Embed Size (px)
Citation preview

Earn
3 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
“Puff, Not the Magic Dragon… The Cost of America’s Tobacco Use”
A Peer-Reviewed Publication Written by Lisa Dowst-Mayo, RDH, BSDH
Publication date: Jan. 2015 Expiration date: Dec. 2017
This educational activity was developed by PennWell’s Dental Group with no commercial support.This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: PennWell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 3 CE credits for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.CE Planner Disclosure: Heather Hodges, CE Coordinator does not have a leadership or commercial interest with products or services discussed in this educational activity. Heather can be reached at [email protected] Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.Image Authenticity Statement: The images in this educational activity have not been altered.Scientific Integrity Statement: Information shared in this CE course is developed from clinical research and represents the most current information available from evidence based dentistry. Known Benefits and Limitations of the Data: The information presented in this educational activity is derived from the data and information contained in reference section. The research data is extensive and provides direct benefit to the patient and improvements in oral health. Registration: The cost of this CE course is $59.00 for 3 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Supplement to PennWell Publications
PennWell designates this activity for 3 continuing educational credits.
Dental Board of California: Provider 4527, course registration number CA# 03-4527-14093“This course meets the Dental Board of California’s requirements for 3 units of continuing education.”
The PennWell Corporation is designated as an Approved PACE Program Provider by the
Academy of General Dentistry. The formal continuing dental education programs of this
program provider are accepted by the AGD for Fellowship, Mastership and membership
maintenance credit. Approval does not imply acceptance by a state or provincial board of
dentistry or AGD endorsement. The current term of approval extends from (11/1/2011) to
(10/31/2015) Provider ID# 320452.
Go Green, Go Online to take your course
AbstractTobacco use remains the single largest preventable cause of death in the United States1,2. Even with the increased cost of tobacco products, increase in anti-tobacco media campaigns and smoke-free laws for workplaces and public places, almost 20% of Ameri-cans still continue to use tobacco. Dental professionals are in an ideal position to directly influence tobacco use among their patients. This course will present tobacco use statistics, tobacco’s effects on the human body and nicotine pharmacology as it relates to cessation pro-grams. The contents of cigarettes, smokeless tobacco,
electronic cigarettes and snus, will be discussed.
Educational ObjectivesAt the conclusion of this educational activity participants will be able to:1. Discuss risk factors associated with tobacco
use.2. Identify patients at higher risk for tobacco
abuse by understanding current statistical trends.
3. Discuss the different forms of tobacco prod-ucts currently on the market in the United States and their components
4. Discuss the difficulties patients have sustain-ing a quit plan and why relapse rates are high for tobacco users.
Author ProfileLisa Dowst-Mayo, RDH, BSDH graduated from Baylor College of Dentistry in 2002 and is currently pursuing a Master’s degree in Healthcare Administration from Ohio University. She is an active member in ADHA and is a full time professor at Concorde Career College in San Antonio. She is a published author and national speaker and can be contacted through her website at www.lisamayordh.com. She is also the co-owner of Diamond Dental Education (www.diamonddentaleducation.com).
Author Disclosure
Lisa Dowst-Mayo has no commercial ties with the sponsors or providers of the unrestricted educational grant for this course.
1501RDH_57 57 1/8/15 10:20 AM

58 | rdhmag.com RDH | January 2015
Educational ObjectivesAt the conclusion of this educational activity participants will be
able to:
1. Discuss risk factors associated with tobacco use.
2. Identify patients at higher risk for tobacco abuse by under-
standing current statistical trends.
3. Discuss the different forms of tobacco products currently on
the market in the United States and their components
4. Discuss the difficulties patients have sustaining a quit plan
and why relapse rates are high for tobacco users.
AbstractTobacco use remains the single largest preventable cause of
death in the United States.1,2 Even with the increased cost of
tobacco products, increase in anti-tobacco media campaigns and
smoke-free laws for workplaces and public places, almost 20%
of Americans still continue to use tobacco. Dental professionals
are in an ideal position to directly influence tobacco use among
their patients. This course will present tobacco use statistics,
tobacco’s effects on the human body and nicotine pharmacology
as it relates to cessation programs. The contents of cigarettes,
smokeless tobacco, electronic cigarettes and snus, will be dis-
cussed.
IntroductionAmerican's dependency on tobacco comes with a high price tag,
with an estimated annual cost of over $96 billion in direct medical
expenses and $97 billion in lost productivity.3 More than ten times
as many U.S. citizens have died prematurely from cigarette smok-
ing than have died in all wars fought by the United States during
its history.3 Smoking causes more deaths annually than HIV,
illegal drug use, alcohol use, motor vehicle injuries and firearm-
related incidents combined.4 A pack of cigarettes has an average
cost of $5.51 and an electronic cigarette starter kit ranges from
$59.95 to $129.95 with refills $0.50-3.00.5,6 The average cost of a
can of smokeless tobacco $3.007 and a can of snus averages $1.99-
3.50.8 Therefore, the average American tobacco user can spend
anywhere from $900-$2,000 annually to support their habit.
It is a requirement for all dental health professionals to as-
sist and advise their patients on the health risks associated with
tobacco abuse. It is imperative clinicians stay up-to-date with new
tobacco products on the market and understand the risks they can
pose to patients. The CDC and FDA allude to a new fear with
the introduction of electronic cigarettes (e-cigarettes) and snus
to the American market with their youthful appearance and ap-
peal.9,10 Healthcare professionals should be aware of the possible
resurgence of adolescent tobacco users.
StatisticsMost statistics reported by varying agencies are centered on tradi-
tional cigarettes and smokeless tobacco, as these two have been the
American staple tobacco products for generations. It is extremely
difficult, if not impossible, to find the long term consequences of
e-cigarettes and snus as neither are fully regulated by the FDA at
this time.
According to the CDC, as of 2011, 19% of Americans (43.8
million) still smoke and of this group, 78% smoke every day and
22% smoke some days.2 A tobacco user’s life expectancy is shorter
than a non-smoker.1 In women, 90% of lung cancer deaths are
attributable to smoking and smoking is now the leading cause of
death in women, surpassing breast cancer.1
The CDC reports a decline in persons who smoke over 30
cigarettes per day in the last nine years. In 2005, the percent was
12.6% and by 2011 this percentage dropped to 9.1%2,4 However,
the percentage of daily smokers who average 1-9 cigarettes per day
rose. In 2005 the percentage was 16.4% and by 2011, this percent-
age had increased to 22.0%.2,4
The CDC reports the highest tobacco use rates in the US are
people age 18-64 (22.8-24.3%). The overall percentage of non-
smokers does not significantly decline until after age 65 (9.7%).
Men of all races smoke more than women of comparable ethnic-
ity.2,4 Hispanics and Asian-Americans have the lowest percentage
of tobacco use, while Caucasian, African-American and mixed
races have the highest.2,4 Tobacco use rates are higher among non-
high school graduates and those with a GED, and lowest among
those with associate, bachelors or graduate degrees. 2,4 Throughout
the regions of the United States, tobacco use rates vary dramati-
cally; the highest rates are found in the midwest and south, with
lower rates in the northeast and west.2,4
Tobacco ComponentsLong gone are the days when a tobacco user only had two choices
in products: cigarettes or smokeless (dip) tobacco. Newer products
have entered the US market in the past decade such as electronic
cigarettes (e-cigarettes) and snus.
Cigarettes
Cigarettes remain the predominant form of tobacco use in the
United States.2,4 Cigarettes contain hundreds of different chemi-
cals and gases in varying concentrations, depending on the specific
brand. There are at least 45 ingredients classified as carcinogens11
Below is a short list of some of the chemicals found in cigarettes:
1. Carbon monoxide: Decreases the ability of hemoglobin to
bind with oxygen and prompts it to bind with the carbon
monoxide. This leads to a decrease in oxygen consumption in
the body as a whole.11
2. Ammonia (NH3): Volatile malodorous gas used to make
fertilizers and explosives.
3. Acetylene (C2H
2): Colorless gas which is used as the fuel in
welding torches.
4. Nicotine: Addictive component of cigarettes. Nicotine will be
discussed in more detail in the pharmacology section of this
course.
5. Cyanide: Smoking cigarettes is one of the major sources of
cyanide exposure for people who do not work in cyanide-
related industries.2,4 Cyanide prevents the body’s cells from
1501RDH_58 58 1/8/15 10:20 AM
RDH | January 2015 rdhmag.com | 59
using oxygen which leads to lysis. It is most harmful to the
human heart and brain.
6. Benzene: An industrial solvent, refined from crude oil.
Benzene can predispose a patient to leukemia.12
7. Formaldehyde: Organic compound used as a disinfectant and
in paint and automobile manufacturing.
8. Tar: Term to describe a collection of solid particles that are
inhaled while smoking. Tar is a mixture of many chemicals
that are known to be carcinogenic. When tar settles, it forms
a sticky, brown residue that is responsible for the staining of
teeth, fingers and lungs in smokers.
9. Cadmium: Not essential for human life although humans
obtain it through their diet. Smokers will have double the
exposure to daily cadmium than non-smokers. Cadmium
exposure is implicated in many different cancers.
10. Polonium-201: A highly radioactive element implicated in
many different cancers.
It is well established in the literature that smoking reduces a
person’s life span and can affect every organ in the body. In 2012,
the CDC reported smoking has been linked to COPD, acute my-
eloid leukemia, coronary artery disease, GERD, stroke and cancer
of the bladder, cervix, colon, rectum, oropharynx, trachea, lung,
esophagus, larynx, kidney, ureter, liver, pancreas and stomach.11
30% of cancer deaths are attributed to smoking and it comprises
80% of all COPD cases.2,5
The effects of second-hand smoke can be just as harmful, if
not more so, than first-hand.1,11 Exposure to second-hand smoke
can put an individual at risk for respiratory symptoms and disease,
decreased pulmonary function, lung cancer and coronary artery
disease.11
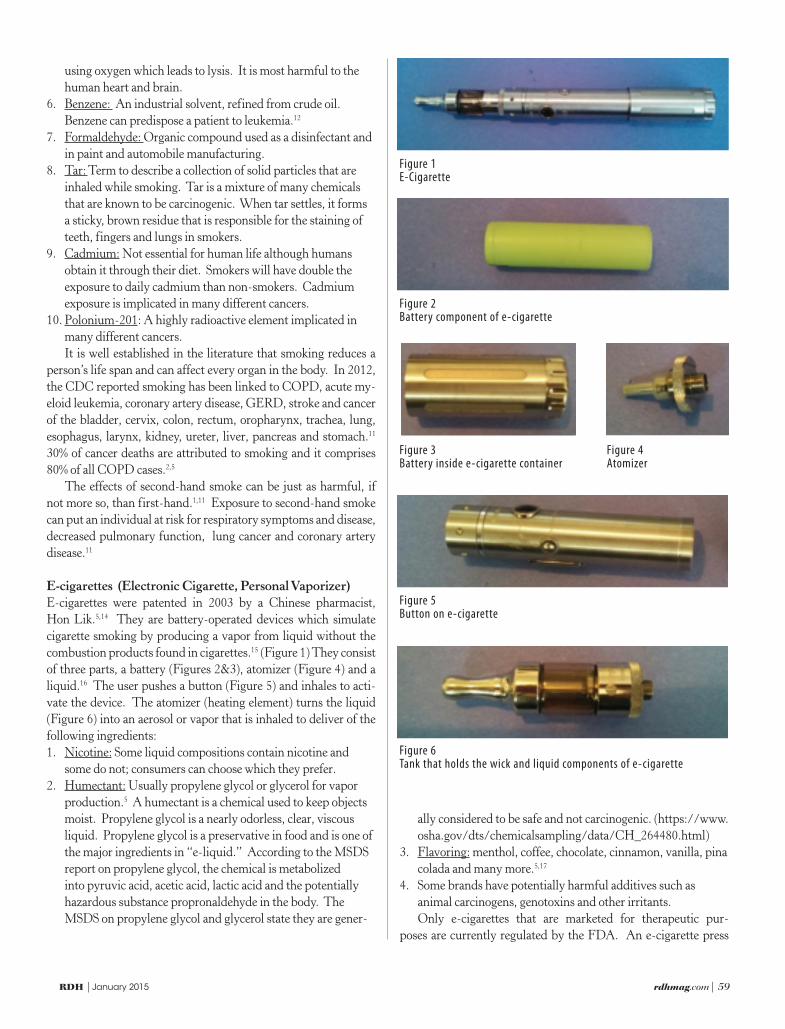
E-cigarettes (Electronic Cigarette, Personal Vaporizer)
E-cigarettes were patented in 2003 by a Chinese pharmacist,
Hon Lik.5,14 They are battery-operated devices which simulate
cigarette smoking by producing a vapor from liquid without the
combustion products found in cigarettes.15 (Figure 1) They consist
of three parts, a battery (Figures 2&3), atomizer (Figure 4) and a
liquid.16 The user pushes a button (Figure 5) and inhales to acti-
vate the device. The atomizer (heating element) turns the liquid
(Figure 6) into an aerosol or vapor that is inhaled to deliver of the
following ingredients:
1. Nicotine: Some liquid compositions contain nicotine and
some do not; consumers can choose which they prefer.
2. Humectant: Usually propylene glycol or glycerol for vapor
production.5 A humectant is a chemical used to keep objects
moist. Propylene glycol is a nearly odorless, clear, viscous
liquid. Propylene glycol is a preservative in food and is one of
the major ingredients in “e-liquid.” According to the MSDS
report on propylene glycol, the chemical is metabolized
into pyruvic acid, acetic acid, lactic acid and the potentially
hazardous substance propronaldehyde in the body. The
MSDS on propylene glycol and glycerol state they are gener-
ally considered to be safe and not carcinogenic. (https://www.
osha.gov/dts/chemicalsampling/data/CH_264480.html)
3. Flavoring: menthol, coffee, chocolate, cinnamon, vanilla, pina
colada and many more.5,17
4. Some brands have potentially harmful additives such as
animal carcinogens, genotoxins and other irritants.
Only e-cigarettes that are marketed for therapeutic pur-
poses are currently regulated by the FDA. An e-cigarette press
Figure 1E-Cigarette
Figure 2Battery component of e-cigarette
Figure 3Battery inside e-cigarette container
Figure 5Button on e-cigarette
Figure 6Tank that holds the wick and liquid components of e-cigarette
Figure 4Atomizer
1501RDH_59 59 1/8/15 10:20 AM

60 | rdhmag.com RDH | January 2015
release from the FDA on April 24, 2014 stated; “E-cigarettes
have not been fully studied, so consumers currently don’t know
the potential risks when used as intended, how much nicotine
or other potentially harmful chemicals are being inhaled during
use, or whether there are any benefits associated with using these
products. Additionally, it is not known whether e-cigarettes may
lead young people to try other tobacco products, including con-
ventional cigarettes, which are known to cause disease and lead to
premature death.”9,17 E-cigarettes are also not approved by the
FDA as part of a smoking cessation program.1,17
Smokeless Tobacco
People who use smokeless (dip, chew, snuff) tobacco have a 50-
fold increased risk for cancer of the mouth, cheek, tongue and gin-
giva than smokers.11 Snuff is a finely ground or shredded tobacco
that is either sniffed through the nose or placed between the cheek
and gum. Chewing tobacco is used by placing a preferred amount
inside the cheek and either spitting out the juices or swallowing.
Regardless of the delivery, all forms put a patient at an increased
risk for caries (due to sugar additives), periodontal disease, coro-
nary artery disease, heart attack, stroke, cancer of the esophagus,
oral cavity, pancreas and kidney.1,11,18,19
According to cancer.gov, smokeless tobacco products contain
many harmful chemicals, some of which are also present in ciga-
rettes. Below is a short-list of those chemicals.20,21
1. Nicotine
2. Nitrosamines: Directly related to cancer development accord-
ing to the National Cancer Institute.
3. Carcinogens called tobacco-specific nitrosamines 28+
4. Benzo(a)pyrene and other polycyclic aromatic carcinogens
5. Cadmium
6. Formaldehyde
7. Lead
8. Polonium 210
9. Acetaldehyde
10. Hydrazine
11. Uranium 235: Used in nuclear weapons.
12. Polycyclic aromatic hydrocarbons
13. Sodium, sugar, fiberglass, sand
According to the National Cancer Institute, smokeless tobacco
contains 28 cancer-causing agents. A panel of experts convened
by the National Institutes of Health in 2006 stated that the “range
of risks, including nicotine addiction, from smokeless tobacco
products may vary extensively because of differing levels of nico-
tine, carcinogens, and other toxins in different products.”23
Dental professionals are in an ideal position to identify epithe-
lial changes in the oral cavity associated with smokeless tobacco
use. Common oral changes seen in patients who smoke or use
smokeless tobacco can include, but are not limited to:
1. Leukoplakia: White plaque-like lesion of the oral mucosa that
cannot be rubbed off and cannot be diagnosed clinically as a
specific disease.18,24,25
2. Smokeless tobacco-associated keratosis: White lesion with
corrugated appearance resulting from an increase in keratin
formation.26 Located at the site in the mouth where smokeless
tobacco is held.18 Histologically, epithelial hyperplasia will
be seen and once the tobacco habit ceases, this condition is
reversible.25
3. Nicotine stomatitis: Often referred to as “pipe smoker’s pal-
ate.” The initial finding will be an erythematous hard palate
followed by hyperkeratosis and raised white-gray nodules
that are benign.25 This condition is reversible once the habit is
stopped.25
4. Melanosis: Brown to gray pigmentation found on the anterior
labial gingiva.25 When smoking ceases, it may take several
months or years for this condition to reverse.25
5. Oral squamous cell carcinoma (OSCC): According to
Mallory et al, smokeless tobacco increases a patients risk for
OSCC.19
6. Verrucous carcinoma: Considered as a low-grade form of
OSCC and often referred to as “snuff dipper’s cancer.”25 This
carcinoma will appear as a slow-growing tumor with a white
and red pebbly surface.25
7. Gingival recession, periodontal disease and attachment
loss24,26
8. Black hairy tongue26
9. Irritation of salivary glands25,26
SnusSnus is a Swedish term for “tobacco” where it was developed in
the 18th century. It is a small, tea bag-like pouch that is placed
under the upper lip for extended periods of time and there is no
need to spit. It is very different then snuff, chew or dip tobacco.
Snus comes in decorative tins that are flavored with mint or cin-
namon. The National Cancer Institute has expressed their public
health concern with this product and its apparent marketing ap-
peal to younger consumers.27 It is fairly new to the US market and
not all products are yet regulated by the FDA. There are varying
amounts of nicotine and carcinogens that are present in the type
of snus produced in the United States. The sale of snus is illegal
in the European Union and Russia.28 It is consumed primarily in
Norway, Denmark, Sweden and the USA.
Tobacco PharmacologyUnderstanding the pharmacology of nicotine will enhance the
practitioner’s understanding of the physiological effects of tobacco
use and will aid in tobacco cessation efforts. Nicotine is a natural
ingredient in tobacco leaves and is a human central nervous system
stimulant that is toxic.29 As a stimulant, it will increase a person’s
heart rate and blood pressure and its chronic use can lead to heart
disease, COPD, oral and lung cancer, gingiva and bone dete-
rioration, gastrointestinal disease, anorexia, allergies, and mouth
diseases such as leukoplakia and nicotine stomatitis.1 Nicotine is
tobacco’s psychoactive agent and its use leads to tolerance, depen-
dence and addiction.
1501RDH_60 60 1/8/15 10:20 AM

RDH | January 2015 rdhmag.com | 61
Addiction is defined as the pattern of abuse that includes com-
pulsive use of a substance despite any physical, financial or social
consequences. The presence of physical dependence is estab-
lished by the withdrawal or abstinence syndrome that occurs
when a person ceases use of the substance.30,31 Tolerance refers
to the dose of a drug that must be increased over time to pro-
duce the same effects.30,31 Nicotine produces a diminishing ef-
fect with time, which means the same dose of nicotine produces
less effect with consecutive dosing.30 More simply stated, the
nicotine user needs higher doses of nicotine over time to achieve
the desired physiological and psychological response.
Understanding the pharmacokinetics of nicotine will help
the practitioner understand the physical and addictive proper-
ties of nicotine and thus the reason why patients have a dif-
ficult time sustaining a cessation program. Due to the pH of
tobacco, nicotine is well absorbed through the mouth and has
rapid pulmonary absorption.32 Nicotine enters the lungs and
passes into arterial circulation by way of blood vessels lining
the sacs of the bronchi. It is delivered to the brain in less than
20 seconds, reaching peak plasma levels in 4-5 minutes.1,33 This
provides the user an instant “high” and fast relief from with-
drawal symptoms. Nicotine is then distributed throughout all
the body tissues, having the highest affinity for organs such as
the liver, spleen, kidney and lungs.33 Nicotine is metabolized
in the liver by several enzyme pathways. The most common
metabolite formed in the liver is cotinine, which accounts for
70-80% of nicotine metabolism. Since nicotine is excreted via
the urine, cotinine is used as a biomarker to determine if some-
one is using tobacco. Due to nicotine’s short half-life, it is not
a useful tool as a biomarker. Cotinine is a highly specific and
sensitive marker for tobacco use and has the advantages of a
longer half-life (16 hours).33 Cotinine will also allow for mea-
surements of ongoing exposure to tobacco both from first and
second hand smoke, but not always overall long-term exposure.
To determine long-term exposure, scientists will use nail and
hair samples or another metabolite marker in the urine.33,34
The rate of excretion of nicotine varies with many factors
such as diet, medical status, exercise, or use of pharmacological
drugs. On average, the plasma half-life of nicotine is about two
hours; 33 at which point, the “craving” for another dose of nico-
tine will begin to set in. The metabolism and therefore half-
life of any drug will vary based on many factors, such as age,
gender, medical status, disease state, age and diet; however, for
most people, two hours is the average half-life of nicotine.
Cessation
According to the CDC, in 2010, 2 out of 3 American adult
smokers wanted to quit and half made a formal quit plan. Den-
tal professionals are in a prime position within the community
to assist patients with a quit plan. Advice from health care
professionals has been shown to be a powerful influence on a
patient’s decision to stop or not begin using tobacco.1 There are
multiple agencies (hospitals, health departments, community
centers) and online programs to assist patients who wish to stop
using tobacco. The American Cancer Society hosts an annual
event whose goal is to promote tobacco cessation and encourage
participants to begin a quit plan called the “Great American
Smokeout.”2 The World Health Organization has multiple in-
tervention programs which have shown to reduce the intensity
of tobacco use and reduce overall tobacco consumption.2
The US government has implemented many laws and regu-
lations aimed at reducing tobacco use. They have increased
the price of tobacco products, implemented smoke-free laws
in workplaces and public areas, required warnings about the
dangers of tobacco use with anti-tobacco media campaigns and
enforced restrictions on tobacco advertising, promotion and
sponsorship. In 2012, the government approved the use of a
mass media depicting graphic personal stories of the adverse
health impacts of smoking. The 2009 Family Smoking Preven-
tion and Tobacco Control Act granted the FDA authority to
regulate manufacture, distribution and marketing of tobacco
products. Currently, many e-cigarette and snus products do
not fall under this Act and the FDA is petitioning to change
this.
Tobacco cessation causes many psychological as well as
physiological challenges to patients. Blood plasma levels of
nicotine have a half-life of two hours, at which time “cravings”
for nicotine will begin to set in. If the patient does not obtain
a dose of nicotine, physiological and psychological withdrawal
symptoms will begin to occur. This can include falling heart
rate and blood pressure, nausea, headache, increased hunger,
constipation, mood alterations (anxiety, irritability, depression)
and problems concentrating.35 Peak withdrawal symptoms
will appear within 2-3 days after cessation.35 Relapse rates are
highest within the first week after cessation due to these fac-
tors. Objectives of assisted cessation strategies are to reduce
withdrawal symptoms and make it easier for patients to abstain
from tobacco by partial replacement of nicotine or by counter-
acting nicotine’s physiological actions.30,31
Nicotine replacement therapies (NRTs) generally provide
plasma levels of nicotine in the range of the low-level cigarette
smoker.33 Normal nicotine levels in the blood plasma of smok-
ers is 1-1.5mg,33,37 and for oral snuff users is 3.6mg if held in the
mouth for 30min.33 NRT’s nicotine levels in the blood plasma
are as follows:
Form of NRT Delivery Nicotine Levels in Plasma
Patch 5mg(33,36)
Gum 2mg(33,36)
Nasal spray 0.7mg(33,38,39)
Inhaler 2mg(40)
Lozenge 1mg(41)
1501RDH_61 61 1/8/15 10:20 AM

62 | rdhmag.com RDH | January 2015
The patch is a transdermal delivery system while gum,
inhalers, and lozenges are transmucosal.1 Nasal sprays are
delivered via nasal mucous membranes.1 Nicotine replacement
gum is chewed until a peppery taste is achieved and then held
between the gum and buccal mucosa.1 Most gums and lozenges
are sweetened with xylitol and flavored with orange, mint or
cinnamon. The patch releases nicotine through the skin and is
sold in either 16 or 24 hour time intervals.1 To use the inhaler,
a patient merely holds the vapor in the mouth to deliver the
nicotine, they do not actually inhale.1 Common adverse ef-
fects of all these products include; taste disturbances, mouth
and jaw soreness, gastrointestinal disturbances such as nausea
and heartburn, nervousness and minor breathing difficulties.30
Toxic overdoses with these agents can lead to respiratory pa-
ralysis and death.30
Nicotine-free therapies are available and sold in the United
States. The first line pharmacological agents are bupropion
hydrochloride (Wellbutrin SR®, Zyban®) and varenicline tar-
trate (Chantix®, Champix®); both of which are approved by the
FDA as part of a tobacco cessation program. These pharma-
cological non-nicotine therapies are pregnancy category D and
could lead to teratogenic effects.30
Bupropion is classified as an atypical selective serotonin
reuptake inhibitor (SSRI) antidepressant drug that is used
to reduce nicotine cravings.1,30 Its mechanism of action is
presumed to be mediated by its ability to block the neuronal
uptake of dopamine and norepinephrine with little effect on
the reuptake of serotonin.30 This drug will increase the levels
of norepinephrine and dopamine in the brain which elevates
a person’s mood. Adverse effects reported with the use of
bupropion are dry mouth, insomnia, gastrointestinal distur-
bances, neurological (seizures) and neuropsychiatric effects
such as confusion, hostility and agitation.30
Varenicline is a selective partial agonist of the nicotinic
acetylcholine receptor.42 It stimulates nicotine receptors more
weakly than nicotine itself does and helps prevent nicotine
from exerting its full effects.30 The most common adverse
effects of varenicline are nausea, vomiting, constipation,
headaches, psychiatric disturbances, mental depression and
suicidal thoughts.30
Lastly, practitioners should not ignore the cognitive
changes that a patient will endure when they withdraw from an
addictive substance. In a 2012 publication from the National
Institute on Drug Abuse (a component of the US Department
of Health and Human Services), it was stated that “addic-
tion makes it difficult for patients to look beyond immediate
gratification to longer term consequences of their actions.”43
When patients were able to focus on the long-term health con-
sequences of their tobacco habit, they were more likely to be
successful with their quit plan.44 Cognitive behavior programs
lessen the emotional impact of cessation and therefore can
alter a patient’s behavior. This is an important component of
cessation programs dental health care professionals should be
involved in. They can assist their patient’s emotional cravings
for nicotine by following up with them in the form of a phone
call or email , as well as using positive reinforcement and en-
couragement each time they are seen in the dental office.
Conclusion
A simple fact exists in regards to all forms of tobacco presented
in this course; they all contain nicotine and carcinogens which
will lead to adverse health events. Newer products, such as
e-cigarettes and snus, are beginning to pose a new and seri-
ous health risk to Americans. They are being advertised as a
safer alternative to smoking and dip/chew tobacco use, when
in fact, there is no sound research to support this claim. The
FDA is chasing companies that promote and manufacture
these products to require them to place the proper warnings on
their products. Until the day comes when all companies will
be held to the same standards as traditional tobacco product
lines, American’s safety is at an increased risk. Dental profes-
sionals should be leading the way in the health care community
by promoting cessation and total body health and wellness.
References
1. Wilkins E. Clinician Practice of the Dental Hygienist. 11th
ed. Philadelphia:PA, Lippincott Williams and Wilkins Wolters
Kluwer Health. Jan 2012.
2. CDC. Current Cigarette Smoking Among Adult – United States,
2011. Morbidity and Mortality Weekly, Report, 2012;61(44):889-
894.
3. CDC. Smoking-attributable mortality, years of potential life lost,
and productivity losses-United states, 2000-2004. Morbidity and
Mortality Weekly Report, 2008;57:1226-8.
4. CDC. State-specific trends in lung cancer incidence and
smoking-United States, 1999-2008. MMWR, 2011;60:1243-7.
5. Henry R, Henderson R. “The rise of e-cigarettes.” Dimension of
Dental Hygiene. May 2014;12(5):46-50.
6. American Lung Association Smoking Cessation: The Economic
Benefits. Accessed online June 22, 2014 at lung.org/stop-
smoking/tobacco-control-advocacy/reports-resources/
cessation-economic-benefits/states/united-states.html.
7. US Department of Health and Human Services: National
Institute of Health: Smokeless Tobacco-A Guide for quitting.
Publication No. 12-3270. August 2012. Accessed online June 27,
2014 at http://www.nidcr.nih.gov/NR/rdonlyres/0AA37918-
9A15-49C5-B982-6D93E6118D11/0/SmokelessTobacco.pdf\
8. Mason, Josh. Camel Snus vs. Marlboro Snus. May 14, 2012.
Accessed online June 27,2014 at http://voices.yahoo.com/
camel-snus-vs-marlboro-snus-5983126.html?cat=46
9. CDC. Notes from the field: electronic cigarette use among
middle and high school students-United States, 2011-2012.
Morbidity and Mortality Weekly Report, 2013;62(35): 729-30.
10. FDA. Electronic Cigarettes (e-Cigarettes). Public health focus,
2014 April 24. Accessed April 20,2014 online at http://www.fda.
gov/newsevents/publichealthfocus/ucm172906.htm.
11. Lewis S. Medical-Surgical Nursing: Assessment and
Management of Clinical Problems. 7th ed. Elsevier Health
Sciences. St. Louis:Missouri. 2007.
12. Korte JE, Hertz-Picciotto I, Schulz MR, Ball LM, Duell EJ. The
contribution of benzene to smoking-induced leukemia. Environ
Health Perspect. Apr 2000;10(4):333-9.
1501RDH_62 62 1/8/15 10:20 AM

RDH | January 2015 rdhmag.com | 63
13. CDC. Great American Smokeout and Current Cigarette Smoking
in Adults-United States 2011. MMWR 2012;61(44):889-894.
14. Bell K, Keane H. Nicotine control: e-cigarettes smoking and
addiction. IInt J Drug PolicyI. 2012;23:242-47.
15. Caponnetto P, Campagna D, Papale G, Russo C, Polosa R. The
emerging phenomenon of electronic cigarettes. Expert Rev
Respir Med. Feb 2012;6(1):63-74.
16. Ayers JW, Ribisl KM, Brownstein JS. Tracking the rise in
popularity of electronic delivery systems using search query
surveillance. Am J Prev Med. 2011;40:448-53.
17. Food and Drug Administration. FDA warns of health risks posed
by e-cigarettes. Accessed June 22, 2014 at fda.gov/downloads/
forconsumers/consumerupdates/UCM173430.pdf.
18. Ibsen O, Phelan J. Oral Pathology for the Dental Hygienist. 6th
ed. New York: NY, Elsevier Health Sciences. March 2013.
19. Mallery S, Tong M, Michaels G. Clinical and Biochemical
studies supports smokeless tobacco’s carcinogenic potential in
the human oral cavity. Cancer Prev Res. Jan 2014;7:23-32.
20. Rice, C. What’s in Dip? So you think all you get is a buzz huh?
Texas A&M AgriLife Extension Service, Texas 4-H, and the
Cancer Prevention and Research Institute of Texas. May 15,
2003. Accessed April 20,2014 at http://dontdip.tamu.edu/
ingredients.htm.
21. National Cancer Institute. Cancer Topics: Smokeless Tobacco.
Accessed April 20,2014 at http://www.cancer.gov/ cancertopics/
tobacco/smokeless-tobacco.
22. American Cancer Society. Smokeless Tobacco: What in tobacco
smoke is harmful? 2014 Feb 13. Accessed online April 20,2014 at
http://www.cancer.org/cancer/cancercauses/tobaccocancer/
questionsaboutsmokingtobaccoandhealth/questions-about-
smoking-tobacco-and-health-cancer-and-health.
23. NIH State of the Science Panel. National Institutes of Health
State of the Science conference statement: tobacco use:
prevention, cessation, and control. Annals of Internal Medicine.
2006;145(11):839-44.
24. Kallischnigg G, Weitkunat R, Lee P. Systematic review of the
relation between smokeless tobacco and non-neoplastic oral
diseases in Europe and the United States. BMC Oral Health.
2008;8(13). Accessed online June 27,2014 at http://www.
biomedcentral.com/1472-6831/8/13
25. Ibsen O. Diagnosing smoking-related lesions. Dimensions
of Dental Hygiene. Sept 2004 accessed online June 29,2014
at http://www.dimensionsofdentalhygiene.com/2004/09_
September/Departments/Oral_Pathology.aspx
26. Taybos G. Oral changes associated with tobacco use. Am J Med
Sci. Oct 2003;326(4):179-182.
27. Phillips, C. A New Tobacco Threat? NCI Cancer Bulletin. Feb
2007;4(8):5-6. Accessed online May 25, 2014 at http://www.
cancer.gov/ncicancerbulletin/archive/2007/022007.pdf.
28. Cohen, A. EU Tobacco Ban Meets It’s Swedish Match. Feb
8, 2008. The wall street journal. Accessed online June 20,2014
http://online.wsj.com/news/articles/SB120242666285452015.
29. Darby M. Mosby’s Comprehensive Review of Dental Hygiene.
7th ed. New York:NY, Elsevier Health Sciences. October 2011.
30. Hinter H, Nagle B. Pharmacology An Introduction. 6th ed. New
York: NY, McGraw Hill, 2012.
31. Haveles E. Applied Pharmacology for the Dental Hygienist. 6th
ed. MI: Maryland Heights, Mosby Elsevier, 2011.
32. Pankow JF. A consideration of the role of gas/particle
partitioning in the deposition of nicotine and other tobacco
smoke compounds in the respiratory tract. Chem Res Toxicol.
2001;14(11):1465-81.
33. Benowitz NL, Hukkanen J, Jacob P. Nicotine Chemistry,
Metabolism, Kinetics and Biomarkers. Handb Exp Pharmacol.
2009;192:29-60.
34. Al-Delaimy WK, Crane J, Woodward A. Is the hair nicotine
level a more accurate biomarker of environmental tobacco smoke
exposure than urine cotinine? J Epidemiol Community Health.
2002;56(1):66-71.
35. Dugdale D. Nicotine and tobacco. ADAM Encyclopedia online.
2014. Accessed May 25, 2014 at http://www.nlm.nih.gov/
medlineplus/ency/article/000953.htm.
36. Schneider NG, Olmstead RE, Franzon MA, Lunell E. The
nicotine inhaler: clinical pharmacokinetics and comparison with
other nicotine treatments. Clin Pharmacokinet. 2001;40(9):661-
684.
37. Benowitz NL, Jocob P, Ahijevych K,Jarvis MJ, Hall S, LeHouezec
J, Hansson A, Lichtenstein E, Henningfield J, Tsoh J, Hurt RD,
Velicer W. Biochemical verification of tobacco use and cessation.
Nicotine and Tobacco Research. 2002;4:149-159.
38. Gourlay SG, Benowitz NL. Arteriovenous differences in plasma
concentration of nicotine and catecholamines and related
cardiovascular effects after smoking, nicotine nasal spray, and
intraveneous nicotine. Clin Pharmacol Ther. 1997;62(4):453-63.
39. Johansson CJ, Olsson P, Bende M, Carlsson T, Gunnarsson PO.
Absolute bioavailability of nicotine applied to different nasal
regions. Eur JClin Pharmacol. 1991;41(6):585-88.
40. Molander L, Lunell E, Anderson SB, Kuylenstierna F. Dose
released and absolute bioavailability of nicotine from a nicotine
vapor inhaler. Clin Pharmacol Ther. 1996;59(4):394-400.
41. Choi JH, Drersler CM, Norton MR, Strahs KR. Pharmacokinetics
of a nicotine polacrilex lozenge. Nicotine Tob Res. 2003;5(5):635-
44.
42. Faessel HM, Obach RS, Rollema H, Ravva P, Williams KE,
Burstaein AH. A review of the clinical pharmacokinetics and
pharmacodynamics of varenicline for smoking cessation. Clin
Pharmacokinet. Dec 2010;49(12):799-816.
43. Whitten L. Cognitive Strategy Reduces Craving by Altering Brain
Activity. Research news and trends from the National Institute
on Drug Abuse. Apr 2012;24(2):1-6.
44. Kober H. Regulation of craving by cognitive strategies in cigarette
smokers. Drug and Alcoh Dependence. 2010. 6(i):52-55.
Author Profile
Lisa Dowst-Mayo, RDH, BSDH graduated from Baylor College
of Dentistry in 2002 and is currently pursuing a Master’s degree
in Healthcare Administration from Ohio University. She is an
active member in ADHA and is a full time professor at Concorde
Career College in San Antonio. She is a published author and na-
tional speaker and can be contacted through her website at www.
lisamayordh.com. She is also the co-owner of Diamond Dental
Education (www.diamonddentaleducation.com).
Author Disclosure
Lisa Dowst-Mayo has no commercial ties with the sponsors or
providers of the unrestricted educational grant for this course.
1501RDH_63 63 1/8/15 10:20 AM

64 | rdhmag.com RDH | January 2015
Online CompletionUse this page to review the questions and answers. Return to www.ineedce.com and sign in. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase.
Once purchased the exam will be added to your Archives page where a Take Exam link will be provided. Click on the “Take Exam” link, complete all the program questions and submit your answers. An immediate grade
report will be provided and upon receiving a passing grade your “Verification Form” will be provided immediately for viewing and/or printing. Verification Forms can be viewed and/or printed anytime in the future by
returning to the site, sign in and return to your Archives Page.
Questions
1. What is the single largest preventable cause
of death in the United States?a. Tobacco useb. Alcohol usec. HIVd. Motor vehicle accidents
2. What percentage of Americans currently
smoke?a. 10%b. 19-20%c. 50%d. 70%
3. What is the estimated annual costs in direct
medical expenses associated with tobacco
use in the US?a. $1 millionb. $10 millionc. $1 billiond. $96 billion
4. Which of the following occurred regarding
the percentage of Americans who smoke
more than 30 cigarettes per day since 2005?a. Increasedb. Decreasedc. Stayed the samed. None of the above
5. Which of the following occurred regarding
the percentage of Americans who smoke less
than 9 cigarettes per day since 2005?a. Increasedb. Decreasedc. Stayed the samed. None of the above
6. Tobacco use rates are highest among which
of the following?a. People who live in the midwestb. People who live in the southc. Non-high school graduatesd. All of the above
7. How many compounds found in cigarettes
are classified as carcinogens?a. 2b. 20c. 45d. 75
8. Which of the following chemicals contained
in cigarettes will lead to a decrease in oxygen
consumption in the body as a whole?a. Carbon monoxideb. Nicotinec. Ammoniad. Benzene
9. Which of the following chemicals can be
found in cigarettes?a. Cyanideb. Formaldehydec. Acetylened. All of the above
10. Which chemical found in cigarettes can
predispose a patient to leukemia?a. Benzeneb. Tarc. Nicotined. Formaldehyde
11. Which chemical found in cigarettes is
responsible for the sticky, brown staining on
teeth?a. Nicotineb. Tarc. Cadmium d. Formaldehyde
12. What is the percentage of COPD case
attributable to smoking?a. 10%b. 20%c. 50%d. 80%
13. What is the percentage of cancer deaths
attributable to smoking?a. 10%b. 30%c. 50%d. 80%
14. Which of the following chemicals can be
found in smokeless tobacco?a. Formaldehydeb. Leadc. Polonium 210d. All of the above
15. Where was snus originally developed?a. Denmarkb. Swedenc. USAd. Russia
16. Where is the sale of snus illegal?a. USAb. Swedenc. Russiad. Denmark
17. Nicotine is a CNS stimulant which can lead
to which of the following?a. Increased heart rateb. Decreased heart ratec. Decreased pulsed. Sedation
18. Nicotine use will lead to which of the
following?a. Toleranceb. Addictionc. Dependenced. All of the above
19. After nicotine ingestion, peak plasma levels
will be reached in:a. 1-2 minutesb. 4-5 minutesc. 20 minutesd. 1 hour
20. Nicotine has a high affinity for the:a. Spleenb. Lungsc. Kidneysd. All of the above
21. What is the average half-life of nicotine in
the human body?a. 30 minutesb. 1 hourc. 2 hoursd. 24 hours
22. What agency sponsors the “Great
American Smokeout”?a. American Cancer Society b. FDAc. EPAd. CDC
23.Nicotine replacement therapies generally
provide plasma levels of nicotine in the
range of the:a. High-level cigarette smokerb. Low-level cigarette smokerc. High-level smokeless userd. None of the above
24. What is the range of nicotine levels in the
blood plasma of smokers?a. 1-1.5mgb. 2-2.5mgc. 3-3.5mgd. 4-4.5mg
25. All of the following are approved tobacco ces-
sation products approved by the FDA except:a. Bupropion hydrochloride(Wellbutrin SR®, Zyban®) b. Varenicline tartrate(Chantix®)c. Electronic cigarettesd. Nicotine patches
26. Which of the following nicotine replace-
ment therapies delivers nicotine via a
transmucosal system?a. Inhalerb. Gumc. Lozenged. All of the above
27. Which of the following nicotine replace-
ment therapies delivers nicotine via a
transdermal system?a. Inhalerb. Gumc. Lozenged. Patch
28. Which nicotine-free pharmacological agent
assists the patient with cessation by blocking
the neuronal uptake of dopamine and
norepinephrine?a. Bupropion hydrochloride(Wellbutrin SR®, Zyban®) b. Varenicline tartrate(Chantix®)c. Electronic cigarettesd. Nicotine patches
29. Both bupropion hydrochloride (Wellbutrin
SR®, Zyban®) and varenicline tartrate
(Chantix®) are medications that fall into
which pregnancy category?a. Ab. Bc. Dd. X
30. Which nicotine-free pharmacological agent has adverse side effects of nausea, vomiting, constipation, headaches, psychiatric disturbances, mental depression and suicidal
thoughts?a. Bupropion hydrochloride(Wellbutrin SR®, Zyban®) b. Varenicline tartrate(Chantix®)c. Electronic cigarettesd. Nicotine patches
1501RDH_64 64 1/8/15 10:20 AM
Customer Service 216.398.7822
ANSWER SHEET
“Puff, Not the Magic Dragon… The Cost of America’s Tobacco Use”
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone: Home ( ) Office ( )
Lic. Renewal Date: AGD Member ID:
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3)
Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 3 CE credits. 6) Complete the Course
Evaluation below. 7) Make check payable to PennWell Corp. For Questions Call 216.398.7822
Educational Objectives
1. Correlate their patient’s tobacco use with the adverse effects to their general health and well-being and be familiar
with the risk factors associated with tobacco use.
2. Identify patients at higher risk for tobacco abuse by understanding current statistical trends.
3. Discuss the different forms of tobacco products currently on the market in the United States and their components
4. Discuss the difficulties patients have sustaining a quit plan and why relapse rates are high for tobacco users.
Course Evaluation1. Were the individual course objectives met?
Objective #1: Yes No Objective #2: Yes No
Objective #3: Yes No Objective #4: Yes No
Please evaluate this course by responding to the following statements, using a scale of Excellent = 5 to Poor = 0.
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Please rate the usefulness and clinical applicability of this course. 5 4 3 2 1 0
9. Please rate the usefulness of the supplemental webliography. 5 4 3 2 1 0
10. Do you feel that the references were adequate? Yes No
11. Would you participate in a similar program on a different topic? Yes No
12. If any of the continuing education questions were unclear or ambiguous, please list them.
________________________________________________________________
13. Was there any subject matter you found confusing? Please describe.
_________________________________________________________________
14. How long did it take you to complete this course?
_________________________________________________________________
15. What additional continuing dental education topics would you like to see?
_________________________________________________________________
For IMMEDIATE results, go to www.ineedce.com to take tests online.
Answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
Payment of $59.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: ______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
If not taking online, mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
AGD Code 158
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
PUFF0115RDH
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification of Participation forms will be mailed within two weeks after taking an examination.
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 3 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $20.00 to $110.00.
PROVIDER INFORMATIONPennWell is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, not does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE Provider may be directed to the provider or to ADA CERP ar www.ada.org/cotocerp/
The PennWell Corporation is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing dental education programs of this program provider are accepted by the AGD for Fellowship, Mastership and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from (11/1/2011) to (10/31/2015) Provider ID# 320452
RECORD KEEPINGPennWell maintains records of your successful completion of any exam for a minimum of six years. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
IMAGE AUTHENTICITYThe images provided and included in this course have not been altered.
© 2014 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
1501RDH_65 65 1/8/15 10:20 AM


![Encyclopaedia - thyamath.comD20]Encyclopaedia_Arcane-Dragon...4 Dragon Magic – An Overview D ragons are able to harness the power of magic without study or training, bringing forth](https://img.pdfslide.us/doc/110x75/5b2cbe017f8b9ad76e8b6917/encyclopaedia-d20encyclopaediaarcane-dragon4-dragon-magic-an-overview.jpg)






![Encyclopaedia - thyamath.comthyamath.com/donjons/[D20]Encyclopaedia_Arcane-Dragon_Magic-Power... · Alejandro Melchor Encyclopaedia Arcane Dragon Magic Contents 2 Introduction 4 Dragon](https://img.pdfslide.us/doc/110x75/5e0cbe25cbf8a63625201b2d/encyclopaedia-d20encyclopaediaarcane-dragonmagic-power-alejandro-melchor.jpg)







![D&D 3.5 - Dragon Magic [OCR]](https://img.pdfslide.us/doc/110x75/5450cfe4b1af9fc8038b493e/dd-35-dragon-magic-ocr-55844afe19a27.jpg)