Embed Size (px)
Citation preview

4/25/2016
1
John R. Bartholomew, MD, FACC, MSVM
Professor of Medicine – Cleveland Clinic Lerner College of Medicine
Section Head – Vascular Medicine
Department of Cardiovascular Medicine
Pulmonary Embolism
A Team Approach to Diagnosis and Management
Disclosure Slide
Consultant - Portola Pharmaceuticals Consultant - Boehringer Ingelheim
Consultant - Daiichi Sankyo Research - Siemens
Burden of Venous Thromboembolism
Am Journal of Therapeutics 2009;16: 300-303
Death
Pulmonary hypertension
Pulmonary embolism
Post-thrombotic syndrome
Symptomatic DVT
Asymptomatic DVT
Circulation 2015;131:e29-e322 © 2015 by the American College of Cardiology Foundation and the American Heart Association, Inc. . Published by American Heart Association.
2
PE is the 3rd Leading Cause of CV Death
AHA - 2015 Statistics
PE
Stroke
MI
Venous Thromboembolism The Incidence is Increasing
• MI: # 1 - rate is trending downward
• Stroke: #2 - rate has plateaued
• PE/DVT: #3 - rate is increasing in men and women
Am J Med 2014;127:829-839
Management of Acute Pulmonary Embolism
Risk Stratification

4/25/2016
2
Classification of Acute PE Risk Stratification
Massive PE (~5%) • Hypotension (< 90 mmHg), syncope, cardiac arrest
• Respiratory failure
• Often fatal if more aggressive treatment not initiated
Submassive PE (~25%) • Normotensive
• RV dysfunction
• Increased risk of adverse outcomes
Low Risk PE (~70%) • Normotensive
• Normal RV function
• Excellent prognosis with anticoagulation alone
Lancet 1999;353:138 Circulation 2011; 123: 1788-1830 Circulation 2013; 127: 2458-2464
Most Patients with PE do well, but some do not!
Chest 2002;122:1801-1817
Thromb Haemost 2008;100(5):747-751 Imaging Insights 2011;2:705-715
Predictors of Mortality from PE and their Influence on Clinical Management
Treatment Options for Acute Pulmonary Embolism • Monotherapy: Heparin, LMWH, Fondaparinux,
Rivaroxaban, Apixaban • Transition Therapy: Dabigatran, Edoxaban, Warfarin • Thrombolytic Therapy (including catheter directed) • IVC filter • Surgery/interventional approaches
CHEST 2016;149(2):313-352
Am J Med 2012; 125: 465-470
• Data from 1999 to 2008
• 2,110,320 patients discharged from short stay hospital in US with a diagnosis of PE
• 72,230 (3.4%) were unstable (in shock or ventilator dependent)
Data from Nationwide Inpatient Sample
Thrombolytic therapy in unstable patients with acute PE saves lives
All-cause case fatality rate in unstable patients with thrombolytic
therapy was 15% vs. 47% without thrombolytic therapy. (p <.0001)
Am J Med 2012; 125: 465-470
Thrombolytic
therapy
No thrombolytic
therapy
In-h
os
pit
al a
ll-c
au
se
ca
se
fata
lity
ra
te in
un
sta
ble
pa
tie
nts
(%
)
15% n=21,390
n=50,840
47%

4/25/2016
3
MOPETT: Half-Dose Fibrinolysis for Anatomically Large PE
0
10
20
30
40
50
60
PulmonaryHypertension (%)
Mean length ofstay (d)
In-HospitalBleeding (%)
Half-Dose t-PA
Standard Anticoagulation
n = 121
16%
57%
2.2 4.9
P < 0.001
P < 0.001
Am J Cardiol 2013;111:273-277
0 0
Variable Low dose Alteplase (n=61)% Control (n=60)%`
P value
Recurrent PE 0 3(5) 0.08
Total mortality 1(1.6) 3(5) 0.30
NEJM 2014;370:1402-1411
PEITHO
Fibrinolysis for PE Meta-Analysis: Mortality Reduction
Fibrinolysis
Anticoagulation0
2
4
6
8
10
All-causemortality
RecurrentPE
Majorbleed
ICH
JAMA 2014;311:2414 -2421
%
2.2
3.9
9.2
3.4
1.2 0.2 1.5
3.0
p = 0.01
p < 0.001
p = 0.002
p = 0.003
Among patients with PE (including those who were hemodynamically stable with RV dysfunction), thrombolytic therapy was associated with lower rates of all-cause mortality and increased risks of major bleeding and ICH.
Major bleeding was not significantly increased in patients 65 years or younger.
• 16 RCT comparing thrombolysis to standard anticoagulation (n=2115)
• 71% (1449) had intermediate risk PE (RV dysfunction)
Risk Factors for Bleeding with, and Contraindications
to Use of, Thrombolytic Therapy (systemic and CDT)
CHEST 2016;149(2):313-352
Potential Advantages of US-Facilitated Catheter-Directed Low-Dose Fibrinolysis
Avoids the high risk of major bleeding associated with systemic fibrinolysis
• Including intracranial hemorrhage
• Dose-related: 25 mg vs. 100 mg
More complete thrombus resolution
• Catheter-directed fibrinolysis targets the area of highest thrombotic burden
More effective for subacute thrombus
• Pharmacomechanical therapy enhances fibrinolytic surface area by conditioning the thrombus
Slide courtesy of Greg Piazza
EKOS + Heparin
Heparin
0
0.1
0.2
0.3
0.4
0.5
0.6
Baseline to 24hours Baseline to 90 days
ULTIMA: Primary Outcomes
Red
ucti
on
in
RV
/LV
Rati
o
p < 0.001 p = 0.07
0.3
0.03
0.35
0.24
Circulation 2014;129:479-486
USAT regimen (10-20 mg t-PA) was superior to heparin alone in reversing RV dilatation at 24 hours without an increase in bleeding complications
59 patients Echo RV/LV ratio >1.0
UFH vs. USAT 1 death (UFH)
No major bleeding

4/25/2016
4
SEATTLE II: RV/LV Ratio (Reduction)
0
0.5
1
1.5
2
Pre-Procedure
48 Hours
1.55
1.13
RV
/LV
Ra
tio
p < 0.0001
JACC Cardiovasc Interv 2015;8(10):1382-1392
Catheter-directed Ultrasound Thrombolysis
150 patients with massive (31) or submassive (119) PE received low dose (24 mg) of tPA with unilateral (24 hours)
or bilateral (12 hours) catheters. NO ICH or fatal bleeds
Catheter Intervention Techniques and Devices
Circulation 2011;124:2139-2144
Hydrolyzer
Amplatz Oasis
Aspirex
Pigtail
Catheter Intervention Techniques and Devices Catheter Interventions without Thrombolysis
Other Therapies
• VORTEX AngioVac® -
thrombus vacuum
• Inari - large bore percutaneous thrombus extraction
• Penumbra - thrombus aspiration
• Argon Cleaner - clot macerator
• ECMO – hemodynamic support as bridge to definitive treatment Argon Cleaner
ECMO
Vortex
Penumbra
Surgical Embolectomy or Catheter-Based Interventions
• Patients with absolute
contraindications to
thrombolysis or (thrombolysis
has failed) surgical
embolectomy is preferred
therapy (Grade 2C)
• If not immediately available,
catheter embolectomy or
thrombus fragmentation may
be considered (Grade 2C)
Chest 2007;132:657-663
Eur Heart Journal 2008; 29: 2276-2315
Circulation 2011; 123: 1788-1830
Grade 2C: weak recommendation,
low or very low quality evidence
Am J Med 2012; 125:478-484
Case fatality rate was lower in each group that received an IVC filter
PREPIC2: Anticoagulation ± IVC Filter for High-Risk PE
JAMA 2015;313:1627-1635
• Among hospitalized patients with severe PE, the use of a ALN retrievable filter plus anticoagulation compared with anticoagulation alone did not reduce the risk of symptomatic recurrent PE at 3 months.
• Findings do not support the use of ALN filter in patients who can be treated with anticoagulation

4/25/2016
5
Case Report
• 69 year old female
• PMH - HTN, diabetes mellitus, asthma
• Previous PE after surgery in 2010
• Left total knee replacement on 6/24/14
• LMWH for DVT prophylaxis
Case Report
• Developed shortness of breath, chest pain and syncope (7/2/14)
• 911 called, BP < 90 mmHg (responded to IV fluids)
• Required O2
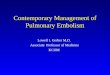
• ER - CTPA positive for an acute saddle PE
• Started on IV heparin
• Thrombocytopenia noted (heparin stopped)
• Argatroban initiated
Case Report
• Hemoglobin 12, platelets 18,000
• BUN 18, creatinine 1.21
• INR 1.1
• aPTT 57 seconds (target 46-84)
• PF4 strongly positive
CTPA
Case Report
• Transferred – Cleveland Clinic Medical ICU
(BP 105/63, HR 108, RR 22)
– Pulse oximetry - 94% on 4 liters of oxygen
• Mild distress
• Echo: moderate RV dilation and moderate to severe RV dysfunction
• Duplex US: acute left femoral-popliteal DVT
Case Report - PERT Call
• Develops atrial fibrillation with RVR 148
– oxygen requirements increasing
– More short of breath
– Hypotensive again (BP < 90 mmHg)
• Troponin positive
• Platelet count 24,000, hemoglobin stable
• PERT TEAM CALLED

4/25/2016
6
What to do Next?
What do the Guidelines Tell Us?
CHEST 2016;149(2):315-352
Grade 2C: weak recommendation, low or very low quality evidence
Grade 2B: weak recommendation, moderate-quality evidence
Benefits closely balanced with risk and burden
Circulation 2011;123:1788-1830
Class IIa; Level of Evidence B = Benefit >> than risk. Reasonable to perform treatment being useful/effective.
PE with Shock or Hypotension (High-Risk) Recommendations Class Level
Thrombolytic therapy is recommended I B
Surgical pulmonary embolectomy is recommended for patients in whom thrombolysis is contraindicated or has failed
I C
Percutaneous catheter-directed treatment should be considered as an alternative to surgical pulmonary embolectomy for patients in whom full-dose systemic thrombolysis is contraindicated or has failed
IIa C
Class I: evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective Class IIb: usefulness/efficacy is less well established by evidence/opinion
Level B: data derived from a single randomized clinical trial or larger non-randomized studies Level C: consensus of opinion of the experts and/or small studies, retrospective studies, registries
European Heart J 2014;35:3033-3080
Circulation 2004;110(6):744-749 Chest 2006;129(4):1043-1050
Interpreting 3 Sets of Guidelines: Who Should Get Advanced Therapy?
• AHA (“reasonable”)
• ACCP (“suggested”)
• ESC (“recommended”)
Massive PE
Factors Associated with Clinical Deterioration Shortly after PE (in our patient)
• Hypotension • Hypoxia • Coronary artery disease • Residual deep vein thrombosis • Right heart strain on echocardiogram • Elevated biomarkers • RV enlargement on CT
Circulation 2004;109(20):2401-2404 Thorax 2104;68:835-842

4/25/2016
7
What did we Do?
Case Report - PERT CALL
• 50 mg tissue plasminogen activator infused over 2 hours
• At the end of the infusion – HR low 70’s (NSR) – Blood pressure normalized – Oxygen requirements decreased – Clinically significantly improved – Discharged home 10 days later on warfarin
Case Report
• 24 year old female develops acute onset SOB, chest pain and a swollen left leg.
• PMH unremarkable • Recently started on OCP’s • ER - hemodynamically stable • Left common femoral/femoral
vein DVT • CT - submassive PE • Elevated biomarkers and echo
reveals moderate RV dysfunction • What are your treatment
options?
Interpreting 3 Sets of Guidelines: Who Should Get Advanced Therapy?
• AHA (severe right ventricular dysfunction and/or major biomarker elevation)
• ACCP (clinical gestalt)
• ESC (right ventricular dysfunction and biomarker elevation (intermediate-high risk)
Submassive PE
(Normotensive, Right Ventricular
Dysfunction, Elevated
Biomarkers)
CHEST 2016;149(2):315-352
Grade 1B: strong recommendation, moderated quality evidence
PE without shock or hypotension Intermediate or Low Risk
European Heart J 2014;35:3033-3080

4/25/2016
8
Circulation 2011;123:1788-1830
Class IIb; Level of Evidence C = Benefit > risk. Limited population studied. Procedure/treatment may be considered. Recommendations/usefulness, efficacy less well established.
Case Report - PERT Call
• 100 mg tissue plasminogen activator infused over two hours
• Patient converted to Rivaroxaban at discharge
PE Therapeutic Options: All Over the Map
Anticoagulation IV Thrombolysis
Catheter Directed Thrombolysis
Pharmaco-Mechanical Catheter Treatment
ECMO
IVC Filter
Surgical Embolectomy
Slide courtesy of PERT Consortium
Which Therapy to Use?
• Best treatment unknown – No standard approach
– No “appropriate use criteria” for intervention
– Practice varies by medical service, location, size
– No standard algorithm or consistency in decision-making
– No single team
– No centralized locations for care or “centers of excellence”
– No systematic evaluation of results
How do we decide whether to “intervene” and by what modality? Who decides? What is the endpoint?
Treatment Gap in Pulmonary Embolism
• <5% of patients with PE receive “advanced therapy”, including those with clear indications (hypotension, RV dysfunction, biomarkers, etc.)
• Many more are eligible than receive
• Reasons: – Failure to recognize potential benefit and integrate
data in “real time”
– Fear of complications
– Inability to respond rapidly (systems issues)
– “Paralysis in decision-making”
Slide courtesy of PERT Consortium
Multidisciplinary Pulmonary Embolism Response Teams:
Making Order out of Chaos
Slide courtesy of PERT Consortium

4/25/2016
9
The Perks of PERTs
• PERTs provide rapid bedside evaluation and risk stratification of patients with acute PE.
• PERTs help interpret recommendations from 3 sets of guidelines in the context of the individual patient.
• PERTs facilitate access to advanced therapies such as systemic fibrinolysis, catheter-directed therapy, surgical pulmonary embolectomy, and IVC filter insertion.
• PERTs guide the utilization of advanced techniques such as ECMO for critically-ill PE patients.
Slide courtesy of PERT Consortium
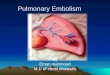
PERT Program Flow Map
Handoff to
therapeutic site
ED
Hospital
OSH
PERT fellow:
History
Physical
Labs
EKG
Echo
CT-PE Ultrasound leg
Massive
Surgery
Vortex
ECMO
Lytic
Submassive CDT
Low Risk
Expeditious input and clinical judgment from
multiple specialties to optimize therapy
A/C
ACTIVATE PERT
Electronic Meeting
Vascular Medicine
Cardiac Surgery ICU/Pulmonary
Cardiology
Interventional Radiology
Hematology
Slide courtesy of PERT Consortium
Cleveland Clinic – PERT Team A Multidisciplinary Team
Internal Medicine and Hematology
Outcomes - 82 patients (July 2014 – Present)
• Average age - -57 years (22 to 89)
• 4 surgical embolectomy
• 20 IVC filters placed
• 13 catheter directed tPA
• 11 half dose tPA (50 mg)
• 2 full dose tPA (100 mg)
• 20 bleeding complications
• 6 deaths (2 CDT and 4 standard heparin)
Summary
• The best methods for risk stratification (ACCP, AHA, ESC) remains to be determined.
• The optimal strategy for selection of advanced therapies for moderate and high-risk PE patients is unclear.
• The role of advanced circulatory support for PE has yet to be defined.
• Multidisciplinary PE Response Teams provide real-time individualized bedside evaluation and recommendations until definitive management algorithms are established.

4/25/2016
10
PE and DVT: A National Crisis The Incidence is Increasing!
• Severely under-recognized and undertreated
• Significant immediate and long-term sequelae
• High recurrence rate
• Treatments available that reduce mortality, morbidity and sequelae
Chest 2008:133:454S-545S
Am J Med 2104;127:829-839