Embed Size (px)
Citation preview

PUBLIC PUBLIC && PRIVATE HEALTH PRIVATE HEALTH CARE IN CANADACARE IN CANADA
before theCanadian Pension & Benefits Institute
Winnipeg - June 15, 2007
by Norma Kozhaya, Ph.D.Economist, Montreal Economic Institute

Possible private contribution
• Possible private contribution in the health care sector:– Out-of-pocket financing – Private insurance – Private provision of publicly funded services– PPP
• I will focus more specifically on the role of private insurance

• Canada is the only OECD country that prohibits the possibility of private insurance for medically required services (through provincial legislation).
• Canada is also one of the « biggest spenders » on health care
• What are the results? Value for our money?
Context

• Health care spending accounts for more than 10% of our GDP (70% public, 30% private)
• With inflation taken into account, per capita public health care spending doubled in 30 years (CIHI).
Financial sustainability

• More than 33% of total provincial government revenues are spent on health care
• In Quebec: 44% of provincial program spending goes toward health care in 2006 compared to 35% in 1990.
Financial sustainability

Factors driving growth:– Population aging (the share of the elderly
in the population 14% today, 23% in 2026)
– Technology– New drugs
Growth Projections for Canada: Increase of 4% of GDP by 2040, (CD Howe), 4,2% in 2050, (OECD)
Financial sustainability
5,5
5,9
6,5
7,2
7,4
7,5
7,7
7,9
7,9
8,0
8,0
8,2
8,3
8,7
8,9
9,1
9,2
9,3
9,6
9,8
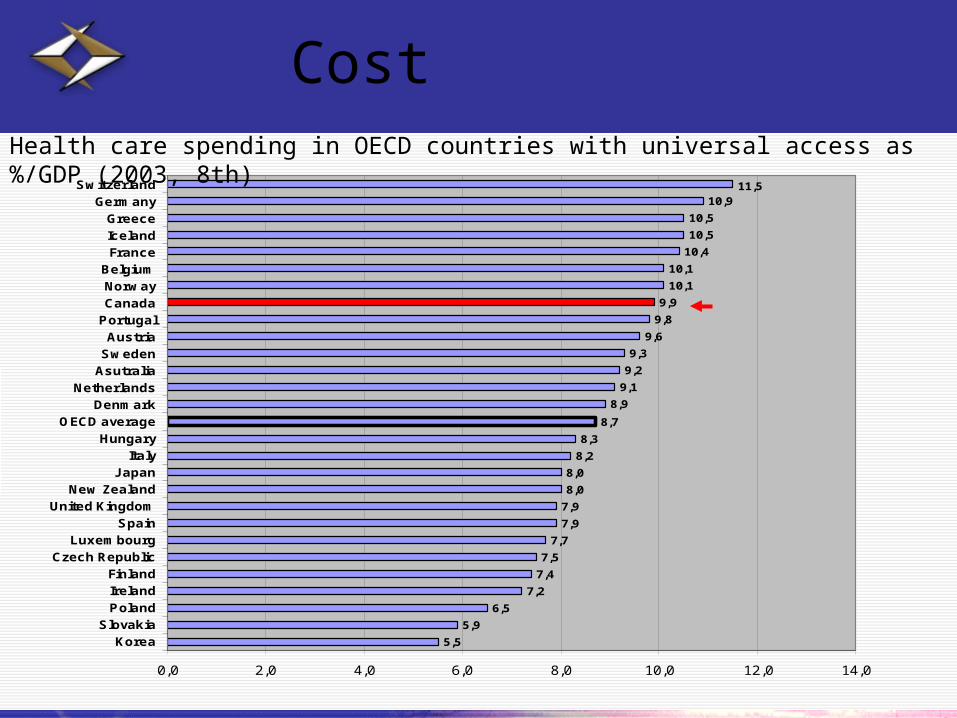
9,9
10,1
10,1
10,4
10,5
10,5
10,911,5
0,0 2,0 4,0 6,0 8,0 10,0 12,0 14,0
Korea
Slovakia
Poland
Ireland
Finland
Czech Republic
Luxembourg
Spain
United Kingdom
New Zealand
Japan
Italy
Hungary
OECD average
Denmark
Netherlands
Asutralia
Sweden
Austria
Portugal
Canada
Norway
Belgium
France
Iceland
Greece
Germany
Switzerland
Health care spending in OECD countries with universal access as %/GDP (2003, 8th)
Cost

Different measures of health care system performance; two are of particular relevance for Canada:
– Access
– Waiting time
Cost and results

1,4
1,7
2,1
2,3
2,3
2,5
2,6
2,8
2,8
2,9
2,9
2,9
3,0
3,0
3,1
3,1
3,2
3,2
3,3
3,4
3,5
3,6
3,6
3,7
3,7
3,7
4,2
4,3
0,0 1,0 2,0 3,0 4,0 5,0
TurkeyJapan (2002)
United KingdomCanadaFinland
South KoreaNew ZealandLuxembourg
PolandAustraliaGermany
SpainDenmarkSweden
HungaryPortugal
FranceIrelandAustriaNorway
SwitzerlandBelgium
ItalyCzech republic
NetherlandsSlovakia
GreeceIceland
Number of doctors per 1000 inhabitants (24th)
Cost and results

1000
1500
2000
2500
3000
1993 1999 2005
co
nsta
nt
2005 d
ollars
5
7
9
11
13
15
17
19
weeks
Public spending per capita and waiting times in Canada1993-2005
Source: Fraser Institute; Canadian Institute for Health Information
Cost and results

• Private health insurance plays varying roles in OECD countries and fulfills different functions within health care systems.
• Five categories of insurance, from the most comprehensive to those complement to the public system.
Private health insurance

• Among the five categories of insurance, only one, supplementary insurance, is already established in Canada for uninsured services.
• Three of the other four are unlikely to be offered, even following the Chaoulli ruling, because of the legal obstacles that remain.
Private health insurance

Private insurance: new opportunities
Duplicate insurance
• Individuals remain insured with the public system while paying for the option of being treated in a parallel private system, with no commitment of public funds to cover this care
• Exists notably in Finland, Italy, U.-K., Australia, Ireland

• For greater overall financing.
• For more capacity to treat patients (more beds, more equipment, more operating rooms, etc.)
• To create more work in the private sector for existing medical staff, underused in the public system because of salary caps and quotas.
Private insurance: new opportunities

Private insurance: new opportunities
• To repatriate thousands of doctors and nurses working abroad.
• Without private insurance, only the wealthiest Canadians could obtain private treatment, often outside Canada, paying directly from their pockets

• User fees (exist in 78% of OECD countries).
(Need to change the Canada Health Act eventually)
• Private provision of publicly funded services (Sweden, France, U.-K.)
Other possible private contribution

Public opinion
52%
42%
6%
65%
33%
1%
YES NO DON'T KNOW
CANADA QUEBEC
Question: Would you find it acceptable or not if the government were to allow those who wish to pay for healthcare in the private sector to have speedier access to this type of care while still maintaining the current free and universal healthcare system?
Conclusion
• It’s not part of Canadian values to let people suffer on waiting lists.
• The private sector does not threaten the public sector as OECD countries experience shows.




![april 8-11, 2009 knox centre 400 edmonton street winnipeg ... · Jesus Camp Fri 1:00 Jesus Christ Superstar [Singalong!] Sat 8:00 Jesus de Montreal [Jesus of Montreal] Sat 1:00](https://img.pdfslide.us/doc/110x75/5f099b897e708231d427a520/april-8-11-2009-knox-centre-400-edmonton-street-winnipeg-jesus-camp-fri-100.jpg)