Embed Size (px)
Citation preview

E728Volume 2
Tonga Health Care ProjectHealth Care Waste Management
Feasibility Study
March 3, 2002
Alfred PicardiSenior Environmental Management Consultant
327 Rosslare DriveArnold, MD 21012
001 (410) 544 - 4295alpicardi @ cablespeed.com
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

Tonya Health Care ProiectHealth Care Waste Management Feasibility Study
Contents
Chapter 1 Introduction
Chapter 2 Background on Health Care Waste
Chapter 3 Review of Current Situation
Chapter 4 Review of Health Care Waste Treatment Technologies
Chapter 5 Options for Treatment and Disposal of Health Care Wastes in Tonga
Chapter 6 Recommendations for Implementation
Annexes:
Annex 1 List of Persons Interviewed and Facilities Visited
Annex 2 Photographs
Annex 3 WHO Guidelines for Incinerator Emissions
Annex 4 Consultant Terms of Reference
Annex 5 DefinitionsAnnex 6 Wastewater Treatment Plant Specifications
2

Chapter 1
Introduction
The World Bank is currently assisting the Government of the Kingdom of Tonga inpreparing a project to support the country's health sector reform. The specific objectiveof the project is to (i) improve the capacity of the Ministry of Health to develop andimplement health financing policy and collect, manage and use health information, and(ii) improve the administrative, functional and technical quality of Vaiola Hospital.
A component of the project will support the redevelopment of Vaiola Hospitalinfrastructure and facilities, to overcome identified major deficiencies, improve thefunctional relationships and overall operational efficiency of the hospital, and enhancethe hospital's capacity to efficiently meet its future service obligations. Thesedevelopments will be guided by a master plan for the hospital, which is to be preparedduring project preparation.
Medical waste generated by the Ministry of Health facilities will likely increase, inquantity and variety. This feasibility study was undertaken as a step to minimize potentialadverse human health and environmental impacts of waste generated by the hospital, andto recommend actions to establish an environmentally sustainable health care wastemanagement system. The terms of reference for the study is in Annex 4.
3

Chapter 2
Background on Health Care Waste
Waste Characterization
Almost 80% of the total of wastes generated by health-care activities are general wastecomparable to domestic waste. The remaining approximate 20% of wastes are consideredhazardous materials that may be infectious, toxic or radioactive. Infectious wastes aredefined to include discarded sharps and infectious non-sharp materials.
Sharps consist of syringe or other needles, blades, broken glass or other items that cancause injury.
Infectious non-sharps include materials that have been in contact with blood or bodyfluids of patients, such as bandages, swabs or items soaked with blood. Excreta is also aninfectious waste.
Non-infectious wastes are materials that have not been in contact with patients, ad mayinclude paper and plastic packaging, metal, glass or other wastes which are similar tohousehold wastes.
The wastes and by-products cover a diverse range of materials, as the following listillustrates (percentages are approximate values):
* Infectious wastes - cultures and stocks of infectious agents, wastes from infectedpatients, wastes contaminated with blood and its derivatives, discarded diagnosticsamples, infected animals from laboratories, and contaminated matenals (swabs,bandages) and equipment (disposable medical devices etc.); and
* Anatomic - recognizable body parts and animal carcasses.
Infectious and anatomic wastes together represent the majority of the hazardous waste, upto 15% of the total waste from health-care activities.
* Sharps - syringes, disposable scalpels and blades etc.
Sharps represent about 1% of the total waste from health-care activities.
* Chemicals - for example solvents and disinfectants; and
* Pharmaceuticals - expired, unused, and contaminated; whether the drugsthemselves (sometimes toxic and powerful chemicals) or their metabolites,vaccines and sera .
Chemicals and pharmaceuticals amount to about 3% of waste from health-care activities.
* Genotoxic waste - highly hazardous, mutagenic, teratogenic or carcinogenic, suchas cytotoxic drugs used in cancer treatment and their metabolites; and
1

* Radioactive matter, such as glassware contaminated with radioactive diagnosticmaterial or radiotherapeutic materials;
* Wastes with high heavy metal content, such as broken mercury thermometers.
Genotoxic waste, radioactive matter and heavy metal content represent about 1% of thetotal waste from health-care activities.
The major sources of health-care waste are hospitals and other health-careestablishments, laboratories and research centers, mortuary and autopsy centers, animalresearch and testing laboratories, blood banks and collection services, and nursing homesfor the elderly.
High-income countries can generate up to 6 kg of hazardous waste per person per year. Inthe majority of low-income countries, health-care waste is usually not separated intohazardous or non-hazardous waste. In these countries, the total health-care waste perperson per year is anywhere from 0.5 to 3 kg.
Risks Caused by Poor Management of Health Care Wastes
Health-care waste management is an integral part of health-care, and creating harmthrough inadequate waste management reduces the overall benefits of health-care. Poormanagement of health-care waste can cause serious disease in health-care personnel,waste workers, patients and the general public. The main source of illness frominfectious waste is probably injuries from used needles, which can cause hepatitis andHIV. There are however numerous other diseases which could be transmitted by contactwith health-care wastes.
Health-care waste is a reservoir of potentially harmful micro-organisms which can infecthospital patients, health-care workers and the general public. Other potential infectiousrisks include the spread of, sometimes resistant micro-organisms from health-careestablishments into the environment. These risks have so far been only poorlyinvestigated. Wastes and by-products can also cause injuries, for example radiation burnsor sharps-inflicted injuries; poisoning and pollution, whether through the release ofpharmaceutical products, in particular, antibiotics and cytotoxic drugs, throughimproperly treated waste water discharge or by toxic elements or compounds such asmercury or dioxins.
Occupational Risk
During handling of wastes, health-care personnel and waste workers (within and outsidethe health care facility) can come in contact with waste if it hasn't been packaged safely.Many injuries occur because syringe needles or other sharps have not been collected insafety boxes, or because these have been overfilled. Also, contact with other infectiouswaste that has not been packaged or treated adequately may cause a risk. On landfills orwaste dumps, waste recyclers or scavengers may come in contact with infectious wastesif the wastes have been disposed of without pnor treatment.
2
Risk to the Public
The reuse of syringes by the general public represents one of the greatest public healthproblems in the developing world related to health-care waste. Worldwide, an estimated10 to 20 million infections of Hepatitis B and C and HIV occur annually from the reuseof discarded syringe needles without pnor sterilisation [Kane et al, 2000]. If health-carewaste is dumped on un-controlled sites or in other areas that can be accessed by thepublic, the public and in particular children can come in contact with infectious wastes.In addition, the contact with toxic chemicals, such as disinfectants, may cause accidentswhen they are accessible to the public.
Sharps
Throughout the world every year an estimated 12,000 million injections are administered.And not all needles and syringes are properly disposed of, generating a considerable riskfor injury and infection and opportunities for re-use.
Worldwide, 8-16 million hepatitis B, 2.3 to 4.7 million hepatitis C and 80,000 to160,000 HIV infections are estimated to occur yearly from re-use of syringeneedles without sterilization. Many of these infections could be avoided ifsynnges were disposed of safely. The re-use of disposable syringes and needlesfor injections is particularly common in certain African, Asian and Central andEastern European countnes.
* Regarding injection practices, public health authorities in West Bengal, India,have recommended a shift to re-usable glass syringes, as the disposalrequirements for disposable syringes could not be enforced.
* In developing countries, additional hazards occur from scavenging on wastedisposal sites and manual sorting of the waste stored at the back doors of health-care establishments. These practices are common in many regions of the world.The waste handlers are at immediate risk of needle-stick injuries and otherexposures to toxic or infectious materials.
Vaccine Waste
In June 2000, six children were diagnosed with a mild form of smallpox (vaccinia virus)after having played with glass ampoules containing expired smallpox vaccine at agarbage dump in Vladivostok, Russia. Although the infections were not life-threatening,the vaccine ampoules should have been treated before being discarded.
Radioactive Wastes
The use of radiation sources in medical and other applications is widespread throughoutthe world. Occasionally, the public is exposed to radioactive waste, usually originatingfrom radiotherapy treatments, that has not been properly disposed of. Serious accidentshave been documented in Goiania, Brazil in 1988 in which four people died from acuteradiation syndrome and 28 suffered serious radiation burns. Similar accidents happened
3

in Mexico City in 1962, Algeria in 1978, Morocco in 1983 and Ciudad Juarez in Mexicoin 1983.
Risks Associated with Waste Disposal
Although treatment and disposal of health-care wastes aim at reducing nsks, indirecthealth risks may occur through the release of toxic pollutants into the environmentthrough treatment or disposal.
* Landfilling can potentially result in contamination of drinking water. Occupationalrisks may be associated with the operation of certain disposal facilities.
* Inadequate incineration, or incineration of materials unsuitable for incineration canresult in the release of pollutants into the air. The incineration of materials containingchlorine can generate dioxins and furans, which are classified as possible humancarcinogens and have been associated with a range of adverse effects. Incineration ofheavy metals or materials with high metal contents (in particular lead, mercury andcadmium) can lead to the spread of heavy metals in the environment. Dioxins, furansand metals are persistent and accumulate in the environment. Materials containingchlorine or metal should therefore not be incinerated.
* Only modem incinerators are able to work at 800-1000 °C, with special emission-cleaning equipment, can ensure that no dioxins and furans (or only insignificantamounts) are produced. Smaller devices built with local materials and capable ofoperating at these high temperatures are currently being field-tested and implementedin a number of countries.
'Background section source: WHO Fact Sheet N° 253 October 2000
4

Chapter 3
Review of Current Situation in Tonga
Existing Kingdom of Tonga Laws and Regulations
Existing and planned laws and regulations related to sanitary sewage and health carewaste disposal were reviewed with the Minister and senior staff of the Ministry of Healthas well as staff of the Department of Environment. The only existing legislation orregulation concerning these issues is the Public Health Act of 1992.
The Ministry of Health administers the Public Health Act. The Act in a general way laysthe groundwork for environmental management. According to the Act, "Any person whocreates or allows the creation of dust, smoke, fumes, effluvia, effluent or noise which is anuisance or prejudicial to the health of the inhabitants of the neighborhood or to thehealth of any person is guilty of an offense," (Part II Summary Offenses, para. 21). Thereare no regulations at this time which define what constitutes a nuisance or prejudice tohealth with which to enforce the Act.
The Department of Environment has been newly created this year under the Minister ofWorks, Environment and Marine. The Department is still developing regulations andlegislation. A bill requinng Environmental Impact Assessment is currently with the LawReform Committee. This bill may reach Parliament next year.
Current Health Care Waste Management Practices in Tonga, Ministry of HealthFacilities
The Ministry of Health operates several health care facilities in Tonga, and there aresome private clinics, but no private hospital facilities. The Public Health Inspectors areresponsible for collection and disposal of health care waste, along with other duties suchas inspection of potable water well installations and private sewage disposal facilities.
Senior staff were interviewed at the Vaiola and Prince Ngu Hospital facilities in order toreview management of health care waste. Discussions were held with the Public HealthInspectors who are responsible for the collection, transport and disposal of the HCW atboth locations. Site tours included the wastewater treatment facilities. The waste disposalareas currently used by the hospitals were also visited in order to assess environmentalconditions and potential hazards.
The Ministry of Health does not currently have a formal Health Care Waste ManagementPolicy, or a Health Care Waste Management Plan.
1

The Ministry of Health operates three hospitals and thirty-three maternal health clinicsthroughout the country.
Location FacilitesTongatapu Vaiola Hospital
7 health centersVava'u Prince Ngu Hospital
4 health centersHa'apai Niu'ui Hospital
2 health centers'Eua Niu'eiki Hospital
Health Care Waste Management at Vaiola Hospital
The 200 bed Vaiola Hospital is located in the city of Nuku'alofa, Tongatapu. Servicesprovided include: medicine, Ob/gyn, surgery, pediatrics, emergency medicine, radiology,laboratory, ear nose and throat and dentistry.
According to staff estimates, Vaiola Hospital generates about one 55-gallon drum ofgeneral domestic waste, two boxes of sharps (less than one kilogram), and half a 55-gallon drum (approximately 18 pounds or 9 kilograms 2) or less of infectious waste perday. There are no estimates of volumes of chemical or pharmaceutical waste. About onecase of thyroid (radioactive) medicine is used per year.
Within the hospital, waste is moved in closed containers. There are no designatedcontainers for infectious waste. Puncture-proof containers are used for storage of usedsharps. There is no designated storage area for health care waste, other than the generalrubbish bin. There is no temperature control for the rubbish bin. There is no color codingsystem to designate hazardous or infectious wastes.
Vaiola Hospital has developed an Infection Control Manual. This manual briefly outlinesa health care waste segregation and treatment program. According to the wastemanagement outline the following types of waste would be segregated for separate andappropriate treatment: paper; garden waste; human tissue; syringes and sharps; and,general garbage. The waste management outline specifies that sharps and infectiouswaste shall be incinerated. There are no training programs in place concerning healthcare waste risk for staff or handlers of health care waste. The Infection Control Manualaddresses needle stick injuries, and a needle stick injury reporting system has just beeninitiated.
The hospital uses disposable syringes. Currently sharps are segregated and autoclaved, atreatment acceptable to WHO: There are currently two autoclaves in operation at VaiolaHospital:
2As a rule of thumb health care waste weighs about 5 pounds per cubic foot. 1/2 drum = 27 gallons = 3.6cubic feet
2

1. Choong Wave - Model CHS-AC250, Serial # 020019, Frequency 50/60Hz, VoltageAC38OV, Input 14.5KW, Manufacture Date 9/2002, size 4ft deep, 6fttall, 2ft wide
2. Rexall Industries Co. LTD. - Model LS-5AXL, Serial 90015, Chamber Diameter60cm, Chamber Depth 120cm, Working Pressure 1.3kg/cm2, HydroTestedPower 3.6 kg/cm2(squared), Sterilizing Temperature 122 C, Power Supply 240,Manufacture Date 2-17-1990
Some infectious waste, including operating room waste (body parts) and laboratory waste(urine samples, test tubes and cultures, and serum) is autoclaved prior to disposal. Out ofdate blood is autoclaved and used for lab media or disposed. Not all of the infectiouswaste is autoclaved.
According to maintenance staff, Vaiola Hospital used an open container on the back ofthe hospital property to bum infectious waste in the past. This is no longer the practice.
Pharmaceutical waste is disposed along with the general domestic waste. Lab chemicalsare collected in plastic and disposed with the general waste or dumped into thewastewater treatment system via the sink. Silver from x-ray developing is recycled onsite. Thermometers are disposed along with the general domestic waste. Oxygencylinders are refilled on site. Nitrous oxide, carbon dioxide, and air cylinders are sent toFiji for refilling.
The general waste and the (treated and untreated) infectious and other health care wastesare commingled and collected in household garbage bags without color coding. An off-site municipal open dump is used for disposal of health care waste from Vaiola Hospital.The dump is used by the entire community and is freely accessed by the public, domesticand wild animals, and poses an ongoing human health and environmental risk..
Risks from Current Waste Management Practices
Practice: Infectious waste is not collected in designated containers.
Risk: There is risk of infection by personnel who handle the containers, who may notrealize the containers are potentially infected. The containers may not be disinfected on aregular basis, prolonging the infection hazard. WHO guidelines call for segregation ofhealth care waste (hazardous and non-hazardous, chemical, sharps) into color-coded anddesignated containers in order to protect hospital staff and the public from inadvertentexposure.
Practice: There is no designated storage area for health care waste, other than the generalrubbish bin. There is no temperature control for the rubbish bin.
3

Risk: There is risk of infection by personnel who handle the containers, who may notrealize the containers are potentiaily infected. WHO guidelines call for separate, secured(locked) temperature-controlled storage areas for hazardous health care waste, to avoidproliferation of infectious agents.
Practice: There are no training programs in place concerning health care waste risk forstaff or handlers of health care waste.
Risk: Hospital staff may become exposed, or expose the public, to hazardous health carewaste (and needle-stick injuries/infections) due to a lack of awareness of the hazards.
Practice: Some infectious waste, including operating room waste (body parts) andlaboratory waste (urine samples, test tubes and cultures, and serum) is autoclaved prior todisposal.
Risk: When doctors operate, body parts could end up in the waste stream. These bodyparts need special attention. The EPA does not allow for the discharge of body parts tolandfills due to aesthetic reasons, and WHO does not consider landfilling a suitabledisposal option for anatomical waste. Wet thermal treatment is not suitable for treatment
3of anatomical waste, according to WHO .
Practice: Not all of the infectious waste is autoclaved.
Risk: There is risk of infection by personnel who handle the containers, as well asexposure of the public from spills during transportation, and at the disposal area.
Practice: There is no designated vehicle for transport of health care waste. The generalrubbish disposal vehicle is used.
Risk: The transport vehicle can carry infectious agents into the community it serves, andexpose waste transport workers as well as the public to hazardous health care waste.WHO guidelines call for a dedicated transport vehicle that is equipped to contain spillage,and can be thoroughly cleaned (sterilized) on a regular basis. The transport vehicleshould have an impermeable bulkhead between the waste and the operator(s).
Practice: Pharmaceutical waste is disposed along with the general domestic waste. Labchemicals are collected in plastic and disposed with the general waste or dumped into thewastewater treatment system via the sink. Thermometers are disposed along with thegeneral domestic waste.
Risk: Toxic chemicals and heavy metals (mercury in thermometers for example) in theseunsegregated waste streams are not properly treated or disposed, allowing them to bereleased into the environment. 1) during transport in a vehicle that is not contained toprevent spillage; 2) through the wastewater treatment system; and 3) once released at the
3Chapter 9, Safe Management of Wastes from Health Care Activities, WHO, 1999.
4
open dump which does not have controlled access for humans and disease vectors, aircontaminant, groundwater contaminant or stormwater runoff controls. WHO guidelinescall for the segregation and proper treatment of each type of health care waste stream.
Sanitary Wastewater Treatment at Vaiola Hospital
The sanitary wastewater treatment system at Vaiola Hospital has deteriorated and isbeyond its useful life. The chambers have been retrofitted with bubblers that provide littleeffective aeration, furthermore, the chambers appear to be clogged with an accumulationof sludge. It is doubtful that designed flow through the treatment chambers, with controlof activated sludge retention times for optimal treatment is controlled or possible. Thesanitary wastewater is receiving little treatment, and the stagnant effluent receiving pondcan be accessed by the public, domestic and wild animals, and poses a potential hazard tohuman health and the environment. The hospital was once isolated, but a residential areahas grown up around the facility. Staff report that there have been odor complaints fromthe community, concerning odors from the wastewater treatment system. Under thePublic Health Act of 1992, creation of nuisance odors is an offense (Part II para.22) as isallowing a sanitary convenience to be in such a condition as to be a nuisance orprejudicial to health (Part II Para. 28).
Health Care Waste Management at Prince Ngu Hospital
The Prince Ngu Hospital was refurbished in 1981 with grant money from Aus AID,including new metal roofs. The facility has 61 beds, with an average occupancy rate offorty to fifty percent. During epidemics the occupancy rate can be as high as sixty toseventy percent. Recent epidemics have been viral (Rubella), and there are sometuberculosis cases.
Services provided by the hospital include: medical; Ob/gyn; pediatrics; diabetes clinic;minor surgery; vaccinations; laboratory; and, emergency medicine. Evacuations aremade via private carrier or the Tongan Army aircraft stationed at Vava'u. The hospitaldoes not have blood storage facilities. The hospital has some tuberculosis cases.Tuberculosis is a persistent pathogen in the environment, and poses a special risk ininfectious wastestreams.
The hospital does not provide training in health care waste hazards, nor is there a budgetfor health care waste management. No records are kept of needle stick injuries.
General domestic, pharmaceutical, infectious waste and mercury thermometers arecommingled and collected in plastic household type garbage bags. The plastic bags arestored in open 55-gallon drums prior to disposal. The storage area is not closed or airconditioned. Waste laboratory chemicals are drained to the septic tank (that does not havea leachfield) via the sink. There is no recycling of silver from x-ray film development.
Waste sharps are segregated, but not disinfected. The sharps are bent by the PublicHealth officer or his staff pnor to being buried in the open town dump. This practice
5
poses a hazard for the waste handlers, as well as a human health and environmental riskat the open dump site.
According to the Public Health Act, waste containers are to be equipped with tight-fittinglids. Infectious medical waste at Prince Ngu Hospital is commingled with general wastein household garbage bags, and stored next to a rear entrance to the hospital in open 55-gallon drums. About two drums of commingled waste is removed from the hospital fourtimes per week. The waste bags are transported in an open truck, and disposed in themunicipal open dump. The household garbage bags sometimes break open before thetransport truck reaches the dump, presenting a hazard to the communities along the haulroute, as well as the waste handlers.
The open dump can be freely accessed by the public, domestic and wild animals, andpresents a human health and environmental hazard. The dump is adjacent to an estuary,and there is a village on the shore of this estuary several hundred meters from the dumpsite.
Water Supply and Sanitary Wastewater Treatment at Prince Ngu Hospital
The hospital has a chlorinated water supply, however the Public Health Inspector lacks achlorine residual test kit to test the water supply for safety.
There are flush toilets in the hospital, but sewage treatment and disposal is not adequate.The sanitary sewage is piped to an underground tank which, according to the PublicHealth Inspector, overflows to the ground on vacant land adjacent to the hospital. Thisarea can be freely accessed by the public, domestic and wild animals, and presents ahuman health and environmental hazard.
6

Chapter 4
Review of Health Care Waste Treatment Technologies
The following are WHO recognized health care waste treatment technologies in useworldwide.
Chemical Disinfection
Chemical disinfection, used routinely in health care to kill microorganisms on medicalequipment and on floors and walls, is now being extended to the treatment of health-carewaste. Chemicals are added to waste to kill or inactivate the pathogens it contains; thistreatment usually results in disinfection rather than sterilization. Chemical disinfectionis most suitable for treating liquid waste such as blood, urine, stools, or hospital sewage.However, solid-and even highly hazardous-health-care wastes, includingmicrobiological cultures, sharps, etc., may also be disinfected chemically, with thefollowing limitations:
* Shredding and/or milling of waste is usually necessary before disinfection;* The shredder is often the weak point in the treatment chain, being subject to
frequent mechanical failure or breakdown.* Powerful disinfectants are required, which are themselves also hazardous and
should be used only by well trained and adequately protected personnel.* Disinfection efficiency depends on operational conditions.* Only the surface of intact solid waste will be disinfected.
Human body parts and animal carcasses should not normally be disinfected chemically. Ifalternative facilities for disposal are not readily available, however, they may be shreddedand then subjected to chemical disinfection. In planning the use of chemical disinfection,requirements for the eventual disposal of the residues should be carefully considered;improper disposal could give rise to serious environmental problems.
At present, chemical disinfection of health-care waste is limited in industrializedcountries. However, it is an attractive option for developing countries, particularly fortreating highly infectious physiological fluids, such as patients' stools in case of choleraoutbreaks.
Chemical disinfection is usually carried out on hospital premises. Recently, however,commercial, self-contained, and fully automatic systems have been developed for health-care waste treatment and are being operated in industrial zones. The disinfected wastemay be disposed of as non-risk health-care waste, but the chemical disinfectants maycreate serious environmental problems in case of leakage or after disposal 4.
4 Source: Safe Management of Wastes from Health Care Activities, WHO, 1999.
1
Chemical shredding systems do not consistently achieve a kill rate as high as sterilisationand therefore are not as effective at killing viral and spore forming pathogens.
Given the situation with landfill availability, and the vulnerability of groundwaterresources in Tonga, as well as the nature and variety of the health care waste that must betreated, disinfection is not recommended as a viable option.
Disinfection is not a suitable treatment option for anatomical waste, pharmaceuticalwaste, cytotoxic waste, chemical waste, or radioactive waste.
Wet Thermal Treatment
Wet thermal-or steam-disinfection is based on exposure of shredded infectious wasteto high-temperature, high-pressure steam, and is similar to the autoclave sterilizationprocess. It inactivates most types of microorganisms if temperature and contact time aresufficient; for sporulated bacteria, a minimum temperature of 121°C is needed. About99.99% inactivation of microorganisms may be expected, compared with the 99.9999%achievable with autoclave sterilization.
The wet thermal process requires that waste be shredded before treatment; for sharps,milling or crushing is recommended to increase disinfection efficiency. The process isinappropriate for the treatment of anatomical waste and animal carcasses, and will notefficiently treat chemical or pharmaceutical wastes.
The disadvantages of the wet thermal process are the following:
* the shredder is liable to mechanical failure and breakdown;5* the efficiency of disinfection is very sensitive to the operational conditions.
The state of New Jersey stipulates that sterilizers utilized for waste treatment shall not beutilized for sterilization of equipment, food or other related items. (Note: This onlyapplies to units that are used to sterilize equipment, i.e., syringes, that will be used onhumans. Equipment used on animals is not covered under this requirement.)
Wet thermal treatment is not suitable for anatomical waste, pharmaceutical waste,cytotoxic waste, chemical waste or radioactive waste.
Microwave Irradiation
Most microorganisms are destroyed by the action of microwaves of a frequency of about2450 MHz and a wavelength of 12.24cm. The water contained within the wastes israpidly heated by the microwaves and the infectious components are destroyed by heatconduction.
5 Source: Safe Management of Wastes from Health Care Activities, WHO, 1999.
2

The microwave process is widely used in several countries and is becoming increasinglypopular. However, relatively high costs coupled with potential operation and maintenanceproblems mean that it is not yet recommended for use in developing countries. Similar
6processes using other wavelengths or electron beams are also being developed .
Microwave systems do not kill spores or viruses that require temperatures above 95 degC for satisfactory kill rates.
The process requires a shredder, which involves high capital and maintenance costs,(about $50,000 for a small unit, plus $20,000 for the shredder) and is not recommendedby WHO for developing countries.
Wet thermal treatment is not suitable for disposal of anatomical waste, pharmaceuticalwaste, cytotoxic waste, chemical waste, or radioactive waste.
Land Disposal
If a municipality or medical authority genuinely lacks the means to treat wastes beforedisposal, the use of a landfill has to be regarded as an acceptable disposal route. Allowinghealth-care waste to accumulate at hospitals or elsewhere constitutes a far higher nsk ofthe transmission of infection than careful disposal in a municipal landfill, even if the siteis not designed to the standard used in higher-income countries. The primary objectionsto landfill disposal of hazardous health-care waste, especially untreated waste, may becultural or religious or based on a perceived risk of the release of pathogens to air andwater or on the risk of access by scavengers.
There are two distinct types of waste disposal to land- open dlumps andsanitary landfills.
* Open dunmps are characterized by the uncontrolled and scattered deposit ofwastes at a site; this leads to acute pollution problems, fires, higher risks ofdisease transmission, and open access to scavengers and animals. Health-carewaste should not be deposited on or around open dumps. The risk of eitherpeople or animals coming into contact with infectious pathogens is obvious,with the further risk of subsequent disease transmission, either directlythrough wounds, inhalation, or ingestion, or indirectly through the food chainor a pathogenic host species.
* Sanitary landfills are designed to have at least four advantages over opendumps: geological isolation of wastes from the environment, appropriateengineering preparations before the site is ready to accept wastes, staff presenton site to control operations, and organized deposit and daily coverage ofwaste. Disposing of certain types of health-care waste (infectious waste andsmall quantities of pharmaceutical waste) in sanitary landfills is acceptable;sanitary landfill prevents contamination of soil and of surface water and
6 ibid.
3
groundwater, and limits air pollution, smells, and direct contact with thepublic.
Upgrading from open dumping directly to sophisticated sanitary landfills may betechnically and financially difficult for many municipalities. It has often been foundimpossible to sustain such efforts from the available local resources. However, this is noreason for municipal authorities to abandon the move towards safer land disposaltechniques. In the absence of sanitary landfills, any site from a controlled dump upwardscould accept health-care waste and avoid any measurable increase in infection risk. Theminimal requirements would be the following:
* an established system for rational and organized deposit of wastes which could beused to dispose of health-care wastes;
* some engineering work already completed to prepare the site to retain its wastesmore effectively;
* rapid burial of the health-care waste, so that as much human or animal contact aspossible is avoided.
It is further recommended that health-care waste be deposited in one of the two followingways:
* In a shallow hollow excavated in mature municipal waste in the layer belowthe base of the working face, and immediately covered by a 2-metre layer offresh municipal waste. Scavenging in this part of the site must be prevented.The same method is often used for hazardous solid industrial wastes; it isspecifically intended to prevent animals and scavengers from re-excavatingthe deposited healthcare waste.
* In a deeper (1-2m) pit excavated in mature municipal waste (i.e. wastecovered at least 3 months previously). The pit is then backfilled with themature municipal waste that was removed. Scavenging in this part of the sitemust be prevented.
Alternatively, a special small burial pit could be prepared to receive health-care wasteonly. The pit should be 2m deep and filled to a depth of 1-1.5 m. After each waste load,the waste should be covered with a soil layer 10-15cm deep. If coverage with soil is notpossible, lime may be deposited over the waste. In case of outbreak of an especiallyvirulent infection (such as Ebola virus), both lime and soil cover may be added. Accessto this dedicated disposal area should be restricted, and the use of a pit would makesupervision by landfill staff easier and thus prevent scavenging7.
Off premises sanitary landfill disposal is not suitable for anatomical waste, sharps,cytotoxic waste, chemical or radioactive waste, according to WHO. On-premises safebunal is not suitable for cytotoxic waste and radioactive waste, and WHO recommends
7 Source. Safe Management of Wastes from Health Care Activities, WHO, 1999.
4
only small quantities of pharmaceutical and chemical waste be disposed in this manner.In the case of Viaola Hospital, with vulnerable groundwater supplies, it is recommendedthat no pharmaceutical or chemical waste be disposed in this manner. Once plans forwater supply for the hospital are finalized, including well placement and characterizationof hydrogeologic strata, the use of on-site disposal should be given a thoroughenvironmental review.
Encapsulation Prior to Landfill
Disposal of health-care waste in municipal landfills is less advisable if it is untreated thanif it is pretreated. One option for pretreatment is encapsulation, which involves fillingcontainers with waste, adding an immobilizing material, and sealing the containers. Theprocess uses either cubic boxes made of high-density polyethylene or metallic drums,which are three-quarters filled with sharps and chemical or pharmaceutical residues. Thecontainers or boxes are then filled up with a medium such as plastic foam, bituminoussand, cement mortar, or clay material. After the medium has dried, the containers aresealed and disposed of in landfill sites.
This process is relatively cheap, safe, and particularly appropriate for establishments thatpractise minimal programs for the disposal of sharps and chemical or pharmaceuticalresidues. Encapsulation alone is not recommended for non-sharp infectious waste, butmay be used in combination with burning of such waste. The main advantage of theprocess is that it is very effective in reducing the risk of scavengers gaining access to the
8hazardous health-care waste .
This treatment method may be useful in disposing of pharmaceutical waste, if there isonly a small quantity.
Inertization
The process of "inertization" involves mixing waste with cement and other substancesbefore disposal in order to minimize the risk of toxic substances contained in the wastemigrating into surface water or groundwater. It is especially suitable, for pharmaceuticalsand for incineration ashes with a high metal content (in this case the process is alsocalled "stabilization").
For the inertization of pharmaceutical waste, the packaging should be removed, thepharmaceuticals ground, and a mixture of water, lime, and cement added. Ahomogeneous mass is formed and cubes (e.g. of Im3) or pellets are produced on site andthen can be transported to a suitable storage site. Alternatively, the homogeneous mixturecan be transported in liquid state to a landfill and poured into municipal waste.
The following are typical proportions for the mixture:65% pharmaceutical waste15% lime
8 ibid.
5

15% cement5% waterThe process is reasonably inexpensive and can be performed using relativelyunsophisticated equipment. Other than personnel, the main requirements are a grinder orroad roller to crush the pharmaceuticals, a concrete mixer, and supplies of cement, lime,and water9 .
Incineration of wastes with mercury or cadmium is not acceptable. The inertizationmethod may be considered for disposal of pharmaceuticals and waste with high heavymetal content. It is not acceptable as a disposal method for mercury. Mercury wasteshould be recycled.
Pyrolytic Incineration
The most reliable and commonly used treatment process for health-care waste is pyrolyticincineration, also called controlled air incineration or double-chamber incineration. Thepyrolytic incinerator comprises a pyrolytic chamber and a post combustion chamber andfunctions as follows:
* In the pyrolytic chamber, the waste is thermally decomposed through anoxygen-deficient, medium-temperature combustion process (800-9000C),producing solid ashes and gases. The pyrolytic chamber includes a fuelburner, used to start the process. The waste is loaded in suitable waste bags orcontainers.
* The gases produced in this way are burned at high temperature (900-1200°C)by a fuel burner in the post-combustion chamber, using an excess of air tominimize smoke and odours.
Adequately maintained and operated pyrolytic incinerators of limited size, as commonlyused in hospitals, do not require exhaust-gas cleaning equipment. Their ashes will containless than 1% unburnt material, which can be disposed of in landfills. However, to avoiddioxin production, no chlorinated plastic bags (and preferably no other chlorinatedcompounds) should be introduced into the incinerator, and should therefore not be usedfor packaging waste before its incinerationl. WHO guidelines for emissions from healthcare waste incinerators are included in Annex 3.
According to a group known as Health Care without Harm Coalition, "Only about 10-15% of hospital waste is infectious waste; the rest is made up of paper, plastics, food,metal, glass, wood, and other materials. Only about 2% of total hospital waste (thepathological waste-body parts and body fluids) needs to be incinerated to protect publichealth, according to the U. S. Centers for Disease Control. Yet some hospitals routinelyincinerate 75-100% of their waste, a needlessly expensive way to dispose of waste. TheHealth Care without Harm Coalition recognizes the Centers for Disease Control's
9 Source: Safe Management of Wastes from Health Care Activities, WHO, 199910 Source: Safe Management of Wastes from Health Care Activities, WHO, 1999.
6

recommendation of incineration for the treatment of pathological waste (body parts andbody fluids) but opposes its use for the other 98% of the medical waste stream.'"
Combustion Control
In an analysis of 169 municipal waste combustors conducted by ASME, 80 percentshowed no statistically significant relationship between vinyl input and dioxin output,even when waste combustors were "spiked" with chlorine-based plastics, such as vinyl.ASME found that facility design and operation -- not waste content control -- are the best
12ways to limit dioxin emissions from waste combustors' . Further, upon review of anumber of studies regarding the relationship between the chlorine content of waste anddioxin emissions, the EPA concluded in its Medical Waste Incinerator Rule: "At thispoint, the effectiveness of a pollution prevention program directed at reducingdioxin/furan emissions through shifting the waste composition from chlorinate plastics tononchlorinated polymers would be questionable. 13"
According to a letter to the New England Journal of Medicine from two University ofNorth Carolina research scientists, no known human health effects have resulted fromincinerator-generated dioxin. More importantly, while the dioxin compound 2,3,7,8-TCDD has been linked to health effects in laboratory animals, medical waste incinerationis not a significant source of this compound. In fact, according to a 1995 study conductedby the American Society of Mechanical Engineers (ASME), 2,3,7,8-TCDD makes up lessthan one-half percent of total MWI dioxin emissions.
Single-Chamber Incinerator
If a pyrolytic incinerator cannot be afforded, health-care waste may be incinerated in astatic-grate, single-chamber incinerator. This type of incinerator treats waste in batches;loading and de-ashing operations are performed manually. The combustion is initiatedby addition of fuel and should then continue unaided. Air inflow is usually based onnatural ventilation from the oven mouth to the chimney; if this is inadequate, however, itmay be assisted by mechanical ventilation. Regular removal of soot and slag is
14essential
"1 Rochester Committee for Scientific Information, Bulletin #324, October 1999, Medical Waste Disposal,by Joanne Mitchell
12 American Society of Mechanical Engineers, "The relationship between chlorine in the waste streams anddioxin emissions from waste combustor stacks " CRTD Vol. 36, 1995.
13 U.S. Federal Register, Volume 61, No. 120, June 20, 1996.
U.S. Federal Register, Volume 62, pg 48347, September 15, 1997.
14 ibid.
7

On-Site Treatment of Wastewater
Many hospitals, in particular those that are not connected to any municipal treatmentplant, have their own sewage treatment plants. Efficient "package" treatment plants,approximately the size of a shipping container, are available from a variety of vendors.These containerized units can be set into operation with a minimum of cost and sitepreparation. The unit chosen should provide at a minimum secondary treatment withdisinfection of effluent.
Efficient on-site treatment of hospital sewage should include the following operations:
* Primary treatment
* Secondary biological purification. Most helminths will settle in the sludgeresulting from secondary purnfication, together with 90-95% of bacteria and asignificant percentage of viruses; the secondary effluent will thus be almost freeof helminths, but will still include infective concentrations of bacteria and viruses.
* Tertiary treatment. The secondary effluent will probably contain at least 20mg/litre suspended organic matter, which is too high for efficient chlorinedisinfection. It should therefore be subjected to a tertiary treatment, such aslagooning; if no space is available for creating a lagoon, rapid sand filtration maybe substituted to produce a tertiary effluent with a much reduced content ofsuspended organic matter (<10mg/litre).
* Chlorine disinfection. To achieve pathogen concentrations comparable to thosefound in natural waters, the tertiary effluent will be subjected to chlorinedisinfection to the breakpoint. This may be done with chlonne dioxide (which isthe most efficient), sodium hypochlorite, or chlorine gas. Another option isultraviolet light disinfection. Disinfection of the effluents is particularlyimportant if they are discharged into coastal waters close to shellfish habitats,especially if local people are in the habit of eating raw shellfish15 .
Sewage Sludge Treatment
The sludge from the sewage treatment plant requires anaerobic digestion to ensurethermal elimination of most pathogens. Alternatively, it may be dried in natural dryingbeds and then incinerated together with solid infectious health-care waste. On-sitetreatment of hospital sewage will produce a sludge that contains high concentrations of
1 6helminths and other pathogens
15 Source: Safe Management of Wastes from Health Care Activities, WHO, 1999.16 ibid.
8

Reuse of Wastewater and Sludge in Agriculture and Aquaculture
According to the relevant WHO guidelines (Mara & Cairncross, 1989), the treatedwastewater should contain no more than one helminth egg per litre and no more than1000 faecal coliforms per 100 ml if it is to be used for unrestricted irrigation. It isessential that the treated sludge contains no more than one helminth egg per kilogram andno more than 1000 faecal coliforms per 100 g. The sludge should be applied to fields intrenches and then covered with soill .
'7 ibid.
9

Chapter 5
Options for Treatment and Disposal of Health Care Waste inTonga
Choice of Health Care Waste Treatment Technologies
Vaiola Hospital generates the following types of health care wastes that must be treatedand disposed:
* Infectious waste* Anatomical waste* Sharps* Pharmaceutical waste* Chemical waste
In the future radioactive waste and cytotoxic waste may be generated at the facility.
Disposal options should be chosen on the basis of:
* suitability of treatment technology to the particular type of health care waste (seetable below);
* acceptable impacts to human health and the environment;* availability of the technology and maintenance services in Tonga;* capital cost, maintenance and training required for each treatment and disposal
technology, and overall cost effectiveness.
An overview of disposal or treatment methods for different categories of health carewastes is presented in Table 1. Among these options, both autoclaving and incinerationrequire exact and precise operation and maintenance. The operators of these machinesmust be trained continuously. The equipment must be maintained and repairs must bemade as required.
Autoclaving is used by medical waste generators to disinfect waste and remove thepotential hazard to waste handlers. This is a primary treatment and is usually followed bysecondary treatment including landfilling, shredding and incineration. Steam sterilizersshould be equipped to continuously monitor and record temperature and pressure duringthe entire length of each cycle.
When doctors operate, anatomical waste (body parts) could end up in the waste stream.Anatomical wastes require special attention. The U.S. EPA does not allow for thedischarge of anatomical waste to landfills due to aesthetic reasons. Therefore, anatomicalwaste is incinerated or steam sterilized following shredding or grinding.
1

Systems that pre-shred before treatment risk contaminating the equipment and theatmosphere, increasing risk to the operators, maintenance and waste management staff.Shredders have high capital and maintenance costs, and are not currently recommendedfor use in developing countries by WHO.
Only pyrolytic incineration is considered by WHO as a suitable treatment option for allthe waste types currently generated by MOH facilities. The incinerator ash can bedisposed in a landfill. However, use of incineration, with its inherent costs, can beminimized if the various wastes are segregated, and given treatment and disposal asappropriate for those wastes, such as autoclaving and landfilling as detailed in thefollowing table.
The hazardous health care waste disposal problem could be rectified by use of acombination of treatment and disposal technologies. These include the existingincineration facilities (operated by the Ministry of Agriculture and Forestry, Quarantineand Quality Management Division), the hospital wet thermal treatment system(autoclave), as well as two planned sanitary landfill facilities. The MOH should plan tomake use of the most cost-effective suitable waste treatment technology, or combinationof technologies, when they develop their Health Care Waste Management Plan.
Cost of Treatment and Disposal Options
Several treatment options were considered and the annual cost of these options werereviewed to see what would be the most viable option for Tonga. These costcomparisons are shown in the Table 2 below. As is shown, a combination of treatmentoptions which include using the existing the existing incineration facilities (operated bythe Ministry of Agriculture and Forestry, Quarantine and Quality ManagementDivision), the hospital wet thermal treatment system (autoclave), as well as two plannedsanitary landfill facilities would have the lowest cost even considering the different feerates for using the incinerator.
2

Table 1: Overview of Disposal or Treatment Methods Suitable for Different Categories of Health Care Wastes*
Technology or Infectious Anatomical Sharps Pharmaceutical Cytotoxic Chemical Radioactivemethod waste waste waste Waste waste waste
Incinerator yes yes yes yes no yes Low levelinfectious waste
Chemical yes no yes no no no nodisinfection __ __
Wet thermal yes no yes no no no no(autoclave)Microwave yes no yes no no no no
Safe burial on yes yes yes Small quantities no Small nohospital grounds quantitiesSanitary landfill yes no no Small quantities no no I_no
Dicharge to no no no Small quantities no no Low levelsewer liquid waste
*from Safe Management of Wastes from Health Care Activities, WHO, 1999

Table 2: Cost Comparison, Treatment Options* (in US$)
Technology Capital Cost Comments 15-year Annual Annual Annual Annual Total AnnualOption annualized Training Maintenance operator cost transport Cost
equipmentcotcosts MOH
personnelcost
Microwave $50,000 Add $50,000 for shredder. $6,666 $3,000 $7,500 $2,500 $10,800 $30,466Steam sterilizer $75,000 Add $100,000 for shredder (vendor $11,666 $3,000 $7,500 $2,500 $10,800 $35,466
does not recommend shredder fordeveloping countries, since repaircost is typically $15,000/visit). _
ChemClave $107,000 Not suitable for anatomic waste. $7,133 $3,000 $7,500 $2,500 $10,800 $30,933Autoclave $45,000 Add $10,000 for waste package, $3,866 $3,000 $7,500 $2,500 $10,800 $27,666
$3,000 install .Incinerator $100,000 fuel tank, pad, install costs $6,666 $3,000 $7,500 $2,500 $10,800 $30,766
included @$40,000 fuel cost/year$300
Use existing transport Incinerator fees are $1,300 Based none Included in Included in Included in $10,800Quarantine vehicle on unsegregated waste @ $ 40/ Quarantine Quarantine Quarantine $12,100incinerator, included in kilo, 9 kilos/day, 360 days. Department Department Departmentexisting annual Quarantine Department charges are fee fee feeautoclaves and transport likely to increase (see below).landfil** cost at leftUse existing included in Incinerator fees are $2,600 Based none Included in Included in Included in $10,800 $13,400Quarantine annual on unsegregated waste @ $.80/ Quarantine Quarantine Quarantineincinerator, transport kilo, 9 kilos/day, 360 days. Department Department Departmentexisting cost at left fee fee feeautoclaves andlandfill**

Use existing included in Incinerator fees are $3,300 Based none Included in Included in Included in $10,800 $14,100Quarantine annual on unsegregated waste @ $1.02/ Quarantine Quarantine Quarantineincinerator, transport kilo, 9 kilos/day, 360 days. Department Department Departmentexisting cost at left fee fee feeautoclaves andlandfill**Use existing included in Incinerator fees are $650- Based none Included in Included in Included in $10,800 $11,450Quarantine annual on segregated waste @ $.40/ kilo, Quarantine Quarantine Quarantineincinerator, transport 4 5 kilos/day, 360 days. Department Department Departmentexisting cost at left Quarantine Department charges are fee fee feeautoclaves and likely to increase (see below).landfill**Use existing included in Incinerator fees are $1,300 Based none Included in Included in Included in $10,800 $12,100Quarantine annual on segregated waste @ $.801 kilo, Quarantine Quarantine Quarantineincinerator, transport 4.5 kilos/day, 360 days. Department Department Departmentexisting cost at left fee fee feeautoclaves andlandfill**Use existing included in Incinerator fees are $1,650 Based none Included in Included in Included in $10,800 $12,450Quarantine annual on segregated waste @ $1.02/ kilo, Quarantine Quarantine Quarantineincinerator, transport 4.5 kilos/day, 360 days. Department Department Departmentexisting cost at left fee fee feeautoclaves andlandfill **
* assumed throughput about 25 lbs/batch, available units nearest required size, U S vendor quotes** costs of operating the autoclaves are already included in the MOH's recurrent budget Waste could be transferred to the landfill using vehicles transfemng waste to incinerator at little additionalcost If a fee is charged for using landfill this could amount to additional costs MOH personnel costs are also covered in the current health care budget The vehicle will be purchased under the project

Preferred Treatment Option
The incineration facility provided by AusAid and operated by the Ministry of Agricultureand Forestry, Quarantine and Quality Management Division18 at the Nuku'olofa wharfhas been used by Vaiola Hospital in the past. According to hospital staff this practice wasdiscontinued because of high cost of disposing all hospital waste (infectious or otherwise)without segregating infectious from general waste, amounting to about 40 kg per daycompared to 9 kg or less of infectious waste. As discussed above, costs of this optioncould be minimized by segregation of wastes, and/or use of other treatment and disposaloptions. The Quarantine incineration unit has been in operation since 1993, and isroutinely used to decontaminate waste from cruise ships, yachts and aircraft.
The Quarantine incinerator is a large two-chamber unit that is operated at 8000C,although the unit is reported to be capable of operation at 1200°C. This is the twochambered pyrolytic incineration technology WHO finds acceptable because airemissions are minimized by the burn temperature, residence time, and the secondarycombustion chamber. This incinerator, if operated properly, should meet the WHO andEPA guidelines for existing small units. It should be born in mind that the estimatedvolume of infectious waste generated by the Vaiola Hospital is on the order of 18 pounds(9 kilograms) per day.
The Quarantine incinerator was not operational at the time of the October 2002 visit,because the burners required replacements. New burners from New Zealand for theincinerator have been obtained and the unit is again operational.
Fleming Electrics, of Tonga, provides the Quarantine and Quality Management Divisionwith maintenance and training services for the incinerator.
Hygiene in the incinerator building is in need of improvement, especially if the facilitywere to be used for infectious health care waste disposal.
In order to minimize cost of treatment, the wastes could be segregated, in order to reducevolume. Different waste types could be given appropriate treatment with cost or otherconsiderations in mind. The Ministry of Health can use a combination of treatmentoptions suitable to each waste type. For example:
the volume of waste requiring treatment as infectious or hazardous would be greatlyreduced if the wastes were segregated at the points of generation, through disposal indesignated containers. This would lessen the cost of treatment, for instance cost ofincineration, which is charged by Quarantine Division by weight;
1 An aid program administered by the Secretariat of the Pacific Community will supply the Quarantine andQuality Management Division with an additional two small incineration units intended for use on theislands of 'Eua and Ha'apai. The one cubic-meter units are manufactured of stainless steel in Australia andoperate at 600°C. The Ministry of Health hospitals on these two islands could make use of these facilitiesfor disposal of segregated infectious waste
1

• the existing hospital autoclave could be used for treatment of infectious waste andsharps. These wastes would then be disposed in a proper landfill facility, minimizingwastes disposed by incineration and saving cost of incineration. The autoclave (wetthermal treatment) is not suitable for the other types of wastes listed above'9 ;
• proper landfilling could be used for some of the segregated wastes, either on site orat the new engineered landfill to be built. Landfilling is not suitable for anatomicalwaste (except on the hospital premises), sharps, cytotoxic waste, chemical orradioactive waste.2 0
There is a treatment/disposal vendor available, that is the Quarantine Department'sincinerator facility at the wharf, located a short distance from the hospital. TheQuarantine and Quality Management Division has already made the investment in thisunit, and has personnel trained in its operation and maintenance. Private maintenance andtraining services are locally available, and used by the Quarantine Division.
The 40 cents per kilo charged for use of the incinerator has not proved adequate to payfor operation and maintenance costs. The Ministry of Agriculture and Forestry plans toincrease the usage fees. The impact of various options of fee increase and transportoptions (MOH staff or private contractor) on the costs of using the Quarantine incineratorare shown in the Table 3.
Private Contractor Cost Versus MOH Personnel for Health Care Waste Transport
A comparison of the recurrent costs for use of the Quarantine incinerator, with MOHpersonnel and vehicle for transport, versus a private waste disposal firm is difficult toascertain. There are at most two small private clinics that could be potential customersfor a specialized health care waste transport service, besides the Viaola Hospital. Aprivate contractor would have the same health care waste transport vehicle capital andmaintenance costs, plus administrative costs for running the business. Given the limited(hospital and possibly two clinics) clientele, there would not be full-time use of personnelor equipment. Use of a health care waste transport vehicle for other purposes would notbe acceptable. MOH personnel have other duties, and waste collection and transport isincidental to these other duties.
Recurrent costs for the option of using a dedicated MOH vehicle and MOH staff fortransporting health carte waste, with landfilling and use of the Quarantine incinerator forinfectious waste are shown in the table below.
t9 Chapter 9, Safe Management of Wastes from Health Care Activities, WHO, 1999.20 Chapter 9, Safe Management of Wastes from Health Care Activities, WHO, 1999
2

Table 3: Capital and Recurrent Waste Transport/Disposal Costs (in $US)
MOH transport Contractor transportCapital cost, vehicle $20,000 $20,00010-year depreciationPersonnel MOH personnel are already Loaded rates, including profit,
assigned to collect and 4 hours/daytransport health care waste
Driver/collector 4hrs/day $1,500 $2,000Administrator 4hrs/day $1,700 $3,500Vehicle maintenance $5,000/year $5,000/yearVehicle fuel, oil, disinfectant $600/year $600/yearAnnual Cost $10,800 $13,100Landfill charges unknown UnkownIncinerator use at $.40/kilo, all $1,300/year based on 9 $1,300infectious waste, no segregation of kilos/day x 360 daysanatomic wasteIncinerator use at $ 80/kilo, all $2,600/year $2,600infectious wasteIncinerator use at $1.02/kilo, all $3,300/year $3,300infectious wasteTotal Annual Cost, all infectious $14,100 $16,400waste (9kilos/day @$1.02/kiloincineration charge)Total annual cost, segregated $12,450 $14,750anatomnic waste only(4.5 kilos/day @ $1.02/kiloincineration charge)Note cost of off-site incineration in the U S vanes from $ 32 -$1 02 (vendor data)
Reduction of cost to the hospital could be achieved if infectious wastes were segregatedfrom the general domestic health care waste, reducing the volume and weight ofinfectious waste. A further reduction of cost for the hospital would be to segregateanatomical waste for incineration, and use the autoclave for treatment of other infectiouswaste, with subsequent disposal in the sanitary landfill when it becomes available (seebelow). This combination of options is the most cost-effective means of safely disposingof infectious health care waste. Incineration is the only acceptable (WHO) means oftreating anatomical waste that is reasonably available in Tonga (see Table 2).
A memorandum of understanding between the Ministry of Health and the Quarantine andQuality Management Division of the Ministry of Agriculture and Forestry will bedeveloped by Year 2 of the project to clearly define the roles and responsibilities of thetwo Ministries in health care waste disposal and to document the agreements between thetwo parties in terms of costs of disposal etc.. A joint monitoring plan will be part of thisMOU. The MOU will be implemented in the last three years of the project.
Sanitary Landrill Development Programs
Sanitary landfill development projects are planned on the Islands of Tongatapu andVava'u. Aus AID is prepared with a schedule for implementation of a sanitary landfill
3

project for Tongatapu. The landfill will be developed in stages, and will have provisionsfor waste segregation and recycling.
The EU aid organization is preparing a sanitary landfill project for the island of Vava'u.The project is ready for implementation. A site has been selected, groundwatermonitoring wells have been installed, and the landfill has been designed. The projectcannot progress any further until the Government of Tonga purchases the land from aprivate owner, and there is some dispute over price. An alternative site may have to beselected. Once the site is finalized, a construction contract could be tendered in a month.If another site is selected, a detailed design for the new site will have to be made, andconstruction could start within three months of land purchase. Construction time isestimated at six to eight months.
The plans include access road improvements and purchase of a front-end loader/tractorfor covering the waste lifts. The landfill will include an asphalt liner, as this is animpervious material that is locally available. The plan includes a leachate collectionsystem, a collection/evaporation pond, and spray of leachate onto the top of the fill.
Use of these new facilities for disposal of health care wastes (after appropriate treatment)would reduce the human health and environmental hazards and potential damage fromthe current practice of inappropriate disposal in open dumps. The open dumps willremain as hazards to human health and the environment until they are adequatelyremediated and reclaimed.
4

Chapter 6
Recommendations
* A Health Care Waste Management Policy should be developed by the Ministryof Health. This would include a legal package (see below). An acceleratedprogram of development and implementation should be undertaken under thetechnical assistance during project implementation (see section on Health CareWaste Management Policy below).
* A complete Health Care Waste Management Plan, to include all Ministry ofHealth and private health care operations in Tonga should be developed (seedetails below). The plan should be developed in conjunction with any otherministry involved in health care waste management such as Ministry ofAgriculture, Quarantine Service, and the Department of Environment. Anaccelerated program of development and implementation should be undertakenunder the technical assistance during project implementation (see section onHealth Care Waste Management Plan below)..
* The Ministry of Health should have a dedicated budget for health care wastemanagement to include staff training, equipment capital and operations andmaintenance costs, and other recurrent costs.
* Section 3 of the Vaiola Hospital Infection Control Manual, under Blood and BodySubstance Precautions, specifies personnel protective equipment and proceduresfor spills of blood and body fluids. This section should be expanded to include allMinistry of Health health care waste handlers (including transporters), as well astransportation spills. The precautions should be implemented without delay. Thepractice of bending infectious sharps prior to disinfection should be discontinued(Prnce Ngu Hospital).
* Proper disposal of segregated infectious health care waste should be implementedwithout delay, and proper disposal practices implemented using available options,such as: autoclave, landfill and existing incineration facilities maintained by theMinistry of Agriculture and Forestry, Quarantine and Quality ManagementDivision.
* A modem sanitary wastewater treatment systems should be installed at Vaiolahospital. The MOH should evaluate use of disinfected effluent for irrigation, andsanitary composting of sludge for use as soil amendment (see Annex 6 forspecifications).
A plan including activities, monitoring and evaluation indicators and the timeline forimplementing these recommendations under the project is in Table 4.
5

Table 4: Proposed Implementation Plan
Outputs Activities Monitoring and evaluation Implementation Periodindicators
Improved capacity of the Ministry of Develop a National Health Care Waste Management Policy olicy Approval by Ministry of Health Year IHealth to plan for management of and legislative package Management structure approved byhealth care waste in an environmentally Ministry of Healthsustainable manner
Improved capacity of the Ministry of Develop a National Health Care Waste Management Plan Plan approval by Ministry of Health (all Year I - 3Health to manage health care waste in pecific to each health care facility outlining procedures and facilities)an environmentally sustainable manner guidelines, waste definition and charactenzation, segregation
echniques, containment and storage practices, collection and pproved budgets for implementation ofransport, treatment and disposal, and emergency procedures ealth Care Waste Management Plansn case of contamination and spills
eveloped MOUIxecuted MOU
Develop a Memorandum of Understanding between MOH Year 2ad Quarantine Department for use of incinerator on a fee Year 3-5
ass_______________________ asis

Outputs Activities Monitoring and evaluation Implementation Periodindicators
Expenditures to enable the Ministry of I Procure appropnate waste containers I Containers procured and in use Year 2Health to manage health care waste inan environmentally sustainable manner
2 vehicle in use and decontaminated. obtain appropnate dedicated vehicle for HCW transport daily
3. Vendors qualified and selectedRequest WWT vendor proposals
elect treatment equipment for Wastewater WT plant contracted
Procure wastewater treatment plant, Vaiola Hospital Civil works and hardware in place
Installation completed
WWT plant operations monitonngshows operation within agreed limits
Train WWT plant operator(s)mprovement in personnel skills and Train health personnel in disposal of clinical waste Training approved and completed Year 2 - 3
zxpenence in managing health carewaste

Development of the Health Care Waste Management Policy
1. Essential elements of a National Health Care Waste Management Policy:
The following are the key elements of national health care waste management policy21.
Comprehensive System
* Assignment of responsibilities for waste management* Allocation of sufficient resources* Waste minimization, including purchasing policies and stock management practices* Segregation of waste into sharps, non-sharps infectious waste and non-infectious waste* Implementation of safe handling, storage, transportation, treatment and disposal options* Tracking of waste production and waste destination
Awareness and Training
* Awareness raising of all staff about risks related to sharps and other infectious wastes* Training of health-care personnel regarding segregation practices* Training of waste workers regarding safe handling, storage and operation and maintenance
of treatment technologies
* Display of written instructions for personnel
Selection of Options
* Identification of available centralized waste management and disposal resources* Choice of sustainable management and disposal options, according to:
- Affordability- Environment-friendliness- Efficiency- Worker's safety- Prevention of the re-use of disposable medical equipment (e.g. syringes)
- Social acceptability
Legal, Regulatory and Policy Aspects
National legislation is the basis for improving health-care waste practices in any country. Itestablishes legal controls and permits the national agency responsible for the disposal of health-care waste, usually the ministry of health, to apply pressure for their implementation. Theministry of environment or national environmental protection agency may also be involved; thereshould be a clear designation of responsibilities
22before the law is enacted
21 Source: WHO, Decision-Making Guide for Management of Health Care Wastes
3

International Agreements and Underlying Legislative and Regulatory Principles
International agreement has been reached on a number of underlying principles that governeither public health or safe management of hazardous waste. These principles-outlined below-should be taken into consideration when national legislation or regulations governing healthcarewaste management are formulated:
The Basel Conventioni
The Basel Convention, signed by more than 100 countries, concerns transboundary movementsof hazardous waste; it is also applicable to health-care waste. Countries that signed theConvention accepted the principle that the only legitimate transboundary shipments of hazardouswaste are exports from countries that lack the facilities orexpertise to dispose safely of certain wastes to other countries that have both facilities andexpertise. Exported waste should be labelled according to the UN recommended standards.
"Polluter Pays" Principle
The "polluter pays" pnnciple implies that all producers of waste are legally and financiallyresponsible for the safe and environmentally sound disposal of the waste they produce. Thisprinciple also attempts to assign liability to the party that causes damage.
"Precauctionary" Principle
The "precautionary" principle is a key principle governing health and safety protection. Whenthe magnitude of a particular risk is uncertain, it should be assumed that this risk is significant,and measures to protect health and safety should be designed accordingly.
"Duty of Care" Principle
The "duty of care" principle stipulates that any person handling or managing hazardoussubstances or related equipment is ethically responsible for using the utmost care in that task.
"Proximity" Principle
The "proximity" principle recommends that treatment and disposal of hazardous waste take placeat the closest possible location to its source in order to minimize the risks involved in itstransport. According to a similar principle, any community should recycle or dispose of thewaste it produces, inside its own territorial limits.
Legal Package
The law should be complemented by a policy document, and by technical guidelines developedfor implementation of the law. This legal "package" should specify regulations on treatment fordifferent waste categories, segregation, collection, storage, handling, disposal, and transport ofwaste, responsibilities, and training requirements; it should take into account the resources andfacilities available in the country concerned and any cultural aspects of waste-handling. A
22 Legal section source: Safe Management of Wastes from Health Care Activities, WHO, 1999.4

national law on health-care waste management may stand alone or may be part of morecomprehensive legislation such as the following:
* law on management of hazardous wastes: application to health-care waste should beexplicitly stated;
* law on hospital hygiene and infection control: a specific chapter or article should bedevoted to health-care waste.
The law should include the following:
* a clear definition of hazardous health-care waste and of its various categories;* a precise indication of the legal obligations of the health-care waste producer regarding
safe handling and disposal;* specifications for record-keeping and reporting;* specifications for an inspection system to ensure enforcement of the law, and for
penalties to be imposed for contravention;* designation of courts responsible for handling disputes arising from enforcement of or
noncompliance with the law.
In addition, hospitals should be run, and health-care waste disposed of, in accordance with allother relevant national legislation, such as regulations pertaining to:
* waste in general;* effects on public health and the environment;* air quality;* prevention and control of infectious disease;* management of radioactive materials.
2. Policy Document and Technical Guidelines
The policy document should outline the rationale for the legislation, plus national goals and thekey steps essential to the achievement of these goals. It may contain the following:
* descriptions of the health and safety risks resulting from mismanagement of health-carewaste;
* reasons for sound and safe health-care waste management practices in health-careestablishments;
* listing of approved methods of treatment and disposal for each waste category;* warning against unsafe practices, such as disposing of hazardous health-care waste in
municipal landfills;* management responsibilities within and outside health-care establishments;* assessment of the costs of health-care waste management.* key steps of health-care waste management: minimization, separation, identification,
handling, treatment, and final disposal of waste; technical specifications for theimplementation of each step should be described in separate technical guidelines;
* record-keeping and documentation;* training requirements;* rules governing the protection of workers' health and safety.
5

The technical guidelines associated with the legislation should be practical and directlyapplicable. They should include the following specifications, with sufficient detail to ensure thatsafe practices are observed and appropriate standards achieved:
* legal framework covering safe management of health-care waste, hospital hygiene, andoccupational health and safety (limits of emission of atmospheric pollutants and measuresfor protection of water resources may be addressed here or in the other nationalguidelines);
* the responsibilities of public health authorities, of the national environmental protectionbody, of the heads of health-care establishments, of the scattered and smaller producersof health-care waste; and of the heads of any private or public waste-disposal agenciesinvolved;
* safe practices for waste minimization;* separation, handling, storage, and transport of health-care waste;* recommended treatment and disposal methods for each category of health-care waste and
for wastewater.
For ease of application, the definitions of health-care waste categories included in the law shouldbe repeated in the technical guidelines. Gradual implementation of the law is recommended inpreference to any attempt to introduce all measures simultaneously, particularly where existingpractices are inadequate.
Development of a Health Care Waste Management Plan
The following is a generalized Health Care Waste Management Plan23 . The Waste ManagementPlan shall be drafted by the Waste Management Office for approval by the Waste ManagementTeam, and shall be based on internationally recognized environment management standards suchas the ISO 14000 series.
The Waste Management Plan should include:
(a) a plan of the hospital showing the waste disposal points for every ward and department,indicating whether each point is for hazardous waste or non-hazardous waste, andshowing the sites of the central storage facility for hazardous waste and the centralstorage facility for non-hazardous waste;
(b) details of the types, numbers and estimated costs of containers, plastic bags and trolleysrequired annually;
(c) time-tables including frequency of waste collection from each ward and department;(d) duties and responsibilities for each of the different categories of hospital staff members
who will generate health care waste and be involved in the management of the waste;(e) an estimate of the number of staff members required for waste collection;(e) procedures for the management of wastes requiring special treatment such as autoclaving
before final disposal;
23 Sources: Safe Management of Wastes from Health Care Activities, WHO, 1999; and Hospital WasteManagement Rules 2000, Draft, Hospital Waste Management Committee, Pakistan Environmental ProtectionCouncil
6

(f) contingency plans for storage or disposal of hazardous waste in the event of breakdownof incinerator, or of maintenance or collection arrangements;
(g) training courses and programs; and(h) emergency procedures.
The representatives of the Ministry of Health responsible for the collection and disposal of wastefrom the hospital and the Ministry of Agriculture, Quarantine Service and the Department ofEnvironment shall be consulted in drafting and finalization of the Waste Management Plan.
The Waste Management Plan shall be regularly monitored, reviewed, revised and updated by theWaste Management Team as and when necessary.
Management Structure
Within the current management structure of the Ministry of Health, at the hospital level healthcare waste management will be the responsibility of:
* Medical Superintendent* Chief Health Inspector* Chief Medical Officer
A new position of Waste Management Officer will be initiated.
At the Health Facility level the Public Health Nurse and the Health Officer will be responsiblefor health care waste management.
During the technical assistance for waste management planning, responsibilities will be assignedto the above personnel. The following section outlines the typical duties for health care wastemanagement, using general staff titles.
Management Responsibilities
The head of the hospital should form a waste management team to develop a waste managementplan. The team should have the following members:
* Head of Hospital (as chairperson)* Heads of Hospital Departments* Infection Control Officer* Chief Pharmacist* Radiation Officer* Matron (or Senior Nursing Officer)* Hospital Manager* Hospital Engineer* Financial Controller* Waste Management Officer (if already designated).
Head of Hospital
The Head of Hospital is responsible for the following tasks:
7

* Forming a waste management team to develop a written waste management plan for thehospital. The plan should clearly define the duties and responsibilities of all members ofstaff, both clinical and non-clinical, in respect of the handling of health-care waste, andestablish lines of accountability.
* Designating a Waste Management Officer (WMO) to supervise and coordinate the wastemanagement plan. The Head of Hospital retains overall responsibility for ensuring thathealth-care and other wastes are disposed of in accordance with national guidelines.
* Keeping the management plan up to date.* Allocating sufficient financial and personnel resources to ensure efficient operation of the
plan. For example, sufficient staff should be assigned to the Waste Management Officerto ensure efficient operation of the waste management plan.
* Ensuring that monitoring procedures are incorporated in the plan. The efficiency andeffectiveness of the disposal system should be monitored so that the system can beupdated and improved when necessary.
* Immediately appointing a successor in the event of personnel leaving key positions in thewaste management team (or temporarily assigning responsibility to another staff memberuntil a successor can be appointed).
* Ensuring adequate training for key staff members and designating the staff responsiblefor coordinating and implementing training courses.
Waste Management Officer (WMO)
The WMO is responsible for the day-to-day operation and monitoring of the waste managementsystem. It is therefore essential that he or she has direct access to all members of the hospitalstaff. The WMO is directly responsible to the Head of Hospital. He or she should liaise with theInfection Control Officer, the Chief Pharmacist, and theRadiation Officer in order to become familiar with the correct procedures for handling anddisposing of pathological, pharmaceutical, chemical, and radioactive wastes.
In the area of waste collection, the WMO should:
* control internal collection of waste containers and their transport to the central wastestorage facility of the hospital on a daily basis;
* liaise with the Supplies Department to ensure that an appropriate range of bags andcontainers for health-care waste, protective clothing, and collection trolleys are availableat all times;
* ensure that hospital attendants and ancillary staff immediately replace used bags andcontainers with the correct new bags or containers;
* directly supervise hospital attendants and ancillary workers assigned to collect andtransport health-care waste.
Concerning waste storage, the WMO should:
* ensure the correct use of the central storage facility for health-care waste, which shouldbe kept locked but should always be accessible to authorized hospital staff;
* prevent all unsupervised dumping of waste containers on the hospital grounds.
To supervise collection and disposal of the waste, the WMO should:
8

* coordinate and monitor all waste disposal operations;* monitor methods of transportation of wastes both on- and off-site and ensure that wastes
collected from the hospital are transported by an appropriate vehicle to the designatedtreatment and disposal site;
* ensure that waste is not stored for longer than specified in the guidelines and that thetransport organization (which may be the local authority or a private contractor) collectsthe waste with the required frequency.
For staff training and information, the WMO should:
* liaise with the Matron (or Senior Nursing Officer) and the Hospital Manager to ensurethat the nursing staff and medical assistants are aware of their own responsibilities forsegregation and storage of waste and that the responsibilities of hospital attendants andancillary staff are limited to the handling and transport of sealed waste bags andcontainers;
* liaise with Department Heads to ensure that all doctors and other qualified clinical staffare aware of their own responsibilities regarding segregation and storage of waste andthat the responsibilities of hospital attendants and ancillary staff are limited to thehandling and transport of sealed bags and containers;
* ensure that hospital attendants and ancillary staff are not involved in waste segregationand that they handle only waste bags and containers that have been sealed in the correctmanner.
For incident management and control the WMO should:
* ensure that written emergency procedures are available, that they are in place at all times,and that personnel are aware of the action to be taken in the event of an emergency;
* investigate and review any reported incidents concerning the handling of health-carewaste.
Department Heads
Department Heads are responsible for the segregation, storage, and disposal of waste generatedin their departments. They should:
* ensure that all doctors, nurses, and clinical and non-clinical professional staff in theirdepartments are aware of the segregation and storage procedures and that all personnelcomply with the highest standards;
* continuously liaise with the WMO to monitor working practices for failures or mistakes;* ensure that key staff members in their departments are given training in waste segregation
and disposal procedures;* encourage medical and nursing staff to be vigilant so as to ensure that hospital attendants
and ancillary staff follow correct procedures at all times.
Matron and Hospital Manager
9

The Matron (or Senior Nursing Officer) and the Hospital Manager are responsible for trainingnursing staff, medical assistants, hospital attendants, and ancillary staff in the correct proceduresfor segregation, storage, transport, and disposal of waste. They should therefore:
* liaise with the WMO and the advisers (Infection Control Officer, Chief Pharmacist, andRadiation Officer) to maintain the highest standards;
* participate in staff introduction to, and continuous training in, the handling and disposalof health-care waste;
* liaise with Department Heads to ensure coordination of training activities, other wastemanagement issues specific to particular departments, etc.
Infection Control Officer
The Infection Control Officer should liaise with the WMO on a continuous basis and provideadvice concerning the control of infection and the standards of the waste disposal system. His orher duties are to:
* identify training requirements according to staff grade and occupation;* organize and supervise staff training courses on safe waste management;* liaise with the Department Heads, the Matron, and the Hospital Manager* to coordinate the training. The Infection Control Officer also has overall responsibility
for chemical disinfection, sound management of chemical stores, and chemical waste* minimization.
Chief Pharmacist
The Chief Pharmacist is responsible for the sound management of pharmaceuticalstores and for pharmaceutical waste minimization. His or her duties are to:
* liaise with Department Heads, the WMO, the Matron, and the Hospital Manager, givingadvice, in accordance with the national policy and guidelines, on the appropriateprocedures for pharmaceutical waste disposal;
* coordinate continuous monitoring of procedures for the disposal of pharmaceutical waste;* ensure that personnel involved in pharmaceutical waste handling and disposal receive
adequate training. The Chief Pharmacist also has the special responsibility of ensuring* the safe utilization of genotoxic products and the safe management of genotoxic waste.
Radiation Officer
The duties and responsibilities of the Radiation Officer are the same as those of thePharmaceutical Officer but relate to radioactive waste.
Supply Officer
The Supply Officer should liaise with the WMO to ensure a continuous supply of the itemsrequired for waste management (plastic bags and containers of the right quality, spare parts foron-site health-care waste treatment equipment, etc.). These items should be ordered in good timeto ensure that they are always available, but accumulation of excessive stores should be avoided.
10

The Supply Officer should also investigate the possibility of purchasing environmentally friendlyproducts (e.g. PVC-free plastic items).
Hospital Engineer
The Hospital Engineer is responsible for installing and maintaining waste storage facilities andhandling equipment that comply with the specifications of the national guidelines. She or he isalso accountable for the adequate operation and maintenance of any on-site waste treatmentequipment and is responsible for the staff involved in waste treatment, ensuring that:
* staff receive training in the principles of waste disposal and are aware of theirresponsibilities under the hospital waste management plan;
* staff operating on-site waste treatment facilities are trained in their operation andmaintenance.
Waste Segregation
Hazardous waste shall be separated from non-hazardous waste at the source, that is at the wardbedside, operation theatre, laboratory, or any other room in the hospital where the waste isgenerated, by the doctor, nurse, or other person generating the waste.
All disposal medical equipment and supplies including syringes, needles, plastic bottles, dripsand infusion bags shall be cut or broken and rendered non-reusable at the point of use by theperson using the same, or in case any such used equipment or supplies is found or comes to thepossession of any person, by such person.
All hazardous waste other than sharps, large quantities of pharmaceuticals, or chemicals, wastewith a high content of mercury or cadmium such as broken thermometers or used batteries, orradioactive waste shall be placed in a suitable container made of metal or tough plastic, with apedal type or swing lid, lined with a strong yellow plastic bag. The bags shall be removed whenit is not more than three quarters full and sealed, preferably with self-locking plastic sealing tagsand not by stapling. Each bag shall be labeled, indicating date, point of production/ward/hospital,quantity and description of waste, and prominently displaying the biohazard symbol. The bagremoved should be immediately replaced with a new one of the same type.
Sharps including the cut or broken syringes and needles shall be placed in metal or high-densityplastic containers resistant to penetration and leakage, designed so that items can be dropped inusing one hand, and no item can be removed. The containers shall be colored yellow and marked"DANGER! CONTAMINATED SHARPS". The sharps container shall be closed when threequarters full. If the sharp container is to be incinerated, it shall be placed in the yellow plastic bagwith the other hazardous waste.
Waste Types not Suitable for Incineration
The following waste types are not suitable for incineration, and should be segregated from thehazardous infectious waste types to be incinerated:
* Pressurized gas containers such as aerosol cans.* Large amounts of reactive chemical waste.
11

* Silver salts and photographic or radiographic wastes.* Halogenated plastics such as polyvinyl chloride (PVC).* Waste with high mercury or cadmium content, such as broken thermometers.* Used batteries, and lead-lined wooden panels.* Sealed ampoules or ampoules containing heavy metals.
Large quantities of pharmaceutical waste shall be returned to the suppliers. Small quantities shallbe placed in a yellow plastic bag, preferably after being crushed,where this can be done safely.
Waste with a high content of mercury or cadmium shall not be incinerated, but shall be placed inchemical resistant containers and sent to specialized treatment facilities (such as sanitarylandfill).
Radioactive waste that must be stored to allow decay to background level shall be placed in aplastic bag, in a large yellow container or drum. The container or drum shall be labeled, showingthe radionuclide's activity on a given date, and the period of storage required, and marked'RADIOACTIVE WASTE', with the radiation symbol. Non-infectious radioactive waste that hasdecayed to background level shall be placed in black plastic bags. Infectious radioactive wastethat has decayed to background level shall be placed in yellow plastic bags. High level andrelatively long half-life radionuclides shall be packaged and stored in accordance withinstructions of the original supplier under supervision of the Radiology Officer, and sent back tothe supplier for disposal.
Non-hazardous waste shall be placed in a suitable container lined with a black plastic bag.Adequate numbers of non-hazardous waste containers shall be placed in all areas of the hospitaland notices affixed to encourage visitors to use them.
Waste Collection
Waste shall be collected in accordance with the schedules specified in the WasteManagement Plan.
Sanitary staff and sweepers shall, when handling waste, wear protective clothing at all timesincluding face masks, industrial aprons, leg protectors, industrial boots and disposable or heavyduty gloves, as required.
Sanitary staff and sweepers shall ensure that:
(a) waste is collected at least daily, but more often if necessary;
(b) all bags are labeled before removal, indicating the point of production, ward andhospital, and contents;
(c) bags and containers which are removed are immediately replaced with new ones ofthe same type; and
(d) where a waste bag is removed from a container, the container is properly cleanedbefore a new bag is fitted therein.
12

Waste Storage
A separate central storage facility shall be provided for yellow-bagged waste, with a signprominently displaying the biohazard symbol and clearly stating that the facility stores hazardouswaste.
The designated central storage facility shall:
(a) be located within the hospital premises close to the incinerator, if installed, but awayfrom food storage or food preparation areas;
(b) be large enough to contain all the hazardous waste produced by the hospital, with sparecapacity to cater for collection or incinerator breakdowns;
(b) be easy to clean and disinfect, with an impermeable base, plentiful water supply and gooddrainage, lighting and ventilation;
(d) have adequate cleaning equipment, protective clothing and waste bags and containerslocated nearby; and
(e) be easily accessible to collection vehicles and authorized staff, but totally enclosed andsecure from unauthorized access, and especially inaccessible to animals, insects andbirds.
No materials other than yellow-bagged waste shall be stored in the central storage facility.
No waste shall be stored at the central storage facility for more than 24 hours. Provided that if inan emergency infectious waste is required to be stored for more than 24 hours, it shall berefn gerated.
Containers with radioactive waste shall be stored in a specifically marked area in a lead-shieldedstorage room.
Containers with chemical waste that are to be specialized treatment facilities shall also be storedin a separate room or area.
The central storage facility shall be thoroughly cleaned in accordance with procedures stipulatedin the Waste Management Plan.
Waste Transportation
For on-site transportation, the waste collection trolley shall be free of sharp edges, easy to loadand unload and to clean, and preferably a stable three or four-wheeled design with high sides.The trolley shall not be used for any other purpose. The trolley shall be cleaned regularly, andespecially before any maintenance work is performed on it.
13

The sealed plastic bags shall be carefully loaded by hand onto the trolley, to minimize the risksof punctures or tears.
Yellow-bagged hazardous waste and black-bagged non-hazardous waste shall be collected onseparate trolleys that shall be painted or marked in the corresponding colors.
The collection route shall be the most direct one from the final collection point to the centralstorage facility designated in the Waste Management Plan. The collected waste shall not be lefteven temporarily anywhere other than at the designated central storage facility.
Transportation off-site shall, unless otherwise agreed, be the responsibility of theMinistry of Health, which shall ensure that:
(i) all yellow-bagged waste is collected at least once daily;
(ii) all staff members handling yellow-bagged waste wear protective clothing;
(ii) yellow-bagged waste is transported separately from all other waste;
(iii)vehicles or skips used for the carriage of yellow- bagged waste are not used for anyother purpose, are free of sharp edges, easy to load and unload by hand, easy toclean/disinfect, and fully enclosed, preferably with hinged and lockable shutters orlids, to prevent any spillage in the hospital premises or on the highway duringtransportation;
(iv)all concerned staff members are properly trained in the handling, loading andunloading, transportation and disposal of yellow bagged waste, and are fully aware ofemergency procedures for dealing with accidents and spillage;
(v) all vehicles carry adequate supply of plastic bags, protective clothing, cleaning toolsand disinfectants to clean and disinfect any spillage;
(vi) the transportation of waste is properly documented, and all vehicles carry aconsignment note from the point of collection to the incinerator or landfill or otherfinal disposal facility; and
(vi)all vehicles are cleaned and disinfected after use.
Waste bags may be placed directly into the transportation vehicle, but it is safer to place them infurther containers (e.g. cardboard boxes or wheeled, rigid, lidded plastic or galvanized bins).This has the advantage of reducing the handling of filled waste bags but results in higher disposalcosts. These secondary containers should be placed close to thewaste source.
Any vehicle used to transport health-care waste should fulfil the following design criteria:
* The body of the vehicle should be of a suitable size commensurate with the design of thevehicle, with an internal body height of 2.2 metres.
14

* There should be a bulkhead between the driver's cabin and the vehicle body, which isdesigned to retain the load if the vehicle is involved in a collision.
* There should be a suitable system for securing the load during transport.* Empty plastic bags, suitable protective clothing, cleaning equipment, tools, and
disinfectant, together with special kits for dealing with liquid spills, should be carried in aseparate compartment in the vehicle.
* The internal finish of the vehicle should allow it to be steam-cleaned, and the internalangles should be rounded.
* The vehicle should be marked with the name and address of the waste carrier.* The international hazard sign should be displayed on the vehicle or container, as well as
an emergency telephone number.
Vehicles or containers used for the transportation of health-care waste should not be used for thetransportation of any other material. They should be kept locked at all times, except whenloading and unloading. Articulated or demountable trailers (temperature-controlled if required)are particularly suitable, as they can easily be left at the site of waste production. Other systemsmay be used, such as specially designed large containers or skips; however, open-topped skips orcontainers should never be used for transporting health-care waste.
Where the use of a dedicated vehicle cannot be justified, a bulk container that can be lifted on toa vehicle chassis may be considered. The container may be used for storage at the health-careestablishment and replaced with an empty one when collected. The finish of these bulkcontainers should be smooth and impervious and permit easy cleansing ordisinfection. The same safety measures should apply to the collection of hazardoushealth-care waste from scattered small sources.
Waste Disposal
Depending upon the type and nature of the waste material and the organisms in the waste,hazardous waste should be inactivated or rendered safe before final disposal by a suitablethermal, chemical, irradiation, incineration, filtration or other treatment method, or by acombination of such methods, involving proper validation and monitoring procedures.
Yellow-bagged waste shall be disposed of by burning in an incinerator or by burial ina sanitary land-fill, or by any other method of disposal approved by the Ministry of Health.
Sharps containers which have not been placed in yellow bags for incinerator shall bedisposed of by encapsulation or other method of disposal approved by the Ministry of Health.
The method of disposal, whether by burning in an incinerator or by burial in a landfillor otherwise, shall be operated by a hospital only after approval of its Waste Management Planby the Ministry of Health.
All hazardous waste delivered to an incinerator shall be burned within 24 hours.
Ash and residues from incineration and other methods shall be placed in robust, noncombustiblecontainers and sent to the designated landfill site.
15

Landfills shall be located at sites with minimal risk of pollution of groundwater and rivers.Access to the site shall be restricted to authorized personnel only. Hazardous waste shall beburied in a separate area of the landfill under a layer of earth or non-hazardous waste of at leastone meter depth which shall then be compacted. The landfill shall be regularly monitored by theMinistry of Health to check for groundwater contamination and air pollution. The Ministry ofHealth shall also ensure that the landfill operators are properly trained, especially in safe disposalprocedures, use of protective equipment and hygiene and emergency response procedures.
Daily collection of hazardous waste from hospitals shall be taken by the vehicles of theMinistry of Health (or approved by the Ministry of Health) immediately to the designated landfillsite or incinerator by the most direct route, in accordance with prior scheduling of collectiontimes and journey times.
Radioactive waste which has decayed to background level shall either be buried in the landfillsite or incinerated.
Liquid radioactive waste shall be discharged into the sewerage system only after it has decayedto background level and after it has been ensured that the radioactive materials are soluble anddispersible in water, failing which it shall be filtered.
Accidents and Spillage
In case of accidents or spillage, the following action shall be taken:
(a) the emergency procedures mentioned in the Waste Management Plan shall beimplemented immediately;
(b) the contaminated area shall be immediately evacuated, if required;
(b) the contaminated area shall be cleared and, if necessary, disinfected;
(d) exposure of staff shall be limited to the extent possible during the clean-up operation,and appropriate immunization carried out, as may be required; and
(e) any emergency equipment used shall be disinfected and immediately replaced in thesame location from which it was taken.
All hospital staff members shall be properly trained and prepared for emergency response,including procedures for treatment of injuries, cleanup of the contaminated area and promptreporting of all incidents of accidents, spillage and near-misses.
The Waste Management Officer (as assigned) shall immediately investigate, record and reviewall such incidents to establish causes and where necessary shall amend the WasteManagement Plan to prevent recurrence.
Waste Minimization and Reuse
To minimize health care waste, each hospital shall introduce:
16

(a) purchasing and stock controls, involving careful management of the ordering process toavoid over-stocking, particularly with regard to date-limited pharmaceutical and otherproducts, and to accord preference to products involving low amounts of packaging;
(b) waste recycling programs, involving return of un-used or waste chemicals in quantity tothe supplier for reprocessing, return of pressurized gas cylinders to suppliers for refillingand reuse, sale of materials such as mercury, cadmium, nickel and lead-acid tospecialized recyclers, and transportation of high level radioactive waste to the originalsupplier; and
(c) waste reduction practices in all hospital departments.
To encourage reuse, each hospital shall separately collect, wash and sterilize, either thermally orchemically in accordance with approved procedures, surgical equipmentand other items which are designed for reuse and are resistant to the sterilization process.
Inspections and Enforcement
A Public Health officer may inspect any hospital, incinerator or landfill located within the area ofhis jurisdiction to check for compliance with the provisions of this Plan.
If a Health officer discovers any contravention of any provision of this plan, he or she shallreport to [enforcement actions to be completed by Ministry of Health.]
17

Annex 1
List of Persons Interviewed and Facilities Visited
Mr. Alfred Picardi, Senior Environmental Specialist, visited Tongatapu and Vava'u betweenOctober 24 and October 30, 2002. The principal purpose of the consultancy was to addresshealth care waste management issues with regards to the Vaiola Hospital rehabilitation project.Interviews were held with staff from the Ministry of Health; Ministry of Land Survey andNatural Resources; the Ministry of Works, Environment and Manne, Department ofEnvironment; and the Ministry of Agriculture and Forestry, Quarantine and Quality ManagementDivision. Meetings were also held with Australia AID, JICA and the EU aid organizationrepresentatives.
The consultant visited the Vaiola Hospital facilities, the Quarantine Division port facility andincinerator, and the Tongatapu waste disposal area currently used by the hospital for health carewaste. On the island of Vava'u the consultant visited the Prince Ngu Hospital facilities, as wellas the waste disposal area currently used by the hospital for health care waste.
Persons Interviewed
Persons Interviewed, Nuku'alofa, Ton atapu, October 23 through October 29, 2002Mr. Asipeli Palaki Acting Director of Environment,
Department of EnvironmentMr. Paula Taiufa Terrestrial Conservation Officer,
Department of EnvironmentSione Foliaki Head, Quarantine and Quality Management
Division, Ministry of Agnculture andForestry
Taniela Sunia Soakai Senior Health Planning OfficerSateki Telefoni Supervising Public Health InspectorVili Moale Vaiola Hospital AdministratorSiale Akauola Acting Medical SuperintendentLata Malu Chief Nursing Officer
Persons Interviewed, Vava'l, October 25 thru October 28, 2002Dr. Litili O'Fanoa Tonga Director of HealthNili Fakakovi Public Health InspectorU. T. Vaea Project Manager, EU AID
Prince Ng HospitalDr. Saia Pinkala Acting Chief Medical OfficerDr. Samson Mesol (Surgeon on regular visit from Vaiola
Hospital)Mayumi Ikarashi JOVC NutritionistFrancis Tinani Lab. Technician Grade IIFuji Takeiffa Senior Staff NurseSelu Tonga Hospital Filter Electrician
18

Dr. Susiting Piukala Dental OfficerSho Totia AnesthetistMele Vainikolo Sister In ChargeAtorni Latu Radiographer
19
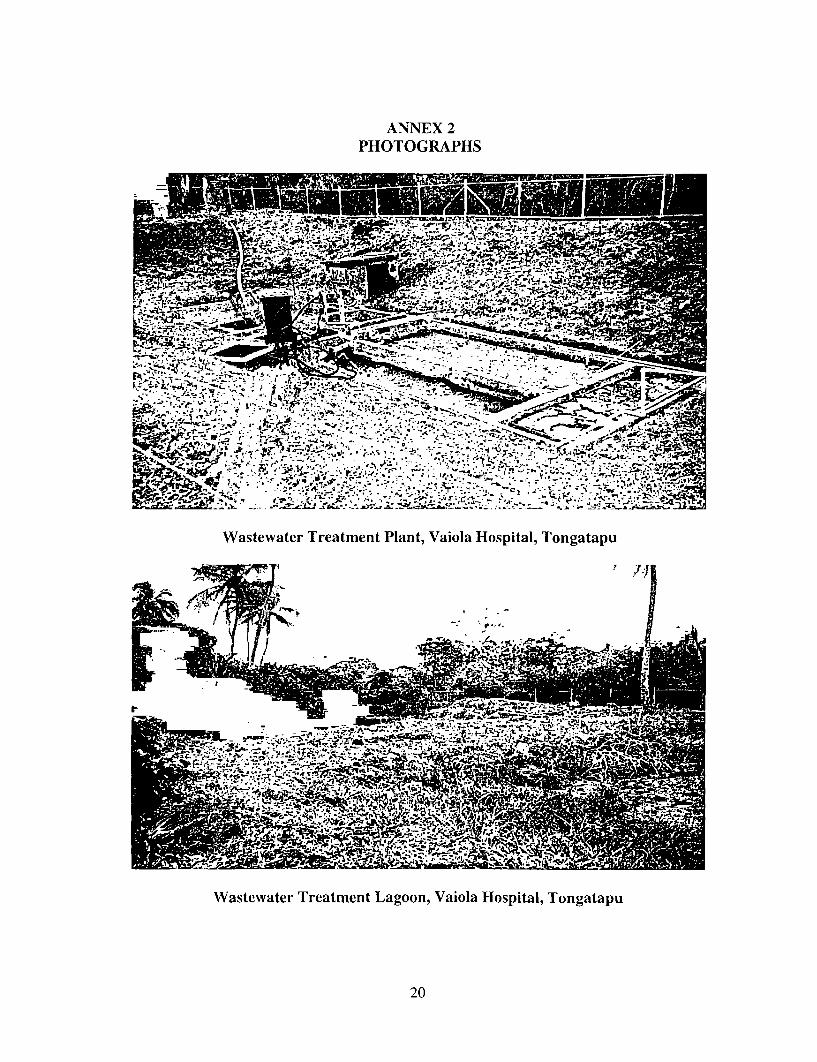
ANNEX 2PHOTOGRAPHS
Wastewater Treatment Plant, Vaiola Hospital, Tongatapu
'~~~~~~~~~:bj ' _,
Wastewater Treatment Lagoon, Vaiola Hospital, Tongatapu
20

- ~ ~ ~ ~ -
Open Dump Where Health care waste is Disposed, Tongatapu - Note Young Scavengers inCenter of Frame
21

* Pr~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~r
SS-'-~~~~t -
Quarantine Incinerator, Port Authority, Tongatapu
22

Health care waste Collection Bag and Central Collection Container, Prince Ngu Hospital,Vava'u
F _ ~~mw
U~~~~~~~~
Health Care Waste Disposal Truck, Prince Ngu Hospital, Vava'u
23

. 1.
'if- -
Open Dump Where Health Care Waste is Disposed from Prince Ngu Hospital, Vava'u -Note Marsh Grasses, Estuary and House Across Water
24
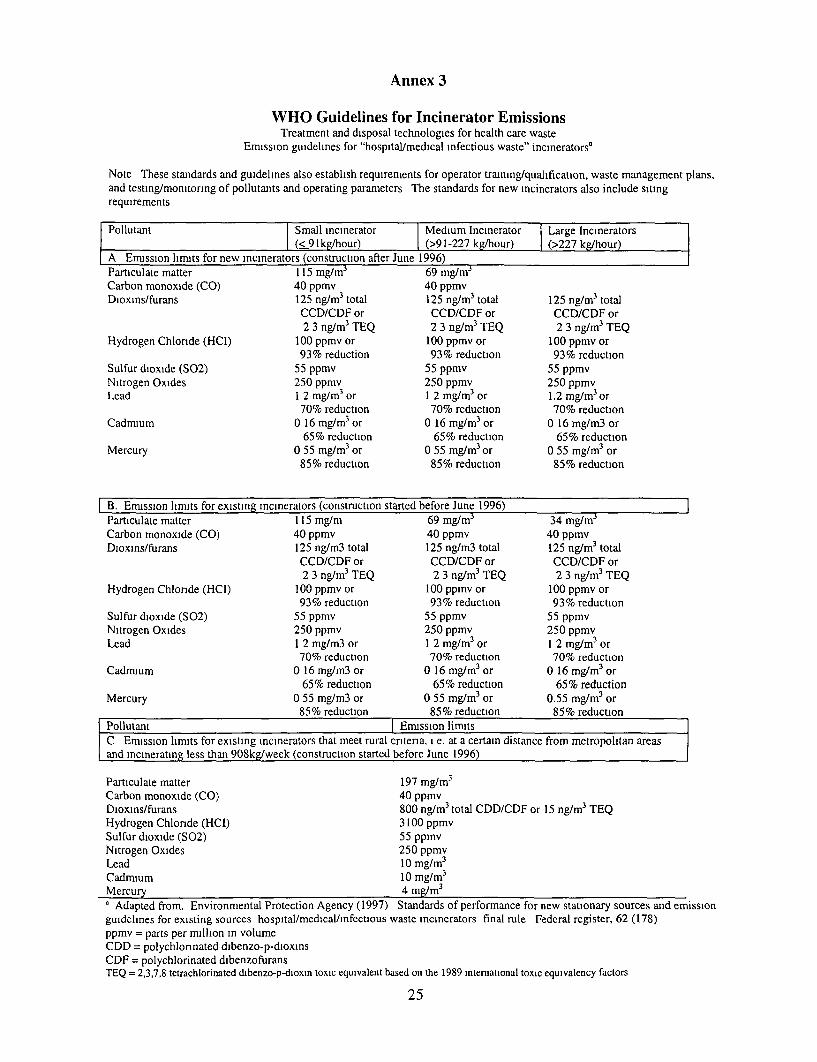
Annex 3
WHO Guidelines for Incinerator EmissionsTreatment and disposal technologies for health care waste
Emission guidelines for "hospital/medical infectious waste" incineratorsa
Note These standards and guidelines also establish requirements for operator training/qualification, waste management plans,and testing/monitonng of pollutants and operating parameters The standards for new incinerators also include sitingrequirements
Pollutant Small incinerator Medium Incinerator [Large IncineratorsI (<91kg/hour) (>91-227 kg/hour) 1 (>227 kg/hour)
A Emission limits for new incinerators (construction after June 1996)Particulate matter 115 mg/m3 69 mg/mrCarbon monoxide (CO) 40 ppmv 40 ppmvDioxins/furans 125 ng/m 3 total 125 ng/m3 total 125 ng/m3 total
CCD/CDF or CCD/CDF or CCD/CDF or2 3 ng/m3 TEQ 2 3 ng/m3 TEQ 2 3 ng/m 3 TEQ
Hydrogen Chlonde (HCI) 100 ppmv or 100 ppmv or 100 ppmv or93% reduction 93% reduction 93% reduction
Sulfur dioxide (S02) 55 ppmv 55 ppmv 55 ppmvNitrogen Oxides 250 ppmv 250 ppmv 250 ppmvLead 1 2 mg/m3 or 1 2 mg/m3 or 1.2 mg/m3 or
70% reduction 70% reduction 70% reductionCadmium 0 16 mg/mr3 or 0 16 mg/m3 or 0 16 mg/m3 or
65% reduction 65% reduction 65% reductionMercury 0 55 mg/m3 or 0 55 mg/m3 or 0 55 mg/m3 or
85% reduction 85% reduction 85% reduction
B. Emussion limuts for existing incinerators (construction started before June 1996)Particulate matter 115 mg/m 69 mg/m3 34 mg/mrCarbon monoxide (CO) 40 ppmv 40 ppmv 40 ppmvDioxins/furans 125 ng/m3 total 125 ng/m3 total 125 ng/m3 total
CCD/CDF or CCD/CDF or CCD/CDF or2 3 ng/m3 TEQ 2 3 ng/m3 TEQ 2 3 ng/m3 TEQ
Hydrogen Chlonde (HCI) 100 ppmv or 100 ppmv or 100 ppmv or93% reduction 93% reduction 93% reduction
Sulfur dioxide (S02) 55 ppmv 55 ppmv 55 ppmvNitrogen Oxides 250 ppmv 250 ppmv 250 ppmvLead 1 2 mg/m3 or 1 2 mg/m3 or 1 2 mg/m 3 or
70% reduction 70% reduction 70% reductionCadmium 0 16 mg/m3 or 0 16 mg/m3 or 0 16 mg/mr3 or
65% reduction 65% reduction 65% reductionMercury 0 55 mg/rn3 or 0 55 mg/m3 or 0.55 mg/mr3 or
85% reduction 85% reduction 85% reductionPollutant Emission limitsC Emission limits for existing incinerators that meet rural critena, i e. at a certain distance from metropolitan areasand incinerating less than 908kg/week (construction started before June 1996)
Particulate matter 197 mg/mr3
Carbon monoxide (CO) 40 ppmvDioxins/furans 800 ng/m3 total CDD/CDF or 15 ng/m3 TEQHydrogen Chlonde (HCI) 3100 ppmvSulfur dioxide (S02) 55 ppmvNitrogen Oxides 250 ppmvLead 10 mg/mr3
Cadmium 10 mg/m3
Mercury 4 mg/m3' Adapted from. Environmental Protection Agency (1997) Standards of performance for new stationary sources and emnissionguidelines for existing sources hospital/medical/infectious waste incinerators final rule Federal register, 62 (178)ppmv = parts per million in volumeCDD = polychlonnated dibenzo-p-dioxinsCDF = polychlorinated dibenzofuransTEQ = 2,3,7,8 tetrachlorinated dibenzo-p-dioxin toxic equivalent based on the 1989 international toxic equivalency factors
25

Annex 4
Consultant Terms of ReferenceFeasibility Study on Health Care Waste Management in Tonga
Background
The World Bank is currently assisting the Govemment of the Kingdom of Tonga in preparing aproject to support the country's health sector reform. The specific objective of the project is to(i) improve the capacity of the Ministry of Health to develop and implement health financingpolicy and collect, manage and use health information, and (ii) improve the functional andtechnical quality of central Hospital (Vaiola Hospital).
A component of the project will support the redevelopment of Vaiola Hospital infrastructure andfacilities, to overcome identified major deficiencies, improve the functional relationships andoverall operational efficiency of the hospital, and enhance the hospital's capacity to efficientlymeet its future service obligations. These developments will be guided by a master plan for thehospital, which is to be prepared during project preparation.
Medical waste will invariably increase, both in quantity and variety. The concern is to ensure theminimum level of adverse human and environmental impacts, if any, from the waste from thehospital.
ObjectiveThe objective of the consultancy is to undertake:
(i) A feasibility study including a legislation study on health care waste management forthe Vaiola Hospital
(ii) An asbestos survey report for Vaiola Hospital
Scope of consultancy
1) A situation analysis on the existing health care waste management in Vaiola Hospital. Thiswill include:
(i) A review of the categories and of health care waste generated (clinical, sharps,pharmaceutical products, cytotoxic and hazardous chemical, radioactive,organic/non-organic domestic, domestic recyclable etc)
(ii) Characterization of health care waste streams and estimation of quantities ofwaste effluence issuing from the hospital
(iii) Waste segregation mechanisms(iv) Identification of risks associated with the current waste management practices(v) Evaluation of existing training and patient/public awareness programs on
healthcare waste management at the hospital.
2) Review and analysis of existing legislative and other regulatory instruments on health carewaste management. This should include an assessment of the opportunities for strengtheningthese regulations.
3) Review any planned donor assistance in health care waste management
26

4) Recommend a process flow for waste minimization, and if necessary, an economic andenvironmentally sound treatment/final disposal of healthcare waste, leading to a choice oftechnology(ies) for Viola Hospital (autoclaving, micro-waving, incineration chemicaldisinfection)
5) Assess the personnel and other training needs. Also outline approaches to consultation withregulations, environmental groups and the public, as necessary.
6) Development of a preliminary implementation plan (including indicators and costs) forhealth care waste management to be included in the Tonga Health Sector Support Project.
7) An asbestos survey of the building will be conducted and the survey report. The surveyreport would confirm or deny the presence of asbestos in the building. If present, then adetailed description of asbestos (in terms of type, location, and quantity) will be preparedincluding a remediation plan along with an implementation schedule and estimation ofabatement costs.
Output
(i) Preliminary design report and draft feasibility study report.(ii) Asbestos survey report including remediation plan, implementation schedule andabatement costs estimation.
27

Annex 5Derinitions
"chemical waste" includes chemicals from diagnostic and experimental work, cleaningprocesses, housekeeping and disinfecting procedures, mercury waste such as from brokenclinical equipment and spillage, and cadmium waste such as from discarded batteries.
"genotoxic waste" includes cytotoxic drugs and outdated materials, vomitus, faeces or urine frompatients treated with cytotoxic drugs or chemicals, and matenals such as syringes and vialscontaminated from the preparation and administration of such drugs.
"hazardous waste" means infectious waste, pathological waste, sharps, pharmaceutical waste,genotoxic waste, chemical waste, and radioactive waste.
"Health Officer" means [Ministry of Health to complete].
"hospital" includes a clinic, laboratory, dispensary, pharmacy, nursing home, health unit,maternity centre, blood bank, research institute and veterinary institution.
"health care waste" includes both hazardous waste and non-hazardous waste.
"Infectious waste" means waste contaminated by any type of pathogens such as bacteria, viruses,parasite or fungi and includes cultures from laboratory work, waste from surgeries and autopsies,waste from infected patients, discarded or disposable materials and equipment which have beenin contact with such patients, and infected animals from laboratories.
"Medical Superintendent" means the Head of the hospital, by whatever designation called
"non-hazardous waste" includes paper and cardboard, packaging, food waste and aerosols andother domestic type waste.
"pathological waste" includes tissue, organs, body parts, foetuses and bloodand body fluids.
"pharmaceutical waste" includes expired or unused pharmaceutical products, spilledcontaminated pharmaceutical products, surplus drugs, vaccines or sera, and discarded items usedin handling pharmnaceuticals such as bottles, boxes, gloves, masks, tubes or vials.
"radioactive waste" includes liquid, solid and gaseous waste contaminated with radionuclidesgenerated from in-vitro analysis of body tissue and fluid, in-vivo body organ imaging andtumour localization, and investigation and therapeutic procedures.
"sharps" include, whether infected or not, needles, syringes, scalpels, infusion sets, saws andknives, blades, broken glass and any other item that could cut or puncture."waste management" includes waste segregation, waste collection, waste transportation, wastestorage, waste disposal and waste minimization and reuse.
28

Annex 6
Vaiola HospitalWastewater Treatment Plant Specifications
Epoxy-coated steel package treatment plant complete with all equipment for operations and start-up. Treatment plant will be appropriate for the Vaiola 200-bed hospital wastewater flows. Thetreatment is to include disinfection prior to discharge.
Five-year spare parts package to be included.
Operator training package with regular maintenance program guidance to be included.
Yearly troubleshooting/operator refresher training to be included.
Guaranteed effluent quality limits (World Bank Guidelines):
Parameter LimitsBOD5 50 mg/lTotal suspended solids (TSS) 50 mg/lOil & Grease 10 mg/lColiform 400 MPN/100mlTotal residual chlorine 0.2 mg/l
29