Embed Size (px)
Citation preview
Public Health andWorld Bank Operations
The World Bank
The Human Development NetworkHealth, Nutri t ion, and Population Series
Copyright © 2002The International Bank for Reconstructionand Development/THE WORLD BANK1818 H Street, N.W.Washington, D.C. 20433, U.S.A.
All rights reserved

HEALTH, NUTRITION, AND POPULATION SERIES
This series is produced by the Health, Nutrition, and Population Family (HNP)of the World Bank’s Human Development Network. It provides a vehicle forpublishing polished material on the Bank’s work in the HNP sector, for consoli-dating previous informal publications, and for improving the standard for qualitycontrol, peer review, and dissemination of high quality analytical work.
The series focuses on publications that expand our knowledge of HNP policyand strategic issues that can improve outcomes for the poor and protect vulnera-ble populations against the impoverishing effects of illness. Best practice exam-ples of both global and regional relevance are presented through thematicreviews, analytical work, and case studies.
The Editor in Chief of the series is Alexander S. Preker. Other members of theEditorial Committee are Mukesh Chawla, Mariam Claeson, ShantayananDevarajan, Gilles Dussault, A. Edward Elmendorf, Armin H. Fidler, Charles C.Griffin, Jeffrey S. Hammer, Peter F. Heywood, Prabhat Jha, Gerard Martin LaForgia, Jack Langenbrunner, Ruth Levine, Maureen Lewis, Samuel S.Lieberman, Benjamin Loevinsohn, Elizabeth Lule, Akiko Maeda, Judith SnavelyMcGuire, Milla McLachlan, Thomas W. Merrick, Philip Musgrove, OkPannenborg, Oscar Picazo, Mead Over, Juan Rovira, George Schieber, andAdam Wagstaff.


v
TABLE OF CONTENTS
Acknowledgements vii
Executive Summary ix
Introduction 1
1 What Is Public Health? 4
A Working Definition: Public Health Categories and Functions 4Why Think in Terms of Functions? 6
2 What Are the Scope and Boundaries of Public Health 8
The Scope of Public Health 8Public Health and Clinical Care 8The Interface of Public Health and Health Systems Development 11
3 Why Should the Bank Invest More in Public Health 13
4 What Are the Bank’s Strategic Options 16
The Role of the Bank at Country Level: Strategic Options 16The Global Role of the Bank: Strategic Options 17
5 Conclusion: Public Health and the World Bank 20
Bibliography 26
Annexes
Annex 1. The Millennium Development Goals for Health,Nutrition and Population 21
Annex 2. “Essential” Public Health Functions (PAHO/CDC/WHO) 22
Tables
Table 1. Public Health Categories and Examples of Functions 5Table 2. Selected Public Health Functions Applied to
Various Health Concerns 7

Boxes
Box 1. Brazil Disease Surveillance and Control Project (VIGISUS) 6Box 2. Road Safety: Working Across Sectors with Governments,
Civil Society and the Private Sector 9Box 3. A Multi-Sectoral Approach to Reducing Indoor Air Pollution 9Box 4. Focused Resources on Effective School Health (FRESH) 10Box 5. Clinical Care and Public Health: The TB Scenario 11Box 6. Achieving Child Health and Nutrition Outcomes 14Box 7. Roll Back Malaria: Aiming at Sustainable Impact through
Sector-Wide Approaches 15Box 8. Partners in Public Health 18
Figures
Figure 1. Public Health and the Health Care System Pyramid 10Figure 2. Determinants of Health-Sector Outcomes 12
vi

ACKNOWLEDGEMENTS
The Public Health Thematic Group would like to thank all those who con-tributed to the development of this public health note through the many inter-views, seminars and discussions organized during the period 1999–2001. Specialthanks go to those who contributed with background work, boxes and figures, orwho devoted time to review and comment on earlier drafts.
The public health note was prepared by Mariam Claeson, A. EdwardElmendorf, Daniel S. Miller and Philip Musgrove.
This note would not have been possible without the support of and collaborationwith our many partners, and we would like especially to acknowledge the supportfrom the World Health Organization, the Pan American Health Organizationand the U.S. Centers for Disease Control and Prevention.
vii

ix
EXECUTIVE SUMMARY
• The World Bank’s commitment to achieving good health, nutrition andpopulation outcomes, including its commitment to the MillenniumDevelopment Goals and the adoption of a Poverty Reduction Strategyframework, underscores the importance of embracing the principles andpractices of public health. Effective public health interventions are directlyrelated to achieving the Millennium Development Goals. Public healthknowledge, advisory services and capacity building are key instruments fordevelopment effectiveness.
• For Bank operational purposes, major public health functions can begrouped into five basic categories: policy development; collection and dis-semination of evidence for health policies, strategies and actions; preventionand control of disease; inter-sectoral action for better health; and humanresource development and capacity building.
• A wide range of activities fall within these basic categories of public healthfunctions, such as surveillance, regulation, evaluation, social mobilization,disease prevention and control and workforce development. Classifyingpublic health functions into a limited number of categories helps to define essential public health functions within each country context,assess public health performance gaps and estimate financial investmentneeds in public health.
• Public health functions are complementary to and supportive of more tradi-tional, vertical program approaches. They provide important mechanisms formonitoring and evaluation in country-specific efforts, in the formulation andimplementation of Poverty Reduction Strategies and in Bank projects.
• Strategic options for an enhanced World Bank role in public health at thecountry level include prioritizing public health action in policy dialogue andlending; assessing performance of public health functions; including publichealth functions in poverty reduction strategy papers, country assistancestrategies and comprehensive development frameworks; and customizingsolutions and investments.
• In addition to the role of public health in the Bank’s country operations, theBank has complementary and mutually reinforcing global roles in publichealth. These include: a) managing and disseminating knowledge on publichealth and public health functions; b) conducting analytic work related topublic health functions; c) selectively engaging in global health initiativesthat will help countries make measurable progress towards their health,nutrition and population goals; d) building capacity for poverty reduction;and e) improving Bank and client performance.

x
• Health, nutrition and population (HNP) staff must take the lead to facilitateand monitor the application and strengthening of public health perspectivesat the country level. Financially and otherwise, the Bank is already engagedin many country-level dimensions of public health. However, in order toincrease its effectiveness, the Bank should broaden and deepen that engage-ment within and across the five categories of public health activities. Doingso is consistent with the Bank’s global and HNP missions, its values, itsmulti-sectoral character and its institutional areas of comparative advantage.

The twentieth century witnessedgreater gains in health, nutrition andpopulation outcomes than at anyother time in history. These gains arepartly the result of improvements inincome and education, with accom-panying improvements in nutrition,access to contraceptives, hygiene,housing, water supplies and sanita-tion. They are primarily the result ofnew knowledge about the causes, pre-vention and treatment of disease, andthe introduction of policies that makesuch interventions more accessible.
As a result of complex synergiesamong income levels, education,behavior, public policy and healthservices, people now live almost twen-ty-five years longer than they wouldhave at similar income levels in 1900.Many of the interventions that haveimproved health are attributable toenvironmental changes and are theresult of public health actions. Thecontrol of diarrheal diseases, including
the development of oral rehydrationtherapy to reduce child mortality, isone example. Smallpox eradicationmade possible through a combinationof advances in public health researchand effective program management, isanother example of a successful twen-tieth century public health effort.
However, the improvements in healthstatus and life expectancy have notbeen equally distributed. The healthstatus and life expectancy of the poor-est nations lag behind the rest of theworld. Within countries, the healthof the poor is worse than that of therest of the population. Poverty is themost important underlying cause ofpreventable death, disease and disabil-ity; and there is growing recognitionthat poor health, malnutrition andlarge family size are key determinantsof poverty (Claeson et al. 2001).Beyond the health sector, literacy, thestatus of women, housing quality, safewater, sanitation, food supply and
urbanization are other key determi-nants of health status that interactwith poverty.
For these reasons, enormous chal-lenges remain (adapted from Mersonet al. 2000):
• More than 10 million childrenbelow age 5 die each year frompreventable causes; 70 percent ofthese deaths are due to pneumo-nia, diarrhea, malaria, malnutri-tion and measles;
• More than 150 million marriedwomen who want to space orlimit child bearing do not haveaccess to modern contraceptives;
• Nearly 600,000 women die annu-ally from complications of preg-nancy and childbirth, and another18 million suffer pregnancy-relat-ed health problems that can bepermanently disabling;
1
Introduction

• Each year 13 million persons diefrom infectious diseases, most ofwhich are preventable or curable;half of these deaths are in adultsand are due to tuberculosis,malaria and HIV/AIDS;
• Thirty percent of the world isstill without access to safe waterand sanitation systems; and
• As populations age and thetobacco epidemic takes hold,most developing regions are likelyto see noncommunicable diseasesbecome leading causes of disabili-ty and premature death. Over thenext twenty-five years, millions ofadults will be affected by heartdiseases, depression, stroke, can-cers and chronic respiratory dis-eases. Traffic injuries are alreadyemerging as a major threat tohealth in developing countries.
The World Health Organization’sWorld Health Report 1999 identifiedfour major challenges to world health (WHO 1999) that the inter-national community must address:reduction of excess mortality andmorbidity among the poor; invest-ing in research and developmentdirected toward diseases of the poor; countering threats to healthresulting from economic crises,unhealthy environments and riskybehaviors; and development of more effective and efficient healthsystems that can improve health sta-tus, reduce health inequities andenhance responsiveness to clients’expectations.
The Bank has given increasing atten-tion to health in recent years. Bank
lending and analytical work in thehealth sector have grown dramatically,peaking above $2 billion in new com-mitments in FY96 and FY98. Thework is guided globally by the Bank’s1997 health, nutrition and population(HNP) sector strategy, which positsthree overall goals for the Bank inhealth—improving health outcomesfor the poor, increasing the efficiencyof health care and other services, andfacilitating sustainable health financ-ing (World Bank 1997a).
The Bank is well placed to increase itscontribution to national and globalefforts to address the challenges tohealth in this new decade, as shownby its commitments to:
• the Millennium DevelopmentGoals, particularly the goals in-volving maternal and child health,nutrition, poverty and the majorcommunicable disease targets;
• Poverty Reduction Strategies(PRSs), with growing emphasis onpoverty and health outcomes, link-ing actions at the household levelwith government policy and action;
• global public and private partner-ships to deal more effectivelywith cross-border health issuesand global public goods; and
• sustainable development and across-sectoral approach to dealingwith multi-sectoral determinantsof health and nutrition.
This strategy note is meant to con-tribute to debate about the appropri-ate roles, functions and services ofdeveloping-country institutions and
their partners in addressing healthissues. The intended audienceincludes HNP operations staff; devel-oping-country managers with health-related responsibilities; country andsector managers; staff in other sectorswhose work has significant healthimpact; and, health policy analysts.The note will be accompanied by aPublic Health Resource toolkit/web-site providing practical, operationallyoriented tools, best practices andguidance derived from interviews withBank staff as well as contributionsfrom partner agencies. The toolkitwill assist Bank staff and clients inidentifying, analyzing and financingpublic health functions appropriate tothe epidemiological, financial andinstitutional capacities of individualborrowing countries. Information onspecific public health interventions isalready available in the form of Public Health at a Glance Fact Sheets(World Bank 2001a). The toolkit will promote best practices byincluding guidelines, tools, lessonslearned, terms of reference,pointers to resource institutions and useful references.
What then is public health? What areits scope and boundaries? Why isinvestment in public health importantto the Bank and what is its institu-tional comparative advantage? Whatpublic health actions are needed toachieve the Millenium DevelopmentGoals? In the twenty-first century,what public health interventions cancontribute to improving the health ofpoor people? What aspects of publichealth are important to the Bank’spolicy dialogue, knowledge manage-ment and lending? How can the Bankuse the tools of public health to
2

improve the content and quality of itsportfolio in health and other sectors?
This note explores some of thesequestions, to promote a commonunderstanding of public health with-
in the Bank that is relevant to itsoperational context and to identifypublic health approaches to help theBank meet its corporate goals andobjectives.
3

Concepts of public health have existedfor millennia. Hippocrates’ book Airs,Waters, and Places, written around 400BC, represented the first systematiceffort to present a causal relationshipbetween environmental factors and dis-ease and to offer a theoretical basis forunderstanding endemic and epidemicdiseases. Early in the twentieth century,C.E.A. Winslow proposed this defini-tion: “Public health is the science andthe art of preventing disease, prolong-ing life and promoting physical healthand efficiency through organized com-munity efforts for the sanitation of theenvironment, the control of communityinfections, the education of the individ-ual in principles of personal hygiene,the organization of medical and nurs-ing service for the early diagnosis andpreventive treatment of disease and thedevelopment of the social machinerywhich will ensure to every individual inthe community a standard of livingadequate for the maintenance ofhealth” (Winslow 1920).
Public health attributes responsibili-ties at both the individual and thecollective level. Social action in healthhas underpinned the evolution ofpublic health over the centuries andtoday social justice is a major pillar ofpublic health. Its basic tenet is thatacquired knowledge about how toensure a healthy population mustextend equally to all groups in anysociety. Public health professionalswork to overcome the barriers causedby differences in gender, social class,ethnicity and race that prevent avail-able tools and interventions frombeing applied equally (Merson et al.2001). Public health is also notablefor embracing clinical care and foremphasizing the link between povertyand ill health and the importance ofequity in material well-being.
Note that despite the emphasis onsocial actions, public health is not theequivalent of publicly provided orfinanced health care. So the public
health budget—to the extent that acountry may have one—is not thesame as the publicly financed budgetfor health services but is usually asubset of it.
A Working Definition:Public Health Categoriesand Functions
The American Public HealthAssociation has synthesized the manydefinitions and perspectives on publichealth and identified six basic princi-ples of contemporary public healththeory and practice (APHA): a) em-phasis on collective responsibility forhealth and the prime role of the statein protecting and promoting the pub-lic’s health; b) focus on whole popula-tions; c) emphasis on prevention, espe-cially the population strategy for pri-mary prevention; d) concern for theunderlying socioeconomic determi-nants of health and disease, as well asthe more proximal risk factors;
4
1. What Is Public Health?
e) multi-disciplinary basis which incor-porates quantitative and qualitativemethods as appropriate; and f ) part-nership with the populations served.
The Pan American Health Organiza-tion (PAHO), in collaboration with theU.S. Centers for Disease Control andPrevention (CDC) and the LatinAmerican Center for Health Research(CLAISS), has built upon the APHA’swork and that of WHO (Bettcher etal., 1998). Through rigorous field test-ing in several countries in LatinAmerica and the Caribbean and a con-sensus building process with ministriesof health, academicians and interna-tional organizations, they have pro-posed eleven “essential” public healthfunctions (see Annex 2). PAHO/CDC/WHO are now field testingways to measure how well health caresystems perform the various publichealth functions (PAHO May 2000).
For the World Bank’s operationalpurposes, the major public healthfunctions can be grouped into fivecategories:
• policy development;
• collecting and disseminating evi-dence for health policies, strate-gies and actions;
• prevention and control of disease;
• inter-sectoral action for betterhealth; and
• human resource development andcapacity building.
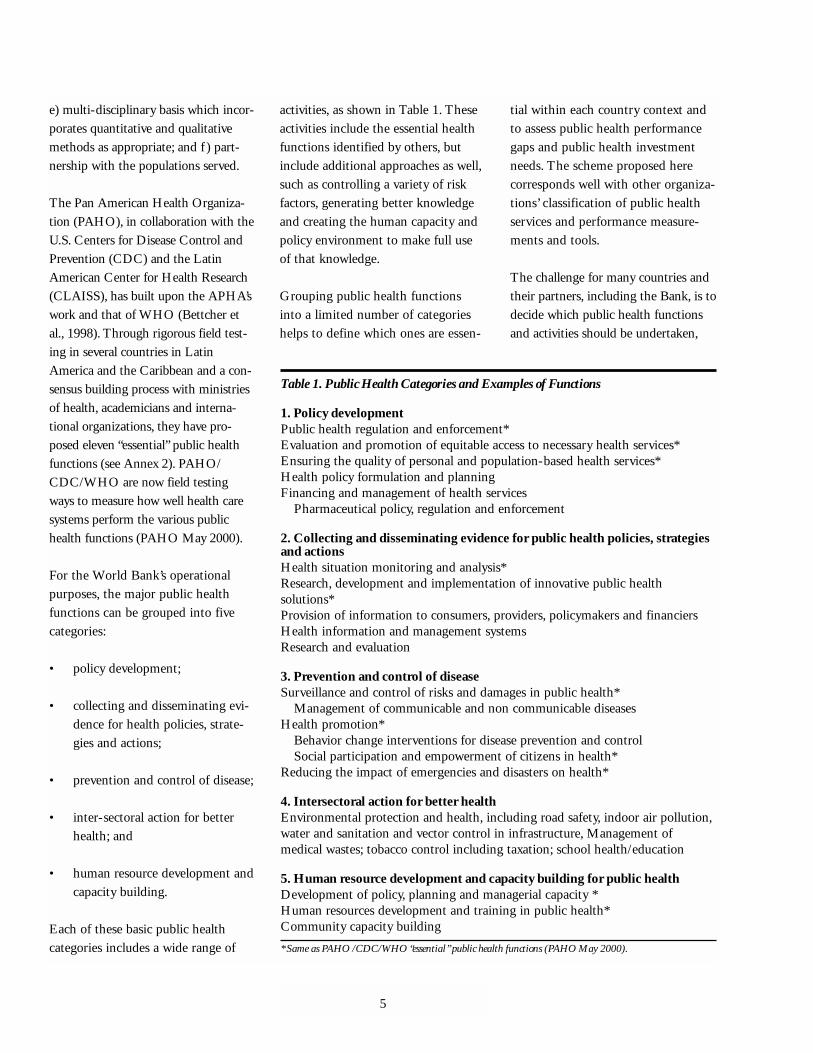
Each of these basic public healthcategories includes a wide range of
activities, as shown in Table 1. Theseactivities include the essential healthfunctions identified by others, butinclude additional approaches as well,such as controlling a variety of riskfactors, generating better knowledgeand creating the human capacity andpolicy environment to make full useof that knowledge.
Grouping public health functionsinto a limited number of categorieshelps to define which ones are essen-
tial within each country context andto assess public health performancegaps and public health investmentneeds. The scheme proposed herecorresponds well with other organiza-tions’ classification of public healthservices and performance measure-ments and tools.
The challenge for many countries andtheir partners, including the Bank, is todecide which public health functionsand activities should be undertaken,
5
Table 1. Public Health Categories and Examples of Functions
1. Policy developmentPublic health regulation and enforcement*Evaluation and promotion of equitable access to necessary health services*Ensuring the quality of personal and population-based health services*Health policy formulation and planningFinancing and management of health services
Pharmaceutical policy, regulation and enforcement
2. Collecting and disseminating evidence for public health policies, strategiesand actionsHealth situation monitoring and analysis*Research, development and implementation of innovative public healthsolutions*Provision of information to consumers, providers, policymakers and financiersHealth information and management systemsResearch and evaluation
3. Prevention and control of diseaseSurveillance and control of risks and damages in public health*
Management of communicable and non communicable diseasesHealth promotion*
Behavior change interventions for disease prevention and controlSocial participation and empowerment of citizens in health*
Reducing the impact of emergencies and disasters on health*
4. Intersectoral action for better healthEnvironmental protection and health, including road safety, indoor air pollution,water and sanitation and vector control in infrastructure, Management ofmedical wastes; tobacco control including taxation; school health/education
5. Human resource development and capacity building for public healthDevelopment of policy, planning and managerial capacity *Human resources development and training in public health*Community capacity building
* Same as PAHO /CDC/WHO “essential” public health functions (PAHO May 2000).

when and by whom. Middle- and low-income countries differ widely in thestatus of health infrastructure, in theircapacity to respond to health needs ofthe population, and in the stage ofdevelopment of the health care system.Depending on country-specific cir-cumstances and resources, some of thepublic health functions considered“essential” may not be relevant orachievable in the short or even medi-um term. International discussions areunderway to prioritize the “essential”
public health functions and to assistcountries to select those functions mostrelevant for local circumstances andresources. This is expected to be moresensible and valuable than trying toestablish priorities among different dis-eases or problems.
Boxes 1 through 4 provide examplesof best practices in Bank operations inseveral public health functions: sur-veillance, road safety, indoor air pollu-tion and school health.
Why Think in Terms ofFunctions?
Analyzing public health in terms offunctions in addition to specific activ-ities or final objectives is consistentwith the World Health Organization’sview that the role of health systems isto carry out a few crucial, generalfunctions. These are: the provision ofservices that promote health; invest-ment in the corresponding physicaland human capacity; financing bothprovision and investment; and exercis-ing “stewardship” over the whole,including informational, evaluativeand regulatory duties (WHO 2000).Some public health activities areinvestment (e.g., training), some areservice delivery (disease management)and several correspond to stewardship(regulation, quality assurance, infor-mation). The boundaries and scope ofpublic health are discussed more fullybelow, but some general statementscan be made about the role of publichealth functions in the context ofhealth systems.
Public health functions describe a spectrumof competencies for health systems that arefundamental to the principles of steward-ship, the one role of the state that can-not be left to the market. Public healthfunctions are required to fulfill respon-sibilities in promoting and assuringaccess, quality, accountability andempowerment of citizenry in healththrough health monitoring, surveil-lance, regulation, evaluation, socialmobilization, disease prevention andcontrol, and workforce development.While the World Development Report1997 (World Bank 1997b) underscoresthe limits of state capability and pro-poses ways of augmenting it, the World
6
Box 1. Brazil Disease Surveillance and Control Project (VIGISUS)
The Brazil Disease Surveillance and Control Project is implemented by theMinistry of Health in collaboration with the U.S. Centers for Disease Controland Prevention, the CDC Foundation, UNDP, PAHO, and the Bank. The aimis to strengthen the National Surveillance System, with particular emphasis onthe health of indigenous populations. The project provides decentralized trainingfor staff (municipal, state, and federal) in epidemiology, disease prevention andcontrol, environmental surveillance, laboratory reporting, and management.International technical assistance focuses on support for studies and research inepidemiological and environmental surveillance as well as on use of surveillancedata for decision making. A public health laboratory network is being rehabili-tated, expanded, and equipped while the telecommunications system is upgradedfor data management.
This project has been key in supporting the decentralization process of thehealth sector and in strengthening the institutional capacity. The innovative fieldepidemiology training has provided opportunities for local surveillance workersto with managers and decision makers in problem solving. Each state has con-ducted its own diagnostics of the surveillance system and designed an investmentplan to address the unfinished agenda. Environmental surveillance has legal sup-port, comprising intersectoral collaboration.
The indigenous population lives in 24 out of 27 states, but mostly in theAmazon Basin. One of the biggest challenges in the project is to tailor healthservices to reach effectively this segment of the population. Seven-percent of theinvestment, about US$13 million, is being applied to programs to benefit indige-nous people. Activities include strengthening of the participation of indigenouspeople in planning and policy decisions through district health councils, assuringthat all indigenous villages have health posts, special programs aimed at indige-nous health issues (for example, alcohol abuse, tuberculosis and nutrition), sup-port for indigenous women’s organizations, and training of both regular andindigenous health workers to improve cultural aspects of service delivery, and tobuild an indigenous health and demographic data base.
Source: Anabela Abreu, LCSHH, focal person for surveillance in the HNP Network, World Bank.

Health Report 2000 (WHO 2000)emphasizes the state’s responsibility toserve as steward for the global societalinterest in improving health outcomes.Putting together the messages of WDR1997 and WHR 2000 implies the needto use limited public capacity where itis most crucial, to “row less and steermore.” However, because so many pub-lic health activities are at least partlypublic goods—and because improve-ments in public health will particularlybenefit the poor—the state role in in-vestment and provision may need to belarger in public health than in clinicalcare. The stewardship function impliesa long-term view of public action andpublic health, and a sense of respon-sibility not only for collective healthoutcomes in the present generation butalso for those in future generations.
No particular organizational structure isinherent in public health functions.Public health functions are comple-mentary to more traditional verticalprograms and offer a framework inwhich to conduct them. “Definingand measuring the essential publichealth functions should contribute tothe institutional development of pub-lic health and to a better dialoguebetween public health and other disci-plines working in public health.Moreover, better definition of what isessential should help to develop moreprecise definitions of institutionalresponsibilities in the delivery of pub-lic health interventions. Of particularinterest is the delineation of responsi-bility between the public and privatesectors” (PAHO October 2000). Rolesand responsibilities can be identifiedand assigned to a variety of partnersworking cooperatively, includinggovernment, the private sector, non-
governmental organizations and civilsociety, based on factors such asexperience, skills, capacity and accessto populations.
Mechanisms for monitoring and evalua-tion are inherent in several public healthfunctions (health situation monitoringand analysis, surveillance, diseaseprevention and control, humanresources development in publichealth). These functions are requiredto select and track key intermediateand outcome indicators to showwhether progress is being made inachieving the Millenium DevelopmentGoals and improving the health ofpoor people, to test the effect of poli-cies and programs, and to adjust poli-cies and programs as needed. They aretherefore essential to formulating andevaluating poverty reduction strategiesand Bank investment projects.
Public health functions emphasize insti-tution and capacity building for sustain-ability. Public health functions pro-
vide a framework for developing theappropriate machinery for policymaking and decision making, and forplanning and evaluation in the healthcare system. “In many ministries ofhealth, this apparatus remains rudi-mentary: the budgeting is separatefrom the planning, which is separatefrom the epidemiology, which is sepa-rate from the demography and vitalstatistics divisions” (Morrow 1997).Correcting this situation means devel-oping capacity for monitoring, inves-tigation, educating, community mobi-lization, legislation, regulation andworkforce development. With thesecapacities, a country can readily adaptto changes in its health profile anddeal with new challenges as they arise.Table 2 provides examples of howpublic health functions can be appliedin different health areas (adaptedfrom PAHO October 2000).Regulating taxes on tobacco is anexample of a regulatory activity topromote health behaviors that preventmajor damage to health.
7
Table 2. Selected Public Health Functions (PHF) Applied to Various Health Concerns
Applied to:
Maternal andEnvironmental Occupational Child Health Chronic Communicable
PHF Health Health (MCH) Diseases Diseases, Etc.
Health Monitoring of Monitoring Monitoring Monitoring MonitoringSituation environmental of risks in the of the risks of the risks of risks andMonitoring risks workplace in MCH of chronic incidence ofand Analysis problems diseases communicable
diseases
Public Health Monitoring of Monitoring Monitoring of Monitoring Monitoring and Regulation and compliance with of the laws compliance and regulation to Enforcement environmental to protect with the laws regulation to prevent and
regulations workers protecting promote control mothers and healthy communicable children behaviors diseases
that prevent major damageto health.
Etc.
Defining health objectives and identi-fying the functions needed to achievethose objectives do not fully clarifyjust how far the sphere of publichealth extends. Two important issuesin particular are often misunder-stood—the relationship between pub-lic health and clinical care, and theplace of public health in overall healthsystem functioning and development.
The Scope of Public Health
The determinants of health are notlimited to the health sector. Sanitationand access to water influence diseaseincidence and mortality, particularlyin young children. Agricultural poli-cies and practices can dramaticallyaffect food prices and household foodsecurity, resulting in acute or chronicmalnutrition, especially among poorpeople. Different forms of indoor andoutdoor air pollution with their con-comitant health effects (acute respira-
tory infections, asthma) result fromuse of biomass and fossil fuels. Publichealth relies heavily on education toimprove the knowledge of healthworkers, educators, schoolchildrenand the general public about hygieneand healthy behaviors (e.g., breast-feeding, proper nutrition, immuniza-tions, family planning and HIV/AIDS prevention). The design andmaintenance of road infrastructureaffect the incidence and severity ofinjuries to vehicle drivers, passengersand pedestrians. Public health alsodepends on other sectors than healthin addressing equity issues that influ-ence health status. Examples of thisare gender-based discrimination, thepolitical situation of certain ethnic orminority groups, or the protectionafforded to refugees.
Sometimes several of these associa-tions are relevant at once. For exam-ple, the full cost of reaching remotepopulations for improved health may
include investment in health andnutrition, roads, electricity and educa-tion. The responsibility for develop-ment and maintenance of this infra-structure rests with other sectors:what matters for public health is tohave a role in the decisions of othersectors when those affect health.
Examples of the Bank’s work acrosssectors on road safety, indoor air pol-lution and school health are given inBoxes 2 through 4.
Public Health andClinical Care
Public health and clinical services(personal health care of individuals)are sometimes presented as mutuallyexclusive entities. However, differen-tial roles may be more a result ofhow public health organizations areused in a health system than ofintrinsic differences. For example, insome countries, immunization services
8
2. What Are the Scope andBoundaries of Public Health?

for children are provided entirely bypublic health organizations with littleor no role played by health care serv-ice providers or the private sector. Inother countries, preventive and cura-
tive health services are provided bypublic health organizations to thepoorest segment of society in a two-tiered system because these popula-tions either do not have access to or
cannot afford services by the “main-stream” health care system. Publichealth and clinical care are betterunderstood as parts of the wholehealth care system that form
9
Box 2. Road Safety: Working Across Sectors with Governments, Civil Society and the Private Sector
The Bank is placing increased emphasis on road safety. At present, about two thirds of transport projects have a road-safetycomponent. The effectiveness of road-safety programs is dependent on partnership between the government, the civil socie-ty and the private sector. Thus, along with other donors, the Bank has promoted the Global Road Safety Partnership(GRSP). This tri-sector collaboration aims to find more effective ways to deal with road safety in low- and middle-incomecountries. It operates in countries where road safety has been identified as a problem, where local authorities have expresseda desire to tackle the issue, and where an agreed framework—such as a national road-safety action program—exists. Thefocus countries are Poland, Romania, Hungary, India/Bangalore, Malaysia, Thailand, Vietnam, Costa Rica, Brazil, Ghanaand South Africa.
The reason for focusing on the issue of road safety is its impact on health and the economy. In 1998, more than one millionpersons died from road traffic injuries (RTIs) worldwide and many more were injured. The situation is particularly criticalin low- and middle-income countries, where 88 percent the world’s deaths from RTIs have occurred even though thesecountries possess fewer motor vehicles than developed countries. Moreover, RTIs are expected to rise in low-and middle-income countries, in contrast to the steady decline in RTIs occurring in recent years in developed nations.
By 2020, road accidents are expected to rise from ninth to third place as the leading contributor to disability-adjusted lifeyears (DALYs) lost in the world. We know now that RTIs can be prevented and that the ensuing burden can be reduced bymore and better targeted investment.
Source: Eva Jarawan, MNSHD, focal person for road safety in the HNP Network, World Bank.
Box 3. A Multi-Sectoral Approach to Reducing Indoor Air Pollution
Indoor Air Pollution is a major health risk factor, accounting for 4 percent of the global burden of disease, on a par withtobacco. It is caused by the use of low-cost and widely available energy sources such as coal and biomass (wood, dung, cropresidues) for cooking and home heating. Biomass is still the main source of energy for 60 to 90 percent of the population indeveloping countries, or for 3.5 billion people. The burden is greater in high-altitude rural areas and among the poor, whoare more likely to rely on biomass and low quality coal fuels, and especially women and children, who are more likely to beexposed because of their household responsibilities indoors.Biomass and coal, while cheap and readily available, are extremely polluting and pose serious health hazards due primarily tochronic exposure to particulates, sulfure and nitrous oxides (SO2, NOX), carbon monoxide (CO), fluoride (coal), aldehydesand para amino hydrocarbons (PAH). These are well-known risk factors for acute respiratory infection, chronic obstructivelung disease (COLD) and cancer. Chronic exposure to indoor air pollution may also result in low birth weight andincreased susceptibility to asthma, tuberculosis and cataract.Ultimately, most developing countries will move up the energy ladder to petroleum or natural gas, or electricity. However,such a move, while ideal, is neither optimal nor feasible in the short run because the poor have no (or only limited) access to,nor can they afford, high-quality fuel such as LPG, natural gas, or electricity. The World Bank is well positioned for advoca-cy, inter-sectoral research and interventions to alleviate indoor air pollution in poor rural settings. Multi-sectoral interventiontrial initiatives and advocacy efforts are underway in China, India and other high-burden countries to improve access to effi-cient and affordable energy through local design and manufacturing of low-cost stoves and renewable energy solutions whiletaking into consideration the adoption of environmentally and socially sound and sustainable energy practices.
Source: Enis Baris, EASHD, focal person for indoor air pollution in the HNP Network, World Bank.
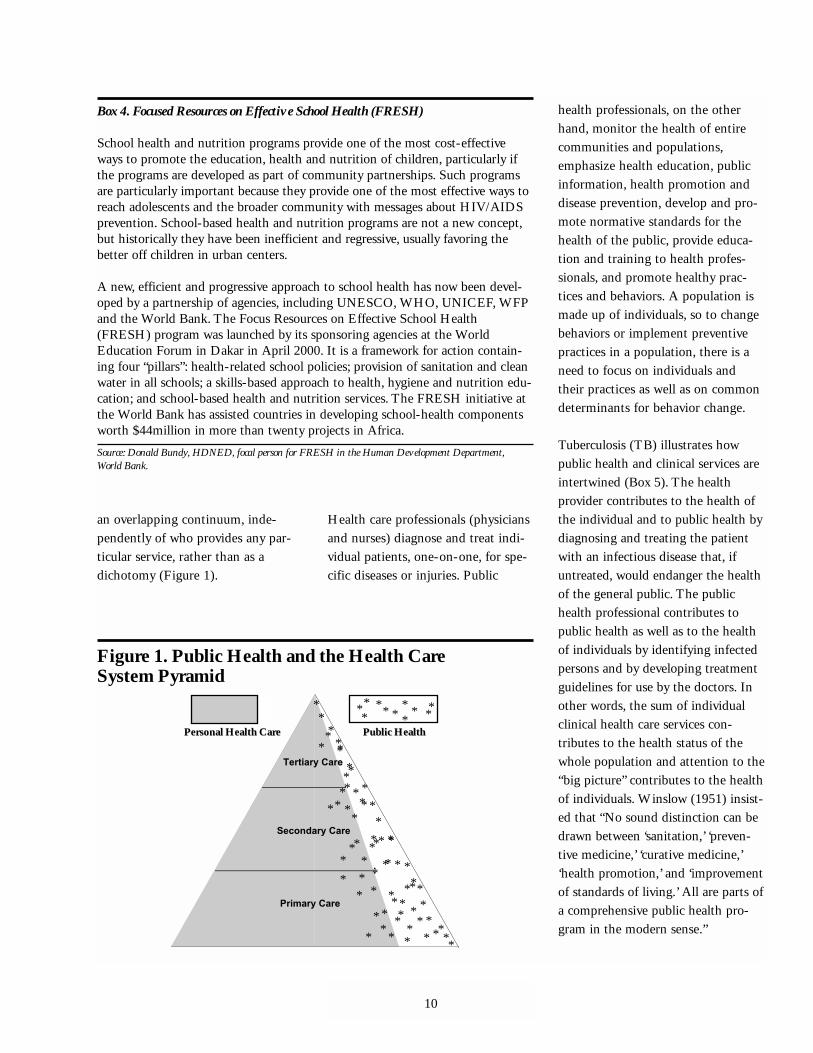
an overlapping continuum, inde-pendently of who provides any par-ticular service, rather than as adichotomy (Figure 1).
Health care professionals (physiciansand nurses) diagnose and treat indi-vidual patients, one-on-one, for spe-cific diseases or injuries. Public
health professionals, on the otherhand, monitor the health of entirecommunities and populations,emphasize health education, publicinformation, health promotion anddisease prevention, develop and pro-mote normative standards for thehealth of the public, provide educa-tion and training to health profes-sionals, and promote healthy prac-tices and behaviors. A population ismade up of individuals, so to changebehaviors or implement preventivepractices in a population, there is aneed to focus on individuals andtheir practices as well as on commondeterminants for behavior change.
Tuberculosis (TB) illustrates howpublic health and clinical services areintertwined (Box 5). The healthprovider contributes to the health ofthe individual and to public health bydiagnosing and treating the patientwith an infectious disease that, ifuntreated, would endanger the healthof the general public. The publichealth professional contributes topublic health as well as to the healthof individuals by identifying infectedpersons and by developing treatmentguidelines for use by the doctors. Inother words, the sum of individualclinical health care services con-tributes to the health status of thewhole population and attention to the“big picture” contributes to the healthof individuals. Winslow (1951) insist-ed that “No sound distinction can bedrawn between ‘sanitation,’ ‘preven-tive medicine,’ ‘curative medicine,’‘health promotion,’ and ‘improvementof standards of living.’ All are parts ofa comprehensive public health pro-gram in the modern sense.”
10
Box 4. Focused Resources on Effective School Health (FRESH)
School health and nutrition programs provide one of the most cost-effectiveways to promote the education, health and nutrition of children, particularly ifthe programs are developed as part of community partnerships. Such programsare particularly important because they provide one of the most effective ways toreach adolescents and the broader community with messages about HIV/AIDSprevention. School-based health and nutrition programs are not a new concept,but historically they have been inefficient and regressive, usually favoring thebetter off children in urban centers.
A new, efficient and progressive approach to school health has now been devel-oped by a partnership of agencies, including UNESCO, WHO, UNICEF, WFPand the World Bank. The Focus Resources on Effective School Health(FRESH) program was launched by its sponsoring agencies at the WorldEducation Forum in Dakar in April 2000. It is a framework for action contain-ing four “pillars”: health-related school policies; provision of sanitation and cleanwater in all schools; a skills-based approach to health, hygiene and nutrition edu-cation; and school-based health and nutrition services. The FRESH initiative atthe World Bank has assisted countries in developing school-health componentsworth $44million in more than twenty projects in Africa.
Source: Donald Bundy, HDNED, focal person for FRESH in the Human Development Department,World Bank.
*
Primary CarePrimary Care
Secondary CareSecondary Care
Tertiary CareTertiary Care
..
*
*
*
* *
*
*
*
*
*
*
*
*
*
***
*
*
**
* ***
*
*
*
*
*
*
*
*
*
*
*
*
*
Personal Health CarePersonal Health Care Public HealthPublic Health
*** * *** *
*
*
*
*
*
*
*
*
*
**
**
*
**
*
*
*
*
*
*
*
*
*
*
*
**
*
*
*
Figure 1. Public Health and the Health Care System Pyramid

The Interface of PublicHealth and HealthSystems Development
Public health is a key part of everyhealth care system. Public health func-tions cannot be adequately carried outunless the health system performs itscrucial functions of providing services;investing in human and physical inputs;financing; and stewardship; and thehealth system cannot work without theproper conduct of public health func-tions. Whether or not it is always rec-ognized, public health permeates the
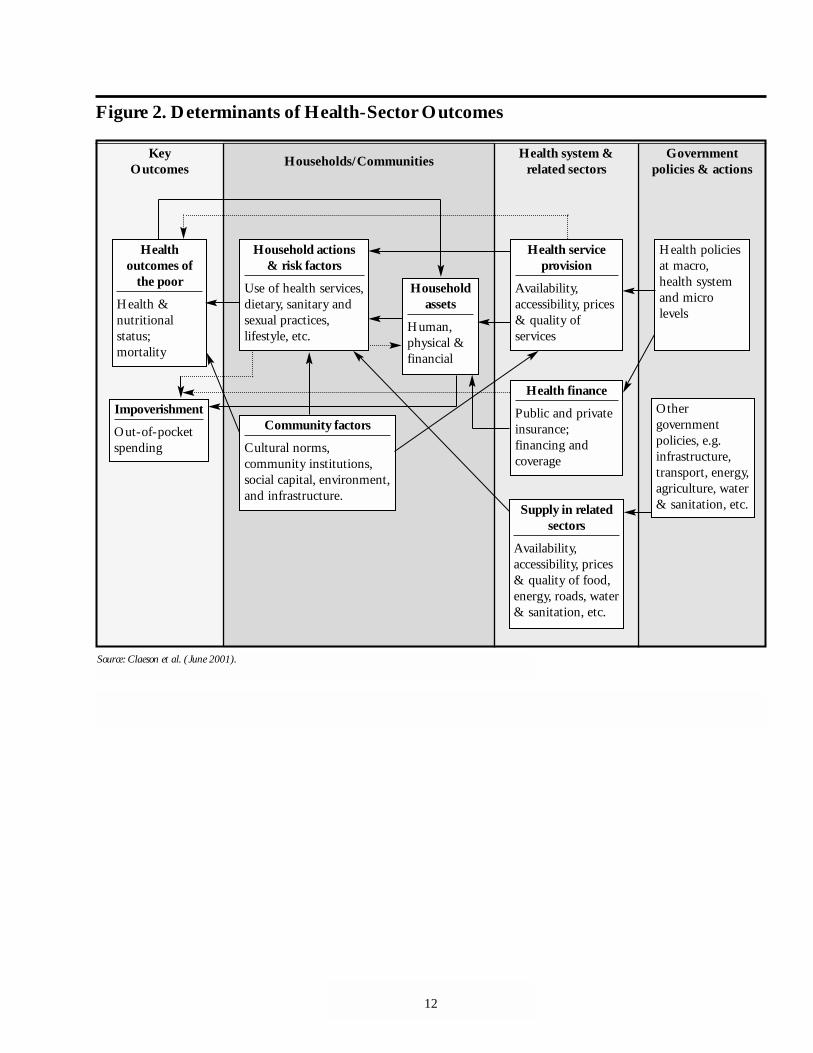
health system at every stage, from poli-cy to outcomes, as shown in Figure 2.
Beyond the required physical inputs, themotivation of the staff and managementof the organizations and institutions thatcomprise health systems have a pro-found influence on how well the publichealth system operates. The world’s poorare often excluded from the benefits ofpublic health interventions because thelarger health system is dysfunctional.
The interface of public health andhealth systems development is also
reflected in the priority themes thatthe Health, Nutrition and Populationthematic groups are working on:achieving progress towards theMDGs, improving developmenteffectiveness and basic services forthe poor. The HNP thematic groups(Public Health, Health SystemsDevelopment, Poverty, Nutrition, andPopulation and Reproductive Health)are all contributing to the commongoal of improving health outcomes ofthe poor through knowledge manage-ment, training, improving quality andworking with partners.
11
Box 5. Clinical Care and Public Health: The TB Scenario
A woman falls ill with chronic cough, fever and weight loss in a rural village or urban shantytown. Others around her mayhave previously been ill with similar symptoms. She may delay seeking care due to other duties or lack of funds to pay fortravel or consults. She may purchase medicines from a drug seller, visit a traditional healer or private physician; she may takedrugs sporadically until her money runs out; symptoms remain and she becomes further incapacitated. Her family or neigh-bors may then bring her to a health center or hospital, where she sees a nurse auxiliary who may or may not refer her to aphysician. The physician may charge her for an X-ray or treat her with general antibiotics and send her home or, alterna-tively, refer her for a free sputum smear examination if available.
She is found to have active infectious tuberculosis. The physician or nurse may tell her about TB, or due to stigma or lack ofinterest or time, they may only tell her that she needs to take more medicines. They may give her a month’s worth to takehome, or tell her to attend the health clinic every day even though it is two hours from her home, or worse yet tell her tobuy the medicines elsewhere, if no drugs are in stock. She might get only two of the four medicines she needs. Familymembers who may also have become infected or ill might not be seen by the health provider. The health provider might notbe able to follow-up to assess whether she tolerated the medicines, took them regularly, was cured, remained ill, or died. Nofunctioning information system may be in place to register that a case was detected and treated. No supervisors may visit toprovide training or feedback on performance.
The delays in seeking care, insufficiently skilled or salaried staff, lack of patient and community health education, poor sup-ply chains, failure to report the TB case, lack of follow-up with the patient or her close contacts, and poor supervision in theuse of the medicines all can increase the risk of failed treatment, chronic disease or death for the patient. This situation alsocontributes to the spread of infection in the community and to the potential emergence of drug-resistant organisms thatpass from community to community and across borders.
To avoid this unfortunate scenario, public health practices can establish the norms and strategies for good disease preven-tion, treatment and control. They can enable health providers and community workers to apply these norms, access neededsupplies, and educate patients and the public. Public health best practices enable the patient to seek care earlier or engageothers to help her seek care. They improve access to appropriate low-cost diagnosis, treatment and referral if necessary. Theycreate community-based or service-based directly observed treatment that meets the patient’s needs, increases probability ofcure and helps prevent transmission. Such an approach increases the credibility of providers, the satisfaction of patients, andthe utilization of health services, and reduces the costs to society of illness.
Source: Diana Weil, HDNHE, focal person for TB in the HNP Network, World Bank.
12
Figure 2. Determinants of Health-Sector Outcomes
KeyOutcomes Households/Communities Health system &
related sectorsGovernment
policies & actions
Healthoutcomes of
the poor
Health &nutritionalstatus;mortality
Impoverishment
Out-of-pocketspending
Household actions & risk factors
Use of health services,dietary, sanitary andsexual practices,lifestyle, etc.
Community factors
Cultural norms,community institutions,social capital, environment,and infrastructure.
Householdassets
Human,physical &financial
Health serviceprovision
Availability,accessibility, prices& quality ofservices
Health finance
Public and privateinsurance;financing andcoverage
Supply in relatedsectors
Availability,accessibility, prices& quality of food,energy, roads, water& sanitation, etc.
Health policiesat macro,health systemand microlevels
Othergovernmentpolicies, e.g.infrastructure,transport, energy,agriculture, water& sanitation, etc.
Source: Claeson et al. (June 2001).

One answer is that the Bank is formallycommitted to achieving health, nutritionand population outcomes that requirepublic health interventions. Some ofthese outcomes are included amongthe Millennium Development Goalsto which the Bank has subscribed(Annex 1). These goals can only beachieved through interventions toreduce maternal and child mortality;improve reproductive health; andachieve the targets for HIV/AIDS,malaria, TB and other communicablediseases, as well as interventions tomake significant progress towardsattainment of water and sanitation andnutritional goals (World Bank 2001c).Box 6 shows what is needed to achievethe child mortality reduction goal towhich the Bank is committed.Intervention-specific tools and moni-toring and evaluation indicators forother public health problems (includ-ing noncommunicable diseases charac-teristic of the epidemiological transi-tion) are included in Public Health at a
Glance (World Bank 2001a) and in thehealth chapter of the Poverty ReductionStrategy Sourcebook (Claeson et al.2001). Additional public health instru-ments and tools will be included inthe Public Health Resource toolkit.These commitments and the tools tocarry them out are consistent with theBank Group’s Strategic Framework(World Bank, 2001b).
A second answer comes from the eco-nomics of public health. Some of thefunctions described above, especiallythose of stewardship, cannot be leftto the market but are inalienableresponsibilities of the state. Thatmakes them natural places for theBank to invest, especially when insti-tutions and capacities need to bebuilt up. Other functions and partic-ular activities within them are purelyor partly public goods, with substan-tial externalities (including activitiesto control negative externalities, aswith pollution or road safety). On
balance, there is at least as much jus-tification for the Bank to invest inpublic health functions as there is forit to invest in clinical care activities,in which the Bank already is involvedin numerous projects. Finally, theprincipal beneficiaries of greater pub-lic health progress will be poor peo-ple, especially in poor countries.Even when the required activities arelargely private goods, public financ-ing is essential if they are to reachthe poor—or else public action isneeded to add knowledge and changeattitudes so that private markets canoperate at prices the poor can afford.Insecticide-treated bednets to reducemalaria transmission are a primeexample; condoms for protectionfrom HIV/AIDS are another.
Clearly, the Bank does not have suffi-cient technical capacity in many pub-lic health areas and depends on theskills and knowledge of partner agen-cies, including those in client coun-
13
3. Why Should the Bank InvestMore in Public Health?

tries. Nonetheless, the Bank has a com-parative advantage in public health thatderives from its client focus, country-specific knowledge, comprehensiveperspective, potential to integrateacross sectors, long-term commit-ment, convening powers and ability towork with the public and private sec-tors. The diversity of functions inpublic health is matched by the vari-ety of instruments at the Bank’s dis-posal, including not only conventionalinvestment projects but also countryassistance strategies (CASs), compre-hensive development frameworks(CDFs) and poverty reduction strate-gy papers (PRSPs).
The Bank is increasingly engaged inmultiple areas related to publichealth—the development of bestpractices in surveillance, immuniza-tion and other services; the design andcosting of basic benefit packages;health promotion and lifestylechanges, pharmaceutical policy; tobac-co taxation and alcoholic beveragepolicies; and investments throughoutthe lifecycle. With this range ofengagements with clients and publicand private partners, the Bank cancredibly play an important catalyticand leveraging role—and increasinglyhelp address the often neglected andcritical public health functions.
This is not simply a question of addi-tional funds to improve health, but ofsustainable financing, and a unifyingapproach to disease control throughhealth systems development and com-munity-driven actions, providing athree tiered approach—macro policy,health systems development and tar-geted interventions. Sector-wideapproaches provide a framework for aunifying approach to disease control,but the challenges are many, as evi-dent in the Roll Back Malaria move-ment (Box 7).
14
Box 6. Achieving Child Health and Nutrition Outcomes
Child mortality reduction is one of the Millennium Development Goals. Malnutrition reduction is a poverty target and isessential to achieving the child mortality reduction goal. Bank staff and partners have reviewed the key determinants andthe main interventions.
The Poverty Reduction Strategy Framework. Achieving child health and nutrition outcomes requires a common frame-work for implementing targeted interventions, to reach the poor through health systems and community action and financ-ing, with an emphasis on equitable distribution and an enabling policy environment.
Key Determinants. Key intermediate determinants are: use of health and nutrition services; water and sanitation practices;home care including infant feeding; the household environment; and maternal education, health and nutritional status.Household behaviors and risk factors are influenced by the quality and availability of services, community factors, householdassets, health systems capacity, financing, and by the supply of services in related sectors. See Figure 2.
Evidence-Based Interventions. The main interventions are Integrated Management of Childhood Illness (which includesprevention and treatment of acute respiratory illness, malaria, diarrhea, malnutrition, measles and HIV/AIDS) and routineimmunization. Other interventions at different stages of the lifecycle that contribute to child mortality reduction are nutri-tion-specific interventions, environmental health, injury prevention, reproductive health including family planning and safedeliveries, and maternal education.
Monitoring and Evaluation. Monitoring and evaluating health, nutrition and population outcomes requires investment inhealth situation monitoring and analysis, surveillance, disease prevention and control, and human resource development inpublic health.
Monitoring Indicators. Core indicators for child mortality reduction are coverage of measles immunization, ARI treat-ment, use of oral rehydration therapy and proportion of infants exclusively breastfed. In malarious areas, monitoring indica-tors should also include the proportion of children sleeping under insecticide-treated nets; and in HIV high-prevalenceareas, they should include the coverage of low-cost antiretroviral treatment of HIV-infected pregnant women.
Sources: World Bank, 2001c.

15
Box 7. Roll Back Malaria: Aiming at Sustainable Impact through Sector-Wide Approaches
Sector-wide approaches endeavor to respond to many different concerns that have arisen in the context of developmentassistance for health. One of these concerns is the failure of “vertical” programs to have a sustainable impact upon publichealth outcomes. Several programs have all run into constraints when scaling up successful effort.
Disease-specific programs are constrained from achieving larger public health outcomes not only by limited commitment,improper technical standards, or lack of designated funds. Rather, children are not immunized, malaria cases are not effec-tively treated, TB is not diagnosed and diarrhea still leads to deaths from dehydration because vaccines, drugs, kerosene andoral rehydration salts are not ordered in time; vehicles to deliver drugs or transport staff and patients are not repaired; com-munications equipment required to contact the pharmaceutical stores or supervisor does not function; financing is not effec-tively disbursed; staff are not paid; or the health system is unable to retain staff in remote areas.
The Roll Back Malaria movement acknowledged at the outset the importance of health systems strengthening to achievingthe goal of reduced deaths from malaria. Progress has been made in recognizing IMCI and reproductive health programs asinputs to malaria reduction (Uganda and Malawi), in bringing global attention to taxes on bednets (Senegal and Ghana)and in ensuring that malaria activities are incorporated into sector-wide programs and Poverty Reduction Strategy Papers(Uganda, Cameron and Tanzania). Nevertheless, there is still pressure to provide countries with “RBM” financing andmalaria-specific inputs, and less attention is paid to incorporating malaria within broader health development efforts. Thechallenge faced by Roll Back Malaria in maintaining a health systems orientation suggests how difficult it is to value actionsthat are not disease specific. Yet without attention to broader health systems, little sustainable impact is likely.
Source: Julie McLaughlin, AFTHI, Malaria Core Team in HNP Network, World Bank.

As the Bank undertakes to implementits corporate strategy for the comingthree to five years, now is an ideal timeto develop an overarching strategy inpublic health as well. A public healthstrategy for the Bank based on theBank’s comparative advantages, consis-tent with corporate priorities and devel-oped in conjunction with or as part of anew HNP strategy could be a very use-ful tool for Bank staff. This section sug-gests strategic options—the What ToDo—for enhanced public health effortsat both country and global levels. HowTo Do It is the subject of the PublicHealth Resource toolkit in preparation.
The Role of the Bank at Country Level:Strategic Options
• Prioritize Public Health Action inPolicy Dialogue and LendingPriority in World Bank financing,knowledge management andclient dialogue in health should be
given to achieving the MilleniumDevelopment Goals—improve-ments in maternal and infantmortality, reproductive health,HIV/AIDS, malnutrition, andwater and sanitation, especiallyamong poor populations (see Box6 for an example). The povertyreduction strategy papers showhow to link project inputs withhealth outcomes, including theMillenium Development Goalsand their intermediate determi-nants. In client countries wherethe epidemiological and demo-graphic transition is well under-way, the public health actions toaddress the emerging burden ofnoncommunicable diseases andinjury, and their determinants, alsoneed to be prioritized in policydialogue and lending.
• Assess Performance of PublicHealth FunctionsThe Bank should fully utilize the
opportunities of client dialogueand knowledge management toengage the government andnational health authorities in aself-assessment exercise. Theobject would be to evaluate howwell the public health functionsare being discharged, determinethe capacity and infrastructure ofthe public health system for ful-filling those functions, and iden-tify the strengths and weaknessesof the system.
Assessment of public health func-tions should focus initially onspecific priority diseases and tar-get populations relevant to theMillenium Development Goals.Public health functions arerequired to select and track keyintermediate and outcome indica-tors to demonstrate that progressis being made in achieving theMDGs. The functions are neededto test the effect of policies and
16
4. What Are the Bank’s Strategic Options?

programs, to assist in diagnosinghow and why goals are not beingachieved, and to adjust policiesand programs as needed. Publichealth functions also provideimportant mechanisms for moni-toring and evaluation of povertyreduction strategies. Those func-tions related to evaluating equityof access and ensuring quality ofhealth services are important tobetter understand the needs ofpoor people and the impact onthem of decisions about healthfinancing and structural or func-tional changes in clinical healthcare services.
Assessment of performance inpublic health functions will iden-tify gaps in knowledge, populationcoverage, resources, human capitaland logistic capacity. Self-assess-ment can lead to better definitionof institutional responsibilitiesincluding the roles of municipalauthorities, nongovernmentalorganizations and the private sec-tor. Thinking about functionshelps identify the core competen-cies in public health for regionaland local health authorities, in anenvironment of decentralization.Assessment of the performance ofpublic health functions will alsopermit better quantification of theresources required to ensure anadequate public health systeminfrastructure—information criti-cal to the government, decisionmakers, the Bank, donors andother international agencies.
• Incorporate Public HealthFunctions in PRSPs and CASsSound diagnosis of poverty, iden-
tification of public actions thatwill have maximum impact onpoverty reduction, and monitor-ing and evaluation are at the coreof the poverty reduction strategyprocess. Since morbidity andmortality from common commu-nicable diseases is a major prob-lem among the poor, and accessto health services is inequitablydistributed to the disadvantage ofthe poor, the PRSPs should helpmake public health issues morevisible and increase accountabilityfor governments in their alloca-tion of public expenditures toaddress these issues.
A country assistance strategy setsout the Bank’s overall assistanceprogram in a country and there-fore has enormous potential toinfluence public health and pro-vide a lever for introducing apublic health perspective on theBank’s entire program in thecountry. One of the greatestchallenges faced in CAS prepara-tion is choosing priority sectors.The Bank can provide or mobi-lize technical support to coun-tries undertaking the PRSP andCAS processes, assist them inmaking rational and sustainablechoices, and then provide sup-port to selected parts of the gov-ernment program.
• Customize Solutions andInvestmentsField tests of self-assessments inLatin America and the Caribbeanhave shown that there is a widerange of performance amongcountries on the eleven PAHO/CDC/WHO “essential” public
health functions. Middle-incomecountries have more resources,infrastructure and human capitalto devote to public health andtherefore tend to perform betteron some key functions than poorcountries. But no predictions orgeneralizations about the patternsof strengths and weaknesses ofpublic health performance can bebased simply on income. Needsdiffer because each country has aunique combination of history,socio-economic characteristics,population composition, healthproblems, resources, human capi-tal and environmental problemsand characteristics.
The Global Role of the Bank:Strategic Options
• Disseminate Knowledge on Public Health and Public Health FunctionsThe Bank should emphasizeknowledge management and dis-semination to address theMillenium Development Goals.The Public Health at a Glanceseries describes the state of theart in what to do. A lifecycleapproach is recommended for theassessment of risks and forchoosing among interventionsfor poor communities (Simon etal. 2001). The Public HealthResource toolkit will provide asimilar set of knowledge manage-ment products related to how toimplement the best buys in dif-ferent country contexts underBank operational constraints.This means focusing on knowl-edge management and dissemi-
17
nation related to the five cate-gories of public health functions.
• Conduct Research and Analysis Related to Public Health FunctionsMore research and analysis isneeded to determine the bestbuys for Bank investment in pub-lic health functions. To under-stand the direct and indirect rela-tions between the specific func-tions and specific outcomesrequires further analysis of thecausal web linking health out-comes with multiple determi-nants. What is the relativeimportance of non-health deter-minants versus direct healthdeterminants in achieving theMillenium Development Goals?What is the evidence that invest-ing in public health and publichealth functions actuallyimproves outcomes for poor peo-ple? How should one set priori-ties in public health given thedifferent economic, epidemiologi-cal and demographic contexts andtransitions? These are all issuesfor research.
• Selectively Engage in GlobalHealth InitiativesIn 1998, the HNP Sector Boarddecided that collaboration withpartners could be optimized bya focus on a few major HNP
issues with large externalities,through multi-country ini-tiatives, and with clarification of the comparative advantage of the Bank and its partners.The priorities selected werebased on the Bank’s ability tomake a significant difference, the
timing and the expectationsfrom clients and partners at thetime. They were:
■ a global noncommunicabledisease problem (tobacco);
■ emerging and re-emergingcommunicable diseases(malaria, TB and HIV/AIDS); and
■ the unfinished agenda ofmaternal and child healthand nutrition (selectedreproductive health, IMCI,immunization and nutritioninterventions).
Since then, the Bank has increasedits engagement in global initiativesand is exploring with partners in-novative financing mechanismsand lending instruments to achievespecific health outcomes (Box 8).As partners expect increasing sup-port from the Bank for new initia-tives, it is important to revisit thecriteria for selecting priority pro-grams and topics and evaluateprogress in those areas that havereceived priority status globally.Possible new criteria for increasedselectivity in global initiatives are:
■ the relevance of the initiativefor achieving the major
18
Box 8. Partners in Public Health
Public health partnerships and initiatives can contribute to strengthening publichealth functions, e.g., investments in immunization can help build surveillancecapacity, a functioning cold chain and other public health infrastructure.Moreover, an increased emphasis on public health functions will enable countriesto assess, prioritize and take advantage of the opportunities that these initiativesoffer to achieve sustainable improvements in health.
Strong partnerships with client governments, beneficiaries, nongovernmentalorganizations, the private sector, bilateral donors, foundations and other agencieshave become critical to the Bank’s work in public health. The Bank relies on theUnited Nations (including WHO, UNICEF, UNAIDS and UNFPA), otheragencies such as the U.S. Centers for Disease Control and Prevention and non-governmental organizations, in knowledge management, client support on tech-nical issues and working with communities.
The Global Alliance for Vaccines and Immunization (GAVI), Safe InjectionGlobal Network (SIGN), Roll Back Malaria (RBM) and Stop TB are a few ofthe technical partnerships of the last five years. The Bank work with partners onpublic health initiatives and programs ranging from the Safe MotherhoodInitiative, the Global Alliance for Improved Nutrition (GAIN), IntegratedManagement of Childhood Illness (IMCI), to curbing the tobacco epidemic andmental health. Through concerted efforts, such as the Multi-country AIDSProject (MAP) in Africa and the Caribbean, the Bank and partners are scalingup efforts to combat AIDS. Through these partnerships, the Bank supports thedevelopment of new vaccines and immunization programs, the improvement ofmaternal and child health and nutrition, the control of communicable diseasessuch as malaria, tuberculosis and HIV/AIDS and emerging noncommunicablediseases and their risk factors.

HNP goals. Will it help inmaking measurable progresstowards the MilleniumDevelopment Goals in clientcountries?
■ the role of the initiativewithin Poverty ReductionStrategies. Will it help buildcapacity for poverty reduc-tion in client countries?
■ the utilization and enhancedapplication of Bank lendinginstruments. Will it improvethe Bank’s performance?
19

Public health is a complex fieldtouching on deep personal and pro-fessional issues and values. It hasboundaries that do not lend them-selves to clear definition, in economicor health terms. Yet its concern forsocietal improvements in health out-comes is central to the agenda of theBank and to any concern for increas-ing welfare in the developing coun-tries, especially among poor people.
At the beginning of the new millen-nium, public health is a rapidly evolv-ing field. New issues are emerging,such as the health aspects of global-ization, public health in post-conflictsocieties, global public health goodsand new and re-emerging diseases. Inlight of the central character of healthin the agreed international develop-ment goals, a public health perspec-tive needs to infuse the entire work ofthe Bank. The HNP staff must take thelead to facilitate and monitor the appli-cation and strengthening of this perspec-
tive at the country level. In some cases,the Bank may finance specific aspectsof global initiatives in individualdeveloping countries (e.g., AIDS vac-cine trials). However, the work onthese initiatives in individual develop-ing countries must be determined bythe particular country’s needs and notsolely by global actions.
The Bank is already engaged in manydimensions of public health, financiallyand otherwise, within countries. TheBank should now broaden and deepenthat engagement within and across thefive categories of public health func-tions. It should do so in accordancewith its global and HNP missions, itsvalues, its multi-sectoral character andits institutional areas of comparativeadvantage. To be fully effective, Bankengagement in public health at thecountry level requires the following:multiple disciplines and skills workingtogether, especially public health spe-cialists and economists; organizational
commitment, through vice presidentialunits (VPUs), country teams and sec-tor boards; and a work program thatreflects these commitments and thatinvolves a wide range of internal andclient country actors, including min-istries of health, other sectoral depart-ments, ministries of finance and plan-ning, and the civil society.
There is a wealth of tools, expertise andcommitment within the Bank andamong its partners on public healthboth in the HNP sector and in othersectors, on which Bank staff can drawto become more effective in publichealth at the country level. The forth-coming web-based Public HealthResource toolkit will address morespecifically the challenge of cooperationon public health issues and outcomesacross sectors and will provide practical,operationally oriented guidance in theform of ideas, tools and shared experi-ence on key public health functions andservices and their financing.
20
5. Conclusion: Public Healthand the World Bank
21
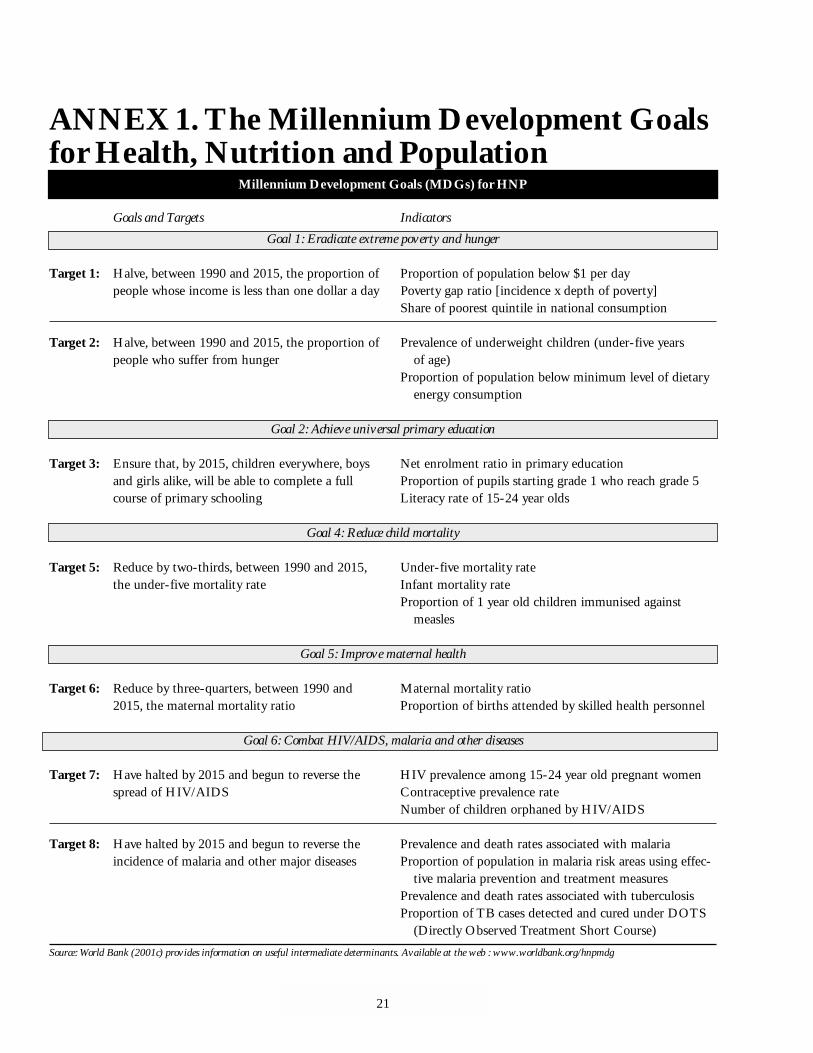
ANNEX 1. The Millennium Development Goalsfor Health, Nutrition and Population
Millennium Development Goals (MDGs) for HNP
Goals and Targets Indicators
Goal 1: Eradicate extreme poverty and hunger
Target 1: Halve, between 1990 and 2015, the proportion of Proportion of population below $1 per daypeople whose income is less than one dollar a day Poverty gap ratio [incidence x depth of poverty]
Share of poorest quintile in national consumption
Target 2: Halve, between 1990 and 2015, the proportion of Prevalence of underweight children (under-five yearspeople who suffer from hunger of age)
Proportion of population below minimum level of dietary energy consumption
Goal 2: Achieve universal primary education
Target 3: Ensure that, by 2015, children everywhere, boys Net enrolment ratio in primary educationand girls alike, will be able to complete a full Proportion of pupils starting grade 1 who reach grade 5course of primary schooling Literacy rate of 15-24 year olds
Goal 4: Reduce child mortality
Target 5: Reduce by two-thirds, between 1990 and 2015, Under-five mortality ratethe under-five mortality rate Infant mortality rate
Proportion of 1 year old children immunised against measles
Goal 5: Improve maternal health
Target 6: Reduce by three-quarters, between 1990 and Maternal mortality ratio2015, the maternal mortality ratio Proportion of births attended by skilled health personnel
Goal 6: Combat HIV/AIDS, malaria and other diseases
Target 7: Have halted by 2015 and begun to reverse the HIV prevalence among 15-24 year old pregnant womenspread of HIV/AIDS Contraceptive prevalence rate
Number of children orphaned by HIV/AIDS
Target 8: Have halted by 2015 and begun to reverse the Prevalence and death rates associated with malariaincidence of malaria and other major diseases Proportion of population in malaria risk areas using effec-
tive malaria prevention and treatment measuresPrevalence and death rates associated with tuberculosisProportion of TB cases detected and cured under DOTS
(Directly Observed Treatment Short Course)
Source: World Bank (2001c) provides information on useful intermediate determinants. Available at the web : www.worldbank.org/hnpmdg
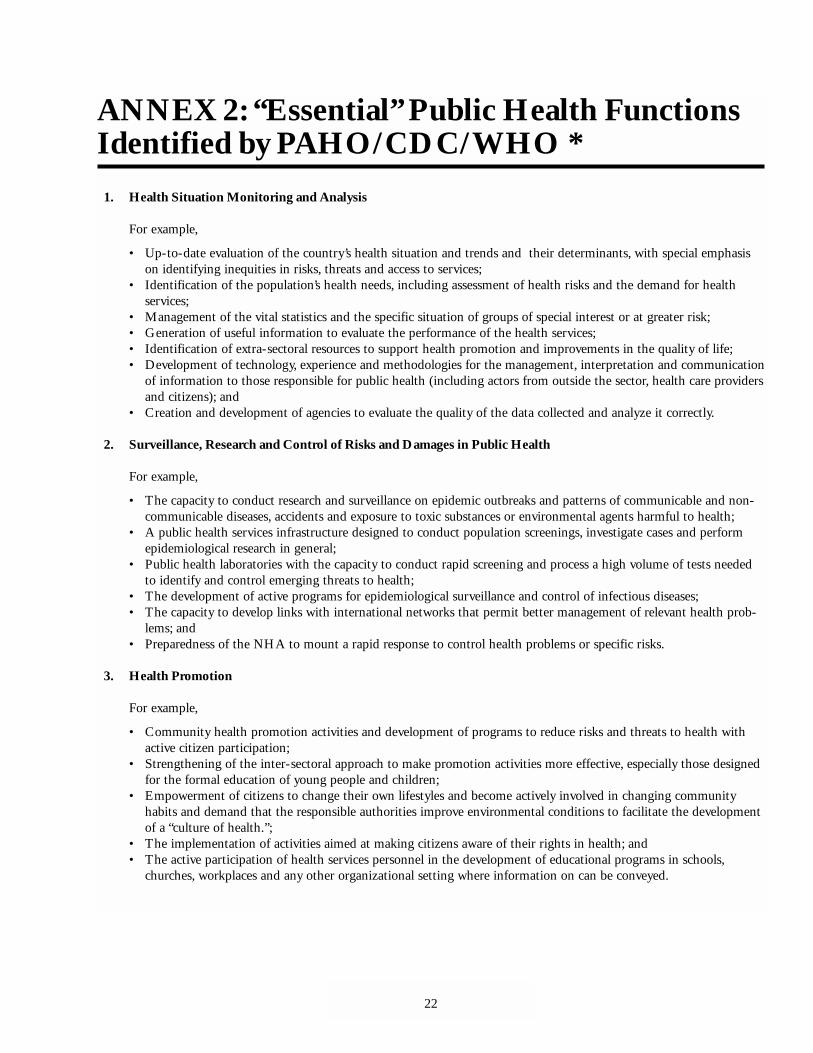
ANNEX 2: “Essential” Public Health FunctionsIdentified by PAHO/CDC/WHO *
1. Health Situation Monitoring and Analysis
For example,
• Up-to-date evaluation of the country’s health situation and trends and their determinants, with special emphasison identifying inequities in risks, threats and access to services;
• Identification of the population’s health needs, including assessment of health risks and the demand for healthservices;
• Management of the vital statistics and the specific situation of groups of special interest or at greater risk;• Generation of useful information to evaluate the performance of the health services;• Identification of extra-sectoral resources to support health promotion and improvements in the quality of life;• Development of technology, experience and methodologies for the management, interpretation and communication
of information to those responsible for public health (including actors from outside the sector, health care providersand citizens); and
• Creation and development of agencies to evaluate the quality of the data collected and analyze it correctly.
2. Surveillance, Research and Control of Risks and Damages in Public Health
For example,
• The capacity to conduct research and surveillance on epidemic outbreaks and patterns of communicable and non-communicable diseases, accidents and exposure to toxic substances or environmental agents harmful to health;
• A public health services infrastructure designed to conduct population screenings, investigate cases and performepidemiological research in general;
• Public health laboratories with the capacity to conduct rapid screening and process a high volume of tests neededto identify and control emerging threats to health;
• The development of active programs for epidemiological surveillance and control of infectious diseases;• The capacity to develop links with international networks that permit better management of relevant health prob-
lems; and• Preparedness of the NHA to mount a rapid response to control health problems or specific risks.
3. Health Promotion
For example,
• Community health promotion activities and development of programs to reduce risks and threats to health withactive citizen participation;
• Strengthening of the inter-sectoral approach to make promotion activities more effective, especially those designedfor the formal education of young people and children;
• Empowerment of citizens to change their own lifestyles and become actively involved in changing communityhabits and demand that the responsible authorities improve environmental conditions to facilitate the developmentof a “culture of health.”;
• The implementation of activities aimed at making citizens aware of their rights in health; and• The active participation of health services personnel in the development of educational programs in schools,
churches, workplaces and any other organizational setting where information on can be conveyed.
22
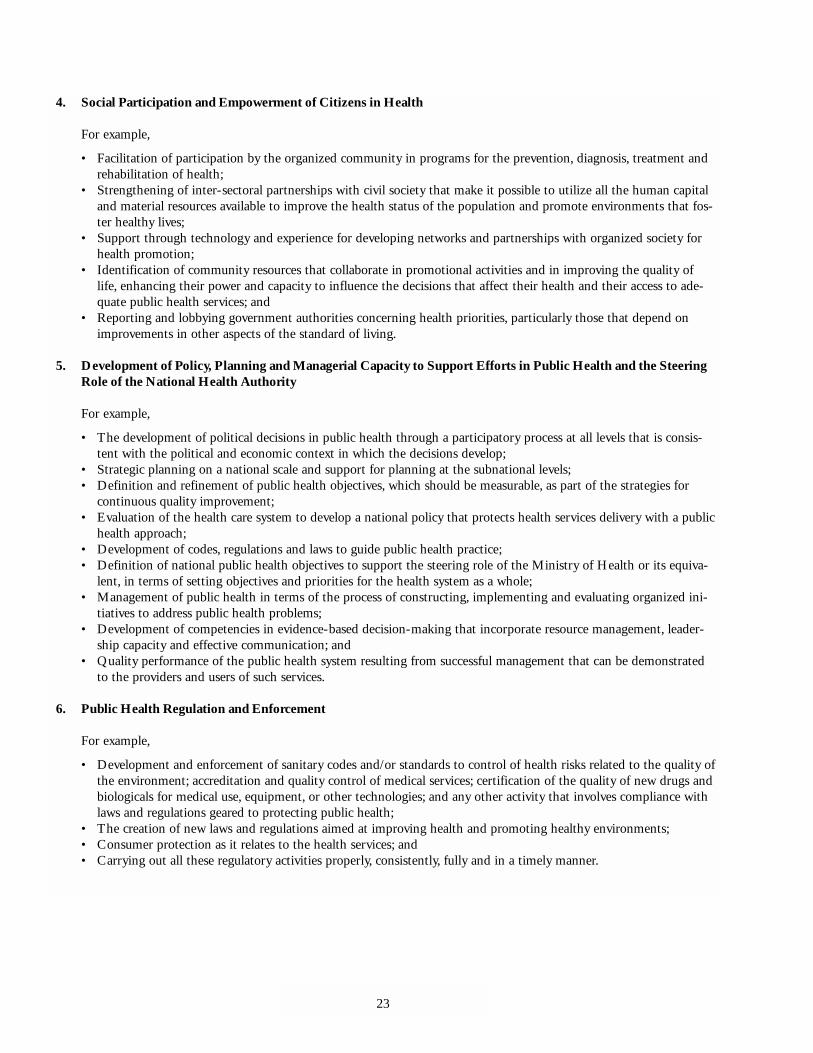
4. Social Participation and Empowerment of Citizens in Health
For example,
• Facilitation of participation by the organized community in programs for the prevention, diagnosis, treatment andrehabilitation of health;
• Strengthening of inter-sectoral partnerships with civil society that make it possible to utilize all the human capitaland material resources available to improve the health status of the population and promote environments that fos-ter healthy lives;
• Support through technology and experience for developing networks and partnerships with organized society forhealth promotion;
• Identification of community resources that collaborate in promotional activities and in improving the quality oflife, enhancing their power and capacity to influence the decisions that affect their health and their access to ade-quate public health services; and
• Reporting and lobbying government authorities concerning health priorities, particularly those that depend onimprovements in other aspects of the standard of living.
5. Development of Policy, Planning and Managerial Capacity to Support Efforts in Public Health and the SteeringRole of the National Health Authority
For example,
• The development of political decisions in public health through a participatory process at all levels that is consis-tent with the political and economic context in which the decisions develop;
• Strategic planning on a national scale and support for planning at the subnational levels;• Definition and refinement of public health objectives, which should be measurable, as part of the strategies for
continuous quality improvement;• Evaluation of the health care system to develop a national policy that protects health services delivery with a public
health approach;• Development of codes, regulations and laws to guide public health practice;• Definition of national public health objectives to support the steering role of the Ministry of Health or its equiva-
lent, in terms of setting objectives and priorities for the health system as a whole;• Management of public health in terms of the process of constructing, implementing and evaluating organized ini-
tiatives to address public health problems;• Development of competencies in evidence-based decision-making that incorporate resource management, leader-
ship capacity and effective communication; and• Quality performance of the public health system resulting from successful management that can be demonstrated
to the providers and users of such services.
6. Public Health Regulation and Enforcement
For example,
• Development and enforcement of sanitary codes and/or standards to control of health risks related to the quality ofthe environment; accreditation and quality control of medical services; certification of the quality of new drugs andbiologicals for medical use, equipment, or other technologies; and any other activity that involves compliance withlaws and regulations geared to protecting public health;
• The creation of new laws and regulations aimed at improving health and promoting healthy environments;• Consumer protection as it relates to the health services; and• Carrying out all these regulatory activities properly, consistently, fully and in a timely manner.
23
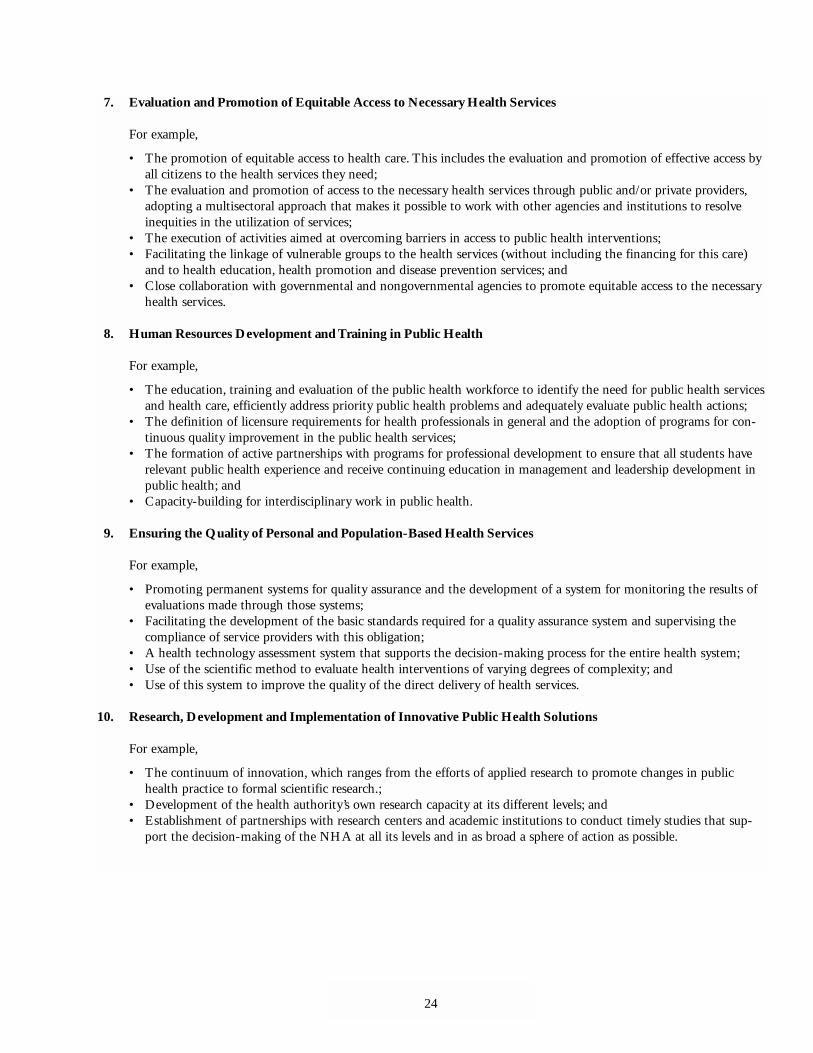
7. Evaluation and Promotion of Equitable Access to Necessary Health Services
For example,
• The promotion of equitable access to health care. This includes the evaluation and promotion of effective access byall citizens to the health services they need;
• The evaluation and promotion of access to the necessary health services through public and/or private providers,adopting a multisectoral approach that makes it possible to work with other agencies and institutions to resolveinequities in the utilization of services;
• The execution of activities aimed at overcoming barriers in access to public health interventions;• Facilitating the linkage of vulnerable groups to the health services (without including the financing for this care)
and to health education, health promotion and disease prevention services; and• Close collaboration with governmental and nongovernmental agencies to promote equitable access to the necessary
health services.
8. Human Resources Development and Training in Public Health
For example,
• The education, training and evaluation of the public health workforce to identify the need for public health servicesand health care, efficiently address priority public health problems and adequately evaluate public health actions;
• The definition of licensure requirements for health professionals in general and the adoption of programs for con-tinuous quality improvement in the public health services;
• The formation of active partnerships with programs for professional development to ensure that all students haverelevant public health experience and receive continuing education in management and leadership development inpublic health; and
• Capacity-building for interdisciplinary work in public health.
9. Ensuring the Quality of Personal and Population-Based Health Services
For example,
• Promoting permanent systems for quality assurance and the development of a system for monitoring the results ofevaluations made through those systems;
• Facilitating the development of the basic standards required for a quality assurance system and supervising thecompliance of service providers with this obligation;
• A health technology assessment system that supports the decision-making process for the entire health system;• Use of the scientific method to evaluate health interventions of varying degrees of complexity; and• Use of this system to improve the quality of the direct delivery of health services.
10. Research, Development and Implementation of Innovative Public Health Solutions
For example,
• The continuum of innovation, which ranges from the efforts of applied research to promote changes in publichealth practice to formal scientific research.;
• Development of the health authority’s own research capacity at its different levels; and• Establishment of partnerships with research centers and academic institutions to conduct timely studies that sup-
port the decision-making of the NHA at all its levels and in as broad a sphere of action as possible.
24

11. Reducing the Impact of Emergencies and Disasters on Health
For example,
• The planning and execution of public health activities in prevention, mitigation, preparedness, response and earlyrehabilitation;
• A multiple focus that addresses the threats and etiology of any and all possible emergencies or disasters that canaffect a country; and
• Participation of the entire health system and the broadest possible intersectoral cooperation to reduce the impact ofemergencies and disasters on health.
* Source: Adapted from Pan American Health Organization (PAHO). May 2000. “National Level Instrument for Measuring Essential Public Health Functions.”Public Health in the Americas. Washington DC: PAHO/U.S. Centers for Disease Control and Prevention/Centro Latino Americano de Investigaciones en Sistemas de Salud.
25

BIBLIOGRAPHY
Ahmed, K. 1999. “World Bank PredictsDevelopment for Next Century.” Lancet354:1005.
American Public Health Association(APHA). www.apha.org
Bettcher D.W., S. Sapirie, and E.H.T.Goon. 1998. “Essential Public HealthFunctions: Results of the InternationalDelphi Study.” World Health StatisticsQuarterly 51(1):44-54.
Claeson, M., C.C. Griffin, T.A. Johnston,M. McLachlan, A.L. Soucat,A.Wagstaff, and A.S. Yazbeck. June2001. “Poverty Reduction and theHealth Sector.” In Poverty ReductionStrategy Sourcebook. Washington DC:World Bank. Available at www.world-bank.org/poverty/health/library/hnptechnotes.pdf
Committee of Inquiry into the FutureDevelopment of the Public HealthFunction. 1988. Public Health inEngland. London: HMSO, Cmd 289.
Detels, R., and L. Breslow. 1984. “History,Determinants, Scope and Strategies.” InOxford Textbook of Public Health, ed.W.W. Holland, R. Detels, and G.Knox. Oxford: Oxford University Press.
Last, J.M. 1987. Public Health and HumanEcology. Sydney: Prentice-Hall.
Maas, P.J. van der, A. Hofman, E. Dekker(eds.). 1989. Epidemiologie en gezond-heidsheleid (Epidemiology and HealthPolicy). Alphen aan de Rijn: SamsonStafleu.
Merson, M.H., R.E. Black, and A.J. Mills.2001. “Introduction” in InternationalPublic Health: Diseases, Programs,Systems, and Policies. Gaithersburg,Maryland: Aspen Publishers, Inc.
Morrow, R.H. 1997. “Primary Health Careand Essential Public Health Functions.”World Health Forum 18:143-146.
Musgrave R.A., and P.B. Musgrave. 1984.Public Finance in Theory and Practice,4th ed. New York: McGraw-Hill.
Pan American Health Organization(PAHO). May 2000. “National LevelInstrument for Measuring EssentialPublic Health Functions.” Public Healthin the Americas. Washington DC:PAHO/U.S. Centers for DiseaseControl and Prevention/Centro LatinoAmericano de Investigaciones enSistemas de Salud.
______. October 2000. “Essential PublicHealth Functions.” Health SectorReform: Reassessing Implications forPAHO’s Technical Cooperation. PAHOAnnual Managers Meeting.Washington DC: PAHO.
Petersen, A. and D.Lupton. 1996. The NewPublic Health: Health and Self in the Ageof Risk. London: SAGE Publications.
Simon, J., S. Rosen, M. Claeson, A.Breman, J. Tulloch. 2001. The FamilyHealth Lifecycle: From Concept toImplementation. Washington DC:World Bank.
Winslow, C.E.A. 1920. The Untilled Fieldsof Public Health. Science, N. S., Vol. 51,p. 23.
______.1951. “The Cost of Sickness andthe Price of Health.” WHO Monograph7:28. Geneva: World HealthOrganization.
World Bank. 1997a. Sector Strategy: Health,Nutrition and Population. WashingtonDC: World Bank.
______. 1997b. World Development Report1997: The State in a Changing World.Washington DC: World Bank.
______. 2001a. Public Health at a GlanceFact Sheets. Available atwww.worldbank.org/hnp
______. 2001b. World Bank StrategicFramework. Available atwww.worldbank.org/whatwedo/strategies.htm
______. 2001c. Monitoring Progress towardsthe HNP Development Goals Using thePRSP Framework. Available at the webwww.worldbank.org/hnpmdg
World Health Organization (WHO).1966. “The Education of the PublicHealth Physician in Relation to hisWork in the Community: Report on aSymposium.” EURO: 337:3. Lisbon.
______. 1999. World Health Report 1999:Making a Difference. Geneva: WHO.
______. 2000. World Health Report 2000:Health Systems—ImprovingPerformance. Geneva: WHO.
26
Public Health andWorld Bank Operations
The World Bank
The Human Development NetworkHealth, Nutri t ion, and Population Series
THE WORLD BANK
1818 H Street, NW
Washington, DC 20433 USA
Telephone: 202.477.1234
Facsimile: 202.477.6391
Telex: MCI 64145 WORLDBANK
MCI 248423 WORLDBANK
Internet: www.worldbank.org
E-mail: [email protected]
T H E W O R L D B A N K
HEAL TH, NUTRITION, AND POPULA TION





























