Embed Size (px)
Citation preview

PTCA following myocardial infarction: Use of bailout fibrinolysis to improve results
The results of percutaneous transluminal coronary angioplasty (PTCA) in 307 lesions in 235 patients within 60 days of myocardial infarction (MI) were compared with the PTCA results in 591 lesions in 469 patients without recent MI, and the effect of fibrinolysis to treat recurring occlusive clot during angioplasty was studied. In 210 lesions in patients with MI who did not receive fibrinolysis during the MI (group A), 56 lesions were categorized as primary failures; bailout fibrinolysis brought the final failure incidence to 42 lesions (20%). In 97 lesions in patients with MI who received fibrinolysis during the acute MI (group B), 22 lesions were categorized as primary failures; bailout fibrinoiysis resulted in final failures of 16 lesions (16.5%). In 591 lesions in patients without a recent Ml (group C), there were 65 primary failures and 61 final failures after bailout fibrinolysis. Analysis of the PTCA results in each group with respect to whether the lesions were totally or partially occluded showed that more of the lesions attempted in the groups with MI (groups A and B) were totally occluded (TO) and that with use of bailout fibrinolysis the success rate of PTCA in TO lesions was the same In all groups. Similarly, with use of fibinolytic bailout during PTCA the success rate in partially occlusive lesions was not different between the groups. We conclude that bailout thrombolysis during PTCA is usually effective, especially in those who have recently had an MI, and that with availability of bailout flbrinolysis, PTCA in those with recent Ml is not any less successful than in those without recent Ml. The failure rate seems higher only because more patients with recent Ml have total occlusions and totally occluded vessels have a higher incidence of PTCA failure regardless of the presence or absence of a recent Ml. (AM HEART J 1990;120:243.)
Jacob I. Haft, MD, Jonathan E. Goldstein, MD, Munther K. Homoud, MD, and Michael Aaronoff. Newark, N. J.
Recent studies have shown that performance of an- gioplasty during the peri-infarction period is associ- ated with a high complication rate. Totally occluded vessels that cannot be crossed with a percutaneous transluminal coronary angioplasty (PTCA) balloon are commonly encountered, and in those lesions crossed and dilated, the incidence of recurrent throm- bosis during the procedure is high.l* 2 We report our results of PTCA during the postinfarction period and our use of “bailout” intracoronary fibrinolysis to im- prove the success rate of PTCA in these patients.
METHODS
Patients. We reviewed the angiopasty procedures on 898 lesions in 724 patients who underwent angioplasty at St. Michael’s Medical Center (SMMC) from 1981 to July 1989. The patients were classified as post myocardial infarction
From the Department of Cardiology at St. Michael’s Medical Center.
Received for publication Feb. 9, 1990, accepted March 28, 1990.
Reprint requests: Jacob I. Haft, MD, Department of Cardiology, St. Michael’s Medical Center, 268 King Blvd., Newark, NJ 07102.
4/l/21180
(MI) patients if they underwent PTCA within 60 days of an MI (307 lesions in 235 patients). Findings in this group were compared with those in patients who had not sus- tained an MI within 60 days of PTCA (591 lesions in 489 patients). The patients in both groups were subclassified into patients who had totally occluded lesions and those with subtotally occluded vessels. The patients with recent MI were further divided into those who had received intravenous fibrinolysis during the acute MI and those who did not.
Procedure. All angioplasties were performed by the same operator (J.G.) using the Judkins or Sones technique with standard left anterior oblique (LAO), right anterior oblique (RAO), and with modified cephalad and caudad views. The grading of the lesions and assessment of the PTCA procedure was performed by the same operator, and by at least one other author. Standard balloon catheters, guiding catheters, and guide wires were used and were continually changed as more sophisticated equipment be- came available between 1981 and 1989.
Bailout fibrinolysis was performed using steptokinase (Kabikinase, KabiVitrum AB, Stockholm, Sweden) 150,000 to 600,000 units administered via the intracoronary route over 1 hour or with tissue plasminogen activator (t-PA) (Activase, Genentech, Inc., South San Francisco, Calif.)
243
244 Haft et al. August 1990
American Heart Journal
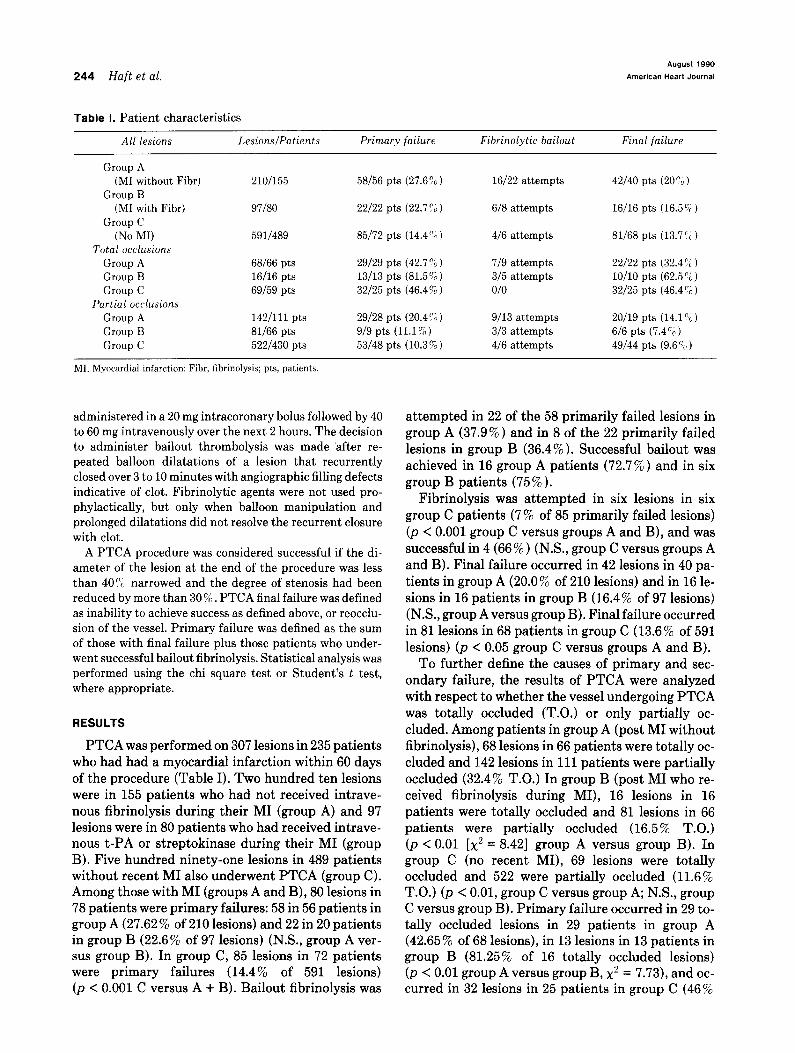
Table I. Patient characteristics
All lesions Lesions/Patients Primary failure Fibrinolytic bailout Final failure
Group A (MI without Fibr)
Group B (MI with Fibr)
Group C (No MI)
Total occlusions Group A Group B Group C
Partial occlusions Group A Group B Group C
210/155
97180
5911489
68166 pts 16/16 pts 69159 pts
142/111 pts 81166 pts 522/430 pts
58/56 pts (27.6%) 16/22 attempts
22/22 pts (22.7%) 6/8 attempts
85/72 pts (14.4%)
29/29 pts (42.7 “;J ) 13/13 pts (81.5%~) 32/25 pts (46.4%)
29/28 pts (20.4%) 9/9 pts (11.1 Z) 53/48 pts (10.3 ‘;;> 1
4/6 attempts
719 attempts 3/5 attempts o/o
9/13 attempts 3/3 attempts 4/6 attempts
42/40 pts (20% 1
16/16 pts (16.5%)
81/68 pts (13.7’<#)
22/22 pts (32.41&) lO/lO pts (62.5%) 32/25 pts (46.4%)
20/19 pts (14.1 “C ) 6/6 pts (7.45) 49/44 pts (9.6 ‘;a )
MI, Myocardial infarction: Fibr, fibrinolysis; pts, patients.
administered in a 20 mg intracoronary bolus followed by 40 to 60 mg intravenously over the next 2 hours. The decision to administer bailout thrombolysis was made ‘after re- peated balloon dilatations of a lesion that recurrently closed over 3 to 10 minutes with angiographic filling defects indicative of clot. Fibrinolytic agents were not used pro- phylactically, but only when balloon manipulation and prolonged dilatations did not resolve the recurrent closure with clot.
A PTCA procedure was considered successful if the di- ameter of the lesion at the end of the procedure was less than 40% narrowed and the degree of stenosis had been reduced by more than 30 % . PTCA final failure was defined as inability to achieve success as defined above, or reocclu- sion of the vessel. Primary failure was defined as the sum of those with final failure plus those patients who under- went successful bailout fibrinolysis. Statistical analysis was performed using the chi square test or Student’s t test, where appropriate.
RESULTS
PTCA was performed on 307 lesions in 235 patients who had had a myocardial infarction within 60 days of the procedure (Table I). Two hundred ten lesions were in 155 patients who had not received intrave- nous fibrinolysis during their MI (group A) and 97 lesions were in 80 patients who had received intrave- nous t-PA or streptokinase during their MI (group B). Five hundred ninety-one lesions in 489 patients without recent MI also underwent PTCA (group C). Among those with MI (groups A and B), 80 lesions in 78 patients were primary failures: 58 in 56 patients in group A (27.62 % of 210 lesions) and 22 in 20 patients in group B (22.6% of 97 lesions) (N.S., group A ver- sus group B). In group C, 85 lesions in 72 patients were primary failures (14.4% of 591 lesions) (p < 0.001 C versus A + B). Bailout fibrinolysis was
attempted in 22 of the 58 primarily failed lesions in group A (37.9%) and in 8 of the 22 primarily failed lesions in group B (36.4% ). Successful bailout was achieved in 16 group A patients (72.7%) and in six group B patients (75%).
Fibrinolysis was attempted in six lesions in six group C patients (7% of 85 primarily failed lesions) (p < 0.001 group C versus groups A and B), and was successful in 4 (66 % ) (N.S., group C versus groups A and B). Final failure occurred in 42 lesions in 40 pa- tients in group A (20.0% of 210 lesions) and in 16 le- sions in 16 patients in group B (16.4% of 97 lesions) (N.S., group A versus group B). Final failure occurred in 81 lesions in 68 patients in group C (13.6% of 591 lesions) (p < 0.05 group C versus groups A and B).
To further define the causes of primary and sec- ondary failure, the results of PTCA were analyzed with respect to whether the vessel undergoing PTCA was totally occluded (T.O.) or only partially oc- cluded. Among patients in group A (post MI without fibrinolysis), 68 lesions in 66 patients were totally oc- cluded and 142 lesions in 111 patients were partially occluded (32.4% T.O.) In group B (post MI who re- ceived fibrinolysis during MI), 16 lesions in 16 patients were totally occluded and 81 lesions in 66 patients were partially occluded (16.5% T.O.) (p < 0.01 [x2 = 8.421 group A versus group B). In group C (no recent MI), 69 lesions were totally occluded and 522 were partially occluded (11.6 % T.O.) (p < 0.01, group C versus group A; N.S., group C versus group B). Primary failure occurred in 29 to- tally occluded lesions in 29 patients in group A (42.65% of 68 lesions), in 13 lesions in 13 patients in group B (81.25% of 16 totally occluded lesions) (p < 0.01 group A versus group B, x2 = 7.73), and oc- curred in 32 lesions in 25 patients in group C (46%

Volume 120
Number 2 Bailout fibrinolysis in PTCA after AMI 245
of 69 totally occluded lesions) (p < 0.025 group C versus group B, x2 = 6.26; N.S., group C versus group A). Among patients with recent MI (groups A and B), primary failure was due to inability to cross the lesion in 21 lesions and to thrombus in 18 lesions (three due to other causes); in group C, the primary failure was due to inability to cross the lesion in 27 instances, to thrombus in two, and to other causes in three. (Group C versus groups A and B, p < .Ol; x2 = 9.41 for thrombus.)
Bailout with fibrinolysis was attempted in 9 of the 29 primarily failed T.O. lesions in group A and was successful in seven (77%), was attempted in 5 of the 13 primarily failed T.O. lesions in group B, was suc- cessful in three failed T.O. lesions (60%) (NS group A versus group B), and was not attempted in any of the primarily failed T.O. lesions in group C. The final failure rate in T.O. lesions in group A was 32.4% (22 of 68), in group B it was 62.5 % (10 of 16), and in group C it was 46% (32 of 69) 0, < 0.025 group A versus B [x2 = 5.1251; NS, A versus C; NS, B versus C).
In partially occluded vessels in group A, 29 lesions were primary failures, (20.4% of 142 partially oc- cluded lesions), in group B, nine partially occluded lesions were primary failures (11.11% of 81 lesions) (NS group A versus group B), and in group C, 53 partially occluded lesions were primary failures (10.2% of 522 lesions) (p < 0.01 [x2 = 9.911 group A versus C; NS, group B versus C). Bailout fibrinolysis was attempted in 13 partially occluded vessels in group A (44.8% of 29 primarily failed PTCAs) in three partially occluded vessels in group B (33% of nine primarily failed PTCAs) (NS Group A versus B), and in six partially occluded vessels in group C (11.3% of 53 failed PTCAs) (p < 0.001 group A ver- sus C [x2 = 11.551; NS, group A versus B; p < .OOl, C versus A and B [x2 = 11.401).
Bailout fibrinolysis was successful in nine of the failed PTCAs in partially occluded vessels in group A (69% of 13 attempts), in three of the failed PTCAs in partially occluded vessels in group B (100% of three attempts) and in four of the failed PTCAs in partially occluded vessels in group C (66% of six at- tempts) (NS between groups A, B, and C). Final fail- ure rate of partially occluded vessels in group A was 14.1% (20 of 142 lesions), in group B it was 7.4% (6 of 81 lesions), and in group C it was 9.4% (49 of 522 lesions) (NS, A versus B, A versus C, B versus C, and C versus A and B).
Complications occurred in 23 group A patients, in 12 group B patients, and in 58 group C patients (Ta- ble II). In group A there were four deaths, five emer- gency coronary artery bypass grafting (CABG) pro- cedures (one died), and three reclosures without
Table II. Complications
Group A Group B Group C 210 lesions 97 lesions 591 lesions
155 pts 80 pts 489 pts
Death 4 0 2 Emergency CABG 5 4 16 Elective CABG 4 1 17 Reclosure without CABG 3 3 2 New MI 2 0 3 V Fib 2 1 1 Groin pseudoaneurysm 1 1 3 Distal clot embolization 1 0 1 Groin hematoma 2 0 8 GI Bleed/CHF/Renal 1 1 2 Groin Staph infection 0 0 1 Other 0 1 2
CABG, Coronary artery bypass grafting (surgery); V Fib, ventricular fibril- lation; GI, gastrointestinal; CHF, congestive heart failure; Staph, Staphy- lococcus sp; other abbreviations as in Table I.
CABG (one small MI), two MIS, and four elective CABG procedures. In group B there were no deaths, four emergency CABG procedures, three reclosures without CABG, and one elective CABG procedure. In group C there were two deaths, 16 emergency CABG procedures, two reclosures without CABG, and 17 elective CABG procedures. There were no significant differences between those with recent MI and those without a recent MI in the incidence of any of these complications.
DISCUSSION
The realization that most MIS are due to acute thrombotic occlusion of a coronary artery3 and the availability of PTCA and of prompt fibrinolysis with intravenous medications has led to a number of pos- sible treatments of patients with myocardial infarction.4p 5 These have included immediate PTCA during acute MI without fibrinolysis,61 7p 8, lo fibrinol- ysis alone,g fibrinolysis plus PTCA for failed patients,14 fibrinolysis plus routine immediate PTCA,11-13 fibrinolysis plus PTCA only in those with symptoms or signs of ischemia (angina or positive stress test),15 or fibrinolysis plus routine remote PTCA in those without early ischemia. Many of these regimens have been tried in randomly assigned patients, and currently after the Thrombolysis In Myocardial Infarction (TIMI) and Thrombolysis and Angioplasty in Myocardial Infarction (TAMI) stud- ies, it is felt that the best strategy is to utilize intra- venous fibrinolysis in all possible patients, to do PTCA immediately only in those who fail fibrinolysis or in whom fibrinolysis is contraindicated and who remain symptomatic, and to do PTCA later only in
246 Haft et al. August 1990
American Heart Journal
those who have ischemic symptoms or a strongly positive stress test. 15s l6 This leaves many patients after fibrinolysis with high-grade lesions or totally occluded vessels who are not even studied with cor- onary arteriography. Follow-up data at 1 year sug- gests that those without symptoms who are managed noninvasively do as well as those who have PTCA,17 although there is an accumulating body of data that suggests that patients after an MI fare better if the artery associated with the area of infarction has been left patent. i2j 18, lg. 22, 23 In all of the controlled stud- ies involving PTCA in the early postinfarction pe- riod, there has been a high incidence of unsuccessful or complicated angioplasty-higher than that usu- ally encountered in patients who have had PTCA who did not have a recent MI.13, 16, so This has largely led to the finding that noninvasive management- rather than PTCA-carries with it a better result. The higher failure rate of PTCA soon after MI has been felt to be due partly to reocclusion after dilatation,15 because perturbation of a fresh lesion that is frequently complex and is associated with clot can lead to recurrence of clot and occlusion; i.e., breaking up a clot or disturbing a recently ulcerated plaque creates a situation that is highly locally thrombogenic. 21 Because of this possibility, for sev- eral years now we have been using fibrinolytic agents in the catheterization laboratory in primarily failed PTCA if there was evidence that clot was playing a significant role. To study the causes for failure in pa- tients with a recent MI, we reviewed our PTCA pa- tients, comparing those with recent MI with those without recent MI. On examining the primary failure rate in patients according to the time after MI, we found that primary failure was common up to 60 days after MI, but thereafter the rate was the same as without MI. We compared those with MI < 60 days prior to PTCA with those without recent MI.
Like other investigators, we have also found that patients treated with PTCA within 60 days of an MI are at significantly greater risk of primary PTCA failure than patients who have not had a recent MI 20, 24 regardless of whether fibrinolysis had been use’d during the acute MI. The use of bailout fibrin- olysis narrows the difference in percentage of final failures between those with and those without recent MI, but the difference remains significant (18.9% versus 13.8% ).
The difference in the success rate between those with and those without recent MI was partly due to the significantly increased incidence of totally oc- cluded vessels that were subjected to attempted PTCA in the recent MI patients (27.4% versus 11.6% ). This may have been due to the expectation
that T.O. lesions in patients with recent MI might be more likely due to clot and thereby might be softer, more easily crossed, and more easily opened. The fact that those with recent MI had fewer failures because of the inability to cross the lesion suggests that this indeed may have been true. Those who had had thrombolysis during their MI had a lesser incidence of T.O. than those with recent MI who had not had fibrinolysis at the time of infarction, probably be- cause the occluding clot had been lysed in most instances. The primary failure rate of T.O. lesions was about the same in patients with and in those without recent MI, although those with T.O. who had had fibrinolysis during MI had a higher primary fail- ure rate than those without fibrinolysis, possibly be- cause the lesions left totally occluded after fibrinol- ysis might have been harder and therefore less easy to cross and to open with a balloon.
As expected, the cause for primary failure was dif- ferent between those with and those without a recent MI. In those without MI, 27 of 32 primary failures were due to the inability to cross the occluding lesion with a balloon and only two were due to thrombus formation, whereas in those with a recent MI, only 21 of 42 unsuccessfully attempted lesions were primary failures because of the inability to cross the lesion, but 18 of the 42 failed lesions were due to recurrent thrombus. Hence use of bailout fibrinolysis was more often appropriate and was more often used in 14 le- sions with recent MI (successful in 10 lesions) but was used in none of those without recent MI. Final fail- ure occurred in fewer T.O. lesions with a recent MI than in those without a recent MI.
In patients with partially occluded vessels, the primary failure rate was greater among those with recent MI, but with bailout fibrinolysis the final fail- ure rate was about the same whether there was a re- cent MI or not. There was no significant difference in deaths, emergency or elective CABG, or other com- plications between those with or those without recent MI. Hence with the use of bailout fibrinolysis, the success rate of PTCA is the same in partially oc- cluded vessels with or without MI. Also, with the use of bailout fibrinolysis, the final success rate of PTCA in totally occluded vessels is about the same whether there is a recent MI or not; if anything, there is a trend toward more success in patients who have had a recent MI. However, the rate of final failure remains significantly higher in those with recent MI com- pared with those without MI, because: (1) the final failure rate in T.O. lesions is always higher than in partially occluded lesions and (2) the incidence of T.O. lesions attempted with PTCA in patients with recent MI is very much higher than in patients with-

Volume 120
Number 2 Bailout fibrinolysis in PTCA after AMI 247
out MI. This latter higher incidence of T.O. lesions is the only reason that the net final failure rate in recent MI patients is higher than the net final failure rate in patients without recent MI, if bailout fibrinolysis is available (Table I).
In conclusion, we have found that if bailout fibrin- olysis is used during a PTCA procedure to open ves- sels closed with thrombus after dilatation, the inci- dence of PTCA failure in partially occluded vessels and in totally occluded vessels is the same whether the patient has had a recent MI or not. However, be- cause the failure rate is higher in totally occluded vessels than in partially occluded vessels regardless of whether there has been recent infarction, and be- cause totally occluded vessels are subjected to at- tempted PTCA more often in patients who have had a recent MI, the incidence of PTCA failure is higher in patients who have had recent MI.
REFERENCES
1.
2.
3.
4.
5.
6.
I.
8.
The TIM1 Research Group. Immediate vs delayed catheter- ization and angioplsty following thrombolytic therapy for AMI. TIM1 IIA. JAMA 1988;260:2849-58. Top01 EJ, Califf RM, George BS, Kereiakes DJ, Abbottsmith CW, Candella RJ, Lee KL, Ptts B, Stack RS, O’Neill WW, and the Thrombolysis and Angioplasty in Myocardial Infarction study group. A randomized trial of immediate vs. delayed elective angioplasty after IV TPA in AMI. N Engl J Med 1987;317:581-8. DeWood MA, Spares J, Natke R, Mouser LT, Burroughs R, Golden MS, Lang HT. Prevalence of total coronary occlusion during the early hours of transluminal MI. N Engl J Med 1980;303:897-902. Rentrop PK. Thrombolytic therapy in patients with acute MI. Circulation 1985;71:627-31. Grouppo Italian0 Por Lo Studio Della Streptochinase Nell Infarto Miocardico (GISSI). Effectiveness of IV thrombolytic treatment in acute MI. Lancet 1986;1:397-402. Kimura T, Nosaka H, Veno K, Nobuyoshi M. Kokura Memo- rial Hospital, Japan. Role of coronary angioplasty in acute MI. Circulation 1986:74(sunnl II):ll-22. Rothbaum DA, Linnemeier ‘TJ, Landin RJ, Steinmetz EF, Hillis JS, Hallam CC, Noble J, See MR. Emergency PTCA in acute MI. J Am Co11 Cardiol 1987;10:264-72. Marco J, Caster L, Szatmary LJ, Fajadet J. Emergency PTCA with thrombolysis as initial therapy in acute MI. Int J Carcliol 1987;15:55-63.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Special Report TIM1 Study Group. Phase 1 findings. N Engl J Med 1985;312:932-6. Prida XA, Holland JP, Feldman RL, Hill JA, MacDonald RG, Conti CR, Pepine CJ. PTCA in evolving acute MI. Am J Car- diol 1986;57:1069-74. Simons ML, Betrie A, Co1 J, Essen R, Lubsen J, Michel PL, Rutsch W, Schmidt W, Thery C, Vahanian A, Williams GM, Arnold AER, deBono DP, Dougherty FC, Lambertz H, Meier B, Raynaud P, Sanz GA, Serruys PW, Vebis R, Van der Werf F, Wood D, Verstraete M. Thrombolysis with tissue plas- minogen activator in acute MI: no additional benefit from im- mediate percutaneous coronary angioplasty. Lancet 1988; 1:197-203. Fung AY, Lai F, Top01 EJ, Bates ER, Douidillon P, Walton JA, Mancini GB, Kryski T, Pitt B, O’Neill WW. Value of PTCA after unsuccessful IV streptokinase therapy in acute MI. Am J Cardiol 1986;58:686-91. The TIM1 Study Group. Comparison of invasive and conser- vative strategies after treatment with IV TPA in acute MI (TIM1 II). N Engl J Med 1989;320:618-27. Califf RM, Top01 EJ, George BS, Boswick JM, Lee KL, Stump D, Dillon J, Abbottsmith C, Candela RJ, Kereiakes DJ, O’Neill WW, Stack RS, and the TAM1 Study Group. Characteristics and outcome of patients in whom reperfusion with intravenous tissue-type plasminogen activator fails: results of the Throm- bolysis and Angioplasty in Myocardial Infarction (TAM1 I trial). Circulation 1988;77:1090-9. Guerci AD, Gerstenblith G, Brinker JA, Chandra NC, Gottlieb SO, Bahr RD, Weiss JL, Shapiro EP, Flaherty JT, Bush DE, Chew PH, Gottlieb SH, Halperin HR, Ouyang P, Walford GD, Bell WR, Fatterpaker AK, Llewellyn M, Top01 EJ, Healy B, Siu CO, Becker LC, Weisfeldt ML. A randomized trial of IV TPA for AM1 with subsequent randomization to elective cor- onary angioplasty. N Engl J Med 1987;317:1613-8. Erbel R, Pop T, Treese N, Diefenbach C, Meyer J. Long-term follow-up after thrombolysis therapy with and without PTCA in MI. Circulation 1987;76 (suppl IV):IV-181. Davies MJ, Thomas AC. Plaque fissuring the cause of acute MI, sudden ischemic death and crescendo angina. Br Heart J 1985;53:363-73. Califf RM, Topal EJ, Kereiakes DJ, George BS, Abbottsmith CW, Candella RJ, Aronson L, Pitt B, Lee KL, and the TAM1 Study Group. Long-term outcome in the Thrombolysis and Angionlastv in Mvocardial Infarction trial. Circulation 1987:76
- . < I
(suppl IV):IV-260. Stack RS, Califf RM, Hinohara T, Phillips HR, Pryor DB, Si- monton CA, Carlson EB, Morris KG, Behar VS, Kong Y, Pe- ter RH. Hlatkv MA. O’Connor CM. Mark DB. Survival and
* I
cardiac event rates in the first year after emergency coronary angioplsty for acute myocardial infarction. J Am Co11 Cardiol I _ 1988;11:1i41-9. Meyer J, Merx W, Dorr R, Erbel R, vonEssen R, Lambertz H, Bethge C, Schmitz HJ, Bardos P, Minale C. Sequential inter- vention procedures after IC thrombolysis, balloon dilatation, bypass surgery and treatment. Int d Cardiol 1985;7:287-93.