Embed Size (px)
Citation preview

Postgrad Med J (1993) 69, 927-929 i) The Fellowship of Postgraduate Medicine, 1993
Delayed Diagnosis
Pubic osteomyelitis caused by Staphylococcus simulans
I. Sturgess, F.C. Martin and S. Eykyn'
Elderly Care Unit and 'Microbiology Department, St Thomas' Hospital, Lambeth Palace Road,London SE] 7EH, UK
Summary: A patient is described who developed pubic osteomyelitis caused by an uncommonpathogen, Staphylococcus simulans.
Introduction
Although community-acquired bacteraemic in-fections with coagulase-negative staphylococci arerare, hospital-acquired infections are common andincreasing, particularly with intravenous devices.'We report a case of pubic osteomyelitis caused byStaphylococcus simulans, an unusual species ofcoagulase-negative staphylococcus, affecting anelderly disabled diabetic woman.
Case report
A 77 year old previously active and independentwoman presented in June 1988 with a profoundright hemiparesis and dense dysphasia due to a leftcerebral hemisphere infarction. Serum C-reactiveprotein (CRP) at this time was less than 10 mg/l.She had had non-insulin-dependent diabetes mel-litus for 14 years controlled with diet and tol-butamide, and psoriasis since childhood in virtualremission on admission with no treatment. Re-covery from her stroke was slow and hampered bya painful left hip due to pre-existing osteoarthritis.
In December 1988 she developed a painful rightgroin with tenderness over the right pubic bone.Neither plain X-rays nor isotope bone scan showedany abnormalities in the pelvis and in particular theregion of the pubic bones was normal (Figure la).The diagnosis was unclear but the pain respondedto a right ilio-inguinal nerve block. Later thatmonth further pain in the right groin was diag-nosed as an adductor femoris tear or tendinitis, andresponded to a steroid and local anaesthetic injec-tion at the right adductor tubercle. CRP at this timewas again less than 10 mg/l. In March 1989 localtreatment with a salicylate derivative was initiatedfor a large psoriatic lesion on the scalp which haddeveloped since her admission. This lesion was notcultured and healed rapidly.
A month later deterioration in her functionalability was noted and the CRP was 252 mg/l, thetotal white cell count was 17.5 x 109/l. Dailyphysical examinations, including regular temp-erature measurements, were normal for 6 days, aswere urine microscopy and culture and a chestX-ray. On the seventh day a tender pubic sym-physis was noted and her CRP was 67 mg/l. Aclinical diagnosis of pubic osteomyelitis was made.Two sets of blood cultures grew S. simulans in allbottles, fully sensitive to all anti-staphylococcalantibiotics, and treatment was started with fluclox-acillin, 2 g intravenously 6 hourly for 11 daysfollowed by 500 mg 6 hourly by mouth, and fusidicacid 500 mg orally three times daily.
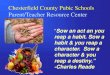
Initially the pubic symphysis was radiologicallynormal but within a week rarefaction was detected(Figure 1 b) and an isotope bone scan revealed alocalized hot spot at the pubic symphysis (Figure2). Clinical examination, repeated urine examina-tion and two echocardiograms were otherwiseunremarkable.Her pain settled and antibiotics were therefore
discontinued after 25 days of therapy. The painrecurred three days later and the CRP was 44 mg/l.In view of this flucloxacillin and fusidic acid wererestarted and continued until not only her symp-toms had resolved but the CRP had fallen to lessthan 10 mg/l. This was achieved after a further 31days of therapy. Following cessation of antibioticsthere were no clinical signs of recurrence of infec-tion. Rehabilitation continued and she was dis-charged from hospital in August 1989, and hasremained well.
Discussion
The coagulase-negative staphylococci are an ubi-quitous group of bacteria that colonize the skin,particularly in areas of excessive surface humiditysuch as the groin, axilla and perineum. They
Correspondence: I. Sturgess, B.Sc., M.R.C.P.Accepted: 24 May 1993
copyright. on M
ay 22, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.69.818.927 on 1 D
ecember 1993. D
ownloaded from

928 I. STURGESS et al.
a
b
Figure 1 Radiographic appearance of pubic symphysis. (a) Normal appearance and (b) demonstrating areas ofrarefaction (arrows) consistent with pubic osteomyelitis.
copyright. on M
ay 22, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.69.818.927 on 1 D
ecember 1993. D
ownloaded from

PUBIC OSTEOMYELITIS 929
Figure 2 Isotope bone scan. Increased uptake in theregion of the pubic symphysis.
include many species of which the commonest isS. epidermidis. In the past, few laboratoriesspeciated coagulase-negative staphylococci andeither reported them as coagulase-negative staphy-lococci or S. epidermidis (senu lato) or even S. albus.Techniques for speciation became available in theearly 1 980s and routine identification of coagulase-negative staphylococcus is now possible. Therehave been occasional recent reports of infectionscaused by S. simulans, including native valveechocarditis' 3 and urinary tract infections,' whichsuggest that S. simulans is an important if rarecause of significant infection. In common withS. lugdunensis, a recently described species ofcoagulase-negative staphylococcus, S. simulans cancause severe infections that are more usuallyassociated with S. aureus than with coagulase-negative staphylococci.
Less than 1% of community-acquired bacter-aemias are caused by coagulase-negativestaphylococci (St Thomas' Hospital figures) andsuch patients usually have endocarditis
occasionally with concomitant vertebral osteo-myelitis. Endocarditis can be notoriously difficultto diagnose, particularly in the elderly, and canpresent with a stroke. The stroke in this patient hadoccurred some 9 months before the development ofpubic osteomyelitis and the CRP on presentationwas normal. Endocarditis was also thought to havebeen excluded by two normal echocardiograms,negative urine microscopy and no clinical stigmata.
Positive blood cultures and a raised CRP withthe clinical picture described was virtually diagnos-tic of pubic osteomyelitis and biopsy was notconsidered justified.
S. simulans is occasionally found as part of thenormal skin flora and it is of relevance that she hada psoriatic lesion on her scalp. She had alsoreceived a steroid injection into the right adductortubercle 4 months before the development of pubicosteomyelitis.
Pubic osteomyelitis has been reported inpreviously fit children,5 and intravenous drugabusers.6 In the elderly it usually follows genito-urinary procedures,7 and Gram-negative organ-isms predominate.
S. simulans has been responsible for only eightepisodes of bacteraemia in patients (including thiscase) at St Thomas' Hospital since 1970 (S. Eykyn,personal communication). Six of these have beenhospital-acquired infections, three associated withintravenous lines, one catheter-associated urinarytract infection and one wound infection. All sixstrains were resistant to beta-lactam antibiotics.One episode of S. simulans bacteraemia was com-munity acquired. This involved a 63 year old manwho had native valve endocarditis, whose strain,like that of the case presented, was fully sensitive.This patient required emergency valve replace-ment.To our knowledge, this is the first case of pubic
osteomyelitis caused by S. simulans and demon-strates, firstly, the insidious nature of osteomyelitisin the elderly and, secondly, the pathogenic poten-tial of coagulase-negative staphylococci other thanS. epidermidis.
References
1. Winston, D.J., Dudnick, D.V., Chapin, M., Ho, W.G., Gale,R.P. & Martin, W.J. Coagulase-negative staphylococcalbacteraemia in patients receiving immunosuppressive therapy.Arch Intern Med 1983, 143: 32-36.
2. McCarthy, J.S., Stanley, P.A. & Mayall, B. A case ofStaphylococcus simulans endocarditis affecting a native heartvalve. J Infection 1991, 22: 211-212.
3. Jansen, B., Schmacher-Perdreau, F., Peters, G., Reinhold, G.& Schonemann, J. Native valve endocarditis caused byStaphylococcus simulans. Eur J Clin Microbiol Infect Dis 1992,11: 268-269.
4. Iwantscheff, A., Kuhen, E. & Brandis, H. Species distributionof coagulase-negative staphylococci isolated from clinicalsources. Zbl Bakt Hyg A 1985, 260: 41-50.
5. Heldrich, F. & Harris, V. Osteomyelitis of the pubis. ActaPaediatr Scand 1979, 68: 62-67.
6. Sequira, W., Jones, E., Siegel, M.E., Lorenz, M. & Kallick, C.Pyogenic infections of the pubic symphysis. Ann Intern Med1982, 96: 604-606.
7. Bouza, E., Winston, D.J. & Hewitt, W.L. Infectious osteitispubis. Urology 1978, 12: 663-669.
copyright. on M
ay 22, 2021 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.69.818.927 on 1 D
ecember 1993. D
ownloaded from