Embed Size (px)
Citation preview
Pulmonary Embolism & DVT
Introduction• Pathophysiology
• Risk Factors
• Symptoms
• Lab Findings
• Radiology Findings
• Treatment
• Prevention
PathophysiologyDislodgement of a blood clot:
• Lower Extremities: 65% to 90%
• Pelvic venous system
• Renal venous system
• Upper Extremity
• Right Heart
Risk Factors for PE and DVT
• Immobilization• Surgery within the last 3
months• Stroke• History of venous
thromboembolism• Malignancy• Preexisting respiratory disease• Chronic Heart Disease• Age >60• Surgery requiring >30mins of
anesthesia
• Recent travel (past 2weeks, >4 hours)
• Varicose veins• Superficial vein thrombosis• Central VV
catheter/port/pacemakerAdditional RF in Women:• Obesity BMI >/=29• Heavy smoking
(>25cigs/day)• Hypertension• Pregnancy
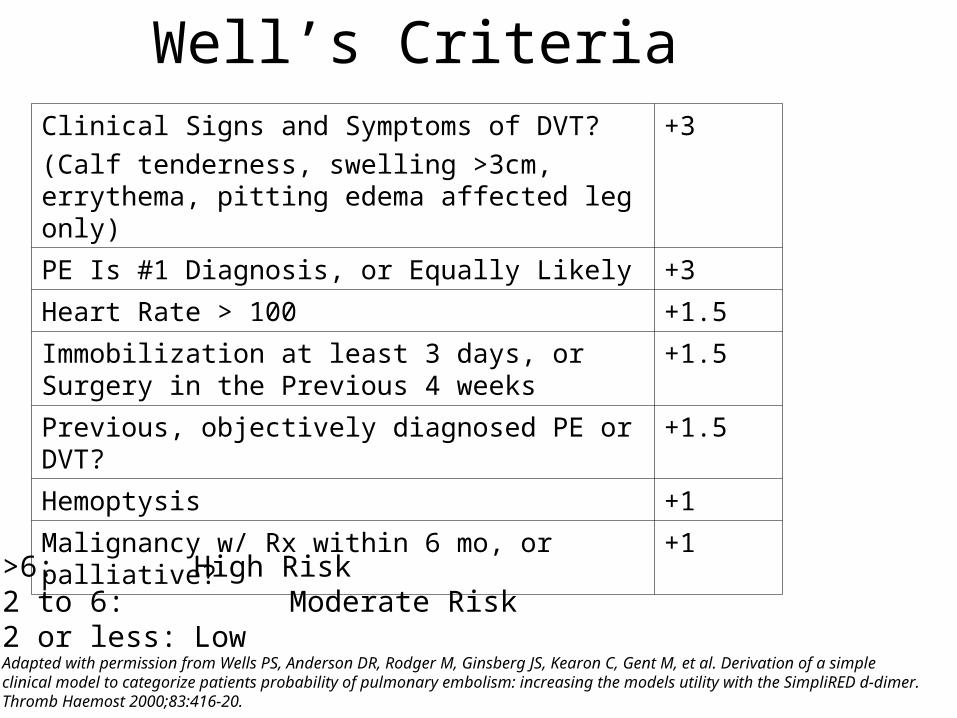
Well’s CriteriaClinical Signs and Symptoms of DVT?
(Calf tenderness, swelling >3cm, errythema, pitting edema affected leg only)
+3
PE Is #1 Diagnosis, or Equally Likely +3
Heart Rate > 100 +1.5
Immobilization at least 3 days, or Surgery in the Previous 4 weeks
+1.5
Previous, objectively diagnosed PE or DVT? +1.5
Hemoptysis +1
Malignancy w/ Rx within 6 mo, or palliative? +1
>6: High Risk2 to 6: Moderate Risk2 or less: LowAdapted with permission from Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED d-dimer.Thromb Haemost 2000;83:416-20.
P.E. and Malignancy
• A Presenting sign in: – Pancreatic cancer– Prostate cancer
• Late sign in:– Breast cancer– Lung cancer– Uterine cancer– Brain cancer
Symptoms of P.E.• Dyspnea
• Pleuritic pain
• Cough
• Hemoptysis (blood tinged/streaked/ pure blood)
Signs of P.E.
• Tachypnea• Rales• Tachycardia• Hypoxia• S4• Accentuated pulmonic component of S2• Fever: T <102 F
Signs in Massive P.E.• “Massive PE”: hemodynamic instability
with SBP <90 or a drop in baseline SBP by >/=40mmHg
• Signs as before PLUS:– Acute right heart failure
• Elevated J.V.P.• Right-sided S3• Parasternal lift
P.E. & Leg Symptoms• Most patients with P.E. do not have leg
symptoms at time of diagnosis
• Patients with leg symptoms may have asymptomatic P.E.
Lab & Radiologic Findings in P.E.
• ABG• BNP• Cardiac Enzymes: Troponin• D-dimer• EKG• CXR• Ultrasound• V/Q Scan• Angiography
Lab Findings in P.E.(ABG)
• ABG:– Hypoxemia– Hypocapnia (low CO2)– Respiratory Alkalosis– Massive PE: hypercapnia, mix resp and metabolic
acidosis (inc lactic acid)– Patients with RA pulse ox readings <95% are at
increased risk of in-hospital complications, resp failure, cardiogenic shock, death
Lab Findings in P.E. (BNP)
• BNP (beta natruretic peptide)– Insensitive test– Patient’s with PE have higher levels than pts without,
but not ALL patients with PE have high BNP– Good prognostic value measure: if BNP >90
associated with adverse clinical outcomes (death, CPR, mechanical vent, pressure support, thrombolysis, embolectomy)
Lab Findings in P.E. (Troponin)
• Troponin– High in 30-50% of pts with mod to large PE– Prognostic value if combined pro-NT BNP
• Trop I >0.07 + NT-proBNP >600 = high 40 day mortality
Lab Findings in P.E. (D-dimer)
• D-dimer:– Degredation product of fibrin– >500 is abnormal– Sensitivity: High, 95% of PE pts will be
positive– Specificity: Low– Negative Predictive Value: Excellent
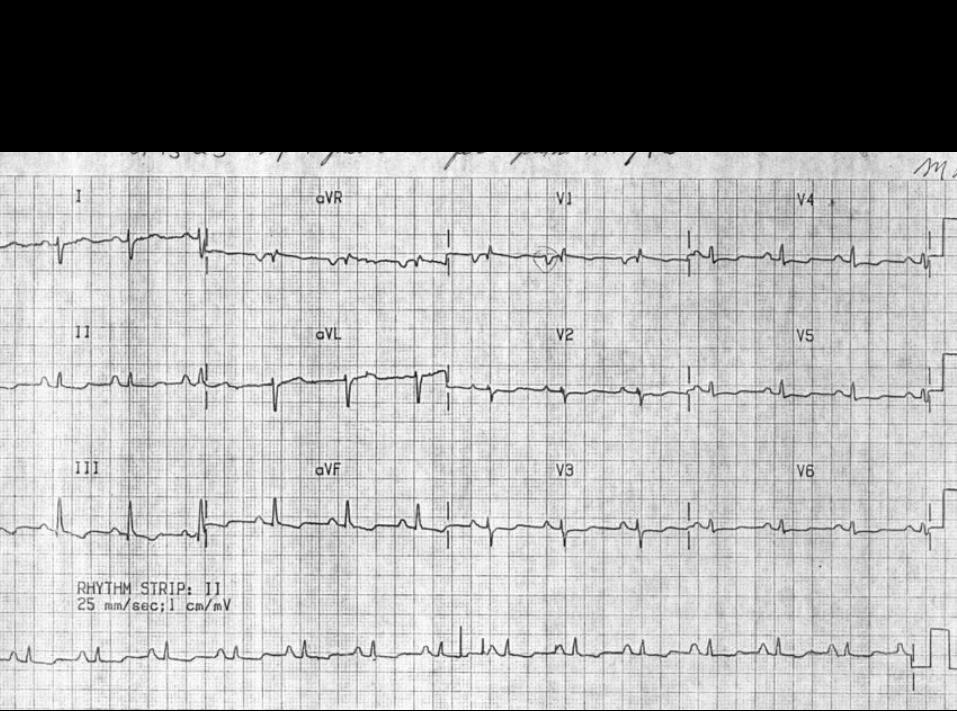
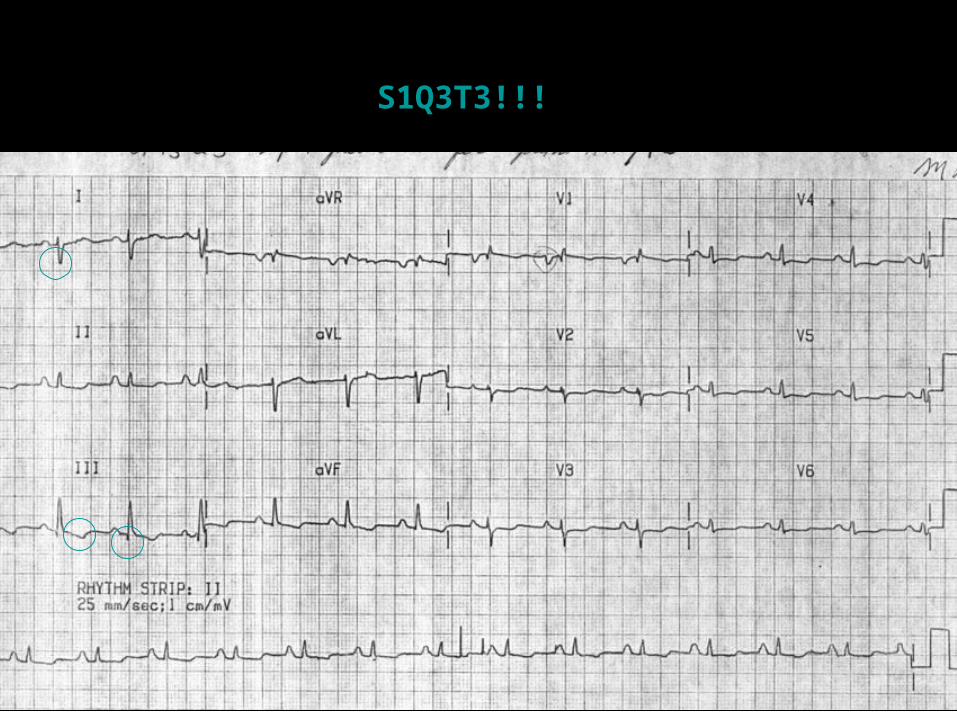
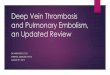
S1Q3T3!!!
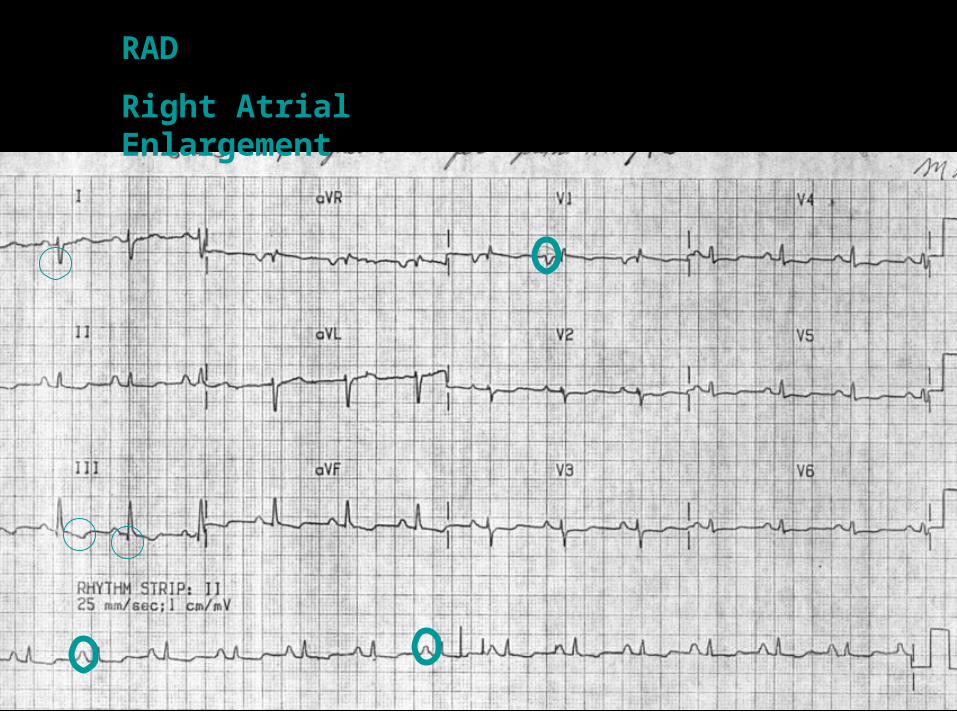
RAD
Right Atrial Enlargement
Lab Findings in P.E. (cont’d)
• EKG– 2 Most Common finding on EKG:
• Nonspecific ST-segment and T-wave changes• Sinus Tachycardia
– Historical abnormality suggestive of PE• S1Q3T3• Right ventricular strain• New incomplete RBBB
Radiologic Findings in P.E.
GOLD STANDARD IN DIAGNOSING PULMONARY
EMBOLISM?
PULMONARY ANGIOGRAM
Radiology Findings in P.E. (cont’d)
• CXR:– Normal– Atelectasis and/or pulmonary parenchymal
abnormality– Pleural Effusion– Cardiomegally
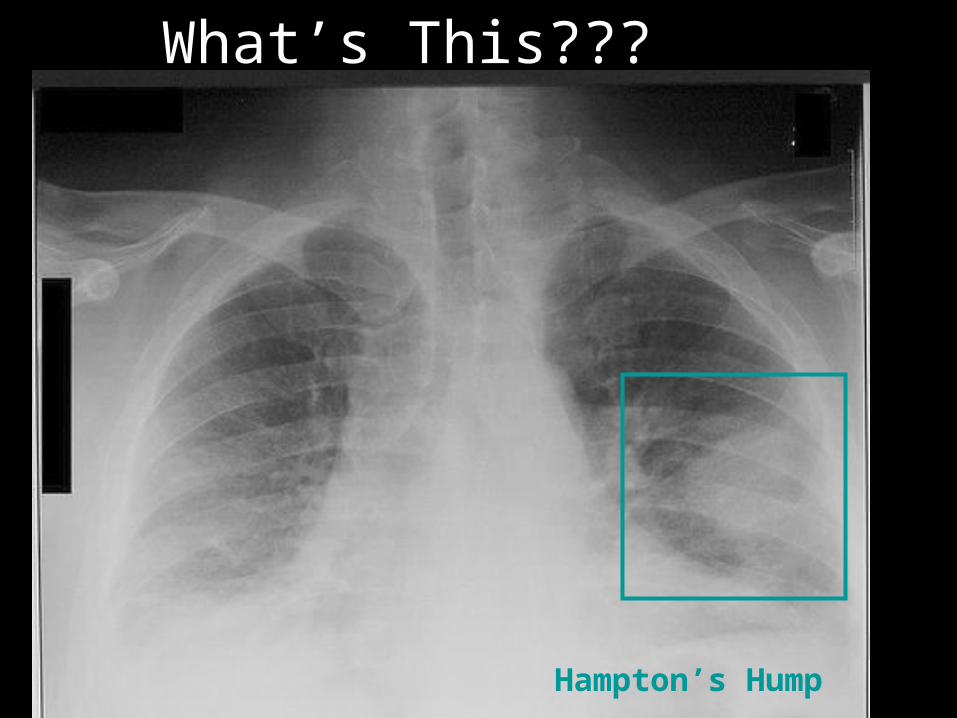
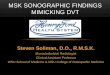
What’s This???
Hampton’s Hump
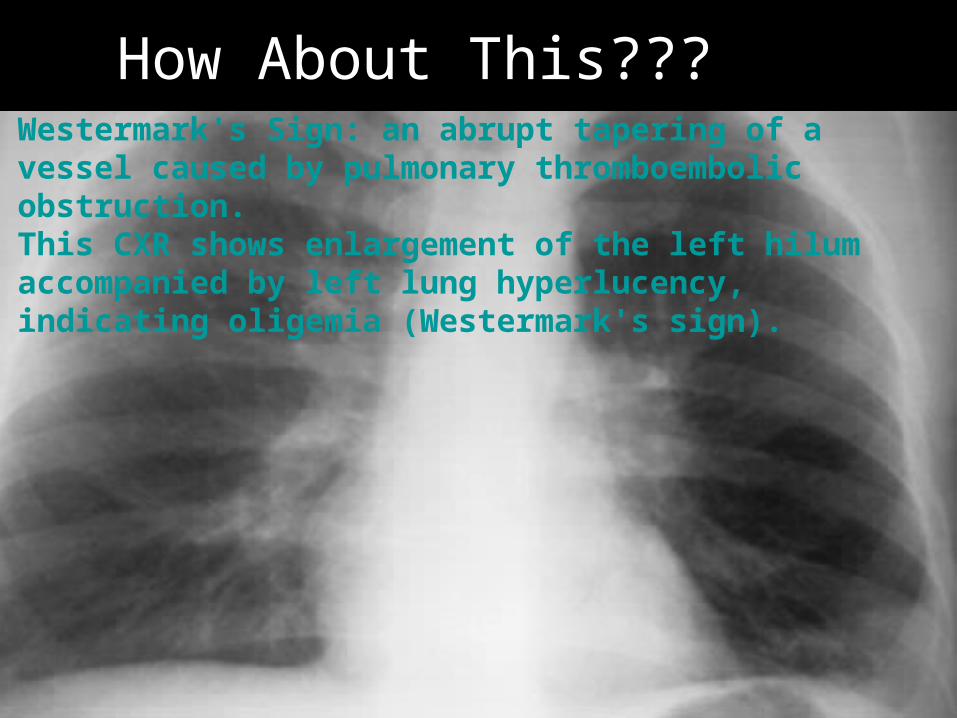
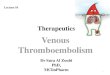
How About This???Westermark's Sign: an abrupt tapering of a vessel caused by pulmonary thromboembolic obstruction. This CXR shows enlargement of the left hilum accompanied by left lung hyperlucency, indicating oligemia (Westermark's sign).
Radiology Findings in P.E. (cont’d)V/Q Scan:
• Results: High, Intermediate, Low Probability• Best if combined with Clinical Probability
(PIOPED study):– High Clinical Prob + High Prob VQ= 95% likelihood
of having a P.E.– Low Clinical Prob + Low Prob VQ= 4% likelihood of
having a P.E.
Radiology Findings in P.E. (cont’d)
Lower Extremity Ultrasounds
• If DVT found then treatment is same if patient has a P.E.
• Disadvantage: – If negative, patients with PE may be missed– If false positive (3%), unnecessary
intervention
Radiology Findings in P.E. (cont’d)
CT Pulmonary Angiography (CT-PA)
• Widely used
• Institution dependent
• Sensitivity (83%)
• Specificity (96%): if negative, very low likelihood that pt has P.E.
Radiology Findings in P.E. (cont’d)
Pulmonary Angiogram
• Gold Standard
• Not easily accessible
• Radiologist dependent
Radiology Findings in P.E. (cont’d)
Echocardiogram• Increased Right Ventricle Size• Decreased Right Ventricular Function• Tricuspid Regurgitation
Rarely:• RV thrombus• Regional wall motion abnormalities that spare
the right ventricle apex (McConnell’s Sign)
Hypercoagulability Work Up
• No consensus on who to test• Increased likelihood if:
– Age <50y/o without immediate identifiable risk factors (idiopathic or provoked)
– Family history– Recurrent clots– If clot is in an unusual site (portal, hepatic, mesenteric,
cerebral)– Unprovoked upper extremity clot (no catheter, no
surgeries)– Patient’s with warfarin induced skin necrosis (they may
have protein C deficiency
Hypercoagulability Work Up
– Protein C/S deficiency– Factor V leiden deficiency– AntiThrombin III deficiency– Prothrombin 20210 mutation– Antiphospholipid antibody– High Homocysteine
Most Common Cause of Congenital Hypercoagulablity
• Protein C resistance d/t Factor V leiden mutation
Treatment of P.E.
• Respiratory Support: Oxygen, intubation
• Hemodynamic Support: IVF, vasopressors
• Anticoagulation
• Thrombolysis
• IVC Filter
Anticoagulation• Start during resuscitation phase itself• If suspicion high, start emperic anticoagulation • Evaluate patient for absolute contraindication
(i.e.: active bleeding)
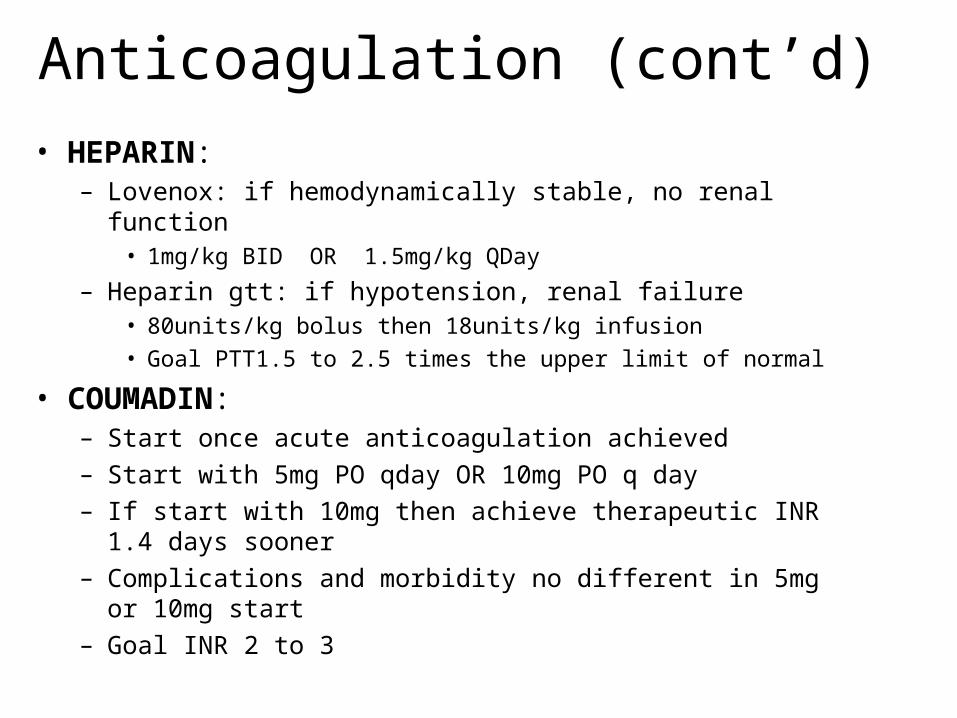
Anticoagulation (cont’d)
• HEPARIN:– Lovenox: if hemodynamically stable, no renal function
• 1mg/kg BID OR 1.5mg/kg QDay
– Heparin gtt: if hypotension, renal failure• 80units/kg bolus then 18units/kg infusion
• Goal PTT1.5 to 2.5 times the upper limit of normal
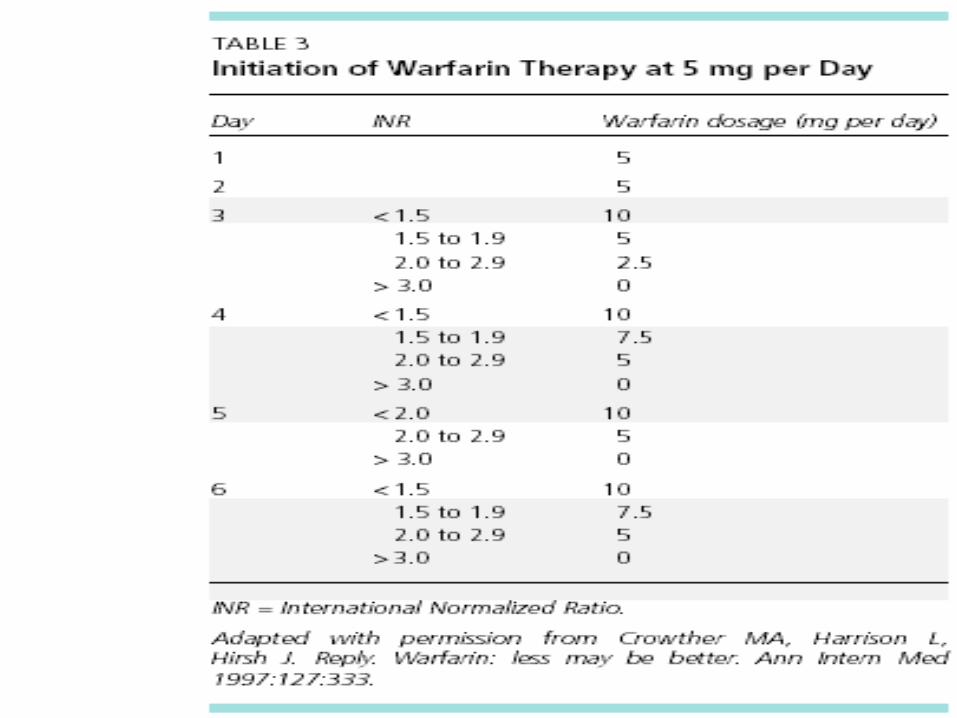
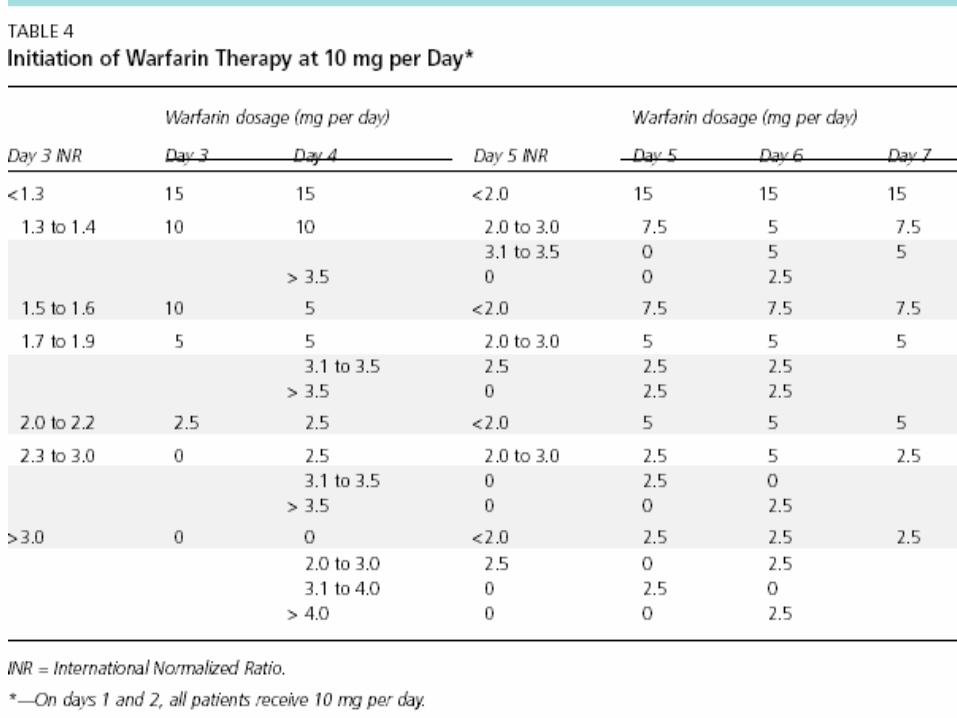
• COUMADIN:– Start once acute anticoagulation achieved– Start with 5mg PO qday OR 10mg PO q day– If start with 10mg then achieve therapeutic INR 1.4 days
sooner– Complications and morbidity no different in 5mg or 10mg
start – Goal INR 2 to 3
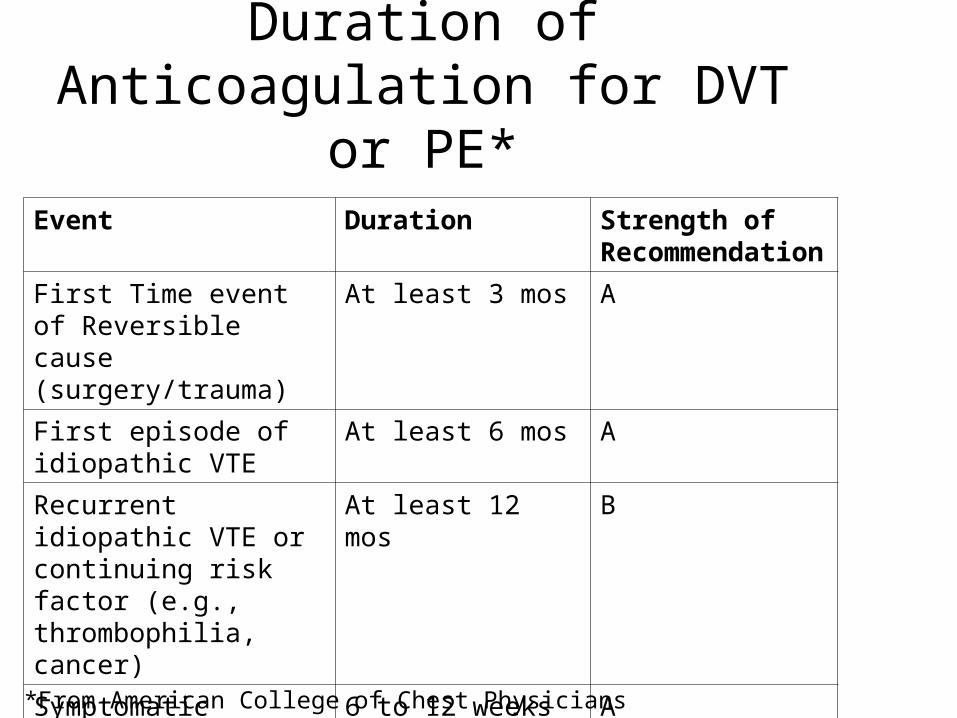
Duration of Anticoagulation for DVT or PE*
Event Duration Strength of Recommendation
First Time event of Reversible cause (surgery/trauma)
At least 3 mos A
First episode of idiopathic VTE
At least 6 mos A
Recurrent idiopathic VTE or continuing risk factor (e.g., thrombophilia, cancer)
At least 12 mos B
Symptomatic isolated calf-vein thrombosis
6 to 12 weeks A
*From American College of Chest Physicians
Thrombolysis• Considered once P.E. diagnosed• If chosen, hold anticoagulation during
thrombolysis infusion, then resumed• Associated with higher incidence of major
hemorrhage • Indications: persistent hypotension, severe
hypoxemia, large perfusion defecs, right ventricular dysfunction, free floating right ventricular thrombus, paten foramen ovale
• Activase or streptokinase
IVC Filter
• Indication: – Absolute contraindication to anticoagulation (i.e.
active bleeding)– Recurrent PE during adequate anticoagulation– Complication of anticoagulation (severe bleeding)
• Also: – Pts with poor cardiopulmonary reserve– Recurrent P.E. will be fatal– Patient’s who have had embolectomy– Prophylaxis against P.E. in select patients
(malignancy)
Embolectomy • Surgical or catheter
• Indication:– Those who present severe enough to warrant
thrombolysis – In those where thrombolysis is
contraindicated or fails
Questions?