Embed Size (px)
Citation preview

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
PULMONARY ARTER IAL HYPERTENS ION
1Department of Medicine, University of Alberta, Edmonton, Alberta T6G2B7, Canada.2Department of Medicine, Imperial College London, London W12 0NN, UK. 3NationalPulmonary Hypertension Service, Imperial College Healthcare National Health ServiceTrust, Hammersmith Hospital, Du Cane Road, London W12 0NN, UK. 4Department ofBiomedical Engineering, University of Alberta, Edmonton, Alberta T6G2B7, Canada.5Medical Research Council, London Institute of Medical Sciences, Hammersmith Hos-pital Campus, Imperial College London, London W12 0NN, UK. 6Sheffield PulmonaryVascularDiseaseUnit, RoyalHallamshireHospital, Sheffield S102JF, UK. 7Department ofSurgery, University of Alberta, Edmonton, Alberta T6G2B7, Canada. 8National Heart andLung Institute, Imperial College London, Dovehouse Street, London SW3 6LY, UK.*Corresponding author. Email: [email protected] (E.D.M.); [email protected](M.R.W.)
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
Copyright © 2017
The Authors, some
rights reserved;
exclusive licensee
American Association
for the Advancement
of Science. No claim
to original U.S.
Government Works
http://stm.sciencem
ag.oD
ownloaded from
Inhibition of pyruvate dehydrogenase kinase improvespulmonary arterial hypertension in geneticallysusceptible patientsEvangelos D. Michelakis,1* Vikram Gurtu,1 Linda Webster,1 Gareth Barnes,2 Geoffrey Watson,2
Luke Howard,3 John Cupitt,2 Ian Paterson,1 Richard B. Thompson,4 Kelvin Chow,4
Declan P. O’Regan,5 Lan Zhao,2 John Wharton,2 David G. Kiely,6 Adam Kinnaird,1
Aristeidis E. Boukouris,1 Chris White,7 Jayan Nagendran,7 Darren H. Freed,7 Stephen J. Wort,8
J. Simon R. Gibbs,3 Martin R. Wilkins2*
Pulmonary arterial hypertension (PAH) is a progressive vascular disease with a high mortality rate. It is char-acterized by an occlusive vascular remodeling due to a pro-proliferative and antiapoptotic environment in thewall of resistance pulmonary arteries (PAs). Proliferating cells exhibit a cancer-like metabolic switch where mito-chondrial glucose oxidation is suppressed, whereas glycolysis is up-regulated as the major source of adenosinetriphosphate production. This multifactorial mitochondrial suppression leads to inhibition of apoptosis anddownstream signaling promoting proliferation. We report an increase in pyruvate dehydrogenase kinase(PDK), an inhibitor of the mitochondrial enzyme pyruvate dehydrogenase (PDH, the gatekeeping enzyme ofglucose oxidation) in the PAs of human PAH compared to healthy lungs. Treatment of explanted humanPAH lungs with the PDK inhibitor dichloroacetate (DCA) ex vivo activated PDH and increased mitochondrialrespiration. In a 4-month, open-label study, DCA (3 to 6.25 mg/kg b.i.d.) administered to patients with idiopathicPAH (iPAH) already on approved iPAH therapies led to reduction in mean PA pressure and pulmonary vascularresistance and improvement in functional capacity, but with a range of individual responses. Lack of ex vivo andclinical response was associated with the presence of functional variants of SIRT3 and UCP2 that predict reducedprotein function. Impaired function of these proteins causes PDK-independent mitochondrial suppression andpulmonary hypertension in mice. This first-in-human trial of a mitochondria-targeting drug in iPAH demon-strates that PDK is a druggable target and offers hemodynamic improvement in genetically susceptible pa-tients, paving the way for novel precision medicine approaches in this disease.
brg/
y guest on January 8, 2020
INTRODUCTIONPulmonary arterial hypertension (PAH) is a complex vascular diseaseleading to right ventricular (RV) failure and death from a proliferativevascular remodeling that obstructs the lumen of resistance pulmonaryarteries (PAs) (1). Approved therapies (phosphodiesterase-5 inhibitors,endothelin receptor antagonists, soluble guanylate cyclase stimulators,and prostanoids) actmainly as vasodilators and improve symptoms butfail to arrest or reverse the disease (2). A cancer-like metabolic remodel-ing drives, at least in part, the structural changes in the pulmonary vas-cular wall. Specifically, a suppression of mitochondrial glucose oxidationin all cellular elements of the PAs [namely, PA smooth muscle cells(PASMCs), endothelial cells, and fibroblasts] leads to inhibition ofmitochondria-dependent apoptosis and secondary up-regulation of gly-colysis promoting pro-proliferative signaling and direction of carbonsources toward cellular building blocks rather than oxidation (3–9). Cen-tral to this is the inhibition of pyruvate dehydrogenase (PDH), the gate-
keeping enzyme of glucose oxidation, which catalyzes the mitochondrialproduction of acetyl–coenzymeA frompyruvate, the end product of gly-colysis,which in turn feeds theKrebs cycle to complete glucose oxidation.
Several potential mechanisms of PDH inhibition have been de-scribed. Induction of PDH kinase (PDK) leads to its complexing with,and tonic inhibition of, mitochondrial PDH by phosphorylation atserine-293. Whereas in healthy tissues PDK expression is low, the en-zyme can be induced selectively in the pulmonary circulation by the ac-tivation, even under normoxia, of hypoxia-inducible factor 1a (HIF1a),which is up-regulated in PAH (10). PDH can also be inhibited by tyro-sine kinase–mediated phosphorylation at tyrosine-301 (11). Anothermechanism is through inhibition of sirtuin 3 (SIRT3), the main mito-chondrial deacetylase, which activates several mitochondrial enzymesincluding PDH; Sirt3 knockout mice develop spontaneous pulmonaryhypertension, and SIRT3 activity is decreased in human PAH lungs(12). Last, inhibition of uncoupling protein 2 (UCP2), a mitochondrialprotein that regulates calcium entry, leads to a decrease in mitochon-drial calcium (13, 14). Manymitochondrial enzymes including PDH arecalcium-dependent, andUcp2 knockoutmice develop spontaneous pul-monary hypertension (13, 15). Thus, deficiency in SIRT3 and/or UCP2inhibits PDH in a PDK-independent manner.
Two relatively common single-nucleotide polymorphisms (SNPs),rs11246020 for SIRT3 and rs659366 forUCP2, have been reported to de-crease the activity and expression of these proteins, respectively (16–18).Both gene variants are relatively frequent in the general population andhave been associated with metabolic syndrome in humans (16, 17, 19),which is highly prevalent in PAH patients (20).
1 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
PDK is a druggable target that has been effectively inhibited by thesmall molecule dichloroacetate (DCA) in animal models and early-phase trials in cancer (21–25). DCA has also been clinically tested, witha good safety profile, in patients with congenital mitochondrial diseases,including PDH deficiency (26–29). Thus, we explored the role of PDKand DCA in human PAH with a series of experiments using archivedhuman lungs, PAH lungs studied ex vivo immediately after removal attransplant surgery [ex vivo lung perfusion (EVLP)] and an explorativeopen-label phase 1 clinical trial in idiopathic PAH (iPAH) patients. Wealso explored whether the presence of loss-of-function gene variants forSIRT3 and UCP2 provides resistance to the ability of DCA to activatePDH and reverse mitochondrial suppression in human PAH.
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
RESULTSPDK expression is increased in the PAs of human PAH lungsWe measured the expression of the two ubiquitously expressed PDKisoforms (1 and 2) (30) and PDH (Fig. 1A) in lung tissues from 10 pa-tients (6 with PAH and 4 non-PAH controls) (Table 1) by confocalmicroscopy and immunoblotting. PDK protein was markedly increasedin the wall of small muscularized PAs fromPAH compared to non-PAHlungs (Fig. 1B and fig. S1). This up-regulation was strong in PASMCsco-stained with smooth muscle actin antibody but was also apparentthroughout the vessel wall in other PA elements (for example, in endo-thelial cells, fibroblasts, and tissue inflammatory cells). This is consistentwith animal studies that show that these cell types in PAH undergo a
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
0
0.4
0.8
1.2
p-PDH-E1 (S293)
Actin
PDH-E1
PDK2
Actin
Actin
PDK1
Actin
1 2 3 4 1 2 4 5 6
Control PAH3
0
0.5
1
Control
PAH
P-E
1 /
E1 *
PD
K1
/ act
in
0
0.5
1
PD
K2
/ act
in**
A B
CSecondary antibody only
Control (no PAH) patient 2
PAH patient 1
50 µm
10 µm
5 µm
50 µm
50 µm
SMA+DIC
SMA+DIC
PDK2 SMA DIC
PDK2 SMA DIC
PDK1
PDK1
DAPI Merge
MergeDAPI
PDK2 SMA DIC
PDK1 DAPI merge
Inhibited SIRT3
Decreased Ca++mito
PDH
HIF1PDKDCA
Pyruvate
Glucose
Krebs cycle
ETC respirationATP production
Acetyl-CoA
Glycolysis
Inhibited UCP2
Decreased apoptosisIncreased proliferation
PA vascularremodeling
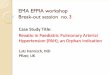
Fig. 1. PDK is important in the metabolic remodeling of PAH and is up-regulated in human PAH lungs. (A) Schematic demonstrating how PDK and SIRT3 andUCP2 suppress mitochondrial function by independent mechanisms (inhibition of PDH and glucose oxidation, global increase in mitochondrial acetylation, and globaldecrease in mitochondrial calcium, respectively). This mitochondrial suppression inhibits apoptosis and promotes proliferation, leading to the proliferative vascularremodeling characteristic of PAH. DCA is a selective PDK inhibitor and does not affect other mechanisms of PDH inhibition. DCA may inhibit the feedback loop that linksPDK-driven mitochondrial suppression and secondary normoxic activation of HIF1a to HIF-induced PDK induction. ETC, electron transport chain; Ca++mito, intramito-chondrial calcium; acetyl-CoA, acetyl–coenzyme A. (B) Confocal immunohistochemistry of a PAH and a non-PAH control lung with parallel staining for PDK1, PDK2,smooth muscle actin (SMA), and 4ʹ,6-diamidino-2-phenylindole (DAPI, a nuclear marker). Yellow boxes on differential interference contrast (DIC) images focus on smallresistance PAs, shown at higher magnification (right). An example of the stain only with secondary antibody is shown at the bottom. See Table 1 for patient information.(C) Immunoblots of peripheral lung tissues from PAH and control (non-PAH) lungs (for patient information, see Table 1) probed for p-PDH-E1a, PDH-E1a, PDK1, andPDK2. Quantification of the PDK1 or PDK2 over actin and p-PDH-E1a/PDH-E1a (normalized to actin) in each gel is shown. *P < 0.05, Mann-Whitney U test. ATP, aden-osine triphosphate.
2 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
metabolic remodeling (suppressed glucose oxidation and up-regulatedglycolysis) (7, 8) similar to that of PASMC (4, 5). Immunoblots fromtissue samples taken from the periphery of lungs, which are enrichedwith small PAs, confirmed the up-regulation of both PDK isoformsin PAH (Fig. 1C). This was associated with phosphorylation of serine-293 on the PDH-E1a subunit, marking PDH inhibition. We concludedthat PDK up-regulation is an active component of metabolic remodelingin human PAH and that the selectivity of this up-regulation to diseasedtissues makes PDK a potential therapeutic target for PAH.
DCA increases PDH activity and mitochondrial function inhuman PAH lungs ex vivoWe then studied mitochondrial function in five human lungs (Table 1)explanted at transplant surgery using EVLPunder conditions (pH, tem-perature, perfusion, and ventilation) that best mimic the in vivo en-vironment. The lungs were perfused and ventilated upon removal(Fig. 2A), and biopsies were taken from peripheral sites of each lung,which are enriched with resistance PAs, as soon as baseline conditionswere established at 37°C. After 1 hour of perfusion with DCA at a con-centration similar to the trough concentrations reported in patientson oral DCA therapy, additional biopsies were taken and pre-post com-parisons were made. PDH activity was measured with two standardtechniques: a biochemical dipstick assay based on the PDH-driven pro-duction of NADH (reduced form of nicotinamide adenine dinucleotide)(Fig. 2B) and immunoblots measuring serine-293 PDH-E1aphosphorylation (Fig. 2C). We also measured mitochondrial respirationin these tissues using a Seahorse protocol (Fig. 2D). Variability in theresponse to DCAwas observed. Lungs 1, 2, and 3 showed an increasein PDH activity and mitochondrial respiration, whereas lung 4 was
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
resistant to DCA and showed a small decrease in respiration duringDCA perfusion. Lung 5 (control) was perfused with vehicle and, likelung 4, exhibited no change in PDH activity and a small decrease inrespiration during the same perfusion period. We speculated thatnon-PDK–dependent mechanisms, such as the presence of reducedSIRT3 and/or UCP2 activity, may impair the response to DCA.
Hemodynamics and functional capacity are improved iniPAH patients after chronic oral DCA administrationTo investigate the therapeutic potential of PDK inhibition with DCAin vivo, a proof-of-concept 4-month, dose-finding trial of 3, 6.25, or12.5mg/kg bymouth twice daily [bis in die (b.i.d.)] was conducted inpatients clinically stable on treatment with approved iPAH therapies(ClinicalTrials.gov NCT01083524). Of the 23 patients screened, 20satisfied the inclusion/exclusion criteria and were enrolled in the study(Table 2). All patients were on sildenafil, 13 on dual therapy (sildenafil +endothelin receptor antagonist), and 1 on triple therapy (sildenafil,endothelin receptor antagonist, and parenteral prostanoid) in additionto background therapies. No patient had initiated PAH-approvedtherapies for a minimum period of 6 months before enrollment, andmaintenance dose was stable during this time except for patient 12(Table 2), who had an increase in the dose of an endothelial receptorantagonist 4.4months before enrollment. This patient, like all others,was stable with no signs of clinical improvement or worsening of dis-ease for at least 8 weeks before enrollment (an eligibility requirement).
There was no clinically significant change in the QT interval of theelectrocardiogram, cardiac rhythm, liver, bone marrow, or renalfunction. Dose-limiting toxicity, specifically paresthesia affecting thedorsum of the foot, toes, and fingers (grade II peripheral neuropathy),
Table 1. Characteristics of patients offering lung tissues. C, control tissue; P, patient tissue; aPAH, associated PAH (collagen vascular disease); CTEPH, chronicthromboembolic pulmonary hypertension; PDE5i, phosphodiesterase type 5 inhibitor; ERA, endothelin receptor antagonist; Prostn, parenteral prostanoid; sGC,soluble guanylate cyclase; WHO, World Health Organization.
Patient
Diagnosis Age Sex WHO class PAH therapyHistology/immunoblots
C1
Lobectomy (tumor) 56 M II NoneC2
Unused transplant donor 25 M I NoneC3
Unused transplant donor 38 F I NoneC4
Unused transplant donor 41 F I NoneP1
aPAH 34 F III PDE5i + ERAP2
iPAH 18 M IV PDE5i + ProstnP3
iPAH 39 F IV ERA + ProstnP4
iPAH 31 F III ERA + ProstnP5
iPAH 42 F III PDE5i + ERA + ProstnP6
aPAH 40 M IV PDE5i + ERA + Prostn SIRT3 variant UCP2 variantEVLP lung
1
aPAH 62 F IV PDE5i + ERA + Prostn G/G A/A2
aPAH 61 F IV PDE5i + ERA + Prostn G/A A/A3
iPAH 32 F IV PDE5i + ERA + Prostn G/G A/A4
iPAH 43 F IV PDE5i + ERA + Prostn G/A G/G5
CTEPH 60 M IV sGC stim + Prostn G/A A/A3 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
consistent with a previously described reversible and dose-dependent,nondemyelinating peripheral neuropathy (26, 28), developed in all fivepatients taking the highest dose tested (12.5 mg/kg b.i.d.). Four patientswithdrew from the study at that point (weeks 3 to 11), and one accepteda protocol-driven decrease in the dose to 6.25 mg/kg b.i.d., with im-provement of symptoms within 1 to 3 months in all patients. Thus, allpatients completing theprotocol (n=16)were taking 3or 6.25mg/kgb.i.d.,and 6.25 mg/kg b.i.d. was established as the highest tolerated dose,consistent with previous studies in patients with genetic mitochondrialdiseases and cancer (23–26). No patient deteriorated clinically or exhibiteda decrease in the 6-min walk of more than 10% from baseline, and nopatient required hospitalization during the study. There were no changesin PAH-approved and background therapies during the study.
Exposure to DCA led to an improvement in hemodynamic mea-surements at right heart catheterization [mean PA pressure (mPAP,P < 0.05), pulmonary vascular resistance (PVR, P < 0.05)] and func-tional capacity (6-min walk test, P < 0.05) in the cohort as a whole,
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
but interindividual variability in response was apparent (Fig. 3A).Seven patients responded toDCAwith a decrease inmPAP greater than5 mmHg (mean decrease, 9.1 mmHg) and an increase or no changein cardiac output (highlighted box in Fig. 3B); mean PVR decreased by118 ± 32 dynes·s·cm−5, and 6-min walk increased by 53 ± 18 m in thisgroup. Considering that these patients were already treated with PAHtherapies, this response is clinically meaningful and of a magnitudecomparable to approved PAH therapies, which have shown a meandecrease inmPAPof less than5mmHg in landmark trialswithpreviouslyuntreatedpatients [epoprostenol,−4.5mmHg(31); bosentan,−1.6mmHg(32); sildenafil, −2.1 mmHg (33)].
To better understand the variation in response, we first looked atplasma DCA concentrations (Fig. 4). Mean trough concentrationin both the 3 mg/kg b.i.d. (0.17 mM) and 6.25 mg/kg b.i.d. (0.59 mM)treatment groups demonstrated adequate exposure of PDK toDCA [theKi (inhibition constant) ofDCA forPDK2 is 0.2mM(30)], and therewasno dose-response relationship with respect to change in mPAP or PVR.
–25
0
25
50
75
Pre-DCA Post-DCA
Lu
ng
1L
un
g 2
Lu
ng
3L
un
g 4
% C
han
ge
in O
2co
nsu
mp
tio
n r
ate
P-E
1P
-E1
P-E
1P
-E1
P-E
1 /
E1P-E1
E1
P-E1
E1
P-E1
E1
P-E1
E1
BC D
Inte
nsi
ty (
AU
)In
ten
sity
(A
U)
Inte
nsi
ty (
AU
)In
ten
sity
(A
U)
0.0
0.2
0.4
0.6
0.0
0.5
1.0
0.0
0.2
0.4
0.0
0.5
1.0
1.5
1 2 3 4 5 Lung #
65
70
75
80
85
90
95
100
0 1 2 3
Pre-DCA
Post-DCA
Time (s)
% O
2 le
vel
(exa
mp
le b
iop
sy f
rom
lun
g #
3)
Human PAH EVLP
Pulmonary artery
Bronchi
Bronchus
PA
PV
ICUventilator
Perfusionpump
HeaterDeoxygenator
Com
pute
r
A
SNP score0
SNP score1
SNP score0
SNP score3
/ E
1 /
E1
/ E
1
DCA Vehicle
Pre Post
Pre- DCA
Post-DCA
0
50
100
0
13
25
0
6
12
0
15
30
Pre Post
Pre- veh.
Post-veh.
0
10
20
0.0
0.5
1.0
Pre-vehicle
Post- vehicle
Lu
ng
5 P-E1
E1
/ E
1
Inte
nsi
ty (
AU
)
Pre-vehicle
Post- vehicle Pre-
veh.Post-veh.
SNP score0
Pyruvate Acetyl-CoA PDH
CO2 + + H+CoA-SH + NAD
Fig. 2. DCAactivates PDHand increases respiration in humanPAHEVLP. (A) Photograph and schematic of the custom-made EVLP systemwith a human lung (seeMaterialsand Methods). ICU, intensive care unit. (B to C) PDH activity measured from lung biopsies before and after 1 hour of DCA perfusion (0.7 mg/ml). (B) PDH activity dipstick assay,measuringNADHproduction from the PDH reaction (see boxon top), quantitation [AU (arbitrary units)], andSNP scores. (C) Immunoblots for p-PDH-E1a andquantitation [(p-PDH-E1a/actin)/(total PDH-E1a/actin)]. Lungs 1, 2, and 3 showed an increase in PDH activity by DCA, whereas lung 4 was resistant to DCA (for patient information, see Table 1). Thecontrol lung 5 (see Table 1)was perfusedwith vehicle (veh.) (perfusate) for the same time as lungs 1 to 4. (D) Mitochondrial respiration (oxygen consumption rate)measured usinga Seahorse protocol frompre- and post-perfusion biopsies. Top: An example of oxygen consumption rate (slope of each line) of a pre- and post-DCA perfusion biopsy from lung 3.Bottom: The % change in oxygen consumption rate after DCA for all lungs. Perfusion of lung 5 with vehicle (perfusate) was a time control experiment.
4 of 12

17 26 F 10 55 8 7.9 465 III P G/G A/A 0 12.5
18 38 F 10 46 13 3 418 III P + E G/G G/A 1 12.5
19 41 F 7 68 8 3 538 II P + E G/G G/A 1 12.5
20 21 M 14 40 11 4 412 II P + E + Pros G/A A/A 1 12.5
*Dose decreased from 12.5 mg/kg.
S C I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
The mean trough DCA concentration in the seven patients with a goodresponse to DCA was 0.22 mM compared to 0.54 mM in the “non-responder” group, excluding underexposure to DCA as an explanationof the lack of response.
Differences in the response to DCA are associated with SIRT3and UCP2 variantsWe speculated that the lack of response to DCA in both the clinical trialand the EVLP experiments has a genetically driven biochemical basis andis associated with the presence of functional variants in SIRT3 andUCP2.As discussed earlier, the presence of these variants may cause a PDK-independent inhibition of PDH, which would not be responsive to DCA.
The SIRT3 rs11246020 “A allele” is associated with a point mutationthat causes a change of valine to isoleucine at residue 208 within theconserved catalytic deacetylase domain, causing a 34% decrease inSIRT3 activity compared to the “G allele” (17). The UCP2 rs659366 Gallele affects the promoter region of the gene, associated with a decreasein transcription and decreased mRNA expression compared to the A
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017 5 of 1
allele (18, 19). Although SIRT3 andUCP2 are both on chromosome 11,they are not in linkage disequilibrium. There is evidence for a “genedose-response” with both variants: Sirt3−/− mice show greater inhibitionof enzymatic activity and worse pulmonary hypertension compared toSirt3+/− mice (12), and UCP2 mRNA expression is associated with thepresence of the G allele, with the GG, GA, and AA alleles associated withprogressively increased mRNA expression (18). Thus, we developed anSNP scorewhere 1 point is given for each loss-of-function variant present:An SNP score of 0 means that both the variants are absent, a score of 4denotes that both variants are present in a homozygous manner, andscores in between represent the sum of points for each allelic risk variantpresent (table S1). A high SNP score predicts inhibition of PDHindependent of PDKand greater resistance toDCA. Lung 4, which exhib-ited resistance toDCA, had an SNP score of 3, whereas lungs 1 to 3,whichresponded toDCA, had SNP scores of 0 or 1 (Fig. 2, B toD, and Table 1).
Consistent with the ex vivo experiments, there was an inverse rela-tionship between the SNP score and change in mPAP, PVR, and 6-minwalk test: The lower the SNP score, the stronger the response to DCA
Table 2. Baseline characteristics of enrolled patients. Pt, patient; RAP, right atrial pressure; PAWP, PA wedge pressure; CO, cardiac output; Tx, therapy; P,phosphodiesterase type 5 inhibitor; E, endothelin receptor antagonist; Pros, parenteral prostanoid. All patients diagnosed with iPAH. Patients 17 to 20 werewithdrawn from the protocol due to a grade II peripheral neuropathy, which was eventually improved (rows shaded in gray). Patients 1 to 16 completed theprotocol and are all included in the Fig. 3 data analysis. The “risk variant” for each of the two alleles of the SIRT3 and UCP2 genes (the variant associated withdecreased SIRT3 activity and UCP2 expression) is shown in bold. The number of risk variants in bold between the two genes corresponds to the SNP score ofeach patient.
Pt
Age Sex RAP(mmHg)mPAP(mmHg)
PAWP(mmHg)
CO(liter/min)
6-minwalk
WHOclass
PAHTx
SIRT3variant
UCP2variant
SNPscore
DCA (mg/kgb.i.d.)
1
67 F 5 43 6 8.9 298 III P G/G G/A 1 32
54 F 3 50 5 3.4 450 II P + E G/G G/A 1 33
43 F 20 55 9 5.6 366 III P + E G/G A/A 0 34
60 F 4 62 11 3.5 409 II P+E G/G A/A 0 6.255
27 F 8 56 7 4.3 533 II P + E A/A A/A 2 6.256
63 F 6 33 10 6.1 385 III P + E G/G G/G 2 6.257
54 F 7 46 11 4.7 407 II P + E G/A A/A 1 6.258
75 M 13 48 13 6.7 262 III P G/G A/A 0 6.259
73 M 8 45 14 6 223 III P G/G A/A 0 310
58 F 11 64 14 4.8 242 III P + E G/G A/A 0 311
41 F 6 34 12 4 392 II P G/A G/A 2 312
64 F 6 46 10 4 393 III P + E G/A A/A 1 313
24 M 9 50 9 5.3 660 II P + E G/A A/A 1 6.2514
37 M 6 48 8 4.9 399 II P + E A/A G/A 3 6.2515
35 F 16 72 15 2.2 465 II P G/G G/A 1 6.2516
62 F 8 35 8 4.9 525 III P + E G/G G/A 1 6.25*2

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
(Table 2 and Fig. 3B). Although the presence of each gene variant alonewas inversely but weakly associated with a decrease in mPAP (fig. S2),their combined presence (fig. S3) exhibited a stronger relationship withthe change in mPAP, suggesting an additive genetically driven resistanceto DCA. A similar pattern characterized the response of RV function, themajor determinant ofmorbidity andmortality in PAH. RV ejection frac-tion, measured by cardiacmagnetic resonance imaging (MRI), improvedin patients with an SNP score of 0 (P < 0.05 compared to their baseline),whereas the patients with SNP scores of 1 had variable responses andthose with higher SNP scores showed no improvement (fig. S4).
Exploratory imaging biomarkers support the clinicalresponse to DCAWe used two imaging biomarkers in patient subsets to assist withbiological interpretation of the response to DCA. Using gadolinium
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
lung perfusion imaging withMRI, we found that the responders witha decrease of mPAP >5 mmHg had a ~150% increase in lung perfu-sion compared to the nonresponder group (a mean decrease in transittime of 0.55 versus 0.22 s, respectively; fig. S5A). We also measured pa-renchymal lung glucose uptake by 18fluorodeoxyglucose positron emis-sion tomography and computed tomography (18FDG-PET-CT).Consistent with increased glycolysis, animal models and patients withPAH exhibit higher lung glucose uptake as measured by lung 18FDG-PET compared to no-PAH controls (8, 34). By increasing glucose ox-idation, DCA is expected to reduce glycolysis and thus glucose uptake.The hemodynamic responders showed an overall decrease in 18FDGuptake, whereas the nonresponders showed an increase (fig. S5B).Consistent with the relationship between hemodynamic response toDCA and SNP score, a low SNP score was associated with a reductionin 18FDG uptake in response to DCA, whereas a high SNP score was
200
600
1000
1400
1800
2200
1.85
25
50
75
1.85
200
300
400
500
600
700
1.85
PV
R (
dyn
es·s
·cm
–5)
mPA
P (
mm
Hg
)6-
min
wal
k (m
)
Pre-DCA Post-DCA
49 ± 3 45 ± 3
400 ± 28 425 ± 23
719 ± 107 649 ± 102
Pre-DCA Post-DCA
Pre-DCA Post-DCA
P < 0.05
3 mg/kg
6.25 mg/kg
–160
–120
–80
–40
0
40
80
–13
–8
–3
2
SNP score0 1 2 or 3
SNP score0 1 2 or 3
0
20
40
60
80
SNP score0 1 2 or 3
A
P < 0.05
3 mg/kg
6.25 mg/kg
P < 0.05
3 mg/kg
6.25 mg/kg
–250
–200
–150
–100
–50
0
50
100
150
200
–60
–20
20
60
100
140
mPA
P (
mm
Hg
)
–25
–20
–15
–10
–5
0
5
10
SNP score
mPA
P (
mm
Hg
)
rS = 0.654
P < 0.01
PV
R (
dyn
es·s
·cm
–5)
rS = 0.532
P < 0.05 PV
R (
dyn
es·s
·cm
–5)
rS = –0.413
P = 0.112
6-m
in w
alk
(m)
6-m
in w
alk
(m)
SNP score
SNP score
B
0 1 2 3
0 1 2 3
0 1 2 3
Fig. 3. The effects of DCA on hemodynamic and functional end points and their association with genetic factors (variants of the SIRT3 and UCP2 genes) that causeresistance toDCA. (A) mPAP, PVR, and6-minwalk performanceofDCA-treatedpatients. Statistical significancewas assessedusingbefore-after paired t test (P<0.05). Themeans±SEM before and after DCA treatment and the P values are shown in each graph. (B) Scatter plots of the DCA-induced changes inmPAP, PVR, and 6-min walk, separated by theSNP score status of eachpatient. Statistical significancewas assessedusing a Spearman’s correlation test and rS, and P values are shown in eachgraph. Highlighted region identifiesseven patients who exhibited a significant decrease in the mPAP (>5 mmHg decrease) associated with an increase or no change in the cardiac output, suggestive of a clinicallymeaningful response. Plots of the DCA-induced change in mPAP, PVR, and 6-min walk (means ± SEM) over the SNP score are shown on the right.
6 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
associated with an increase in 18FDGuptake. Examples of two respond-ers are shown in Fig. 5.
DISCUSSIONIn a first attempt to target amitochondrial enzyme to treat humanswithvascular disease, we report that DCA in doses up to 6.25 mg/kg po(per os) b.i.d. over 4 months are generally well tolerated and can re-sult in a significant reduction in mPAP and PVR in iPAH. PDK in-hibition by DCA increases PDH activity and oxygen consumption inisolated perfused/ventilated PAH lungs, consistent with improve-ment in mitochondrial function.
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
DCAhas a very specificmechanism of action:Mimicking pyruvate’sstructure, it competeswith pyruvate for its binding “pocket” in PDKandthusmimics the “end-product inhibition” that results from pyruvate-PDKbinding (35). This has been confirmed by crystallization studies of PDKwithpyruvate orDCA in situ (36). In addition,molecular (small interferingRNA–induced) inhibition of PDK2 in cancer cells mimics DCA, whichdoes not exert any additional effects in cells lacking PDK (21). PDK2 isinduced in the lungs of PAH patients, and of all the PDK isoforms,PDK2 is the most sensitive to DCA (30).
Poor DCA responders were characterized by a biochemical resistancethat was associated, both in the ex vivo experiments and the clinical trial,with the presence of variants in SIRT3 and UCP2 that predict reducedprotein activity. We propose that PDH inhibition in these patients is lessdependent on PDK. Specifically, DCA may inhibit PDK but fail to in-crease PDH activity and respiration in patients in whom PDH is alsoinhibited by increased acetylation and/or lack of mitochondrial calciumin vascular cells due to SIRT3 andUCP2 gene variants that inhibit SIRT3activity and are associated with decreased UCP2 expression.
The correlation between the SNP score and clinical response toDCAwas a post hoc analysis. However, unlike randomized trials where a posthoc exploration of a biomarker can introduce bias, this concern doesnot apply in studies of genetic variants with known effects that arenot in linkage disequilibrium. The random distribution of the relevantvariants during miosis reduces bias and “Mendelian randomization” isbeing increasingly used to dissect genotype-response relationships (37).Post hoc analysis of genetic factors causing resistance to a drug has beenused successfully in cancer, leading to conclusions strong enough tochange clinical practice, without evidence from prospective studies(38, 39). Our hypothesis-driven selection of these gene variants wasbased on strong preclinical studies, which directly link the function ofthese geneswith PAHpathogenesis.Our sample size is too small to eval-uate whether these variants are enriched in PAH compared to healthypopulations. Nevertheless, a gene variantmay not be enriched in a pop-ulation with the disease but may still affect the response to therapy.
Weusednoninvasive imaging biomarkers, 18FDG-PET-CTandMRIlung perfusion, to aid the biological interpretation of the hemodynamicresponses. These tools may not be necessary to assess response in futurestudies, but it would be of interest to know whether patients exhibitinghigh lung 18FDGuptake aremore responsive toDCA in future trials. Anincrease in lung perfusion shown in the gadolinium-MRI studies, even inareas not perfused before DCA therapy (Fig. 5A), is consistent withpotential regression of occlusive vascular remodeling.
Previous studies in animals and humans have described an inotropiceffect of DCA on the right ventricle, perhaps due to a shift in the utili-zation of metabolic substrate (carbohydrates versus fatty acids) (40, 41).The combined effect of a decrease in RV afterload due to regression ofpulmonary vascular remodeling and RV inotropy is clinically very at-tractive. The long-term direct effects of DCA onRV remodeling are notknown but do not appear to be adverse, considering that none of ourpatients deteriorated clinically.We did detect an increase in RV ejectionfraction in DCA responders but did not detect a decrease in RV hyper-trophy (fig. S4). This is not necessarily a disadvantage. Given that theRV afterload is still high inDCA responders, themaintenance of a com-pensating RV state (hypertrophy) is beneficial compared to a potentialtransition to a decompensated state of RV dilatation and failure (42).
Activated immune cells play a paramount role in the pathogenesis ofPAH (43), and activation of these cells is associated with a suppressionof glucose oxidation and switch to glycolysis (44). Although the role ofPDK in these cells is not known, it is possible thatDCAmayhave effects
0.0
0.5
1.0
1.5
2.0
2.5
3 mg/kg b.i.d. 6.25 mg/kg b.i.d.
0.0
0.5
1.0
1.5
2.0
2.5
mPAP>5 mmHg
mPAP<5 mmHg
DCA trough concentration(mM)
Fig. 4. Trough serumDCA concentrations. Top: DCA concentration (means ± SEM)in patients exposed to 6.25mg/kg b.i.d. compared to 3mg/kg b.i.d. Bottom:DCA con-centration (means ± SEM) in responder patients (decrease in mPAP by more than5 mmHg) compared to nonresponder patients.
7 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
on these cells, limiting their activation and the inflammatory burden inPAH—a possibility that requires further studies.
PDK is induced by HIF, and this has been confirmed in both cancerand PAH models, where HIF activity is increased even under nor-moxia (10, 45). A primary mitochondrial suppression can lead tosecondary activation of HIF, completing a positive feedback loop(Fig. 1A) (12, 25, 46). There are many potential mechanisms that cancontribute to primary mitochondrial suppression in PAH (includingthe presence of SIRT3 and UCP2 variants), leading to a positivefeedback loop between mitochondrial suppression and HIF activa-tion, where PDK plays a central role (5). PDK inhibition can breakthis feedback loop and reverse the metabolic remodeling, promotingapoptosis and inhibiting proliferation within the PA wall.
Other molecular factors contributing to the metabolic reprogram-ming in PAH could contribute to a biochemical resistance tomitochon-drial activators. In the case of DCA, these include a decrease in SIRT3protein abundance by nongenetic mechanisms (12) or a potential de-crease in the mitochondrial calcium uniporter (MCU), an importantcalcium entry regulator in mitochondria, recently found to be im-portant in PAH (47). UCP2 has been shown to regulate the functionof the MCU (14). However, the identification of these potential molec-ular causes of DCA resistance in patients requires lung biopsies, whichare contraindicated in PAH patients. On the other hand, the gene var-iants that we studied here can be easily detected in many tissues, in-cluding blood,making them attractive tools for future precisionmedicinetrial designs. Lastly, there is some evidence that SNPs in glutathionetransferase z 1/maleylacetoacetate isomerase lead to hyper- or hypome-tabolizers of DCA, at least in children (48). Although there does notappear to be a relation between the clinical response and DCA troughconcentration in our small cohort (Fig. 4), we did not measure DCAmetabolites, and the possibility that such SNPs may be relevant shouldbe studied in future studies.
This work translates to humans the knowledge accumulated frommultiple preclinical studies and supports the newly proposed metabolictheory of PAH (4, 5). The beneficial hemodynamic effects of DCAwereobserved in patients already taking licensed medications for PAH. Theseagents are not known to have any effect on PDH activity, and our obser-vations suggest that the decreased PDH activity is an unexploited thera-peutic target in clinical practice. A factor to consider in future clinicaltrials of DCA is combination with a tyrosine kinase inhibitor, becausetyrosine kinases can both inhibit PDHby phosphorylating a site differentthan that of PDK (11) and activate PDK by phosphorylating PDK itself(49).We suggest that genotype should be considered as a basis for strat-ification in future clinical studies of DCA or other metabolic modula-tors, with a precisionmedicine design, either ensuring randomization of
End-diastole
End-diastole
Pre-DCA
Post-DCA
mPAP = 55 mmHg
mPAP = 42 mmHg
Patient 3
Lung perfusion
Lung perfusion
10
5
10
5
Mea
n tra
nsit
time
(s)
Mea
n tra
nsit
time
(s)
Patient 10
Pre-DCA
PA p
ress
ure
(m
mH
g)
Post-DCA
Pre-DCA Post-DCA 18FDG-PET-CT 18FDG-PET-CT
mPAP = 64 mmHg
mPAP = 44 mmHg
No
rmal
ized
fre
qu
ency
Distribution of 18FDG uptake before and after DCA
Score
BeforeAfter
100
50
0
100
50
0
100
60
024713052
20
A
B
Fig. 5. Examples of functional imaging biomarkers in two DCA responders.(A) MR images showinggadolinium transit timebefore and afterDCAand resolutionofthe D-shaped septum (arrow) in the heart of patient 3. Note the color scale of the gad-olinium transit time: Blue indicates short transit time and increased perfusion; yellow/red indicates long transit time and little/no perfusion at baseline. (B) PA pressure re-cordings and 18FDG uptake pre- and post-DCA from right heart catheterization and18FDG-PET-CT, respectively, of patient 10. A shift to the left of the distribution of the18FDGuptake suggests a decrease in glucose uptake due to decreased glycolysis. Colorheat maps show Patlak slope per gram of tissue (score) per voxel in lung sections, in-dicating the density of high-value voxels (colored in yellow and red, indicating areas ofhigh glucose uptake), overlaid on corresponding CT images.
8 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
patients according to their SIRT3/UCP2 SNP score or excluding patientswith an SNP score of >1 from the study, to maximize detection of abeneficial response.
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
MATERIALS AND METHODSStudy designThiswork consists of a preclinical component, where the effects ofDCAwere tested on human PAH lungs ex vivo and the amount of its targetenzyme (PDK) was measured in human PAH and control lungs, and aclinical component where a phase 1, dose discovery trial (NCT01083524)was conducted to measure the effects of DCA on several clinical para-meters in patients with iPAH. The investigators performing theexperiments were blinded for the preclinical data, but the clinical studywas open-label.
Human tissues samplesThe protocols for clinical and human tissue studies were approvedby the human studies ethics committees at the University of Alberta(Edmonton, UK) and Imperial College/Hammersmith Hospital(London, UK). Human tissues were processed and studied underidentical tissue handling and staining protocols (Table 1).
Mitochondrial respiration measurementsLung biopsies were taken before and after treatment with DCA duringEVLP for further analysis of oxygen consumption using the SeahorseXFe24 Analyzer (Agilent Technologies). Tissue was cut into segmentsweighing about 5mg and immediately plated onto anXF24 Islet CaptureMicroplate, with islet capture screens to secure the tissue at the bottom ofthewell, and submerged in the EVLPperfusate.Oxygen consumption ratewas measured and normalized to mass of tissue per well.
PDH activity analysisPDH activity was measured with a commercially available Mito-Profile Dipstick assay kit (MitoSciences) as previously described(50, 51). Protein (200 mg) was incubated with the dipstickcontaining the PDH complex antibody. With this method, thePDH complex is immunocaptured and the production of PDH-driven NADH is measured.
ImmunoblotsImmunoblots were performed with SDS–polyacrylamide gel electro-phoresis as previously described and analyzed using ImageJ (NationalInstitutes of Health) (12, 25). Antibodies used were as follows: PDK1(Abcam, ab110025; detected at 49 kDa), PDK2 (Abcam, ab68164;detected at 46 kDa), PDH-E1a (Abcam, ab168379; detected at 43 kDa),phospho-Ser293–PDH-E1a (EMDMillipore, AP1062; detected at 44 kDa),and actin (Abcam, ab3280; detected at 42 kDa). The PDK-PDHantibodieshave been validated in a recent publication (52).
Confocal imagingImmunofluorescence staining was performed as previously described, andimagingwasdoneusingaZeissLSM-510NLOmodel (CarlZeiss) (12,25,52).Antibodies usedwere PDK1 (Abcam, ab110025), PDK2 (SantaCruzBio-technology, sc-14484), and a–smooth muscle actin (Abcam, ab5694).
SNP genotyping assayGenomicDNAwas extracted frombuffy coat usingAllPrepRNA/DNAkits (Qiagen). DNA samples were quantified with a NanoDrop
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
spectrophotometer (ND-8000) and normalized to a concentration of50 ng/ml (diluted in 10 mM tris/1 mM EDTA). Samples were geno-typed by TaqMan SNP Genotyping Assays for rs11246020 andrs659366 (Applied Biosystems) and processed in triplicates accordingto standard protocol and read on theABI Prism 7900 SequenceDetector(Applied Biosystems) (12).
Ex vivo lung perfusionEVLP allowed the perfusion and ventilation of human lungs fromdonors and recipients at transplant surgery. The perfusate entered thePA via a tube, controlled by a pump in combination with pressure andflow-sensing catheters. The bronchi were connected with tubes to anintensive care unit ventilator. The efflux from the pulmonary veinsentered a deoxygenator, returning deoxygenated blood into the PAs,mimicking in vivo conditions. Flow was initiated slowly in a retrogradefashion to remove air from the circuit. Anterograde flow started at150 ml/min with an albumin-based solution supplemented with Na+
(138 mmol), K+ (6 mmol), Mg2+ (0.8 mmol), Cl− (142 mmol), SO4−2
(0.8 mmol), H2PO4 (0.8mmol), and glucose (5mmol). The perfusatetemperature was increased to 37°C, and flow rate was gradually in-creased to 40 to 50% of the estimated patient cardiac output. A protec-tive mode of ventilation was applied with a tidal volume of 7 ml/kg at7 breaths/min, positive end-expiratory pressure of 5 cmH2O, and frac-tion of inspired oxygen of 21%. The lungs were periodically expandedwith inspiratory holds to an airway pressure of 20 cmH2O. pH, partialpressure ofCO2, electrolytes, and glucoseweremaintained at physiologicconcentrations with frequent measurements. After baseline conditionswere established, DCA (sodium salt, TCI America) (0.7 mg/ml) wasadded to the perfusate. Peripheral lung biopsies were obtained beforeand afterDCAperfusion. The recipient’s lungs were obtained at the timeof lung transplantation and transferred immediately (within 5 min) tothe laboratory for EVLP, under a patient consent and protocol approvedby the Institutional Review Board at the University of Alberta. EVLP de-tails are shown in Fig. 2A.
Clinical protocol (NCT01083524)Adult patients with iPAH diagnosed by recognized criteria (53) weretreatedwithDCA for 4months (Table 2). All were receiving backgroundand approved PAH therapies and had to be clinically stable with nodosing changes for at least 8 weeks before enrollment (an eligibilityrequirement). Although initially, enrollment of patients in WHOfunctional classes III and IVwas planned, the protocolwas subsequentlyamended to also allow enrollment of patients in class II. Exclusioncriteria included concomitant diabetes, chronic kidney and liver dis-ease, and a history of neuropathy. There were three screen failuresout of 23 patients screened. All patients signed informed consentsapproved by the local human ethics committees. Three doses ofDCA were tested: 3, 6.25, and 12.5 mg/kg po b.i.d. Starting fromthe lowest dose, at least three patients in each site (Canada andUK) had to be treated without evidence of toxicity for 4 weeks beforeanother patient could be enrolled to the higher dose. Because themain anticipated toxicity, peripheral neuropathy, was previously de-scribed to be a dose-dependent and reversible, nondemyelinating neu-ropathy, a decrease in the dose was allowed for the two higher doses ifsymptoms occurred. Pathogen-freeDCA (sodium salt) was purchasedfrom TCI America. Pharmacists placed the individual doses of DCApowder (according to patient weight) in individual 20-cm3 sterile light-proofed vials, and patients added water to each bottle and dissolvedDCA, which is highly water soluble, before drinking it.
9 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
The primary end point was safety and tolerability, and secondaryend points included change from baseline in (i) mPAP and PVRmeasured by standard right heart catheterization, (ii) functional capac-ity measured by the 6-min walk test, and (iii) RV mass and ejectionfraction measured with standard cardiac MRI protocols. We also as-sessed two exploratory end points: (i) the biochemical response toDCA using lung 18FDG-PET-CT (London site) as a measure of glucoseuptake in the lungs, because it was hypothesized that a DCA-inducedactivation of glucose oxidation would result in suppression of glycolysisand thus a decrease in glucose uptake; and (ii) MRI-measured lungperfusion, measuring the transit time of gadolinium through the pul-monary circulation, because it was hypothesized that a DCA-inducedregression of pulmonary vascular remodeling would increase lung per-fusion (decreasing gadolinium transit time) even in areas not perfusedbefore DCA therapy (more than increasing the perfusion in alreadyperfused areas). The safety visits, which included blood tests for renal,hepatic, and bone marrow toxicity, electrocardiography, physical ex-amination, and 6-min walk distance, were performed monthly. Rightheart catheterization, MRI, and PET studies were performed atbaseline and at 4 months. There were no patients lost to follow-up.The protocol was terminated when the dose-limiting toxicity was clear-ly reached.
MRI studiesRV mass and volumes were measured using a standard approach bytwo readers blinded to the patient’s background or state (pre-DCAversus post-DCA). Lung perfusion was studied with three-dimensionaldynamic contrast-enhanced MRI using 1.5T Siemens Sonata systems.Typical scan parameters included 0.54-ms echo time, 1.5-ms repetitiontime, 15° flip angle, 192 × 72 × 20 matrix with a 400 × 300 × 150–mmfield of view (axial orientation), rate 2 parallel imaging [GRAPPA(Generalized Autocalibrating Partial Parallel Acquisition)], with a tem-poral resolution of 1.24 s per image, and a total of 30 acquired images. Allsubjects were injected with gadopentetate dimeglumine (0.1 mmol/kg;Magnevist, Bayer) at a rate of 5 ml/s followed by 20 ml of saline flush.Injectionswere timed to ensure five baseline (noncontrast) image acqui-sitions. Subjects were instructed to hold their breath at end-expiration.MRI studies were not possible on patient 16 for the RV mass and ejec-tion fraction protocols (patient declined) and on patients 8, 11, and 15 forthe perfusion studies because ofmotion artifacts (Table 2). The underlyingtheory and application of contrast-enhanced dynamic perfusion in thelungs has previously been described (54, 55). Briefly, signal intensitycurves from the lung tissue and blood pool (main trunk of the PA, arterialinput function)were first converted to contrast agent concentration usinga Bloch-equation look-up table approach. The tissue time-intensity curveswere subsequently used to estimate the mean transit time (MTT) of thecontrast agent in the lung parenchyma, using an exponential de-convolution approach to account for the effects of the arterial inputfunction. MTT values were calculated in each pixel, and the averagevalues over the entire lung are reported, with exclusion of pixels withcontributions from larger arteries or veins.
PET-CT studiesLung 18FDG (120megabecquerel) distribution was measured 1.5 hoursafter intravenous administration as previously described (34). Regionalglucose metabolic rate was calculated from the PET image data andfrom blood samples taken during the scan. The lung region of interestwas identified from the CT image, and the rate of change of activity wascalculated for each voxel. Blood rate was plotted against image rate for
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
each lung voxel to produce a plot, which tends to a straight line (Patlakplot), the slope of which gives rate of tissue uptake. The Patlak slope wascalculated for every voxel in the lung region. A voxel score was thencalculated by dividing by the CT-derived tissue density and scaling by1000, giving an index of the glucose metabolic rate. Histograms of thevoxel score distribution were plotted as “before-after” pairs, and a left-ward shift in distribution indicates a reduction in 18FDGuptake (Fig. 5).The mode of the voxel score histogram was found by smoothing datawith a Gaussian filter and searching for the peak. The PET-CT studieswere only performed at the London site (n = 7).
Trough DCA concentrationsPlasma samples were prepared using dextran sulfate sodium (DSS) so-lution (0.5 mM) as an internal chemical shift reference. The samplesthemselves consisted of 250ml of 90%plasma and10%standard internalreference andwere placed inNorell S-3-200 3-mmnuclearmagnetic res-onance (NMR) tubes. NMR data were collected on an Agilent 700MHz(16.45T) NMR spectrometer equipped with a VNMRS four-channelconsole as previously described (52). The system had a cryogenicallycooled inverse triple-resonance (HCN) probe containing a Z-pulsedfield gradient coil. An Agilent 7620 sample-handling robot was used.Samples were run at 25°C and individually tuned andmatched via anAgilent ProTune module. Each spectral was automatically phasedand manually corrected to reduce baseline distortion due to residualsolvent signal. The spectra were referenced to DSS, and then re-phased and re-referenced for each sample to confirm consistency.Regions for integration were 8.6364 to 6.5572 parts per million(ppm), 6.1000 to 6.000 ppm, 5.9682 to 5.6456 ppm, 5.4766 to5.1386 ppm, 5.0259 to 0.5397 ppm, and 0.1200 to 0.1200 ppm. Regionsnot included in the integration were used to apply a standard VNMRJbaseline correction. The 6.1 to 6 and 0.12 to −0.12 integrated regionswere subsequently used for DCA to DSS quantitation calculation,respectively.
Statistical analysisStatistical analysis was performed using IBM SPSS, version 24.0 (IBMAnalytics).Data are shown asmeanswith error bars indicating SEM.Alldata undergoing statistical analysis were subjected to Shapiro-Wilk testof normality. Some groups in Fig. 1 did not follow anormal distribution.Thus,meandata from immunoblots (Fig. 1)were comparedwith thenon-parametric Mann-Whitney U test. Mean differences (pre-post DCA)from clinical parameters (Fig. 3 and fig. S4) did not deviate from nor-mality; therefore, mean differences were compared via the parametricpaired t test. For correlation of SNP score to clinical parameters, theSpearman rank correlation was chosen given the small sample size insome SNP categories. Spearman rank correlation coefficient is shown(rS) with respective P values in Fig. 3 and fig. S4. Significance for all sta-tistical testing was determined to be P < 0.05.
SUPPLEMENTARY MATERIALSwww.sciencetranslationalmedicine.org/cgi/content/full/9/413/eaao4583/DC1Fig. S1. Confocal immunohistochemistry of six PAH lungs and three non-PAH control lungs.Fig. S2. Relationship between risk variants (SNP scores) and decrease in mPAP in patientstreated with DCA.Fig. S3. Relationship between the combined SNP score of both SIRT3 and UCP2 risk variantsand the change in mPAP in patients treated with DCA.Fig. S4. The effects of DCA on RV size and function.Fig. S5. The effects of DCA on lung perfusion (MRI) and glucose uptake (18FDG-PET-CT).Table S1. Gene variants score (SNPs) for DCA resistance.
10 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
REFERENCES AND NOTES1. G. Sutendra, E. D. Michelakis, Pulmonary arterial hypertension: Challenges in translational
research and a vision for change. Sci. Transl. Med. 5, 208sr205 (2013).2. V. V. McLaughlin, S. L. Archer, D. B. Badesch, R. J. Barst, H. W. Farber, J. R. Lindner,
M. A. Mathier, M. D. McGoon, M. H. Park, R. S. Rosenson, L. J. Rubin, V. F. Tapson, J. Varga,R. A. Harrington, J. L. Anderson, E. R. Bates, C. R. Bridges, M. J. Eisenberg, V. A. Ferrari,C. L. Grines, M. A. Hlatky, A. K. Jacobs, S. Kaul, R. C. Lichtenberg, J. R. Lindner,D. J. Moliterno, D. Mukherjee, G. M. Pohost, R. S. Schofield, S. J. Shubrooks, J. H. Stein,C. M. Tracy, H. H. Weitz, D. J. Wesley; ACCF/AHA, ACCF/AHA 2009 expert consensusdocument on pulmonary hypertension: A report of the American College of CardiologyFoundation Task Force on Expert Consensus Documents and the American HeartAssociation: Developed in collaboration with the American College of Chest Physicians,American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation119, 2250–2294 (2009).
3. P. Dromparis, E. D. Michelakis, Mitochondria in vascular health and disease. Annu. Rev. Physiol.75, 95–126 (2013).
4. R. Paulin, E. D. Michelakis, The metabolic theory of pulmonary arterial hypertension.Circ. Res. 115, 148–164 (2014).
5. G. Sutendra, E. D. Michelakis, The metabolic basis of pulmonary arterial hypertension.Cell Metab. 19, 558–573 (2014).
6. K. R. Stenmark, R. M. Tuder, K. C. El Kasmi, Metabolic reprogramming andinflammation act in concert to control vascular remodeling in hypoxic pulmonaryhypertension. J. Appl. Physiol. 119, 1164–1172 (2015).
7. L. Plecitá-Hlavatá, J. Tauber, M. Li, H. Zhang, A. R. Flockton, S. S. Pullamsetti,P. Chelladurai, A. D’Alessandro, K. C. El Kasmi, P. Ježek, K. R. Stenmark, Constitutivereprogramming of fibroblast mitochondrial metabolism in pulmonary hypertension.Am. J. Respir. Cell Mol. Biol. 55, 47–57 (2016).
8. W. Xu, T. Koeck, A. R. Lara, D. Neumann, F. P. DiFilippo, M. Koo, A. J. Janocha, F. A. Masri,A. C. Arroliga, C. Jennings, R. A. Dweik, R. M. Tuder, D. J. Stuehr, S. C. Erzurum,Alterations of cellular bioenergetics in pulmonary artery endothelial cells. Proc. Natl.Acad. Sci. U.S.A. 104, 1342–1347 (2007).
9. J. Rehman, S. L. Archer, A proposed mitochondrial–metabolic mechanism for initiationand maintenance of pulmonary arterial hypertension in fawn-hooded rats: TheWarburg model of pulmonary arterial hypertension. Adv. Exp. Med. Biol. 661, 171–185(2010).
10. S. Bonnet, E. D. Michelakis, C. J. Porter, M. A. Andrade-Navarro, B. Thébaud, S. Bonnet,A. Haromy, G. Harry, R. Moudgil, M. S. McMurtry, E. K. Weir, S. L. Archer, An abnormalmitochondrial–hypoxia inducible factor-1a–Kv channel pathway disrupts oxygensensing and triggers pulmonary arterial hypertension in fawn hooded rats: Similaritiesto human pulmonary arterial hypertension. Circulation 113, 2630–2641 (2006).
11. J. Fan, H.-B. Kang, C. Shan, S. Elf, R. Lin, J. Xie, T.-L. Gu, M. Aguiar, S. Lonning, T.-W. Chung,M. Arellano, H. J. Khoury, D. M. Shin, F. R. Khuri, T. J. Boggon, S. Kang, J. Chen, Tyr-301phosphorylation inhibits pyruvate dehydrogenase by blocking substrate binding andpromotes the Warburg effect. J. Biol. Chem. 289, 26533–26541 (2014).
12. R. Paulin, P. Dromparis, G. Sutendra, V. Gurtu, S. Zervopoulos, L. Bowers, A. Haromy,L. Webster, S. Provencher, S. Bonnet, E. D. Michelakis, Sirtuin 3 deficiency is associatedwith inhibited mitochondrial function and pulmonary arterial hypertension in rodentsand humans. Cell Metab. 20, 827–839 (2014).
13. P. Dromparis, R. Paulin, G. Sutendra, A. C. Qi, S. Bonnet, E. D. Michelakis, Uncouplingprotein 2 deficiency mimics the effects of hypoxia and endoplasmic reticulum stress onmitochondria and triggers pseudohypoxic pulmonary vascular remodeling andpulmonary hypertension. Circ. Res. 113, 126–136 (2013).
14. A. I. Bondarenko, W. Parichatikanond, C. T. Madreiter, R. Rost, M. Waldeck-Weiermair,R. Malli, W. F. Graier, UCP2 modulates single-channel properties of a MCU-dependent Ca2+
inward current in mitochondria. Pflugers Arch. 467, 2509–2518 (2015).15. O. Pak, N. Sommer, T. Hoeres, A. Bakr, S. Waisbrod, A. Sydykov, D. Haag, A. Esfandiary,
B. Kojonazarov, F. Veit, B. Fuchs, F. C. Weisel, M. Hecker, R. T. Schermuly, F. Grimminger,H. A. Ghofrani, W. Seeger, N. Weissmann, Mitochondrial hyperpolarization inpulmonary vascular remodeling. Mitochondrial uncoupling protein deficiency as diseasemodel. Am. J. Respir. Cell Mol. Biol. 49, 358–367 (2013).
16. L. T. Dalgaard, Genetic variance in uncoupling protein 2 in relation to obesity, type 2diabetes, and related metabolic traits: Focus on the functional −866G>a promoter variant(rs659366). J. Obes. 2011, 340241 (2011).
17. M. D. Hirschey, T. Shimazu, E. Jing, C. A. Grueter, A. M. Collins, B. Aouizerat,A. Stančáková, E. Goetzman, M. M. Lam, B. Schwer, R. D. Stevens, M. J. Muehlbauer,S. Kakar, N. M. Bass, J. Kuusisto, M. Laakso, F. W. Alt, C. B. Newgard, R. V. Farese Jr.,C. R. Kahn, E. Verdin, SIRT3 deficiency and mitochondrial protein hyperacetylationaccelerate the development of the metabolic syndrome. Mol. Cell 44, 177–190(2011).
18. S. Vogler, R. Goedde, B. Miterski, R. Gold, A. Kroner, D. Koczan, U.-K. Zettl, P. Rieckmann,J. T. Epplen, S. M. Ibrahim, Association of a common polymorphism in the promoter of UCP2with susceptibility to multiple sclerosis. J. Mol. Med. 83, 806–811 (2005).
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
19. H. Esterbauer, C. Schneitler, H. Oberkofler, C. Ebenbichler, B. Paulweber, F. Sandhofer,G. Ladurner, E. Hell, A. D. Strosberg, J. R. Patsch, F. Krempler, W. Patsch, A commonpolymorphism in the promoter of UCP2 is associated with decreased risk of obesity inmiddle-aged humans. Nat. Genet. 28, 178–183 (2001).
20. R. T. Zamanian, G. Hansmann, S. Snook, D. Lilienfeld, K. M. Rappaport, G. M. Reaven,M. Rabinovitch, R. L. Doyle, Insulin resistance in pulmonary arterial hypertension.Eur. Respir. J. 33, 318–324 (2009).
21. S. Bonnet, S. L. Archer, J. Allalunis-Turner, A. Haromy, C. Beaulieu, R. Thompson, C. T. Lee,G. D. Lopaschuk, L. Puttagunta, G. Harry, K. Hashimoto, C. J. Porter, M. A. Andrade,B. Thebaud, E. D. Michelakis, A mitochondria-K+ channel axis is suppressed in cancer andits normalization promotes apoptosis and inhibits cancer growth. Cancer Cell 11,37–51 (2007).
22. G. Sutendra, E. D. Michelakis, Pyruvate dehydrogenase kinase as a novel therapeutictarget in oncology. Front. Oncol. 3, 38 (2013).
23. Q. S.-C. Chu, R. Sangha, J. Spratlin, L. J. Vos, J. R. Mackey, A. J. B. McEwan, P. Venner,E. D. Michelakis, A phase I open-labeled, single-arm, dose-escalation, study ofdichloroacetate (DCA) in patients with advanced solid tumors. Invest. New Drugs 33,603–610 (2015).
24. E. M. Dunbar, B. S. Coats, A. L. Shroads, T. Langaee, A. Lew, J. R. Forder, J. J. Shuster,D. A. Wagner, P. W. Stacpoole, Phase 1 trial of dichloroacetate (DCA) in adults withrecurrent malignant brain tumors. Invest. New Drugs 32, 452–464 (2014).
25. E. D. Michelakis, G. Sutendra, P. Dromparis, L. Webster, A. Haromy, E. Niven, C. Maguire,T.-L. Gammer, J. R. Mackey, D. Fulton, B. Abdulkarim, M. S. McMurtry, K. C. Petruk,Metabolic modulation of glioblastoma with dichloroacetate. Sci. Transl. Med. 2, 31ra34(2010).
26. M. Abdelmalak, A. Lew, R. Ramezani, A. L. Shroads, B. S. Coats, T. Langaee, M. N. Shankar,R. E. Neiberger, S. H. Subramony, P. W. Stacpoole, Long-term safety of dichloroacetate incongenital lactic acidosis. Mol. Genet. Metab. 109, 139–143 (2013).
27. K. Berendzen, D. W. Theriaque, J. Shuster, P. W. Stacpoole, Therapeutic potential ofdichloroacetate for pyruvate dehydrogenase complex deficiency. Mitochondrion 6,126–135 (2006).
28. P. W. Stacpoole, L. R. Gilbert, R. E. Neiberger, P. R. Carney, E. Valenstein, D. W. Theriaque,J. J. Shuster, Evaluation of long-term treatment of children with congenital lacticacidosis with dichloroacetate. Pediatrics 121, e1223–e1228 (2008).
29. P. W. Stacpoole, T. L. Kurtz, Z. Han, T. Langaee, Role of dichloroacetate in the treatment ofgenetic mitochondrial diseases. Adv. Drug Deliv. Rev. 60, 1478–1487 (2008).
30. M. M. Bowker-Kinley, I. W. Davis, P. Wu, R. A. Harris, M. K. Popov, Evidence for existenceof tissue-specific regulation of the mammalian pyruvate dehydrogenase complex.Biochem. J. 329, 191–196 (1998).
31. R. J. Barst, L. J. Rubin, W. A. Long, M. D. McGoon, S. Rich, D. B. Badesch, B. M. Groves,V. F. Tapson, R. C. Bourge, B. H. Brundage, S. K. Koerner, D. Langleben, C. A. Keller,S. Murali, B. F. Uretsky, L. M. Clayton, M. M. Jöbsis, S. D. Blackburn Jr., D. Shortino,J. W. Crow; Primary Pulmonary Hypertension Study Group, A comparison of continuousintravenous epoprostenol (prostacyclin) with conventional therapy for primarypulmonary hypertension. N. Engl. J. Med. 334, 296–301 (1996).
32. R. N. Channick, G. Simonneau, O. Sitbon, I. M. Robbins, A. Frost, V. F. Tapson, D. B. Badesch,S. Roux, M. Rainisio, F. Bodin, L. J. Rubin, Effects of the dual endothelin-receptorantagonist bosentan in patients with pulmonary hypertension: A randomisedplacebocontrolled study. Lancet 358, 1119–1123 (2001).
33. N. Galiè, H. A. Ghofrani, A. Torbicki, R. J. Barst, L. J. Rubin, D. Badesch, T. Fleming, T. Parpia,G. Burgess, A. Branzi, F. Grimminger, M. Kurzyna, G. Simonneau; Sildenafil Use inPulmonary Arterial Hypertension (SUPER) Study Group, Sildenafil citrate therapy forpulmonary arterial hypertension. N. Engl. J. Med. 353, 2148–2157 (2005).
34. L. Zhao, A. Ashek, L. Wang, W. Fang, S. Dabral, O. Dubois, J. Cupitt, S. S. Pullamsetti,E. Cotroneo, H. Jones, G. Tomasi, Q.-D. Nguyen, E. O. Aboagye, M. A. El-Bahrawy,G. Barnes, L. S. Howard, J. S. R. Gibbs, W. Gsell, J.-G. He, M. R. Wilkins, Heterogeneity inlung 18FDG uptake in pulmonary arterial hypertension: Potential of dynamic 18FDGpositron emission tomography with kinetic analysis as a bridging biomarker forpulmonary vascular remodeling targeted treatments. Circulation 128, 1214–1224 (2013).
35. S.-C. Tso, X. Qi, W.-J. Gui, C.-Y. Wu, J. L. Chuang, I. Wernstedt-Asterholm, L. K. Morlock,K. R. Owens, P. E. Scherer, N. S. Williams, U. K. Tambar, R. M. Wynn, D. T. Chuang,Structure-guided development of specific pyruvate dehydrogenase kinase inhibitorstargeting the ATP-binding pocket. J. Biol. Chem. 289, 4432–4443 (2014).
36. M. Kato, J. L. Chuang, S.-C. Tso, R. M. Wynn, D. T. Chuang, Crystal structure of pyruvatedehydrogenase kinase 3 bound to lipoyl domain 2 of human pyruvate dehydrogenasecomplex. EMBO J. 24, 1763–1774 (2005).
37. G. Thanassoulis, C. J. O’Donnell, Mendelian randomization: Nature’s randomized trial inthe post-genome era. JAMA 301, 2386–2388 (2009).
38. C. S. Karapetis, S. Khambata-Ford, D. J. Jonker, C. J. O’Callaghan, D. Tu, N. C. Tebbutt,R. J. Simes, H. Chalchal, J. D. Shapiro, S. Robitaille, T. J. Price, L. Shepherd, H.-J. Au,C. Langer, M. J. Moore, J. R. Zalcberg, K-ras mutations and benefit from cetuximab inadvanced colorectal cancer. N. Engl. J. Med. 359, 1757–1765 (2008).
11 of 12

SC I ENCE TRANS LAT IONAL MED I C I N E | R E S EARCH ART I C L E
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from
39. A. Lièvre, J.-B. Bachet, D. Le Corre, V. Boige, B. Landi, J.-F. Emile, J.-F. Côté, G. Tomasic,C. Penna, M. Ducreux, P. Rougier, F. Penault-Llorca, P. Laurent-Puig, KRAS mutation statusis predictive of response to cetuximab therapy in colorectal cancer. Cancer Res. 66,3992–3995 (2006).
40. J. Nagendran, V. Gurtu, D. Z. Fu, J. R. B. Dyck, A. Haromy, D. B. Ross, I. M. Rebeyka,E. D. Michelakis, A dynamic and chamber-specific mitochondrial remodeling in rightventricular hypertrophy can be therapeutically targeted. J. Thorac. Cardiovasc. Surg.136, 168–178 (2008).
41. L. Piao, Y.-H. Fang, V. J. J. Cadete, C. Wietholt, D. Urboniene, P. T. Toth, G. Marsboom,H. J. Zhang, I. Haber, J. Rehman, G. D. Lopaschuk, S. L. Archer, The inhibition of pyruvatedehydrogenase kinase improves impaired cardiac function and electrical remodelingin two models of right ventricular hypertrophy: Resuscitating the hibernating rightventricle. J. Mol. Med. 88, 47–60 (2010).
42. R. Paulin, G. Sutendra, V. Gurtu, P. Dromparis, A. Haromy, S. Provencher, S. Bonnet,E. D. Michelakis, A miR-208–Mef2 axis drives the decompensation of right ventricularfunction in pulmonary hypertension. Circ. Res. 116, 56–69 (2015).
43. M. Rabinovitch, C. Guignabert, M. Humbert, M. R. Nicolls, Inflammation and immunity inthe pathogenesis of pulmonary arterial hypertension. Circ. Res. 115, 165–175 (2014).
44. K. Ganeshan, A. Chawla, Metabolic regulation of immune responses. Annu. Rev. Immunol.32, 609–634 (2014).
45. J.-w. Kim, I. Tchernyshyov, G. L. Semenza, C. V. Dang, HIF-1-mediated expression ofpyruvate dehydrogenase kinase: A metabolic switch required for cellular adaptation tohypoxia. Cell Metab. 3, 177–185 (2006).
46. G. Sutendra, P. Dromparis, A. Kinnaird, T. H. Stenson, A. Haromy, J. M. R. Parker,M. S. McMurtry, E. D. Michelakis, Mitochondrial activation by inhibition of PDKIIsuppresses HIF1a signaling and angiogenesis in cancer. Oncogene 32, 1638–1650 (2013).
47. Z. Hong, K.-H. Chen, A. DasGupta, F. Potus, K. Dunham-Snary, S. Bonnet, L. Tian, J. Fu,S. Breuils-Bonnet, S. Provencher, D. Wu, J. Mewburn, M. L. Ormiston, S. L. Archer,MicroRNA-138 and MicroRNA-25 down-regulate mitochondrial calcium uniporter,causing the pulmonary arterial hypertension cancer phenotype. Am. J. Respir. Crit. CareMed. 195, 515–529 (2017).
48. A. L. Shroads, T. Langaee, B. S. Coats, T. L. Kurtz, J. R. Bullock, D. Weithorn, Y. Gong,D. A. Wagner, D. A. Ostrov, J. A. Johnson, P. W. Stacpoole, Human polymorphisms in theglutathione transferase zeta 1/maleylacetoacetate isomerase gene influence thetoxicokinetics of dichloroacetate. J. Clin. Pharmacol. 52, 837–849 (2012).
49. T. Hitosugi, J. Fan, T.-W. Chung, K. Lythgoe, X. Wang, J. Xie, Q. Ge, T.-L. Gu,R. D. Polakiewicz, J. L. Roesel, G. Z. Chen, T. J. Boggon, S. Lonial, H. Fu, F. R. Khuri, S. Kang,J. Chen, Tyrosine phosphorylation of mitochondrial pyruvate dehydrogenase kinase1 is important for cancer metabolism. Mol. Cell 44, 864–877 (2011).
50. G. Sutendra, P. Dromparis, S. Bonnet, A. Haromy, M. S. McMurtry, R. C. Bleackley,E. D. Michelakis, Pyruvate dehydrogenase inhibition by the inflammatory cytokine TNFacontributes to the pathogenesis of pulmonary arterial hypertension. J. Mol. Med. 89,771–783 (2011).
51. G. Sutendra, P. Dromparis, P. Wright, S. Bonnet, A. Haromy, Z. Hao, M. S. McMurtry,M. Michalak, J. E. Vance, W. C. Sessa, E. D. Michelakis, The role of Nogo and themitochondria–endoplasmic reticulum unit in pulmonary hypertension. Sci. Transl. Med. 3,88ra55 (2011).
52. G. Sutendra, A. Kinnaird, P. Dromparis, R. Paulin, T. H. Stenson, A. Haromy, K. Hashimoto,N. Zhang, E. Flaim, E. D. Michelakis, A nuclear pyruvate dehydrogenase complex is importantfor the generation of acetyl-CoA and histone acetylation. Cell 158, 84–97 (2014).
Michelakis et al., Sci. Transl. Med. 9, eaao4583 (2017) 25 October 2017
53. N. Galiè, M. Humbert, J.-L. Vachiery, S. Gibbs, I. Lang, A. Torbicki, G. Simonneau,A. Peacock, A. Vonk Noordegraaf, M. Beghetti, A. Ghofrani, M. A. Gomez Sanchez,G. Hansmann, W. Klepetko, P. Lancellotti, M. Matucci, T. McDonagh, L. A. Pierard,P. T. Trindade, M. Zompatori, M. Hoeper, V. Aboyans, A. Vaz Carneiro, S. Achenbach,S. Agewall, Y. Allanored, R. Asteggiano, L. Paolo Badano, J. Albert Barberà, H. Bouvaist,H. Bueno, R. A. Byrne, S. Carerj, G. Castro, C. Erol, V. Falk, C. Funck-Brentano, M. Gorenflo,J. Granton, B. Iung, D. G. Kiely, P. Kirchhof, B. Kjellstrom, U. Landmesser, J. Lekakis,C. Lionis, G. Y. H. Lip, S. E. Orfanos, M. H. Park, M. F. Piepoli, P. Ponikowski, M. P. Revel,D. Rigau, S. Rosenkranz, H. Voller, J. Luis Zamorano, 2015 ESC/ERS guidelines for thediagnosis and treatment of pulmonary hypertension: The Joint Task Force for theDiagnosis and Treatment of Pulmonary Hypertension of the European Society ofCardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Associationfor European Paediatric and Congenital Cardiology (AEPC), International Society for Heartand Lung Transplantation (ISHLT). Eur. Heart J. 37, 67–119 (2016).
54. Y. Ohno, H. Hatabu, K. Murase, T. Higashino, H. Kawamitsu, H. Watanabe, D. Takenaka,M. Fujii, K. Sugimura, Quantitative assessment of regional pulmonary perfusion in theentire lung using three-dimensional ultrafast dynamic contrast-enhanced magneticresonance imaging: Preliminary experience in 40 subjects. J. Magn. Reson. Imaging20, 353–365 (2004).
55. Y. Ohno, H. Hatabu, K. Murase, T. Higashino, M. Nogami, T. Yoshikawa, K. Sugimura,Primary pulmonary hypertension: 3D dynamic perfusion MRI for quantitative analysis ofregional pulmonary perfusion. AJR Am. J. Roentgenol. 188, 48–56 (2007).
Acknowledgments: We are grateful to the physicians and staff of the University of AlbertaPulmonary Hypertension Program and the Hammersmith and Sheffield Pulmonary HypertensionService for the assistance with the recruitment and investigation of patients. We are indebtedto the patients for their participation in the study. Funding: This paper presents independentresearch that was funded by the Canadian Institutes of Health Research, the Heart and StrokeFoundation of Canada, and theHecht Foundation (Vancouver, Canada) to E.D.M.; and a jointMedicalResearch Council and British Heart Foundation grant (G0701637) and Wellcome Trust–GlaxoSmithKline program award to M.R.W. This work was supported by the Mazankowski AlbertaHeart Institute (Edmonton, Canada) and the National Institute for Health Research/Wellcome TrustImperial Clinical Research Facility at Imperial College Healthcare National Health Service Trust(London, UK). Author contributions: E.D.M. conceived the study. E.D.M. and M.R.W. designed,funded, and supervised the study. E.D.M., V.G., and M.R.W. analyzed the data. E.D.M. wrote the firstdraft, whichwas edited byM.R.W. andV.G. All the authors contributed to the acquisition of either thepreclinical or clinical data and coedited and approved the first and subsequent drafts and revisionsof the paper. Competing interests: The authors declare that they have no competing interests.Data andmaterials availability: All data are included in the paper or the Supplementary Materials.
Submitted 27 July 2017Accepted 22 September 2017Published 25 October 201710.1126/scitranslmed.aao4583
Citation: E. D. Michelakis, V. Gurtu, L. Webster, G. Barnes, G. Watson, L. Howard, J. Cupitt,I. Paterson, R. B. Thompson, K. Chow, D. P. O’Regan, L. Zhao, J. Wharton, D. G. Kiely,A. Kinnaird, A. E. Boukouris, C. White, J. Nagendran, D. H. Freed, S. J. Wort, J. S. R. Gibbs,M. R. Wilkins, Inhibition of pyruvate dehydrogenase kinase improves pulmonary arterialhypertension in genetically susceptible patients. Sci. Transl. Med. 9, eaao4583 (2017).
12 of 12

in genetically susceptible patientsInhibition of pyruvate dehydrogenase kinase improves pulmonary arterial hypertension
and Martin R. WilkinsKinnaird, Aristeidis E. Boukouris, Chris White, Jayan Nagendran, Darren H. Freed, Stephen J. Wort, J. Simon R. GibbsIan Paterson, Richard B. Thompson, Kelvin Chow, Declan P. O'Regan, Lan Zhao, John Wharton, David G. Kiely, Adam Evangelos D. Michelakis, Vikram Gurtu, Linda Webster, Gareth Barnes, Geoffrey Watson, Luke Howard, John Cupitt,
DOI: 10.1126/scitranslmed.aao4583, eaao4583.9Sci Transl Med
genotype in clinical trial design and identifies a drug target for PAH.mitochondrial proteins were less responsive to DCA. This work highlights the importance of considering patient functional capacity. The authors determined that patients with inactivating mutations in two genes encodingthis variable response was mirrored in a phase 1 trial, with some patients showing improved hemodynamics and pyruvate dehydrogenase kinase. DCA increased mitochondrial function; however, the response was variable, and(DCA), a drug used to treat cancer and congenital mitochondrial disease that inhibits the mitochondrial enzyme
. treated lungs from patients with PAH with dichloroacetateet alpulmonary arterial hypertension (PAH). Michelakis In addition to thickening and occlusion of the pulmonary arteries, mitochondrial respiration is suppressed in
Progress for PAH
ARTICLE TOOLS http://stm.sciencemag.org/content/9/413/eaao4583
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2017/10/23/9.413.eaao4583.DC1
CONTENTRELATED
http://stm.sciencemag.org/content/scitransmed/11/480/eaan0457.fullhttp://stm.sciencemag.org/content/scitransmed/10/445/eaap7294.fullhttp://stm.sciencemag.org/content/scitransmed/10/438/eaao0303.fullhttp://science.sciencemag.org/content/sci/358/6367/eaan4368.fullhttp://stm.sciencemag.org/content/scitransmed/9/416/eaai9048.fullhttp://stm.sciencemag.org/content/scitransmed/7/294/294ra107.fullhttp://stm.sciencemag.org/content/scitransmed/5/200/200ra117.fullhttp://stm.sciencemag.org/content/scitransmed/3/88/88ra55.fullhttp://stm.sciencemag.org/content/scitransmed/7/308/308ra159.fullhttp://stm.sciencemag.org/content/scitransmed/5/208/208sr5.fullhttp://stm.sciencemag.org/content/scitransmed/2/44/44ra58.full
REFERENCES
http://stm.sciencemag.org/content/9/413/eaao4583#BIBLThis article cites 55 articles, 17 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
of Science. No claim to original U.S. Government WorksCopyright © 2017 The Authors, some rights reserved; exclusive licensee American Association for the Advancement
by guest on January 8, 2020http://stm
.sciencemag.org/
Dow
nloaded from