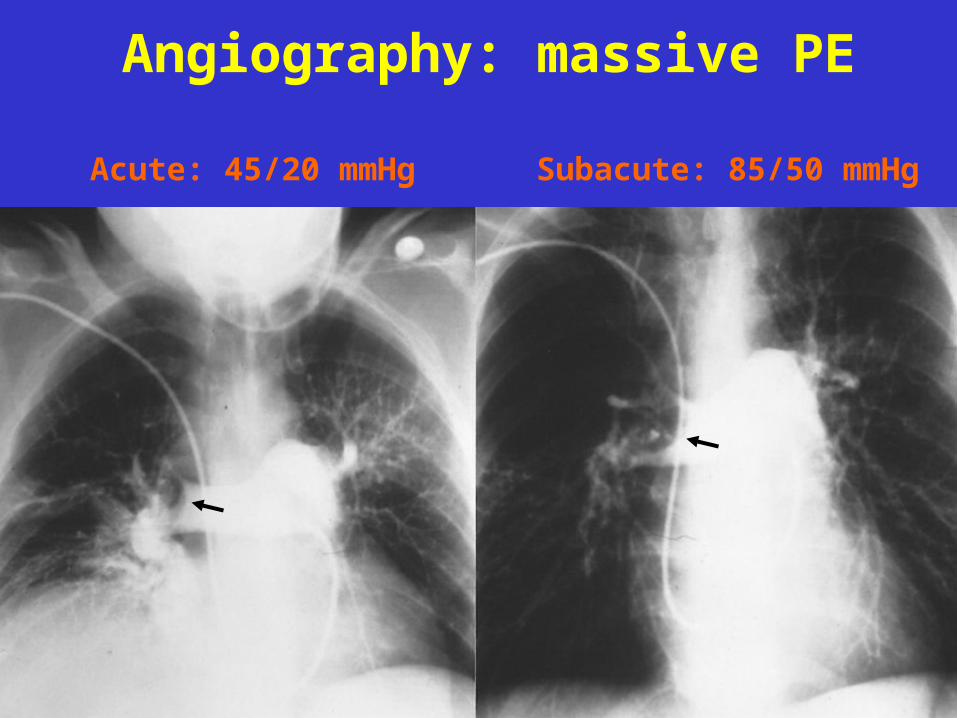
Angiography: massive PE
Acute: 45/20 mmHg Subacute: 85/50 mmHg

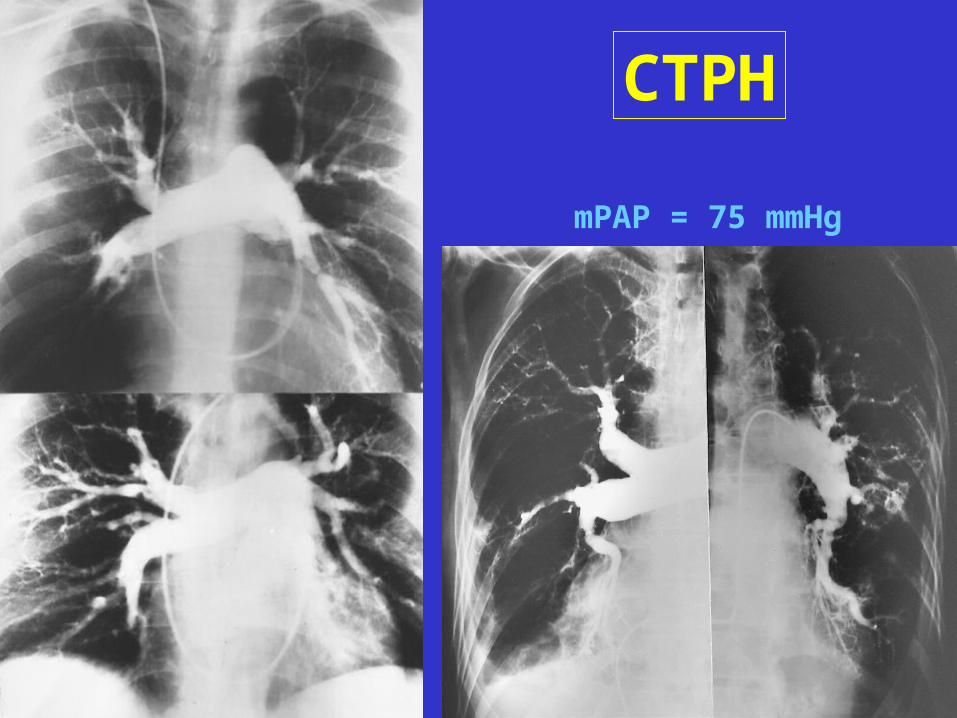
CTPH
mPAP = 75 mmHg
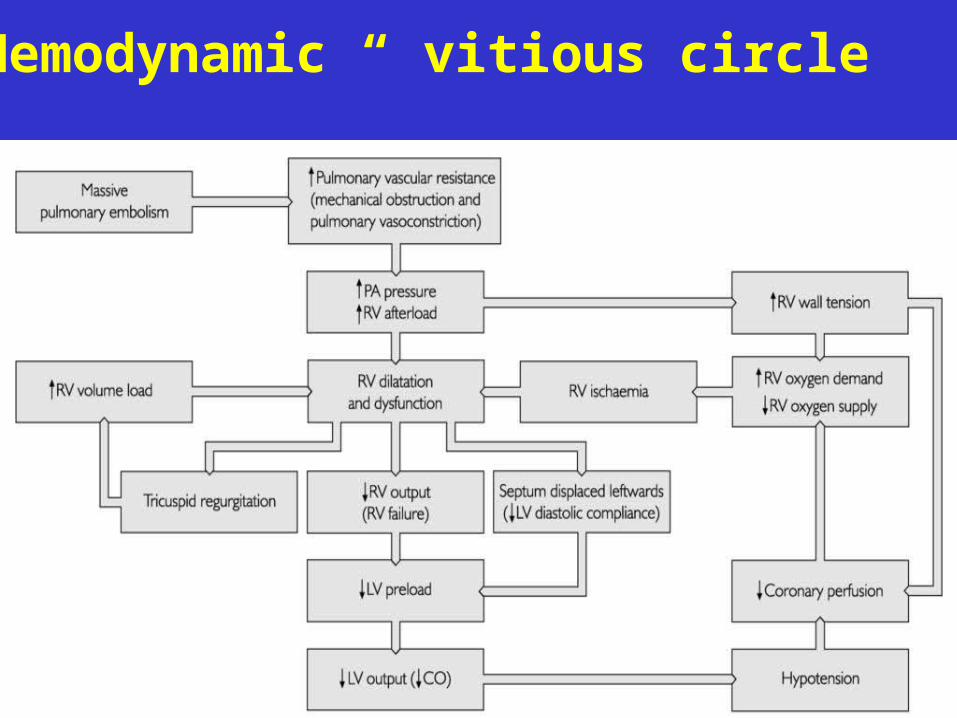
Hemodynamic “ vitious circle”
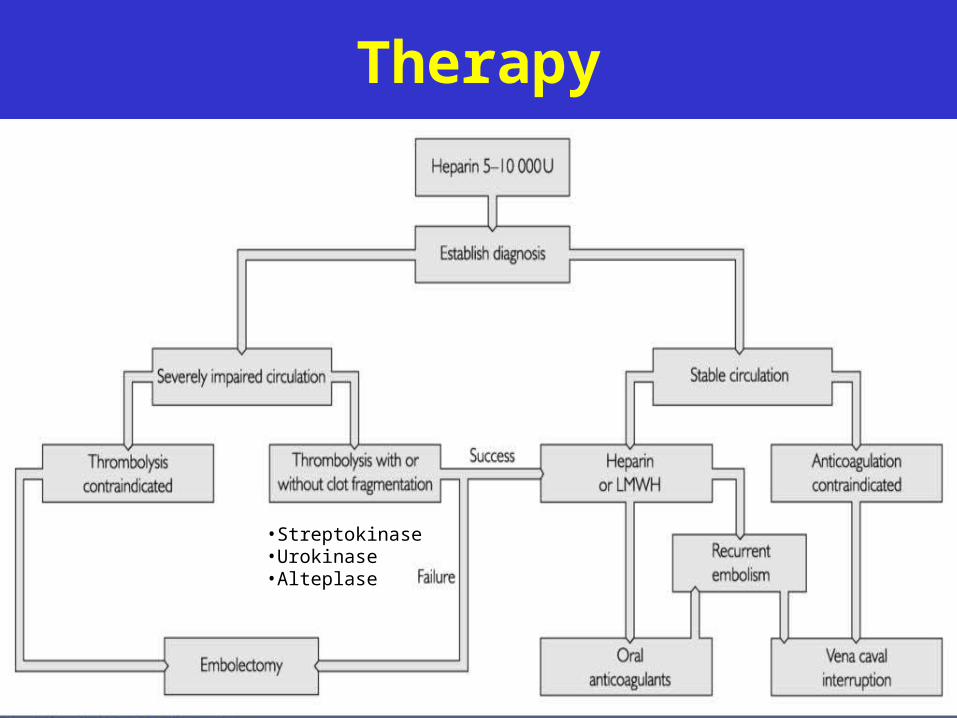
Therapy
•Streptokinase•Urokinase•Alteplase
Treatment
• Sodium-heparin iv. bolus (5-10 000 U) followed by either- continouos infusion or- low molecular weight (ultrafractionated) heparin (LMWH) s.c.
• Coumarin for 6-12 months (if irreversible or unknown etiology: lifeterm anticoagulation)
therapeutic level: INR: 2-3
• Ximelagatran, Dabigatran (and some more novel oral direct thrombin or Xa f. inhibitors), for long-term prevention of VTE, no need to monitor coagulation
New therapy
• Oral thrombin inhibitor - dabigatran (Pradaxa)• Xa inhibitor - rivaroxaban (Xarelto)• No need to control coagulability• Side effect: bleeding• Disadvantage: no antidotum, expansive
Rare forms of PE
• Fat (trauma, surgery - diffuse alveolar infiltrates)
• Septic (osteomyelitis, tricuspid valve endocarditis)
• Air (canulla insertion, gynecological intervention)
• Amniotic fluid (delivery)
Etiology of chronic cor pulmonale
• Airway or parenchymal disease
• Alveolar hypoventilation
• Pulmonary vascular disease (arteria, vena – pulmonary veno-occlusive disease)
• Mediastinal compression (tumor, aneurysm)
• Chest deformity (e.g. kiphoscoliosis)
Classification of PAH • Postcapillary
- LV systolic or diastolic dysfunction
- pericardial constriction- LA disease (MS, MI, thrombus), veno-occlusive disease
• Precapillary- iPAH
- airway or parenchyma disease (COPD, fibrosis, collagen diseases, cancer, resection)- embolism- vasculitis (Wegener, Churg-Strauss sy, CREST-sy, SLE, PN)- Eisenmenger-sy- Alveolar hypoventilation (chest deformity, pleural callus, SAS, neuromuscular diseases)- other (pulmonal stenosis, high altitude, hemoglobinopathies)
Treatment of CCP
• Treatment of primer disease• Oxygen supplementation• Diuretics, vasodilators with caution – preload !• New vasodilators for iPAH (PD-5 inhibitors,
Pg analogs, endothelin antagonists)• Venesection, in case of polyglobulia• Anticoagulation